
Semi‑quantitative analysis cerebrospinal fluid chemistry and cellularity using
40
JOURNAL REVIEW DR. SUMIT KAMBLE SENIOR RESIDENT DEPT. OF NEUROLOGY GMC, KOTA
-
Upload
neurologykota -
Category
Health & Medicine
-
view
393 -
download
0
Transcript of Semi‑quantitative analysis cerebrospinal fluid chemistry and cellularity using
JOURNAL REVIEWDR. SUMIT KAMBLESENIOR RESIDENT
DEPT. OF NEUROLOGY GMC, KOTA
Semi quantitative analysis cerebrospinal fluid ‑chemistry and cellularity using urinary reagent
strip: An aid to rapid diagnosis of meningitis
Neurology India / January 2016 / Volume 64 / Issue 1
• Meningitis is a medical emergency.• Disease is more prevalent in rural areas and in low
socioeconomic groups.• Timely identification and treatment of this condition
is essential to prevent permanent neurological deficits and death.
• Examination of the cerebrospinal fluid (CSF) for leucocytes, glucose, proteins, and culture are the cornerstones in the diagnosis of meningitis.

Materials and Methods
• Prospective study• Period of 4 months from September to December
2014.• All consecutive CSF samples were included in the
study.• Hemorrhagic CSF samples were excluded from the
study• On all the CSF samples collected, both the definitive
test and index test were carried out.
Definitive test-• For leucocytes- total count was carried out by
Neubauer’s counting chamber.• Differential count- cytocentrifuged smears stained
with Leishman stain. • Proteins and sugar- automated analyzer
Index test• Combur 10 urinary reagent strip- can detect 10 ‑
parameters such as specific gravity, pH, leucocytes, nitrate, proteins, glucose, ketone body, urobilinogen, bilirubin, and hemoglobin.
• With the help of a micropipette, 2–3 drops of
undiluted CSF was added to patches of leucocytes, proteins and sugar, and the color changes were recorded.
• Combur reagent strip - detect range of leucocytes from 10 cells/mm3 to 500 cells/mm3
• Detects leucocytes by estimation of peroxidase. • Depending on color changes, leucocytes are graded
as negative for the cell count of <10 cells/cumm, 1+ for 10–75 cells/cumm, 2+ for 75–500 cells/cumm, and 3+ for cells >500 cells/cumm


• Reagent strip detects proteins in the range of 30 mg/dl to 500 mg/dl.
• Observations for CSF proteins include no color ‑(negative) if CSF proteins are <30 mg/dl, 1+ if they are between 30 and 100 mg/dl, 2+ if they are between 100 and 500 mg/dl, and 3+ if they are >500 mg/dl.
• Glucose : No color for a concentration of glucose <50 mg/dl, 1+ for 50–100 mg/dl, 2+ for a count between 100 and 300 mg/dl, 3+ for a count between 300–1000 mg/dl, and 4+ for a count >1000 mg/dl.

Statistical analysis
• Diagnostic accuracy of the reagent strip versus the reference standard was estimated
• Box and whisker plot indicating the distribution of ‑‑ ‑‑reference standard values for each of the visual categories of strip color.‑
• Data were analyzed and graphed using the R statistical software package.

The various cut off levels for index test and reference‑standard used for estimation of diagnostic accuracy
Reagent strip Reference standard
Leukocytes (cells/cumm)0 (no color) <10
1 (any color) ≥10
Protein (mg/dL)
0 (no color) <30
1 (any color) ≥30
2 ≥100
Glucose (mg/dL)
0 (no color) ≤40 and ≤50
1 (any color) >50

Results
• Study included 103 cases dispersed in a wide range of age from 2 days to 75 years, with the maximum number of cases in the age group of 41–50 years.
• Of the 103 cases, 27 (26.2%) were <12 years and 14
cases were <1 year of age. • Male: female ratio being 1.86:1


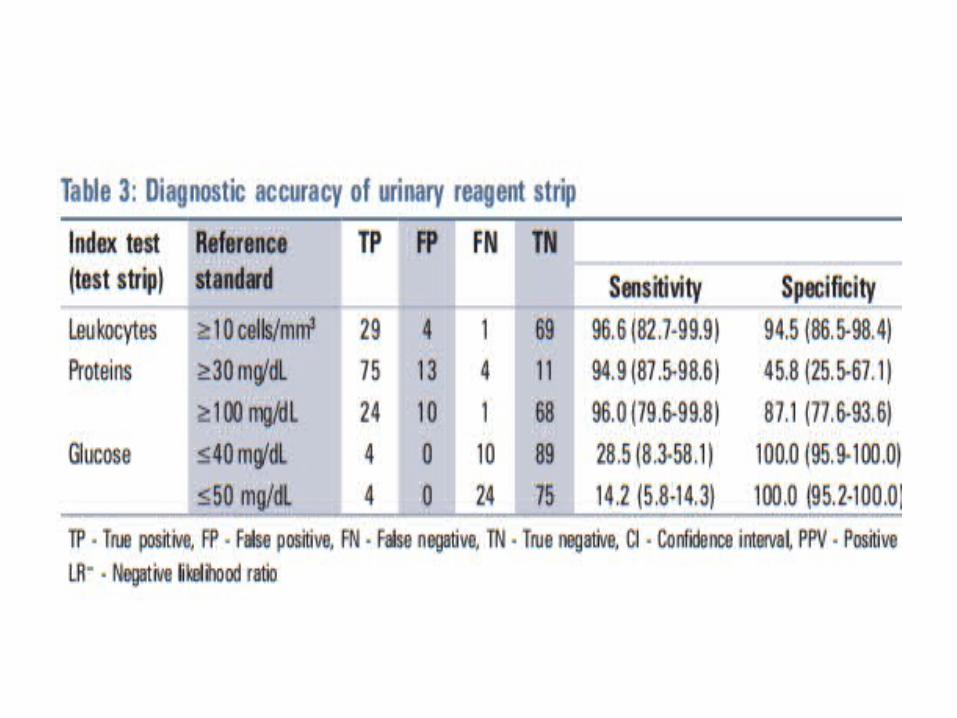

Leucocytes• Sensitivity and specificity for leucocytes by the strip method
for >10 cells/cumm were 96.6% and 94.5% , respectively.
Proteins• Reagent strip had a high sensitivity of 94.9% and a low
specificity of 45.8% for the protein levels ≥30 mg/dl• If the cut off level of the proteins was increased to ≥100 ‑
mg/dl, both sensitivity and specificity were acceptable (sensitivity: 96% and specificity 87.1%).
Glucose• Reagent strip test for glucose at cut off levels of ≤40 mg/dl ‑
and ≤50 mg/dl was highly specific with a specificity of 100% but it was less sensitive

Discussion
• Strip had a high sensitivity and specificity for leucocytes ≥10 cells/cumm.
• With respect to proteins, results are acceptable for a higher cut off level of ≥100mg/dl, where the ‑sensitivity and specificity were 96% and 87.1%, respectively, while at ≥30 mg/dl, the strip was more sensitive and less specific.
• With respect to glucose, strip was highly specific (100%) and less sensitive at both the cut off levels.‑
Joshi et al.2013• CSF samples of 75 patients were included in the study• Of the three tests, diagnostic accuracy of protein estimation
(1 + or more on reagent strip) was best for detection of CSF proteins greater than 30 mg/dL sensitivity 98.1% ; specificity 57.1% . Sensitivity and specificity for 2 + on reagent strip and CSF protein > 100 mg/dL were 92.6% and 87.5% , respectively.
• Leukocyte esterase positivity by test strip had a sensitivity of 85.2 and specificity of 89.6 for detection of CSF granulocytes of more than 10/mm 3

Parmar et al.2004• Sample size-63• Sensitivity, specificity, positive predictive value and the negative predictive
values of the reagent strips for the diagnosis of meningitis were 97.14%, 96.42%, 97.14% and 96.42% respectively.
• Sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of bacterial meningitis were 100%, 96.55%, 92.3% and 100% respectively.
• Sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of tuberculous meningitis were 100%, 96.55%, 92.14% and 100% respectively.
• Sensitivity, specificity, positive predictive value and the negative predictive values of the reagent strips for the diagnosis of aseptic meningitis were 70%, 96.55%, 87.5% and 92.5% respectively
• Moosa et al. using the Combur-9 urine test patches missed 2 of 69 cases of BM but had no false positive results.
• Molyneux, et al., tested the Multistix 10 with similar results.
Maclennan et al.2004 • Tested the usefulness of the nitrate patch for the diagnosis of
bacterial meningitis.• They concluded that nitrate patch, which is also a component of
Combur 10 urinary reagent strip, will become positive in bacterial ‑meningitis.
• Thus, additional information may be obtained without any extra cost.
Limitations• It is useful only if the CSF is clear and is not
applicable in the presence of bloody CSF.• It is designed for urine and not for CSF. The lower
limit of protein and glucose levels vary between urine and CSF.
Conclusion• If this method is used in routine clinical practice, the
rapidity of diagnosis will considerably decrease the morbidity and mortality that occurs due to meningitis.

THANK YOU
• Higher mortality in patients with right hemispheric intracerebral haemorrhage: INTERACT 1 and 2
• Sato S, et al. J Neurol Neurosurg Psychiatry 2015;86:1319–1323

• Objective- elucidate the association of hemispheric lateralisation of lesions with clinical outcomes in approximately 3000 patients with acute ICH, represented by pooling data from the pilot and the main phases of the Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT) studies.
• Aimed to test hypothesis that patients with right-sided ICH would have worse clinical outcomes.

• METHODS• Study design and participants• INTERACT Pilot and INTERACT2 were international,
multicentre, open, blinded end point, randomised controlled trials
• 404 and 2839 patients, respectively, with spontaneous ICH within 6 h of onset and elevated systolic blood pressure (SBP, 150– 220 mm Hg) were randomly assigned to receive intensive (target SBP <140 mm Hg within 1 h) or guideline-recommended (target SBP <180 mm Hg) BP lowering therapy.
• Procedures• Demographic and clinical characteristics were recorded at the
time of enrolment, with stroke severity measured with the Glasgow Coma Scale (GCS) and National Institutes of Health stroke scale (NIHSS) at baseline.
• Laterality was determined on the basis of a baseline scan.• Outcomes of interest in these analyses were death, death or
major disability and major disability (modified Rankin scale (mRS) of 6, 3–6 and 3–5, respectively) at 90 days.
• Primary causes of death were classified into three categories:• (1) Direct effects of initial ICH• (2) Recurrent cardiovascular event• (3) Other causes, defined by clear evidence of death due to a
non-neurological cause, including pneumonia, sepsis or injury.
Statistical analysis
• Considering hemispheric bias in the NIHSS score, only GCS was included as a measure of stroke severity and a sensitivity analysis was conducted including NIHSS.
• Variables were included in the adjusted model if they were either significant in univariable analysis (SBP, GCS score (3 categories of <9, 9–12 and >12)) or prespecified variables determined to be clinically important (age, sex, region, time from onset to randomisation, glucose, baseline haematoma volume, deep (hemispheric) haematoma location, intraventricular extension, trial and randomised treatment).
• Survival probability curves were drawn using Kaplan-Meier analysis and compared using the Cochran Mantel-Haenszel log-rank test

RESULTS
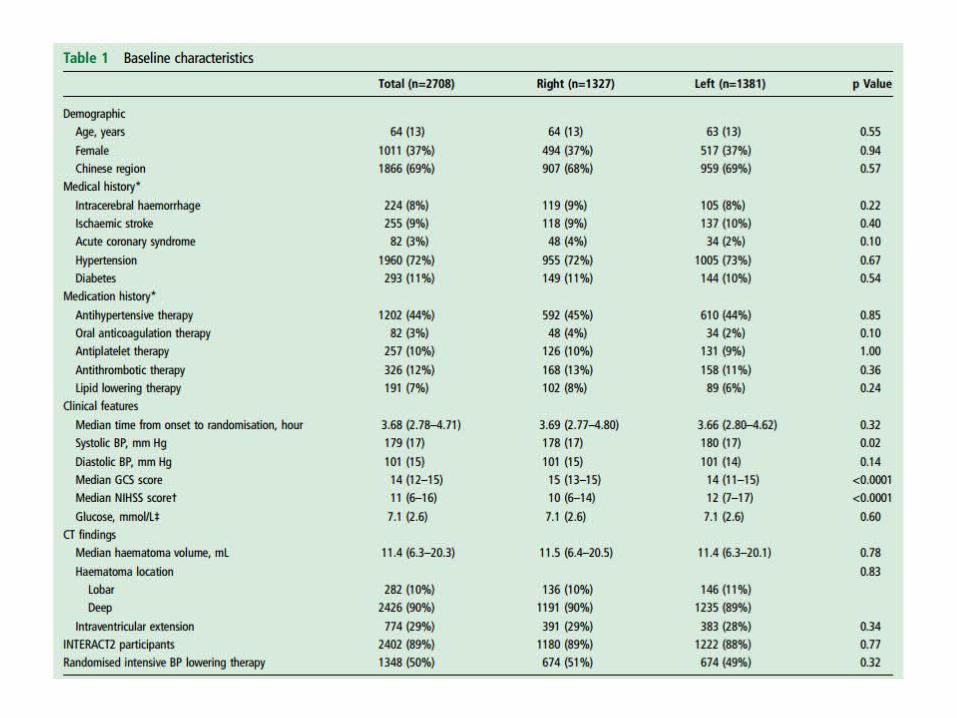
• Baseline characteristics• Among 3233 participants of the combined INTERACT studies,
2708 (84%) patients with deep or lobar ICH and information on mRS available at 90 days were included ;
• Main exclusions were unavailability of the baseline scan (n=274) or non-hemispheric site of ICH (n=204).
• A total of 1327 (49%) patients had right hemispheric ICH;
Right hemispheric ICH and clinical outcomes
• A total of 327 (12%), 1468 (54%) and 1141 (42%) patients had death, death or major disability and major disability at 90 days, respectively.
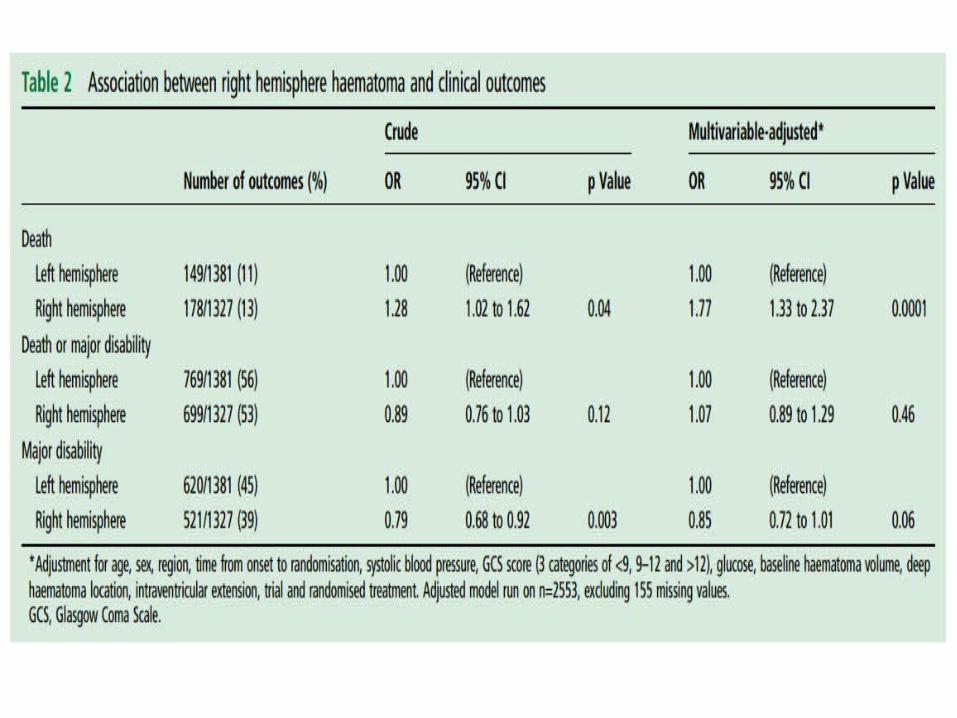
• Patients with right hemispheric ICH had a higher risk of death at 90 days as compared to those with left hemispheric ICH (OR 1.28, 95% CI 1.02 to 1.62).
• This increased risk of death remained statistically significant after multivariable-adjustment (OR 1.77, 95% CI 1.33 to 2.37).
• No clear association was observed for death or major disability.
Sensitivity analysis• There were interactions between NIHSS score and
hemispheric lateralisation of ICH in the adjusted models with death (p=0.004) and with death or major disability (p<0.0001) as the outcomes.
• In the high NIHSS score group, ( ≥11) patients with right ICH had significantly higher risks for death and for death or major disability, as compared to those with left ICH after adjustment for confounders.

Survival analysis• Of patients who died within 90 days of ICH, those with right
hemispheric ICH had a shorter time to death, with a median of 6 days compared to 10 days for those with left hemispheric ICH (p=0.009).
Primary causes of death• Primary causes of death in INTERACT2 participants (n=297).
Patients with right ICH were more likely to die from the direct effects of initial ICH.

• Acute stroke care during the first 7 days
• Patients with right hemispheric ICH were less likely to have been admitted to an intensive care unit, and to have received nasogastric feeding or pulse oximetry.
DISCUSSION• The present pooled analysis of the two INTERACT studies included
over 3000 patients with acute ICH and demonstrated an association of right hemispheric ICH with higher mortality.
• In patients with a high NIHSS score, the right hemispheric ICH was significantly associated with higher risks for death and for death or major disability when compared to those with left hemispheric ICH.
• Patients with right hemispheric ICH were more likely to die from the direct effect of the initial ICH .
• Less likely to receive several components of stroke care within first 7 days
• However, the laterality of the ICH does not appear to affect the level of disability in survivors.
Causes of high mortality in right ICH
• 1.Increased risk of death in patients with right hemispheric stroke is due to the impairment of autonomic cardiovascular control, especially with regard to damage of the right insular cortex (or ‘cardunculus’), which might predispose patients to cardiac arrest from ventricular arrhythmia.
• 2.Another hypothesis is that there is differential stroke management according to hemispheric location, thereby creating a survival difference.
• 3.Another possibility is that patients with right hemispheric ICH had retained capacity for speech and were able to decline treatment, whereas aphasic patients from left hemispheric ICH were more likely to be treated through surrogate consent.

Conclusion• Patients with right hemispheric ICH had higher mortality at 90
days than those with left hemispheric ICH in the INTERACT pooled cohort.
• This was particularly marked in patients with more severe NIHSS scores at presentation.
• Higher mortality in right hemispheric ICH might be avoidable by hemispheric unbiased standardised treatment.


















