
Scientific evidence for the benefits of walking and physical activity – and how to take the...
39
Scientific evidence for the benefits of walking and physical activity – and how to take the “next steps”
-
Upload
felicity-shields -
Category
Documents
-
view
213 -
download
0
Transcript of Scientific evidence for the benefits of walking and physical activity – and how to take the...
Scientific evidence for the
benefits of walking and
physical activity –
and how to take the “next
steps”

CHD
mood, anxiety, QOL, depression, socialbenefits,mental health
PhysicalActivity
Other possiblehealth benefits?prostate Ca. ?lung disease?breast cancerarthritis
diabetes colon cancerosteoporosis
BMI
BP
Cholesterol
Health benefits of physical activity
Stroke, CVD

0
20
40
60
80
100
1 3 5 7
Sandvik et al Ekelund et al Leon et alBlair et al Pafferbarger et al
CV
D M
ort
ality
, R
ela
tive
Ris
k
Level of Physical Fitness or Activity
Overall summary

Relative Risks (RR) of Total Mortality According to Level of Physical Activity Among 40 417 Post-
menopausal Women in Iowa, 1986-1992
Physical Activity Deaths Person-Years
Risk of death
Freq. of walking Rarely/never 722 55404 1.00 1/wk 621 76318 0.71 2-4 times/wk 560 82633 0.63 >4 times/wk 365 55973 0.59 Physical Activity Index Low 1309 126545 1.00 Medium 519 74170 0.77 High 415 67138 0.68

Nurses health study n=72,488 [>10 year
f/up] Walking and risk of CHD
Manson J, NEJM 1999;341:650-8
50
60
70
80
90
100
0 1 hr 3 hrs 7 hrs 10 hrs
time walked per week
Honolulu Heart health : walking & CVD risk
Elderly males
N=2678
Followed for 4 yrs
Hakim AA, Circulation 1999:100:9-13

Walking and CHD (Hakim 1999)
Effects on other risk factors
• Hypertension
• Lipid levels, HDL:total chol ratio
• Overweight and obesity – need 1 hour /day walking
Physiological benefits of walking
• Moderate to Brisk walking
• May help cardiovascular training
• strength, flexibility
• energy/expenditure
• lower injury incidence than most other physical activity (Powell 1998)

Metabolic effects of walking
• Bone density?
• Muscle strength
• influences HDL cholesterol
• improves glucose metabolism
• reduces risk of acute thrombosis
• ?immuno-potentiation
Social and Psychological benefits
• Social activity
• Sense of well being, positive mental health, reduces anxiety
• Sense of community

National Recommendations for physical activity
• every adult should accumulate at least 30 mins + of moderate intensity Physical activity on most days
• can be accumulated in short bouts, intermittently
• use opportunities in everyday life
Burden of disease and injury in AUSTRALIA
AIHW November 1999
• Building on Global BOD study Alan Lopez et al (WHO 1993)
Uses DALYs as a metric
• Comparable across countries
• Useful for assessing health burden
What is the contribution of PA?
• Compared to other risk factors
• Overall to the “burden of disease”
• What conclusions can we draw from this about PA and its positioning among risk factors ?

8.5
6.8
5.4
4.8
- 3
4.3
2.7
2.6
1.8
1.7
0.9
-4 -2 0 2 4 6 8 10
tobacco
phys activity
hypertension
alcohol harm
alc benefit
obesity
low fruit/veg
cholesterol
illicit drugs
occupation
unsafe sex
Percent of total DALYs
Percent of total burden attributed to risk factorsBoD study, AIHW 1999

The health costsof physical inactivity

Introduction
• direct costs (of health care)
• indirect costs (cost productivity)
• intangible costs (QOL)
• economic sector factors beyond the scope of costing studies

28.2 2829.9
13.9
05
101520253035
high moderate low sedentary
Category of level of physical activity
Percent
Australian adults : physical activity levels, November 1997
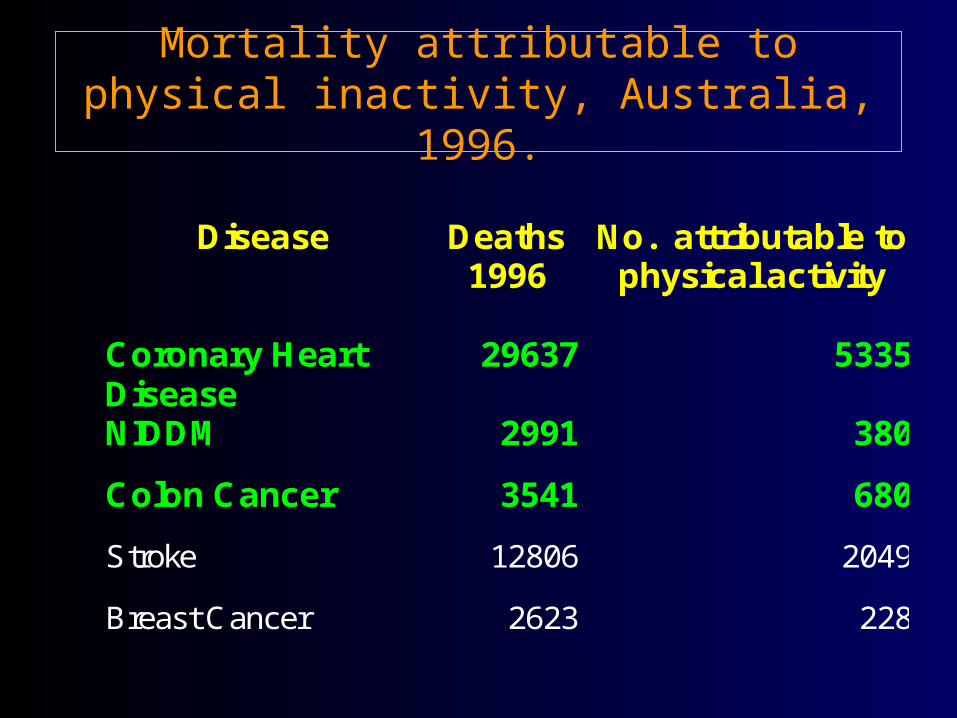
Mortality attributable to physical inactivity, Australia, 1996.
Disease Deaths 1996
No. attributable to physical activity
Coronary Heart Disease
29637 5335
NIDDM 2991 380
Colon Cancer 3541 680
Stroke 12806 2049
Breast Cancer 2623 228
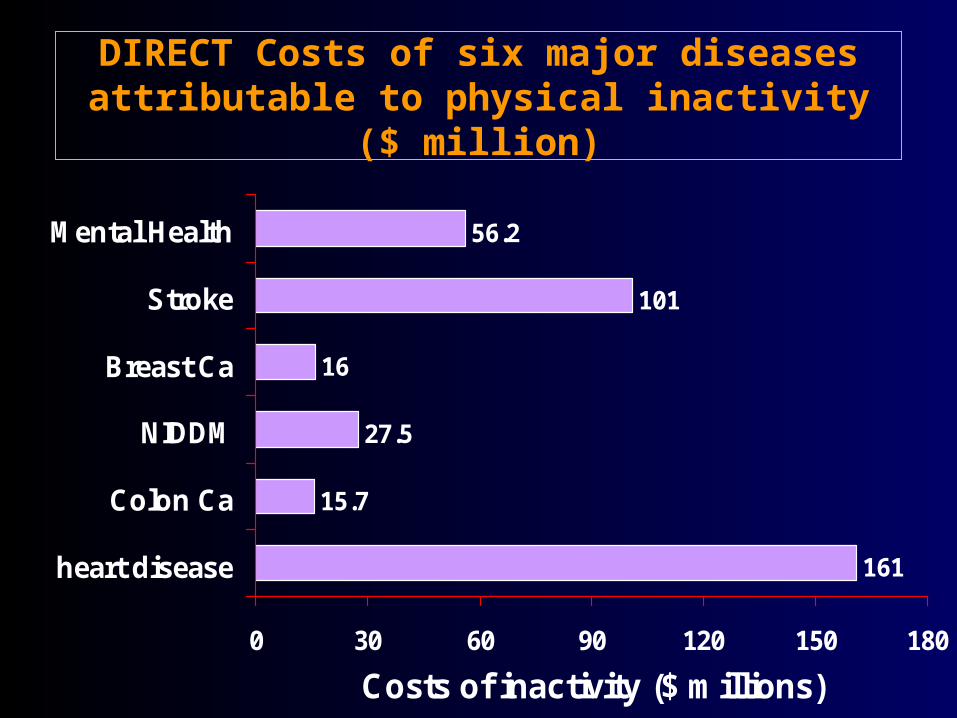
DIRECT Costs of six major diseases attributable to physical inactivity ($
million)
161
16
101
56.2
27.5
15.7
0 30 60 90 120 150 180
heart disease
Colon Ca
NIDDM
Breast Ca
Stroke
Mental Health
Costs of inactivity ($ millions)

Effect of increasing physical activity on health costs avoided from Coronary Heart Disease
Indicator Proportion of Adult Australianswho are Sufficiently Active
56% 61% 66% 100%
Person years gained(<70 years) from CHDdeaths avoided
6465 13311 55144
A.M.I hosp admavoided
558 1149 5906
CHD health care costsattributable to PA ($m).
161 148 130 0
Potential CHD healthcare savings fromincreased PA ($m).
13 31 161

Potential Savings of Direct Health Care Costs from increased P.A., 1993/94 ($m)
Disease Proportion of Adult Australianswho are sufficiently active
61% 66% 100%
CHD 13 31 161
Stroke 10 20 101
NIDDM 3 6 28
Colon Cancer 2 3 16
Breast Cancer 2 4 16
DepressiveDisorders
6 12 56
Sub-Total 36* 76 378All Causes 439 1003 5651

Recent trends in Australia
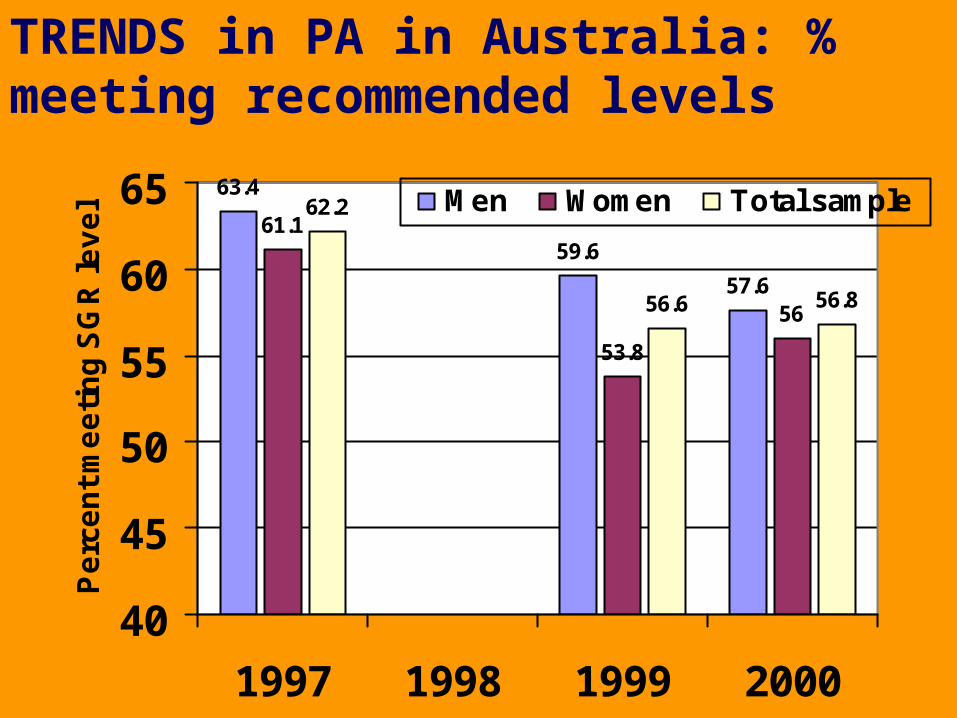
63.4
59.6
57.6
61.1
53.8
56
62.2
56.6 56.8
40
45
50
55
60
65
1997 1998 1999 2000
Pe
rce
nt
me
eti
ng
SG
R le
ve
l Men Women Total sample
TRENDS in PA in Australia: % meeting recommended levels

13.714.6
17.5
13.114.7
13.113.414.6 15.3
0
5
10
15
20
97 99 2000
% s
eden
tary
Men Women Persons
Completely sedentary (Nat PA surveys, Australia, November 1997, 99, 2000

Relevance of walking to physical activity
promotion• Accessible to all (equity)
• few age, gender seasonal restrictions
• initial activity most easily adopted
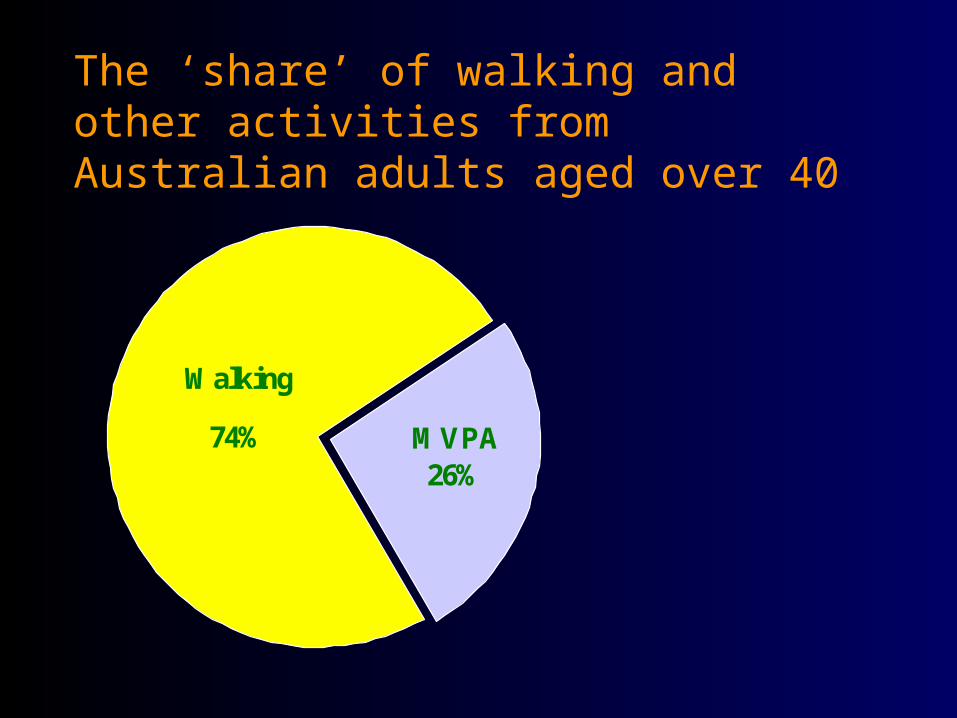
The ‘share’ of walking and other activities from Australian adults aged over 40
MVPA26%
Walking
74%

Physical Activity Interventions more likely
to succeed if:• Not “facilities” or “program attendance”
based – adherence wanes over time
• increased routine or incidental physical activity
• include environmental change - “making walking an easier choice”

Risks of Activity - [i] Cardiac and [ii]
Injury
• cardiac events and injury increased slightly in vigorous activity
• Injuries when running - up to 35-65% p.a.
• very low risk - walking, gardening <1% p.a
The evidence is very good for
health benefits of walking and
physical activity

“Walk a mile per day” (1.6 km)
• Achievable strategy for most people
• expend about 2 mega joules/week
• without any extra energy intake, would consume enough energy for 3 kg weight loss/year

Walking project in RockhamptonQueensland Govt, 2001- 2002 Investment $ 800,000

Other [beyond health] issues in promoting
walking• ecological impact of reduced car use
• increased DOT/ public transport usage
• Social well being / social capital strategy
• community growth – shops, restaurants
• urban planning – fits into designs for sustainable urban growth
• increased recreation / leisure sector
• walk to schools - PA among children

What to do next ?

NEW SOUTH WALES, Australia, 1996-2002
The NSW Premier’s Physical Activity
Taskforce

NSW Physical Activity Task Force
• An intersectoral [inter agency] and whole of Government strategic approach to the promotion of physical activity in NSW
• Partners : NSW Health, Sport and Recreation, Education, Local Government, Fitness Industry, Heart Foundation,, DUAP, DOT, RTA
NSW PATF achievements
• International model for strategic planning for PA
• Achieved major goals in PA when focused programs 1998-2000
• prevented national decline in PA – ONLY in NSW

NSW PATF : future• Existing PATF infrastructure and network
will continue for future programs
• After 5 years, undergoing a strategic review March- April 2002
• current review will suggest clear need for future integrated program directions
• Needs program resources – never had any to date [a remarkable model, but not sustainable in the climate of PA decline]
Conclusions• physical inactivity, and especially
walking is an issue for all in NSW
• infrastructure exists in NSW – PATF – to assist with PA interventions
• needs the commitment and political will to move (forwards)


















