
Screening Pharmaceuticals for Possible Carcinogenesis: Three Decades of Experience Supercourse...
30
Screening Pharmaceuticals for Possible Carcinogenesis: Three Decades of Experience Supercourse Lecture April 2, 2010 Gary D. Friedman, M.D., M.S. Adjunct Investigator and Former Director Kaiser Permanente Division of Research Consulting Professor of Epidemiology Department of Health Research and Policy Stanford University School of Medicine
-
date post
22-Dec-2015 -
Category
Documents
-
view
216 -
download
3
Transcript of Screening Pharmaceuticals for Possible Carcinogenesis: Three Decades of Experience Supercourse...

Screening Pharmaceuticals for Possible Carcinogenesis:
Three Decades of Experience
Supercourse Lecture April 2, 2010
Gary D. Friedman, M.D., M.S.
Adjunct Investigator and Former DirectorKaiser Permanente Division of Research
Consulting Professor of EpidemiologyDepartment of Health Research and Policy
Stanford University School of Medicine

Pharmaceuticals and Cancer Study:
Current team of investigators
Laurel A. Habel, Principal InvestigatorGary D. Friedman
Charles P. Quesenberry, Jr.James Chan
Natalia UdaltsovaNinah Achacoso
Kaiser Permanente Division of Research

Other contributors
Hans Ury Donna WellsJoe V. Selby Bruce FiremanStephan Van Den Eeden Sheng-Fang (Sophie) Jiang
Lisa Herrinton Nina OestreicherTamirah Haselkorn Elizabeth (Dawn) FlickAlice Whittemore Kristin SainaniStephan Woditschka Christopher Rowan*Christine Iodice*
*Pending as of August 2010
History
• FDA-supported drug reaction monitoring system at Kaiser Permanente1-3
• Initial data sources: pharmacy and clinics.
• Initial (1977) and subsequent NCI grant support for our screening-for-carcinogenesis studies

Initial Kaiser Permanente surveillance
• Drugs: 1969-1973 San Francisco KP pharmacy records: cohort of 143,574 subscribers who received prescribed drugs.
• Cancers– Pre-existing: 1968-9 manual SF hospital files– Incident
• Tumor registry: 1969-• Hospitalizations: 1971-• All manually confirmed, then only hospital• Later: total tumor registry coverage

Initial Kaiser Permanente surveillance (cont’d)
• Users of 215 most commonly dispensed drugs carefully followed up for cancer compared to non-users, adjusted only for age and sex.– >=500 prescriptions or >=300 recipients

Initial Kaiser Permanente surveillance (cont’d)
• Biennial analyses: each site, all combined– Lag analyses: 1-year, 2-year (to avoid
associations due to treatment of pre-diagnostic cancer symptoms)
– Optional dose-response, crudely based on number of dispensings
Initial Kaiser Permanente surveillance (cont’d)
• Associations found are just clues– Most due to chance or confounding– Select interesting ones for more detailed
study, mostly chart review of exposed cases, some comparisons with non-exposed cases, exposed non-cases
Evolving view of screening for associations
• “Hypothesis-seeking”
• “Data-dredging”
• “Hypothesis-free research”

Some accomplishments of our non-drug hypothesis-seeking
• Alcohol and coronary heart disease (1974)4
• Alcohol and blood pressure (1977)5
• Leukocyte count and coronary heart disease (1974)6
• Obesity and multiple myeloma (1994)7
Question of statistical significance and multiple comparisons
• Thousands of comparisons
• Adjustment controversial
• What we have done: – Switch from .05 to .01 for screening– Constantly emphasize in publications that
most of what we see is due to chance

Examples of confounding by prediagnostic cancer symptoms or
by indication• Observed positive associations
– Iron and large bowel cancer (anemia treated before the cancer, which has bled, is diagnosed)– Antacids or cimetidine and stomach cancer (treatment of ulcer-like symptoms of the cancer)– Tetracycline and lung cancer (treatment of exacerbations of chronic bronchitis in smokers, who are also prone to develop lung cancer)
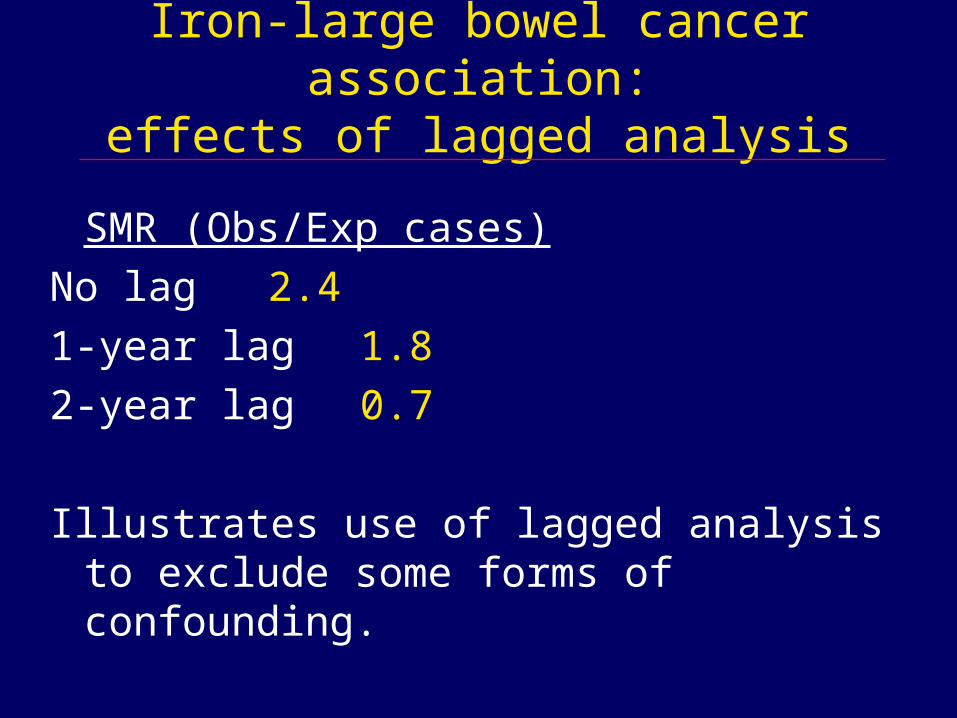
Iron-large bowel cancer association:effects of lagged analysis
SMR (Obs/Exp cases)
No lag 2.4
1-year lag 1.8
2-year lag 0.7
Illustrates use of lagged analysis to exclude some forms of confounding.
Findings in initial database
• Follow-up to 2002, up to 33 years
• 4 papers on screening results; follow-up up to 7, 9, 15, 19 years 8-11
• Not much that can’t be attributable to chance or confounding. Fairly reassuring.

Findings in initial database (cont’d)
• Association most studied: barbiturates and lung cancer. – Tumor promoter in rodent liver– In two follow-ups can’t readily rule out
confounding by smoking—too few cases in nonsmokers.12,13
– Negative association with bladder cancer in smokers.14

Findings in initial database (cont’d)
• We published several findings, most of which did not confirm drug/cancer associations, reported mostly by others– Antidepressive drugs15
– Cimetidine16
– Clofibrate9
– Digitalis17
– Diphenylhydantoin (phenytoin)8,10
– Iron18,19
– Lindane20
– Methylergonovine21
– Metronidazole8,22,23

Findings in initial database (cont’d)
• Additional published findings, most of which did not confirm drug/cancer associations, reported mostly by others– Phenylbutazone8,24
– Propoxyphene9,25
– Rauwolfia (reserpine)8,26
– Selenium sulfide11
– Several drugs with colon cancer27
– Spironolactone8
– Tertiary amine drugs including oxytetracycline8,9
Important source of data on humans
• IARC evaluations of carcinogenic risks to humans.
• Six monographs concerning pharmaceuticals, 1980 through 200128-33: our data were cited on 18 drugs.
• Our data were the only source concerning humans (other than case reports) for 9 of these.

New drug surveillance for possible carcinogenesis
• Pharmacy Information Management System (PIMS).• Phased in starting in 1991, with complete coverage of
all pharmacies in the Northern California Kaiser Permanente Medical Care Program by mid-1994.
• Over 3 million subscribers; more than 90% have at least partial financial coverage for prescriptions filled at Program pharmacies. Currently over 7 million current and former subscribers in this database.
• Follow-up for cancer in the Kaiser Permanente Cancer Registry, part of the national Surveillance, Epidemiology, and End Results (SEER) program.

Evolving statistical methods
• SIR: Standardized incidence ratio (formerly referred to as SMR, standardized morbidity ratio) Observed/expected cases, expected based on age-sex-specific incidence in non-users of the drug. Poisson test.
• Cox model: with age as time variable, control for calendar year to account for changes in drug use/cancer incidence
• Nested case-control analysis.– 10 then 50 person-time controls per case, matched
for age, sex, length of membership– Why so many controls? (Hennessy S. et al,
AJE;149:195-7, 1999)

50 vs 10 controls/case (1)
• Example: drug not commonly used by adults: methylphenidate (Ritalin), 3+ Rx’s
• Few exposed subjects, e.g., prostate cancer
OR(95% CI)– Exposed cases 10– Exposed controls (10/case) 52 1.92 (0.98-3.78)– Exposed controls (50/case) 218 2.30 (1.22-4.33)
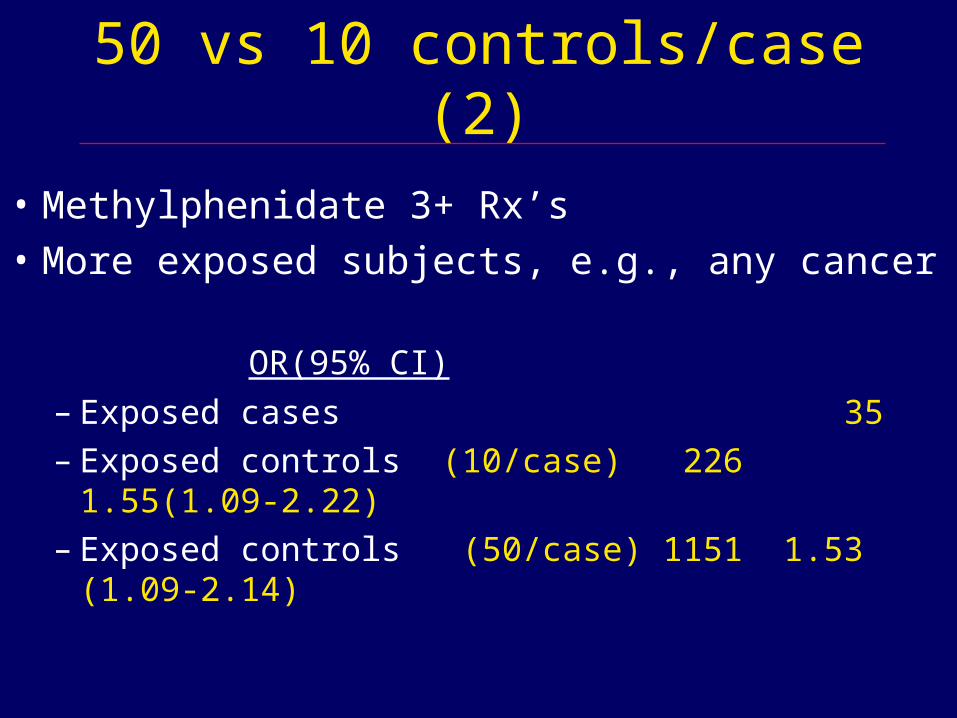
50 vs 10 controls/case (2)
• Methylphenidate 3+ Rx’s
• More exposed subjects, e.g., any cancer
OR(95% CI)
– Exposed cases 35– Exposed controls (10/case) 226 1.55(1.09-2.22)– Exposed controls (50/case) 1151 1.53 (1.09-2.14)

External adjustment
• Only confounders available for all subjects– Age, sex, length of membership (matched)– Some drugs, e.g., hormone use for female cancers– Need to control for others
• External adjustment using the method of Schneeweiss et al.; spreadsheet available for downloading from the Internet at www.drugepi.org
• Requires estimates of:– Confounder/drug use association– Confounder/outcome association– Prevalence of confounder– Prevalence of drug use

Example of external adjustment
• Statins and smoking-related cancers.
• Drug/confounder: linked pharmacy data to Member Health Survey
• Confounder/disease: literature
• Drug use prevalence: pharmacy, membership
• Confounder prevalence: Member Health Survey
• Statins/lung cancer/men: OR 1.060.82

External adjustment for sensitivity analysis
• Limitation: can only adjust for one variable• For sensitivity analysis of breast cancer37, we
generated a range of odds ratios by assuming – a dichotomy of overall risk among the subjects,
varying over a range of 3-fold to 1/3-fold – prevalence of high or low risk: 10%-50%– drug/high-or-low-risk association: 1.5, 2.0
• Example: reserpine, early data base (834 users) – OR (95% CI) 1.07 (0.74-1.55)– OR (sensitivity limits*) 1.07 (0.89-1.25)– Uncertainty due to chance>uncertainty due to
uncontrolled confounding.*Sensitivity limits are the OR’s that differed the most from the point
estimate given the above assumptions about confounding.

Some recent screening results
• Criteria for positive associations of interest– OR for 2-year lag, 3+ dispensings >=1.50, p<0.01– OR for 3+ dispensings > OR for 1 dispensing
(crude confirmation of dose-response)
• Recent paper 39 on 105 newly studied drugs• There were 101 positive associations for 61 drugs.• 66 associations were judged to have involved
substantial confounding– e.g., smoking-related cancers, corpus uteri with
antidiabetic drugs (both related to obesity)
• 35 associations probably not due to confounding
Associations deserving further study
• 35 associations probably not due to confounding• 11 with some evidence that may not be due to
chance-deserve further study.• Examples:
– sulindac and gallbladder cancer: sulindac is excreted in bile and its metabolites found in gallstones
– hydrochlorothiazide (HCTZ} and lip cancer: HCTZ is a photosensitizer and sun exposure is a risk factor for lip cancer
– fluoxetine (Prozac) and paroxetine (Paxil) and testicular cancer: both SSRI’s have been reported to cause testicular damage in rats at high doses
Comments about screening
• A reviewer for the journal suggested that we switch one of the screening criteria from p<0.01 to p<0.001.
• If this were done, we would have missed the sulindac/gallbladder cancer and the paroxetine/testicular cancer associations.
• Some reassuring findings confirming known associations using our criteria.– Hydrochlorothiazide and renal cancer– Cyclophosphamide and bladder cancer and myeloid
leukemia

Not just screening
• Also studies to help evaluate other findings about possible pharmaceutical carcinogens– Antibiotics and breast cancer: did not confirm except
weakly for tetracyclines and macrolides. Possible confounding by indication (acne) 35.
– Animal mammary carcinogens: weak support for furosemide and griseofulvin 37.
– IARC: drugs with limited evidence of carcinogenicity in humans; some supporting evidence for griseofulvin, metronidazole, and phenytoin38.
– Methylphenidate (Ritalin) (chromosomal abnormalities): some evidence for lymphocytic leukemia in children34.

Thanks and References
• Thank you for your interest in this lecture and our work
• References are provided in the note below.


















