Searching for predictors of long-term stability
14
Searching for predictors of long-term stability Scott Franklin, DDS, P. Emile Rossouw, BSc, BChD, BChD (Hons-Child Dent), MChD (Ortho), PhD, FRCD(C), Donald G. Woodside, DDS, MSc, PhD(H), and Jimmy C. Boley, DDS, MS The purpose of this investigation was to evaluate a unique sample of orthodontically treated subjects (N ¼ 114; post-retention ¼ 11.97 years). All subjects were treated by one clinician utilizing a consistent diagnostic and treatment protocol. Subjects were grouped into two distinct groups according to the lower incisor irregularity: group 1, “moderate change” and group 2, “minor change.” Statistical analyses were performed at a level of r Z0.6, p o 0.01. Satisfactory long-term stability was achieved in 79% of the subjects; moreover, no subject exhibited severe incisor irregularity post- retention. Similar to previous studies, no individual or single predictor for long-term change could be identified. However, different to most studies, useful predictors of the post-retention incisor alignment included the relationship of the lower incisor to the A-Pogonion plane at the end of treatment (at T 2 ), posterior face height (at T 2 ), the mandibular plane angle SN-GoGn (at T 2 ), anterior crowding (at T 2 ), and starting age (at T 1 ). It is clearly noted that the vertical dimension features in the equation. (Semin Orthod 2013; 19:279–292.) Published by Elsevier Inc. L ongitudinal investigations to identify treat- ment and post-treatment variables of clinical significance in controlling future mandibular incisor crowding have been unsuccessful in identi- fying the individual or exact etiology of post- treatment and post-retention changes in the lower incisor alignment. 1–8 Moreover, longitudinal data show that changes in arch dimensions as well as lower incisor crowding occur as a part of the normal aging process. 9–11 In addition, the velocity of this change was found to decrease after 40 years of age. 12 Thus, late mandibular incisor crowding may be unrelated to any previous orthodontic treatment. An evaluation of the National Health and Nutrition Examination Survey (NHANES) data provided a compilation of variables that could assist in the determination of long-term lower incisor crowding. 13 The post-retention incisor irregularity in premolar extraction cases increased at a rate approximately twice that of untreated cases. 1,10 Little et al. 6 and McReynolds and Little 14 also showed that post-retention incisor irregularity in orthodontically treated serial extraction cases did not differ from treated premolar extraction cases. In a comparison of long-term lower incisor alignment in serial extraction cases with no subsequent orthodontic treatment to untreated matched controls, no significant differences in the amount of mandibular incisor irregularity, or crowding, existed between the two groups or between males and females. 15 Therefore, since orthodontically treated premolar extraction cases (serial and late) showed greater post-retention changes in incisor alignment than patients who would have been candidates for premolar extraction but were not treated, one may con- clude that the orthodontic mechanotherapy in the above studies may have contributed to the long-term changes. 1,6,14 In general, dental parameters tend to return to their pre-treatment values after treatment. 16 Overcorrection thus appears to favor success. 17 Published by Elsevier Inc. 1073-8746/13/1801-$30.00/0 http://dx.doi.org/10.1053/j.sodo.2013.07.008 Private practice, Austin, TX; Department of Orthodontics, University of North Carolina School of Dentistry, Chapel Hill, NC; Department of Orthodontics, University of Toronto, Toronto, Canada; Private practice, Richardson, TX. Address correspondence to P. Emile Rossouw, BSc, BChD, BChD (Hons-Child Dent), MChD (Ortho), PhD, FRCD(C), Department of Orthodontics, University of North Carolina School of Dentistry, 277 Brauer Hall, Campus Box 7450, Chapel Hill, NC 27599-7450. E-mail: [email protected] 279 Seminars in Orthodontics, Vol 19, No 4 (December), 2013: pp 279–292
Transcript of Searching for predictors of long-term stability

Searching for predictors
of long-term stabilityScott Franklin, DDS, P. Emile Rossouw, BSc, BChD, BChD (Hons-Child Dent),MChD (Ortho), PhD, FRCD(C), Donald G. Woodside, DDS, MSc, PhD(H), andJimmy C. Boley, DDS, MS
Publishe1073-87http://d
PrivateUniversity oDepartmentCanada; Pr
Address(Hons-Childof OrthodonBrauer HalE-mail: emil
The purpose of this investigation was to evaluate a unique sample of
orthodontically treated subjects (N ¼ 114; post-retention ¼ 11.97 years). All
subjects were treated by one clinician utilizing a consistent diagnostic and
treatment protocol. Subjects were grouped into two distinct groups
according to the lower incisor irregularity: group 1, “moderate change”
and group 2, “minor change.” Statistical analyses were performed at a level
of r Z0.6, p o 0.01. Satisfactory long-term stability was achieved in 79% of
the subjects; moreover, no subject exhibited severe incisor irregularity post-
retention. Similar to previous studies, no individual or single predictor for
long-term change could be identified. However, different to most studies,
useful predictors of the post-retention incisor alignment included the
relationship of the lower incisor to the A-Pogonion plane at the end of
treatment (at T2), posterior face height (at T2), the mandibular plane angle
SN-GoGn (at T2), anterior crowding (at T2), and starting age (at T1). It is clearly
noted that the vertical dimension features in the equation. (Semin Orthod
2013; 19:279–292.) Published by Elsevier Inc.
L ongitudinal investigations to identify treat-ment and post-treatment variables of clinical
significance in controlling future mandibularincisor crowding have been unsuccessful in identi-fying the individual or exact etiology of post-treatment and post-retention changes in the lowerincisor alignment.1–8 Moreover, longitudinal datashow that changes in arch dimensions as well aslower incisor crowding occur as a part of thenormal aging process.9–11 In addition, the velocityof this change was found to decrease after 40 yearsof age.12 Thus, late mandibular incisor crowdingmay be unrelated to any previous orthodontictreatment. An evaluation of the National Healthand Nutrition Examination Survey (NHANES)data provided a compilation of variables that
d by Elsevier Inc.46/13/1801-$30.00/0x.doi.org/10.1053/j.sodo.2013.07.008
practice, Austin, TX; Department of Orthodontics,f North Carolina School of Dentistry, Chapel Hill, NC;of Orthodontics, University of Toronto, Toronto,
ivate practice, Richardson, TX.correspondence to P. Emile Rossouw, BSc, BChD, BChDDent), MChD (Ortho), PhD, FRCD(C), Department
tics, University of North Carolina School of Dentistry, 277l, Campus Box 7450, Chapel Hill, NC [email protected]
Seminars in Orthodontics, Vol 19, No
could assist in the determination of long-termlower incisor crowding.13
The post-retention incisor irregularity inpremolar extraction cases increased at a rateapproximately twice that of untreated cases.1,10
Little et al.6 and McReynolds and Little14 alsoshowed that post-retention incisor irregularity inorthodontically treated serial extraction cases didnot differ from treated premolar extractioncases. In a comparison of long-term lower incisoralignment in serial extraction cases with nosubsequent orthodontic treatment to untreatedmatched controls, no significant differences inthe amount of mandibular incisor irregularity, orcrowding, existed between the two groups orbetween males and females.15 Therefore, sinceorthodontically treated premolar extraction cases(serial and late) showed greater post-retentionchanges in incisor alignment than patients whowould have been candidates for premolarextraction but were not treated, one may con-clude that the orthodontic mechanotherapy inthe above studies may have contributed to thelong-term changes.1,6,14
In general, dental parameters tend to returnto their pre-treatment values after treatment.16
Overcorrection thus appears to favor success.17
2794 (December), 2013: pp 279–292

Franklin et al280
Changes in mandibular growth direction androtation during the post-treatment and post-retention periods (vertical dimension) havealso been implicated in the etiology of late incisorcrowding.18,19 In addition, the vertical develop-ment of the mandibular ramus continues untillate adolescence.20 Crowding of the mandibularincisors was observed in vertical growers as aresult of chronic airway obstruction.21,22 Inaddition, Fudalej and Artun23 concluded in theirstudy on short facial height, long facial height,and normal facial height at the post-treatmentappliance removal interval (T2) that the high- orlow-angled facial patterns were not associatedwith post-retention (T3) relapse of the man-dibular incisor alignment; thus providing poorprediction of this post-retention malalignment.
It appears that the degree of post-treatmentincisor crowding is both unpredictable and vari-able irrespective of the treatment. In addition, nopre-treatment variables that were obtained eitherbefore or after treatment from clinical findings,dental casts, or cephalometric radiographs havebeen found as clinically useful predictors. Fur-ther investigation is needed in this area.
The purpose of this study was to (1) present thefindings from a large sample of orthodonticallytreated patients who have been without retentionfor a minimum of 5 years, (2) identify any stat-istically significant differences in cast or cepha-lometric variables between subjects with minor(clinically acceptable) and major (clinicallyunacceptable) post-retention changes in lowerincisor alignment, and (3) attempt to identify anydescriptive, cast, or cephalometric variables whichmight aid the clinician in controlling long-termchanges or predicting future changes.
Materials and methods
Pre-treatment (T1), post-treatment (T2), andpost-retention (T3) patient records includingdental casts, lateral cephalograms, facial photo-graphs, and treatment records of large sample(N ¼ 114) treated by one clinician using con-ventional edgewise appliances and Tweed diag-nostic principles and mechanotherapy wereobtained. No subjects in the sample received anyinterproximal re-approximation during the post-treatment period.
All lateral cephalograms were taken with thesame unit (Weber, model #6B; Reeve Dental
Supply, 1421 Champion Drive #317, Carrollton,TX 75006). Cephalometric variables wereobtained using the Dentofacial Planner SoftwareSystem (Dentofacial Software Inc, 1 First Cana-dian Place, P.O. Box 300, Toronto, CanadaM5X 1C9).
Cephalometric angular measurements wereincluded as described in the cephalometricanalyses by Downs,24 Steiner,25 and Legan andBurstone.26
Cephalometric linear measurements wereincluded as described in the cephalometric analy-ses by Steiner,25 Harvold,27 Bjork/Jarabak (Jarabakand Fizzell),28 Ricketts,29 and McNamara.30
Mitutoyo electronic digital calipers (MitutoyoCorporation, 31-19 Shiba 5-Chome, Manato-Ku,Tokyo 108, Japan) were used to measure dentalcast variables to the nearest 0.01 mm.
Dental cast measurements included man-dibular total crowding, mandibular anteriorcrowding, overbite, overjet, mandibular archlength, mandibular arch width, inter-first molarwidth, first and second inter-premolar width, andincisor irregularity index as suggested by Little.31
The entire sample was evaluated as a unit ateach time interval (T1, T2, and T3), as well aslongitudinally (T1–T2, T2–T3, and T1–T3). A finalsubdivision was then made on the basis of post-retention lower incisor irregularity using Little'sIrregularity Index (Little)31 of 3.5 mm as a cutoff.Subjects at T3 demonstrating “moderate” (clini-cally unacceptable) changes in post-retentionlower incisor alignment (irregularity index43.5 mm) were placed in group 1 (N¼ 24). Thisgroup was then matched and compared to asimilar-sized group (group 2, N ¼ 30) demon-strating only “minor” (clinically acceptable,irregularity index o3.5 mm) changes in lowerincisor alignment at post-retention. The follow-ing matching criteria were used (prioritized) atT1: age, anterior crowding, gender, ANB, andAngle classification. Characteristics of groups 1and 2 are presented in Table 1. It should bepointed out that since groups 1 and 2 werematched in part on the basis of initial (T1) age,there was a disparity in mean post-retention time(Table 1). This final breakdown of the entiresample on the basis of “minor” and “moderate”incisor irregularity indices was done in anattempt to better detect statistically significantdifferences among the various descriptive, cast,and cephalometric parameters included.

Table 1. Characteristics of group 1 and group 2
Group 1 (“moderate change”) Group 2 (“minor change”)Number of subjects 24 30
Sex Male: 3 Male: 8Female: 21 Female: 22
Age (y) T1: 13.00 (range 8.25–26.50) T1: 12.76 (range 11.83–14.08)T2: 16.79 (range 13.17–29.42) T2: 15.30 (range 14.00–16.75)T3: 34.92 (range 24.83–45.75) T3: 29.33 (range 22.83–37.92)
Angle classification (first molar and cuspid) Class I: 4 Class I: 7Class II division 1: 18 Class II division 1: 22Class II division 2: 2 Class II division 2: 1
Treatment Extraction: 21 Extraction: 26Non-extraction: 3 Non-extraction: 4
Post-retention (y) 15.95 (range 8.25–24.00) 10.76 (range 5.00–19.67)
Searching for Predictors of Long-term Stability 281
Analysis of data
The entire sample (N ¼ 114) and individualsubgroups were subjected to descriptive statisticssuch as themean (X ) and standard deviation (SD)at each of the three evaluations (T1, T2, and T3) aswell as longitudinally (T1–T2, T2–T3, and T1–T3).In addition, between-group and within-groupcomparisons were made using independent andpaired Student's t-tests, respectively. A PearsonProduct-Moment correlation coefficient was usedto assess possible associations among variables anda level of clinical significance was established at r¼0.6. Multiple regression analysis was used in anattempt to establish predictive indicators for boththemandibular incisor irregularity index (Little)31
and anterior crowding.32 The significance levelwas set at po 0.01. All statistics were performed onSPSS (version 6.1) statistics software.
Error analysis
Intra-examiner measurement error was deter-mined by random selection and re-measurementof 10 dental casts and 10 lateral cephalograms (alsore-digitized) 1 week following the original meas-urements. Pearson product-moment correlationcoefficients and paired t-tests were used to identifysignificant differences between the measurements.
Results
The results for differences between groups 1 and2 are portrayed in Table 2.
Dental cast data
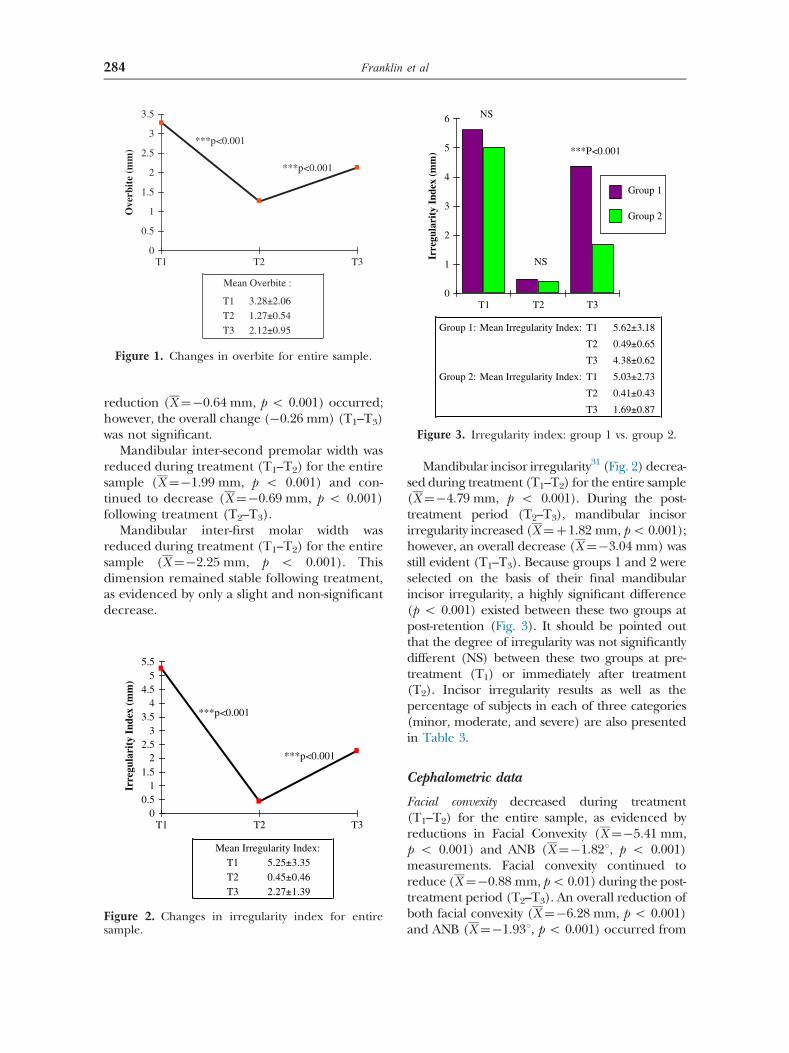
Overbite was reduced during treatment (T1–T2)for the entire sample (X ¼�2:0 mm, p o 0.001).
During the post-treatment period (T2–T3), overbiteincreased (X ¼þ0:85 mm, p o 0.001); however,an overall decrease (X ¼–1:15 mm, p o 0.001) inoverbite remained post-retention (T1–T3).
Overjet was reduced during treatment (T1–T2)for the entire sample (X ¼�3:91 mm, po 0.001).During the post-treatment period (T2–T3),an increase in overjet occurred (X ¼þ0:54 mm,po 0.001); however, there was an overall decrease(X ¼�3:37 mm, p o 0.001) at post-retention(T1–T3) (Fig. 1).
Mandibular arch length was reduced duringtreatment (T1–T2) for the entire sample(X ¼�7:98 mm, p o 0.001). Arch length con-tinued to decrease (X ¼�2:12 mm, p o 0.001)during the post-treatment period (T2–T3). Notsurprisingly, subjects in the extraction subgroupexhibited significantly shorter mandibular archlengths at post-treatment and post-retention thansubjects in the non-extraction subgroup (p o0.001).
Mandibular intercanine width increased dur-ing treatment (T1–T2) for the entire sample(X ¼þ0:97 mm, p o 0.001). This dimensiondecreased (X ¼�1:45 mm, p o 0.001) duringthe post-treatment period (T2–T3), resulting in apost-retention value that was 0.45 mm less (p o0.001) than the pre-treatment value. Group 1(“moderate change”) experienced a 0.78 mmgreater increase in mandibular intercanine widththan group 2 (“minor change”) during treatment(T1–T2). However, group 1 subsequently showeda 1.26 mm greater decrease in mandibularintercanine width than group 2 following treat-ment (p o 0.001).
Mandibular inter-first premolar width was notsignificantly altered during treatment (T1–T2) forthe entire sample. Following treatment (T2–T3), a
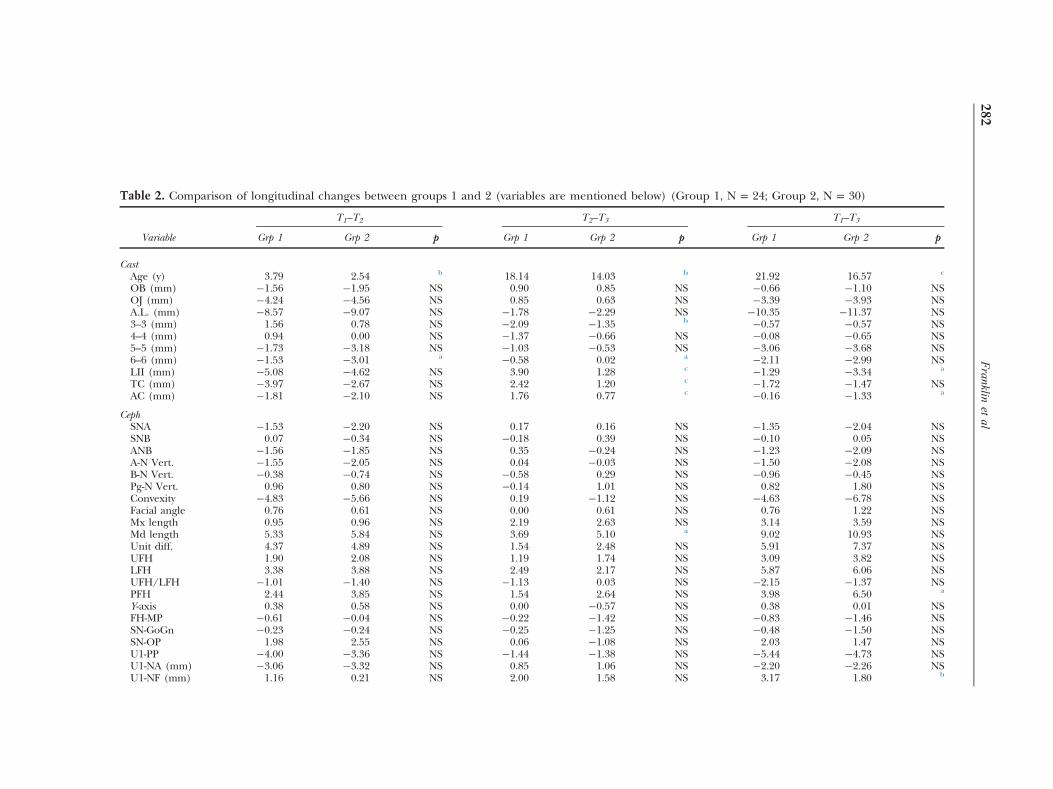
Table 2. Comparison of longitudinal changes between groups 1 and 2 (variables are mentioned below) (Group 1, N = 24; Group 2, N = 30)
T1–T2 T2–T3 T1–T3
Variable Grp 1 Grp 2 p Grp 1 Grp 2 p Grp 1 Grp 2 p
CastAge (y) 3.79 2.54 b 18.14 14.03 b 21.92 16.57 c
OB (mm) �1.56 �1.95 NS 0.90 0.85 NS �0.66 �1.10 NSOJ (mm) �4.24 �4.56 NS 0.85 0.63 NS �3.39 �3.93 NSA.L. (mm) �8.57 �9.07 NS �1.78 �2.29 NS �10.35 �11.37 NS3–3 (mm) 1.56 0.78 NS �2.09 �1.35 b �0.57 �0.57 NS4–4 (mm) 0.94 0.00 NS �1.37 �0.66 NS �0.08 �0.65 NS5–5 (mm) �1.73 �3.18 NS �1.03 �0.53 NS �3.06 �3.68 NS6–6 (mm) �1.53 �3.01 a �0.58 0.02 a �2.11 �2.99 NSLII (mm) �5.08 �4.62 NS 3.90 1.28 c �1.29 �3.34 a
TC (mm) �3.97 �2.67 NS 2.42 1.20 c �1.72 �1.47 NSAC (mm) �1.81 �2.10 NS 1.76 0.77 c �0.16 �1.33 a
CephSNA �1.53 �2.20 NS 0.17 0.16 NS �1.35 �2.04 NSSNB 0.07 �0.34 NS �0.18 0.39 NS �0.10 0.05 NSANB �1.56 �1.85 NS 0.35 �0.24 NS �1.23 �2.09 NSA-N Vert. �1.55 �2.05 NS 0.04 �0.03 NS �1.50 �2.08 NSB-N Vert. �0.38 �0.74 NS �0.58 0.29 NS �0.96 �0.45 NSPg-N Vert. 0.96 0.80 NS �0.14 1.01 NS 0.82 1.80 NSConvexity �4.83 �5.66 NS 0.19 �1.12 NS �4.63 �6.78 NSFacial angle 0.76 0.61 NS 0.00 0.61 NS 0.76 1.22 NSMx length 0.95 0.96 NS 2.19 2.63 NS 3.14 3.59 NSMd length 5.33 5.84 NS 3.69 5.10 a 9.02 10.93 NSUnit diff. 4.37 4.89 NS 1.54 2.48 NS 5.91 7.37 NSUFH 1.90 2.08 NS 1.19 1.74 NS 3.09 3.82 NSLFH 3.38 3.88 NS 2.49 2.17 NS 5.87 6.06 NSUFH/LFH �1.01 �1.40 NS �1.13 0.03 NS �2.15 �1.37 NSPFH 2.44 3.85 NS 1.54 2.64 NS 3.98 6.50 a
Y-axis 0.38 0.58 NS 0.00 �0.57 NS 0.38 0.01 NSFH-MP �0.61 �0.04 NS �0.22 �1.42 NS �0.83 �1.46 NSSN-GoGn �0.23 �0.24 NS �0.25 �1.25 NS �0.48 �1.50 NSSN-OP 1.98 2.55 NS 0.06 �1.08 NS 2.03 1.47 NSU1-PP �4.00 �3.36 NS �1.44 �1.38 NS �5.44 �4.73 NSU1-NA (mm) �3.06 �3.32 NS 0.85 1.06 NS �2.20 �2.26 NSU1-NF (mm) 1.16 0.21 NS 2.00 1.58 NS 3.17 1.80 b
Franklin
etal
282
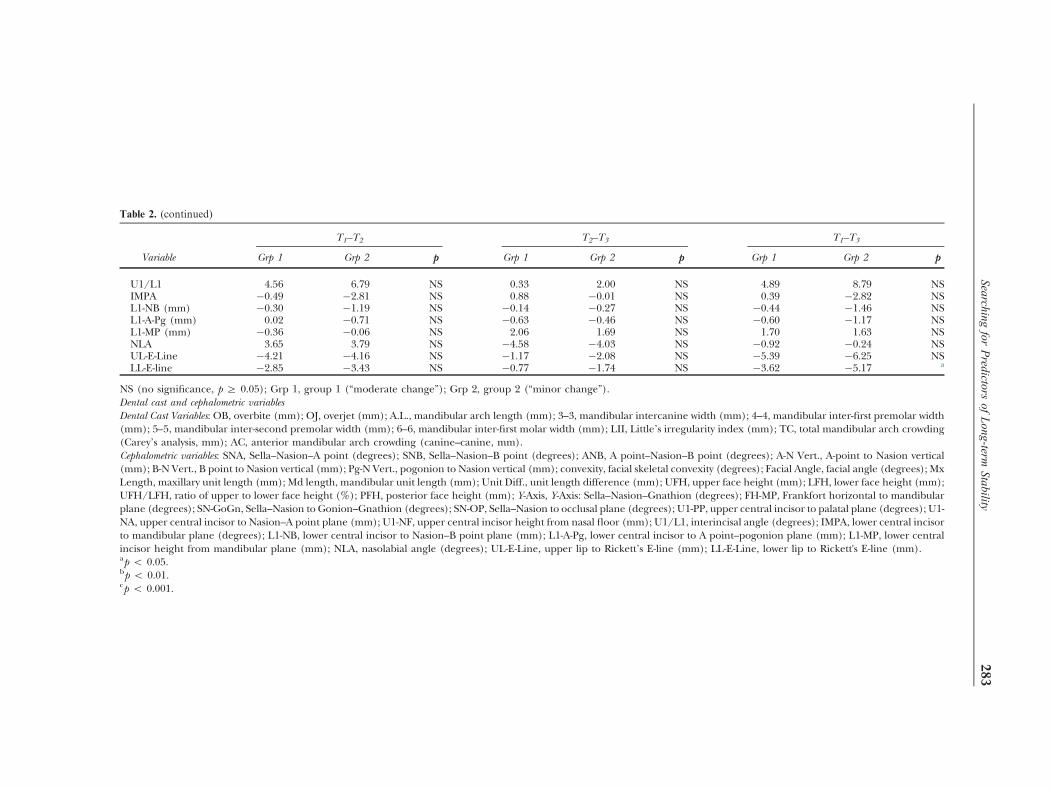
Table 2. (continued)
T1–T2 T2–T3 T1–T3
Variable Grp 1 Grp 2 p Grp 1 Grp 2 p Grp 1 Grp 2 p
U1/L1 4.56 6.79 NS 0.33 2.00 NS 4.89 8.79 NSIMPA �0.49 �2.81 NS 0.88 �0.01 NS 0.39 �2.82 NSL1-NB (mm) �0.30 �1.19 NS �0.14 �0.27 NS �0.44 �1.46 NSL1-A-Pg (mm) 0.02 �0.71 NS �0.63 �0.46 NS �0.60 �1.17 NSL1-MP (mm) �0.36 �0.06 NS 2.06 1.69 NS 1.70 1.63 NSNLA 3.65 3.79 NS �4.58 �4.03 NS �0.92 �0.24 NSUL-E-Line �4.21 �4.16 NS �1.17 �2.08 NS �5.39 �6.25 NSLL-E-line �2.85 �3.43 NS �0.77 �1.74 NS �3.62 �5.17 a
NS (no significance, p Z 0.05); Grp 1, group 1 (“moderate change”); Grp 2, group 2 (“minor change”).Dental cast and cephalometric variablesDental Cast Variables: OB, overbite (mm); OJ, overjet (mm); A.L., mandibular arch length (mm); 3–3, mandibular intercanine width (mm); 4–4, mandibular inter-first premolar width(mm); 5–5, mandibular inter-second premolar width (mm); 6–6, mandibular inter-first molar width (mm); LII, Little’s irregularity index (mm); TC, total mandibular arch crowding(Carey’s analysis, mm); AC, anterior mandibular arch crowding (canine–canine, mm).Cephalometric variables: SNA, Sella–Nasion–A point (degrees); SNB, Sella–Nasion–B point (degrees); ANB, A point–Nasion–B point (degrees); A-N Vert., A-point to Nasion vertical(mm); B-N Vert., B point to Nasion vertical (mm); Pg-N Vert., pogonion to Nasion vertical (mm); convexity, facial skeletal convexity (degrees); Facial Angle, facial angle (degrees); MxLength, maxillary unit length (mm); Md length, mandibular unit length (mm); Unit Diff., unit length difference (mm); UFH, upper face height (mm); LFH, lower face height (mm);UFH/LFH, ratio of upper to lower face height (%); PFH, posterior face height (mm); Y-Axis, Y-Axis: Sella–Nasion–Gnathion (degrees); FH-MP, Frankfort horizontal to mandibularplane (degrees); SN-GoGn, Sella–Nasion to Gonion–Gnathion (degrees); SN-OP, Sella–Nasion to occlusal plane (degrees); U1-PP, upper central incisor to palatal plane (degrees); U1-NA, upper central incisor to Nasion–A point plane (mm); U1-NF, upper central incisor height from nasal floor (mm); U1/L1, interincisal angle (degrees); IMPA, lower central incisorto mandibular plane (degrees); L1-NB, lower central incisor to Nasion–B point plane (mm); L1-A-Pg, lower central incisor to A point–pogonion plane (mm); L1-MP, lower centralincisor height from mandibular plane (mm); NLA, nasolabial angle (degrees); UL-E-Line, upper lip to Rickett’s E-line (mm); LL-E-Line, lower lip to Rickett's E-line (mm).ap o 0.05.bp o 0.01.cp o 0.001.
Searchingfor
Predictors
ofLong-term
Stability283
Ove
rbit
e (m
m)
0
0.5
1
1.5
2
2.5
3
3.5
T1 T2 T3
***p<0.001
***p<0.001
Mean Overbite :
T1 3.28±2.06
T2 1.27±0.54
T3 2.12±0.95
Figure 1. Changes in overbite for entire sample.
Irre
gula
rity
Ind
ex (
mm
)
0
1
2
3
4
5
6
T1 T2 T3
Group 1
Group 2
NS
NS
***P<0.001
Group 1: Mean Irregularity Index: T1 5.62±3.18
T2 0.49±0.65
T3 4.38±0.62
Group 2: Mean Irregularity Index: T1 5.03±2.73
T2 0.41±0.43
T3 1.69±0.87
Figure 3. Irregularity index: group 1 vs. group 2.
Franklin et al284
reduction (X ¼�0:64 mm, p o 0.001) occurred;however, the overall change (�0.26 mm) (T1–T3)was not significant.
Mandibular inter-second premolar width wasreduced during treatment (T1–T2) for the entiresample (X ¼�1:99 mm, p o 0.001) and con-tinued to decrease (X ¼�0:69 mm, p o 0.001)following treatment (T2–T3).
Mandibular inter-first molar width wasreduced during treatment (T1–T2) for the entiresample (X ¼�2:25 mm, p o 0.001). Thisdimension remained stable following treatment,as evidenced by only a slight and non-significantdecrease.
Irre
gula
rity
Ind
ex (
mm
)
00.5
11.5
22.5
33.5
44.5
55.5
T1 T2 T3
***p<0.001
***p<0.001
Mean Irregularity Index:T1 5.25±3.35T2 0.45±0.46T3 2.27±1.39
Figure 2. Changes in irregularity index for entiresample.
Mandibular incisor irregularity31 (Fig. 2) decrea-sed during treatment (T1–T2) for the entire sample(X ¼�4:79 mm, p o 0.001). During the post-treatment period (T2–T3), mandibular incisorirregularity increased (X ¼þ1:82 mm, po 0.001);however, an overall decrease (X ¼�3:04 mm) wasstill evident (T1–T3). Because groups 1 and 2 wereselected on the basis of their final mandibularincisor irregularity, a highly significant difference(p o 0.001) existed between these two groups atpost-retention (Fig. 3). It should be pointed outthat the degree of irregularity was not significantlydifferent (NS) between these two groups at pre-treatment (T1) or immediately after treatment(T2). Incisor irregularity results as well as thepercentage of subjects in each of three categories(minor, moderate, and severe) are also presentedin Table 3.
Cephalometric data
Facial convexity decreased during treatment(T1–T2) for the entire sample, as evidenced byreductions in Facial Convexity (X ¼�5:41 mm,p o 0.001) and ANB (X ¼�1:821, p o 0.001)measurements. Facial convexity continued toreduce (X ¼�0:88 mm, po 0.01) during the post-treatment period (T2–T3). An overall reduction ofboth facial convexity (X ¼�6:28 mm, p o 0.001)and ANB (X ¼�1:931, p o 0.001) occurred from

Table 3. Mandibular incisor irregularity for entire sample and individual subgroups
Group Irregularity index (mm) Percentage distribution at T3
T1 T2 T3 Minor(o3.5 mm) (%)
Moderate(3.5–6.5 mm ) (%)
Severe(46.5 mm) (%)
Entire sample 5.25 0.45 2.27 78.9 21.1 0Males 5.58 0.36 1.75 90.9 9.1 0Females 5.14 0.48 2.48 74.1 25.9 0Extraction 5.84 0.41 2.28 77.7 22.3 0Non-extraction 2.77 0.60 2.24 85.0 15.0 0Class I 7.15 0.39 2.03 88.2 11.8 0Class II 4.41 0.47 2.37 75.0 25.0 0
Searching for Predictors of Long-term Stability 285
pre-treatment to post-retention (T1–T3) (Table 2).Males exhibited significantly less facial convexitythan females at post-treatment (p o 0.01) andpost-retention (p o 0.001).
Mandibular rotation
Statistically significant changes were found inmandibular rotation measurements for the entiresample during treatment (T1–T2). These minimalchanges are depicted by a mean increase of only0.411 in the Y-axis angle (p o 0.01). Minimal butstatistically significant, changes also occurred in theY-axis angle from post-treatment to post-retention(T2–T3). The Y-axis angle returned to near itsoriginal value (X ¼�0:471, po 0.001), resulting inan overall change (T1–T3) that was not significant.Males showed higher values for the Y-axis and FHto MP angles than females at post-retention (p o0.01). The extraction subgroup showed highervalues for Y-axis, FH toMP, and SN to GoGn anglesat pre-treatment (p o 0.001) and post-treatment(p o 0.01), but only small and non-significantdifferences at post-retention. No statistically sig-nificant differences in mandibular rotation werefound between Class I and Class II subgroups orbetween groups 1 and 2 at post-treatment and post-retention.
In order to more closely examine mandibularrotation and its relationship to mandibular incisorirregularity, lateral cephalograms for the subjects ingroups 1 and 2 were superimposed at all three timeperiods (T1, T2, and T3). An average (mean)rotation value of the mandible (Gnathion relativeto the S–N plane) was determined for each subjectin both groups. Group means were then calculatedand compared to see if the two groups had sig-nificantly different mandibular growth directionsor rotations across time (T1–T3). Results of thiscomparison showed that the mean mandibular
rotation across time was nearly identical for the twogroups, as evidenced by values of 68.661� 3.61 and68.411 � 3.69 for groups 1 and 2, respectively.
Facial heights
Linearmeasurements of anterior facial height showedincreases in both upper face height (X ¼þ2:49 mm,p o 0.001) and lower face height (X ¼þ3:95 mm,p o 0.001) for the entire sample during treat-ment (T1–T2). Increases continued followingtreatment (T2–T3) for both upper face height(X ¼þ1:56 mm, p o 0.001) and lower faceheight (X ¼þ2:35 mm, p o 0.001). The linearmeasurement of posterior facial height showed anincrease (X ¼þ3:32 mm, p o 0.001) for theentire sample during treatment (T1–T2), and afurther increase (X ¼þ3:04 mm, p o 0.001)following treatment (T2–T3). Group 2 showed aslightly larger posterior face height measurementthan group 1 (p o 0.05) at post-retention (T3).
Anteroposterior incisor positions
Treatment produced a retroclination of themaxillary incisors for the entire sample, as evi-denced by changes in the U1 to PP value(X ¼�2:061, p o 0.05). The maxillary incisorscontinued to retrocline relative to the palatalplane following treatment (X ¼�1:311, po 0.01).
Vertical incisor positions
Maxillary incisor heights were not altered signifi-cantly during treatment for the entire sample.Following treatment, however, an increaseoccurred, as shown by an increase in the U1 toNF value (X ¼þ1:68 mm, p o 0.001).
Mandibular incisor heights remained relativelyunchanged during treatment for the entire sample.Following treatment, however, an increase in

Franklin et al286
mandibular incisor height occurred, as shownby an increase in the L1 to MP value(X ¼þ1:89 mm, p o 0.001).
Soft tissue changes
The distance from both upper lip to E-Line(X ¼�4:35 m, po 0.001) and lower lip to E-Line(X ¼�3:28 mm, p o 0.001) reduced duringtreatment for the entire sample. Reductionscontinued to occur during the post-treatmentperiod in both variables (p o 0.001).
Interparameter correlations (Pearson product-moment correlation coefficients). None of thedental cast or cephalometric variables correlatedsignificantly (r 4 0.6) with the post-retentionmeasures of mandibular incisor irregularity orcrowding. However, some of the cast andcephalometric variables were correlated witheach other at different time periods (T1, T2,and T3) making regression analysis for predictionpossible.
Prediction of post-retention mandibular incisorirregularity (multiple regression analysis). Anattempt was made to identify any pre- or post-treatment dental cast variables, combinations ofvariables, or changes in variables across time (T1–
T2 and T2–T3) that might serve as clinically usefulpredictors of the post-retention mandibularincisor alignment or changes in alignment fromT2–T3. Therefore, irregularity index
31 and anteriorcrowding at post-retention as well as the changes inthese variables from post-treatment to post-retention were used as dependent variables inthe regression model. The significance of the t-value of the β coefficient assigned to the particularvariable had to be p o 0.05 for inclusion in theregression model.The general formula for the regression equa-
tion is as follows:
Y ¼ b0þb1x1þb2x2þ⋯þbnxn
where : Y ¼ dependent variable, b ¼ Y-intercept,b1 – bn ¼ β coefficients of the independentvariables, and x1–xn ¼ independent variablesThose subjects from the entire sample who
demonstrated clinically unacceptable incisoralignment (43.5 mm) at post-retention (group1, N¼ 24) were further analyzed in an attempt toidentify specific factors that might help the
orthodontist predict future incisor instability.Multiple regression analysis showed the followingthree independent variables combined toexplain 65.8% of the variation in incisor irreg-ularity at post-retention: L1 to A-Pg (T2), U/L faceheight ratio (T1), andMx/Md unit difference (T1). Ofthe three variables, L1 to A-Pg (T2) accounted forthe majority of the variation.Those subjects from the entire sample who
demonstrated good stability of lower incisoralignment (o3.5 mm) at post-retention (group2, N ¼ 30) were also analyzed in an attempt toidentify predictors of long-term incisor alignment.Interestingly, the following three independentvariables combined to explain 49.3% of thevariation in incisor irregularity at post-retention:Posterior Face Height (T2), Arch Length (T2), andUpper to Lower Face Height Ratio (T1). Furthermore,the following three variables combined to explain51.3% of the variation in the change in incisorirregularity from T2–T3: SN to GoGn (T2), Age (T1),and A point to Nasion Vertical (T2).
Error analysis
Paired t-tests failed to show any statistically sig-nificant (p o 0.05) differences between first andsecond measurements during intra-examinererror determination; therefore, no systematicerrors in measurement occurred.
Discussion and clinical implications
The study is unique as three difficult aspects of anorthodontic clinical study is satisfied; that is, asufficiently large sample of subjects studied, apost-retention time that can truly be considered“long-term”(mean of 11.97 years), and treatmentperformed by one clinician following one specificphilosophy of treatment.
Overbite and overjet demonstrated reason-able stability following treatment. Changes lessthan 1mm were observed. Overcorrection inmost cases required a slight “rebound” followingactive treatment in order to establish normaloverbite and coupling of the incisors. Similarfindings were reported by Glenn et al.33 andPaquette et al.8 Class II subjects exhibited agreater degree of overbite at post-retention thanthe Class I subjects (p o 0.01).
Not surprisingly, the present study agrees withprevious findings from studies of both treated and
Searching for Predictors of Long-term Stability 287
untreated occlusions that mandibular intercaninewidth typically decreases with time.2,12,33,34 Thepost-treatment changes observed in intercaninewidth were most likely a reflection of maturationalchanges in the dentition rather than the influencesof orthodontic treatment. One particularly note-worthy finding was that the mandibular inter-canine width in group 1 (“moderate change”) wasincreased twice as much during treatment (T1–T2)compared to group 2 (“minor change”). Followingtreatment (T2–T3), group 1 showed a significantlygreater reduction in this dimension than group 2(p o 0.01). Moreover, these differences in inter-canine width changes between groups 1 and 2 mayalso partly explain the dichotomy in post-retentionincisor alignment.
Inter-first molar width demonstrated the beststability of any of the arch dimension parametersinvestigated in this study. A statistically significantreduction in inter-first molar width occurredduring treatment (p o 0.001) for the entiresample. The findings on inter-first molar width inthe present study coincide with those fromstudies on both untreated occlusions9–12 andorthodontically treated occlusions.33,35
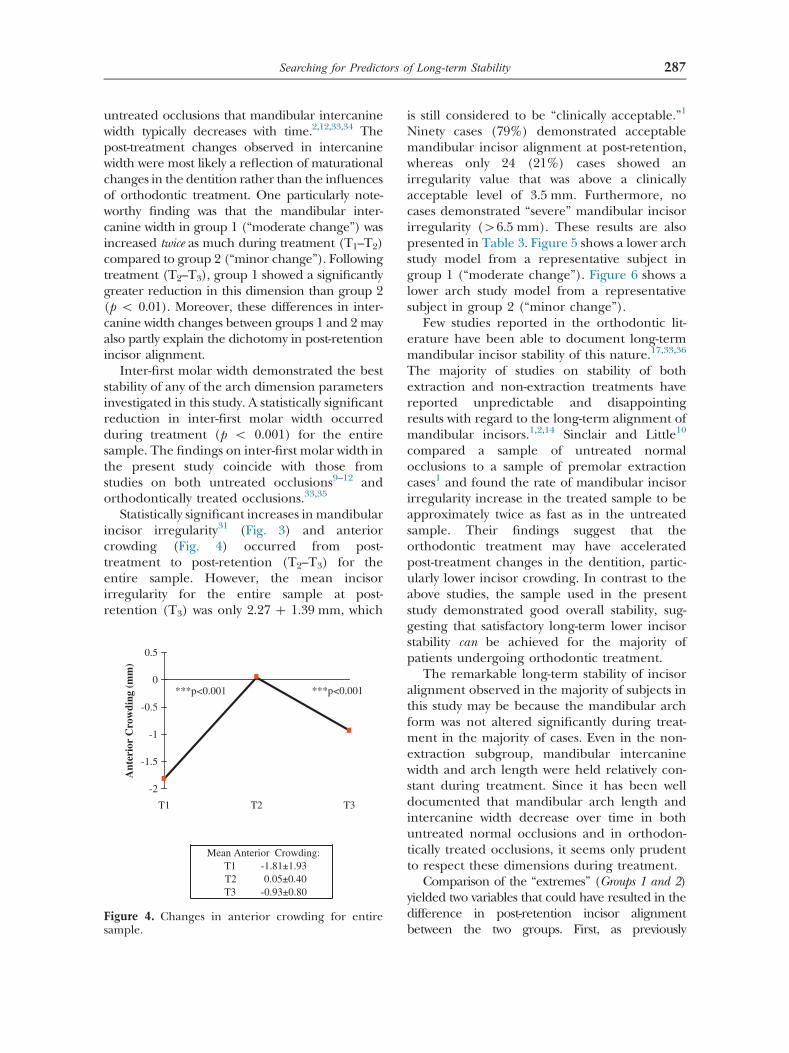
Statistically significant increases in mandibularincisor irregularity31 (Fig. 3) and anteriorcrowding (Fig. 4) occurred from post-treatment to post-retention (T2–T3) for theentire sample. However, the mean incisorirregularity for the entire sample at post-retention (T3) was only 2.27 þ 1.39 mm, which
Ant
erio
r C
row
ding
(m
m)
-2
-1.5
-1
-0.5
0
0.5
T1 T2 T3
***p<0.001 ***p<0.001
Mean Anterior Crowding: T1 -1.81±1.93T2 0.05±0.40T3 -0.93±0.80
Figure 4. Changes in anterior crowding for entiresample.
is still considered to be “clinically acceptable.”1
Ninety cases (79%) demonstrated acceptablemandibular incisor alignment at post-retention,whereas only 24 (21%) cases showed anirregularity value that was above a clinicallyacceptable level of 3.5 mm. Furthermore, nocases demonstrated “severe” mandibular incisorirregularity (46.5 mm). These results are alsopresented in Table 3. Figure 5 shows a lower archstudy model from a representative subject ingroup 1 (“moderate change”). Figure 6 shows alower arch study model from a representativesubject in group 2 (“minor change”).
Few studies reported in the orthodontic lit-erature have been able to document long-termmandibular incisor stability of this nature.17,33,36
The majority of studies on stability of bothextraction and non-extraction treatments havereported unpredictable and disappointingresults with regard to the long-term alignment ofmandibular incisors.1,2,14 Sinclair and Little10
compared a sample of untreated normalocclusions to a sample of premolar extractioncases1 and found the rate of mandibular incisorirregularity increase in the treated sample to beapproximately twice as fast as in the untreatedsample. Their findings suggest that theorthodontic treatment may have acceleratedpost-treatment changes in the dentition, partic-ularly lower incisor crowding. In contrast to theabove studies, the sample used in the presentstudy demonstrated good overall stability, sug-gesting that satisfactory long-term lower incisorstability can be achieved for the majority ofpatients undergoing orthodontic treatment.
The remarkable long-term stability of incisoralignment observed in the majority of subjects inthis study may be because the mandibular archform was not altered significantly during treat-ment in the majority of cases. Even in the non-extraction subgroup, mandibular intercaninewidth and arch length were held relatively con-stant during treatment. Since it has been welldocumented that mandibular arch length andintercanine width decrease over time in bothuntreated normal occlusions and in orthodon-tically treated occlusions, it seems only prudentto respect these dimensions during treatment.
Comparison of the “extremes” (Groups 1 and 2)yielded two variables that could have resulted in thedifference in post-retention incisor alignmentbetween the two groups. First, as previously
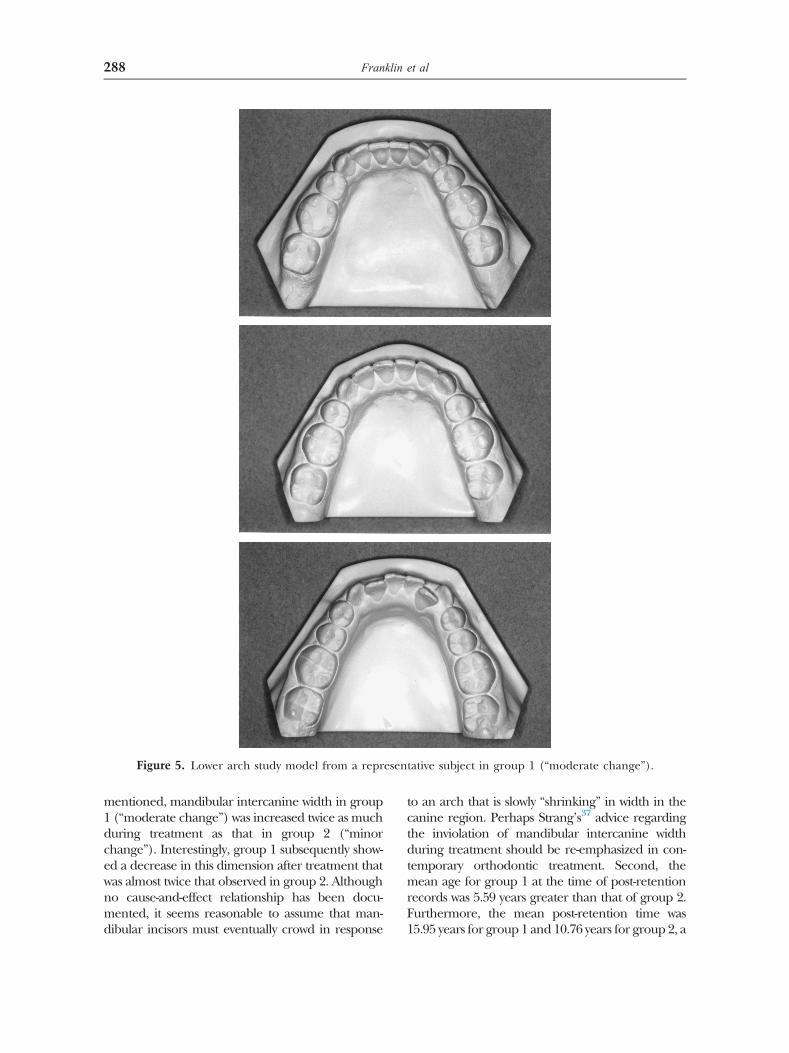
Figure 5. Lower arch study model from a representative subject in group 1 (“moderate change”).
Franklin et al288
mentioned, mandibular intercanine width in group1 (“moderate change”) was increased twice as muchduring treatment as that in group 2 (“minorchange”). Interestingly, group 1 subsequently show-ed a decrease in this dimension after treatment thatwas almost twice that observed in group 2. Althoughno cause-and-effect relationship has been docu-mented, it seems reasonable to assume that man-dibular incisors must eventually crowd in response
to an arch that is slowly “shrinking” in width in thecanine region. Perhaps Strang’s37 advice regardingthe inviolation of mandibular intercanine widthduring treatment should be re-emphasized in con-temporary orthodontic treatment. Second, themean age for group 1 at the time of post-retentionrecords was 5.59 years greater than that of group 2.Furthermore, the mean post-retention time was15.95 years for group 1 and 10.76 years for group 2, a

Figure 6. Lower arch study model from a representative subject in group 2 (“minor change”).
Searching for Predictors of Long-term Stability 289
difference of 5.19 years. These differences in finalage and post-retention time are important since ithas been shown that developmental crowdingoccurs as a part of the natural aging process.10,12
Sinclair and Little10 calculated a mean annualincrease in incisor irregularity of þ0.21 mm up tothe age of 20 years in a sample of treated individuals.If one uses this estimation (þ0.21 mm/y), it can beassumed that group 2 would have experienced an
additional 1 mm of lower incisor irregularity over anadditional 5 years of aging. Hence, a finalirregularity index of 2.69 mm (1.69 þ 1.0) can beprojected for group 2, which is still below the finalirregularity value of 4.38 mm found in group 1, andwell within the range of clinical acceptability31 andphysiological stability.38 It should be noted that themean annual rate of increase from Sinclair andLittle’s study10 was derived from a sample of

Franklin et al290
untreated subjects who showed more post-retentionirregularity than group 2 (X ¼3:5–4:8 mm vs.1.69 mm). Therefore, the calculated value of2.69 mm probably represents an over-estimation ofwhat might have actually occurred in group 2,further illustrating the remarkable stability of thesubjects in this group.
One of the most noteworthy findings was thecontrol of vertical skeletal proportions duringtreatment. Undesirable backward rotation of themandible was minimized during the treatmentperiod. In addition, anterior vertical facial pro-portions remained constant both during andafter treatment, while posterior face heightcontinued to increase from pre-treatment topost-retention. These changes represent normalpatterns of mandibular growth11,18,19 and furtherillustrate that treatment favored normal growth.
The reduction of facial convexity is a frequentobjective of orthodontic treatment, especially inpatients with Class II malocclusions. In thissample, facial convexity was reduced duringtreatment, as illustrated by the normalization ofthe ANB and Convexity angles from T1–T2.Following active treatment, A point (SNA angle)remained relatively constant, while the mandible(SNB angle) continued to grow in an anteriordirection. This post-treatment mandibulargrowth could play a role in the noted dentalchanges.
Maxillary and mandibular incisors wereantero-posteriorly positioned in conformity withTweed philosophy cephalometric and facialstandards. Thus, mandibular incisors were ret-roclined or maintained in their original ante-roposterior position, with no active advancementor proclination performed. In some cases,mandibular incisors were slightly over-corrected,leading to a slight “rebound” in an anteriordirection following active treatment. Althoughthe IMPA showed a stable position from T2–T3,the slight forward “rebound”may have assisted inthe creation of additional space to accommodatethe lower incisors as intercanine width and archlength decreased. Sandusky17 experienced asimilar finding in his study of long-term incisorstability.
In the vertical direction, neither maxillary normandibular incisors were altered significantlyduring treatment. Schudy39 suggested that theocclusal plane was more stable when the lowerincisors were not intruded during leveling.
Statistically significant increases in maxillaryand mandibular incisor heights were observedfrom post-treatment to post-retention, whichprobably reflect continued vertical growth of thealveolar processes. In addition, overbite wasslightly over-corrected in most cases, which mayhave resulted in a “rebound” in order to establishnormal overbite and coupling of the incisors.Group 1 (“moderate change”) experienced asignificantly greater increase in maxillary incisorheight from pre-treatment to post-retention thangroup 2 (“minor change”), which could havecontributed to the greater degree of mandibularincisor irregularity in group 1.
Soft tissue changes during and following activetreatment were also observed. Both upper andlower lips became more retrusive relative toRickett’s E-line29 during these time periods. Itshould be mentioned that these measurementsare functions of not only the position of the lipsbut also the positions of the anterior-most aspectsof the nose and chin. Therefore, one wouldexpect to see reductions in lip protrusion relativeto the nose and chin, especially after treatment,since it has been documented that the nose andsoft tissue chin become more prominent withage.11 One particularly important finding was thesimilarity in upper and lower lip positionsbetween extraction and non-extraction sub-groups at post-retention. This finding contradictsthe popular opinion that extraction treatment“flattens” the profile.
Prediction of long-term incisor irregularity
Multiple regression analysis of the entire sampledata failed to yield any clinically useful pre-dictors of the post-retention mandibular incisorirregularity or crowding. However, regressionanalysis of the group 1 (“moderate change”)data yielded independent variables that com-bined to explain the variation in incisor irreg-ularity at post-retention. Interestingly, theanterior–posterior post-treatment lower incisorposition considered in the regression equationby itself accounted for 41.5% of the variation inincisor irregularity at post-retention. Thus, forevery millimeter increase L1 to A-Pg at T2,incisor irregularity at T3 increased by 0.16 mm,when all other variables were held constant.Furthermore, the vertical dimension played arole in the regression analysis. It is noteworthy

Searching for Predictors of Long-term Stability 291
that when the changes in inter-first molar widthand maxillary length from T2–T3 were added tothe equation with L1 to A-Pg (T2–T3), 67% of thevariation in the change in anterior crowdingfrom T2–T3 was explained.
Multiple regression analysis of the group 2(“minor change”) data also revealed severalsignificant findings. Forty-nine percent of thevariation in incisor irregularity at post-retentionwas explained by a combination of the followingthree independent variables: Posterior Face Height(T2), Arch Length (T2), and Upper to Lower FaceHeight Ratio (T1). For every millimeter increase inposterior face height at T2, a decrease in incisorirregularity of 0.10 mm at T3 is produced. Thefollowing three independent variables combinedto explain 51.3% of the variation in the change inincisor irregularity from T2–T3: SN to GoGn (T2),Age (T1), and A-point to Nasion Vertical (T2). In thismodel, each degree increase in SN to GoGn at T2
elicited an increase in incisor irregularity of0.11 mm from T2–T3, while each year increase inage at T1 elicited an increase in incisor irregu-larity of 0.55 mm from T2–T3. It is apparent thatthe vertical dimension features also in this group.
Clinical implications
In contrast to many of the published findings onthe stability of orthodontic treatment, this studyoffers a degree of optimism. First, it is extremelyimportant for the orthodontist to know thatsatisfactory long-term stability can be achieved inthe majority of patients if sound treatmentprinciples are followed. These principlesincluded the maintenance of mandibular archform during treatment, in particular intercaninewidth, as well as treating to near-ideal cephalo-metric and clinical standards.
Second, it appears that there are several varia-bles that may aid in predicting the outcome of thelower incisors following treatment. In particular,lower incisor to the A-Pg plane at T2 appears to beone variable with considerable predictive value ofthe final incisor alignment. In addition, post-treatment vertical skeletal dimensions, such asposterior face height and SN to GoGn, may havesome value for predicting the post-retention incisoralignment. Furthermore, the patient’s age may bean important variable that should be consideredwhen planning a retention protocol.
Finally, we cannot escape the developmentalchanges that occur with aging. Hence, we shouldexpect some degree of changes in the dentition,especially lower incisor crowding, with time.38,40,41
Patients should always be well-informed before thecommencement of orthodontic treatment thatsome changes will occur, and that at present, theonly means of preventing these changes is withretention after treatment. Developmental changesin the dentition must not be interpreted as“relapse” associated with orthodontic treatment,unless improper treatment has been performed.
Conclusions
1.
Satisfactory long-term stability of the dentitionwas achieved in this sample.2.
Overbite and overjet showed clinically goodstability. It is recommended to overcorrectthese variables, example to an almost end-to-end relationship, and should some changeoccur post-treatment, the tendency of thechange will be in a direction towards theoriginal, thus establishing the norm.3.
Mandibular intercanine width generallydecreased in the long-term, even when min-imal expansion occurred during treatment. Itappeared that the greater the increase in thisdimension during treatment, the greater thedecrease after treatment. Minimal expansion,if at all, should be the treatment goal.4.
Useful clinical predictors of the long-term meas-ures of incisor irregularity required a combina-tion of variables in a regression equation.5.
The results from the regression analysissuggest that vertical management of treatmentcould play a role in stability. Vertical control isthe corner stone of all excellent orthodontictreatment and thus it is no surprise to seethese variables feature as indicated.References1. Little RM, Wallen TR, Riedel RA: Stability and relapse of
mandibular anterior alignment-first premolar extractioncases treated by traditional edgewise orthodontics. Am JOrthod 80:349-365, 1981
2. Little RM, Riedel RA, Artun J: An evaluation of changes inmandibular anterior alignment from 10 to 20 years post-retention. Am J Orthod Dentofac Orthop 93:423-428, 1988
3. Little RM, Riedel RA: Post-retention evaluation of stabilityand relapse—Mandibular arches with generalized spac-ing. Am J Orthod Dentofac Orthop 95:37-41, 1989

Franklin et al292
4. Ades AG, Joondeph DR, Little RM, Chapko MK: A long-term study of the relationship of third molars to changesin the mandibular dental arch. Am J Orthod DentofacOrthop 97:323-335, 1990
5. Little RM: Stability and relapse of dental arch alignment.Br J Orthod 17:235-241, 1990
6. Little RM, Riedel RA, Engst ED: Serial extraction of firstpremolars-post-retention evaluation of stability andrelapse. Angle Orthod 60:255-262, 1990
7. Little RM, Riedel RA, Stein A: Mandibular arch lengthincrease during the mixed dentition: post-retentionevaluation of stability and relapse. Am J Orthod DentofacOrthop 97:393-404, 1990
8. Paquette DE, Beattie JR, Johnston LE: A long-termcomparison of non-extraction and premolar extractionedgewise therapy in “borderline” Class II patients. Am JOrthod Dentofac Orthop 102:1-14, 1992
9. Moorrees CFA: The Dentition of the Growing Child.Cambridge, MA Harvard University Press; , 1959
10. Sinclair PM, Little RM: Maturation of untreated normalocclusions. Am J Orthod 83:114-123, 1983
11. Behrents RG: Growth in the Aging Craniofacial Skeleton.Monograph 17 Craniofacial Growth Series Ann Arbor,Michigan, Centre for Human Growth and Development,University of Michigan, 1985
12. Eslambolchi S, Woodside DG, Rossouw PE: A descriptivestudy of mandibular incisor alignment in untreatedsubjects. Am J Orthod Dentofac Orthop 133:343-353, 2008
13. Buschang PH, Shulman JD: IncisorcCrowding inuntreated persons 15–20 years of age: United States,1988–1994. Angle Orthod 73:502-508, 2003
14. McReynolds DC, Little RM: Mandibular second premolarextraction-post-retention evaluation of stability andrelapse. Angle Orthod 61:133-144, 1991
15. Shearer DH: Evaluation of Post-Retention MandibularIncisor Stability in Premolar Extraction Cases Treated bySerial Extraction Without Subsequent Fixed OrthodonticMechanotherapy Diploma Thesis, University of Toronto,Toronto, Canada, 1994
16. Uhde MD, Sadowsky C, Begole EA: Long-term stability ofdental relationships after orthodontic treatment. AngleOrthod 53:240-252, 1983
17. Sandusky WC: A Long-Term Postretention Study ofTweed Extraction Treatment Master’s Thesis, Universityof Tennessee, Memphis, Tennessee, 1983
18. Björk A: Prediction of mandibular growth rotation. Am JOrthod 55:585-599, 1969
19. Björk A, Skieller V: Facial development and tootheruption: an implant study at the age of puberty. Am JOrthod 62:339-383, 1972
20. Buschang PH, Baume RM, Nass GG: A craniofacial growthmaturity gradient for males and females between 4 and 16years of age. Am J Phys Anthrop 61:373-381, 1983
21. Woodside DG, Linder-Aronson S, Stubbs DO: Relation-ship between mandibular incisor crowding and nasalmucosal swelling. Proc Finn Dent Soc 87:127-138, 1991
22. Linder-Aronson S, Woodside DG, Hellsing E, EmersonW: Normalization of incisor position after adenoidec-tomy. Am J Orthod Dentof Orthop 103:412-427, 1993
23. Fundalej P, Artun J: Mandibular growth rotation effectson postretention stability of mandibular incisor align-ment. Angle Orthod 77:199-205, 2007
24. Downs WB: Variations in facial relationships; theirsignificance in treatment planning and progress. Am JOrthod 34:812-840, 1948
25. Steiner CC: The use of cephalometrics as an aid toplanning and assessing orthodontic treatment. Am JOrthod 46:721-735, 1960
26. Legan H, Burstone CJ: Soft tissue cephalometric analysisfor orthognathic surgery. J Oral Surg 38:744-751, 1980
27. Harvold EP: The Activator in Interceptive OrthodonticsSt.Louis, CV Mosby Company, 1974
28. Jarabak JR, Fizzell JA: 2nd ed. Technique and TreatmentWith Light-Wire Appliances 1. St. Louis, CV MosbyCompany, 1972
29. Ricketts RM: Perspectives in the clinical application ofcephalometrics. Angle Orthod 51:115-150, 1981
30. McNamara JA: A method of cephalometric evaluation.Am J Orthod 86:449-469, 1984
31. Little RM: The irregularity index: a quantitative score ofmandibular anterior alignment. Am J Orthod 68:554-563,1975
32. Carey CW: “Linear arch dimensions and tooth size” Anevaluation of the bone and dental structures in casesinvolving the possible reduction of dental units intreatment. Am J Orthod 35:762-775, 1949
33. Glenn G, Sinclair PM, Alexander RG: Non-extractionorthodontic therapy: post-treatment dental and skeletalstability. Am J Orthod Dentofac Orthop 92:321-328,1987
34. Sillman JH: Dimensional changes of the dental arches:longitudinal study from birth to 25 years. Am J Orthod50:824-841, 1964
35. Freeman BV: A Comparison of Post-Retention Mandib-ular Incisor Irregularity in Treated Class II Division 1Malocclusions Versus Untreated Class I Normals DiplomaThesis, University of Toronto, Toronto, Canada, 1993
36. Rossouw PE, Preston CB, Lombard CJ, Truter JW: Alongitudinal evaluation of the anterior border of thedentition. Am J Orthod Dentof Orthop 104:146-152, 1993
37. Strang R: The fallacy of denture expansion as a treatmentprocedure. Angle Orthod 19:12-22, 1949
38. Rossouw PE: Terminology: semantics of postorthodontictreatment changes in the dentition. Sem Orthod 5:138-141, 1999
39. Schudy FF: Concepts to live by. J Clin Orthod 27:121-122,1993
40. Little RM: Clinical implications of the University ofWashington post-retention studies. J Clin Orthod 43:645-651, 2009
41. Little RM, Robert M: Little on the University ofWashington post-retention Studies. J Clin Orthod43:723-727, 2009