
Self-study Module Primary Stroke Center Orders
20
Self-study Module Primary Stroke Center Orders 2009 After reading the module, Complete the post-test on LEO
Transcript of Self-study Module Primary Stroke Center Orders

Self-study Module
Primary Stroke Center Orders
2009
After reading the module, Complete the post-test on LEO

Primary Stroke Center Orders Purpose: The purpose of this module is to provide education and information
related to the primary stroke center orders. The primary stroke center orders consist of three order sets:
Acute ischemic stroke admission orders Intracranial hemorrhage admission orders Subarachnoid hemorrhage admission orders
These are referred to collectively as primary stroke center orders.
Goal: Successfully implement the primary stroke center orders to improve and evaluate patient outcomes based on measures.
Objectives: • Describe the purpose of the Primary Stroke Center orders. • Review the Stroke and TIA guidelines • Delineate the roles and responsibilities of the interdisciplinary team to
implement and evaluate the Primary Stroke Center orders. • Review the Primary Stroke Center orders, Stroke teaching guidelines,
and the trigger (audit) tool. • Identify the Stroke Measures used to evaluate the medical
management and patient care. Instructions: Read the self-study module. You can also find the module on LEO
under Protocols/Order sets – Disease Specific Learning Modules - Stroke • Complete the Stroke Posttest on LEO. This is the only way to
record completion of the module. • To get to the posttest; from LEO
Select Luther Midelfort Academy Select Learning Center (CBT’s, Transcript, Online Registration) Select Online Course Catalog Select LM Eau Claire Posttests Select Stroke Posttest
Questions about the Primary Stroke Center orders, contact members of the Stroke Expert Team:
Felix Chukwudelunzu MD Angie Oldenberg NP Kelly Buchholtz RN
Kerri Crank RN Shannara Faupl RN
Lu Caulkins for measures questions
2
Why has the Stroke routine orders been developed?
• The interdisciplinary Stroke Expert Team developed Stroke orders as part of the process to provide evidence–based care for stroke patients. Successful implementation of these orders will be evaluated using audit tools.
• The Luther Midelfort is certified as a Primary Stroke Center (PSC) by the Joint Commission (JC). The JC will visit us every two years to recertify our PSC designation. It is important you know this information, as a member of the JC survey team will probably approach you to ask questions.
What are included in the Stroke Measures?
• Measures of effective care of patients with stroke include medical management and patient education components:
Thrombolytic Therapy Administered
Patients who present to the hospital with symptoms of an ischemic stroke with symptom onset of 3 hours or less were given t-PA if not contraindicated.
Screened for Dysphagia
Patients screened for dysphagia before being given food, fluids, or medications by mouth.
DVT Prophylaxis
Patients with an ischemic stroke and who are non-ambulatory that received DVT prophylaxis by end of day two.
Discharged on Cholesterol Reducing Medication
Patients with ischemic stroke and elevated LDL cholesterol were prescribed cholesterol reducing medication.
Smoking Cessation Advice/Counseling
Stroke patients who smoke received smoking cessation advice or counseling during their hospitalization.
Patients with Atrial Fibrillation Receiving Anticoagulation Therapy
Patients with an ischemic stroke with atrial fibrillation discharged on anticoagulation therapy unless it is contraindicated.
3
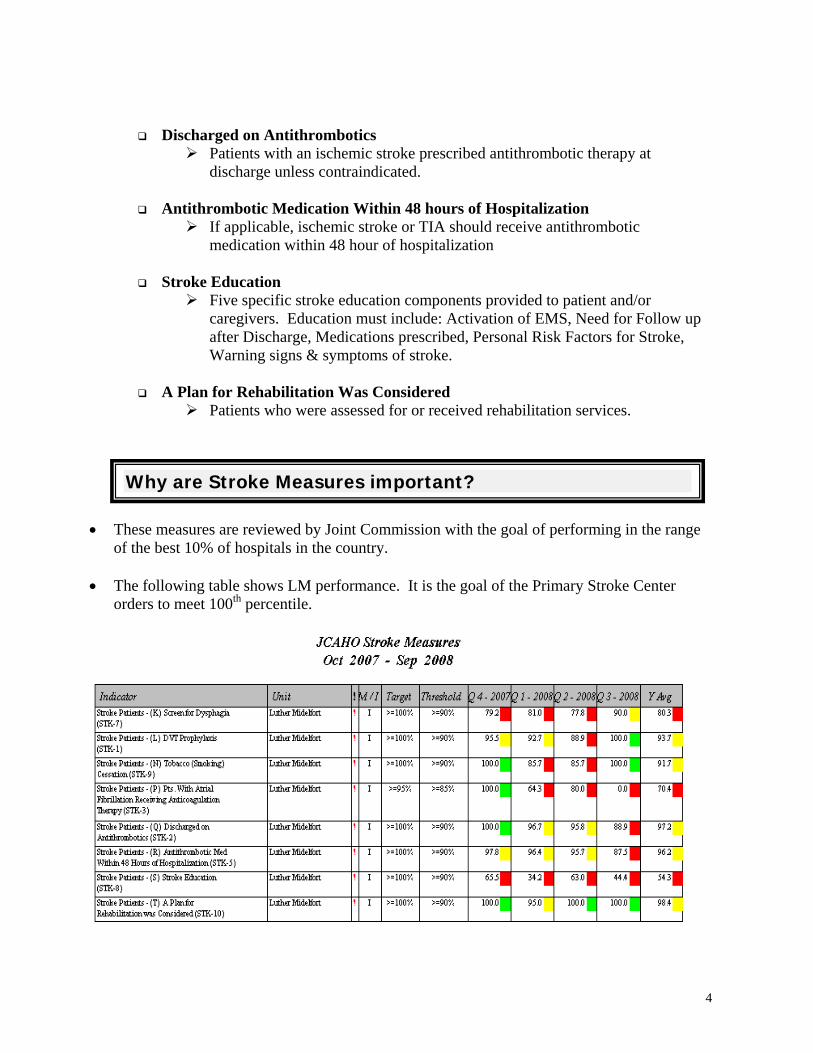
Discharged on Antithrombotics Patients with an ischemic stroke prescribed antithrombotic therapy at
discharge unless contraindicated.
Antithrombotic Medication Within 48 hours of Hospitalization If applicable, ischemic stroke or TIA should receive antithrombotic
medication within 48 hour of hospitalization
Stroke Education Five specific stroke education components provided to patient and/or
caregivers. Education must include: Activation of EMS, Need for Follow up after Discharge, Medications prescribed, Personal Risk Factors for Stroke, Warning signs & symptoms of stroke.
A Plan for Rehabilitation Was Considered
Patients who were assessed for or received rehabilitation services.
Why are Stroke Measures important?
• These measures are reviewed by Joint Commission with the goal of performing in the range of the best 10% of hospitals in the country.
• The following table shows LM performance. It is the goal of the Primary Stroke Center
orders to meet 100th percentile.
4

How does the Primary Stroke Center orders process help improve measures?
The Primary Stroke Center orders guide the physician in ordering medications, diagnostic workup, preventive therapy and consultations appropriate for the patient’s condition, based on current evidence-based, best practice guidelines. • These orders reflect the recommendations from the American Stroke Association’s task force
on the development of stroke systems. • Historically, rates for screening for dysphasia, obtaining a lipid profile, preventative therapy,
and organized teaching of stroke patients and their families have been low. • Implementing the Primary Stroke Center orders should improve the documentation that is
needed to evaluate the measures.
Who will be placed on the Primary Stroke Center orders?
• Any patient that is admitted with Stroke or is later diagnosed with Stroke must be placed on the Primary Stroke Center orders.
5

Stroke Guidelines Target Population: All patients ≥ 18 years-old presenting with neurological symptoms suggestive of:
Spontaneous Intracerebral Hemorrhage (ICH)
Revised: 7/05; Reviewed: 03/07 Source: http://stroke.ahajournal.org/cgi/content/full/30/4/905 Reviewed: 05/08
Airway and Oxygenation: Airway protection and adequate ventilation are critical. Intubation should be guided by imminent respiratory insufficiency. Consider intubation if pO2 < 60 mm Hg or pCO2 > 50 mm Hg or obvious risk of aspiration exist with or without impairment of arterial oxygenation.
Imaging Studies: Initial imaging modality of choice is non-contrast head CT scan. After rapid identification of the lesion, MRI and/or MRA or CTA may be obtained at the discretion of the physician for further assessment and management. 4-vessel cerebral angiography may be indicated in some patients.
Hypertension: Blood pressure should be maintained below a mean arterial pressure (MAP) of 130 mm Hg [MAP = 2(DP) + SBP/3]. In patients with elevated intracranial pressure (ICP) who have ICP monitor, cerebral perfusion pressure (MAP-ICP) should be kept > 70 mm Hg.
Stroke/Audit Forms: ICH admission order form should be used and stroke audit forms completed for all patients.
Fluid Management: Goal of fluid management should be euvolemia. When indicated central venous pressure (CVP) should be maintained between 5 and 12 mm Hg or pulmonary wedge pressure at 10 to 14 mm Hg.
DVT Prophylaxis: DVT prophylaxis using pneumatic compression devices should be instituted for bedridden patients with hemiplegia within 24 hours of presentation.
Other Medical Management Issues: Body temperature: Should be maintained at normal level. Acetaminophen or cooling blanket should be used to treat hyperthermia > 38.5 C (>100.4 F) Agitation: For management of prolonged agitation unresponsive to non-pharmacologic intervention, prudent use of minor tranquilizers is recommended. Short acting benzodiazepines or propofol are preferred.
Ischemic Stroke Imaging Studies: All stroke patients should have a head CT scan completed within 45 minutes of presentation to the ED. Brain MRI may be substituted for CT scan at the discretion of the physician, but should not delay any appropriate acute intervention such as thrombolysis.
Thrombolysis. Intravenous thrombolysis (IV-tPa): Should be administered to all eligible patients within 3 hours of onset of symptoms and within 60 minutes of arrival to ED. Document rationale for not using thrombolysis in all patients that present within the time window. Intra-arterial thrombolysis (IA-tPa) or Mechanical clot removal therapy: Should be considered for eligible patients who are otherwise ineligible for IV-tPa, presenting within 3-6 hours of onset of symptoms attributable to middle cerebral artery occlusion or up to 12 hours for vertebrobasilar artery occlusion.
Stroke Order/Audit Forms: Should be used for all stroke patients
Hypertension: Blood pressure ≤ 220/120 should not be treated for the first 24 hours unless there are other medical indications to be determined by the treating physician.
Anti-platelet therapy: 50-325 mg of aspirin should be administered to all stroke patients within 48hrs of presentation unless there is absolute contraindication to aspirin therapy.
Nutrition and hydration: Assessment of patients baseline nutritional status and need for hydration and institution of appropriate measures for correction should be done within 48 hours of presentation.
DVT Prophylaxis: Should be instituted within 24 hours in all stroke patients confined to bed rest and/or with paralysis/ataxia that impairs ambulatory activity.
Education: Education regarding stroke symptoms, diagnostic procedures, treatment options, prognosis and risk factors should be offered to patients and family and documented in the patient’s chart.

TIA Guideline Target population: All patients ≥ 18 years old. Definition: A focal neurological deficit localizable to a defined cerebral vascular
territory lasting < 24 hours. Specific to this guideline, patients with persistent symptoms at the conclusion of ED evaluation (even if the total time of symptoms is < 24 hours) should be treated as a Stroke. Assessment: The ED provider should:
•Assess stroke risk factors, counsel, and initiate follow-up appointment with primary Doctor or Neurologist if admission to hospital is not indicated.
•Perform “ABCD or ABCD2” assessment and follow the TIA Algorithm for appropriate triaging.
•Discuss case with the Neurologist-on-call
•Obtain appropriate laboratory/Radiological tests to include but not limited to Electrolytes, CBC, PT/PTT, Non-contrast Head CT and Carotid Duplex Ultrasound when indicated (if CUS not done within the previous 6 months).
Treatment: Give Aspirin (50-325mg) in the ED, and discharge home on aspirin if no contraindication and if not previously on Aspirin. Education: Educate patients about their risk factors and warning symptoms of stroke. Initial Draft: F. Chukwudelunzu/Stroke Expert Team; 6/06 Based on: AHA/ASA Guidelines: Stroke. 2006;37:577 Rothwell , PM and Johnston, SC; Stroke. 2006;37(2):320 Reviewed: 03/07; 05/08
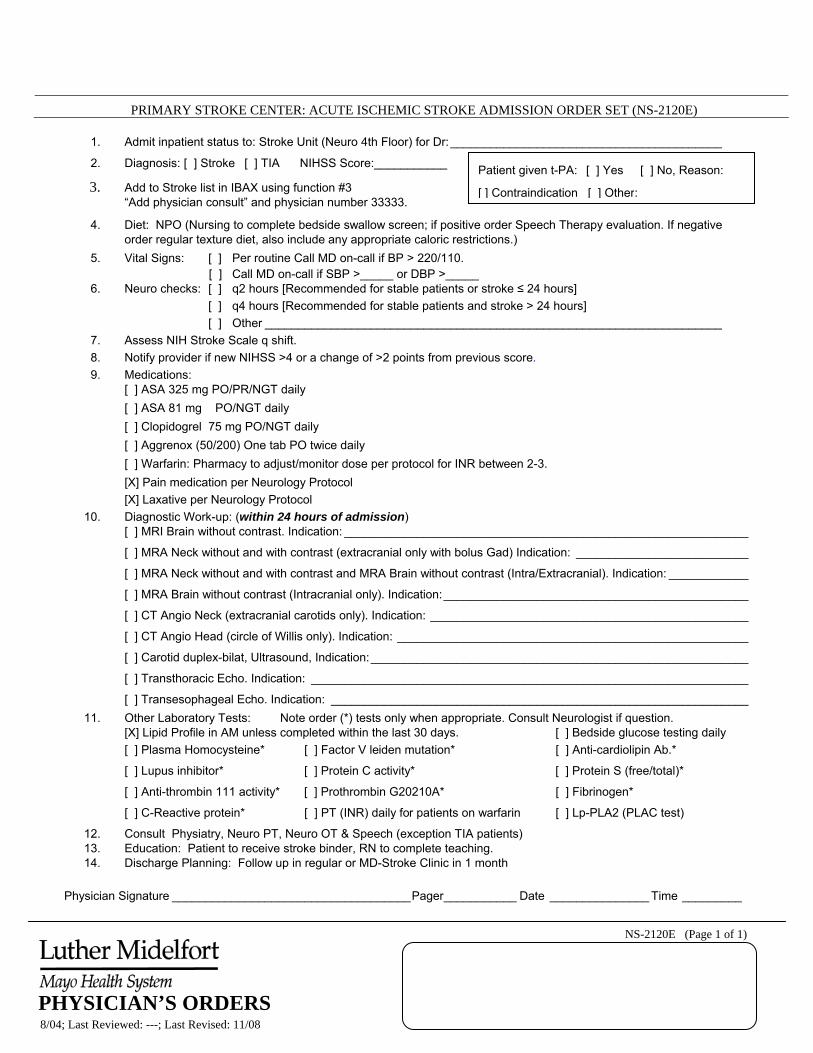
PRIMARY STROKE CENTER: ACUTE ISCHEMIC STROKE ADMISSION ORDER SET (NS-2120E)
NS-2120E (Page 1 of 1)
8/04; Last Reviewed: ---; Last Revised: 11/08
1. Admit inpatient status to: Stroke Unit (Neuro 4th Floor) for Dr:_________________________________________
Patient given t-PA: [ ] Yes [ ] No, Reason:
[ ] Contraindication [ ] Other:
2. Diagnosis: [ ] Stroke [ ] TIA NIHSS Score:___________
3. Add to Stroke list in IBAX using function #3 “Add physician consult” and physician number 33333.
4. Diet: NPO (Nursing to complete bedside swallow screen; if positive order Speech Therapy evaluation. If negative order regular texture diet, also include any appropriate caloric restrictions.)
5. Vital Signs: [ ] Per routine Call MD on-call if BP > 220/110. [ ] Call MD on-call if SBP >_____ or DBP >_____
6. Neuro checks: [ ] q2 hours [Recommended for stable patients or stroke ≤ 24 hours] [ ] q4 hours [Recommended for stable patients and stroke > 24 hours] [ ] Other _____________________________________________________________________
7. Assess NIH Stroke Scale q shift. 8. Notify provider if new NIHSS >4 or a change of >2 points from previous score. 9. Medications:
[ ] ASA 325 mg PO/PR/NGT daily [ ] ASA 81 mg PO/NGT daily [ ] Clopidogrel 75 mg PO/NGT daily [ ] Aggrenox (50/200) One tab PO twice daily [ ] Warfarin: Pharmacy to adjust/monitor dose per protocol for INR between 2-3. [X] Pain medication per Neurology Protocol [X] Laxative per Neurology Protocol
10. Diagnostic Work-up: (within 24 hours of admission) [ ] MRI Brain without contrast. Indication: _____________________________________________________________
[ ] MRA Neck without and with contrast (extracranial only with bolus Gad) Indication: __________________________
[ ] MRA Neck without and with contrast and MRA Brain without contrast (Intra/Extracranial). Indication: ____________
[ ] MRA Brain without contrast (Intracranial only). Indication:______________________________________________
[ ] CT Angio Neck (extracranial carotids only). Indication: ________________________________________________
[ ] CT Angio Head (circle of Willis only). Indication: _____________________________________________________
[ ] Carotid duplex-bilat, Ultrasound, Indication:_________________________________________________________
[ ] Transthoracic Echo. Indication: __________________________________________________________________
[ ] Transesophageal Echo. Indication: _______________________________________________________________ 11. Other Laboratory Tests: Note order (*) tests only when appropriate. Consult Neurologist if question.
[X] Lipid Profile in AM unless completed within the last 30 days. [ ] Bedside glucose testing daily [ ] Plasma Homocysteine* [ ] Factor V leiden mutation* [ ] Anti-cardiolipin Ab.*
[ ] Lupus inhibitor* [ ] Protein C activity* [ ] Protein S (free/total)*
[ ] Anti-thrombin 111 activity* [ ] Prothrombin G20210A* [ ] Fibrinogen*
[ ] C-Reactive protein* [ ] PT (INR) daily for patients on warfarin [ ] Lp-PLA2 (PLAC test)
12. Consult Physiatry, Neuro PT, Neuro OT & Speech (exception TIA patients) 13. Education: Patient to receive stroke binder, RN to complete teaching. 14. Discharge Planning: Follow up in regular or MD-Stroke Clinic in 1 month
Physician Signature ____________________________________Pager___________ Date _______________ Time _________
PHYSICIAN’S ORDERS

PRIMARY STROKE CENTER: INTRACRANIAL HEMORRHAGE ADMISSION ORDER SET (NS-2120F)
NS-2120F (Page 1 of 1)
8/04; Last Reviewed: ---; Last Revised: 11/08
1. Admit inpatient status to: [ ] Critical Care Unit [ ] Other__________ for Dr: ____________________________
2. Diagnosis: Intracerebral Hemorrhage (ICH)
3. Add to Stroke list in IBAX using function #3 “Add physician consult” and physician number 33333.
4. Diet: NPO (Nursing to complete bedside swallow screen; if positive order speech therapy evaluation. If negative order regular texture diet, also include any appropriate caloric restrictions.)
5. Vital Signs and Neuro Checks: [ ] every 1 hour [ ] every 2 hours [ ] every 4 hours [ ] Other ______________________________________________________
6. Assess NIH Stroke Scale q shift.
7. Notify provider if new NIHSS >4 or a change of >2 points from previous score.
8. Medications:
[ ] Labetalol 20 mg IVP over 2 minutes q 30 minutes for MAP > 130 (Max. 300 mg/24 hours)
[ ] Nicardipine 5mg/hr IV infusion. Titrate to target BP (MAP<130) by increasing 2.5mg/hr every 5 minutes,
maximum dose of 15mg/hr
[ ] Nitropruside infusion start at 0.5 mcg/kg/min then titrate to target BP (MAP <130). Maximum of 10 mcg/kg/min.
[X] Pain medication per Neurology Protocol
[X] Laxative per Neurology Protocol
[ ] Other: __________________________________________________________________________________
9. Diagnostic Work-up: (within 24 hours of admission)
[ ] MRI Brain with contrast. Indication: ___________________________________________________________
[ ] MRI Brain without contrast. Indication: _________________________________________________________
[ ] MRI Brain without contrast (with GRE sequence). Indication: _______________________________________
[ ] Urine drug screen
[ ] Serum drug screen
[ ] Other: __________________________________________________________________________________
10. Notify UW-OPO of patients meeting Clinical triggers.
11. Education: Patient to receive stroke binder, RN to complete teaching.
12. Discharge Planning: Follow up in regular or MD-Stroke Clinic in 1 month
Physician Signature ____________________________________Pager___________ Date _______________ Time _________
PHYSICIAN’S ORDERS
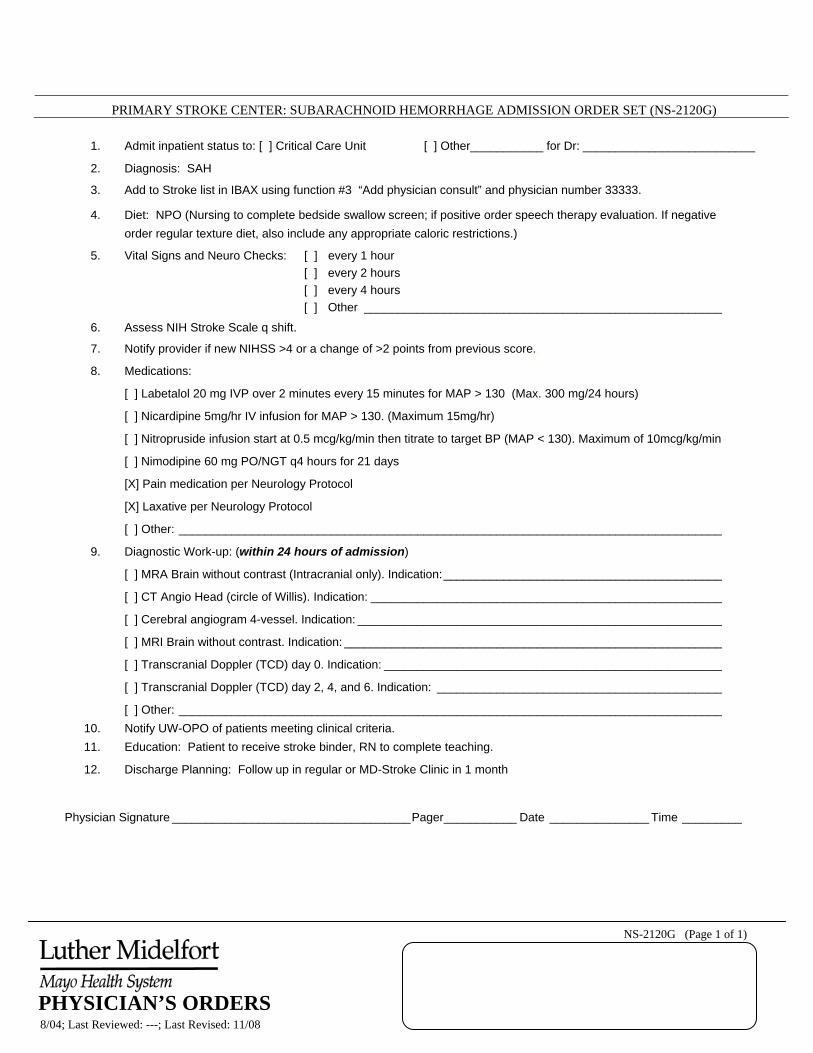
PRIMARY STROKE CENTER: SUBARACHNOID HEMORRHAGE ADMISSION ORDER SET (NS-2120G)
NS-2120G (Page 1 of 1)
8/04; Last Reviewed: ---; Last Revised: 11/08
1. Admit inpatient status to: [ ] Critical Care Unit [ ] Other___________ for Dr: __________________________
2. Diagnosis: SAH
3. Add to Stroke list in IBAX using function #3 “Add physician consult” and physician number 33333.
4. Diet: NPO (Nursing to complete bedside swallow screen; if positive order speech therapy evaluation. If negative order regular texture diet, also include any appropriate caloric restrictions.)
5. Vital Signs and Neuro Checks: [ ] every 1 hour [ ] every 2 hours [ ] every 4 hours [ ] Other ______________________________________________________
6. Assess NIH Stroke Scale q shift.
7. Notify provider if new NIHSS >4 or a change of >2 points from previous score.
8. Medications:
[ ] Labetalol 20 mg IVP over 2 minutes every 15 minutes for MAP > 130 (Max. 300 mg/24 hours)
[ ] Nicardipine 5mg/hr IV infusion for MAP > 130. (Maximum 15mg/hr)
[ ] Nitropruside infusion start at 0.5 mcg/kg/min then titrate to target BP (MAP < 130). Maximum of 10mcg/kg/min
[ ] Nimodipine 60 mg PO/NGT q4 hours for 21 days
[X] Pain medication per Neurology Protocol
[X] Laxative per Neurology Protocol
[ ] Other: __________________________________________________________________________________
9. Diagnostic Work-up: (within 24 hours of admission)
[ ] MRA Brain without contrast (Intracranial only). Indication:__________________________________________
[ ] CT Angio Head (circle of Willis). Indication: _____________________________________________________
[ ] Cerebral angiogram 4-vessel. Indication: _______________________________________________________
[ ] MRI Brain without contrast. Indication: _________________________________________________________
[ ] Transcranial Doppler (TCD) day 0. Indication: ___________________________________________________
[ ] Transcranial Doppler (TCD) day 2, 4, and 6. Indication: ___________________________________________
[ ] Other: __________________________________________________________________________________ 10. Notify UW-OPO of patients meeting clinical criteria. 11. Education: Patient to receive stroke binder, RN to complete teaching.
12. Discharge Planning: Follow up in regular or MD-Stroke Clinic in 1 month
Physician Signature ____________________________________Pager___________ Date _______________ Time _________
PHYSICIAN’S ORDERS

Stroke Orders – Questions & Answers
Question: How is Ischemic Stroke, ICH, and TIA determined? Answer: The physician will determine Ischemic Stroke versus ICH (Intracranial Hemorrhage) versus TIA (Transient Ischemic Attack) based on the clinical presentation of the patient and diagnostic work-up. The physician will choose the appropriate order-set based on his/her assessment. Question: Why is it important to IMMEDIATELY report stroke symptoms to the physician? Answer: The physician will consider ordering t-PA (if the patient meets the strictly defined criteria). For t-PA to be of benefit, it must be administered within 3 hours of the onset of stroke symptoms. Question: What is a Acute Stroke Team and how is it different from Stroke Expert Team Answer: Luther Midelfort Acute Stroke team is made up Neurologists and ER physicians. They are responsible for acute management of patients with Stroke 24-7 by providing direct clinical care. The members of the acute Stroke Team are represented in the Stroke Expert Team. Question: What is a Stroke Expert Team? Answer: It is a group of providers and staff that oversees the process of stroke care and evaluates the measures for the entire Luther Midelfort system. This includes neurologists, nurses from inpatient and outpatient settings, primary care physicians, therapists, and regional site representation. Question: What are the recommendations of the committee to improve these measures? Answer: Some recommendations are to:
1. Never delay reporting of stroke symptoms to the physician. Make it a priority.. 2. Remind physicians to use the stroke orders sets for ALL stroke patients. 3. Learn more about stroke and educate staff. 4. Implement NIHSS for MDs and Neuro RNs..
Question: What is a Primary Stroke Center? Answer: A designation by Joint Commission or other certifying body signifying a hospitals capability of treating stroke patients to the highest standard available. Question: Why do the routine orders include a lipid profile during hospitalization? Answer: This is important because an elevated cholesterol level is a risk factor for coronary heart disease and stroke. If discovered, should be treated aggressively.
- 7 -

Question: Why do the stroke routine orders include orders for tobacco cessation? Answer: The Framingham Heart Study concluded that smoking made a significant independent contribution to the risk of stroke. Hospitalization can be an ideal opportunity for a patient to stop smoking and smoking cessation may promote the patient’s medical recovery. Patient’s who receive even brief smoking cessation advice are more likely to quit than those who receive no counseling at all. In addition, rates for smoking cessation counseling are monitored by Joint Commission for several diseases including stroke. Luther Hospital’s performance in providing smoking cessation counseling is available to the public (http://www.wicheckpoint.org/).
Why is patient/family education so important? • Patient/family education is key to preventing future stroke or disability. • Each discipline is responsible for documenting the appropriate education on the EMR
Education Power Form. • On the EMR Education Power Form, indicate under the comments under the Teaching
Method section when written materials such as the Tobacco Free Folder and Stroke binder are given and reviewed with the patient/family. Order Stroke 3-ring binders from Central Supply.
• Essential patient education objectives related to stroke are covered in the teaching guidelines to ensure the key points are reviewed and evaluated with the patient and family.
RN Guidelines for Stroke Education
1. Give Pt and/or Family stroke binder 2. Educate pt/family on all the tabs in the binder 3. Document the following in EMR:
a. Ad Hoc b. Pt. Education tab c. Education Stroke tab- check all that apply d. Document these 5 specific components:
1. Personal Risk Factors for Stroke 2. Medications Prescribed 3. Warning Signs and Symptoms of Stroke 4. Activation of EMS if experiencing signs and symptoms of stroke 5. Need for follow-up after discharge
These are JCHAO requirements and needs to be documented in order to keep our Primary Stroke Center Certification. If you need to review the Tobacco Cessation Learning Module or Stroke binder, you can review that information which is located on LEO – Protocols/Order Sets – Disease Specific Learning Modules.
- 8 -
What is the Luther Midelfort Stroke Clinic?
The Luther Midelfort Stroke Clinic is located in the Neuroscience Department on the 5th floor of Luther Hospital. The Luther Midelfort Stroke Clinic provides individualized answers to patient and family concerns and questions regarding stroke. It offers a focused exam and consultation for patients who have already had a stroke or are at risk of having a stroke. In addition to serving as an information resource, the Stroke Clinic works with patients and families to prevent stroke by identifying and controlling risk factors. Patients who may benefit from the Stroke Clinic include:
• Those who received treatment for a stroke and have been discharged from the hospital
• Those at risk for a stroke, such people with asymptomatic carotid disease. During a visit to the Stroke Clinic, Dr Felix Chukwudelunzu evaluates the patient, and the plan of care. Nurses and therapists in the clinic complete follow-up therapy and treatment. The patient’s primary care physician is included in the treatment plan and recommendations to ensure continuity of care. For information or questions or to make an appointment, call 8-1900.
What is the Stroke Zones for Management Action Plan?
This document is a visual tool given to patients to direct them as to what actions to take if they are experiencing any stroke warning signs. It is based on a stoplight – green means you are doing OK (go), Yellow means take some caution/action, Red means danger, get help fast. The Stroke Zones for Management is a generic action plan, and used to provide a general guideline to the patient/family. The next page is a sample of this form, found in the Stroke binder.
- 9 -

Stroke Zones for Management Action Plan
GREEN ZONE: All Clear
IF: NO new or worsening:
o Weakness or numbness on one side of your body.
o Trouble swallowing, speaking or changes in vision.
o Loss of balance or dizziness. o Severe headaches, especially headache with
vomiting. • NO trouble taking your medicines. • NO blood in your urine or stool if you are taking
coumadin/warfarin.
THEN: • Your symptoms are under control. • Continue taking your medications as directed. • Keep all appointments.
YELLOW ZONE: Caution Work closely with your healthcare team if you are going into the yellow zone.
IF: You develop mood swings or depression. • Develop new or worsening pain. • Develop tiredness or sleepiness. • Have questions or concerns about your
medications or stroke.
THEN: Call your neurologist or primary care provider. Name_______________________ Number _____________________
RED ZONE: Danger Call your healthcare team if you are going into the red zone.
IF: • New or Worsening:
o Weakness or numbness on one side of your body.
o Trouble swallowing, speaking or changes in vision.
o Loss of balance or dizziness. o Severe headaches, especially headache with
vomiting. o Find blood in your urine or stool if you are
taking coumadin/warfarin
THEN…… • Call 911 immediately!
Form #5071 05/06

Audit Tools
There are three audit tools that will be used at Luther Hospital.
1. One is for the Emergency Department only – a pink form titled Acute Stroke Treatment Outcome and Continuous Improvement Data Collection Form.
2. Another is for all other Luther Hospital Departments – titled Stroke Trigger Tool. 3. Another is the RN Worksheet for Patients with Stroke for all RNs caring for stroke
patients. Use the form appropriate for your department. • The 33333 IBAX inquiry list will be pulled from IBAX. • The patient’s primary RN will be responsible to audit for completion of the core measure
items and documentation. The Stroke Trigger Tool was developed as an effort to increase our compliance concerning the Joint Commission measures. The Board of Directors has identified achievement of 100% compliance with these measures as a key organizational objective.
Refer to the Stroke Trigger Tool & Acute Stroke Treatment Collection Form on the next 2 pages. Stroke Trigger tool – to be used by all departments except Emergency Dept.
• The Stroke Trigger Tool is part of the Stroke Admission order packet. • The Trigger Tool is to be placed in the clear plastic holder on the computer pull down
with a patient sticker on the back of the form. • Follow the Stroke order set and complete the trigger tool throughout the patient’s hospital
stay. • For those triggers that have not been met and are time sensitive place a √ mark in the red
column indicating it was not completed within the time frame (a √ in the red column will never turn green if it is time sensitive).
• When completing patient education, remember to document education under the Stroke Education tab.
• When a standard has been met, place your initials and department in the green column. • When a patient is transferred, the trigger tool is to be transferred with the patient for
continued completion. • Prior to discharge, the trigger tool should be reviewed and completed. When the patient
is discharged, the trigger tool should be returned to the department director. Emergency Department: use the Acute Stroke Treatment Outcome and Continuous Improvement Data Collection Form. • Is part of the Emergency Department Stroke Admission packet. • Indicators on the data collection form have been changed to include only “Date and time of
onset of stroke symptoms”, “Time Neurologist notified” and “Time Neurologist arrived”. • Upon discharge from the Emergency Department, the data collection form should be
reviewed and completed. When the patient is discharged, return to Shannara Faupl RN, Neuro 4th Floor LH.
10
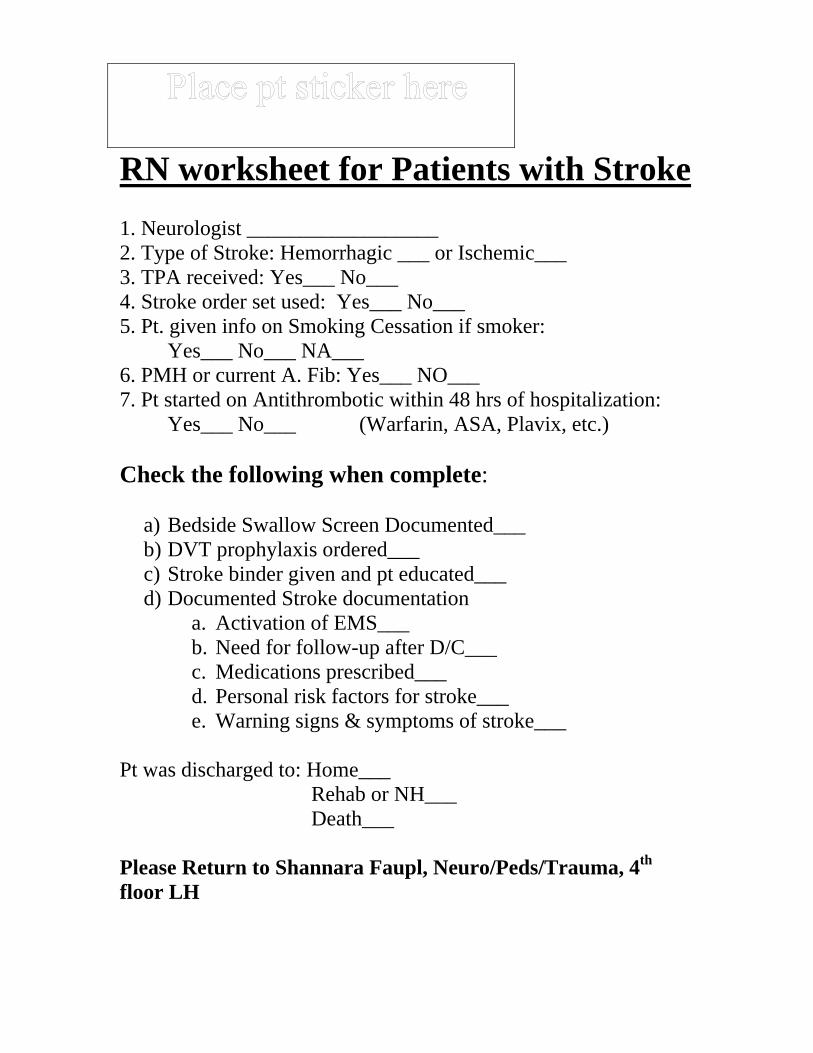
RN worksheet for Patients with Stroke 1. Neurologist __________________ 2. Type of Stroke: Hemorrhagic ___ or Ischemic___ 3. TPA received: Yes___ No___ 4. Stroke order set used: Yes___ No___ 5. Pt. given info on Smoking Cessation if smoker: Yes___ No___ NA___ 6. PMH or current A. Fib: Yes___ NO___ 7. Pt started on Antithrombotic within 48 hrs of hospitalization: Yes___ No___ (Warfarin, ASA, Plavix, etc.) Check the following when complete:
a) Bedside Swallow Screen Documented___ b) DVT prophylaxis ordered___ c) Stroke binder given and pt educated___ d) Documented Stroke documentation
a. Activation of EMS___ b. Need for follow-up after D/C___ c. Medications prescribed___ d. Personal risk factors for stroke___ e. Warning signs & symptoms of stroke___
Pt was discharged to: Home___ Rehab or NH___ Death___ Please Return to Shannara Faupl, Neuro/Peds/Trauma, 4th floor LH

Patient Sticker goes on the BACK of this form Stroke Trigger Tool
This is not part of the permanent record
Standard
Red (standard not met)
N/A
Green (initial when
standard met)
1. Bedside swallow screen by RN documented in clinical notes-Bedside swallow screen, before pt. has anything po.
2. DVT Prophylaxis ordered
3. Patient and/or family was given a Stroke Binder, it was reviewed and it was so documented under the Stroke Education Tab in EMR, as follows:
3a. a. Stroke binder given to pt
3b. b. Personal Risk Factors for stroke (“Risk Factors” tab) c. Warning signs and symptoms for stroke
3c. d. Medications Prescribed (“Medications” tab and Discharge medications)
3d. Discharge Instructions: (“Discharge” tab) e. Activation of EMS if experiencing signs and symptoms of stroke f. Importance of follow-up visits
Comments: **1. Click on ad hoc 2. Pt. Education tab 3. Education Stroke & check those that apply
~Document the following: a) Stroke binder given b) Risk factors c) Medications Prescribed d) Signs and symptoms e) Activating EMS and f) Follow-up.
These are JCHAO requirements!
Return this form to the Neurosciences unit. NS-2120H U:\Acute Care Redesign\Stroke Trigger Tool 02-06.doc stf 09-08 11/2008
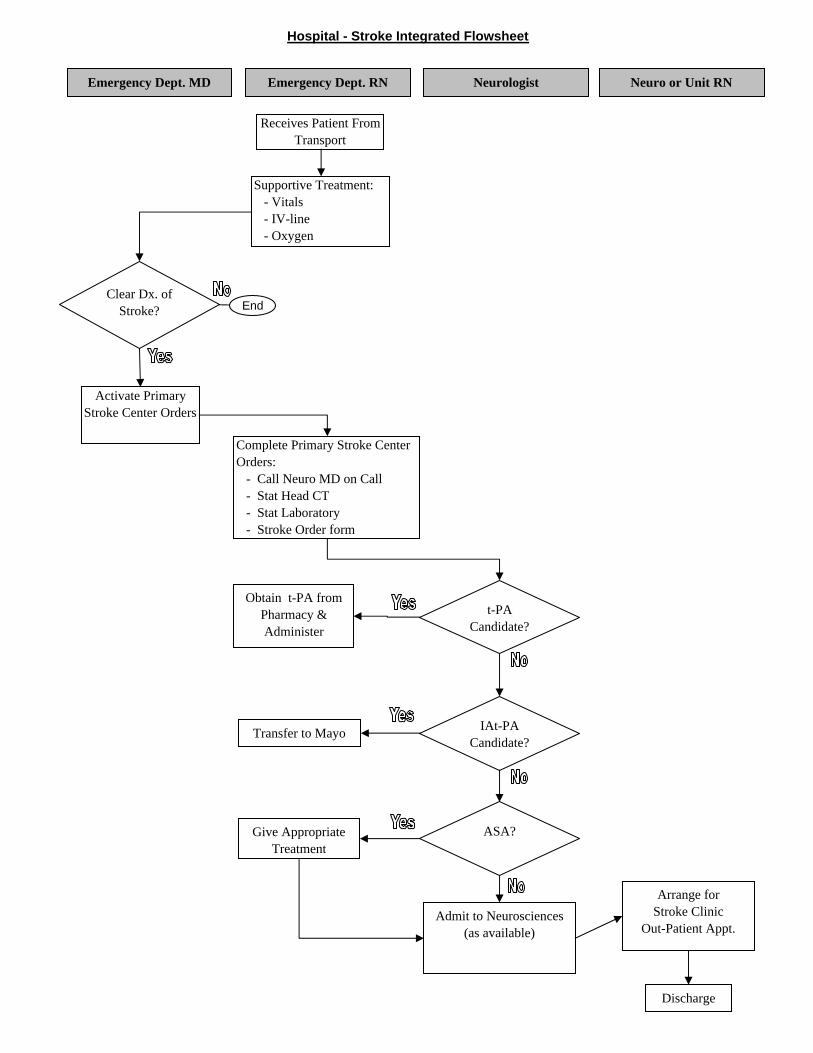
Hospital - Stroke Integrated Flowsheet
Clear Dx. of Stroke?
t-PA Candidate?
Transfer to Mayo
Obtain t-PA from Pharmacy & Administer
Give Appropriate Treatment
Admit to Neurosciences (as available)
Discharge
Arrange forStroke Clinic
Out-Patient Appt.
Emergency Dept. RNEmergency Dept. MD Neurologist
Receives Patient From Transport
Supportive Treatment: - Vitals - IV-line - Oxygen
Activate Primary Stroke Center Orders
Complete Primary Stroke Center Orders: - Call Neuro MD on Call - Stat Head CT - Stat Laboratory - Stroke Order form
IAt-PA Candidate?
Neuro or Unit RN
End
ASA?

What is my specific role and responsibility in implementing the Primary Stroke Center orders?
HUC Role and Responsibility Place the patient on the 33333 census list on IBAX. Double check that all of the following are placed on the patient’s chart: Primary Stroke Center Admission Orders (Initiated on admission one of three
options: Acute Ischemic Stroke, Intracranial Hemorrhage or Subarachnoid Hemorrhage)
ER Audit Tool (place in plastic pocket at the front of the chart) Stroke Trigger Tool (place in plastic pocket at the front of the chart) Place a patient sticker on the Stroke Audit log at the Neuro Nurse’s Station. Transcribe the orders. Pull audit tool at discharge and send to Shannara Faupl—Neuro/Peds/Trauma 4th Floor,
LH. Care Provider RN Role and Responsibility Implement the orders. Complete NIHSS and Bedside Swallow Screen Place the Stroke Trigger Tool in the clear plastic holder on the Proxima nurse server. When appropriate, contact the physician that core measure component(s) are currently incomplete. Provide the patient/family with the appropriate stroke education binder (i.e. Ischemic vs. Hemorrhagic Stroke) Review core education components with the patient/family. Document 5 patient education elements and response in the EMR Stroke Education powerform and on the Stroke Trigger tool.
1. Personal Risk Factors 2. Medications Prescribed 3. Warning Signs & Symptoms of Stroke 4. Activation of EMS 5. Need for follow-up after discharge
Complete RN worksheet and return to Shannara Faupl, 4th floor LH On discharge give the completed trigger tool to the department director. Auditor Role and Responsibility Access the 33333 list on IBAX Use the audit tool to review status of orders meeting the core measures. Continue audit on a daily basis until the patient is discharged using the same trigger tool. If the audit is missing core measures, notify the nurse that the core measures are currently incomplete. Audit the Stroke discharge log to verify appropriate patients are scheduled for follow-up with the Stroke Clinic.
11

MD/PA/NP Role and Responsibility The emergency department or admitting physician should initiate the Primary Stroke Center order set. Document rationale for any missing components in the order set or in the progress notes. Respond to the nurse/auditor communication to order or explain missing components. Therapist Role and Responsibility Receive consults. Provide patient/family education appropriate to Stroke Core measures and document on the EMR Education Powerform. Pharmacist Role and Responsibility Enter clinical message as appropriate. Provide patient/family education related to medications and document response on the the EMR Education Powerform.
Complete the Stroke PostTest on LEO – This is the only way to record completion of the module
To get to the posttest on LEO:
Select Luther Midelfort Academy Select Learning Center (CBT’s, Transcript, Online Registration) Select Online Course Catalog Select LM Eau Claire Posttests Select Stroke Posttest
12


















