Sepsis and Multiple Organ Failure - … en MODS.pdf · Sepsis and Multiple Organ Failure ......
31
Sepsis and Multiple Organ Failure J.G. van der Hoeven Radboud University Nijmegen Medical Centre
Transcript of Sepsis and Multiple Organ Failure - … en MODS.pdf · Sepsis and Multiple Organ Failure ......

Sepsis and Multiple Organ Failure
J.G. van der HoevenRadboud University Nijmegen Medical Centre

Microorganism
Sepsis - initiation
Pathogen Associated Molecular Pattern(PAMP)
Immune cell
Pattern Recognition Receptor(PRR)
Tissue Damage
Immune cell
Pattern Recognition Receptor(PRR)
Damage Associated Molecular Patterns(DAMP)
Inflammatory Response
Alarmins
= =

Pro-inflammatory cytokines/chemokines
Activation of endothelium + PMN migration
IL-17cytokine family
Activation of coagulation
Induction of “late” cytokines
HMGB-1 and MIFC5a
Adaptive immune response
+ +
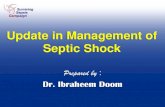
N = 1664
0
10
20
30
40
Mortality D28 Mortality D 90
32,7
24,2
34,1
26,4
Mor
talit
y (%
)
aPC Placebo
Ranieri VM. N Engl J Med 2012

Systolic and diastolicmyocardial dysfunction
Increased endothelial permeability
Excessive vasodilation
Venous pooling
Microcirculatory shuntingMitochondrial dysfunction

Vasodilatation in SepsisSeptic shock with lactate acidosis
iNO synthase ↑
NO ↑
cGMP ↑
Vasopressin secretion ↑
Vasopressin stores ↓
Vasopressin plasma ↓
ATP ↓, H+ ↑, Lactate ↑ vascular smooth muscle
Open KATPOpen KCa
Cytoplasmic Calcium ↓
Phosphorylated myosin ↓
Vasodilatation


IFN-Υ ± IL-10 ↑
IDO activity ↑
Tryptophan ↓ & kynurenine ↑
Increased KT ratio plasma
Lymphocyte apoptosis ↑
Microvascular reactivity ↓
IL-6 ↑e NO ↓
Darcey CJ. PLOSone 2011;6:e21185
N = 80

Changsirivathanathamrong D. Crit Care Med 2011;39:2678-2683
INOTROPIC DOSE
IDO ACTIVITY
N = 16

Changsirivathanathamrong D. Crit Care Med 2011;39:2678-2683

Treatment
• Early antibiotics and source control
• Volume therapy
• Increasing afterload with NE / vasopressin
• Inotropic agents
• Standard ICU treatment

HES 130/0.42 versus Ringer’s acetate
• Adult patients with severe sepsis
• MC (N = 26), blinded, stratified clinical trial
• HES 130/0.42 vs Ringer’s acetate
• Daily maximum dose 33 mL/kg IBW
• Primary outcome composite death/dialysis dependence at D90
Perner A. N Engl J Med 2012;367:124-134

HES 130/0.42 versus Ringer’s acetate
0
15
30
45
60
Death/DD Day 90 Death Day 90 Severe bleeding RRT
Ringer’s HES 130/042
P = 0.03 P = 0.03 P = 0.09 P = 0.04
No differences in total amount of fluid neededPerner A. N Engl J Med 2012;367:124-134

HES 130/0.4 versus NaCl 0.9%
CHEST trialMyburgh JA. N Engl J Med 2012;367:1901-1911

AKI and HES 130/0.4
0
2
4
6
8
10
RRT
7
5,8
Placebo HES 130/0.4
P = 0.04
Myburgh JA. N Engl J Med 2012;367:1901-1911

Lactate driven therapy
0
10
20
30
40
50
33,9
43,5
Mor
talit
y (%
)
Control Lactate driven
N = 348P = 0.067
Admission lactate ≥ 3 mmol/lGoal: lactate ↓ ≥ 20% in 2 hrs
• After correction for risk factors mortality lower in lactate group (HR 0.61, p = 0.006)
• Duration MV ↓, duration ICU stay ↓, lower SOFA score
Jansen TC. Am J Respir Crit Care Med 2010, 182:752-761

Anti-‐inflammatoryresponse
Time (days)
Pro-‐inflammatoryresponse
Homeostasis
A
Anti-‐inflammatoryresponse
Time (days)
Pro-‐inflammatoryresponse
Homeostasis
CDeath Death
Pro-‐inflammationAnti-‐inflammationBacterial load
Death
Pro-‐inflammatoryresponse
Anti-‐inflammatoryresponse
Time (days)
HomeostasisB

Immunoparalysis• Monocyte Class II MHC
expression ↓
• LPS-induced cytokine production ↓
• Lymphocyte apoptosis ↑
• T-reg dominant adaptive immune response
• Changes in lymphocyte phenotype
-100
-75
-50
-25
0
TNF-α IL-1β IL-12 IF-ϒ% c
ytok
ine
redu
ctio
n af
ter L
PS s
timul
atio
n

Draisma A. Crit Care Med 2009;37:1261-1267

Immunoparalysis
Spleen of septic and control patients

HLA-DR expression in patients with sepsis
Monneret G. Intensive Care Med 2006;32:1175-1182

Boomer JS. Crit Care 2012;16:R112
IFNγ secretion

Clinical evidence
• Low virulence bacterial infections
• CMV
• HS
• Aspergillus



Leentjes J. Am J Respir Crit Care Med 2012;186:838-845

GM-CSF treatment in sepsisPRCT N = 38
Meisel C. Am J Respir Crit Care Med 2009;180:640-648

Meisel C. Am J Respir Crit Care Med 2009;180:640-648
Decreased time on MV
Improvement in APACHE II score
Decrease in LOS (NS)Inte
rleu
kin-
10In
terl
euki
n-6
Inte
rleu
kin-
8T
NF-α
HLA
-DR

Important questions remain
• What should we administer?
• When should we administer?
• Which markers should we use?

• HLA-DR expression
• Cytokine production after ex-vivo stimulation
Skrupky LP. Anesthesiology 2011;115:1349-1362
What can be done?

Skrupky LP. Anesthesiology 2011;115:1349-1362
PD-1Negative costimulatory
molecule on Tcells

Conclusions
• Hemodynamic instability in sepsis is multi- factorial
• Starch products should be avoided
• Sepsis induced immunoparalysis may result in severe opportunistic infections
• Immunoparalysis may be reversed with IFN-γ, GM-CSF and IL-7




![Antithrombotic Agents in the Management of Sepsis · was observed in neonates and patients over 55 years of age[3]. Severe sepsis is defined as sepsis associated with acute organ](https://static.fdocuments.us/doc/165x107/5f0adc7d7e708231d42db367/antithrombotic-agents-in-the-management-of-was-observed-in-neonates-and-patients.jpg)
![Effects of dapagliflozin in experimental sepsis model in rats · for sepsis and 270 out of 100,000 for severe sepsis. [2] During the management of sepsis, organ failure must be carefully](https://static.fdocuments.us/doc/165x107/5e7a8e4d8250d6006254c4e5/effects-of-dapagliflozin-in-experimental-sepsis-model-in-rats-for-sepsis-and-270.jpg)