
Secondary progressive multiple sclerosis: current knowledge and future challenges
12
http://neurology.thelancet.com Vol 5 April 2006 343 Introduction During the past decade, the advent of disease-modifying treatments has substantially changed the work-up of relapsing remitting multiple sclerosis (MS). Early treatment initiation is now recommended to maximise the efficacy of currently available therapies, which are known to mainly act against the inflammatory components of MS. By contrast, understanding and treatment of the progressive phase of MS, which is characterised by the steady accumulation of fixed disability, is suboptimum. Clinical and paraclinical predictors of a transition from an initial relapsing remitting phase to a secondary progressive course have little prognostic value. Moreover, the immunological and pathological substrates of secondary progressive MS are poorly defined. With respect to neuroimaging aspects, conventional MRI seems to lose sensitivity for monitoring the secondary progressive phase of MS and more specific in-vivo markers of neurodegeneration are needed for a reliable assessment of putative new treatment options. This review aims to critically summarise and provide a background for the planning of future studies and therapeutic trials of secondary progressive MS. Clinical aspects Consensus definition of secondary MS progression During the relapsing remitting phase of MS, neurological sequelae from relapses can persist but, by definition, they are stable—ie, do not worsen between the episodes of acute neurological dysfunction. The word progression denotes the continuous worsening of neurological impairment over at least 6 or 12 months. 1–5 The date of onset of MS progression is difficult to define and is usually assessed retrospectively once the duration of continuous neurological worsening has been established. When the initial relapsing remitting phase is followed by a transition to the progressive phase, the disease is named secondary progressive MS. To standardise the terminology used in the description of MS clinical phenotypes, an international panel of experts defined secondary progressive MS as an “initial relapsing remitting disease course followed by progression with or without occasional relapses, minor remissions, and plateaus”. 6 Overall, in a representative population of patients with MS, onset of disease is of the relapsing remitting type in 85% of patients. 6 In MS surveys, the higher the duration of the follow-up, the higher the proportion of cases with a relapsing remitting onset who will have converted to secondary progressive MS. Epidemiology Thanks to the numerous available long-term natural history studies, 7 knowledge of the onset of progression in MS is evidence based. McAlpine and Compston 8 first showed clearly that “there is a fairly constant rate of change from a remitting to a progressive course, and that there is a gradual rise in the total percentage of progressive cases as the disease advances”. A similar progression has been proven in series in Lyon, France, 9–11 and in Gothenburg, Sweden. 12,13 As estimated by survival analysis, the median time to secondary progression in MS patients with a relapsing remitting onset in the Lyon series was 19·1 years, with a mean yearly rate of 2·5% of relapsing remitting patients converting to secondary progressive MS. 11 In a Canadian series, 14 however, 30–40% of patients with an initial relapsing remitting course developed secondary progressive MS within 10 years from disease onset, with a median time to conversion of between 10 and 15 years. For patients presenting with a distinct clinically isolated syndrome, the median time to onset of secondary progression was 19·0 years in the Gothenburg series. 13 Consistent results have been reported in other Italian 15 and Swedish 16 series. Thus a reasonable estimate of the median time from relapsing remitting MS onset to secondary progression is about 19 years. 7 Age at onset is the strongest predictor of the conversion to secondary progressive disease: the older Secondary progressive multiple sclerosis: current knowledge and future challenges Marco Rovaris, Christian Confavreux, Roberto Furlan, Ludwig Kappos, Giancarlo Comi, Massimo Filippi The secondary progressive phase of multiple sclerosis (MS), which is characterised by a steady accrual of fixed disability after an initial relapsing remitting course, is not clearly understood. Although there is no consensus on the mechanisms underlying such a transition to the progressive phase, epidemiological and neuroimaging studies indicate that it is probably driven by the high prevalence of neurodegenerative compared with inflammatory pathological changes. This notion is lent support by the limited efficacy of available immunomodulating and immunosuppressive treatment strategies, which seems to be further decreased in the late stages of secondary progressive MS. No established clinical or paraclinical predictors of the transition from relapsing remitting to secondary progressive MS have been described. However, the use of quantitative MRI-derived measures is warranted to monitor natural history studies and therapeutic trials of secondary progressive MS with increased reliability. In view of the small effects of immunomodulating and immunosuppressive treatments in preventing the transition to secondary progression, the development of treatments promoting neuroaxonal repair remains an important goal in this disease. Lancet Neurol 2006; 5: 343–54 Neuroimaging Research Unit (M Rovaris MD, M Filippi MD), Department of Neurology (M Rovaris MD, R Furlan MD, G Comi MD, M Filippi MD), and Neuroimmunology Research Unit (R Furlan MD), Scientific Institute and University Ospedale San Raffaele, Milan, Italy; Department of Neurology and EDMUS Coordinating Center, Hôpital Neurologique Pierre Wertheimer, Université Claude Bernard, Lyon, France (C Confavreux MD); and Department of Neurology and Research, University Hospital, Basel, Switzerland (L Kappos MD) Correspondence to: Dr Massimo Filippi, Neuroimaging Research Unit, Scientific Institute and University Ospedale San Raffaele, Via Olgettina 60, 20132 Milan, Italy fi[email protected] Review
-
Upload
marco-rovaris -
Category
Documents
-
view
213 -
download
0
Transcript of Secondary progressive multiple sclerosis: current knowledge and future challenges
http://neurology.thelancet.com Vol 5 April 2006 343
IntroductionDuring the past decade, the advent of disease-modifying treatments has substantially changed the work-up of relapsing remitting multiple sclerosis (MS). Early treatment initiation is now recommended to maximise the effi cacy of currently available therapies, which are known to mainly act against the infl ammatory components of MS. By contrast, understanding and treatment of the progressive phase of MS, which is characterised by the steady accumulation of fi xed disability, is suboptimum. Clinical and paraclinical predictors of a transition from an initial relapsing remitting phase to a secondary progressive course have little prognostic value. Moreover, the immunological and pathological substrates of secondary progressive MS are poorly defi ned. With respect to neuroimaging aspects, conventional MRI seems to lose sensitivity for monitoring the secondary progressive phase of MS and more specifi c in-vivo markers of neurodegeneration are needed for a reliable assessment of putative new treatment options. This review aims to critically summarise and provide a background for the planning of future studies and therapeutic trials of secondary progressive MS.
Clinical aspectsConsensus defi nition of secondary MS progressionDuring the relapsing remitting phase of MS, neurological sequelae from relapses can persist but, by defi nition, they are stable—ie, do not worsen between the episodes of acute neurological dysfunction. The word progression denotes the continuous worsening of neurological impairment over at least 6 or 12 months.1–5 The date of onset of MS progression is diffi cult to defi ne and is usually assessed retrospectively once the duration of continuous neurological worsening has been established. When the initial relapsing remitting phase is followed by a transition to the progressive phase, the disease is named secondary progressive MS. To standardise the terminology used in the description of MS clinical
phenotypes, an international panel of experts defi ned secondary progressive MS as an “initial relapsing remitting disease course followed by progression with or without occasional relapses, minor remissions, and plateaus”.6 Overall, in a representative population of patients with MS, onset of disease is of the relapsing remitting type in 85% of patients.6 In MS surveys, the higher the duration of the follow-up, the higher the proportion of cases with a relapsing remitting onset who will have converted to secondary progressive MS.
EpidemiologyThanks to the numerous available long-term natural history studies,7 knowledge of the onset of progression in MS is evidence based. McAlpine and Compston8 fi rst showed clearly that “there is a fairly constant rate of change from a remitting to a progressive course, and that there is a gradual rise in the total percentage of progressive cases as the disease advances”. A similar progression has been proven in series in Lyon, France,9–11 and in Gothenburg, Sweden.12,13 As estimated by survival analysis, the median time to secondary progression in MS patients with a relapsing remitting onset in the Lyon series was 19·1 years, with a mean yearly rate of 2·5% of relapsing remitting patients converting to secondary progressive MS.11 In a Canadian series,14 however, 30–40% of patients with an initial relapsing remitting course developed secondary progressive MS within 10 years from disease onset, with a median time to conversion of between 10 and 15 years. For patients presenting with a distinct clinically isolated syndrome, the median time to onset of secondary progression was 19·0 years in the Gothenburg series.13 Consistent results have been reported in other Italian15 and Swedish16 series. Thus a reasonable estimate of the median time from relapsing remitting MS onset to secondary progression is about 19 years.7
Age at onset is the strongest predictor of the conversion to secondary progressive disease: the older
Secondary progressive multiple sclerosis: current knowledge and future challengesMarco Rovaris, Christian Confavreux, Roberto Furlan, Ludwig Kappos, Giancarlo Comi, Massimo Filippi
The secondary progressive phase of multiple sclerosis (MS), which is characterised by a steady accrual of fi xed disability after an initial relapsing remitting course, is not clearly understood. Although there is no consensus on the mechanisms underlying such a transition to the progressive phase, epidemiological and neuroimaging studies indicate that it is probably driven by the high prevalence of neurodegenerative compared with infl ammatory pathological changes. This notion is lent support by the limited effi cacy of available immunomodulating and immunosuppressive treatment strategies, which seems to be further decreased in the late stages of secondary progressive MS. No established clinical or paraclinical predictors of the transition from relapsing remitting to secondary progressive MS have been described. However, the use of quantitative MRI-derived measures is warranted to monitor natural history studies and therapeutic trials of secondary progressive MS with increased reliability. In view of the small eff ects of immunomodulating and immunosuppressive treatments in preventing the transition to secondary progression, the development of treatments promoting neuroaxonal repair remains an important goal in this disease.
Lancet Neurol 2006; 5: 343–54
Neuroimaging Research Unit (M Rovaris MD, M Filippi MD), Department of Neurology (M Rovaris MD, R Furlan MD, G Comi MD, M Filippi MD), and Neuroimmunology Research Unit (R Furlan MD), Scientifi c Institute and University Ospedale San Raff aele, Milan, Italy; Department of Neurology and EDMUS Coordinating Center, Hôpital Neurologique Pierre Wertheimer, Université Claude Bernard, Lyon, France (C Confavreux MD); and Department of Neurology and Research, University Hospital, Basel, Switzerland (L Kappos MD)
Correspondence to: Dr Massimo Filippi, Neuroimaging Research Unit, Scientifi c Institute and University Ospedale San Raff aele, Via Olgettina 60, 20132 Milan, Italyfi [email protected]
Review

Review
344 http://neurology.thelancet.com Vol 5 April 2006
the patient at onset, the shorter the time to onset of progression.10,11,13,17–21 Male sex has been associated with a shorter time to progression than female sex in many series,11,13,17,18,20 but not in others.8,10,15,19,21 With respect to initial symptoms, most series reported that visual or sensory and sometimes brainstem-related symptoms are associated with an increased time to secondary progression, whereas spinal-cord-related symptoms are associated with a diminished time to evolution.11,13,17–20,22 An incomplete recovery from the initial exacerbation has consistently been associated with a reduced time to secondary progression.13,15,21 A shortened time from the clinical onset of MS to the second episode was shown to be predictive in some studies,10,11,21 but not in others.13,15 The number of relapses during the fi rst 2–5 years of disease was shown to be inversely related to the time to secondary progression in some studies,17,18 but not in others.13,15,21 A Norwegian study showed that the higher the disability score or the number of aff ected functional systems 5 years after the onset of MS, the shorter the time to progression.13
Among the 1844 patients of the Lyon Natural History MS cohort, 27% were classifi ed as having secondary progressive MS at the time of the survey. To investigate the dynamics of clinical MS progression, three robust landmarks of disability were assessed: disability status scale (DSS)23 score 4 (walking without aid and a limited walking distance but exceeding 500 m without rest), score 6 (walking with unilateral support and a walking distance not exceeding 100 m without rest), and score 7 (home restriction, a few steps still being possible while holding onto a wall or furniture but not exceeding 10 m without rest). In this cohort, the median times to reach irreversible disability from MS onset, as estimated by survival analysis, were 6·1 years for DSS 4, 12·5 years for DSS 6, and 19·1 years for DSS 7. The same cohort study showed that the median times to reach these disability scores from the onset of the disease were signifi cantly shorter in patients with primary progressive MS.24 By contrast, the time course of disability accumulation during the progressive phase of the disease was more rapid in secondary progressive MS than in primary progressive MS.25 This fi nding is in agreement with those from other series.26–28 In the London Ontario cohort, the median survival time from onset of progression to reach DSS 6 was 5·5 years in patients with secondary progessive MS and 9·5 years in those with primary progressive MS.27,28 However, in the Gothenburg cohort,20 the median survival time from the onset of progression to DSS 6 was about 5 years and was not signifi cantly diff erent between secondary progressive MS and primary progressive MS. In the Lyon MS cohort,24 the progression of irreversible disability from DSS 4 to DSS 6 was closely similar, whether relapses occurred or not. In these patients, however, the time from score 4 to score 7, as well as the time from score 6 to score 7, were longer when relapses occurred during the progression. In any case, the speed
of progression from DSS 4 to DSS 6 seems to have a wide interpatient variability and its predictors are still unknown.
ImmunopathologyThe immunopathological characteristics of the transition from relapsing remitting MS to secondary progressive MS have been poorly investigated. A debated concept is whether the progressive phase is associated with the decrease in infl ammatory and demyelinating processes, which are substituted by neurodegenerative features. Few pathological studies have focused on patients with secondary progressive MS.29,30 The most relevant fi nding in these reports is an unusual type of demyelination characterised by slowly expanding plaques with foamy macrophages containing lipids, especially in periplaque white matter. The description of absent or modest perivascular cuff s in the lesions, but the presence of lymphocytes and plasma cells in the periplaque white matter, is consistent with reduced infl ammatory activity in and around lesional areas,30 although the activity is more prominent than in primary progressive MS.29 Very scarce elements of an ongoing neurodegenerative process are available in these reports, although Wallerian degeneration and other axonal alterations are reported in the spinal cord.30 More recently, Kutzelnigg and colleagues31 did a pathological study on a series of more than 50 patients, of whom 20 had secondary progressive MS. In this study, several distinguishing characteristics of secondary progressive MS have been described. Demyelination in the cerebral cortex, diff use injury in the form of focal axonal swelling and axonal end bulbs, and diff use rather than focal infl ammation (defi ned as diff use T-lymphocyte infi ltration and microglial activation) were shown to be signifi cantly increased in primary progressive MS and secondary progressive MS compared with relapsing remitting MS. Serafi ni and colleagues32 reported, in a very small group of patients, that ectopic lymphoid follicle-like structures containing B cells, T cells and plasma cells, and a network of follicular dendritic cells producing CXCL13 (a fi nding usually associated with chronic infl ammation) were present in the cerebral meninges of patients with secondary progressive MS, but not in those with relapsing remitting MS and primary progressive MS. The results of these studies seem to indicate that infl ammatory characteristics remain an important aspect of pathological changes in secondary progressive MS, albeit with diff erent patterns than in the relapsing remitting phase of the disease. Whether infl ammation could completely burn out during the latest stages of secondary progressive MS, as suggested by evidence from neuroimaging studies and treatment trials, needs to be established.
The underlying immunological mechanisms that parallel the evolution from relapsing remitting to secondary progressive MS are diffi cult to identify on the basis of these pathlogical data alone. Furthermore,
Review
http://neurology.thelancet.com Vol 5 April 2006 345
available data can seem to contrast with the assumption that infl ammation is decreased in secondary progressive MS. Interleukin 10 has been shown to be decreased and interleukin 12p40 to be upregulated in supernatants of peripheral blood mononuclear cells from patients with secondary progressive MS compared with those with relapsing remitting MS.33 According to the Th1/Th2 paradigm this fi nding is not suggestive of reduced proinfl ammatory activity. Other studies have described an increase in CCR2+ cells and a decrease in CCR5+ cells in patients with secondary progessive MS compared with those with relapsing remitting MS. These fi ndings have been interpreted as a possible Th2 shift occurring in secondary progressive MS.34,35 In a study that compared the concentration of mRNA in peripheral blood mononuclear cells from a large population of patients with MS, signifi cantly (p<0·005) increased expression of IL-1α, IL-5, IL-10, TNFβ, and CXCL10, and signifi cantly decreased expression of CCL5, CCR3, and CXCR5 were found in samples from patients with secondary progressive MS compared with those from clinically stable patients with relapsing remitting MS.36 These results cannot be clearly explained in terms of current knowledge on infl ammatory vs anti-infl ammatory patterns. Adhesion molecules LFA-1 and α4-integrin have been analysed on peripheral blood mononuclear cells from patients with MS and shown to be up-regulated in patients with secondary progressive MS compared with those with relapsing remitting MS.37 These fi ndings have been discussed by the authors in light of prominent disease activity in patients with secondary progressive MS, in parallel with the same type of rise in patients with relapsing remitting MS who are having a clinical relapse. In another study,38 proinfl ammatory cytokine concentrations were shown to be higher in female than in male patients with secondary progressive MS, whereas they did not diff er between men and women aff ected by relapsing remitting MS. This fi nding indicates that sex diff erences in cytokine profi les might be another immunological hallmark of the progressive phase of MS.
All these observations indicate that there is no consensus on the immunological mechanisms underlying the evolution from relapsing remitting MS to secondary progressive MS. This can be explained by the limitations of the available methods of investigation, which are inadequate in case of changes occurring in the target organ. The series of patients who are included in post-mortem studies are, in fact, hardly representative of the general MS population. On the other hand, investigations on peripheral blood mononuclear cells are limited by the fact that the blood stream can represent a mere traffi cking compartment in which pathogenically relevant lymphocyte subpopulations could be unevenly represented. Thus, the identifi cation of the immunological changes associated with the shift to secondary progressive MS will have to rely on new approaches, such as gene-expression microarrays and proteomics.
NeuroimagingConventional MRIThe average burden of brain T2-hyperintense lesions tends to be higher in patients aff ected by secondary progressive MS than in those with relapsing remitting or primary progressive MS.39-41 The load of focal spinal cord lesions was also shown to be higher in patients with secondary progressive MS than in those with relapsing remitting or primary progressive MS in some,41,42 but not in all studies.43 However, the correlations between locomotor disability and brain or cord T2 lesion loads in secondary progressive MS are generally null or weak.41,43,44 The number of gadolinium-enhancing lesions tends to decrease in patients with relapsing remitting MS as they enter the secondary progressive phase and becomes very low in advanced secondary progressive disease.45–47 However, this fi nding has not been confi rmed in other studies.48 The number of gadolinium-enhancing lesions on a baseline scan is a signifi cant predictor of subsequent MRI activity in both relapsing remitting and secondary progressive MS,49 but only modestly predicts the clinical evolution in the subsequent 2 years.50 On the other hand, the frequency of large51 and ring-enhancing52 lesions were shown to be correlated with subsequent expanded disability status scale (EDSS) worsening in patients with relapsing remitting MS, which suggests that specifi c
Figure 1: An illustrative example of lesion evolution to “black hole” in a patient with secondary progressive MSAn enhancing lesion (the scan on which the lesion enhances is shown on the left) appears hypointense to surrounding white matter at the fi rst scan after the enhancement (baseline scan; middle panel). After 6 months of follow-up, the signal intensity of the lesion is still hypointense compared with surrounding white matter (right panel). Reproduced with permission of the American Academy of Neurology.56

Review
346 http://neurology.thelancet.com Vol 5 April 2006
patterns of contrast enhancement might be predictors of an increased risk of unfavourable clinical evolution.
Several fi ndings indicating that a greater load of T1-hypointense lesions is the best discriminant between secondary progressive MS and relapsing remitting or primary progressive MS42,43,47,53–55 have not been confi rmed by other studies,40,41 possibly because of the known methodological limitations of T1 lesion count and volume measurement. Interestingly, however, a recent study56 comparing the evolution of newly formed gadolinium-enhancing lesions in patients with secondary progressive MS and relapsing remitting MS has shown a four-fold higher risk of black-hole development in the secondary progressive group (fi gure 1).
A greater severity of brain57–61 and cord42,62–66 atrophy is seen in secondary progressive MS than in benign or relapsing remitting MS, which signifi cantly correlates with the degree of neurological disability. By contrast with this fi nding, the rate of brain atrophy progression over short-term periods has been shown not to diff er among the various MS phenotypes.67,68 In confl ict with earlier reports,43 neither the severity of brain and cord atrophy nor their short-term progression rates were shown to diff er between secondary progressive and primary progressive MS in large-scale studies in which these two patient groups were matched for disease duration and disability.41,69,70 Preliminary evidence61 seems to indicate that the distribution patterns, rather than the overall rate, of brain atrophy might diff er between relapsing and progressive MS, being predominant in secondary progressive MS in the cortical and deep grey matter areas (fi gure 2).
Conventional MRI has been widely applied to monitor therapeutic trials of secondary progressive MS and proven to provide valid surrogate endpoints for disability progression (table).71 However, the consistent fi nding of a signifi cant treatment eff ect in reducing gadolinium-enhancing lesion frequency and T2-hyperintense lesion load accumulation72–75 was not accompanied by a comparable eff ect on T1-hypointense lesion load
accrual and brain atrophy.76–80 This lends support to the notion of a dissociation between the infl ammatory and neurodegenerative aspects during the secondary progressive phase of MS.
Quantitative MR-based techniquesQuantitative MR-based techniques have the potential for increased specifi city to the most destructive pathological characteristics of MS. Among these techniques, magnetisation transfer (MT) MRI,81 diff usion MRI,82 and T1 relaxation time measurements83 enable us to quantify the extent of structural changes both in T2-visible lesions and in tissue that appears normal on conventional MR images. Proton MR spectroscopy (¹H-MRS)84 can add information about the biochemical nature of such changes, with the potential to improve signifi cantly our ability to monitor infl ammatory demyelination and axonal injury.
Cross-sectional MT MRI studies of patients with secondary progressive MS40,41,55,85–87 have shown that normal-appearing brain tissues are damaged, as shown by a signifi cant decrease of the average MT ratio values when compared with those from healthy individuals and patients with less disabling disease phenotypes. The most compelling piece of evidence that a reduction of MT ratio values indicates severe tissue damage comes from post-mortem studies showing a strong correlation of MT ratio values from MS lesions and normal-appearing white matter with the percentage of residual axons and the degree of demyelination.88,89 The scarce correlations between MT MRI fi ndings and T2-visible lesion load or brain volume indicate that damage to normal-appearing brain tissue in secondary progressive MS does not merely depend on the degeneration of fi bres that pass through macroscopic lesions. Longitudinal MT MRI studies have shown that newly-enhancing lesions from patients with secondary progressive MS had lower MT ratio values at the time of their appearance and presented a more severe and signifi cant MTR reduction during the follow-up than did those from patients with relapsing remitting disease.85,90 The 1-year changes of metrics derived from the histogram analysis of brain MT ratio maps were more prominent in patients with secondary progressive MS than in those with relapsing remitting disease.85 That MT MRI is sensitive to the accrual of brain pathology in secondary progressive MS accords with the results of a subcohort analysis from a clinical trial.91 MT MRI studies of the cervical cord showed that MTR abnormalities were more pronounced in secondary progressive MS than in relapsing remitting disease.92,93 Another study comparing cervical cord MT MRI fi ndings from patients with secondary progressive MS and primary progressive MS showed no signifi cant diff erences (fi gure 3).41
Several diff usion MRI studies94–99 have achieved confl icting results when comparing secondary pro-gressive MS with the other disease phenotypes. Only two histogram-based studies95,98 showed that water
Figure 2: Colour-coded areas of brain atrophy development in secondary progressive MS overlaid on a template T1-weighted imageInvolvement of the bilateral anterior orbital gyrus and left mammillary body (A). Involvement of the caudate nuclei; left middle temporal gyrus; left thalamus; and frontal, parietal, temporal, and occipital region (B). Involvement of the cingulate sulcus and regions of frontal and parietal cortex (C). Reproduced with permission of the American Society of Neuroradiology.61

Review
http://neurology.thelancet.com Vol 5 April 2006 347
diff usivity and anisotropy abnormalities of the whole brain were signifi cantly more pronounced in secondary progressive MS than in relapsing remitting MS. Bozzali and colleagues,100 using diff usion MRI and brain tissue segmentation techniques, showed that grey matter changes are more pronounced in patients with secondary progressive MS than in those with relapsing remitting MS. Rovaris and colleagues69,70 also showed that the diff usion abnormalities of T2-visible lesions, normal-appearing white matter, and grey matter are more severe in patients with secondary progressive MS than in those with primary progressive disease. On the other hand, a 1-year follow-up study70 has shown a signifi cant increase of water diff usivity in lesions and grey matter of patients with secondary progressive and primary progressive MS compared with baseline. This fi nding suggests that progressive grey matter damage might yet be an additional factor leading to the accumulation of disability in progressive MS. Recent advances in diff usion MRI acquisition and post-processing have made the study of the cervical cord feasible. In the cervical cord of patients with secondary progressive disease, water diff usivity and tissue anisotropy are abnormal and these abnormalities tend to be of a greater magnitude than in relapsing remitting disease.66 When comparing various MRI-derived metrics, cervical cord diff usion parameters showed the strongest relation with patients’ motor disability.66
In a study that used T1 relaxation time measure-ments,101 both normal-appearing white matter and grey matter T1 relaxation time histogram-derived parameters showed greater abnormalities in patients with secondary progressive MS than in those with relapsing remitting MS. However, grey matter T1 histogram peak location was the strongest predictor of disability in patients with secondary progressive MS together with a measure of brain atrophy. In the cervical cord of MS patients,102 T1 relaxation time was shown to be signifi cantly prolonged compared with controls, with signifi cantly higher values in secondary progressive MS than in relapsing remitting MS. Signifi cant correlations between cord T1 relaxation time values, patients’disability, and cord atrophy were also shown.
¹H-MRS-measured N-acetyl aspartate (NAA) is known to be associated with neuronal and axonal viability.103 Early studies104,105 reported a marginal diff erence between secondary progressive and relapsing remitting MS in the NAA concentrations of normal-appearing white matter. Other cross-sectional studies106–109 noted lower NAA concentrations in secondary progressive MS than in relapsing remitting MS or benign MS and moderate correlations with the severity of neurological disability. More recently, Adalsteinsson and colleagues110 showed that in grey matter, and not normal-appearing white matter, NAA concentrations diff ered between secondary progressive and relapsing remitting MS. These diff erences among studies could be indicative of
known variability of 1H-MRS measurements related to methodological issues. However, in a study by Vrenken and colleagues,111 only the ratio between NAA and creatine was signifi cantly lower in the normal-appearing white matter from patients with MS than in the controls, without diff erences among the various MS phenotypes; whereas, the absolute concetrations of NAA were similar in patients and healthy individuals. The authors conclude that, in the normal-appearing white matter of patients with secondary progressive MS and other courses of MS, increased glial activity, as shown by increased creatine concentrations, can occur without axonal dysfunction.
Functional MRICortical activations during motor, sensory, or cognitive tasks can be interrogated with functional MRI (fMRI). In patients with MS112–114 a reorganisation of the motor network has been described, which could account for the small association between structural pathology and levels of disability. Such a reorganisation is especially extensive and widespread in primary progressive MS115,116 and its degree is highly correlated with the severity of damage to normal-appearing brain tissue. Only one study116 has electively investigated the fMRI pattern of cortical activations during simple motor tasks in patients with secondary progressive MS compared with healthy individuals. Similar to what was described in patients with primary progressive MS who had high levels of
Technique Summary fi ndings in SPMS Interpretation
T2-weighted MRI Greater lesion load than in RRMS and PPMSWeak correlation with disability
Refl ects the accrual of pathologically heterogeneous macroscopic lesions without a phenotype-specifi c pattern
Gadolinium-enhanced MRI Lesser frequency and amount of active lesions than in RRMS (controversial)
Prevalence of neurodegeneration over infl ammation Persistence of “low-burning” grade, MRI-undetectable infl ammatory processes?
T1-weighted MRI “Black hole” load best discriminant between SPMS and other MS phenotypesImproved correlation with disability (controversial)
Suboptimum reliability of this approachInability to quantify tissue damage within macroscopic lesions and in the NABT
Brain and cord atrophy measurement
More severe and faster rate of accumulation than in RRMSSimilarity with PPMSImproved correlation with disability
Atrophy refl ects the fi nal outcome of neurodegenerationMay lose sensitivity in the later stages of SPMS
Magnetisation transfer MRI More pronounced abnormalities within lesions than in RRMSDiff use and severe NABT damageDetectable short-term changes
NABT damage contributes to disability progressionMT MRI is a potentially useful tool to monitor SPMS trial
Diff usion MRI More pronounced GM damage than in RRMS and PPMS, with signifi cant short-term worsening
GM damage seems to be an important feature of progressive MS
Proton MR spectroscopy More severe neuroaxonal dysfunction than in RRMS (controversial)Strong correlations with disability
Axonal damage underlies MS irreversible disability
Functional MRI Activation of a widespread sensorimotor network for simple motor tasks
The failure of compensatory mechanisms may be a key aspect of MS progression
SPMS=secondary progressive MS; RRMS=relapsing remitting MS; PPMS=primary progressive MS; NABT=normal-appearing brain tissue; MT MRI=magnestisation transfer MRI; GM=grey matter.
Table: Neuroimaging features of secondary progressive MS

Review
348 http://neurology.thelancet.com Vol 5 April 2006
physical disability,114,115 the activation of a widely distributed sensorimotor network was reported in patients with secondary progressive MS, with the recruitment of several cortical and subcortical areas, which might help to limit the functional consequences of tissue injury (fi gure 4). In another cross-sectional study117 that compared patients with diff erent MS disease phenotypes by use of a simple motor task, those with secondary progressive MS showed an increased activation of several regions, mostly located in the frontal and parietal lobes, when compared with patients with relapsing remitting MS and mild disability. Thus, the failure of fi rst-line compensatory mechanisms could, at least in part, explain the accrual of disability reported in progressive MS.
TreatmentInterferon-betaFour large-scale, double-blind, randomised, placebo-controlled studies assessing the eff ectiveness of inter-feron beta in patients with secondary progressive MS have yielded controversial results. The European multi center trial on interferon beta-1b in SPMS (EUSPMS)118 enrolled 718 patients who were treated with either interferon beta-
1b or placebo for up to 3 years. The primary outcome was the time to confi rmed disability progression, as measured by an increase in EDSS23 sustained for at least 3 months. This progression was shown to be signifi cantly delayed (p=0·007) in treated patients. The proportion of patients with either progression or relapses decreased by nearly 30% in the treated group. Subgroup analysis suggested that patients with high prestudy disease activity had a pronounced eff ect from treatment.118–120 Additional analyses indicated that treatment with interferon beta-1b had also a signifi cant positive eff ect on patients’ health-related quality of life.121 MRI results from the trial showed that interferon beta-1b did not signifi cantly prevent cerebral atrophy, but it reduced the development of T1-hypointense lesions.44,77
In the SP Effi cacy Trial of Rebif (interferon beta-1a) in MS (SPECTRIMS), 618 patients received interferon beta-1a (22 µg or 44 µg) or placebo subcutaneously three times per week for 3 years.122 The primary outcome, time to confi rmed progression in disability, was not signifi cantly aff ected by active treatment. However, the relapse rate was signifi cantly reduced by active treatment. Signifi cant eff ects were also seen on other exacerbation-related outcomes and on a composite measure incorporating fi ve separate clinical and MRI outcomes. The hazard ratio for time to progression for the combined interferon beta-1a groups compared with placebo was 0·74 in patients with prestudy relapses (p=0·055) and 1·01 for those without (p=0·934). Exploratory post-hoc analyses suggested greater benefi t in women and in patients who had reported more than one relapse in the 2 years before the study. However, the latter eff ect did not achieve statistical signifi cance. Interferon beta-1a treatment signifi cantly reduced the median numbers of active lesions per patient per scan and the accumulation of T2 lesion load.75
In the North American Study of interferon beta-1b in secondary progressive MS (NASPMS),123 939 patients were randomly assigned placebo, an interferon beta-1b dose of 8 million IU, or an interferon beta-1b dose adjusted for bodyweight and size (5 million IU/m²). Each treatment was administered every other day. The primary endpoint was time to confi rmed progression of disability defi ned as an EDSS increase sustained for 6 months or more. This study was stopped early because of a lack of effi cacy. However, the relapse rate was signifi cantly lower for patients who received interferon beta than for those receiving placebo, and total T2 lesion volume increased by 11% in the placebo group compared with only 0·4% for the 8 million IU group and 0·8% for the 5 million IU/m² group. The number of new gadolinium-enhancing lesions was reduced by 64% and 76% in the two active treatment groups.123
The eff ectiveness of interferon beta-1a in the treatment of patients with secondary progressive MS has also been assessed in the International MS SP Avonex Clinical Trial (IMPACT) study.124 This trial included 436 patients, who were randomised to receive interferon beta-1a (60 µg) or
0
10
20
30
40
50
60
70
0 10 20 30 40 50 60 70 80MT ratio (%)
Nor
mal
ised
pixe
l cou
nt
Healthy patientsPrimary progressive MSSecondary progressive MS
Figure 3: Average MT ratio histograms of the cervical cord The histograms from patients with primary progressive and secondary progressive MS are almost overlapped. Reproduced with permission of Oxford University Press.41
Figure 4: Relative cortical activations in right-handed patients with secondary progressive MS during the performance of a simple motor task with their functionally normal right hand Compared with healthy volunteers, patients showed increased recruitment of the ipsilateral inferior frontal gyrus (A), middle frontal gyrus bilaterally (B, C), and contralateral infraparietal sulcus (C). Reproduced with permission of Elsevier.116
Review
http://neurology.thelancet.com Vol 5 April 2006 349
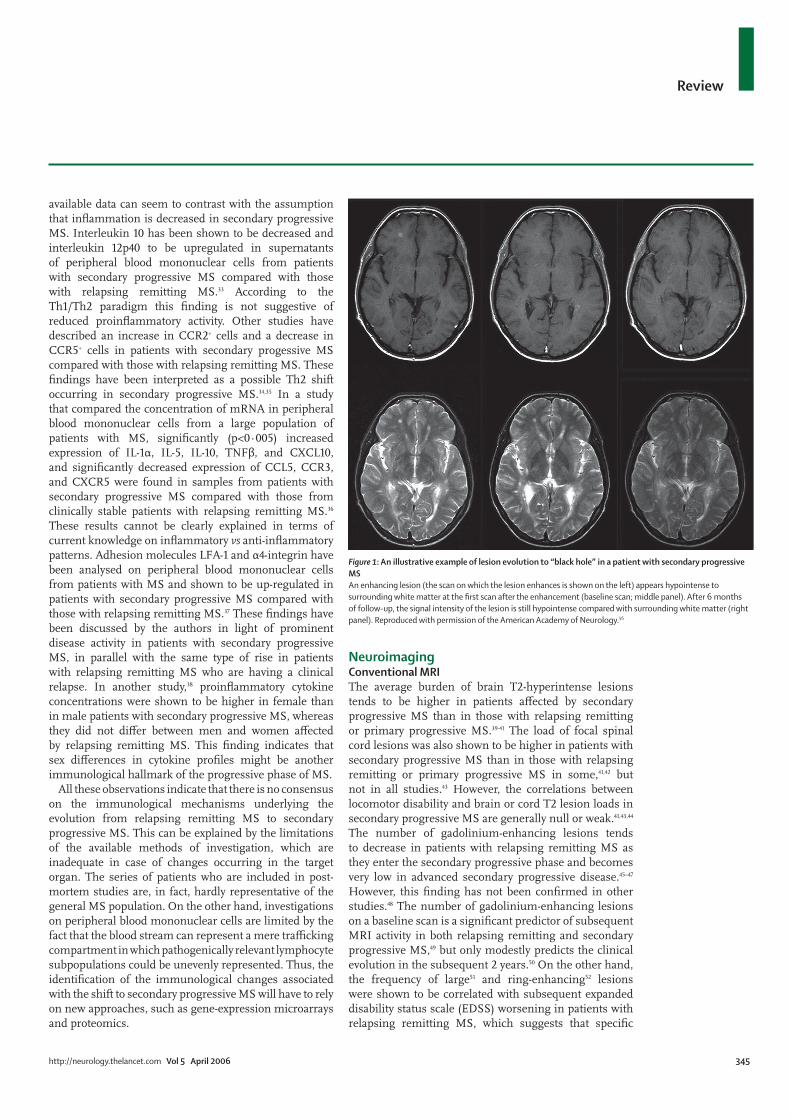
placebo by weekly intramuscular injection for 2 years. The primary outcome measure was baseline to month 24 change in the MS functional composite (MSFC). At the end of follow-up, the change in median MSFC Z score was reduced by 40·4% in the patients who received interferon beta-1a compared with those treated with placebo (p=0·033). Active treatment had no signifi cant eff ect on EDSS, but patients treated with interferon beta-1a did have 33% fewer relapses (p=0·008), and there was a signifi cant benefi t of active treatment on eight of 11 MS quality-of-life inventory subscales. New or enlarging T2-hyperintense lesions and gadolinium-enhancing lesions were signifi cantly reduced at months 12 and 24 in patients who received inteferon beta-1a.
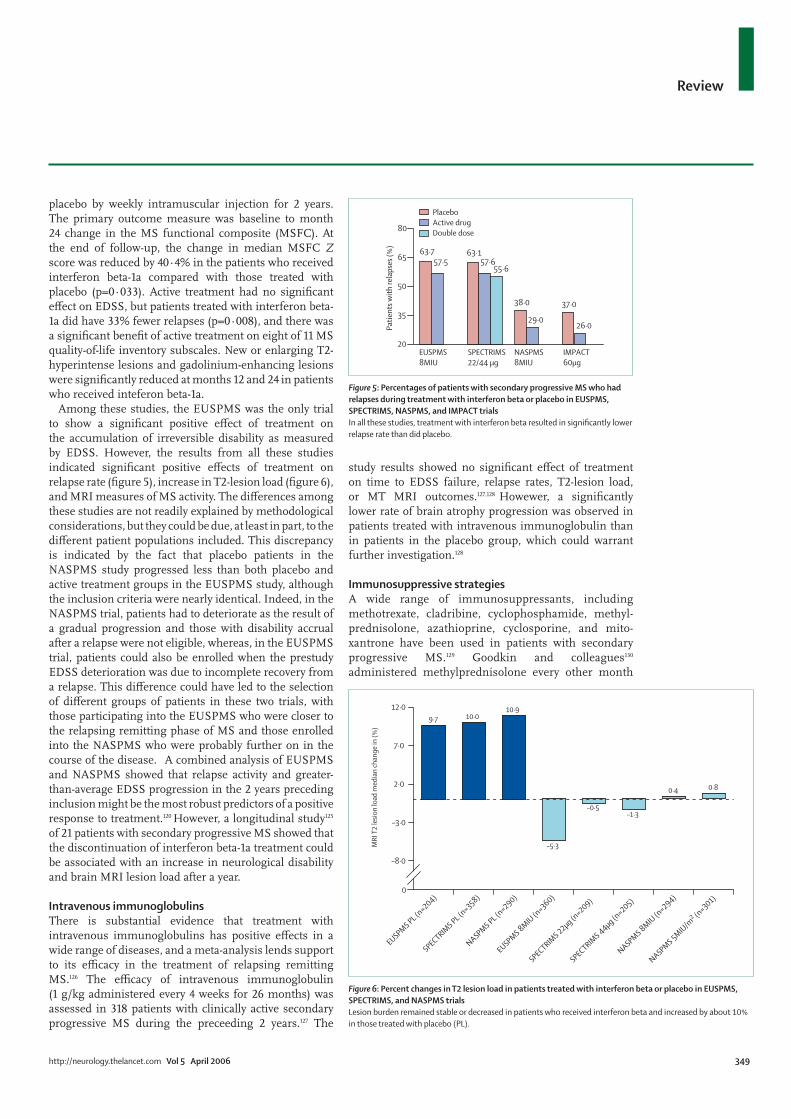
Among these studies, the EUSPMS was the only trial to show a signifi cant positive eff ect of treatment on the accumulation of irreversible disability as measured by EDSS. However, the results from all these studies indicated signifi cant positive eff ects of treatment on relapse rate (fi gure 5), increase in T2-lesion load (fi gure 6), and MRI measures of MS activity. The diff erences among these studies are not readily explained by methodological considerations, but they could be due, at least in part, to the diff erent patient populations included. This discrepancy is indicated by the fact that placebo patients in the NASPMS study progressed less than both placebo and active treatment groups in the EUSPMS study, although the inclusion criteria were nearly identical. Indeed, in the NASPMS trial, patients had to deteriorate as the result of a gradual progression and those with disability accrual after a relapse were not eligible, whereas, in the EUSPMS trial, patients could also be enrolled when the prestudy EDSS deterioration was due to incomplete recovery from a relapse. This diff erence could have led to the selection of diff erent groups of patients in these two trials, with those participating into the EUSPMS who were closer to the relapsing remitting phase of MS and those enrolled into the NASPMS who were probably further on in the course of the disease. A combined analysis of EUSPMS and NASPMS showed that relapse activity and greater-than-average EDSS progression in the 2 years preceding inclusion might be the most robust predictors of a positive response to treatment.120 However, a longitudinal study125 of 21 patients with secondary progressive MS showed that the discontinuation of interferon beta-1a treatment could be associated with an increase in neurological disability and brain MRI lesion load after a year.
Intravenous immunoglobulinsThere is substantial evidence that treatment with intravenous immunoglobulins has positive eff ects in a wide range of diseases, and a meta-analysis lends support to its effi cacy in the treatment of relapsing remitting MS.126 The effi cacy of intravenous immunoglobulin (1 g/kg administered every 4 weeks for 26 months) was assessed in 318 patients with clinically active secondary progressive MS during the preceeding 2 years.127 The
study results showed no signifi cant eff ect of treatment on time to EDSS failure, relapse rates, T2-lesion load, or MT MRI outcomes.127,128 Howewer, a signifi cantly lower rate of brain atrophy progression was observed in patients treated with intravenous immunoglobulin than in patients in the placebo group, which could warrant further investigation.128
Immunosuppressive strategiesA wide range of immunosuppressants, including methotrexate, cladribine, cyclophosphamide, methyl-prednisolone, azathioprine, cyclosporine, and mito-xantrone have been used in patients with secondary progressive MS.129 Goodkin and colleagues130
administered methylprednisolone every other month
PlaceboActive drugDouble dose
63·1
38·0 37·0
63·7
26·029·0
57·657·555·6
20
35
50
65
80
EUSPMS8MIU
SPECTRIMS22/44 μg
NASPMS8MIU
IMPACT60μg
Pa
tient
s with
rela
pses
(%)
Figure 5: Percentages of patients with secondary progressive MS who had relapses during treatment with interferon beta or placebo in EUSPMS, SPECTRIMS, NASPMS, and IMPACT trialsIn all these studies, treatment with interferon beta resulted in signifi cantly lower relapse rate than did placebo.
10·010·9
–5·3
–0·5–1·3
0·4 0·8
9·7
MRI
T2
lesio
n lo
ad m
edia
n ch
ange
in (%
)
–8·0
0
–3·0
2·0
7·0
12·0
EUSPMS PL (n=204)
SPECTRIMS PL (n
=358)
SPECTRIMS 22μg (n
=209)
SPECTRIMS 44μg (n
=205)
NASPMS 8MIU (n=294)
NASPMS 5MIU/m2 (n
=301)
NASPMS PL (n=290)
EUSPMS 8MIU (n=360)
Figure 6: Percent changes in T2 lesion load in patients treated with interferon beta or placebo in EUSPMS, SPECTRIMS, and NASPMS trialsLesion burden remained stable or decreased in patients who received interferon beta and increased by about 10% in those treated with placebo (PL).

Review
350 http://neurology.thelancet.com Vol 5 April 2006
for up to 2 years to 108 patients with secondary progressive MS. The study results indicated that treatment with high-dose methylprednisolone might have a modest benefi t in delaying time to onset of sustained progression of disability. Methotrexate and cyclophosphamide have also been reported to be eff ective in stabilising disease in some studies, including patients with chronic progressive MS, but this eff ect has not been confi rmed in other studies.130–135 The results of recent controlled and uncontrolled trials of cyclophosphamide136–138 have, however, reported a strong eff ect in patients with secondary progressive MS with poor response to other disease-modifying treatments. Cladribine, an antineoplastic drug approved for the treatment of hairy-cell leukemia, did not show any clinical benefi t in a phase III trial of progressive MS.74 In this cohort, cladribine had a signifi cant eff ect in reducing MRI activity and T2-lesion volume increase, but not in preventing brain atrophy progression and T1-hypointense lesion load increase.78 Mitoxantrone is a synthetic anthracenedione chemotherapeutic agent with broad immunosuppressive and cytotoxic activity. The Mitoxantrone in MS Study (MIMS) included 194 patients with worsening relapsing remitting or secondary progressive MS.139 These patients were assigned treatment with placebo or mitoxantrone (5 mg/m² or 12 mg/m²), given every 3 months for 2 years. The primary endpoint was a composite of fi ve clinical measures: changes from baseline in EDSS, ambulation index, and standard neurological status; number of relapses treated with corticosteroids; and time to fi rst treated relapse. At 24 months, patients treated with mitoxantrone had signifi cant benefi t over the placebo group for the primary outcome, but this eff ect was reported in the total group and not specifi cally in those patients with secondary progressive MS. However, in the same trial, mitoxantrone treatment did not show signifi cant effi cacy on the primary MRI outcome measure—ie, the frequency of active MRI scans at 12 and 24 month assessments.140
Major toxic eff ects could signifi cantly restrict the use of non-selective immunosuppression to treat patients with secondary progressive MS. Toxic eff ects of long-term, low-dose methotrexate treatment include interstitial pulmonary fi brosis, hepatotoxicity, bone marrow suppression, spontaneous abortions, and teratogenesis.129 The modest clinical benefi ts achieved with cyclophosphamide must be weighed against side-eff ects, such as haemorrhagic cystitis, nausea, vomiting, alopecia, and infertility.129 The use of cyclophosphamide has also been associated with the development of secondary malignancies.129 Although the results of MIMS indicated good tolerability for mitoxantrone, safety data from other studies suggest that use of the drug could result in bone-marrow suppression, dose-related cardiotoxicity indicated by reduced left ventricular ejection fraction, and irreversible congestive heart failure.
Because of this potential cardiotoxicity, treatment with mitoxantrone has to be restricted to a cumulative lifetime dose of 140 mg/m².129
A humanised antileucocyte monoclonal antibody, alemtuzumab, which causes prolonged T-lymphocyte depletion, has also been used as immunosuppressive treatment in secondary progressive MS.141–143 Treatment-related adverse events included an acute cytokine release syndrome, associated with the transient exacerbation of neurological symptoms, and, in about 30% of patients, the occurrence of Graves disease. After a single course of alemtuzumab 100 mg given intravenously, a signifi cant reduction of the relapse rate and a suppression of conventional MRI activity were noted in 36 patients with secondary progressive MS who were followed-up for more than 8 years. Unfortunately, these patients continued to show a sustained accumulation of disability due to uncontrolled progression, marked by unrelenting cerebral atrophy on follow-up MRI scans.143 The rate of brain volume reduction was greatest in patients with secondary progressive MS who had the highest infl ammatory lesion burden before treatment.141,143
Intense immunosuppression followed by autologous haemopoietic stem-cell transplantation (ASCT) is a relatively new therapeutic strategy for MS. Mancardi and colleagues75 used ASCT in ten patients with rapidly evolving secondary progressive MS who were transplanted with unmanipulated autologous peripheral blood stem cells mobilised with high-dose cyclophosphamide and granulocyte-colony-stimulating factor after a BEAM conditioning regimen (carmustine, etoposide, cytarabine, and melphalan). Triple-dose gadolinium-enhanced scans were undertaken monthly for a pretreatment period of 3 months, for the following 6 months, and then once every 3 months. These patients were followed up for an average of 15 months. The number of gadolinium-enhancing lesions decreased immediately after mobilisation with cyclophosphamide and dropped to zero in all cases after the conditioning regimen. Clinically, patients improved slightly or remained stable. However, the progression rate of brain atrophy after treatment remained signifi cant.75 These results are consistent with those from a large retrospective analysis of patients with progressive MS who were treated with ASCT.144 In the latter series, 66% of 60 patients with secondary progressive MS had no disease progression over 3 years of follow-up. Although these positive results warrant further prospective study of ASCT in patients with secondary progressive MS, the short-term and long-term toxic eff ects associated with such treatment, including a reported mortality of about 5%, remain an important concern.
In summary, the observed failures of immunosuppressive treatments suggest that once the cascade of events leading to neuronal and axonal loss is established, even an eff ective suppression of infl ammation does not protect from clinical disease progression in secondary progressive MS.

Review
http://neurology.thelancet.com Vol 5 April 2006 351
ConclusionAlthough there is no consensus on the mechanisms underlying the evolution from the relapsing remitting to the secondary progressive phase of MS, epidemiological and MRI studies indicate that this transition can be mainly driven by the prevalence of neurodegenerative over infl ammatory pathological features. The limited effi cacy of available immunomodulating and immunosuppressive therapeutic strategies, which can strongly reduce infl ammation, in prevention of accumulation of irreversible disability suggests that, in secondary progressive MS, infl ammation does play a minor part in driving the dysfunction and progressive loss of neurons and axons.
Quantitative MRI-derived parameters are more sensitive to the progression of MS tissue degeneration than the conventional measures of lesion burden and activity; thus, their use is warranted to monitor natural history studies and therapeutic trials of secondary progressive MS. However, no established clinical or paraclinical predictors of the future transition from relapsing remitting to secondary progressive MS have been described yet. The development of treatments that promote neuroaxonal repair and remyelination remains, therefore, an important goal to enable the work-up of patients with secondary progressive MS in the near future.AcknowledgmentsLK’s work is supported by the Swiss MS Society. No funding was received to write this review.
Authors’ contributionsMR and MF wrote the introduction, neuroimaging, and conclusion sections. CC wrote the clinical aspects section. RF wrote the immunopathology section. LK wrote the treatment section. GC contributed to the preparation of the neuroimaging and treatment sections. MR and MF merged and integrated the individual co-authors’ contributions. All the authors reviewed and discussed the whole paper. We confi rm that this review is solely the work of the authors listed, that all contributors to it are listed as authors and that none of the authors were asked to write, to be named on, or to submit the paper by any organisation.
Confl icts of interestMR has received honoraria for lectures and travel expense refunds from Teva, Serono, and Biogen-Dompè. CC has been acting as an external expert and has given lectures at the request of Biogen-Idec, Sanofi -Aventis, Schering, Serono, and Teva laboratories. RF has received honoraria for lectures and travel expense refunds from Serono and Biogen-Dompé. LK has participated and is currently participating
Search strategy and selection criteria
Data for this review were identifi ed by searches of Medline, Current Contents, and references from relevant articles. The search terms “secondary progressive MS”, “epidemiology”, “immunology”, “pathology”, “magnetic resonance imaging”, and “treatment” were used. The search strategy was carried out in December, 2005. Only papers published in English and from 1995 onwards were reviewed. The fi nal reference list was generated on the basis of originality and relevance to the topics covered in the Review.
as principal investigator, member, or chair of planning and steering committees or advisory boards in corporate-sponsored clinical trials in MS. The sponsoring pharmaceutical companies for these trials include Abbott, Bayer, Bayhill, Berlex, Biogen Idec, Centocor, Eisai, Elan, Genzyme, Neurocrine, Novartis, Sanofi Aventis, Schering, Serono, Roches, Teva, and Wyeth. LK has also lectured at medical conferences or in public on various aspects of the diagnosis and management of MS. In many cases these talks have been sponsored by non-restricted educational grants from one or another of the above listed companies. Honoraria and other payments for these activities have been exclusively used for funding of research at LK’s department. Research and the clinical operations (nursing and patient care services) of the MS Center led by LK have been supported by non-restricted grants from one or more of these companies. GC and MF have received honoraria for lectures and travel expense refunds, as well as consulting fees as investigators in previous and on-going treatment trials from Teva, Serono, Schering, and Biogen-Dompè.
References1 Schumacher GA, Beebe G, Kibler RF, et al. Problems of
experimental trials of therapy in MS: report by the panel on the evaluation of experimental trials of therapy in MS. Ann N Y Acad Sci 1965; 122: 552–68.
2 Poser CM, Paty DW, Scheinberg L, et al. New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann Neurol 1983; 13: 227–31.
3 Confavreux C, Compston DAS, Hommes OR, et al. EDMUS, a European Database for Multiple Sclerosis. J Neurol Neurosurg Psychiatry 1992; 55: 671–76.
4 Thompson AJ, Polman CH, Miller DH, et al. Primary progressive multiple sclerosis. Brain 1997; 120: 1085–96.
5 McDonald WI, Compston A, Edan G et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the international panel on the diagnosis of multiple sclerosis. Ann Neurol 2001; 50: 121–27.
6 Lublin FD, Reingold SC, for the National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Defi ning the clinical course of multiple sclerosis: results of an international survey. Neurology 1996; 46: 907–11.
7 Confavreux C, Compston DAS. The natural history of multiple sclerosis. In: Compston DAS, ed. McAlpine’s multiple sclerosis, 4th edn. London: Churchill-Livingstone, 2005.
8 McAlpine D, Compston ND. Some aspects of the natural history of disseminated sclerosis: incidence, course and prognosis, factors aff ecting onset and course. Q J Med 1952; 21: 135–67.
9 Confavreux C. L’histoire naturelle de la sclérose en plaques: etude par informatique de 349 observations. Lyon, France: Thèse de Médecine, Université Claude Bernard–Lyon, 1977.
10 Confavreux C, Aimard G, Devic M. Course and prognosis of multiple sclerosis assessed by the computerized data processing of 349 patients. Brain 1980; 103: 281–300.
11 Vukusic S, Confavreux C. Prognostic factors for progression of disability in the secondary progressive phase of multiple sclerosis. J Neurol Sci 2003; 206: 135–37.
12 Broman T, Andersen O, Bergmann L. Clinical studies on multiple sclerosis I: presentation of an incidence material from Gothenburg. Acta Neurol Scand 1981; 63: 6–33.
13 Eriksson M, Andersen O, Runmarker B. Long-term tollow-up of patients with clinically isolated syndromes, relapsing-remitting and secondary progressive multiple sclerosis. Mult Scler 2003; 9: 260–74.
14 Weinshenker BG, Bass B, Rice GP, et al. The natural history of multiple sclerosis: a geographically based study I: clinical course and disability. Brain 1989; 112: 133–46.
15 Amato MP, Ponziani G. A prospective study on the prognosis of multiple sclerosis. Neurol Sci 2000; 21 (suppl 2): 831–38.
16 Myhr KM, Riise T, Vedeler C, et al. Disability an prognosis in multiple sclerosis: demographic and clinical variables important for the ability to walk and awarding of disability pension. Mult Scler 2001; 7: 59–65.
17 Müller R. Studies on disseminated sclerosis: with special reference to symptomatology, course and prognosis. Acta Med Scand 1949; 133 (suppl 222): 1–214.

Review
352 http://neurology.thelancet.com Vol 5 April 2006
18 Müller R. Course and prognosis of disseminated sclerosis in relation to age at onset. Arch Neurol Psychiatry 1951; 66: 561–70.
19 Riise T, Gronning M, Fernandez O, et al. Early prognostic factors for disability in multiple sclerosis, a European multicenter study. Acta Neurol Scand 1992; 85: 212–18.
20 Runmarker B, Andersen O. Prognostic factors in a multiple sclerosis incidence cohort with twenty fi ve years of follow-up. Brain 1993; 116: 117–34.
21 Trojano M, Avolio C, Manzari C, et al. Multivariate analysis of predictive factors of multiple sclerosis with a validated method to assess clinical events. J Neurol Neurosurg Psychiatry 1995; 58: 300–06.
22 Confavreux C, Vukusic S, Adeleine P. Early clinical predictors and progression of irreversible disability in multiple sclerosis: an amnesic process. Brain 2003; 126: 770–82.
23 Kurtzke JF. Rating neurological impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983; 33: 1444–52.
24 Confavreux C, Vukusic S, Moreau T, Adeleine P. Relapses and progression of disability in multiple sclerosis. N Eng J Med 2000; 343: 1430–38.
25 Vukusic S, Confavreux C. Primary and secondary progressive multiple sclerosis. J Neurol Sci 2003; 206: 153–55.
26 Minderhoud JM, van der Hoeven JH, Prange AJA. Course and prognosis of chronic progressive multiple sclerosis: results of an epidemiological study. Acta Neurol Scand 1988; 78: 10–15.
27 Cottrell DA, Kremenchutzky M, Rice GPA, et al. The natural history of multiple sclerosis: a geographically based study 5: the clinical features and natural history of primary progressive multiple sclerosis. Brain 1999; 122: 625–39.
28 Kremenchutzky M, Cottrell D, Rice G, et al. The natural history of multiple sclerosis—a geographically based study 7: progressive-relapsing and relapsing-progressive multiple sclerosis, a re-evaluation. Brain 1999; 122: 1941–49.
29 Revesz T, Kidd D, Thompson AJ, Barnard RO, McDonald WI. A comparison of the pathology of primary and secondary progressive multiple sclerosis. Brain 1994; 117: 759–65.
30 Prineas JW, Kwon EE, Cho ES, et al. Immunopathology of secondary-progressive multiple sclerosis. Ann Neurol 2001; 50: 646–57.
31 Kutzelnigg A, Lucchinetti CF, Stadelmann C, et al. Cortical demyelination and diff use white matter injury in multiple sclerosis. Brain 2005; 128: 2705–12.
32 Serafi ni B, Rosicarelli B, Magliozzi R, Stigliano E, Aloisi F. Detection of ectopic B-cell follicles with germinal centers in the meninges of patients with secondary progressive multiple sclerosis. Brain Pathol 2004; 14: 164–74.
33 Soldan SS, Alvarez Retuerto AI, Sicotte NL, Voskuhl RR. Dysregulation of IL-10 and IL-12p40 in secondary progressive multiple sclerosis. J Neuroimmunol 2004; 146: 209–15.
34 Sorensen TL, Sellebjerg F. Distinct chemokine receptor and cytokine expression profi le in secondary progressive MS. Neurology 2001; 57: 1371–76.
35 Trebst C, Sorensen TL, Kivisakk P, et al. CCR1+/CCR5+ mononuclear phagocytes accumulate in the central nervous system of patients with multiple sclerosis. Am J Pathol 2001; 159: 1701–10.
36 Furlan R, Rovaris M, Khademi M, et al. Immunological patterns identifying disease course and disease evolution in multiple sclerosis patients. J Neuroimmunol 2005; 165: 192–200.
37 Eikelenboom MJ, Killestein J, Izeboud T, et al. Expression of adhesion molecules on peripheral lymphocytes predicts future lesion development in MS. J Neuroimmunol 2005; 158: 222–30.
38 Eikelenboom MJ, Killestein J, Uitdehaag BM, Polman CH. Sex diff erences in proinfl ammatory cytokine profi les of progressive patients in multiple sclerosis. Mult Scler 2005; 11: 520–23.
39 Thompson AJ, Kermode AG, Wicks D, et al. Major diff erences in the dynamics of primary and secondary progressive multiple sclerosis. Ann Neurol 1991; 29: 53–62.
40 Filippi M, Iannucci G, Tortorella C, et al. Comparison of MS clinical phenotypes using conventional and magnetization transfer MRI. Neurology 1999; 52: 588–94.
41 Rovaris M, Bozzali M, Santuccio G, et al. In vivo assessment of the brain and cervical cord pathology of patients with primary progressive multiple sclerosis. Brain 2001; 124: 2540–49.
42 Stevenson VL, Miller DH, Rovaris M, et al. Primary and transitional progressive MS: a clinical and MRI cross-sectional study. Neurology 1999; 52: 839–45.
43 Lycklama à Nijeholt GJ, van Walderveen MAA, Castelijins JA, et al. Brain and spinal cord abnormalities in multiple sclerosis: correlation between MRI parameters, clinical subtypes, and symptoms. Brain 1998; 121: 687–97.
44 Molyneux PD, Barker GJ, Barkhof F, et al. Clinical-MRI correlations in a European trial of interferon beta-1b in secondary progressive MS. Neurology 2001; 57: 2191–97.
45 Filippi M, Rossi P, Campi A, Colombo B, Pereira C, Comi G. Serial contrast-enhanced MR in patients with multiple sclerosis and varying levels of disability. AJNR Am J Neuroradiol 1997; 18: 1549–56.
46 Koziol JA, Wagner S, Adams HP. Assessing information in T2-weighted MRI scans from secondary progressive MS patients. Neurology 1998; 51: 228–33.
47 Wolinsky JS, Narayana PA, Noseworthy JH, et al. Linomide in relapsing and secondary progressive multiple sclerosis: MRI results. Neurology 2000; 54: 1734–41.
48 Tubridy N, Coles AJ, Molyneux P, et al. Secondary progressive multiple sclerosis: the relationship between short-term MRI activity and clinical features. Brain 1998; 121: 225–31.
49 Molyneux PD, Filippi M, Barkhof F, et al. Correlations between monthly enhanced MRI lesion rate and changes in T2 lesion volume in multiple sclerosis. Ann Neurol 1998; 43: 332–39.
50 Kappos L, Moeri D, Radue EW, et al. Predictive value of gadolinium-enhanced magnetic resonance imaging for relapse rate and changes in disability or impairment in multiple sclerosis: a meta-analysis. Lancet 1999; 353: 964–69.
51 Smith ME, Stone LA, Albert PS, et al. Clinical worsening in multiple sclerosis is associated with increased frequency and area of gadopentetate dimeglumine-enhancing magnetic resonance imaging lesions. Ann Neurol 1993; 33: 480–89.
52 Morgen K, Jeff ries NO, Stone R, et al. Ring-enhancement in multiple sclerosis: marker of disease severity. Mult Scler 2001; 7: 167–71.
53 Truyen L, van Waesberghe JHTM, van Walderveen MAA, et al. Accumulation of hypointense lesions (“black holes”) on T1 spin-echo MRI correlates with disease progression in multiple sclerosis. Neurology 1997; 47: 1469–76.
54 Tortorella C, Viti B, Bozzali M, et al. A magnetization transfer histogram study of normal appearing brain tissue in multiple sclerosis. Neurology 2000; 54: 186–93.
55 van Walderveen MAA, Lycklama à Nijeholt GJ, Ader HJ, et al. Hypointense lesions on T1-weighted spin-echo magnetic resonance imaging: relation to clinical characteristics in subgroups of patients with multiple sclerosis. Arch Neurol 2001; 58: 76–81.
56 Minneboo A, Uitdehaag BMJ, Ader HJ, Barkhof F, Polman CH, Casteljins JA. Patterns of enhancing lesion evolution in multiple sclerosis are uniform within patients. Neurology 2005; 65: 56–61.
57 Losseff NA, Wang L, Lai HM, et al. Progressive cerebral atrophy in multiple sclerosis: a serial MRI study. Brain 1996; 119: 2009–19.
58 Ge Y, Grossman RI, Udupa JK, et al. Brain atrophy in relapsing-remitting multiple sclerosis and secondary progressive multiple sclerosis: longitudinal quantitative analysis. Radiology 2000; 214: 665–70.
59 Kalkers NF, Bergers E, Castelijns JA, et al. Optimizing the association between disability and biological markers in MS. Neurology 2001; 57: 1253–58.
60 Lin X, Blumhardt LD. Infl ammation and atrophy in multiple sclerosis: MRI associations with disease course. J Neurol Sci 2001; 189: 99–104.
61 Pagani E, Rocca MA, Gallo A, et al. Regional brain atrophy evolves diff erently in patients with multiple sclerosis according to clinical phenotype. Am J Neuroradiol 2005; 26: 341–46.
62 Filippi M, Campi A, Colombo B, et al. A spinal cord MRI study of benign and secondary progressive multiple sclerosis. J Neurol 1996; 243: 502–05.
63 Losseff NA, Webb SL, O’Riordan JI, et al. Spinal cord atrophy and disability in multiple sclerosis: a new reproducible and sensitive MRI method with potential to monitor disease progression. Brain 1996; 119: 701–08.

Review
http://neurology.thelancet.com Vol 5 April 2006 353
64 Lin X, Tench CR, Turner B, Blumhardt LD, Constantinescu CS. Spinal cord atrophy and disability in multiple sclerosis over four years: application of a reproducible automated technique in monitoring disease progression in a cohort of the interferon β-1a (Rebif) treatment trial. J Neurol Neurosurg Psychiatry 2003; 74: 1090–94.
65 Stevenson VL, Leary SM, Losseff NA, et al. Spinal cord atrophy and disability in MS: a longitudinal study. Neurology 1998; 51: 234–38.
66 Valsasina P, Rocca MA, Agosta F, et al. Mean diff usivity and fractional anisotropy histogram analysis of the cervical cord in MS patients. NeuroImage 2005; 26: 822–28.
67 Kalkers NF, Ameziane N, Boost JCJ, Minneboo A, Polman CH, Barkhof F. Longitudinal brain volume measurement in multiple sclerosis: rate of brain atrophy is independent of the disease subtype. Arch Neurol 2002; 59: 1572–76.
68 Rovaris M, Agosta F, Sormani MP, et al. Conventional and magnetization transfer MRI predictors of clinical multiple sclerosis evolution: a medium-term follow-up study. Brain 2003; 126: 2323–32.
69 Rovaris M, Bozzali M, Iannucci G, et al. Assessment of normal-appearing white and gray matter in patients with primary progressive multiple sclerosis. Arch Neurol 2002; 59: 1406–12
70 Rovaris M, Gallo A, Valsasina P, et al. Short-term accrual of grey matter pathology in patients with progressive multiple sclerosis: an in vivo study using diff usion tensor MRI. NeuroImage 2005; 24: 1139–46.
71 Sormani MP, Bruzzi P, Beckmann K, et al. MRI metrics as surrogate endpoints for EDSS progression in SPMS patients treated with IFN beta-1b. Neurology 2003; 60: 1462–66.
72 Miller DH, Molyneux PD, Barker GJ, et al. Eff ect of interferon-beta1b on magnetic resonance imaging outcomes in secondary progressive multiple sclerosis: results of a European multicenter, randomized, double-blind, placebo-controlled trial. Ann Neurol 1999; 46: 850–59.
73 Rice GP, Filippi M, Comi G. Cladribine and progressive MS: clinical and MRI outcomes of a multicenter controlled trial. Neurology 2000; 54: 1145–55.
74 Li DKB, Zhao GJ, Paty DW. Randomized controlled trial of interferon-beta-1a in secondary progressive MS: MRI results. Neurology 2001; 56: 1505–13.
75 Mancardi GL, Saccardi R, Filippi M, et al. Autologous hematopoietic stem cell transplantation suppresses Gd-enhanced MRI activity in MS. Neurology 2001; 57: 62–68.
76 Molyneux PD, Kappos L, Polman C, et al. The eff ect of interferon beta-1b treatment on MRI measures of cerebral atrophy in secondary progressive multiple sclerosis. Brain 2000; 123: 2256–63.
77 Barkhof F, van Waesberghe JH, Filippi M, et al. T1 hypointense lesions in secondary progressive multiple sclerosis: eff ect of interferon beta-1b treatment. Brain 2001; 124: 1396–402.
78 Filippi M, Rovaris M, Iannucci G, Mennea S, Sormani MP, Comi G. Whole brain volume changes in patients with progressive MS treated with cladribine. Neurology 2000; 55: 1714–18.
79 Filippi M, Rovaris M, Rice GPA, et al. The eff ect of cladribine on T1 ‘black hole’ changes in progressive MS. J Neurol Sci 2000; 176: 42–44.
80 Inglese M, Mancardi GL, Pagani E, et al. Brain tissue loss occurs after suppression of enhancement in MS patients treated with AHSCT. J Neurol Neurosurg Psychiatry 2004; 75: 643–44.
81 Filippi M, Grossman RI, Comi G. Magnetization transfer in multiple sclerosis. Neurology 1999; 53 (suppl 3): S40–45.
82 Rovaris M, Gass A, Bammer R, et al. Diff usion MRI in multiple sclerosis. Neurology 2005; 65: 1526–32.
83 Bot JC, Blezer EL, Kamphorst W, et al. The spinal cord in multiple sclerosis: relationship of high spatial-resolution quantitative MR imaging fi ndings to histopathologic results. Radiology 2004; 233: 531–40.
84 Filippi M, Arnold DL, Comi G. Magnetic resonance spectroscopy in multiple sclerosis. Milan, Italy: Springer-Verlag, 2000.
85 Filippi M, Inglese M, Rovaris M, et al. Magnetization transfer imaging to monitor the evolution of MS: a one-year follow up study. Neurology 2000; 55: 940–46.
86 Kalkers NF, Hintzen RQ, van Waesberghe JH, et al. Magnetization transfer histogram parameters refl ect all dimensions of MS pathology, including atrophy. J Neurol Sci 2001; 184: 155–62.
87 Ge Y, Grossman RI, Udupa JK, Babb JS, Mannon LJ, McGowan JC. Magnetization transfer ratio histogram analysis of normal-appearing gray matter and normal-appearing white matter in multiple sclerosis. J Comput Assist Tomogr 2002; 26: 62–68.
88 van Waesberghe JH, Kamphorst W, De Groot CJ, et al. Axonal loss in multiple sclerosis lesions: magnetic resonance imaging insights into substrates of disability. Ann Neurol 1999; 46: 747–54.
89 Schmierer K, Scaravilli F, Altmann DR, Barker GJ, Miller DH. Magnetization transfer ratio and myelin in post mortem multiple sclerosis brain. Ann Neurol 2004; 56: 407–15.
90 Rocca MA, Mastronardo G, Rodegher M, Comi G, Filippi M. Long term changes of MT-derived measures from patients with relapsing-remitting and secondary-progressive multiple sclerosis. Am J Neuroradiol 1999; 20: 821–27.
91 Inglese M, van Waesberghe JHTM, Rovaris M, et al. The eff ect of interferon beta-1b on quantities derived from MT MRI in secondary progressive MS. Neurology 2003; 60: 853–60.
92 Filippi M, Bozzali M, Horsfi eld MA, et al. A conventional and magnetization transfer MRI study of the cervical cord in patients with multiple sclerosis. Neurology 2000; 54: 207–13.
93 Rovaris M, Bozzali M, Santuccio G, et al. Relative contributions of brain and cervical cord pathology to MS disability: a study with MTR histogram analysis. J Neurol Neurosurg Psychiatry 2000; 69: 723–27.
94 Droogan AG, Clark CA, Werring DJ, Barker GJ, McDonald WI, Miller DH. Comparison of multiple sclerosis clinical subgroups using navigated spin echo diff usion-weighted imaging. Magn Reson Imaging 1999; 17: 653–61.
95 Nusbaum AO, Tang CY, Wei TC, Buchsbaum MS, Atlas SW. Whole-brain diff usion MR histograms diff er between MS subtypes. Neurology 2000; 54: 1421–26.
96 Filippi M, Cercignani M, Inglese M, Horsfi eld MA, Comi G. Diff usion tensor magnetic resonance imaging in multiple sclerosis. Neurology 2001; 56: 304–11.
97 Ciccarelli O, Werring DJ, Wheeler-Kingshott CA, et al. Investigation of MS normal-appearing brain using diff usion tensor MRI with clinical correlations. Neurology 2001; 56: 926–33.
98 Cercignani M, Inglese M, Pagani E, Comi G, Filippi M. Mean diff usivity and fractional anisotropy histograms in patients with multiple sclerosis. Am J Neuroradiol 2001; 22: 952–58.
99 Cercignani M, Bozzali M, Iannucci G, Comi G, Filippi M. Intra-voxel and inter-voxel coherence in patients with multiple sclerosis assessed using diff usion tensor MRI. J Neurol 2002; 249: 875–83.
100 Bozzali M, Cercignani M, Sormani MP, Comi G, Filippi M. Quantifi cation of brain gray matter damage in diff erent MS phenotypes by use of diff usion tensor MR imaging. Am J Neuroradiol 2002; 23: 985–88.
101 Vrenken H, Geurts JJG, Knol DL, et al. Whole-brain T1-mapping in multiple sclerosis: global changes of normal-appearing grey and white matter. Radiology (in press).
102 Vaithianathar L, Tench CR, Morgan PS, Constantinescu CS. Magnetic resonance imaging of the cervical spinal cord in multiple sclerosis: a quantitative T1 relaxation time mapping approach. J Neurol 2003; 250: 307–15.
103 Simmons MS, Frondosa CG, Coyle JT. Immunocytochemical localization of N-acetyl aspartate with monoclonal antibodies. Neuroscience 1991; 45: 37–45.
104 Fu L, Matthews PM, De Stefano N, et al. Imaging axonal damage of normal-appearing white matter in multiple sclerosis. Brain 1998; 121: 59–166.
105 De Stefano N, Matthews PM, Fu LQ, et al. Axonal damage correlates with disability in patients with relapsing-remitting multiple sclerosis: results of a longitudinal magnetic resonance spectroscopy study. Brain 1998; 121: 1469–77.
106 Falini A, Calabrese G, Filippi M, et al. Benign versus secondary progressive multiple sclerosis: the potential role of proton MR spectroscopy in defi ning the nature of disability. Am J Neuroradiol 1998; 19: 223–29.
107 Tourbah A, Stievenart JL, Gout O, et al. Localized proton magnetic resonance spectroscopy in relapsing remitting versus secondary progressive multiple sclerosis. Neurology 1999; 53: 1091–97.
108 Sarchielli P, Presciutti O, Pelliccioli GP, et al. Absolute quantifi cation of brain metabolites by proton magnetic resonance spectroscopy in normal-appearing white matter of multiple sclerosis patients. Brain 1999; 122: 513–21.

Review
354 http://neurology.thelancet.com Vol 5 April 2006
109 De Stefano N, Narayanan S, Francis GS, et al. Evidence of axonal damage in the early stages of multiple sclerosis and its relevance to disability. Arch Neurol 2001; 58: 65–70.
110 Adalsteinsson E, Langer-Gould A, Homer RJ, et al. Gray matter N-acetyl aspartate defi cits in secondary progressive but not relapsing-remitting multiple sclerosis. Am J Neuroradiol 2003; 24: 1941–45.
111 Vrenken H, Barkhof F, Uitdehaag BMJ, Casteljins JA, Polman CH, Pouwels PJW. MR spectroscopic evidence for glial increase but not for neuro-axonal damage in MS normal-appearing white matter. Magn Reson Med 2005; 53: 256–66.
112 Reddy H, Narayanan S, Arnoutelis R, et al. Evidence for adaptive functional changes in the cerebral cortex with axonal injury from multiple sclerosis. Brain 2000; 123: 2314–20.
113 Pantano P, Iannetti GD, Caramia F, et al. Cortical motor reorganization after a single attack of multiple sclerosis. Brain 2002; 125: 1607–15.
114 Rocca MA, Matthews PM, Caputo D, et al. Evidence for widespread movement-associated functional MRI changes in patients with PPMS. Neurology 2002; 58: 866–72.
115 Filippi M, Rocca MA, Falini A, et al. Correlations between structural CNS damage and functional MRI changes in primary progressive MS. NeuroImage 2002; 15: 537–46.
116 Rocca MA, Gavazzi C, Mezzapesa DM, et al. A functional magnetic resonance imaging study of patients with secondary progressive multiple sclerosis. NeuroImage 2003; 19: 1770–77.
117 Rocca MA, Colombo B, Falini A, et al. Cortical adaptation in patients with MS: a cross-sectional functional MRI study of disease phenotypes. Lancet Neurol 2005; 4: 618–26.
118 European Study Group on interferon β-1b in secondary progressive MS. Placebo-controlled multicentre randomised trial of interferon beta-1b in treatment of secondary progressive multiple sclerosis. Lancet 1998; 352: 1491–97.
119 Kappos L, Polman C, Pozzilli C, Thompson A, Beckmann K, Dahlke F. Final analysis of the European multicenter trial on IFNβ-1b in secondary-progressive MS. Neurology 2001; 57: 1969–75.
120 Kappos L, Weinshenker B, Pozzilli C, et al. Interferon beta-1b in secondary progressive MS: a combined analysis of the two trials. Neurology 2004; 63: 1779–87.
121 Freeman JA, Thompson AJ, Fitzpatrick R, et al. Interferon-β1b in the treatment of secondary progressive MS: impact on quality of life. Neurology 2001; 57: 1870–75.
122 Secondary Progressive Effi cacy Clinical Trial of Recombinant Interferon-beta-1a in MS (SPECTRIMS) Study Group. Randomized controlled trial of interferon-beta-1a in secondary progressive MS: clinical results. Neurology 2001; 56: 1496–504.
123 Panitch H, Miller A, Paty D, et al. Interferon beta-1b in secondary progressive MS: results from a 3-year controlled study. Neurology 2004; 63: 1788–95.
124 Cohen JA, Cutter GR, Fischer JS, et al. Benefi t of interferon beta-1a on MSFC progression in secondary progressive MS. Neurology 2002; 59: 679–87.
125 Wu X, Dastidar P, Kuusisto H, Ukkonen M, Huhtala H, Elovaara I. Increased disability and MRI lesions after discontinuation of IFN-β-1a in secondary progressive MS. Acta Neurol Scand 2005; 112: 242–47.
126 Sorensen PS, Fazekas F, Lee M. Intravenous immunoglobulin G for the treatment of relapsing-remitting multiple sclerosis: a meta-analysis. Eur J Neurol 2002; 9: 557–63.
127 Hommes OR, Sorensen PS, Fazekas F, et al. Intravenous immunoglobulin in secondary progressive multiple sclerosis: randomised placebo-controlled trial. Lancet 2004; 364: 1149–56.
128 Fazekas F, Sorensen PS, Filippi M, et al. MRI results from the European study on intravenous immunoglobulin in secondary progressive multiple sclerosis (ESIMS). Mult Scler 2005; 11: 433–40.
129 Polman CH, Thompson AJ, Murray GJ, McDonald WI. Multiple sclerosis: the guide to treatment and management, 5th edn. New York: Demos Medical Publishing, 2001.
130 Goodkin DE, Kinkel RP, Weinstock-Guttman B, et al. A phase II study of i.v. methylprednisolone in secondary-progressive multiple sclerosis. Neurology 1998; 51: 239–45.
131 Lugaresi A, Caporale C, Farina D, et al. Low-dose oral methotrexate treatment in chronic progressive multiple sclerosis. Neurol Sci 2001; 22: 209–10.
132 La Mantia L, Eoli M, Salmaggi A, Torri V, Milanese C. Cyclophosphamide in chronic progressive multiple sclerosis: a comparative study. Ital J Neurol Sci 1998; 19: 32–36.
133 Currier RD, Haerer AF, Meydrech EF. Low-dose methotrexate treatment of multiple sclerosis: a pilot study. J Neurol Neurosurg Psychiatry 1993; 56: 1217–18.
134 Goodkin DE, Rudick RA, Vanderburg-Medendorp S, et al. Low-dose (7.5 mg) oral methotrexate reduces the rate of progression in chronic progressive multiple sclerosis. Ann Neurol 1995; 37: 30–40.
135 Smith DR, Weiner HL. Cyclophosophamide treatment of multiple sclerosis. In: Cohen JA, Rudick RA, eds. Multiple sclerosis therapeutics, 2nd edn. London: Martin Dunitz, 2003: 483–500.
136 The Canadian Cooperative Multiple Sclerosis Study Group. The Canadian cooperative trial of cyclophosphamide and plasma exchange in progressive multiple sclerosis. Lancet 1991; 337: 441–46.
137 Patti T, Reggio E, Palermo F, et al. Stabilization of rapidly worsening multiple sclerosis for 36 months in patients treated with interferon beta plus cyclophosphamide followed by interferon beta. J Neurol 2004; 251: 1502–06.
138 Perini P, Gallo P. Cyclophosphamide is eff ective in stabilizing rapidly deteriorating secondary progressive multiple sclerosis. J Neurol 2003; 250: 834–38.
139 Hartung HP, Gonsette R, Konig N, et al. Mitoxantrone in progressive multiple sclerosis: a placebo-controlled, double-blind, randomised, multicentre trial. Lancet 2002; 360: 2018–25.
140 Krapf H, Morrissey SP, Zenker O, et al. Eff ect of mitoxantrone on MRI in progressive MS: results of the MIMS trial. Neurology 2005; 65: 690–95.
141 Coles AJ, Wing MG, Molyneux P, et al. Monoclonal antibody treatment exposes three mechanisms underlying the clinical course of multiple sclerosis. Ann Neurol 1999; 46: 296–304.
142 Paolillo A, Coles AJ, Molyneux P, et al. Quantitative MRI in patients with secondary progressive MS treated with monoclonal antibody Campath 1H. Neurology 1999; 53: 751–57.
143 Coles AJ, Cox A, Le Page E, et al. The window of therapeutic opportunity in multiple sclerosis: evidence from monoclonal antibody therapy. J Neurol (in press).
144 Fassas A, Passweg JR, Anagnostopoulos A, et al. Hematopoietic stem cell transplantation for multiple sclerosis: a retrospective multicenter study. J Neurol 2002; 249: 1088–97.


















