send each photograph or diagram as a - BRAVO - Menu€¦ · Veterinary School, a post that he held...
141
1 Committee members • Tim Knott (Chairperson) • Ida Gilbert (Chairperson to be) • Natasha Mitchell (Joint secretary) • Negar Hamzianpour (Joint secretary) • Helen Appleboam (Hotel and conference organiser) • Michael Ziglar (International liaison) • David Nutbrown-Hughes (Website and audio-visual) • Charlie Barton (Disease surveillance officer) • Rachael Grundon (Scientific programme) • Christine Heinrich (Scientific programme) • Chris Dixon (Scientific programme) • Mike Rhodes (Editor) • Jenny Lambert (Clinical auditor) • Rob Lowe/Alistair Oldfield (Treasurer) Publisher British Association of Veterinary Ophthalmologists. Enquiries should be directed to Mike Rhodes, Willows Referral Service, Highlands Road, Shirley, Solihull, West Midlands, B90 4NH. Tel: 0121 712 7070. Email: [email protected] Membership information Full membership is open to veterinary surgeons with an interest in the field of ophthalmology. Associate membership is open to those with professional interest in the field of ophthalmology. Membership is for 12 months and starts on 1 st April. Membership fees are £40 per year. Abstracts / lecture notes submission Please follow the guidelines below: • The first line should give the title. • The authors’ names should appear on the next line – initials followed by last name. • Provide the name of your practice / institution. • Use single spacing. • Use 10 point Trebuchet MS font for all text. • Photographs or diagrams are encouraged, but do not place them within the main body text. Instead send each photograph or diagram as a separate JPEG image with a title such as ‘Figure 1: The eye before surgery’. Up to four images may be included. If additional images are required, please discuss this in advance of the deadline. • The abstract should be 500-1000 words. • Please send in electronic format to [email protected] Deadlines Deadlines will be published on the website but are usually the first day of the month, two months prior to the meeting. Abstracts will be reviewed and the author notified one week after the submission deadline with time allowed for alterations if required. Twelve minutes will be allocated for each presentation, with a further three minutes for discussion. All oral presentations must be made in English. Presentations must be compatible with Microsoft PowerPoint 2003. Copyright and Photocopying © British Association of Veterinary Ophthalmologists 2017. All rights reserved. No part of this publication may be produced, stored or transmitted in any form or means without the prior permission in writing from the copyright holder. Advertising Enquiries about advertising should be directed to the Editor. Copies need to be received one month prior to the meeting for inclusion in the proceedings. Disclaimer The Publisher, the British Association of Veterinary Ophthalmologists and the Editor cannot be held responsible for errors or any consequences arising from the use of material contained in this journal. The views and opinions expressed do not necessarily reflect those of the Publisher or Editor; neither does publication of advertisements constitute any endorsement by the Publisher or the Editor of the products advertised.
Transcript of send each photograph or diagram as a - BRAVO - Menu€¦ · Veterinary School, a post that he held...

1
Committee members • Tim Knott (Chairperson) • Ida Gilbert (Chairperson to be) • Natasha Mitchell (Joint secretary) • Negar Hamzianpour (Joint secretary) • Helen Appleboam (Hotel and
conference organiser) • Michael Ziglar (International liaison) • David Nutbrown-Hughes (Website and
audio-visual) • Charlie Barton (Disease surveillance
officer) • Rachael Grundon (Scientific
programme) • Christine Heinrich (Scientific
programme) • Chris Dixon (Scientific programme) • Mike Rhodes (Editor) • Jenny Lambert (Clinical auditor) • Rob Lowe/Alistair Oldfield
(Treasurer) Publisher British Association of Veterinary Ophthalmologists. Enquiries should be directed to Mike Rhodes, Willows Referral Service, Highlands Road, Shirley, Solihull, West Midlands, B90 4NH. Tel: 0121 712 7070. Email: [email protected] Membership information Full membership is open to veterinary surgeons with an interest in the field of ophthalmology. Associate membership is open to those with professional interest in the field of ophthalmology. Membership is for 12 months and starts on 1st April. Membership fees are £40 per year. Abstracts / lecture notes submission Please follow the guidelines below: • The first line should give the title. • The authors’ names should appear on
the next line – initials followed by last name.
• Provide the name of your practice / institution.
• Use single spacing. • Use 10 point Trebuchet MS font for all
text. • Photographs or diagrams are
encouraged, but do not place them within the main body text. Instead
send each photograph or diagram as a separate JPEG image with a title such as ‘Figure 1: The eye before surgery’. Up to four images may be included. If additional images are required, please discuss this in advance of the deadline.
• The abstract should be 500-1000 words.
• Please send in electronic format to [email protected]
Deadlines Deadlines will be published on the website but are usually the first day of the month, two months prior to the meeting. Abstracts will be reviewed and the author notified one week after the submission deadline with time allowed for alterations if required. Twelve minutes will be allocated for each presentation, with a further three minutes for discussion. All oral presentations must be made in English. Presentations must be compatible with Microsoft PowerPoint 2003. Copyright and Photocopying © British Association of Veterinary Ophthalmologists 2017. All rights reserved. No part of this publication may be produced, stored or transmitted in any form or means without the prior permission in writing from the copyright holder. Advertising Enquiries about advertising should be directed to the Editor. Copies need to be received one month prior to the meeting for inclusion in the proceedings. Disclaimer The Publisher, the British Association of Veterinary Ophthalmologists and the Editor cannot be held responsible for errors or any consequences arising from the use of material contained in this journal. The views and opinions expressed do not necessarily reflect those of the Publisher or Editor; neither does publication of advertisements constitute any endorsement by the Publisher or the Editor of the products advertised.

2
SPEAKER BIOGRAPHIES
Chris Dixon BVSc Cert. VOphthal MRCVS
RCVS Advanced Practitioner in Veterinary Ophthalmology
Chris graduated from the University of Bristol and spent several years working in first opinion mixed practice in the North Yorkshire Moors and Cumbria. During his time at the University of Bristol Chris was lucky enough to be mentored by Professor Sheila Crispin, and this tuition inspired a persistent interest in ophthalmology. Early in his veterinary career, Chris decided to focus on ophthalmology due to the exciting mixture of microsurgery and medicine, and attained the RCVS postgraduate certificate. In 2010 Chris joined fellow ophthalmologist Gary Lewin, and in 2012 they formed Veterinary Vision, a dedicated ophthalmology referral practice based in Penrith, Cumbria. Chris has presented clinical research at national and international veterinary ophthalmology conferences, and has a particular interest in topographical analysis of the cornea and retinal reattachment surgery.
Jo Wolfer DVM ACVO
DVM Ontario Veterinary College, University of Guelph 1988 Internship Western College of Veterinary Medicine, Saskatoon, 1989 Residency in ophthalmology Ontario Veterinary College 1990-1992
American College of Veterinary Ophthalmologists 1994
American Society of Retina Specialists

3
Mr Malcolm Woodcock Consultant Ophthalmic Surgeon
BM MSc DAvMed MRCOphth FRCS(Ed)
Malcolm Woodcock is a consultant ophthalmologist and vitreoretinal surgeon who carries out his NHS work at Worcestershire Acute Hospitals NHS Trust. He set up and runs the vitreoretinal (VR) service in Worcestershire and is part of the wider regional vitreoretinal service based at the Birmingham and Midland Eye Centre (BMEC) at City Hospital in Birmingham. He is the nominated specialist in the Worcestershire for the referral cataract cases that have had complications and require further treatment. He specialises in the surgical treatment of complex cataracts as well as doing a high volume of routine cataract surgery himself. Mr. Woodcock also carries out a high volume of retinal surgery including macular hole repairs, peeling epiretinal membranes and retinal detachment repairs. In addition to his vitreoretinal work Mr. Woodcock is also a specialist in aviation medicine and from 2007 until 2014 was the head of Aviation Ophthalmology for the 3 armed Services (Fleet Air Arm, Army Air Corps and RAF). Mr. Woodcock speaks widely on ophthalmology and vitreoretinal surgery to other doctors and professional groups including optometrists, GPs and military medial officers. He also lectures on aviation ophthalmology regularly at the Royal Air Force's Centre for Aviation Medicine and King's College London, in particular on its internationally renowned Diploma of Aviation Medicine course. He has also been involved in teaching and lecturing to medical students at the universities of Cambridge, Birmingham, Cape Town and UCL. Mr. Woodcock has very active research interests with active collaboration with Moorfields Hospital in London and the Centre of Aviation Medicine at the test and evaluation centre RAF Boscombe Down. He has numerous publications in the medical literature and given many presentations at both national and international meetings. He is a reviewer of papers for 4 international scientific journals in ophthalmology.

4
John Goulding BVMS (Hons) MRCVS
Group Veterinary Advisor INDEPENDENT VETCARE
John Goulding graduated with honours from Glasgow in 1989 and until joining IVC last year, worked at St George’s Veterinary Group in the Midlands. Under his stewardship it grew to become a multisite small animal and equine practice with a team of over 100. He has had articles published on management topics and spoken at several congresses. He is currently a member of the Certification and Training committee of the VPMA. He is particularly interested in maximising the use of computer databases for strategic planning, marketing and analysing performance. He enjoys empowering all team members to work together synergistically.
David Gould BSc(Hons) BVM&S PhD FRCVS DVOphthal DipECVO
RCVS & European Veterinary Specialist in Ophthalmology
David Gould graduated from the University of Edinburgh in 1992 and, after a period in general practice, completed a PhD at the University of Cambridge in the molecular genetics of inherited eye diseases of dogs. Following this he moved to the University of Bristol for a three year clinical residency in veterinary ophthalmology. After this he was appointed Lecturer in Veterinary Ophthalmology at Bristol University Veterinary School, a post that he held for three years before joining Davies Veterinary Specialists in October 2003 to jointly run their ophthalmology service. He holds both RCVS and European Diplomas in Veterinary Ophthalmology and is an RCVS recognised Specialist in Veterinary Ophthalmology and European Veterinary Specialist in Ophthalmology. David was awarded Fellowship of the Royal College of Veterinary Surgeons for Meritorious Contributions to Clinical Practice (MCCP) in 2017.

5
Claudia Hartley
BVSc CertVOphthal DipECVO MRCVS
European & RCVS Specialist in Veterinary Ophthalmology
Claudia graduated from the University of Bristol in 1995, and worked in first opinion practice in both farm animal and small animal practices for nine years. During this period she gained her RCVS Certificate in Veterinary Ophthalmology, which tempted her into a residency at the Animal Health Trust (AHT) in 2004. She gained her European Diploma in Veterinary Ophthalmology in 2007. Claudia became head of the AHT unit of Comparative Veterinary Ophthalmology in 2009, and then moved to Davies Veterinary Specialists in 2015. Since March 2017 Claudia has been head of Ophthalmology at Langford Veterinary Services, Bristol Veterinary School.
Claudia is particularly interested in ophthalmic surgery and treatment of wild or zoological species with ophthalmic problems. She has worked with a number of international charities worldwide to alleviate ocular discomfort and treat visual impairment. Claudia loves working as part of a team of highly qualified and dedicated specialists at Langford Veterinary Services, and teaching both undergraduate and postgraduate veterinary nurses and surgeons.
Charlotte Dawson BVetMed MVetMed DipECVO MRCVS
Lecturer in Veterinary Ophthalmology at the RVC
Hello, I am Charlotte and I graduated from the RVC in 2009. After a short period in private practice I undertook two rotating internships (one in private practice and one at the RVC). I then continued with a residency and am now a lecturer at the RVC. I enjoy all aspects of life working at a university including the clinical activities, teaching and research. In my spare time I like spending time with my family, friends and traveling with my dog Frank.

Introduction to canine vitreo-retinal surgery A U.K. Perspective
Chris Dixon Veterinary Vision [email protected] 01768 877255 Before embarking on vitreo-retinal surgery, the surgeon should have a comprehensive understanding of the posterior segment anatomy and surgical techniques involved. These notes are only a very brief overview and I would highly recommend reading Chapter 25 ‘Surgery of the Canine Posterior Segment’ by Vaninisi S., Wolfer J., and Hoffman A. In Veterinary Ophthalmology 5th Edition., Ed. Gelatt, Gilger, Kern. Anatomy Interface between the vitreous and retina is the posterior vitreal membrane - Relatively weak except at the pars plana retinae and optic disk - Collagen fibrillar insertions link into the internal limiting membrane of the retina
Potential space exists between the neurosensory retina and retinal pigment epithelium
Vitreal conditions to consider - Persistent of the primary hyaloid vasculature - Vitreal syneresis - Asteroid hyalosis - Vitreal haemorrhage - Prolapsed vitreous into the anterior segment
Classification of retinal detachment Partial or complete Rhegmatogenous (tear / hole) or non-rhegmatogenous Rhegmatogenous Primary – spontaneous preceded by a change in the vitreous Secondary – related to trauma, glaucoma, inflammatory disease, surgery Non-rhegmatogenous Bullous - Serous - Exudative - Haemorrhagic
Traction - band or membrane formation Congenital Vitreal surgery includes - Vitreal paracentesis (hyalocentesis) - Anterior vitrectomy (anterior chamber and trans-pupillary) - Complete vitrectomy (Pars plana)

Vitreal paracentesis Collection of a vitreal sample for laboratory analysis - Preoperative mydriasis - General anaesthesia - Careful preparation with iodine solution - Measure 6mm from the dorsal limbus - Penetrate a 23G needle into the vitreal body aiming at the posterior pole - Can only aspirate liquefied vitreous – limit to 0.1ml Potential Complications include: - Lens touch / lens capsule rupture – cataract formation / lens induced uveitis - Haemorrhage - Retinal hole – retinal detachment - Contamination – vitritis / endophthalmitis
Same technique can be used for the delivery of medication into the vitreous Anterior Vitrectomy Often performed during lendectomy Herniated vitreous around disrupted lens zonule fibres e.g. lens subluxation / luxation Prolapsed vitreal filaments during planned or unplanned posterior capsulotomy Planned anterior vitrectomy for excision of persistent hyperplastic primary vitreous, malignant glaucoma, removal of a foreign body, removal of lens fragments Instrumentation - Micro-intraocular instruments - Vitreous / ONG / Vannus scissors, cyclodialysis spatula and
cellulose spears - Anterior vitrector with the phacoemulsification machine (electric / pneumatic)
Aim to keep all vitreous posterior to the pupil Vitreal filaments can serve as a scaffold for inflammatory membrane formation +/- traction bands Vitreous in contact with corneal endothelium will result in persistent oedema Potential for occlusion to aqueous outflow – glaucoumatous pressure spike Complete Vitrectomy Indications include: - Rhegmatogenous retinal detachment - Removal of vitreous traction bands - Removal of foreign bodies - Vitritis, vitreal opacification, haemorrhage - Malignant glaucoma
Veterinary VR surgery has been performed since the 1970’s so why are there so few clinics offering this service globally? - Very high set-up costs (e.g. VR machine
£80k+, BIOM, invertor, and laser filter £20k) - High consumable costs - Time-consuming training - Excellent bi-manual dexterity required
Surgical Anatomy Multiple (usually three) sclerotomies through the pars plana ciliaris - I.e. between the end of the anterior pars
plicata and the ora ciliaris - Do not want to puncture the ciliary body or
retina - Width of the pars plana varies by quadrant

Smith et al measurement from the limbus Sullivan et al measurement from the limbus - Dorsolateral 6mm - dorsal quadrant, 9.25 +/- 0.81 mm - Dorsomedial 5mm - medial quadrant, 5.30 +/- 0.77 mm - Ventromedial 7mm - ventral quadrant, 7.18 +/- 0.89 mm - Ventrolateral 9mm - lateral quadrant, 9.41 +/- 0.79 mm
Vasculature to consider: - Intrascleral plexus ‘circle of Hovius’, drains aqueous humor – 4-5mm posterior to the limbus
and 3-4mm wide - Vortex veins exit each quadrant at the equator - Long posterior ciliary arteries and veins (branches of the external ophthalmic artery and vein) –
3 o’clock and 9o’clock position
The interface between the neurosensory retina and vitreous is critical in the development of rhegmatogenous retinal detachment. Liquification of the vitreous allows for counter-current motion over the retinal surface with ocular movement. Turbulence within the posterior segment can lead to tearing especially if there is pre-existing retinal atrophy or a retinal hole. It has been reported that dogs with a tendency to violently shake their heads are more likely to develop a spontaneous giant retinal tear – Vainisi S., Wolfer J. 2004 Veterinary Ophthalmology. It is thought that Shih Tzu, Boston Terrier, Toy and Minature Poodles develop vitreal degeneration leading to syneresis. In the population of dogs that I have seen at our clinic, Shih Tzu’s are over-represented.
In humans the central ‘nucleus’ of the vitreous is semi-fluid and the peripheral ‘cortex’ has increased density. In our canine patients, the nucleus has increased density compared to the cortex. Proliferative vitreoretinopathy (PVR) is the growth of cellular membranes in contact with the neurosensory retina. Contraction of the membranes results in detachment of the neurosensory retina and immobilization. PVR has been reported by Blair et al 1985 in Labradors with oculoskeletal dysplasia. We have seen PVR in our clinic with a spectrum of severity. It is not uncommon for the detection of a membrane without retinal distortion, and occasionally we encounter the ‘clam shell’ fixed in position. Equipment required for high-speed posterior vitrectomy for retinal detachment: Microscope with suitable head for posterior segment surgery accessory attachment BIOM / EIBOS non-contact wide-view lens system to visualise the posterior segment Invertor, manual vs automatic Microscope laser filter Phacoemulsification unit High speed (6000+ cuts/min) VR unit Laser 810nm vs 532nm generator with endoprobe Anterior segment and posterior segment instruments

Steps in retinal reattachment surgery (giant tear) 1. Remove lens / cataract by small port phacoemulsification 2. Insertion of a prosthetic IOL 3. Careful closure of the corneal incisions 4. Peritomy 5. One-stepped 23G self-sealing trocar insertion 6. Core vitrectomy (2500 cut) 7. Triamcinolone acetonide 8. High-speed (6000+) low vacuum vitrectomy 9. Reposition retina (peel membranes if required) 10. Heavy liquid perfluro-n-octane 11. Laser retinopexy 12. Heavy liquid – air exchange 13. Laser again if required 14. Silicone oil infusion 15. Remove trocars and suture port closed 16. Close lateral canthotomy
Silicone Oil - 5000 centistoke with a specific gravity of 0.971 forms a buoyant viscous bubble - In humans silicone oil is normally removed after 3-6 months, but generally life-long in dogs
Barrier retinopexy / prophylactic retinopexy Trans-pupillary approach with clear visualisation – can use a scleral depressor Indirect headset (£6k-12k) with modified optics for the laser generator Endo approach through posterior capsulotomy ‘Seal’ around small tears and holes Prophylactic therapy for ‘at-risk’ breeds and ‘fellow eyes’ Please feel free to contact me if you have a question regarding VR surgery or if you have a case which you wish to discuss

Rhomboid blepharoplasty and cryotherapy for the treatment of a squamous cell carcinoma on the lower eyelid in a horse E. C. Jeanes (AHT), S. Koll (RVC), C. Dawson (RVC), B. Dunkel (RVC) and R. Tetas Pont (RVC). A 9-year-old grey Irish Draught horse gelding was presented to the Royal Veterinary College for excision of a medial lower eyelid squamous cell carcinoma. The diagnosis had been made 18 days previously using a fine needle aspirate by the referring veterinary surgeon. The 10mm x 12mm tumour was resected en-bloc under general anaesthetic. This was done using full thickness cuts of equal length medial, lateral and ventral to the mass, so that a square of tissue was removed. The cuts were made 5mm from the edge of the mass. The wound edges were treated with liquid nitrogen cryotherapy. Two freeze-thaw cycles were used of 10 seconds freezing then 60 seconds melting. Reconstruction of the lower eyelid was achieved using a rhomboid blepharoplasty. An incision was made extending ventro-medially from the ventromedial aspect of the excision site. This incision was the same length as the previous incisions. A proximal vertical incision was then made from the ventromedial edge of the last incision to create a rhomboid shaped skin graft. Blunt dissection was used to undermine the rhomboid graft and the skin medial to the graft to mobilise the tissue. The rhomboid graft was swung dorsally and laterally to fill the eyelid defect. The wound was closed using routine subcutaneous and dermal sutures. Clean margins were achieved with the surgery and the surgical wounds healed well with no complications. In the follow-up period of six months, no recurrence of the tumour was noted. Squamous cell carcinoma (SCC) is the most common tumour of the equine orbit and adnexa and the second most common tumour in the horse overall. The incidence of ocular SCC in equines is positively correlated with increased exposure to ultraviolet light. Lack of skin pigmentation also increases the risk of becoming affected. Ocular SCCs are typically highly locally invasive but the reported metastatic rate is low. Eyelid SCC has been shown to carry a poorer prognosis compared to other ocular locations. The mainstay of treatment of eyelid SCC is surgical excision. Recurrence after surgical excision is likely, particularly if clear surgical margins cannot be achieved. The recurrence rate reported varies and adjuvant therapy, such as cryotherapy, radiofrequency hyperthermia, radiotherapy, topical and intralesional chemotherapy with cisplatin or 5-fluorouracil, bacille Calmette-Guerin (BCG) cell wall extract, and carbon dioxide laser ablation is often considered to avoid further recurrences. Blepharoplasties in horses are rarely reported in the literature due to the challenges of the poorly mobile tissue around the horse eye; subsequently enucleation or exenteration may be required at the expense of a visual eye. The rhomboid blepharoplasty allows closure of a large eyelid defect using haired skin. After a rhomboid graft is performed, the retraction force vectors are expected to be directed alongside the palpebral fissure. This may be an advantage compared to other blepharoplasties, for example an H-plasty, where these vectors are expected to develop perpendicularly to the palpebral fissure and potentially predispose to post-operative ectropion and lagophthalmus. The surgeons prioritized not altering the lateral canthus and the normal lateral part of the lower eyelid. The advantage achieved with the rhomboid technique is that the cornea is shielded by the nictitans membrane from trichiasis, thus minimizing the risk of post-operative corneal irritation. Furthermore, if excision of a tumour is later shown to be incomplete on histopathology, sparing the lateral canthus would allow a sliding lateral blepharoplasty to be performed at a later date. This case demonstrates that a rhomboid blepharoplasty can be used to achieve functional and cosmetic eyelid reconstruction at the medial canthus in the horse.





AN INVESTIGATION INTO THE BACTERIAL CONTAMINATION OF GONIOLENSES IN USE IN CLINICAL
PRACTICE.
RA Grundon¹, EJ Scurrell², J Mould¹, E Hayton-Lee¹, CL Heinrich¹
1 The Eye Vet Clinic, Marlbrook, Herefordshire, UK
2 CytoPath Ltd, Ledbury, Herefordshire, UK
Purpose - To report the incidence and evaluate the clinical significance of goniolens bacterial
contamination in clinical use.
Methods - Three groups of twenty dogs undergoing gonioscopy in the UK had goniolenses swabbed
for bacteriology culture and identification prior to placement on the cornea. Three protocols of
lens use, with 2 different goniolenses (Koeppe and Barkan-lovac), were studied. At the end of data
collection the storage boxes were also swabbed. Telephone follow up was made to assess the
impact of goniolens placement on the dogs. A final group of 21 dogs then had the goniolenses
swabbed before use as before, but with an implemented cleaning protocol after use and before
storage.
Results - Low levels of bacterial contamination were found in all 3 initial groups (10-15%). Seven
positive lens bacterial cultures and one box culture occurred with eight different bacterial species
cultured. No statistical correlation was found between protocol used and rate of contamination,
nor between length of storage between use and contamination. All the bacterial species cultured
were considered commensals in the eye or the environment and were not consistent within or
between protocols. Two of thirty nine dogs (5%) available for follow up had transient mild epiphora;
neither dog had a goniolens that had cultured positive placed on their eyes. In the group with
cleaned lenses there was a single positive culture (4.8%). There was no significant difference
between the contamination rate of the pooled “unwashed” lenses (11.7%) and the “washed” lenses
(4.8%).
Conclusions - The rate of bacterial contamination of goniolenses in clinical practice in this study is
low and the bacterial contaminants consist of commensal bacterial, unlikely to be of detriment to
an eye with an intact epithelium. Extensive cleaning protocols of the lenses between dogs are not
required however cleanliness could be improved. Although the washing protocol did not
significantly reduce contamination with these sample numbers cleaning lenses should be
encouraged between corneal contacts.
Support - The generous support of BrAVO Research Grant is acknowledged.

Retin
a an
d Vi
treou
s Bu
ildin
g Bl
ocks
Joe
Wol
fer D
VM D
ACVO
To
ront
o C
anad
a
Результаты
поиска
m

Retin
a
•10
laye
rs
•Re
tinal
pig
men
t epi
thel
ium
(RPE
), vi
sual
laye
r (ro
ds a
nd c
ones
), ou
ter l
imiti
ng m
embr
ane
(OLM
), ou
ter n
ucle
ar la
yer,
oute
r ple
xifo
rm la
yer,
inne
r nuc
lear
laye
r, in
ner p
lexi
form
laye
r, ga
nglio
n ce
lls, n
erve
fibr
e la
yer a
nd IL
M.

•Th
e ou
ter m
ost (
RPE)
and
the
inne
r mos
t (IL
M)
are
the
mos
t im
porta
nt la
yers
to th
e re
tina
surg
eon. RPE
hyp
ertro
phy,
“to
mbs
toni
ng”

•It
is th
e in
terfa
ce b
etw
een
the
visu
al la
yer a
nd
the
RPE
that
is m
ost i
mpo
rtant
to v
isua
l re
habi
liatio
n.
•An
d it
is th
e in
terfa
ce b
etw
een
the
vitre
ous
and
the
ILM
that
is m
ost i
mpo
rtant
to th
e pa
thog
enes
is o
f ret
inal
det
achm
ent
•Th
e in
timat
e in
terfa
ce b
etw
een
the
retin
al
phot
orec
epto
rs a
nd th
e RP
E m
ust b
e re
-es
tabl
ishe
d ex
actly
for v
isio
n to
be
re-
esta
blis
hed.

•Th
e m
ain
func
tions
of t
he R
PE a
re th
e fo
llow
ing:
(1
) Tra
nspo
rt of
nut
rient
s, io
ns, a
nd w
ater
(2)
abso
rptio
n of
ligh
t and
pro
tect
ion
agai
nst
phot
ooxi
datio
n, (3
) rei
som
eriz
atio
n of
all-
trans
-re
tinal
into
11-
cis-
retin
al, w
hich
is a
key
ele
men
t of
the
visu
al c
ycle
, (4)
pha
gocy
tosi
s of
she
d ph
otor
ecep
tor m
embr
anes
•W
ithou
t the
clo
se a
ppro
xim
atio
n of
the
RPE
to
the
phot
orec
epto
rs, v
isio
n w
ill no
t occ
ur.
•So
, the
mai
n go
al o
f the
retin
a su
rgeo
n is
to
repl
ace
the
phot
orec
epto
rs w
ithin
phy
siol
ogic
di
stan
ce to
the
RPE

Ora
cilia
risre
tinae
•Th
ere
is n
o ac
tual
atta
chm
ent,
no c
ell m
embr
ane
atta
chm
ents
bet
wee
n th
e ph
otor
ecep
tors
and
th
e RP
E
•Th
e on
ly th
ing
hold
ing
the
retin
a to
the
RPE
is a
la
yer o
f gly
cosa
min
ogly
cans
that
sur
roun
ds th
e ro
d an
d co
ne o
uter
seg
men
ts.
Thes
e G
AG a
re
know
n as
the
inte
r pho
tore
cept
or m
atrix
or I
PM.

•W
hat?
????
•H
ow c
an th
is p
ossi
bly
be??
??
•H
ow c
an a
thin
laye
r of G
AG h
old
an e
ntire
retin
a in
pla
ce.
•Th
e an
swer
is tw
o fo
ld.
•O
ne.
Ther
e is
a c
onst
ant v
acuu
m o
f the
sub
re
tinal
spa
ce m
aint
aine
d by
a) t
he in
tegr
ity o
f the
re
tina
surfa
ce it
self
and
b) b
y th
e io
n pu
mp
of
the
RPE

•Tw
o. T
he in
tact
vitr
eous
gel
pre
vent
s an
y ce
ntrip
etal
or i
nwar
d m
ovem
ent o
f the
retin
a,
and
the
inte
rface
bet
wee
n th
e IL
M a
nd th
e po
ster
ior h
yalo
id m
embr
ane
prev
ents
any
sl
ippa
ge o
f the
retin
a in
a lo
ngitu
dina
l dire
ctio
n.
•Es
sent
ially
, the
inta
ct v
itreo
us g
el p
reve
nts
any
mov
emen
t wha
tsoe
ver o
f the
inta
ct re
tina.

•Th
e vi
treou
s is
the
larg
est s
truct
ure
in th
e ey
e an
d co
mpo
ses
2/3
of th
e vo
lum
e of
the
eye
•M
ean
vitre
ous
volu
me
in th
e do
g is
list
ed a
t ab
out 2
mL,
giv
e or
take
•H
owev
er, a
s a
retin
a su
rgeo
n, o
ne fi
nds
that
it
take
s ab
out 4
mL
of s
ilicon
e ge
l to
com
plet
ely
refil
l the
pos
terio
r seg
men
t at t
he c
oncl
usio
n of
su
rger
y.
•Th
is is
act
ually
in k
eepi
ng w
ith li
sted
vitr
eous
vo
lum
e in
the
hum
an e
ye, w
hich
is q
uite
sim
ilar
in s
ize
and
shap
e to
the
cani
ne e
ye

•Th
ere
are
3 ty
pes
of v
itreo
us.
Prim
ary
vitre
ous,
se
cond
ary
vitre
ous
and
terti
ary
vitre
ous
•Th
e pr
imar
y vi
treou
s de
velo
ps fi
rst a
nd
esta
blis
hes
the
hyal
oid
arte
ry s
yste
m to
sup
port
the
deve
lopi
ng le
ns
•Th
e se
cond
ary
vitre
ous
(defi
nitiv
e vi
treou
s)
form
s ar
ound
the
prim
ary
vitre
ous
and
is o
f ne
urec
tode
rmal
orig
in.

•Th
e te
rtiar
y vi
treou
s fo
rms
the
lens
zon
es
•As
retin
a su
rgeo
ns, w
e ar
e co
ncer
ned
mai
nly
with
the
seco
ndar
y vi
treou
s ex
cept
in c
erta
in
rela
tivel
y ra
re s
ituat
ions
suc
h as
per
sist
ent
prim
ary
hype
r pla
stic
vitr
eous
(PH
PV) o
r len
s zo
nule
loss
and
lens
inst
abilit
y.
•Th
e vi
treou
s is
mai
nly
wat
er w
ith a
sm
all a
mou
nt
of c
olla
gen
and
hyal
uron
ic a
cid
to g
ive
it st
ruct
ure
•Al
mos
t all
visi
ble
light
is tr
ansm
itted
thro
ugh
the
vitre
ous.

•Th
e vi
treou
s fo
rms
a fir
m a
ttach
men
t to
the
retin
a in
onl
y 2
plac
es.
The
ora
cilia
ris re
tinae
(p
erip
hera
l ext
ent o
f the
retin
a ne
ar th
e le
ns) a
nd
the
edge
of t
he o
ptic
ner
ve.
Thes
e ar
e tw
o “h
ot
spot
s” in
the
path
ogen
esis
of r
etin
al d
etac
hmen
t (R
D)

•Th
e ou
ter e
xten
t of t
he p
oste
rior v
itreo
us c
orte
x fo
rms
a ra
ther
loos
e at
tach
men
t with
the
base
men
t mem
bran
e of
the
Mul
ler c
ells
. Th
is
base
men
t mem
bran
e is
kno
wn
as th
e IL
M, w
hich
is
ver
y im
porta
nt in
the
path
ogen
esis
of r
etin
al
deta
chm
ents
in h
uman
s.
•Th
e w
eak
atta
chm
ent o
f the
pos
terio
r hya
loid
m
embr
ane
and
the
ILM
is a
noth
er “h
otsp
ot”.
•In
mos
t dom
estic
ani
mal
s re
tinal
thic
knes
s is
ab
out 2
00um
at t
he o
ptic
ner
ve a
nd a
bout
10
0um
at t
he o
ra c
iliaris
retin
ae.
•Th
us in
man
y in
stan
ces,
tear
s oc
cur i
n th
e w
eake
r thi
nner
per
iphe
ry o
f the
retin
a.
•An
d in
deed
, as
a re
tina
surg
eon,
the
maj
ority
of
case
s th
at w
e se
e ar
e 36
0 de
gree
tear
s ne
ar th
e or
a ci
liaris
retin
ae.

•O
ne o
f the
stro
nges
t vitr
eal a
ttach
men
ts is
the
vitre
ous
base
nea
r the
ora
cilia
ris re
tinae
and
th
is c
ombi
ned
with
a th
inne
r wea
ker r
etin
a in
this
ar
ea, m
ake
this
a b
ig h
otsp
ot fo
r ret
inal
tear
s
•In
the
cani
ne e
ye, m
uch
path
olog
y oc
curs
nea
r th
e vi
treou
s ba
se th
at c
an le
ad to
RD
. W
e w
ill ta
lk a
bout
this
are
a m
ore
in th
e re
tinal
dis
ease
s se
ctio
n.

•So
, in
sum
mar
y
•Th
e re
tina
adhe
res
to th
e RP
E th
roug
h a
varie
ty
of c
ompl
ex c
ompl
imen
tary
mec
hani
sms.

•Th
ese
mec
hani
sms
incl
ude;
•Pr
essu
re o
n th
e re
tina
from
the
vitre
ous,
the
IPM
w
hich
act
s lik
e gl
ue, i
nter
digi
tatio
n w
ith th
e RP
E m
icro
villi,
and
the
ioni
c pu
mp
of th
e RP
E w
hich
de
hydr
ates
the
sub
retin
al s
pace
.
•Es
sent
ially
phy
sica
l AN
D m
etab
olic
pro
cess
es
play
a ro
le
•Th
us th
e m
anag
emen
t of R
D s
houl
d in
clud
e at
tent
ion
to b
oth
the
phys
ical
, as
wel
l as
the
met
abol
ic p
rope
rties
of r
etin
al a
ttach
men
t

Pseu
doph
akic
retin
al
deta
chm
ent
Joe
Wol
fer
Toro
nto
Can
ada
Ridi
culo
usly
goo
d lo
okin
g
•If
anyo
ne is
inte
rest
ed in
con
tact
ing
me
with
qu
estio
ns, m
y ad
dres
s is
•jw
olfe
r@sy
mpa
tico.
ca

•Th
e ex
act i
ncid
ence
of R
D a
fter c
atar
act s
urge
ry
in th
e do
g is
unk
now
n an
d th
ere
real
ly h
ave
been
no
thor
ough
stu
dies
don
e to
det
erm
ine
this
•H
owev
er, m
y be
lief i
s th
at 2
-4%
of c
atar
act
patie
nts
will
deve
lop
RD p
ost-o
pera
tivel
y
•Et
iopa
thog
enes
is o
f pse
udop
haki
c RD
is
unkn
own,
how
ever
, pos
sibl
e pr
oble
ms
incl
ude:

•D
isru
ptio
n of
the
post
erio
r len
s ca
psul
e. T
ears
in
the
post
erio
r len
s ca
psul
e in
crea
se th
e ris
k of
RD
and
mak
e re
tinal
sur
gery
mor
e di
fficu
lt, a
s si
licon
e oi
l will
mig
rate
thro
ugh
the
PC te
ar a
nd
into
the
ante
rior s
egm
ent
•Te
ars
in th
e PC
allo
w fl
uid
from
the
ante
rior
segm
ent i
nto
the
post
erio
r seg
men
t, de
stab
ilizin
g th
e vi
treor
etin
al in
terfa
ce
•C
atar
act s
urge
ry c
ause
s m
inor
trau
ma
to th
e le
ns a
nd m
ay a
pply
forc
es to
the
lens
zon
ules
. Th
is c
ould
pos
sibl
y ap
ply
forc
es to
the
atta
chm
ent o
f the
retin
a at
the
ora
cilia
ris re
tinae
, an
d/or
exa
cerb
ate
cyst
oid
retin
al d
egen
erat
ion
in th
is a
rea,
cre
atin
g a
retin
al te
ar.
•Po
st-o
pera
tive
IOP
spik
es, m
ay s
tretc
h th
e gl
obe
appl
ying
tens
ion
to th
e re
tina
and
caus
ing
tear
s

•Pr
e-op
erat
ive
lens
indu
ced
uvei
tis h
as b
een
asso
ciat
ed w
ith a
n in
crea
sed
inci
denc
e of
RD
. C
hang
es in
the
vitre
ous
due
to in
flam
mat
ion
of
the
cilia
ry b
ody
may
resu
lt in
RD
•H
yper
mat
ure
cata
ract
s. A
s th
e ca
tara
ct
prog
ress
es fr
om m
atur
e to
hyp
er m
atur
e, le
ns
prot
eins
leak
from
the
lens
, cau
sing
lens
in
duce
d uv
eitis
whi
ch w
e kn
ow in
crea
ses
the
risk
of R
D
•Al
so, a
s th
e le
ns s
hrin
ks a
nd th
e ca
psul
e be
com
es w
rinkl
ed te
nsio
n m
ay b
e br
ough
t to
bear
on
the
lens
zon
ules
incr
easi
ng th
e ris
k fo
r RD
•Al
so, a
s th
e ca
tara
ct re
ache
s th
is s
tage
, len
s ep
ithel
ium
mig
rate
s on
to th
e po
ster
ior c
apsu
le
and
may
nec
essi
tate
pos
terio
r cap
sule
ctom
y to
gi
ve a
cle
ar v
isua
l axi
s.
•Po
ster
ior c
apsu
lect
omy
incr
ease
s th
e ris
k fo
r RD

•D
iabe
tic c
atar
acts
; m
any
diab
etic
cat
arac
ts
beco
me
intu
mes
cent
(sw
olle
n) s
tretc
hing
the
zonu
les
and
alte
ring
the
vitre
ous
base
. Th
is m
ay
lead
to R
D
•If
the
lens
bec
omes
too
swol
len,
the
post
erio
r le
ns c
apsu
le m
ay ru
ptur
e ex
trudi
ng p
art o
f the
le
ns in
to th
e vi
treou
s an
d in
crea
sing
the
risk
for
RD

•Le
ns lu
xatio
n; i
f the
lens
mus
t be
rem
oved
by
an in
traca
psul
ar te
chni
que
due
to lu
xatio
n,
inci
denc
e of
RD
is h
ighe
r.
•Le
ns lu
xatio
n di
srup
ts th
e an
terio
r hya
loid
face
pr
edis
posi
ng to
RD
•So
me
surg
eons
rout
inel
y pe
rform
TPL
R af
ter
lens
luxa
tion
surg
ery.
•Th
e m
ost i
mpo
rtant
spe
cific
pro
blem
to
pseu
doph
akic
RD
is d
isru
ptio
n of
the
bloo
d oc
ular
bar
rier b
y pr
ior c
atar
act s
urge
ry
•It
take
s m
onth
s fo
r the
BO
B to
refo
rm c
ompl
etel
y af
ter c
atar
act s
urge
ry, a
nd s
urge
ry o
n ps
eudo
phak
ic p
atie
nts
is u
sual
ly p
erfo
rmed
w
ithin
wee
ks a
fter t
he in
itial
cat
arac
t sur
gery

•Th
e BO
B is
ther
efor
e w
eak
and
the
eye
is m
ore
infla
mm
ed.
This
lead
s to
a s
ofte
r eye
and
po
ssib
le o
paci
ficat
ion
of th
e oc
ular
med
ia.
This
m
akes
vis
ualiz
atio
n of
the
retin
a m
ore
diffi
cult
•An
terio
r an
d po
ster
ior s
egm
ent b
leed
ing
is
mor
e co
mm
on
•Th
ere
is o
ften
an IO
L pr
esen
t and
this
mak
es
visu
aliz
atio
n of
the
retin
a m
ore
diffi
cult
as w
ell.
•To
cou
nter
act t
hese
fact
ors,
it is
impo
rtant
to
plac
e pa
tient
s on
ora
l cor
ticos
tero
ids
prio
r to
surg
ery

•If
poss
ible
, tw
o da
ys p
rior t
o re
tinal
sur
gery
, the
vi
treou
s is
inje
cted
with
1.2
5mg
of A
vast
in
(bev
aciz
umab
), an
ant
i-vas
cula
r end
othe
lial
grow
th fa
ctor
(veg
f) ag
ent.
•Th
is w
ill st
abiliz
e th
e BO
B an
d fa
cilit
ate
an
easi
er s
urge
ry
•W
ith y
our p
ost-c
atar
act s
urge
ry p
atie
nts
you
neve
r kno
w w
hat y
ou w
ill ge
t bre
ed-w
ise.
•M
any
are
not b
rach
ycep
halic
and
it m
ay b
e di
fficu
lt to
pro
ptos
e th
e ey
e.
•Th
is m
akes
it d
ifficu
lt to
get
ade
quat
e ex
posu
re
to th
e pa
rs p
lana
are
a
•H
owev
er, w
ith th
e ne
w 2
3g tr
ocar
tech
nolo
gy it
is
muc
h ea
sier
to d
o su
rger
y on
eye
s th
at h
ave
not
been
pro
ptos
ed


A novel ADAMTS17 mutation is associated with primary open angle glaucoma and primary lens luxation in the Shar Pei
James A. C. Oliver1, Sophie Rustidge1, Louise Pettitt1, Christopher A. Jenkins1, Fabiana H. G. Farias2, Elizabeth A. Giuliano3, Cathryn S. Mellersh1
1The Canine Genetics Research Department of The Animal Health Trust, Lanwades Park, Kentford, Newmarket, Suffolk, CB8 7UU, United Kingdom
2The Department of Pathobiology, The College of Veterinary Medicine, University of Missouri, Columbia, MO 65211, U.S.A.
3The Department of Veterinary Medicine and Surgery, The College of Veterinary Medicine, University of Missouri, Columbia, MO 65211, U.S.A.
Abstract
Introduction. Mutations in ADAMTS17 (CFA3) are associated with both primary open angle glaucoma (POAG) and primary lens luxation (PLL) in several dog breeds. We investigated ADAMTS17 as a candidate gene for these conditions in the Shar Pei – a breed in which both POAG and PLL have been reported.
Materials & Methods. DNA was obtained from Shar Pei classified as either affected or unaffected for POAG and/or PLL. We initially performed ADAMTS17 exon resequencing in 10 Shar Pei with POAG and/or PLL. We identified a provocative candidate mutation, which was then genotyped in additional affected and unaffected Shar Pei and in dogs of other breeds to confirm association with disease. RNA was extracted from ocular tissues of one affected and one unaffected dog and reverse transcribed to cDNA. Sanger sequencing of the cDNA was undertaken, as well as expression analysis of ADAMTS17 using qRT-PCR.
Results. All affected Shar Pei were homozygous for a 6 bp deletion in exon 22 of ADAMTS17. Forty-two clinically unaffected Shar Pei were all either heterozygous or homozygous for the wild type allele. The association of the deletion with POAG/PLL was statistically significant (p = 3.79 x10-14), and this variant was not identified in 95 dogs of other breeds. Sanger sequencing of cDNA confirmed the presence of the mutant transcript in the affected eye and the normal transcript in the unaffected eye. Quantitative RT-PCR revealed a 4-fold reduction in the expression of ADAMTS17 transcript in affected ocular tissue (p = 0.0006).
Conclusions. POAG and PLL are both associated with the same novel mutation in ADAMTS17 in the Shar Pei providing evidence that the diseases are genetically indistinguishable. This finding has led to the development of a DNA test which will allow the diseases to be eradicated from the breed.

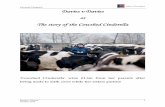
BrAVO travel scholarship report 2017 Introduction Orangutans (Pongo pygmaeus and Pongo abeii) are the only great apes of Asia (Borneo and Sumatra respectively), and have been recently reclassified as critically endangered on the IUCN red list. Wild orangutan populations are threatened by poaching (especially in animal-human conflicts e.g. palm oil plantations), habitat loss or degradation, and the illegal pet trade. Several conservation and rehabilitation organisations are dedicated to the survival of orangutans in the wild. During the period 1973–2010, 39% of Bornean forests were lost (Gaveau et al. 2014), representing a net loss of 98,730 km² of prime orangutan habitat. It is estimated that a further 37% of suitable orangutan habitat (155,106 km²) will be converted to plantations between 2010 and 2025, which accounts for the loss of an additional 57,140 km² of orangutan habitat (Wich et al. 2012). Using a questionnaire survey it was estimated that 630–1357 Bornean Orangutans were killed in 2008 and that an average of 2383–3882 per year had been killed during the lifetimes of the survey respondents (Meijaard et al. 2011). The mean estimate (2256 orangutans poached in Kalimantan each year) equates to 2.6% of the 2010 population for Kalimantan. The combined impacts of habitat loss, habitat degradation and illegal hunting equate to an 86% population reduction between 1973 and 2025 which qualifies the species for listing as Critically Endangered. This estimate is relatively conservative, as it does not include additional future population losses anticipated due to stochastic effects that will reduce populations inhabiting increasingly small forest fragments. Orangutans are arboreal and make nests (from branches and foliage) each evening to sleep in. Orangutans are generally solitary, with social bonds occurring primarily between mothers and their dependent and weaned offspring. Infants remain completely dependent on their mother until 2 years of age, and are weaned at approximately 4 years old. Juveniles learn ‘forest skills’ from their mothers who generally have a period of 8 years between offspring. Males are generally larger, and dominant adult males (post-pubescence, approx. 15 years old) have distinctive cheek pads (‘flanges’) and produce long calls that attract females and intimidate rivals. Younger males resemble adult females. Adult males in the presence of a dominant male remain unflanged, but can reproduce if the opportunity arises (he can mate with a female in oestrus without getting caught by the dominant male). Fruit is the most important component of an orangutan's diet (65-90%), although they will also eat vegetation. Life expectancy in the wild is approx. 25years (Wich et al 2009). ‘Aan’, an estimated 20 year old female Orangutan was rescued in 2012 following air-rifle injuries on a palm oil plantation (human-animal conflict). Multiple superficial pellets were removed but deeper pellets could not be retrieved. (see Fig 1.) Due to behaviour suggestive of blindness, ‘Aan’ was kept in a forest cage (solitary) for her own safety.
Fig 1. Radiograph of Aan at time of rescue
The ophthalmic examination In September 2016, and under anaesthesia Aan was examined at Camp Gemini, Pangkalan Bun, Indonesia. Examination of the right eye revealed a Schirmer tear test reading of

0mm/min (likely secondary to the xylazine). The cornea was clear and revealed a mature cataract with iridal trauma at approximately 5 o’clock on the iris margin. There was a strand of fibrotic tissue and exposure of a triangle of posterior pigmented iris epithelium. There were multifocal spots of pigment on her anterior lens capsule (likely dispersed from the iris on trauma). The pupil was responsive to light; tropicamide was applied to dilate the pupil. Direct examination of the posterior segment was not possible due to the presence of the cataract (obscuring visualisation). Her intraocular pressure was 20mmHg in this eye. There was no discernible aqueous flare. Ocular ultrasound confirmed the presence of a cataract with some vitreal degeneration and mobile membranes. There was a hyperechoic line close to the optic nerve head in the medial retina that could represent a partial retinal detachment. It is possible it represented posterior vitreal detachment, although it remained partially visible even on reduction of the gain. Orbital ultrasound was also performed which revealed some images of an apparently intact optic nerve. There was a cross-shaped hyperechoicity adjacent to the optic nerve but this was not accompanied by an acoustic shadow (as might be expected for an air rifle pellet). Ocular electroretinography was also performed after (partial, approx. 75%) dilation of the pupil (tropicamide). This revealed a repeatable positive trace. Optic nerve disruption more posteriorly could not be excluded (no access to MRI for example), although the presence of a pupillary light reflex was considered a positive indicator.
Fig. 2 a. Right eye b. Left eye c. ultrasound of right eye b. Left eye
BrAVO sponsored surgical expedition The expedition planned to undertake phacoemulsification of the cataract in Aan’s right eye and enucleation of her left (phthisical) eye. The aim was to restore uniocular vision in this animal, to permit release and potential breeding from this conservationally valuable individual.
Surgery was performed under general anaesthesia (medetomidine, tiletamine and zolazepam, with gaseous isofluorane & O2) performed by Dr John Lewis MA, VetMB, PhD, MRCVS, RCVS Specialist in Zoo and Wildlife Medicine. Stay sutures were placed as neuromuscular blockade was not attempted. Phacoemulsification was straightforward although no artificial intraocular lens was placed due to a radial capsular tear. The left eye was removed by a transconjunctival approach. Recovery from anaesthesia was extended, requiring veterinary supervision overnight at the island camp.
Topical medications were not possible. A subconjunctival injection of aqueous dexamethasone and chloramphenicol ointment were administered at the completion of surgery. Oral paediatric ibuprofen suspension and amoxycillin tablets were given orally disguised in fruit.
Although her right eye was exceptionally clear post-operatively, Aan did not regain vision, and optic nerve/chiasm trauma was assumed. Lifelong solitary captivity was now the only option and environmental enrichment was prioritised.

VitreoretinalSurgery
Malcolm Woodcock Worcestershire Acute NHS Trust &
Birmingham and Midland Eye Centre
VITREORETINAL SURGERY
▪ Macular holes ▪ Epiretinal membranes ▪ Retinal detachments ▪ Severe diabetic retinopathy ▪ Complications from cataract surgery ▪ Complications or Age-related Macular
Degeneration (AMD) ▪ Ocular trauma
VITRECTOMY - HISTORY
▪ Machemer 1970 reported the successful removal of longstanding vitreous haemorrhages in a group of diabetic patients
▪ Over the next four decades refinements in surgical techniques have expanded the indications and capability of vitreous surgery
▪ Some of the advances are the use of long-term vitreous replacements, endolaser photocoagulation, panoramic viewing systems, and perfluorocarbon liquids.

VITRECTOMY
▪ This is done through three small (20G, 23G or 25G) pars plana incisions entering the vitreous space. An infusion line is placed to restore fluid which is aspirated by a vitreous cutter
VISUALISATION
▪ Wide field or panoramic viewing system
▪ Optical principles of indirect ophthalmoscopy creating a virtual image with high plus condensing lenses.
▪ Large field of view up to 130º.
▪ Inverted image. The image is reverted by a prism system mounted on the surgical microscope.

Epiretinal Membrane
▪ Sheet of fibroblast-like cells
▪ Scrunches macula beneath
▪ Distortion and reduced vision
▪ Vitrectomy/ERM peel
Epiretinal Membrane Peel
Macular Hole
▪ Hole at fovea (≤ 400µm) ▪ Drops VA to 6/60 +
distortion ▪ F>M, 15% risk to fellow
eye ▪ Vitrectomy, peel of
retinal inner limiting membrane + gas tamponade

Peeling the Inner Limiting Membrane of the Retina
Posterior Vitreous Detachment and Retinal Detachment
▪ Vitreous is a polymer of water which breaks down with age
▪ New cobweb-like floater (Red flag - flashes, multiple small floaters, shadows, loss of vision)
▪ Past ocular surgery – previous cataract surgery
Retinopexy
cryotherapy
laser

Retinopexy-laser
Retinal Detachment
Surgical treatment - Objectives
1. mechanically appose the sensory retina and retinal pigment layer (closing the break)
2. to prevent the retinal tear from reopening

RD-Surgical manoeuvres
1. Retinal coagulation (cryotherapy and laser)
1. Scleral buckling (indentation of the eye wall) +/- additional procedures
2. Vitrectomy and internal tamponade
Risks of Surgery
▪ < 1 in 800 chance of blindness due to surgery ▪ 20% chance of requiring more than one
procedure ▪ Overall 97% success rate ▪ Cataract ▪ Glaucoma
INTRAOCULAR GASES
1. Usually either perfluropropane (C3F8) or sulphur hexafluoride (SF6)
2. When mixed with sterile air have the property of remaining in the eye for extended periods of time (up to two months)
3. Possible complications of intraocular gas include progression of cataracts and elevated eye pressure (glaucoma)
4. It is unsafe to fly in a plane while gas remains in the eye.
5. Nitrous Oxide?

Cyro/buckle procedure
Scleral buckling appliances
Encircling silicone band
Solid silicone tyre
Silicone sponge
Severe diabetic retinopathy
▪ Extensive fibrovascular membrane
▪ Lead to tractional retinal detachment
▪ Chronic macular oedema

Complications of cataract surgery
▪ “dropped nucleus” ▪ If anterior lens
capsulae intact – sulcus fixated IOL
▪ If no capsular support then other lens options available.
Suprachoroidal and Subretinal Haemorrhages
❖Often secondary to age related macular degeneration
❖Rapid loss, & sometimes devastating, loss of vision
❖Clearing blood from beneath the macula is vital if any vision is to be salvaged
TRAUMA

Machete or “Panga”

Scleral lacerations
These are not always obvious. Look for:
▪ Slightly oval pupil ▪ Anterior chamber deeper
than other eye ▪ Hyphaema in the
presence of a lid laceration
Total hyphaema with edge of scleral laceration visible on downgaze

Military Setting
Conflict Eye Injuries % US Civil War 0.52
WW1 1.54 WW2 2-3 Korea 2-8
Arab-Israeli 5-10 Vietnam 5-9
Gulf 13

Source Metal Composition Shells (Naval 5” and 155mm Artillery)
High grade steel (98% Fe, 1.7% Cu, 0.2% Mn) with 99.5% Cu rotation band
Bombs (2000, 1000 and 500 lbs)
Grade 302/303 stainless steel (69% Fe, 18% Cr, 9% Ni & Mn) and lead based paint.
Cluster Bomb Units Grade 301 steel (69% Fe, 19% Ni, 0.15% Cr), pyrotechnic Sirconium and plastic fins
Land Mines Aluminium alloy Grenades Zn alloy base, Grade 302 steel lever, Barium chromate
parts & zirconium-nickel alloy parts Bullets (Rifle) Brass or Cu jacket, lead-tin alloy and steel core (brass
jackets usually have pure copper rotating bands) Bullets (small calibre) Lead and lead-tin alloy BBs Various (Brass, Cu alloy, steel) Pellet-gun pellets Lead-tin alloy
Thank You

Retin
al d
etac
hmen
t; ca
use
and
type
Joe
Wol
fer
Toro
nto
Can
ada
•Re
tinal
det
achm
ent i
s th
e se
para
tion
of th
e ne
uros
enso
ry re
tina
from
the
unde
rlyin
g re
tinal
pi
gmen
t epi
thel
ium
(RPE
)

•A
retin
al d
etac
hmen
t can
be
eith
er
rheg
mat
ogen
ous
(RRD
) or n
on-rh
egm
atog
enou
s (n
on-R
RD)
•Rh
egm
atog
enou
s m
eans
that
ther
e ha
s be
en a
n ac
tual
tear
in th
e re
tina
itsel
f.

•In
a R
RD, fl
uid
from
the
vitre
ous
cavi
ty e
nter
s th
e su
b re
tinal
spa
ce th
roug
h a
brea
k in
the
retin
a.
•RR
D c
an b
e ei
ther
prim
ary
or s
econ
dary
•Pr
imar
y RR
D a
re s
pont
aneo
us a
nd a
re n
ot th
e re
sult
of tr
aum
a, in
flam
mat
ion,
sur
gery
or a
ny
othe
r spe
cific
ocu
lar d
isor
der

•Pr
imar
y RR
D is
pre
cede
d by
alte
ratio
ns in
the
vitre
ous
whi
ch p
redi
spos
e to
retin
al d
etac
hmen
t
•Th
e m
ost c
omm
on R
RD is
retin
al d
ialy
sis
or
gian
t ret
inal
tear
see
n in
the
Shih
Tzu
•In
this
bre
ed th
e re
tinal
tear
is th
ough
t to
occu
r af
ter v
igor
ous
head
sha
king
•Th
e vi
goro
us h
ead
shak
ing
cau
ses
a co
up-
cont
rcou
p ef
fect
dam
agin
g th
e re
tina.
Bec
ause
th
ese
Shih
Tzu
’s ha
ve a
liqu
ified
vitr
eous
, the
re is
no
thin
g to
hol
d th
e re
tina
in p
lace
dur
ing
this
vi
goro
us s
haki
ng.
•It
is a
lso
my
opin
ion,
that
man
y of
thes
e do
gs
have
per
iphe
ral c
ystic
cha
nge
in th
e re
tina
that
re
sults
in a
wea
k sp
ot th
at te
ars
mor
e ea
sily
du
ring
head
sha
king
.

Can
ine
•I b
elie
ve th
at p
rem
atur
e vi
treal
liqu
efac
tion
occu
rs in
the
Shih
Tzu
, and
man
y ot
her b
reed
s,
as a
prim
ary
inhe
rited
dis
orde
r.

•W
hen
a re
tinal
dia
lysi
s oc
curs
, the
neu
rose
nsor
y re
tina
tear
s aw
ay a
t the
ora
cilia
ris re
tinae
.
•A
gian
t ret
inal
tear
(GRT
) inv
olve
s 90
deg
rees
or
mor
e of
retin
al c
ircum
fere
nce
with
atta
ched
vi
treou
s ge
l to
an a
nter
ior fl
ap o
f ret
ina
•Th
ese
tear
s us
ually
, and
fairl
y ra
pidl
y, pr
ogre
ss
from
a d
orsa
l RD
to a
com
plet
e de
tach
men
t
•Th
is re
sults
in a
retin
a th
at h
angs
lim
ply
from
the
optic
ner
ve h
ead
in a
vei
l-lik
e co
nfigu
ratio
n.
•Th
is re
tina
may
als
o be
twis
ted
arou
nd it
self,
up
to 9
0 de
gree
s


•An
othe
r for
m o
f prim
ary
RRD
invo
lves
opt
ic
nerv
e co
lobo
ma,
suc
h as
in s
een
in C
ollie
eye
an
omal
y (C
EA)
•In
this
dis
orde
r the
re is
sep
arat
ion
of re
tinal
la
yers
at t
he ju
nctio
n of
the
colo
bom
a an
d no
rmal
retin
al ti
ssue
•Th
is a
llow
s flu
id fr
om th
e re
tina
to e
nter
the
sub
retin
al s
pace

•O
ther
type
s of
prim
ary
retin
al d
etac
hmen
ts
invo
lve
atro
phic
retin
al te
ars
or h
oles

•Th
ese
atro
phic
hol
es c
an o
ccur
sec
onda
ry to
ag
e or
occ
ur in
are
as o
f pre
viou
s re
tinal
in
flam
mat
ion

•Se
cond
ary
RRD
is c
ause
d by
trau
ma,
gla
ucom
a (s
tretc
hing
of t
he g
lobe
), le
ns s
urge
ry (e
ither
le
nsec
tom
y fo
r len
s lu
xatio
n, o
r ph
acoe
mul
sific
atio
n), a
ggre
ssiv
e la
ser
retin
opex
y, or
sur
gery
invo
lvin
g th
e ci
liary
bod
y
•Th
e m
ost p
rom
inen
t cau
se o
f sec
onda
ry R
RD is
ca
tara
ct s
urge
ry.

•N
on-R
RD is
cla
ssifi
ed a
s ei
ther
ser
ous
(flui
d bu
ild u
p un
der t
he re
tina)
or t
ract
iona
l
•Se
rous
retin
al d
etac
hmen
t occ
urs
with
out a
br
eak
in th
e re
tina
and
resu
lts fr
om fl
uid
accu
mul
atio
n be
twee
n th
e ph
otor
ecep
tors
and
th
e RP
E. S
erou
s RD
can
be
eith
er in
flam
mat
ory
or e
xuda
tive.
•Th
e m
ost c
omm
on c
ause
s ar
e im
mun
e m
edia
ted
chor
oidi
tis, i
nfec
tious
cho
roid
itis,
neo
plas
ia, o
r hy
perte
nsio
n.

•Tr
actio
nal R
D o
ccur
s w
hen
ther
e is
a p
ullin
g fo
rce
(ban
d or
mem
bran
e) in
the
vitre
ous
that
fo
rces
the
retin
a to
sep
arat
e fro
m th
e RP
E
•Th
is c
an re
sult
from
pen
etra
ting
inju
ry to
the
post
erio
r seg
men
t, pr
evio
us in
flam
mat
ion,
pr
evio
us v
itrea
l hem
orrh
age
or a
s a
prim
ary
vitre
al d
yspl
asia
in s
ome
bree
ds
•Tr
actio
nal R
D is
ver
y di
fficu
lt to
trea
t in
the
dog
•Re
quire
s m
etic
ulou
s vi
trect
omy
and
mem
bran
e pe
elin
g w
hich
is v
ery
diffi
cult
in th
e do
g
•M
embr
anes
ofte
n re
grow
afte
r sur
gery
mak
ing
RD re
curre
nces
hig
h
•In
hum
ans
the
mos
t com
mon
cau
se o
f tra
ctio
nal
RD is
dia
betic
retin
opat
hy

•En
doph
thal
miti
s or
infla
mm
atio
n of
the
entir
ety
of
the
glob
e is
ano
ther
cau
se o
f RD
•It
is a
n in
flam
mat
ory
resp
onse
to in
fect
ion,
ba
cter
ial,
fung
al, p
aras
itic
or v
iral
•In
dog
s, th
e m
ost c
omm
on c
ause
for
endo
phth
alm
itis
is c
atar
act s
urge
ry
•Al
l pos
t-ope
rativ
e en
doph
thal
miti
s ca
ses
shou
ld
unde
rgo
ocul
ar u
ltras
ound
•Be
st th
erap
y fo
r end
opht
halm
itis
is in
travi
treal
an
tibio
tics
and
ster
oids
(Trie
ssen
ce)
•C
ompl
ete
vitre
ctom
y m
ay b
e re
quire
d bu
t is
diffi
cult
due
to th
e br
eakd
own
in th
e bl
ood
ocul
ar
barri
er
•In
travi
treal
van
com
ycin
and
Trie
ssen
ce is
my
mai
nsta
y th
erap
y

•Le
ns lu
xatio
n ca
n be
ano
ther
pre
curs
or to
RD
du
e to
dis
rupt
ion
of le
ns z
ones
at t
he o
ra e
rrata
.
•Th
ere
is a
lso
disr
uptio
n of
the
ante
rior h
yalo
id
face
cau
sing
liqu
efac
tion
of th
e vi
treou
s.
•Ad
junc
tive
trans
pupi
llary
lase
r ret
inop
exy
may
de
crea
se th
e ra
te o
f RD
afte
r sur
gery
for l
uxat
ed
lens
.
•D
ropp
ed n
ucle
ar fr
agm
ents
dur
ing
phac
oem
ulsi
ficat
ion
•In
hum
ans,
PPV
and
frag
men
t rem
oval
is
perfo
rmed
if >
25%
of t
he n
ucle
us is
pre
sent

•In
dog
s, P
PV d
urin
g th
e co
urse
of a
cat
arac
t su
rger
y is
ext
rem
ely
diffi
cult
to d
o. T
he c
orne
al
inci
sion
mus
t be
clos
ed a
nd th
e ey
e pr
opto
sed
for p
rope
r exp
osur
e.
•20
g PP
V is
then
per
form
ed a
n a
fragm
atom
e is
in
trodu
ced
to e
mul
sify
the
nucl
ear f
ragm
ents
•In
my
opin
ion,
it is
act
ually
eas
ier,
and
safe
r to
perfo
rm a
nter
ior v
itrec
tom
y th
roug
h th
e co
rnea
l in
cisi
on, a
nd th
en u
se th
e ph
acop
robe
to
capt
ure
and
emul
sify
the
nucl
ear f
ragm
ents
. So
me
fragm
ents
may
be
left
behi
nd if
they
are
sm
all.
•Sy
stem
ic s
tero
ids
are
requ
ired
post
-ope
rativ
ely

Tran
pupi
llary
lase
r re
tinop
exy;
whe
n is
this
us
eful
Joe
Wol
fer
Toro
nto
Can
ada
•Tr
ying
to d
ecid
e if
you
shou
ld d
o fu
ll pa
rs p
lana
re
tinal
sur
gery
, or s
impl
y do
tran
spup
illary
lase
r re
tinop
exy
can
be c
onfu
sing
.

•Tr
ansp
upilla
ry la
ser r
etin
opex
y, or
TPL
R, is
onl
y us
eful
if th
ere
is s
ome
retin
a st
ill at
tach
ed.
•La
ser b
urns
into
the
chor
oid,
can
onl
y be
mad
e if
the
retin
a is
in d
irect
app
ositi
on to
the
RPE
•Th
e m
ost c
omm
on ti
me
for T
PLR
to b
e us
ed is
in
a re
tinal
det
achm
ent i
mm
edia
tely
afte
r cat
arac
t su
rger
y. S
ince
thes
e do
gs a
re b
eing
mon
itore
d ca
refu
lly, t
he d
etac
hmen
t is
usua
lly s
een
at a
n ea
rly s
tage

•Th
e ot
her c
omm
on ti
me
for T
PLR
to b
e us
ed is
w
hen
a la
tera
l or v
entra
l det
achm
ent i
s se
en o
n ul
traso
und
and
the
owne
rs c
anno
t affo
rd
com
bine
d ph
aco/
pars
pla
ns v
itrec
tom
y
•In
that
cas
e, I
will
perfo
rm ro
utin
e ph
acoe
mul
sific
atio
n w
ith n
o IO
L. A
nd th
en
perfo
rm p
erfo
rm a
tran
spup
illary
lase
r re
tinop
exy
(bar
rier r
etin
opex
y)

•O
nce
the
retin
a is
com
plet
ely
deta
ched
, we
are
beyo
nd th
e po
int o
f doi
ng T
PLR.
•TP
LR is
use
d in
circ
umst
ance
s w
here
ther
e is
a
parti
al re
tinal
det
achm
ent,
but p
ars
plan
a vi
trect
omy
is u
ndes
irabl
e.
•So
me
owne
rs c
anno
t affo
rd fu
ll re
tinal
sur
gery
or
the
eye
may
be
too
fragi
le to
with
stan
d pa
rs
plan
a vi
trect
omy
•Ba
rrier
retin
opex
y w
orks
bes
t if t
he te
ar in
the
retin
a is
late
ral t
o th
e op
tic n
erve
hea
d an
d no
t su
perio
r.
•Su
perio
r tea
rs te
nd to
pro
gres
s ra
pidl
y an
d br
eak
thro
ugh
the
lase
r ret
inop
exie
s du
e to
gr
avity
and
the
wei
ght o
f the
retin
a.


•TP
LR is
per
form
ed w
ith a
lase
r ind
irect
hea
dset
an
d a
diod
e la
ser a
ttach
men
t. A
20g
lens
is
used
to fo
cus
the
lase
r bea
m to
a p
inpo
int o
n th
e re
tinal
sur
face
•Pa
tient
is in
dor
sal o
r ste
rnal
recu
mbe
ncy
depe
ndin
g on
the
natu
re a
nd p
ositi
on o
f the
de
tach
men
t
•Th
e pu
pil i
s di
late
d m
axim
ally
prio
r to
indu
ctio
n of
ane
sthe
sia.
Int
rave
nous
neu
ropa
raly
tic is
re
quire
d to
mov
e th
e ey
e ce
ntra
lly.
•Li
d sp
ecul
um a
nd s
tay
sutu
res
may
als
o be
re
quire
d

•La
ser b
urns
are
then
pla
ced
in a
dou
ble
or tr
iple
ro
w a
long
the
lead
ing
edge
of t
he d
etac
hmen
t to
prev
ent p
rogr
essi
on o
f the
det
achm
ent
•La
ser s
ettin
gs v
ary
depe
ndin
g up
on d
egre
e of
pi
gmen
tatio
n, a
ngle
of i
ncid
ence
of t
he la
ser
beam
, and
rela
tive
opac
ifica
tion
of th
e oc
ular
m
edia
•I g
ener
ally
sta
rt at
abo
ut 2
00m
W a
nd 5
00m
s.
•G
radu
ally
wor
k up
war
ds in
pow
er u
ntil
whi
te
spot
s ap
pear
in th
e re
tina
so th
at y
ou k
now
that
a
burn
has
bee
n cr
eate
d.

•It
take
s ap
prox
imat
ely
14 d
ays
for t
he la
ser
burn
s to
reac
h th
eir m
axim
um s
treng
th, s
o th
e pa
tient
mus
t be
kept
ent
irely
qui
et fo
r tha
t du
ratio
n.
•C
age
rest
is id
eal
•TP
LR w
orks
bes
t on
phak
ic p
atie
nts.
Aph
akic
ey
es d
o no
t foc
us th
e la
ser b
eam
as
wel
l.
•Ps
eudo
phak
ic e
yes
are
mor
e di
fficu
lt as
you
m
ust s
omet
imes
wor
k ar
ound
the
IOL
to g
et th
e la
ser b
urns
in th
e rig
ht p
lace
•Th
e ot
her t
echn
ique
for b
arrie
r ret
inop
exy
is
perfo
rmed
via
use
of a
n en
dola
ser.

•Th
is p
roce
dure
invo
lves
rem
oval
of t
he c
atar
acts
le
ns, f
ollo
wed
by
mak
ing
a sm
all i
ncis
ion
in th
e po
ster
ior l
ens
caps
ule.
•Th
e vi
treou
s is
left
inta
ct a
nd th
e en
dola
ser
prob
e is
adv
ance
d fro
m th
e co
rnea
l inc
isio
n,
thro
ugh
the
tear
in th
e po
ster
ior l
ens
caps
ule
and
thro
ugh
the
vitre
ous
to th
e ar
ea o
f ret
ina
in
ques
tion.
•Th
is fi
lm is
cou
rtesy
of D
r Din
elli
Bras
, Pue
rto
Rico

•Th
e en
dola
ser c
an a
lso
be u
sed
afte
r in
traca
psul
ar le
ns e
xtra
ctio
n in
cas
es o
f ant
erio
r or
pos
terio
r len
s lu
xatio
n, to
insp
ect t
he
perip
hera
l ret
ina
and
lase
r any
retin
al te
ars
that
ar
e pr
esen
t.
•Ba
rrier
retin
opex
y ca
n be
per
form
ed b
y th
e tra
nssc
lera
l app
roac
h, h
owev
er, i
t is
actu
ally
qu
ite e
asy
to c
reat
e a
full
thic
knes
s ho
le in
the
retin
a an
d w
orse
n th
e de
tach
men
t


Com
plic
atio
ns o
f VR
surg
ery
Joe
Wol
fer
Toro
nto
Can
ada
•C
ompl
icat
ions
of V
R su
rger
y ca
n be
div
ided
into
in
traop
erat
ive
com
plic
atio
ns a
nd p
osto
pera
tive
com
plic
atio
ns.

•In
traop
erat
ive
com
plic
atio
ns in
clud
e bu
t are
not
lim
ited
to;
•Lo
ss o
f pro
ptos
is d
urin
g su
rger
y
•Th
e gl
obe
sudd
enly
dro
ps b
ack
into
the
orbi
t
•Th
is is
why
brid
le s
utur
es a
re p
lace
d at
3 a
nd 6
o’
cloc
k, to
qui
ckly
faci
litat
e re
prop
tosi
s of
the
glob
e
•Pl
acem
ent o
f the
infu
sion
por
t int
o th
e su
b re
tinal
sp
ace.
•If
the
fluid
s ar
e tu
rned
on
at th
is p
oint
, flui
d w
ill flo
w s
ub re
tinal
and
furth
er d
etac
h th
e re
tina
•Ve
ry im
porta
nt to
che
ck p
lace
men
t of t
he p
ort
befo
re in
itiat
ing
surg
ery

•C
horo
idal
hem
orrh
age
•O
ccur
s sp
onta
neou
sly
and
may
com
plet
ely
obsc
ure
view
of f
unds
•Th
e po
le is
rais
ed to
incr
ease
intra
ocul
ar
pres
sure
and
tam
pona
de th
e bl
eed

•Re
tain
ed p
erflu
oroc
tane
(PFO
)
•PF
O is
hig
hly
toxi
c to
the
retin
a an
d if
left
in th
e ey
e w
ill ca
use
retin
itis,
uve
itis
and
blin
dnes
s

•Re
tain
ed P
FO c
an a
lso
emul
sify
and
mig
rate
into
th
e an
terio
r cha
mbe
r cau
sing
uve
itis
and
dam
age
to th
e en
doth
elia
l sur
face
of t
he c
orne
a
•Po
stop
erat
ive
com
plic
atio
ns in
clud
e bu
t are
not
lim
ited
to;

•C
orne
al u
lcer
atio
n
•Pr
opto
sis
of th
e gl
obe
seem
s to
pre
disp
ose
to
corn
eal u
lcer
atio
n
•C
orne
a is
cov
ered
with
vis
coel
astic
dur
ing
the
surg
ery
•To
pica
l lub
ricat
ing
oint
men
t is
used
for o
ne w
eek
post
sur
gery
•G
lauc
oma
•Po
st o
pera
tive
ocul
ar h
yper
tens
ion
can
occu
r, es
peci
ally
if th
e ey
e is
ove
rfille
d w
ith s
ilicon
e oi
l
•To
pica
l car
boni
c an
hydr
ase
inhi
bito
rs a
re u
sed
lifel
ong
afte
r sur
gery
•Le
akag
e of
silic
one
oil i
nto
the
ante
rior c
ham
ber
can
occu
r pos
t ope
rativ
ely
espe
cial
ly if
ther
e is
an
y zo
nule
loss
aro
und
the
lens
•If
the
leak
age
is s
igni
fican
t eno
ugh
and
even
tual
ly re
sults
in d
ecom
pens
atio
n of
the
corn
eal e
ndot
helia
l cel
ls re
sulti
ng in
cor
neal
ed
ema,
it m
ust b
e re
mov
ed

•U
nder
gen
eral
ane
sthe
sia,
the
ante
rior c
ham
ber
is fi
lled
with
vis
coel
astic
, to
pres
suriz
e th
e fro
nt
of th
e ey
e, a
nd th
e si
licon
e oi
l is
“milk
ed” o
ut o
f th
e ey
e th
roug
h a
smal
l 20
g in
cisi
on m
ade
with
an
MVR
bla
de

•Si
licon
e oi
l will
also
som
etim
es le
ak fr
om th
e sc
lera
l wou
nds
into
a s
ubco
njun
ctiv
al lo
catio
n
•Th
is d
oes
not g
ener
ally
cau
se a
nyth
ing
but a
co
smet
ic p
robl
em a
nd th
e oi
l gen
eral
ly d
oes
not
need
to b
e re
mov
ed.
•Sl
ippa
ge o
f the
retin
a, u
nder
neat
h th
e si
licon
e oi
l, w
ill, in
rare
inst
ance
, occ
ur a
nd m
ay le
ad to
re
datc
hmen
t of t
he re
tina

•So
me
dogs
, yea
rs d
own
the
road
will
expe
rienc
e de
gene
ratio
n of
the
retin
a, th
at is
thou
ght
poss
ibly
to b
e du
e to
pre
senc
e of
silic
one
oil i
n th
e ey
e
•In
hum
an V
R su
rger
y, th
e si
licon
e oi
l is
gene
rally
re
mov
ed fr
om th
e ey
e af
ter a
bout
3 m
onth
s.
•Th
is is
ver
y di
fficu
lt an
d ex
pens
ive
to d
o in
the
dog,
so
the
silic
one
oil i
s ge
nera
lly le
ft in
pla
ce
for t
he li
fetim
e of
the
patie
nt

•To
try
and
prot
ect t
he re
tina,
pat
ient
s ar
e pu
t on
an o
ral c
alci
um c
hann
el b
lock
er (a
mlo
dipi
ne
0.62
5 m
g/5k
g) fo
r life
•So
met
imes
due
to s
ilicon
e oi
l lea
kage
, or f
or n
o ap
pare
nt re
ason
at a
ll, o
ne w
ill en
d up
with
an
inco
mpl
ete
silic
one
oil fi
ll.
•Th
is le
aves
the
vent
ral r
etin
a pr
one
to
rede
tach
men
t

•In
rare
inst
ance
s, fo
r a v
arie
ty o
f rea
sons
, the
re
tina
cann
ot b
e su
cces
sful
ly re
atta
ched
. Si
nce
we
know
that
chr
onic
retin
al d
etac
hmen
t lea
ds to
pr
e-iri
dal fi
brov
ascu
lar m
embr
ane
(PIF
M)
form
atio
n an
d ne
ovas
cula
r gla
ucom
a, I
will
usua
lly a
t tha
t poi
nt, p
erfo
rm a
com
plet
e re
tinec
tom
y (re
mov
al o
f the
retin
a)
•Th
e ey
e is
then
fille
d w
ith s
ilicon
e oi
l as
usua
l.


29/09/2017
1
BrAVO discussion 2017 ‘How I treat….’
SCCEDs
David Gould
BSc (Hons), BVM&S, PhD, DVOphthal, DipECVO, FRCVS
Davies Veterinary Specialists
Spontaneous Chronic Corneal Epithelial Defect (SCCED)
Shallow, epithelial loss only
Underrun edges
Older dogs
Ineffective vascularisation response

29/09/2017
2
Anterior corneal anatomy
1 Epithelium
2 Basement membrane
3 Anterior stroma
Integrins, hemidesmosomes
Anchoring fibrils
(VII collagen)
BM
Stroma
Epithelium
Anchoring plaque
(laminin, I collagen)
Adhesion complex fibronectin
Pathology of SCCED
• Reduction/ loss of
hemidesmosomes, BM and
adhesion complexes
• Hyper-innervation
•Hyalinized layer anterior stroma
Integrins, hemidesmosomes
Anchoring fibrils
(VII collagen)
BM
Stroma
Epithelium
Anchoring plaque
(laminin, I collagen)
fibronectin

29/09/2017
3
Medical treatments?
Serine protease inhibitors
Tetracyclines
Serum
Serine Protease inhibitors?
Theory
Increased proteolysis occurs in chronic ulcers
• Erosion of ECM proteins
• Delayed healing
SP inhibitors may counteract this
C o l l a g e n o l y s i s
MMPs Serine proteases

29/09/2017
4
Evidence?
Debridement + aminocaproic acid for SCCEDs (Regnier et al Vet Record 2005)
At 3 weeks • ACA 94% healed
• Controls 41% healed
C o l l a g e n o l y s i s
MMPs Serine proteases
Serine Protease inhibitors?
Evidence?
Debridement + aminocaproic acid for SCCEDs (Regnier et al Vet Record 2005)
At 3 weeks • ACA 94% healed
• Controls 41% healed
Critique
Control Tx was gentamicin
Not all SCCEDs show elevated proteolysis (Willeford et al VO 1998)
C o l l a g e n o l y s i s
MMPs Serine proteases
Serine Protease inhibitors?

29/09/2017
5
Tetracyclines?
Theory Doxycycline and tetracycline
inhibit MMPs in vitro and in equine tears
Oxytetracycline upregulates TGF-β in corneal epith cells and promotes migration
(Chandler et al Exp Eye Res 2007)
C o l l a g e n o l y s i s
MMPs Serine proteases
Tetracyclines?
Evidence Following grid keratotomy,
topical oxytetacycline shortens healing time compared to controls or those treated with oral
doxycycline (Chandler et al JAVMA 2010)
Critique Recent study reported opposite
Slower healing time with OTC cf ofloxacin
(Dees et al 2017)
C o l l a g e n o l y s i s
MMPs Serine proteases

29/09/2017
6
Serum?
Theory
Contains antiproteases, fibronectin…
May reduce collagenolysis and supply glycoproteins for wound healing
C o l l a g e n o l y s i s
MMPs Serine proteases
serum
Serum?
Critique
No reported studies for SCCEDs
Fibronectin already at wound site
C o l l a g e n o l y s i s
MMPs Serine proteases
serum

29/09/2017
7
Medical treatments
Conclusion
No evidence for serum
OTC reduces healing time in 1 study, prolongs it in another
Aminocaproic acid reported effective
• Commercial availability?
Surgical treatment of SCCED
Technique
Debridement
Grid /punctate keratotomy
Diamond burr/ Algerbrush
Thermokeratoplasty
Superficial keratectomy
Success rate
~50%
~ 80%
92%
100%
100% (Bentley JAAHA 2005, Gosling et al VO 2013, Dees et al 2017)

29/09/2017
8
My approach?
Diamond burr once, perhaps twice
i/v sedation Butorphanol 0.2mg/kg i/v bolus
Medetomidine 10ug/kg, diluted in 5mls saline and given to effect
My approach?
Diamond burr once, perhaps twice
i/v sedation Butorphanol 0.2mg/kg i/v bolus
Medetomidine 10ug/kg, diluted in 5mls saline and given to effect
Contact lens
Chloramphenicol, ± lubricants, systemic NSAIDs

29/09/2017
9
My approach?
Diamond burr once, perhaps twice
i/v sedation Butorphanol 0.2mg/kg i/v bolus
Medetomidine 10ug/kg, diluted in 5mls saline and given to effect
Contact lens
Chloramphenicol, ± lubricants, systemic NSAIDs
3 weeks between procedures
If possible, SK before vascularisation
Questions?

29/09/2017
10
Refs: Medical treatment of SCCED
Treatment Success rate Reference
Protease inhibitors
Aprotinin 33% PSGAG 82% Aminocaproic acid 94% Serum?
Morgan & Abrams VCO 1994, Miller VetMed 1996, Willeford et al VO 1998, Regnier et al VR 2005
Substance P 70% Murphy et al IOVS 2001
Epidermal GF 80% Kirschner et al VCNA 1991
Chondroitin sulfate 81% Ledbetter et al Prog ACVO 2003
Tetracyclines
N/A Chandler et al JAVMA 2010
Refs: Surgical treatment of SCCED
Treatment Success rate Reference
Debridement ≈ 50% Kirschner et al VCNA 1991, Morgan et al VCO 1994, Stanley et al VO 1998
Debridement + BCL or TEF
58-64% Morgan et al VCO 1994
Debridement + punctate/ grid keratotomy
68-88% Champagne et al JAAHA 1992, Morgan et al VCO 1994, Stanley et al VO 1998
Diamond burr + BCL 92% Gosling et al VO 2013 Dees et al VO 2017
Thermal cautery 100% Bentley and Murphy JAVMA 2004
Superficial keratectomy 100% Stanley et al VO 1998

LENS LUXATION
ClaudiaHartleyBVScCertVOphthalDipECVOMRCVS
LENSLUXATIONIntroducAonFirstdescribedinacasereportin1969ThenaseriesofpapersbyRogerCurAs–bodyofworkonprimarylensluxaAon1978-1990Histopathology-Morris&DubielzigTreatment–Gloveretal,O’Reillyetal,Binderetal,Wilkieetal,Stuhretal,Montgomeryetal,Inheritance–Willisetal,CurAsetal,LazarusetalGeneAcs–Sarganetal,Fariasetal,Gouldetal
LENSLUXATIONPrimarylensluxaAonDisintegraAonofzonulesProgressivelooseningofthelensIridodenesisVitrealprolapsePhacodenesisAnteriorlensluxaAonPosteriorlensluxaAon
JRTTibetanterrierSharpeiBordercollieMiniaturebullterriermutaAonADAMTS17

• Suspension• zonules
Lens
• Suspension• zonules
Lens
• Pathogenesis• degeneratezonules
Lens

• LensluxaAon/subluxaAon
aphakiccrescentvitreousprolapse
anteriorposterior
cataract
Lens
• LensluxaAon/subluxaAon
inheriteddefect(s)trauma2’glaucoma
Lens
• LensluxaAon/subluxaAon
treatment• Surgery• IntracapsularlensextracAon(ICLE)• PhacoemulsificaAon
Lens
MedicalCouchingProstaglandinanalogue

• LensluxaAon/subluxaAon
treatment• Surgery• IntracapsularlensextracAon(ICLE)• PhacoemulsificaAon
Lens
MedicalCouchingProstaglandinanalogue
• LensluxaAon/subluxaAon
treatment• Surgery• IntracapsularlensextracAon(ICLE)• PhacoemulsificaAon
Lens
MedicalCouchingProstaglandinanalogue
TLGlover,MGDavidson,MPNasisse,andDKOlivero(1995)TheintracapsularextracAonofdisplacedlensesindogs:aretrospecAvestudyof57cases(1984-1990).JournaloftheAmericanAnimalHospitalAssocia7on:January1995,Vol.31,No.1,pp.77-81.
• LensluxaAon/subluxaAon
treatment• Surgery• IntracapsularlensextracAon(ICLE)• PhacoemulsificaAon
Lens
MedicalCouchingProstaglandinanalogue
Intracapsular lensectomy and sulcus intraocular lens fixationin dogs with primary lens luxation or subluxation
Charles M. Stuhr, Hillary K. Schilke and Christina ForteAnimal Eye Clinic, 2 Pimpewaug Rd., Wilton, CT 06897, U.S.A.
Address communications to:
C. M. Stuhr
Tel.: (203) 762-9399
Fax: (203) 762-2775
e-mail: [email protected]
AbstractObjective To evaluate the postoperative results of lensectomy and sulcus intraocularlens fixation (SIOLF) via an ab interno approach in dogs with progressive lens
subluxation or early luxation.Study design Retrospective study.Animals studied Twenty eyes from 19 dogs presented to the Animal Eye Clinic for
lens luxation or subluxation between 1999 and 2006.Methods Medical records were reviewed to evaluate preoperative lens position, vision
status, intraocular pressure (IOP), and whether surgery was performed on anemergent or elective nature. Lensectomy and SIOLF were performed and
postoperative status including vision, glaucoma, and retinal detachment was assessed.Results Average age was 8.6 years (range 4–14 years) and 55% (11/20) were terriers.
Patients were followed a mean of 29.2 months (range 1–92 months) after surgery.Retinal detachment or secondary glaucoma was observed in 1 of 20 (5%) and 5 of 20(20%) eyes, respectively, with 1 of 20 (5%) exhibiting both. Mean preoperative IOP
was 16 mmHg and preoperative lens position was equally divided between luxatedand subluxated lenses. Surgery was performed more frequently as an elective
procedure (18/20; 90%) due to normalized IOP vs. an emergency procedure (2/20;10%). Vision was retained in 70% (14/20) of eyes with a mean time to vision loss of
41 months in the remaining eyes due to glaucoma, retinal detachment, or retinaldegeneration.
Conclusions Complications of glaucoma and retinal detachment after SIOLF in thisstudy were less when compared with previously reported incidence rates in the
literature for lensectomy alone which may reflect improved patient selection.
Key Words: lens, lensectomy, luxation, subluxation, sulcus IOL
INTRODUCTION
Acute lens luxation with an associated rapid pressure spike isone of the true surgical emergencies in veterinary ophthal-mology.1 Surgical repair by lensectomy alone or with pri-mary placement of a sulcus-fixated intraocular lens (SIOLF)has been described previously in the veterinary literaturewith only a modicum of long-term success in a limited num-ber of publications.2–4 Complications, primarily retinaldetachment and secondary glaucoma, are not uncommonand are typically associated with irreversible vision loss.1 Asthis surgery is commonly performed on an emergency basiswhen the lens presents in the anterior chamber with a pupil-lary block glaucoma, the intraocular inflammatory response
and its cascade of destructive events have already been initi-ated, which may contribute to postoperative failure. There-fore, early surgical intervention has been advised by some inefforts to minimize these postoperative complications.2,3
In recent years, the goals of intraocular lenticular surgery,primarily cataract extraction, have been focused on achiev-ing a comfortable, sighted eye that is emmetropic.5,6
Emmetropia is achieved by placement of an intraocular lens(IOL) made of polymethylmethacrylate (PMMA) or acrylicinto the capsular bag that remains after routine phacoemul-sification. IOL placement is not possible in intracapsularlensectomy repair without sulcus fixation. Routine place-ment of an IOL after lensectomy has not achieved universalacceptance due to the perceived increase in postoperative
� 2009 American College of Veterinary Ophthalmologists
Veterinary Ophthalmology (2009) 12, 6, 357–360

• LensluxaAon/subluxaAon
treatment• Surgery• IntracapsularlensextracAon(ICLE)• PhacoemulsificaAon
Lens
MedicalCouchingProstaglandinanalogue
SM
ALL A
NIM
ALS
JAVMA, Vol 231, No. 1, July 1, 2007 Scientific Reports: Retrospective Study 89
Lens luxation is a well-recognized clinical disorder in dogs, and common causes include primary lens
zonule disease (primary lens luxation), senescence, and hypermature cataracts.1 Other causes include glau-coma, uveitis, and trauma.1 Canine primary lens luxa-tion is characterized by spontaneous rupture of lens zonules, resulting in lens instability and eventual luxa-tion.1,2 A heritable pattern of disease has been estab-lished in a number of breeds, including various terrier breeds, Shar Peis, and Border Collies, although numer-ous other dog breeds have been suggested to be affected by primary lens luxation.2-11 Although canine primary lens luxation is invariably bilateral, complete lens dis-location generally occurs in 1 eye some time (days to months) before the other eye.1,2,12
Vision-threatening complications of lens luxation include glaucoma and, less commonly, retinal detach-ment. Other complications include uveitis and intraoc-ular hemorrhage. Glaucoma may develop in eyes with
Outcomes of nonsurgical management and efficacy of demecarium bromide treatment
for primary lens instability in dogs: 34 cases (1990–2004)
Daniel R. Binder, DVM, PhD; Ian P. Herring, DVM, MS, DACVO; Tobias Gerhard, BS
From the Department of Small Animal Clinical Sciences, Virginia-Maryland Regional College of Veterinary Medicine, Virginia Tech, Blacksburg, VA 24061-442 (Binder, Herring); and the Department of Pharmacy Health Care Administration, University of Florida, Gainesville, FL 32610-0496 (Gerhard).
Presented in part at the American College of Veterinary Ophthal-mologists Annual Meeting, Washington, DC, October 2004.
Address correspondence to Dr. Herring.
Objective—To determine outcome of initial conservative management for primary lens luxation and evaluate topically administered demecarium bromide miotic treatment for pre-vention of anterior lens luxation, glaucoma, and vision loss in dogs.Design—Retrospective case series.Animals—34 dogs with primary lens luxation.Procedures—Medical records of affected dogs were reviewed for times to anterior luxa-tion, luxation of the lens in the opposite eye, development of glaucoma, and vision loss. Results—At 4 to 6 weeks and at 3 months after diagnosis of lens instability (subluxation or posterior luxation), 100% (34/34 and 29/29, respectively) of conservatively managed eyes retained vision. At 1 year after diagnosis of lens instability, 80% (16/20) of conservatively managed eyes retained vision, and at 2 years after diagnosis of lens instability, 11 of 19 conservatively treated eyes retained vision. The only significant effect of miotic treatment was to delay anterior lens luxation in eyes with lens instability. Miotic treatment did not sig-nificantly affect the time from anterior lens luxation in 1 eye to anterior luxation in the other eye, time to onset of glaucoma, or time to loss of vision in eyes with an unstable lens.Conclusions and Clinical Relevance—Prophylactic topically administered miotic treat-ment may be effective at delaying anterior luxation of an unstable lens in eyes affected by primary lens instability. Conservative medical management of dogs with primary lens insta-bility is a reasonable alternative to surgical removal of a subluxated or posteriorly luxated lens via intracapsular lens extraction. (J Am Vet Med Assoc 2007;231:89–93)
ABBREVIATION
ICLE Intrascapular lens extraction
primary lens instability, regardless of lens position.4,10 Although it is more common for this complication to develop when the lens is displaced into the anterior chamber, it also occurs in a large percentage of eyes with lens subluxation.4,10
Because of the high likelihood of developing sec-ondary glaucoma with subsequent vision loss, anterior lens luxation is considered an ocular emergency requir-ing prompt lens removal via ICLE. In dogs with anterior lens luxation, careful evaluation of the opposite eye of-ten reveals evidence of a subluxated or posteriorly lux-ated lens, which may include vitreous in the anterior chamber, abnormal anterior chamber depth, iridoden-esis, lentodenesis, or an aphakic crescent.1 Although it is widely accepted that prompt ICLE is indicated for an-terior lens luxation, the most appropriate management approach to lenses that are subluxated or posteriorly luxated is unclear.
Broadly speaking, management of a subluxated or posteriorly luxated lens may include surgical ex-traction or a more conservative approach of waiting until anterior luxation occurs prior to surgical inter-vention. Advocates of surgical removal of a sublux-
• LensluxaAon/subluxaAon
treatment• Surgery• IntracapsularlensextracAon(ICLE)• PhacoemulsificaAon
Lens
MedicalCouchingProstaglandinanalogue
TLGlover,MGDavidson,MPNasisse,andDKOlivero(1995)TheintracapsularextracAonofdisplacedlensesindogs:aretrospecAvestudyof57cases(1984-1990).JournaloftheAmericanAnimalHospitalAssocia7on:January1995,Vol.31,No.1,pp.77-81.
• LensluxaAon/subluxaAon
Lens
MedicalCouchingProstaglandinanalogue
InheritanceToy/headshaking

• Bears• PinnipedsandOtariids• Matshchie’streekangaroo
LensLuxaAoninWildAnimals
• Bears• PinnipedsandOtariids• Matshchie’streekangaroo
LensLuxaAoninWildAnimals
JAVMA, Vol 237, No. 4, August 15, 2010 Scientific Reports 429
AQ
UATIC
AN
IMA
LS
Diseases of the cornea and lens are common in captive pinnipeds; environmental factors including water qual-
ity and salinity, light intensity, nutrition, and spatial charac-teristics (eg, orientation of sun on wet and dry areas, depth, exhibit surface color [for reflected light], and animal loading per cubic meter [because of potential water-quality effects]) have been reporteda as the most likely predominant causes. On the basis of results of a study by Dunn et al,b most captive pinnipeds are now housed in saltwater rather than freshwater. However, other factors have been more difficult to implicate as direct causes of ocular disease. There are few published studies1–3 that characterize the ocular changes observed in captive pinnipeds or attempt to identify environmental influ-ences on lens health in these species.
One of the goals of the study reported here was to iden-tify the incidence of lens luxations and cataracts in selected
Risk factors associated with cataracts and lens luxations in captive pinnipeds in the United States and the Bahamas
Carmen M. H. Colitz, DVM, PhD, DACVO; William J. A. Saville, DVM, PhD, DACVIM; Michael S. Renner, DVM; James F. McBain, DVM; Thomas H. Reidarson, DVM, DACZM; Todd L. Schmitt, DVM;
Elizabeth C. Nolan, DVM, MS, DACZM; Steven J. Dugan, DVM, MS, DACVO; Felicia Knightly, DVM; Maya M. Rodriguez, DVM; Johanna C. Mejia-Fava, DVM; Steven D. Osborn, DVM;
Patricia L. Clough, MAT; Scott P. Collins, BS; Beverly A. Osborn, BS; Kimberly Terrell, BS
Objective—To determine risk factors for lens luxation and cataracts in captive pinnipeds in the United States and the Bahamas.Design—Cross-sectional study.Animals—111 pinnipeds (99 California sea lions [Zalophus californianus], 10 harbor seals [Phoca vitulina], and 2 walruses [Odobenus rosmarus]) from 9 facilities.Procedures—Eyes of each pinniped were examined by a veterinary ophthalmologist for the presence of cataracts or lens luxations and photographed. Information detailing husbandry practices, history, and facilities was collected with a questionnaire, and descriptive statisti-cal analyses were performed for continuous and categorical variables. Odds ratios and as-sociated 95% confidence intervals were estimated from the final model.Results—Risk factors for lens luxation, cataracts, or both included age 15 years, history of fighting, history of ocular disease, and insufficient access to shade.Conclusions and Clinical Relevance—Diseases of the lens commonly affect captive pinnipeds. Access to UV-protective shade, early identification and medical management of ocular diseases, and prevention of fighting can limit the frequency or severity of lens-related disease in this population. An extended life span may result from captivity, but this also allows development of pathological changes associated with aging, including cataracts. (J Am Vet Med Assoc 2010;237:429–436)
populations of captive pinnipeds. The authors also sought to identify risk factors that may have a role in the development of lens luxations or cataracts in captive pinnipeds. Califor-nia sea lions (Zalophus californianus) are the most common captive pinniped in most facilities and, consequently, were analyzed as a separate subset of pinnipeds.
Materials and Methods
Animals—One hundred eleven captive pinnipeds of both sexes (99 California sea lions, 10 harbor seals [Phoca
From the Departments of Veterinary Clinical Sciences (Colitz) and Veterinary Preventive Medicine (Saville), College of Veterinary Medicine, The Ohio State University, Columbus, OH 43210; Dolphin Research Center, 58901 Overseas Hwy, Grassy Key, FL 33050 (Renner, Clough); Theater of the Sea, 84721 Overseas Hwy, Islamorada, FL 33036 (Renner, BA Osborn); Busch Entertainment Corporation, 500 SeaWorld Dr, San Diego, CA 92109 (McBain); SeaWorld San Diego, 500 SeaWorld Dr, San Diego, CA 92109 (Reidarson, Schmitt, Collins); SeaWorld Orlando, 7007 Sea Harbor Dr, Orlando, FL 32821 (Nolan); Eye Specialists for Animals PC, 4175 E Iliff Ave, Denver, CO 80222 (Dugan); Denver Zoo, 2300 Steele St, Denver, CO 80205 (Knightly); The Miami Seaquarium, 4400 Rickenbacker Causeway, Miami, FL 33149 (Rodriguez, Mejia-Fava); SeaWorld San Antonio, 10500 SeaWorld Dr, San Antonio, TX 78251 (SD Osborn); and Dolphin Encounters Limited, PO Box SS 6257, Nassau, SS19055, Bahamas (Terrell). Dr. Reidarson’s present address is Reidarson Group, Sea Aquarium, Netherlands Antilles. Ms. Nolan’s present address is Disney’s Animal Programs, Walt Disney World, 1000 W Buena Vista Dr, Lake Buena Vista, FL 32830.
Supported by the Columbus Zoo and The Ohio State University.The authors thank Pamela Ollen-Hughes and Sarah Jayne Buchanan for technical assistance.Address correspondence to Dr. Colitz ([email protected]).
ABBREVIATIONS
LEC Lens epithelial cellMMP Matrix metalloproteinase
JAVMA, Vol 237, No. 4, August 15, 2010 Scientific Reports 429
AQ
UATIC
AN
IMA
LS
Diseases of the cornea and lens are common in captive pinnipeds; environmental factors including water qual-
ity and salinity, light intensity, nutrition, and spatial charac-teristics (eg, orientation of sun on wet and dry areas, depth, exhibit surface color [for reflected light], and animal loading per cubic meter [because of potential water-quality effects]) have been reporteda as the most likely predominant causes. On the basis of results of a study by Dunn et al,b most captive pinnipeds are now housed in saltwater rather than freshwater. However, other factors have been more difficult to implicate as direct causes of ocular disease. There are few published studies1–3 that characterize the ocular changes observed in captive pinnipeds or attempt to identify environmental influ-ences on lens health in these species.
One of the goals of the study reported here was to iden-tify the incidence of lens luxations and cataracts in selected
Risk factors associated with cataracts and lens luxations in captive pinnipeds in the United States and the Bahamas
Carmen M. H. Colitz, DVM, PhD, DACVO; William J. A. Saville, DVM, PhD, DACVIM; Michael S. Renner, DVM; James F. McBain, DVM; Thomas H. Reidarson, DVM, DACZM; Todd L. Schmitt, DVM;
Elizabeth C. Nolan, DVM, MS, DACZM; Steven J. Dugan, DVM, MS, DACVO; Felicia Knightly, DVM; Maya M. Rodriguez, DVM; Johanna C. Mejia-Fava, DVM; Steven D. Osborn, DVM;
Patricia L. Clough, MAT; Scott P. Collins, BS; Beverly A. Osborn, BS; Kimberly Terrell, BS
Objective—To determine risk factors for lens luxation and cataracts in captive pinnipeds in the United States and the Bahamas.Design—Cross-sectional study.Animals—111 pinnipeds (99 California sea lions [Zalophus californianus], 10 harbor seals [Phoca vitulina], and 2 walruses [Odobenus rosmarus]) from 9 facilities.Procedures—Eyes of each pinniped were examined by a veterinary ophthalmologist for the presence of cataracts or lens luxations and photographed. Information detailing husbandry practices, history, and facilities was collected with a questionnaire, and descriptive statisti-cal analyses were performed for continuous and categorical variables. Odds ratios and as-sociated 95% confidence intervals were estimated from the final model.Results—Risk factors for lens luxation, cataracts, or both included age 15 years, history of fighting, history of ocular disease, and insufficient access to shade.Conclusions and Clinical Relevance—Diseases of the lens commonly affect captive pinnipeds. Access to UV-protective shade, early identification and medical management of ocular diseases, and prevention of fighting can limit the frequency or severity of lens-related disease in this population. An extended life span may result from captivity, but this also allows development of pathological changes associated with aging, including cataracts. (J Am Vet Med Assoc 2010;237:429–436)
populations of captive pinnipeds. The authors also sought to identify risk factors that may have a role in the development of lens luxations or cataracts in captive pinnipeds. Califor-nia sea lions (Zalophus californianus) are the most common captive pinniped in most facilities and, consequently, were analyzed as a separate subset of pinnipeds.
Materials and Methods
Animals—One hundred eleven captive pinnipeds of both sexes (99 California sea lions, 10 harbor seals [Phoca
From the Departments of Veterinary Clinical Sciences (Colitz) and Veterinary Preventive Medicine (Saville), College of Veterinary Medicine, The Ohio State University, Columbus, OH 43210; Dolphin Research Center, 58901 Overseas Hwy, Grassy Key, FL 33050 (Renner, Clough); Theater of the Sea, 84721 Overseas Hwy, Islamorada, FL 33036 (Renner, BA Osborn); Busch Entertainment Corporation, 500 SeaWorld Dr, San Diego, CA 92109 (McBain); SeaWorld San Diego, 500 SeaWorld Dr, San Diego, CA 92109 (Reidarson, Schmitt, Collins); SeaWorld Orlando, 7007 Sea Harbor Dr, Orlando, FL 32821 (Nolan); Eye Specialists for Animals PC, 4175 E Iliff Ave, Denver, CO 80222 (Dugan); Denver Zoo, 2300 Steele St, Denver, CO 80205 (Knightly); The Miami Seaquarium, 4400 Rickenbacker Causeway, Miami, FL 33149 (Rodriguez, Mejia-Fava); SeaWorld San Antonio, 10500 SeaWorld Dr, San Antonio, TX 78251 (SD Osborn); and Dolphin Encounters Limited, PO Box SS 6257, Nassau, SS19055, Bahamas (Terrell). Dr. Reidarson’s present address is Reidarson Group, Sea Aquarium, Netherlands Antilles. Ms. Nolan’s present address is Disney’s Animal Programs, Walt Disney World, 1000 W Buena Vista Dr, Lake Buena Vista, FL 32830.
Supported by the Columbus Zoo and The Ohio State University.The authors thank Pamela Ollen-Hughes and Sarah Jayne Buchanan for technical assistance.Address correspondence to Dr. Colitz ([email protected]).
ABBREVIATIONS
LEC Lens epithelial cellMMP Matrix metalloproteinase
• Bears• PinnipedsandOtariids• Matshchie’streekangaroo
LensLuxaAoninWildAnimals

• Bears• PinnipedsandOtariids• Matshchie’streekangaroo
LensLuxaAoninWildAnimals
NY, USA). The ophthalmic examination findings includedminimal direct and consensual pupillary light reflexes inboth eyes (OU) and the intraocular pressures were29 mmHg OD and 33 mmHg OS. The menace responsesand dazzle reflexes were negative, and this was attributedto the deep level of sedation. A small nictitating mem-brane was noted, extending dorsotemporally from the ven-tromedial aspect of the orbit OU. There was a focal areaof full-thickness corneal edema immediately ventral ofaxial in the right eye. The pupils were round, the irideswere dark brown, and a corpora nigra was not presentOU. In the right eye, the lens was anteriorly luxated andthere was an early immature anterior cortical cataract. Inthe left eye, the lens was clear but was subluxated and anaphakic crescent was present dorsotemporally. Iridodone-sis was not present in either eye and neither iris appearedto be hyperpigmented when compared to those of anothertree kangaroo. The retina and optic discs were visibleOU. The optic discs were similar OU and were roundand pale pink in color. A small tuft of vessels was presenton the surface of the optic discs OU but retinal blood ves-sels were not present (paurangiotic retinal vascular pat-tern).4 Clinically, the appearance of the posterior segmentwas similar to that of the guinea pig. A tapetum lucidumwas not present and the retinal pigmented epitheliumappeared to be only partially pigmented creating a red huefrom the underlying choroidal vessels. A complete bloodcell count and biochemistry panel were performed, andthe results were normal. Based on the exam findings, theanimal was diagnosed with an anterior lens luxation ODand a lens subluxation OS. Although the normal range ofintraocular pressures has not been established for this spe-cies, ocular hypertension was also suspected because themeasured pressures were higher than the normal valuesreported for other marsupials.5 Intracapsular lens extractionwas recommended OU. Surgical removal of both lensessimultaneously was considered, but the decision was madeto operate on each eye individually due to concern over thelength of the anesthetic event needed for bilateral surgeryand transport to the surgical facility. No medications wereprescribed prior to surgery because the zookeepers couldnot safely administer topical medications.Forty-one days after the initial exam, the animal was
again immobilized by intramuscular injection using thesame drug combination used for the initial exam and wasthen intubated and maintained under general anesthesiawith isoflurane. The animal was transported under anes-thesia to the surgical facility for a planned intracapsularlens extraction OD. Topical ciprofloxacin 0.3% ophthal-mic solution (Akorn Inc., Lake Forest, IL, USA) and topi-cal neomycin, polymyxin, dexamethasone solution (AlconLab Inc., Fortworth, TX, USA) were administered topi-cally every 5 min (3 drops of each) during transport. Anocular exam found an absence of direct and consensualpupillary light reflexes in both eyes and intraocular pres-sures of 23 mmHg OD and 21 mmHg OS. Other changes
from the initial exam included resolution of the previouslynoted corneal edema OD, progression of the cataract ODto a mature cataract, posterior movement of the lens ODinto the patellar fossa with a nasal aphakic crescent(Fig. 1), enlargement of the aphakic crescent OS, and anearly immature anterior cortical cataract OS. Because theintraocular pressures were elevated at the initial exam,consideration was given to the fact that the lens luxationscould be secondary to chronic glaucoma and buphthalmia.If this were the case, glaucomatous retinal degenerationwould be expected. Thus, a flash electroretinogram (ERG)(BPM-200; Retinographics, Inc., Norwalk, CT, USA) wasperformed OU. The ERGs were performed after 5 min ofdark adaptation. The time permitted for dark adaptionwas shortened from the more typical 15 min due to adesire to limit the length of general anesthesia. The pupilswere not dilated for the ERG due to the lenticular insta-bility. Normal a- and b-waves were apparent when com-pared to other mammals.6 A-wave amplitudes were 51 lVOD and 29 lV OS and the a-wave implicit times were21 ms OD and 19 ms OS. B-wave amplitudes were111 lV OD and 62 lV OS (b-wave reference range>100 lV in our electrodiagnostic laboratory for dogs;ERG values for normal tree kangaroos have not beenestablished) and the b-wave implicit times were 44 ms ODand 39 ms OS. The lower b-wave amplitude OS wasattributed to the lack of pupillary dilation although retinaldegeneration could not be definitively excluded. The rightpupil was more dilated than the left presumably due tomechanical interference from the luxated lens.The right eye was aseptically prepared for surgery.
Atracurium (0.1 mg/kg; Sagent Pharmaceuticals, Inc.,Schaumburg, IL, USA) was administered intravenously tocentralize the globe, and the animal was mechanically ven-tilated; this single dose provided adequate globe centrationfor the procedure. An intracapsular lens extraction wasperformed using an operating microscope (OPMI VISU
Figure 1. Photograph of the right eye immediately prior to
intracapsular lens extraction. Note the mature cataract and temporal
aphakic cresent.
© 2014 American College of Veterinary Ophthalmologists, Veterinary Ophthalmology, 18, 81–85
82 MC L E AN AND Z IMM E RMAN
CASE REPORT
Bilateral lens luxation and intracapsular lens extractionsin a Matshchie’s tree kangaroo
Nancy Johnstone McLean* and Ralph Zimmerman†*VCA Veterinary Care Animal Hospital and Referral Center, 9901 Montgomery Boulevard NE, Albuquerque, NM, 87111, USA;
and †ABQ Biopark, Rio Grande Zoo, 903 Tenth St. SW, Albuquerque, NM, 87102, USA
Address communications to:
N. J. McLean
Tel.: +1 505-296-2982
Fax: +1 866-822-2573
e-mail: nancyjmclean@gmail.
com
AbstractAn adult, female, captive, Matshchie’s tree kangaroo was diagnosed with an anteriorlens luxation in the right eye and a lens subluxation in the left eye. Both eyes were
treated surgically with intracapsular lens extractions. A 360° rhegmatogenous retinaldetachment was diagnosed 6 months postoperatively in the left eye. Aphakic vision
was maintained in the right eye 9 months postoperatively. Based on family history andthe lack of antecedent ocular disease, the lens luxations were presumed to be inherited
and veterinarians should be aware of this condition within the captive tree kangaroopopulation.
Key Words: intracapsular lens extraction, lens luxation, marsupial, Matshchie’s treekangaroo, veterinary, zoo
INTRODUCTION
Matshchie’s tree kangaroo (Dendrolagus mastchiei) is anarboreal marsupial native to Papua New Guinea. The spe-cies belongs to the family Macropodidae and is found onlyat high altitudes in the rainforests in the Huon Peninsulaof Papua New Guinea. Matshchie’s tree kangaroo isendangered due to habitat destruction and hunting. Thecaptive population was established from 19 individuals,but only four females contribute to the majority of theoffspring.1 The captive tree kangaroo in this case report isone of the few cycling females in captivity and is, thus, animportant player in the preservation of this species.Because this population is so small and importation ofadditional animals from the wild is restricted, the genepool is limited and there is a significant founder effect.1
With limited genetic diversity, the risk of inherited dis-eases increases and this case report documents bilaterallens luxations in a Matshchie’s tree kangaroo that aresuspected to be hereditary.With the exception of one report of retinal degenera-
tion in a captive Goodfellow’s tree kangaroo (Dendrolagusgoodfellowii) and a description of retinal ganglion celltopography in Doria’s tree kangaroo (Dendrolagus doriana),there are no reports within the veterinary literature detail-ing normal ocular anatomy, pathologic ocular conditions,or the treatment of ocular disease in this species.2,3 We
present a case of bilateral lens luxations and cataracts in acaptive Matshchie’s tree kangaroo that were addressed sur-gically with bilateral intracapsular lens extraction. Becausethe gene pool for this population is small, this problemmay become more prevalent within the captive populationin the United States.
CASE REPORT
A 7-year-old female captive Matschie’s tree kangaroo(Dendrolagus mastchiei) was evaluated because her zoo-keeper and the zoo veterinarian had noted an opacity inthe right eye (OD). The animal could not be handledawake and was immobilized by an intramuscular injectionof a combination of medetomidine (62 mcg/kg; Zoo-Pharm, Laramie, WY, USA), ketamine (3.9 mg/kg; Boeh-ringer-IngelheimVetmedica Inc., St. Joseph, MO, USA),and butorphanol (0.13 mg/kg; Torbugesic, Fort DodgeAnimal Health, Fort Dodge, IA, USA) delivered via aremote delivery system (Telinject 1763 Air Pistol, AguaDulce, CA, USA). The animal was placed in sternalrecumbency for the ophthalmic exam which included dif-fuse illumination (transilluminator), slit-lamp biomicrosco-py (SL-15; Kowa Company, Tokyo, Japan) and indirectfunduscopy (Keeler Vantage Plus; Broomall, PA, USA).The intraocular pressure (IOP) was estimated using appla-nation tonometry (Tono-pen Vet; Reichert Inc., Depew,
© 2014 American College of Veterinary Ophthalmologists
Veterinary Ophthalmology (2015) 18, Supplement 1, 81–85 DOI:10.1111/vop.12207
CASE REPORT
Bilateral lens luxation and intracapsular lens extractionsin a Matshchie’s tree kangaroo
Nancy Johnstone McLean* and Ralph Zimmerman†*VCA Veterinary Care Animal Hospital and Referral Center, 9901 Montgomery Boulevard NE, Albuquerque, NM, 87111, USA;
and †ABQ Biopark, Rio Grande Zoo, 903 Tenth St. SW, Albuquerque, NM, 87102, USA
Address communications to:
N. J. McLean
Tel.: +1 505-296-2982
Fax: +1 866-822-2573
e-mail: nancyjmclean@gmail.
com
AbstractAn adult, female, captive, Matshchie’s tree kangaroo was diagnosed with an anteriorlens luxation in the right eye and a lens subluxation in the left eye. Both eyes were
treated surgically with intracapsular lens extractions. A 360° rhegmatogenous retinaldetachment was diagnosed 6 months postoperatively in the left eye. Aphakic vision
was maintained in the right eye 9 months postoperatively. Based on family history andthe lack of antecedent ocular disease, the lens luxations were presumed to be inherited
and veterinarians should be aware of this condition within the captive tree kangaroopopulation.
Key Words: intracapsular lens extraction, lens luxation, marsupial, Matshchie’s treekangaroo, veterinary, zoo
INTRODUCTION
Matshchie’s tree kangaroo (Dendrolagus mastchiei) is anarboreal marsupial native to Papua New Guinea. The spe-cies belongs to the family Macropodidae and is found onlyat high altitudes in the rainforests in the Huon Peninsulaof Papua New Guinea. Matshchie’s tree kangaroo isendangered due to habitat destruction and hunting. Thecaptive population was established from 19 individuals,but only four females contribute to the majority of theoffspring.1 The captive tree kangaroo in this case report isone of the few cycling females in captivity and is, thus, animportant player in the preservation of this species.Because this population is so small and importation ofadditional animals from the wild is restricted, the genepool is limited and there is a significant founder effect.1
With limited genetic diversity, the risk of inherited dis-eases increases and this case report documents bilaterallens luxations in a Matshchie’s tree kangaroo that aresuspected to be hereditary.
With the exception of one report of retinal degenera-tion in a captive Goodfellow’s tree kangaroo (Dendrolagusgoodfellowii) and a description of retinal ganglion celltopography in Doria’s tree kangaroo (Dendrolagus doriana),there are no reports within the veterinary literature detail-ing normal ocular anatomy, pathologic ocular conditions,or the treatment of ocular disease in this species.2,3 We
present a case of bilateral lens luxations and cataracts in acaptive Matshchie’s tree kangaroo that were addressed sur-gically with bilateral intracapsular lens extraction. Becausethe gene pool for this population is small, this problemmay become more prevalent within the captive populationin the United States.
CASE REPORT
A 7-year-old female captive Matschie’s tree kangaroo(Dendrolagus mastchiei) was evaluated because her zoo-keeper and the zoo veterinarian had noted an opacity inthe right eye (OD). The animal could not be handledawake and was immobilized by an intramuscular injectionof a combination of medetomidine (62 mcg/kg; Zoo-Pharm, Laramie, WY, USA), ketamine (3.9 mg/kg; Boeh-ringer-IngelheimVetmedica Inc., St. Joseph, MO, USA),and butorphanol (0.13 mg/kg; Torbugesic, Fort DodgeAnimal Health, Fort Dodge, IA, USA) delivered via aremote delivery system (Telinject 1763 Air Pistol, AguaDulce, CA, USA). The animal was placed in sternalrecumbency for the ophthalmic exam which included dif-fuse illumination (transilluminator), slit-lamp biomicrosco-py (SL-15; Kowa Company, Tokyo, Japan) and indirectfunduscopy (Keeler Vantage Plus; Broomall, PA, USA).The intraocular pressure (IOP) was estimated using appla-nation tonometry (Tono-pen Vet; Reichert Inc., Depew,
© 2014 American College of Veterinary Ophthalmologists
Veterinary Ophthalmology (2015) 18, Supplement 1, 81–85 DOI:10.1111/vop.12207
LENS LUXATION
QUESTIONS?

1
2

Forthis talkwearegoingtodividethingsintoprimaryandsecondaryglaucomas
3
Ithink abouttheeyeasthekitchensink.
Ifyouturnthetaponandthedrainisworkingproperlythenasmuchwatercomingintothesinkgoesout– hencethesinkdoesnotfill.Ifthereisfoodintheplugholethenthewaterdoesnotdrainasexpectedandthesinkbeginstofill.
ThisishowItrytounderstandtheglaucomas
4

Glaucomaisalways anoutflowproblemandnotanoverproductionofaqueousfluid.
5
Listofbreedspredisposedtoprimaryglaucomas:AkitaAlaskanMalamuteBassetHoundBeagleBorderCollieBostonTerrierBouvier desFlandres BrittanySpanielCairnTerrierCardiganWelshCorgiChihuahuaAmericanCockerSpanielDachshundDalmatianDandie Dinmont TerrierEnglishCockerSpanielEnglishSpringerSpanielGermanShepherdGiantSchnauzerGreyhoundIrishSetterItalianGreyhoundLakelandTerrierMalteseMiniaturePinscherMiniatureSchnauzerNorfolkTerrierNorwegianElkhoundNorwichTerrierPoodle-Toy/MiniatureSamoyedScottishTerrierSealyhamTerrierShihTzuSiberianHuskySkyeTerrier
6

Listofbreedspredisposedtoprimaryglaucomas:AkitaAlaskanMalamuteBassetHoundBeagleBorderCollieBostonTerrierBouvier desFlandres BrittanySpanielCairnTerrierCardiganWelshCorgiChihuahuaAmericanCockerSpanielDachshundDalmatianDandie Dinmont TerrierEnglishCockerSpanielEnglishSpringerSpanielGermanShepherdGiantSchnauzerGreyhoundIrishSetterItalianGreyhoundLakelandTerrierMalteseMiniaturePinscherMiniatureSchnauzerNorfolkTerrierNorwegianElkhoundNorwichTerrierPoodle-Toy/MiniatureSamoyedScottishTerrierSealyhamTerrierShihTzuSiberianHuskySkyeTerrier
6
SmoothFoxTerrierTibetanTerrierWelshSpringerSpanielWelshTerrierWestHighlandWhiteTerrierWireFoxTerrier
6
7

Technicallynotaglaucoma butwilladdithereforcompleteness:Postoperativeocularhypertension(highintraocularpressure afterphacoemulsificaiton)
8

- Physicalexaminationmayuncoversomeothersignsofsystemicdiseasemakingsecondaryglaucomaduetouveitismorelikely
- Lookingattheothereyecanuncoversomeothersignsofuveitishencebilateraluveitis,makingsecondaryglaucomaduetouveitismorelikely
- Gonioscopy ofthe‘normaleye’canrevealabnormalappearanceofpectinateligamentsandpotentiallyshowclosureofthedrainageangle,thismaymakeprimaryglaucomamorelikely
- Ocularultrasoundofanyeyethatyoucannotseeinside(duetomarkeddiffusecornealoedema orhyphema forexample)willhelpwithfindingtheunderlyingdiagnosis(neoplasiaorlensluxationforexample)– don’tforgetmostofthetimeyouhavetheother‘normal’eyetocompareto!
- Ifyouaresuspectinganunderlyingsystemicdiseasethenbloodsandimagingcanbehelpfultoo!
9

Iamavoidofusingtopicalbetablockersiscats,dogs<10kgandpatientswithcardiacorpulmonarydisease.IhavealsohadLurcher /Whippetbreedsthathavebeenmorethan10kgwithseverbradycardiaandsystemichypertensioninICUafteradministrationofCosopt postphacoemulsificaiton.Takecareandmonitorpatentsstartingonbetablockersclosely.
Itendtousetheseasalastresortadditiontoatopicalantihypertensiveprotocolratherthanafirstline.
ItisimportanttorememberthatafteraspikeinIOPtherecanbeinflammationinsidetheeyesoIusesystemicortopicalanti-inflammatoriestoo!
10

IOP Curvesarecarriedoutinthefollowingway:- IOPreadingtakenwithaTonoVet everythreehoursfora30hperiodstartingat9amonthefirstmorning(thisissoaswecangettwomorningreadingsin)
- AprotocolissetforeachpatientwhereiftheIOPisoveracertainparameterthenatopicalmediationshouldbegiven
- IfthisoccursthenIOPisrepeatedonehourlater- IOPcurvesareperformedanywherefrommonthlytosixmonthlydependingoneachpatientandtheresultsofthepreviouscurve
Wehavehadpatientsthathavekepttheirremainingeyefor3yearsafterthefirsteyewasremovedbymonitoringthreemonthlywithIOPcurvesandtopicalmedications.Frequentalterationsoftiming,frequencyandtypeoftopicalantihypertensivehavehelpedthesecases.
11

I generallyliketousetopicalratherthansystemicmedicationstoreduceIOPinprimaryglaucoma’s.IworryabouttreatingwithMannitolorsystemiccarbonicanhydraseinhibitorsduetotheirsystemicsideeffectsandpotentialcomplications.
ItisimportanttorememberthatafteraspikeinIOPtherecanbeinflammationinsidetheeyesoIusesystemicortopicalanti-inflammatoriestoo!
12

Ihaveneveryet performedparacentesis forprimaryglaucoma.Ifthepressureisnotrespondingtolatanoprost andisblindIwouldrecommendenucleation.
Idonotoften offersurgicaltherapiesforprimaryglaucomaduetothereportedsuccessratesbeinglowandthattopicalmedicationsareoftenstillrequired.ThissaidIammindfulthatIprobablydonotoffersurgeryuntilverylateinthediseaseprocessandthatperhapsifIdiditsoonermysuccessratesmaybeimproved.IhavefoundthatwithlasertherecanbealotofinflammationinsidetheeyesaftersurgeryandthereforeaspikeinIOP.AlsowithGonioimplants Ihavefoundthattheyblockwithfibrinandneedsomeinterventions.AllthisaddstothecostandIhavefoundIhavetocouncilclientsbeforeembarkingontheseinterventionstoavoiddisappointment.MaybeIamatoonegative!
P.S.Ihavehadgoodexperienceswithlaserandlensluxationpatients
13

Further investigationsareimportanttohelpyoufindanunderlyingcaseforexampletreatinglymphomawillreducetheIOPbyclearingthedrainageangleofneoplasticcells.Ordiagnosisofanintraocularneoplasiaviaultrasoundwillguideyoumoretowardssurgicalintervention.
14

MannitolandPGanalogues willpotentiallyincreaseIOPincasesofsecondaryglaucomawhenuveitisisaplayer.ThisisbecausethebloodaqueousbarrierisalreadyleakyandthenthelargemannitolmoleculeswilldiffuseinandbringwaterwiththemincreasingIOP.WithPGanaloguestheyarepro-inflammatoryhenceexacerbatingtheincreaseinIOP.
Thatsaid,sometimesyourhandmaybeforcediftherearenootheroptionsandtheeyeispainful.
15

16
17

CO
2 La
ser a
ssis
ted
scle
rect
omy
Joe
Wol
fer D
VM,
Lisa
Bird
RVT
To
ront
o An
imal
Eye
Clin
ic
•C
02 la
ser a
nd th
e IO
Ptim
ate
lase
r aim
ing
syst
em
was
kin
dly
prov
ided
by
Imed
Pha
rma.
•N
o fin
anci
al in
tere
st

•M
y in
tere
st in
tryi
ng to
find
a g
lauc
oma
surg
ery,
that
wor
ked
for m
e, w
as to
try
and
avoi
d an
y m
ore
of th
is…
……
CLA
SS
•C
o2 L
aser
Ass
iste
d Sc
lere
ctom
y Su
rger
y

•A
80-1
00 d
egre
e pe
ritom
y is
cre
ated
at 1
2 o'
cloc
k
•5
x 5
mm
lim
bal b
ased
par
tial t
hick
ness
scl
eral
fla
p
•La
ser a
blat
ion
of s
cler
a at
the
prox
imal
end
of t
he
bed
to fo
rm a
n ar
ea fo
r aqu
eous
hum
our t
o po
ol
•Th
en la
ser a
blat
ion
of th
e sc
lera
dire
ctly
nex
t to
the
limbu
s to
“der
oof”
the
angu
lar a
queo
us
plex
us
•O
nce
aque
ous
hum
our b
egin
s to
per
cola
te o
ut,
lase
r abl
atio
n is
dis
cont
inue
d.
•N
ext,
a 5
x 5
mm
pie
ce o
f Olo
gen
is p
lace
d in
to
the
scle
ral b
ed.
•O
loge
n is
pur
porte
d to
dec
reas
e fib
rosi
s an
d m
aint
ain
a pa
thw
ay fo
r aqu
eous
flow
•Th
e sc
lera
l flap
is lo
osel
y su
ture
d w
ith 2
stit
ches
of
8-0
Vic
ryl a
nd th
e pe
ritom
y is
clo
sed
with
8-0
Vi
cryl
sim
ple
cont
inuo
us


•C
LASS
is a
nov
el, n
on-in
vasi
ve fi
lterin
g pr
oced
ure
to tr
eat e
leva
ted
IOP
in th
e do
g
•Sa
fety
pro
file
is e
xcel
lent
as
ocul
ar p
enet
ratio
n do
es n
ot o
ccur
. U
nles
s in
tend
ed b
y th
e su
rgeo
n (m
ore
abou
t tha
t lat
er)
•In
flam
mat
ion,
a h
allm
ark
of c
yclo
dest
ruct
ive
proc
edur
es, i
s m
inim
al w
ith C
LASS
•Th
e al
ignm
ent l
aser
-aim
ing
beam
, cre
ated
by
IOPt
imat
e, g
reat
ly im
prov
es p
reci
sion
in
reac
hing
the
corre
ct s
cler
al d
epth
to fa
cilit
ate
aque
ous
outfl
ow.
•3-
5 ye
ar re
sults
in h
uman
ele
vate
d IO
P ar
e go
od
with
CLA
SS.
•In
one
stu
dy o
f 111
eye
s, C
ompl
ete
succ
ess
at
36 m
onth
s w
as 4
7.8%
, and
Qua
lified
suc
cess
at
36 m
onth
s w
as 8
4.8%
•In
ano
ther
Hun
garia
n st
udy
of 2
1 ey
es, s
ucce
ss
rate
s w
ere
sim
ilar a
nd a
nti g
lauc
oma
med
icat
ions
dec
reas
ed fr
om a
lmos
t 3 to
2 d
rops
pe
r pat
ient

•J
Gla
ucom
a 20
16 J
ul: 2
5(7)
Gre
ener
et a
l
•Re
sults
of C
LASS
as
com
pare
d w
ith
Con
vent
iona
l Dee
p Sc
lere
ctom
y (N
PDS)
•C
LASS
was
foun
d to
be
just
as
effic
ient
in
low
erin
g IO
P as
NPD
S
•C
LASS
is c
onsi
dere
d to
be
easi
er to
per
form
th
an N
PDS
Resu
lts o
f thi
s st
udy
•10
eye
s, 9
dog
s
•5
FS, 4
MN
•av
erag
e ag
e - 8
.8 y
ears
•av
erag
e fo
llow
up
- 24
days
•Lo
nges
t fol
low
up
- 46
days
•Pr
imar
y gl
auco
ma
= 5
•Se
cond
ary
glau
com
a =
5

•Si
x bl
ind
eyes
- al
l rem
aine
d bl
ind
afte
r sur
gery
•Fo
ur s
ight
ed e
yes
- all
rem
aine
d si
ghte
d af
ter
surg
ery
•In
the
blin
d ey
es, t
here
wer
e 2
failu
res
as IO
P re
mai
ned
elev
ated
. Bo
th o
f the
se e
yes
wer
e en
ucle
ated
•Th
e fir
st e
ye h
ad p
rimar
y gl
auco
ma

•Th
e se
cond
eye
had
a P
IFM
, ret
inal
det
achm
ent
and
retin
osch
isis
.


•Sh
ort t
erm
suc
cess
rate
in lo
wer
ing
IOP
to
norm
al p
aram
eter
s or
mai
ntai
ning
IOP
with
in
norm
al p
aram
eter
s =
80%
•Th
ere
wer
e no
intra
oper
ativ
e or
pos
t-ope
rativ
e co
mpl
icat
ions

•Pa
tient
s w
ere
treat
ed p
ost-o
pera
tivel
y w
ith
topi
cal A
zopt
tid,
Tra
vata
n bi
d, a
nd T
obra
dex
bid.
•O
ral T
ram
adol
was
giv
en fo
r pai
n re
lief.
Con
clus
ion
•C
LASS
is a
n ef
fect
ive
and
safe
trea
tmen
t for
prim
ary
and
seco
ndar
y gl
auco
ma
in th
e ca
nine
, in
the
shor
t te
rm.
•W
e w
ill be
con
tinui
ng th
is s
tudy
by
enro
lling
new
pa
tient
s an
d ho
pe to
pre
sent
one
and
two
year
follo
w
ups
in th
e fu
ture
.
•O
ur n
ext i
nnov
atio
n w
ill be
to im
plan
t a g
old
shun
t int
o th
e sc
lera
l bed
to m
aint
ain
flow
of a
queo
us h
umou
r an
d to
sup
port
the
filtra
tion
bleb
with
cro
ss li
nked
HA

Cav
eat
•M
aint
aini
ng v
entro
med
ial p
ositi
on o
f the
eye
du
ring
gene
ral a
nest
hesi
a, w
hich
is e
ssen
tial f
or
prop
er e
xpos
ure
of th
e 12
o'c
lock
scl
era,
can
be
diffi
cult.
Ane
sthe
tic p
lane
can
cha
nge
durin
g su
rger
y af
fect
ing
eye
posi
tion.
•W
e ha
ve a
ltere
d ou
r pro
toco
l to
a Pr
opof
ol C
RI
and
have
muc
h m
ore
cons
iste
nt p
lane
of
anes
thes
ia n
ow.

NOTES:


BRAVO COMMITTEE MEMBERS 2017
Chairperson – Tim Knott Tim Graduated with an honours degree in Anatomical Science from Bristol University in 1991, followed by his Veterinary degree in 1995. Tim holds the RCVS certificate in Veterinary Ophthalmology and runs Rowe Referrals, Bristol. Hi is interested in all aspects of mixed practice but has special interests in ophthalmology, exotic animal medicine and surgery and fish disease. As chairperson, Tim overseas the running of the committee and chairs our meetings. Soon to be Chairperson – Ida Gilbert (NEW) Ida graduated from Bristol Veterinary School in 1995. Following two years in mixed practice she decided to commit to her interests in ophthalmology and moved to Eastcott Veterinary hospital in Swindon, where she gained her RCVS Certificate in Veterinary Ophthalmology in 2001. She enjoys all areas of Veterinary Ophthalmology and still works and lives in rural Wiltshire. Ida will be taking over the chair role next year when Tim steps down. Joint Secretary – Natasha Mitchell Natasha graduated from University College Dublin in 1998 with a degree in Veterinary Medicine. She obtained the Royal College of Veterinary Surgeons’ (RCVS) Certificate in Veterinary Ophthalmology in 2004. She later joined the Eye Veterinary Clinic in Herefordshire where she completed an alternative residency programme for the RCVS Diploma in Veterinary Ophthalmology, which she obtained in 2011. She is a Veterinary Council of Ireland recognised specialist in Veterinary Ophthalmology. Natasha runs a referral veterinary ophthalmology service, Eye Vet, in Limerick, Ireland. She assists Negar in her very busy role as secretary, enrolling new members and answering general enquiries. Joint Secretary - Negar Hamzianpour (NEW) Negar graduated from the University of Liverpool in 2011. She developed a passion for veterinary ophthalmology during her general internship at the Royal Veterinary College (2012-2013). After several years in general practice (Goddard Veterinary Group), where she completed a post-graduate certificate in small animal ophthalmology, she returned to referral work to undertake an ophthalmology internship at Willows Veterinary Referrals. Negar will undertake an ECVO residency programme at the Eye Veterinary Clinic (Leominster) in the New Year. As secretary, she is involved with the enrolment of new members and answering general enquiries. Hotel and conference organiser – Helen Appelboam Helen qualified from Royal Veterinary College, London in 2001. Originally from Hampshire but keen to see the world, veterinary work has taken her to South Africa and New Zealand where she gained experience in small animal and equine practice. Her interest in ophthalmology grew after seeing practice with specialist veterinary ophthalmologists in these countries. On returning to the UK, she spent 4 years developing her skills in a small animal and eye referral practice in Bristol and studying for the RCVS Veterinary Ophthalmology Certificate, which she achieved in 2011. She joined Optivet Referrals in 2012. Helen’s job is to research the venues for our conferences each year and oversee the running of the conference itself. International liaison – Michael Ziglar Michael completed his Bachelor of Science degree in 1975 at the University of Guelph. He went on to complete his DVM in 1979 at the Ontario Veterinary College, University of Guelph. From 1979 to 1982 he worked as an associate veterinarian in two different Alberta small-animal clinics. He then returned to Ontario in 1982 and opened Bronte Road Animal Hospital in 1984. In 1993 Michael completed examinations and received the RCVS Certificate in Veterinary Ophthalmology. Michael has been involved with both undergraduate teaching and delivering numerous continuing education presentations across North America. He has also been past President of both the American Society of Veterinary Ophthalmology and Canadian Association of Veterinary Ophthalmology where he is also an Honorary Life Member. This new role of international liaison is to try and promote BrAVO abroad and encourage international contacts. Website and audio-visual – David Nutbrown-Hughes After graduating from Bristol in 1995, David had worked in practices in Worcestershire, Somerset and West Sussex where he built on his interest in ophthalmology, gaining the RCVS Certificate in Veterinary Ophthalmology in 2004. Since June 2012 David has joined the ophthalmology team at Rowe Referrals, Bristol. David runs the BrAVO website and is also involved with setting up the audio-visual facilities at each meeting.
TIM KNOTT
IDA GILBERT
NATASHA MITCHELL
NEGAR HAMZIANPOUR
HELEN APPELBOAM
MICHAEL ZIGLAR
DAVID NUTBROWN-HUGHES
CHARLIE BARTON
BRAVO COMMITTEE MEMBERS 2017

Disease surveillance officer – Charlie Barton (NEW) Charlie graduated from Bristol in 2004, and worked in a variety of mixed, and latterly small animal practices. He gained the RCVS Ophthalmology certificate in 2011 and became an advanced practitioner in Veterinary Ophthalmology in 2013. Whilst working in general practice he started a client communications and compliance software company, Virtual Recall, which he now manages full time as it continues to grow internationally. Unfortunately this means that Charlie does not currently have time to see clinical cases, but he still maintains a strong interest in everything Veterinary based, especially Ophthalmology. Outside of this, Charlie enjoys life in Norfolk with his family including 2 kids and a scrappy Lurcher – Dougal; playing tennis, climbing, running and cycling whenever possible (rarely!). This new role will specifically examine the incidence and prevalence of ocular conditions through-out the UK using BrAVO members as a database.
Scientific programme organiser – Rachael Grundon Rachael graduated from Cambridge and spent many years in mixed general practice before specialising in ophthalmology. She undertook her residency in Melbourne gaining the ANZCVS Fellowship in 2014. She is now working at the Eye Vet Clinic in Herefordshire while completing an ECVO residency.
Scientific programme organiser – Chris Dixon (NEW) Chris graduated from the University of Bristol and spent several years working in first opinion mixed practice in the North Yorkshire Moors and Cumbria. During his time at the University of Bristol Chris was lucky enough to be mentored by Professor Sheila Crispin, and this tuition inspired a persistent interest in ophthalmology. Early in his veterinary career, Chris decided to focus on ophthalmology due to the exciting mixture of microsurgery and medicine, and attained the RCVS postgraduate certificate. In 2010 Chris joined fellow ophthalmologist Gary Lewin, and in 2012 they formed Veterinary Vision, a dedicated ophthalmology referral practice based in Penrith, Cumbria. Chris has presented clinical research at national and international veterinary ophthalmology conferences, and has a particular interest in topographical analysis of the cornea and retinal reattachment surgery.
Scientific programme organiser – Christine Heinrich Christine graduated from Munich Veterinary School in 1994 and immediately afterwards moved to the UK, where she undertook both an Internship and a Residency in Ophthalmology at the Animal Health Trust in Newmarket. Since 2000, Christine has been in private ophthalmic referral practice in the UK and she is both a diplomate of the Royal College of Veterinary Surgeons (Ophthalmology) and of the European College of Veterinary Ophthalmologists. In 2015, Christine took over the Eye Veterinary Clinic in Leominster, a dedicated ophthalmic referral clinic for all species. Despite a busy clinical work-load, Christine has continued to enjoy the teaching of Veterinary Ophthalmology both to pre-and post-graduate veterinary surgeons, including lecturing nationally and internationally and the mentoring of residents under the ECVO residency program. Editor – Mike Rhodes Mike graduated from Edinburgh University in 2004 and spent the next three and half years working in small animal practice in Peterborough and Suffolk. During this time he developed a keen interest in veterinary ophthalmology and completed the RCVS Certificate in Veterinary Ophthalmology in 2008. He then undertook a three-year ECVO residency programme at Willows Referral Service and obtained the European Diploma in Veterinary Ophthalmology in 2013. Mike has just started his own peripatetic referral business within the M40 corridor called Focus Referrals Ltd. Mike’s job is to prepare the meeting proceedings as well as to assist Christine, Rachael and Chris in putting together the scientific programme. Clinical Auditor – Jenny Lambert Jenny works at Bath Referrals and obtained the RCVS Certificate in Veterinary Ophthalmology in 2003. As clinical auditor, Jenny aims to create an ongoing cycle of continuous improvement, by collecting data and comparing current practice with evidence of good practice. Soon to be treasurer – Alistair Oldfield (NEW) Having graduated in 1997 from Bristol University, Alistair joined Woodcroft Veterinary Group in June 2002 after working nearly five years at the PDSA clinic in Manchester. Having attained his RCVS Certificate in Veterinary Ophthalmology, Alistair sees referral ophthalmology cases as well as continuing his work in general small animal practice. Alistair is due to take over the role of treasurer when Rob steps down this year.
RACHAEL GRUNDON
CHRIS DIXON
CHRISTINE HEINRICH
MIKE RHODES
JENNY LAMBERT
ALISTAIR OLDFIELD
RACHAEL GRUNDON
CHRIS DIXON
CHRISTINE HEINRICH
MIKE RHODES
JENNY LAMBERT
ALISTAIR OLDFIELD
RACHAEL GRUNDON
CHRIS DIXON
CHRISTINE HEINRICH
MIKE RHODES
JENNY LAMBERT
ALISTAIR OLDFIELD
RACHAEL GRUNDON
CHRIS DIXON
CHRISTINE HEINRICH
MIKE RHODES
JENNY LAMBERT
ALISTAIR OLDFIELD
TIM KNOTT
IDA GILBERT
NATASHA MITCHELL
NEGAR HAMZIANPOUR
HELEN APPELBOAM
MICHAEL ZIGLAR
DAVID NUTBROWN-HUGHES
CHARLIE BARTON

PROGRAMME FRIDAY 3rd NOVEMBER MASTERCLASSES
Friday morning 09.30-12.30 (with flexible 30min comfort/coffee break midway):
1) Pathology (Emma Scurrell)
2) Photography (Tim Knott and Chris Dixon)
3) Anaesthesia (Karen Walsh and Carl Bradbrook)
4) Ocular surgery wet lab (Rob Lowe, Heidi Featherstone, Rachael Grundon)
12.30-13.30 LUNCH, travel between Marriott and Versalius clinical training suite on
Southwell Street Friday afternoon 14.00-17.00 (with flexible 30min comfort/coffee break midway):
1) Pathology (Emma Scurrell)
2) Photography (Tim Knott and Chris Dixon)
3) Anaesthesia (Karen Walsh and Carl Bradbrook)
4) Ocular surgery wet lab (Rob Lowe, Heidi Featherstone, Rachael Grundon)