Segmental nature of the choroidal vasculature*Segmental nature ofthe choroidal vasculature 635 FIG....
18
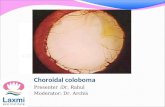
Segmental nature of the choroidal vasculature* SOHAN SINGH HAYREH From the Department of Ophthalmology, University of Iowa, Iowa City, Iowa, USA The classical textbook description of the choroidal vasculature was well summed up by Hogan, Alvarado, and Weddell (I97I) when they wrote that, in the choroid, 'extensive anastomoses exist between the various branches of all the short ciliary arteries, so that occlusion of one vessel ordinarily does not produce infarction of the choroid'. It is also well known that inflammatory, metastatic, and degenerative lesions in the choroid are usually localized. Duke-Elder (I96I) commen- ted: 'The tendency for inflammatory and degenera- tive diseases of the choroid to show a considerable degree of selective localization, despite the fact that anatomically the vessels would appear to form a continuous network, has given rise to specula- tions regarding the anatomical isolation of specific choroidal areas'. Over the past few years I have investigated the choroidal vascular bed anatomically and clinically (in the human) and experimentally (in rhesus monkeys). These studies have been reported from time to time piecemeal (Hayreh, I962-1975), but in this paper an attempt is made to summarize concisely the overall results of my investigations. My various studies can be likened to pieces of a jig-saw puzzle; now by fitting all the pieces to- gether, we can, I believe, arrive at a much clearer insight into the true pattern of the choroidal blood supply. My observations show that the posterior ciliary arteries and their branches, as well as the vortex veins, have a segmental distribu- tion in the choroid, and that the choroidal arteries are end-arteries. Arterial supply of the choroid ANATOMY OF THE POSTERIOR CILIARY ARTERIES The earlier textbook descriptions of the posterior ciliary arteries (PCAs) tend to be misleading and there has been much confusion about their intra- orbital course. For example, Duke-Elder (I96I) stated: 'These arteries have a variable origin from Part of this work was supported by a research grant from the Medical Research Council, London Requests for reprints: S. S. Hayreh, Department of Ophthalmology, University of Iowa Hospitals, Iowa City, Iowa 52242, USA the ophthalmic artery within the orbit, and may be subdivided into two groups-the short and the long'. A detailed account of my studies of the anatomy of the PCAs in man is given elsewhere (Hayreh, 1962); the ophthalmic artery gives out not short and long PCAs, but parent trunks (mostly two or three in number). These I have designated the 'PCAs', either medial (MPCA) or lateral (LPCA) depending upon their relationship with the optic nerve at the point of penetration of their branches into the sclera (Fig. i). Occasionally an additional superior PCA may be seen (Meyer, I887; Hayreh, Eyeball LPCA PPS OA 1MPCA *CAR Intro canalicular part of ON Col. br of OA FIG. I Photograph of inferior surface of optic nerve (ON) and eye ball, showing ophthalmic artery (OA), central artery of retina (CAR), medial (MPCA) and lateral (LPCA) posterior ciliary arteries filled with Neoprene latex. Also shown are collateral branches (Col. br.) of OA to intracanalicular part of ON Brit. Y. Ophthal. (I 975) 599 63 I copyright. on February 11, 2020 by guest. Protected by http://bjo.bmj.com/ Br J Ophthalmol: first published as 10.1136/bjo.59.11.631 on 1 November 1975. Downloaded from
Transcript of Segmental nature of the choroidal vasculature*Segmental nature ofthe choroidal vasculature 635 FIG....

Segmental nature of the choroidal vasculature*
SOHAN SINGH HAYREHFrom the Department of Ophthalmology, University of Iowa, Iowa City, Iowa, USA
The classical textbook description of the choroidalvasculature was well summed up by Hogan,Alvarado, and Weddell (I97I) when they wrotethat, in the choroid, 'extensive anastomoses existbetween the various branches of all the shortciliary arteries, so that occlusion of one vesselordinarily does not produce infarction of thechoroid'. It is also well known that inflammatory,metastatic, and degenerative lesions in the choroidare usually localized. Duke-Elder (I96I) commen-ted: 'The tendency for inflammatory and degenera-tive diseases of the choroid to show a considerabledegree of selective localization, despite the factthat anatomically the vessels would appear to forma continuous network, has given rise to specula-tions regarding the anatomical isolation of specificchoroidal areas'.Over the past few years I have investigated the
choroidal vascular bed anatomically and clinically(in the human) and experimentally (in rhesusmonkeys). These studies have been reported fromtime to time piecemeal (Hayreh, I962-1975),but in this paper an attempt is made to summarizeconcisely the overall results of my investigations.My various studies can be likened to pieces of ajig-saw puzzle; now by fitting all the pieces to-gether, we can, I believe, arrive at a much clearerinsight into the true pattern of the choroidalblood supply. My observations show that theposterior ciliary arteries and their branches, aswell as the vortex veins, have a segmental distribu-tion in the choroid, and that the choroidal arteriesare end-arteries.
Arterial supply of the choroidANATOMY OF THE POSTERIOR CILIARY ARTERIES
The earlier textbook descriptions of the posteriorciliary arteries (PCAs) tend to be misleading andthere has been much confusion about their intra-orbital course. For example, Duke-Elder (I96I)stated: 'These arteries have a variable origin from
Part of this work was supported by a research grant from theMedical Research Council, London
Requests for reprints: S. S. Hayreh, Department of Ophthalmology,University of Iowa Hospitals, Iowa City, Iowa 52242, USA
the ophthalmic artery within the orbit, and may besubdivided into two groups-the short and thelong'.A detailed account of my studies of the anatomy
of the PCAs in man is given elsewhere (Hayreh,1962); the ophthalmic artery gives out not shortand long PCAs, but parent trunks (mostly two orthree in number). These I have designated the'PCAs', either medial (MPCA) or lateral (LPCA)depending upon their relationship with the opticnerve at the point of penetration of their branchesinto the sclera (Fig. i). Occasionally an additionalsuperior PCA may be seen (Meyer, I887; Hayreh,
Eyeball
LPCAPPS
OA
1MPCA
*CAR
Introcanalicularpart of ON
Col. brof OA
FIG. I Photograph of inferior surface of optic nerve(ON) and eye ball, showing ophthalmic artery (OA),central artery of retina (CAR), medial (MPCA)and lateral (LPCA) posterior ciliary arteries filledwith Neoprene latex. Also shown are collateral branches(Col. br.) of OA to intracanalicular part of ON
Brit. Y. Ophthal. (I 975) 599 63 I
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

632 British Journal of Ophthalmology
FIG. 2 Fluorescein fundusangiogram of right eye of66-year-old man with oldcentral retinal arteryocclusion but patent cilio-retinal arteries. Note fillingof choroid on temporal andnasal sides with watershedzone between them still notfilled. Small isolated islandof choriocapillaris is fillinginferotemporal to optic disc.There are two cilio-retinalarteries on temporal side
I962), although Weiter and Ernest (I974) claimed tohave seen it in over one-third of their specimens.From their origin, the PCAs run forwards to-
wards the eyeball and divide into a large number ofbranches before piercing the sclera. Out of these,two small branches (one on the medial side andthe other on the lateral side) are called thelong PCAs, while the rest are the short PCAs(SPCAs). The temporal SPCAs generally pierce thesclera in the area corresponding to the macularregion. The intrascleral course of the SPCAs isstraight and very short, while that of the longPCAs is oblique and long (Hayreh, I974d). Itis therefore important that we clearly define in anydescription the type of artery concerned. Inalmost all previous descriptions 'PCA' and 'SPCA'have been considered synonymous, and yet theformer is the mother and the latter one of the manydaughters (the long PCA being another daughter)!My experimental studies were carried out in
rhesus monkeys; the normal anatomical pattern ofthe PCAs in the monkeys (Hayreh, I964) revealedthat there is usually one large LPCA and sometimes
two, usually two MPCAs and sometimes one orthree. This pattern was similar to that seen in man.
DISTRIBUTION IN THE CHOROID BY THE VARIOUSARTERIES
Posterior ciliary arteries (PCA)The MPCA and LPCA usually supply the nasaland temporal halves respectively of the choroid(Figs 2, 3). LPCA may supply up to two-thirdsof the choroid with MPCA supplying a correspon-dingly smaller area (Hayreh, 1970; Hayreh andBaines, 1972a) (Fig. 4). In some instances thearea of supply by the MPCA and LPCA may besomewhat obliquely oriented (Fig. 3), In 20 percent of the eyes in rhesus monkeys I found that,instead of the lateral and medial distribution, therewas a superior and inferior distribution (Hayreh,1970) (Fig. 5). The border between the area ofsupply by the MPCA and LPCA usually passesthrough the optic disc (Figs 2 to 5). When thenumber of either LPCAs or MPCAs is more thanone, the choroid supplied by the PCA may be a
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 633
FIG. 3 Fluorescein fundusangiogram during retinalarterial phase of right eyeof 76-year-old woman,with anterior ischaenicoptic neuropathy ofsuperiornasal half of opticdisc and temporal arteritis,showing non-filling ofsuperiornasal half ofchoroid and optic disc
segment of the usual distribution by the medial orlateral PCA (Fig. 6).
Short posterior ciliary arteries (SPCA)These were investigated only in the area of theLPCA (Hayreh, 1974c). The area of the choroidsupplied by each temporal SPCA varies greatly insize, shape, and location; and these segmentsresemble a jig-saw puzzle in the distribution of theLPCA (Fig. 7). Each piece of the jig-saw patternhas a well-defined margin which forms the water-shed zone between the adjacent SPCAs. Since thetemporal SPCAs pierce the sclera to enter the eyeballin the macular region and spread out to the peri-phery of the fundus radially to supply the temporalhalf of the choroid it is natural that most of thesegments of the choroid supplied by the temporalSPCAs and their watershed zones should meet inthe macular region and extend from the posteriorpole to the periphery (Fig. 7). Smaller sub-divisionsof the SPCAs supply still smaller segments ofirregular shape and size with well-defined margins.
These are frequently seen on fluorescein angio-graphy as geographical spatial filling defects in thenormal human choroid (Fig. 8). Each of the ter-minal choroidal arterioles supplies a small segmentof choriocapillaris, and these are arranged like amosaic (Fig. 9).
Long posterior ciliary artery (long PCA)My studies revealed that one long PCA branchesfrom the MPCA and the other from the LPCA:they do not arise directly from the ophthalmicartery; this contradicts the classical textbook des-cription (Leber, 1903; Wolff, 1948; Duke-Elder,I96I).Once again, contrary to the accepted description
of distribution in the choroid by the long PCA,my studies (Hayreh, 1974d) have revealed that thetemporal long PCA invariably supplies a sector ofthe choroid posterior to the equator, starting almostimmediately from the point where it joins thechoroid after it has pierced the sclera (Fig. 7)and extending forwards. Weiter and Ernest (I974)
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

634 British Journal of Ophthalmology
FIG. 4 Fluorescein fundus angiogramof right eye of monkey afterexperimental occlusion of centralretinal artery. Lateral posteriorciliary artery supplies temporal halfand superior nasal part of choroid.Early filling of medial posteriorciliary artery in inferior nasal sectorof choroid is seen. Border zonebetween these and nasal peripapillaryregion is still not filled. Part of opticdisc supplied by lateral posteriorciliary artery is filled
also described a similar distribution in humaneyes.
Is there a special macular artery supplying thesubmacular choroid?
To explain the selective localization of manypathological lesions in the macular region, theexistence of such an artery has been postulated byHepburn (1912) and Amalric (I973) but not on ananatomical basis. Weiter and Ernest (I974), fromstudies involving intravascular injection of bothIndian ink and Neoprene latex into 67 humancadaver eyes, described the invariable presence of adiscrete submacular choroidal circulation providedby a direct submacular artery and a recurrentsubmacular branch of the temporal long PCA.Using identical injection methods in human eyes,Wybar (1954a) (27 eyes) and Ring and Fujino(I967) (I25 eyes) failed to find any such artery intheir meticulous studies. It is worth noting thatWybar (1954a, b) was specifically interested inexploring the submacular blood supply and yetfailed to find what Weiter and Ernest (I974) claimed
to have seen in all of their 67 eyes. It is difficultto understand how all the previous workers investi-gating the submacular choroid by the same tech-nique could have failed to find what Weiter andErnest (1974) claimed to be a constant feature. Inmy experimental study in 47 eyes of rhesus mon-keys, in which my primary objective was to investi-gate the submacular choroidal blood supply, Idid not find any submacular artery (Hayreh,1974c). In spite of the claims of Weiter and Ernest(1974) to have discovered a special submacularartery (although little definite evidence is offeredin their paper), there is so far a preponderance ofevidence against the existence of such an artery.The subject of the submacular choroidal vasculatureis discussed at length elsewhere (Hayreh, 1974c).
ChoriocapillarisThe textbook description of the choriocapillaris isthat it forns a single continuous layer ofwide-lumencapillaries arranged in one plane, and that theseform a continuous anastomotic network over theentire choroid. Although Rohen (i965) stated that
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 635
FIG. 5Fluoresceinfundusangiograms ofright eye ofmonkey afterexperimentalocclusion ofcentral retinalartery, showingfdling of upperhalf of choroidand optic discwith.well-demarcatedhorizontal border
'the entire choriocapillaris network undoubtedlyhas a continuity by capillary anastomoses', he didfind that 'the finer branches of the choroidal ar-
teries run in relatively delimited sectors of thechoriocapillaris'. Henkind (I967) stated that 'block-ing a choroidal artery leads to diminished or absentflow in a large segment of the choriocapillaris; thisis in spite of the fact that the choriocapillaris seems
to be a continuous anastomostic network over theentire choroid'. Dollery, Henkind, Kohner, andPaterson (1968) described fluorescein angiographyof pigs' eyes with experimentally raised intraocularpressure; they recorded the filling of the chorio-capillaris in the form of dots, and stated that 'thiswould indicate that the choriocapillaris fills as a
series of small independent segments rather thanas a continuum over the entire surface'.My fluorescein angiographic studies on the
choriocapillaris (Hayreh, I974b) revealed that eachterminal choroidal arteriole supplied an indepen-dent segment of the choriocapillaris, with thearteriole joining the segment in its centre, and thedrainage venules lying around the periphery ofthis segment (Fig. io). Each segment is a functionalunit, usually of a polygonal shape (Fig. 9) with no
anastomosis with the adjacent segments in vivo. Thevarious segments are arranged like a mosaic, theborders of the mosaic being formed by the venous
channels (Figs 9, io). This has been confirmedby the finding of a lobular arrangement in thechoriocapillaris, in a study of flat preparations ofthe choriocapillaris (Torczynski and Tso, I974).The size of each unit of the mosaic varies, and itwas found that the diameter of each unit wasusually about one-quarter of the disc diameter orless (Figs 2, 9). Krey (I975) recently confirmed thesegmental distribution by the choriocapillaris inman, by using the histochemical alkaline phos-phatase reaction in cadaver eyes. He stated, how-ever, that his technique showed that the feedingarteriole was at the periphery and the drainingvenule in the centre of the choriocapillaris lobule.This picture of the feeding arteriole and drainingvenule in a choriocapillaris lobule is the reverseof that seen not only by me on fluorescein angio-graphy in the living eye but also on fluoresceinangiography by Dollery, Henkind, Kohner, andPaterson (I968) and others, on flat preparationexamination of the choriocapillaris by Torczynskiand Tso (1974), and on injection studies in cadavereyes by Weiter and Ernest (I974), and many others.The filling pattern sequence of the vascular bedon fluorescein angiographic studies (Fig. 9) showsthe state in the living eye while histochemicalstaining techniques do not give the same informa-tion and can be misleading. Unfortunately, we
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

636 British Journal of Ophthalmology
FIG. 6 Fluorescein fundusangiogram of normalhuman right eye, showingsectoral filling of choroidand adjacent prelaminarregion of optic nerve head
already know that post-mortem studies in thechoroidal vascular bed are markedly inferior toin vivo studies to obtain information about thestate of the circulation in the living eye and havegiven rise to some misleading artefacts.
CHOROIDAL ARTERIAL ANASTOMOSES
The classical concept was well summed up byRing and Fujino (I967) when they concluded thatSPCAs 'do not have the characteristics of end-arteries for they anastomose freely with each otherand communicate as well with recurrent branchesfrom the long posterior ciliaries, the anterior cilia-ries, and vessels from the major circle of the iris'.This view has been shared by a majority of theworkers in the field. In the literature interarterialand arterio-venous anastomoses in the humanchoroid have been described after post-morteminjection studies; however, it has been suggestedby others that the choroidal arterial supply issegmental in vivo (Hayreh and Baines, 1972a).
In my in vivo experimental studies in rhesusmonkeys, involving cutting of the PCAs (Hayreh,
1973b; Hayreh and Baines, 1972a), SPCAs (Hay-reh, I974c) and long PCAs (Hayreh, I974d) andinvestigating the choroidal circulation with fluores-cein angiography, I found that these arteries donot anastomose at any level with any neighbouringartery, and are functional end-arteries. My studies(Hayreh, 1974b) also demonstrated that lobules ofchoriocapillaris supplied by each terminal choroidalarteriole show no functional anastomosis in vivowith one another. These haemodynamic studiestherefore place a contrary interpretation upon thestatement of Ring and Fujino (I967) and the pre-valent concept based on post-mortem studies, anddemonstrate the in vivo segmental distribution inthe choroid not only of the main PCAs but also ofall their subdivisions right down to the terminalchoroidal arterioles and the choriocapillaris. Theborder between any two neighbouring vessels,from the main PCAs down to the terminal choroidalarterioles, forms a watershed zone. The watershedzone between the main PCAs usually passes throughthe optic disc, as shown in Figs 2 to 7. The water-shed zones between the various temporal SPCAsand also those of the temporal long PCA are shown
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 637
schematically in Fig. 7. The watershed zonesbetween the various units of the choriocapillarisare shown in Fig. 9. The post-mortem studies,
FIG. 7 Diagrammatic representation of distribution byvarious temporal SPCAs and their watershed zones inposterior part offundus. Dotted circle in region ofdistribution of temporal SPCAs represents macularregion. Areas of supply by medial PCA and temporallong PCA are also shown
although extremely useful, have misled us tosome extent about the actual haemodynamics inthe choroid in general, and of the choriocapillarisin particular.The peripapillary choroid, via recurrent pial
branches in the pia of the retro-ocular optic nervewas found to establish anastomoses with pialbranches from other sources (Hayreh, I963b). Inexperimental occlusion studies of the PCAs(Hayreh, 1973b; Hayreh and Baines, I972a), wefound a filling of the peripapillary choroid viathese anastomoses. This was also seen in similarstudies by Anderson and Davis (1974). However,no such peripapillary choroid filling was ever seenin patients with PCA occlusion and consequentanterior ischaemic optic neuropathy (Hayreh,1974g, 1975). This discrepancy between the clinicaland experimental findings is discussed below(p. 641).
POSTERIOR CILIARY ARTERY DISTRIBUTION
These arteries supply the following tissues:
The choroidSPCAs supply the choroid presumably as farforward as the equator of the eyeball. Because of
FIG. 8 Fluorescein fundus angiogramof normal human eye, showing threegeographical filling defects inchoriocapillaris bed
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

638 British Journal of Ophthalmology
FIG. 9 Choriocapilloris pattern in fluoresceinfundus angiograms of monkey's eyes(a) Showing various units of choriocapiUlarismosaic (each unit supplied by terminal choroidalarteriole) : note presence of some empty unitsamong normally filled units (compare withfilling defects in Fig. 8)(b) and (c) Two consecutive angiograms ofmonkey eye showing: (b) Earliest arterialfilling of choriocapillaris and their feedingterminal choroidal arterioles; (c) Venous-phases of choriocapillaris filling with honeycombpattern. Fluorescence of optic disc is due toearlier injection offluoresceinNote that the time interval between (b) and(c) is about o.8 s, indicating tremendous speedof normal circulation in choriocapillaris andchoroid. This is because wide lumen ofchoriocapillaris offers much less resistance toblood flow than retinal-or any other capillaries
FIG. ga
FIG. 9b
,
611..hF.#z
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 639
limitations of the ordinary fundus camera in photo-graphing the fundus near the equator and anteriorto that, it has not been possible to investigate thesupply by the SPCAs in the equatorial region andin front of it. In studies involving occlusion of thePCAs (Hayreh, 1973b; Hayreh and Baines, I972a)and SPCAs (Hayreh, I974c), no retrograde fillingof the choroid from the equator backwards was
ever recorded, demonstrating the absence of anyfunctional anastomoses between the SPCAs andthe anterior choroidal arteries. The long PCAs, inaddition to their contribution to the posteriorchoroid (Hayreh, I974d) (Fig. 7), also supply thechoroid anterior to the equator because of theirfinal destination in the ciliary body.
The retina
The choroid supplies the overlying retina to a depthof about 130 ,um which includes the pigmentepithelium layer, the layer of rods and cones, theouter nuclear and plexiform layers, and the wholethickness of the foveal retina. In eyes with cilio-retinal arteries (Fig. 2), a variable area of the innerlayers of the retina is also supplied; a cilio-retinalartery may supply an area of the retina varyingfrom a tiny insignificant piece to as much as half
FIG. 9C
and, rarely, even the entire retina (Hayreh, I963a).In some animals, such as cats, the entire bloodsupply to the retina is via the cilio-retinal arteriesbecause of their lack of a central retinal artery.Thus the PCAs have a very important role to playin the blood supply of the retina.
Anterior part of the optic nerve (including the opticnerve head)The PCAs are the only source of blood supply tothe lamina cribrosa and prelaminar regions, and themain (if not the only) source to the retrolaminarregion, and may supply the surface nerve fibrelayer of the optic disc in some instances. Theprelaminar region is mainly supplied from theperipapillary choroid (Figs 3 to 6). The subject ofblood supply of the anterior part of the opticnerve is fully discussed elsewhere (Hayreh, I969,1974a, 1975).
Anterior uveal tract
The long PCAs play a role in the blood supply ofthe anterior uvea-that is, iris, ciliary body, andanterior part of the choroid.The blood supply in the choroid and anterior
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

640 British Journal of Ophthalmology
'i. p
FIG. IO Three-dimensionalschematic representation ofchoriocapillaris flow pattern.A choroidal arteriole;V choroidal vein
V*
part of the optic nerve by the PCAs and theirsubdivisions, down to the terminal arterioles, issegmental. The blood supply by the long PCAis segmental in the choroid posterior to the equator,and presumably also in the anterior uvea.
Venous drainage of the uveal vasculatureIt is generally assumed that the uveal veins freelycommunicate and that the vortex veins have nosegmental distribution. Our in vivo studies inrhesus monkeys (Hayreh and Baines, 1973) re-vealed that each vortex vein has a well-definedsegmental distribution extending throughout theentire antero-posterior length of the uveal tractinvolving the veins in the corresponding segmentof the iris, ciliary processes, and the choroid.Occlusion of one vortex vein, therefore, producedmarked localized venous engorgement in the corres-ponding segment of the iris, ciliary processes, andthe choroid without involving veins in the restof the uveal tract. The watershed zones between thevarious vortex veins, therefore, extend antero-posteriorly through the entire length of the uvealtract, a horizontal watershed between the upperand lower vortex veins passes through the opticdisc and macular region, while a vertical watershedbetween the temporal and nasal vortex veins passesin between the optic disc and macular region (Fig.ii). This divides the entire uveal venous systeminto four functionally independent segments; ifthe number of vortex veins is less or more than theusual four, the number of segments would alsochange accordingly.
Clinical significance of segmental distributionof uveal vasculatureThe various aspects of this subject are discussedin detail elsewhere (Hayreh, I973b, I974b-g,
1975; Hayreh and Baines, I972b, c, I973). Vascularocclusive disorders of the choroid are consideredhere under the three following headings:a. Arterial occlusive disordersb. Choriocapillaris occlusive disordersc. Venous occlusive disorders.
OCCLUSIVE DISORDERS OF THE POSTERIOR CILIARYARTERY AND ITS SUBDIVISIONS
It has been demonstrated above that the arterialsupply to the choroid is segmental from the PCAsright down to the choriocapillaris. However, ourexperimental occlusion of the various PCAs inrhesus monkeys did not produce infarction of theentire choroid supplied by the occluded PCA:instead there were only small patchy choroidalinfarcts distributed in the territory of the occludedartery, and sometimes, indeed, no lesion at all inthe choroid (Hayreh, 1973b; Hayreh and Baines,1972b). On occluding the SPCA and long PCA,no choroidal infarct was usually seen in experi-
Vortex venous watershedsQ0 55(0Q33-0 66)mm
X0 057mm
~FRight eye
FIG. I I Diagrammatic representation of watershedzones of vortex veins. F and Xfovea; M macularregion; OD optic dise
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 64I
ments with rhesus monkeys. These findings seemto conflict with the above-mentioned concept ofsegmental supply by the choroidal arteries. It is,therefore, imperative to discuss the various factorsinvolved in these discrepancies.i. There is a very important difference between
these experimental occlusions in rhesus mon-keys and those occurring as a disease processin humans. All the animals used in experi-mental studies were young and healthy; theirage corresponded to that of a IO to I5-year-oldhuman or younger. The normal healthy vascularbed, in almost all of the body of young, healthyindividuals, has a great potential to developquick collaterals and it is extremely difficult toproduce any massive infarctions. By contrast,in elderly arteriosclerotic individuals withdiseased vasculature, the response to similararterial occlusion would be totally different.In an attempt to produce experimental ocularischaemia (Henkind, I974), similar to that seenin pulseless disease, a common carotid arterywas ligated in a dog; this failed to produce anyischaemia. After some time the second commoncarotid artery was ligated, also with no effect.Then one vertebral artery, followed later by thesecond, was ligated but the animal still did notdevelop ocular or cerebral ischaemia, because ofquickly developed collaterals. In elderly indi-viduals, on the other hand, it is well known thatligation of one or two of these arteries would becatastrophic. Similarly, in my young monkeys,I have on many occasions ligated the femoraland axillary arteries high up while cannulatingthem without producing any ischaemia in thelimbs, although similar arterial occlusions inelderly humans would produce massive gan-grene. From these and many similar reportsin the literature, and from the developmentof prominent extraocular anastomoses afterPCA occlusion in rhesus monkeys (Hayrehand Baines, I972a), it seems logical to concludethat occlusion of the various types of PCAs,which produces minor choroidal lesions or nonein young, healthy monkeys, would produce amarked ischaemic lesion in an old, arterio-sclerotic human patient. This is an importantconsideration to be borne in mind.
2. Perfusion of intraocular vessels is dependentupon the perfusion pressure (perfusion pressure= mean blood pressure minus intraocularpressure). In experimental studies involvingocclusion of the PCA, SPCA, and long PCA byorbitotomy there was a marked fall in, intra-ocular pressure, which became unrecordablylow i or 2 days after the occlusion (Hayreh,I974d, Hayreh and Baines, I972b). Such amarked fall in the intraocular pressure would
assist the filling of the occluded segment of thechoroid from the channels mentioned below.The perfusion of the occluded choroid in eyeswith nortnal intraocular pressure would bemuch less than that in eyes with unrecordablylow pressure. This is another important differ-ence between these experimental occlusionsand those occurring in patients.
3. The segment of the choroid supplied by anartery does not correspond exactly with thesegment drained by a large choroidal vein; thereis always a certain amount of overlap betweenthe adjacent arterial segments via the veins.For example, the mechanism of retrograde flowinto the occluded choroid, when one of theSPCAs is occluded, is shown diagrammaticallyin Fig. 12. This shows two adjacent segmentsof the choroid supplied by two arteries-theartery to the upper segment is patent whilethat to the lower segment is occluded. Theblood from the patent artery fills the chorio-capillaris in its territory and drains into thecorresponding vein which joins the vein fromthe occluded segment. The common vein thusdrains one nornally filling segment and oneoccluded segment of the choroid. Since theblood pressure in the vein from the occludedsegment is practically zero, some blood fromthe large vein regurgitates into the empty veinand partially fills the empty segment. This wasseen on fluorescein angiography in all experi-mental occlusions of the SPCAs. Most probablythis reflux of blood from a large vein into theoccluded segment is due to the pumping actionproduced by ocular pulsation.
Fig. 13 illustrates diagrammatically whathappens when an MPCA or LPCA is occluded.The territory of the uveal tract drained by onevortex vein is usually supplied by two PCAs
Chor ocapilari i
normally fillinq
c oroidol Choroidolarter Ivein
A 7 mV
choro'dol fluorescein flowartery ~ ' in choroidal vein
La tefiliinq
FIG. 12 Diagrammatic representation of mechanism ofretrograde filling of choroid in area of an occludedshort PCA
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

642 British Journal of Ophthalmology
FIG. 13 Diagram showing route of retrograde flow ofblood via vortex vein into part of choroid supplied byoccluded PCA. Arrows indicate direction offlow ofblood in various vessels
(to the posterior uvea) and a large number ofof the anterior ciliary arteries (to the anterioruvea). Thus, occlusion of the MPCA or LPCAreduces the blood pressure in the venous tribu-taries draining the non-filling sector of thechoroid. Blood would regurgitate from themain stem of the vortex vein into these tribu-taries and lead to retrograde filling of the choroid.This is supported by the fact that in the occlu-ded territory isolated areas of the choroidstart to fill with fluorescein on angiographyduring the late venous phase. These fluores-cent patches are not continuous with any partof the normally filled choroid (Hayreh andBaines, 1972a). The normal ocular pulsation,by acting as a pumping mechanism, wouldhelp in filling and emptying the veins from theoccluded choroid. When the main PCA isoccluded, the occluded area of the choroid isso large that there is not enough overlap be-tween the occluded and unoccluded segmentsby the mechanism mentioned above, and hencefundus lesions are almost always seen. Thusthe various arterial segments communicatevia the choroidal veins, with no direct communi-cation between the arteries.
4. The venous blood in the choroid is known tohave a very high concentration of oxygen (Co-han and Cohan, I963; Elgin, I964; Pilkerton,Bulle, and O'Rourke, I964; Alm and Bill,I970). Any part of the choroid which showedany perfusion during the transit of the dye onfluorescein angiography did not develop choroi-dal lesions in our studies (Hayreh and Baines,1972b); thus indicating that a slow trickle ofvenous choroidal blood was enough to supplythe required amount of oxygen. It was interest-ing to observe that in our experimental PCAocclusion, elongated pointed lesions occurred
with narrow intervening strips of normal-looking fundus (Hayreh, I973b; Hayreh andBaines, 1972b) (Fig. 14); the latter were mostlyoverlying large choroidal veins. This wouldindicate that diffusion of oxygen through thethin-walled choroidal veins was enough to pre-vent ischaemic damage in the overlying tissue.
5. Other extraocular anastomoses which help tofill the occluded choroid are described elsewhere(Hayreh and Baines, 1972a). The blood whichcomes through these anastomoses also reachesthe choroid by the venous phase of the transitof dye, and is thus of a venous nature and hassufficient oxygen in it.The interpretation of the effects of occlusion of
the PCA or its further subdivision must thereforebe considered in the light of these important factors.The following clinical lesions are seen in eyes
with occlusion of the PCA which is usually due toarteriosclerosis but may occur in other vasculardiseases-such as hypertension, collagen disease,temporal arteritis, diabetes, syphilis, hypercholes-terolaemia, thromboangiitis obliterans, Raynaud'sdisease, migraine, pulseless disease, embolism, andvarious haematological disorders.
(a) Chorio-retinal lesionsIn our studies of PCA occlusion, we described thedevelopment of patchy chorio-retinal lesions in thefundus situated posterior to the equator and in the
FIG. 14 Fundus photograph of monkey, showingwhite chorio-retinal lesions 2 days after occlusion ofLPCA. Note absence of lesion over major choroidalveins
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 643
part supplied by the artery (Hayreh, I973b;Hayreh and Baines, I972b). These were due toinfarction of the pigment epithelium and the outerretina (Fig. 14). Within 24 hours after the occlu-sion, white patches of markedly varied shape, size,and distribution were seen; after 2 to 3 weeksthese became greyish-white, granular, and depig-mented areas. Similar chorio-retinal lesions havebeen described in patients (Hepburn, 1935; Amalric,1971; Foulds, Lee, and Taylor, 1971). Presumablymany of the segmental chorio-retinal degenerativelesions of obscure aetiology and some of the atypicalsectoral or uniocular retinitis pigmentosas belongto this group.
(b) Anterior ischaemic optic neuropathy (AION)I have investigated the subject recently and discus-sed it at length elsewhere (Hayreh, 1974f, g, 1975).In AION there is a comparatively sudden loss ofvision in the entire eye or in one sector of thefield of vision of the eye, initially associated withoedema of the optic disc, which resolves to opticatrophy within a month or two, leaving a permanentvisual defect. Its pathogenesis has been the centreof a good deal of controversy. My clinical (Hayreh,1974f, g, 1975) and experimental (Hayreh andBaines, I972c) studies, and a review of histopatho-logical findings in such eyes reported in the litera-ture (Henkind, Charles, and Pearson, 1970) showthat AION is due to occlusion of the PCAs. Re-cently, Anderson and Davis (1974), from experi-mental occlusion of the- PCAs in II Squirrelmonkeys, concluded that the AION 'must repre-sent disease of more than just the PCAs' becauseonly minute areas of atrophy in the optic nervehead were found instead of the large areas of infarc-tion seen in patients. I have discussed the fallacyof such a statement elsewhere (Hayreh, 1975) andit can be understood if one considers the followingdifferences between experimental studies andpatients with AION.I. The age of the monkey used in the experimental
PCA occlusion by us (Hayreh and Baines,1972c) and by Anderson and Davis (I974) iscomparable with an age of I0 to 15 years oryounger in humans. AION, however, is adisease of persons who are past middle agewith arteriosclerosis, arterial disease, hyper-tension, etc. The importance of this age factoris discussed on p. 641.
2. The other important complicating factor inexperimental PCA occlusion as compared withthe PCA occlusion occurring in patients is themarked fall in intraocular pressure to unre-cordably low levels in the monkeys after lateralorbitotomy (Hayreh, I974d; Hayreh and Baines,1972b) (see p. 641).
We have demonstrated clearly that PCA occlu-sion in young monkeys immediately opens up theanastomoses between the peripapillary choroid andthe pial plexus on the optic nerve via the recurrentpial branches from the peripapillary choroid (Hay-reh and Baines, I972a). The perfusion of vesselsin the peripapillary choroid and optic nerve headfurther improves markedly after the above-men-tioned fall in intraocular pressure (Hayreh, 1975).This explains the frequent absence of markeddamage to the anterior optic nerve in animals.On the other hand, a similar or even much lesssevere occlusion of the PCAs in elderly arterio-sclerotic persons with normal intraocular pressureand diseased arteries would produce massiveinfarction (Fig. 3). Evidently Anderson and Davis(I974) did not take these additional factors intoconsideration in reaching their conclusions.
Role of the choroidal blood supply in macular lesions
The localized involvement of the macular regionby a large number of conditions is well known andthis has naturally excited a good deal of curiosityabout the reasons for this marked vulnerability ofthe macular region to degenerative disease. Ihave discussed the submacular choroidal vascularpattern and its possible role elsewhere (Hayreh,1974c). It may be stated at the outset that we haveso far no definite evidence of the existence of aspecial artery to the submacular choroid, despitesome claims (p. 634). My in vivo studies in monkeysshowed that the macular region is the meetingpoint not only of many watershed zones of thevarious SPCAs (Fig. 7), but also of all the watershedzones of the vortex veins (Hayreh and Baines,1973) (Fig. II).To understand the clinical significance of the
fact that the macular region of the retina is locatedat the meeting-place of the watershed zones of theSPCAs, one must discuss the circulatory disordersof the watershed or boundary zones. Of all thevarious endarterial systems with watershed zonesin the body the cerebral circulation has been investi-gated most thoroughly. It has been known forsome time that the watershed zones between largearterial systems are more vulnerable to ischaemiaor anoxia than others in the brain (Blackwood,McMenemey, Meyer, Norman, and Russell, 1963).This phenomenon was first demonstrated byLindenberg and Spatz (1940) and has subsequentlybeen described by many workers (Meyer, 1953;Zulch, 1953; Norman, Urich, and McMenemey,1975; Zulch and Behrend, I96I). The haemody-namic peculiarities of these watershed zones werediscussed by Eich and Wiemers (1950). Schneider(1956), while discussing the special vulnerabilityof the watershed zones of the vascular tree to
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

644 British Journal of Ophthalmology
ischaemia, compared the process to failure of afarm irrigation system in which 'the meadows atthe end of the line suffer most when the main pipesupplies too little water'. When there is a generalizedreduction of blood supply to the brain, ischaemiais felt most in the most distal part of the irrigationareas-that is the watershed zones (Alajouanine,Castaigne, Lhermitte, Cambier, and Gautier,I959). This process, in the German literature, hasaptly been called wipfeldaire, which literally meanswithering away of the peripheral twigs of a treebecause nutrition is not reaching them (Fig. IS).In the cerebral circulation it is known that ischae-mic anoxia of the terminal vascular net results insmall vessel changes, particularly at the junctionof the watershed zones of the principal cerebralarteries, and it has been stated that cerebral ischae-mia may occur in spite of a continuing circulation,because it is insufficient to meet the metabolicneeds of the tissue (Meyer, I96I). It has also beenshown experimentally in monkeys that anastomoticcerebral circulation does not become established ifthe blood pressure in the arterial field surroundingthe ischaemic zone falls below 6o mm Hg (Meyer,Fang, and Denny-Brown, 1954). In the eventof a fall of blood pressure in the cerebral cir-culation, it can be presumed that the bloodsupply may be adequate for the proximal butnot for- the distal territories; this, however, isnot so, because the proximal supply may bemore severely affected than the distal (Normanand-others, 1957).From the observations of the wateshed zones of
the cerebral circulation, it would seem logical toconsider that the macular region in the eye, wherenumerous watershed zones of the SPCAs (Fig. 7)and of the vortex veins (Fig. i i) meet, would behighly vulnerable to ischaemic disorders in anygeneralized chronic ischaemic disorder of the choroid.This process may be compared with that illus-trated in Fig. I6, where, on a fall of water pressurein the garden sprinklers, the central area whichpreviously received an adequate water supplyfrom all the surrounding sprinklers, has dried up.A reduction and even disappearance of the chorio-capillaris in the macular region which may beseen in senile macular degeneration is shownschematically in Fig. I7. It is postulated (Hayreh,I 974c) that senile macular degeneration, seniledisciform macular degeneration, and allied maculardisorders are most probably due to this unusualpattern of the submacular choroid, compared withthe rest of the choroid. Similarly, pigmentary andother degenerations seen in old persons in theperipheral part of the fundus may represent anischaemic phenomenon in the watershed zonesbetween the short posterior and the anterior ciliaryarteries.
Role of the long PCA in anterior segment ischaemiaThe occurrence of anterior segment ischaemiaafter diathermy, scleral buckling, and some otherprocedures for retinal detachment has been attri-buted to interference with the long PCAs, so that
FIG. I5 Photograph of tree showing phenomenon ofwipfeldiure (withering away of peripheral twigsbecause nutrition is not reaching them). Note that evenone of the lower branches has completely withered(arrow); this is comparable with early macular branchesfrom SPCAs
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 645
-tend to be localized. The segmental nature ofthe choriocapillaris already described (p. 635) helpsto explain such localization. Elschnig's spots,
FIG. I6 Two illustrations demonstrating effect ofreducing water pressure in eight garden sprinklerswatering a lawn(a) Watering at normal water pressure(b) Same area supplied by sprinklers with reducedwater pressure. Note that in area where water supplyby various sprinklers meets in centre, lawn has dried up,as have peripheral parts of lawn although intermediatezone is still normal
these arteries have become a 'sacred cow' forophthalmologists. My studies of the in vivo effectsof occlusion of the long PCAs in rhesus monkeys(Hayreh, 1974d) revealed that occlusion of thelong PCAs produces no significant effect on theanterior segment. The sacred-cow status of thelong PCAs is based on previous studies in rabbitsin which the long PCAs are the only source ofblood supply to the anterior segment-whereasin primates and man the anterior segment issupplied by the anterior ciliary arteries (usuallyseven in number) and the long PCAs (two innumber).Many unsuccessful attempts have been made in
human subjects to find out if occlusion of the longPCA would help to control the raised intraocularpressure in glaucoma; this subject is reviewedelsewhere (Hayreh, I974d).
OCCLUSIVE DISORDERS OF THE CHORIOCAPILLARIS
It is known that choroidal lesions-particularlyinflammatory, metastatic, and degenerative lesions
FIG. 17 Diagrammatic representation of distribution ofchoriocapillaris supplied by various temporal SPCAs(a) Normal pattern(b) Postulated pattern caused by generalized chronicischaemic disorder of choroid, with reduction ofchoriocapillaris most marked in macular region andequatorial choroid (compare Fig. I 6b)
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

646 British Journal of Ophthalmology
I feel that so-called 'acute posterior multifocalplacoid pigment epitheliopathy' (Gass, I968)represents an occlusive disorder of the terminalchoroidal arteriole because each focus in thisdisease has a close resemblance in size and shapeto a unit of choriocapillaris supplied by a terminalchoroidal arteriole. The initial whitish focusprobably- represents pigment epithelial infarctionand the later depigmented spots probably representpigment epithelial degeneration overlying theoccluded units of the choriocapillaris (similar tothat seen in our experimental posterior ciliaryartery occlusion-Hayreh, 1973b: Hayreh andBaines, 1972b). However, the cause of the occlusionstill remains obscure. Similarly the fluorescein-leaking spot seen on fluorescein angiography incentral serous retinopathy, and the multiplefluorescent spots in Harada's disease, seem tocorrespond to individual choriocapillaris units(Fig. 9).
FIG. I8 Fluorescein fundus angiogram of eye withmultiple drusen, about 3 min after injection offluorescein,showing pigment epithelial defects (unmasking thechoroidal fluorescence); each fluorescent patch resemblesgreatly area of supply by terminal choroidal arterioleto choriocapillaris. (Reproduced by courtesy ofProfessor J. A. Oosterhuis)
Siegrist's streak, and other allied lesions in malig-nant hypertension and associated diseases, and incollagen disease (for example, polyarteritis nodosa),represent pigment epithelium degenerative changesover a segment of the choriocapillaris, which are
due to fibrinoid necrosis and obliteration of thechoroidal arteriole and its segment of the chorio-capillaris. Microsphere embolization of choroidalarteries in dogs (Golder and Gay, I967) and in cats(Henkind, I967) produced similar fundus lesions.The shapes and sizes of many of the conditionsincluded in the category of 'flecked retina syndrome'(Krill and Klien, I965) very much resemble thechoriocapillaris pattern. For example, lesions inso-called Doyne's honeycomb dystrophy correspondto the arterial part of the choriocapillaris units(Figs 9 and I8) and suggest that they may bedue to a disorder of the arterial segment of thechoriocapillaris. In fundus flavimaculatus the shapeand distribution of the 'fish tail' lesions resemblevenous segments of the choriocapillaris units andsuggest that this may be a disorder of the venous
part of the choriocapillaris unit. A vascular basisfor the flecked retina syndrome is further suggestedby the occurrence in the mid and far periphery ofthe fundus of chorio-retinal lesions (Newell, 1975)similar to those seen in choroidal ischaemia.However, the inheritance patterns seen in thissyndrome are hard to explain on a vascular basis.
OCCLUSIVE DISORDERS OF THE VORTEX VEINS
The clinical picture of retinal venous occlusion iswell known, but no corresponding description ofvortex vein occlusion in man has previously beenavailable. Following on my experimental studies,involving in vivo occlusion of the vortex veins inrhesus monkeys (Hayreh and Baines, 1973), I havepresented a clinical picture of such an occlusion, anddiscussed its possible clinical significance as well asthe role of segmental distribution by the vortex veinin its production. The findings strongly suggest thatinterference with the vortex vein circulation (andits segmental distribution) could play an importantrole in the pathogenesis of some of the majorcomplications of retinal detachment surgery-forexample, glaucoma, anterior uveitis, ischaemiaand necrosis of the anterior segment, and choroidaland intraocular haemorrhages. Experimental vortexvein occlusion produced in all eyes a thick flare orthick gelatinous deposit in the anterior chamberand hyperaemia of the iris (this mimics perfectlythe non-granulomatous iritis of sudden onset),and in some eyes hyphaema.
SummaryThe various in vivo studies on posterior ciliaryarteries and choroidal vasculature reported piece-meal by the author over the past few years have nowbeen collated. A coherent picture of the vasculatureemerges which is of considerable clinical signifi-cance. The observations show that the posteriorciliary arteries and their branches right down to theterminal choroidal arterioles, the choriocapillaris,and the vortex veins have a segmental distribution
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

Segmental nature of the choroidal vasculature 647
in the choroid, and that the posterior ciliary arteries significance of this segmental distribution of theand choroidal arteries function as end-arteries. uveal vasculature is discussed.No special macular artery supplying the submacular It is a pleasure to acknowledge the help of my wife,choroid has been found. The posterior ciliary Shelagh, in the preparation of the manuscript and of Mrarteries not only supply the choroid but are also Lee Allen for drawing Figs 7, io, and I2, and of Msthe main source of blood supply to the anterior Vicky Dingman for secretarial assistance. Figures 7-IIpart of the optic nerve, and have an important role are reproduced by courtesy of the editor of Albrechtin the blood supply of the retina. The clinical v. Graefes Archiv fur Ophthalmologie.
ReferencesALAJOUANINE, T., CASTAIGNE, P., LHERMITTE, F., CAMBIER, j., and GAUTIER, J. c. (1959) Sem. H6p. Paris, 35, 1149ALM, A., and BILL, A. (1970) Acta physiol. scand., 8o, I9AMALRIC, P. (I97I) Trans. ophthal. Soc. U.K., 91, 305
(I973) Trans. Amer. Acad. Ophthal. Otolaryng., 77, OP-29IANDERSON, D. R., and DAVIS, E. B. (1974) Arch. Ophthal. (Chicago), 92, 422BLACKWOOD, W., MCMENEMEY, W. H., MEYER, A., NORMAN, R. M., and RUSSELL, D.S. (I963) In 'Greenfield's Neuro-
pathology', p. 260. Williams & Wilkins, BaltimoreCOHAN, B. E., and COHAN, S. B. (1963) Amer. J. Physiol., 205, 6oDOLLERY, C. T., HENKIND, P., KOHNER, E. M., and PATERSON, J. W. (I968) Invest. Ophthal., 7, 191DUKE-ELDER, S. (I96I) In 'System of Ophthalmology', vol. 2, pp. 339, 346, 35I. Kimpton, LondonEICH, j., and WIEMERS, K. (1950) Dtsch. Z. Nervenheilk., I64, 537ELGIN, S. S. (1964) Invest Ophthal., 3, 417FOULDS, W. S., LEE, W. R., and TAYLOR, W. O. G. (1971) Trans. ophthal. Soc. U.K., 91, 323GASS, J. D. M. (I968) Arch. Ophthal. (Chicago), 8o, 177GOLDER, H., and GAY, A. J. (I967) Invest. Ophthal., 6, 51HAYREH, S. S. (I962) Brit. J. Ophthal., 46, 212
(I963a) Ibid., 47, 71(I963b) Ibid., 47, 65I(1964) Exp. Eye Res., 3, i6(I969) Brit. J. Ophthal., 53, 721(1970) Ibid., 54, 289(I973a) Exp. Eye Res., 17, 387(1973b) Trans. Amer. Acad. Ophthal. Otolaryng., 77, OP-300(1974a) Ibid., 78, OP-240(1974b) v. Graefes Arch. Ophthal., x92, I65(1974c) Ibid., x92, I8i(1974d) Ibid., 192, 197(1974e) Brit. J7. Ophthal., 58, 391(1974f) Ibid., 58, 955(1974g) Ibid., 58, 964(I975) In 'Anterior Ischemic Optic Neuropathy'. Springer-Verlag, New Yorkand BAINES, J. A. B. (1972a) Brit. J. Ophthal., 56, 719
(1972b) Ibid., s6, 736- ~~~(1972C) Ibid., 56, 754-(I973) Ibid., 57, 217
HENKIND, P. (1967) Invest. Ophthal., 6, 56(I974) Personal communicationCHARLES, N. C., and PEARSON, J. (1970) Amer. 7. Ophthal., 69, 78
HEPBURN, M. L. (I912) Trans. ophthal. Soc. U.K., 32, 36I(I935) Ibid., S5, 434
HOGAN, M. j., and ALVARADO, J. A., and WEDDELL, J. E. (1971) In 'Histology of the Human Eye', p. 372.Saunders, Philadelphia
KREY, H. F. (I975) Amer. J. Ophthal., 80, I98KRILL, A. E., and KLIEN, B. A. (1965) Arch. Ophthal. (Chicago), 74, 496LEBER, T. (1903) Die Circulations- und Emrnhrungsverhiiltnisse des Auges, in 'Graefe-Saemisch: Handbuch der
gesamten Augenheilkunde', Bd. 2, Abt. 2, pp. 33-35, 43-46. Engelmann, LeipzigLINDENBERG, R., and SPATZ, H. (1940) Virchows Arch. path. Anat., 305, 531MEYER, F. (I887) Morph. Jb., X2, 414MEYER, J. E. (I953) Arch. Psychiat. Nervenkr., I90, 328MEYER, J. S. (I96I) In 'Pathogenesis and Treatment of Cerebrovascular Disease', ed. W. S. Fields, p. 8o.Thomas, Springfield, Ill.
, FANG, H. C., and DENNY-BROWN, D. (1954) Arch. Neurol. Psychiat. (Chic.), 72, 296
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from

648 British Journal of Ophthalmology
NEWELL, F. W. (1975) 'Variants of flecked retina syndrome', presented at ioth Congreso Pan Americano deOftalmologian, San Juan, Puerto Rico
NORMAN, R. M., URICH, H., and MCMENEMEY, W. H. (1957) Brain, So, 49
PILKERTON, R., BULLE, P. H., and o'RoURKE, J. (1964) Invest. Ophthal., 3, 237RING, H. G., and FUJINO, T. (i967) Arch. Ophthal. (Chicago), 78, 431ROHEN, j. w. (1965) Int. Ophthal. Clin., 5, 58ISCHNEIDER, M. (I956) Therapievoche, 6, 217TORCZYNSKI, E., and TSo, M. o. (1974) Abstracts, Ass. Res. Vision Ophthal., Spring Meeting Sarasota, FloridawEITER, j. j., and ERNEST, J. T. (I974) Amer. Y. Ophthal., 78, 583WOLFF, E. (I948) In 'The Anatomy of the Eye and Orbit', p. 68-72. Lewis, LondonWYBAR, K. C. (x954a) J. Anat. (Lond.), 88, 94
(I954b) Brit. J. Ophthal., 38, 513ZULCH, K. J. (I953) Zbl. allg. Path. path. Anat., 90, 402
and BEHREND, R.C.H. (I96I) In 'Cerebral Anoxia and the Electroencephalogram', ed. H. Gastaut andJ. S. Meyer, p. I44. Thomas, Springfield, Ill.
copyright. on F
ebruary 11, 2020 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.59.11.631 on 1 Novem
ber 1975. Dow
nloaded from



![Unilateral Choroidal Osteoma with Choroidal Neovascularization...Surgical evacuation of the choroidal neovascular membrane has been reported [12] but the visual outcome was not favorable.](https://static.fdocuments.us/doc/165x107/6053732923e31173be575e28/unilateral-choroidal-osteoma-with-choroidal-neovascularization-surgical-evacuation.jpg)