Sepsis Lisa Cabrera, Kat Pugh, & SWizel. Sepsis Statistics Severe sepsis is a significant global...
21
Sepsis Lisa Cabrera, Kat Pugh, & SWizel
-
Upload
cathleen-pierce -
Category
Documents
-
view
215 -
download
2
Transcript of Sepsis Lisa Cabrera, Kat Pugh, & SWizel. Sepsis Statistics Severe sepsis is a significant global...

Sepsis
Lisa Cabrera, Kat Pugh, & SWizel

Sepsis Statistics
Severe sepsis is a significant global medical problem
● 750,000+ reported cases in the US● 19,000,000+ reported cases worldwide● 10% of all ICU admissions ● 20-30% mortality rate ● Shock develops in 40% of septic patients● Survivors exhibit significant dysfunction &
increased risk of death

Infection or Trauma
SIRS SepsisSevere Sepsis
Septic Shock
DICMODS

Infection Focal Infection – microorganism invades susceptible host tissues and initiates an inflammatory response
● Common routes of entry: o contaminated inhalation therapy equipment, peripheral IV sites,
central lines, indwelling urinary catheters, open wounds, and surgical sites
● Bacteria – most significant causative agent of sepsiso Gram positive – more than half of all sepsis cases o Gram negative – less than half of all sepsis cases, but most lethal
● Protozoa, fungi, virus – much less common

Bacteremia → SIRSBacteremia – focal bacterial infection progresses to the bloodstream and becomes a systemic infection
● due to weakened host defenses● elderly, neonates, immunocompromised
SIRS – A generalized uncontrolled inflammatory reaction involving cellular, humoral, compliment, and cytokine activity, in response to a major infection, trauma, or insult to the body. SIRS can be diagnosed by the presence of two or more vital sign markers:
● Temp > 38ºC● HR > 90 BPM● RR > 20 BPM or PaCO2 < 32 mmHg● WBC > 12,000 or immature cells (Bands) > 10%

SIRS → SepsisDiagnostic Criteria for Sepsis – Uncontrolled systemic inflammation (SIRS) and the presence of an infectious bacterial agent in the bloodstream (bacteremia).

Sepsis → Severe Sepsis
[Severe Sepsis = sepsis + 1 organ failure]
Any of the following that is a change from baseline: - Respiratory: SpO2 < 90% or increasing O2 requirement- Cardiovascular: SBP < 90 mmHg, MAP < 65 mmHg, or SBP drop
> 40 mmHg from baseline- Renal: urine output < 0.5 mL/kg/hr or creatinine increase > 0.5
mg/dL from baseline- Hematologic: platelets < 100,000 or INR > 1.5- Hepatic: serum total bilirubin > 2 mg/dL or elevated LFTs- Metabolic: lactate > 2.0 mmol/L

Severe Sepsis → Septic Shock[Septic Shock = sepsis + hypotension despite fluid resuscitation along w/ the presence of inadequate tissue perfusion resulting in hypoxia]
In septic shock, blood vessels can no longer constrict sufficiently to maintain an adequate blood pressure. Three processes contribute to the unresponsiveness of the arterial wall muscles in septic shock:● High levels of lactic acid hyperpolarize the arterial muscle cells, making
them unable to respond when stimulated.● Sepsis suppresses the release of vasopressin (ADH), a pituitary hormone
that, among other functions, maintains arterial wall muscle tone.● Sepsis causes endothelial cells to produce excess nitric oxide, which is a
vasodilator.

Septic Shock → DIC & MODS

DIC & MODS
Sepsis is almost invariably associated with haemostatic (retarding or stopping the flow of blood within the blood vessels ) abnormalities ranging from subclinical activation of blood coagulation (hypercoagulability), which may contribute to localized venous thromboembolism, to acute disseminated intravascular coagulation
(DIC), characterized by massive thrombin formation and widespread microvascular thrombosis, partly responsible of the
multiple organ dysfunction syndrome (MODS)

DIC (Disseminated Intravascular Coagulation)
● Consumption of platelets and coagulation proteins causing, in most severe cases, bleeding manifestations
● The key event underlying this life-threatening sepsis complication is the overwhelming inflammatory host
● Leading to the overexpression of inflammatory mediators
● Mechanistically, the latter, together with the micro-organism and its derivatives, causes DIC

DIC● Platelet activation, enhancing aggregation and augmenting platelet
functions in coagulation
● Activation of factors VIII, V, and XI, yielding further thrombin generation
● Enhanced activation of proinflammatory factors via protease-activated receptors (PARs)
● Activation of factor XIII to factor XIIIa, which augments production of fibrin clots from fibrinogen
● Activation of thrombin-activatable fibrinolysis inhibitor (TAFI), making clots resistant to fibrinolysis
● Enhanced expression of adhesion molecules (eg, L-selectin), thereby promoting the inflammatory effects of white blood cells (WBCs)
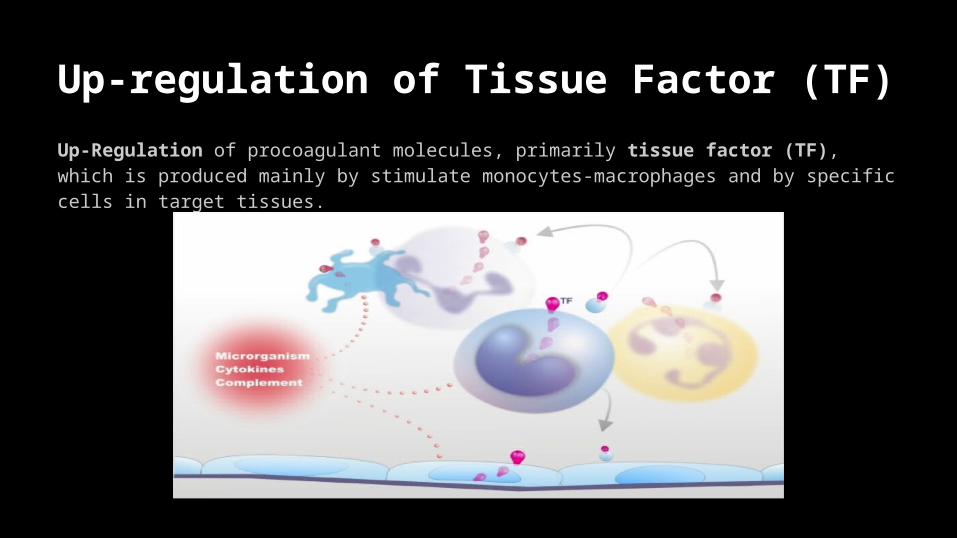
Up-regulation of Tissue Factor (TF)
Up-Regulation of procoagulant molecules, primarily tissue factor (TF), which is produced mainly by stimulate monocytes-macrophages and by specific cells in target tissues.

Impairment of Physiological Anticoagulant Pathways Impairment of physiological anticoagulant pathways (antithrombin, protein C pathway, tissue factor pathway inhibitor), which is orchestrated mainly by dysfunctional endothelial cells (ECs).

Suppression of Fibrinolysis Suppression of fibrinolysis due to increased plasminogen activator inhibitor-1 (PAI-1) by ECs and likely also to thrombin-mediated activation of thrombin-activatable fibrinolysis inhibitor (TAFI).

MODS (Multi Organ Dysfunction Syndrome)
MODS is the presence of altered organ function in an acutely ill patient such that homeostasis cannot be maintained without intervention.● Primary MODS is the direct result of a well-defined insult in which
organ dysfunction occurs early and can be directly attributable to the insult itself.
● Secondary MODS develops as a consequence of a host response and is identified within the context of SIRS. The inflammatory response of the body to toxins and other components of microorganisms causes the clinical manifestations of sepsis.

MODS

Quick RecapInfection = presence of microorganism in host tissues
SIRS = microbial infection + 2 or more ↑ Temp, ↑ HR, ↑ RR, ↑ WBC
Sepsis = SIRS + known or suspected infection
Severe Sepsis = sepsis + 1 organ failure
Septic Shock = sepsis + hypotension despite fluid resuscitation
DIC = profuse bleeding + widespread thrombosis
MODS = acutely ill patient + failure of 2 or more organ systems + inability to maintain homeostasis

Infection or Trauma
SIRS SepsisSevere Sepsis
Septic Shock
DICMODS

ReferencesAngus, D., & van der Poll, T. (n.d). Severe sepsis and septic shock.
New England Journal Of Medicine, 369(9), 840-851. doi: 10.1056/NEJMra1208623.
Baird, M.S., Bethel, S. (2011). Manual of critical care nursing (6th ed.). St. Louis, MO: Mosby.
Urden, L.D., Stacy, K.M., Lough, M.E., (2014). Critical care nursing:
Diagnosis and management. (7th ed.) St. Louis,MO: Mosby.