SCHOOL BASED SERVICES. …Ensure all children with disabilities have available to them a free...
41
PHYSICAL & OCCUPATIONAL THERAPY SCHOOL BASED SERVICES
Transcript of SCHOOL BASED SERVICES. …Ensure all children with disabilities have available to them a free...

PHYSICAL & OCCUPATIONAL THERAPY
SCHOOL BASED SERVICES

…Ensure all children with disabilities have available to them a free appropriate public education that emphasizes special education and related services designed to meet their unique needs and prepare them for further education, employment, and independent living (Sec 300.1)
…Meet the child’s needs that result from the child’s disability to enable the child to be involved and progress in the general curriculum; and
Meet each of the child’s other educational needs that results from the child’s disability
(Sec. 300.320(a)(2)(A-B)
Purpose of IDEA

Related services means transportation and such developmental, corrective, and other supportive services as are required to assist a child with a disability to benefit from special education, and includes speech-language pathology and audiology services, interpreting services, psychological services, physical and occupational therapy, ….
(Sec. 300.34[a]) http://idea.ed.gov/explore/home
Related Services

All students with an IEP are ELIGIBLE for PT & OT
Student with documented disabilities may be ELIGIBLE for PT & OT
NOT ALL STUDENTS WITH IEP NEED PT & OT
Students without an IEP??
Who is ELIGIBILE for PT & OT?

Deliver services to improve ability to perform tasks for independent function◦ Includes accommodating a disability
Promote access to special education programming. ◦ Does not necessarily mean maximizing motor skills
Conduct context-based assessments to evaluate access, participation in educational activities and environments◦ Emphasis on function within performance environment
Enhance participation/performance in school with specific, skilled interventions focused on attainment of educational outcomes.
WHAT DO PT’s & OT’s DO?

Gross Motor ◦ Functional mobility for changing positions,
negotiating the classroom and campus alongside peers
◦ Postural stability for attention and focus on educational tasks
◦ Transportation, Carrying Items/materials, using the bathroom, participating at recess or in PE
◦ Assist in incorporating movement activities into instruction
◦ Motor Planning◦ Body Awareness
AREAS PT’s & OT’s ADDRESS

Fine Motor◦ Pre-writing and Handwriting difficulties related to
disability and that limit access/participation◦ Self Help Skills – fasteners for clothing
management◦ Scissor skills ◦ Visual motor skills – tracking, copying from
blackboard, scanning, etc.
AREAS PT’s & OT’s ADDRESS

Support ◦ Support early intervening services/RtI model◦ Reduce environmental barriers that limit student
participation◦ Use assistive technology to support student
success◦ Sensory integration strategies/supports ◦ Maintain Health, Prevent Contractures/Deformities ◦ Staff education – body mechanics, classroom
adaptation, reduce risk for injury◦ Suggest adaptive equipment ◦ Team Meetings◦ Parent Contact◦ Student Advocate!
AREAS PT’s & OT’s ADDRESS

Safely navigate environment?
YESSafe navigation
indicates that within their individual
classroom they have functional gross
motor skills to access and functionally
perform the tasks required of them
within their classroom.
NO This may look like the student who steps on other
students when finding their spot on the
carpet or trips over classroom obstacles.
This may be an indication of a gross
motor concern.
Safely Access All Areas of School?
YES Remember that all
students may not be the most active kid on the playground. Our goal is that they are able to access all the equipment and
are able to participate in games/activities with their peers.
NOThis may be the
student who can’t climb the stairs to the slide or auditorium,
the student who avoids certain
equipment due to fear, or the student
who consistently spills food off their
tray. This may be an indication of a gross
motor concern.
Concern: Functional Mobility

Falling significantly more
than peers?
YESFalling significantly
more than peers can indicate a gross
motor concern. Fall risk can also increase with increased fatigue
when walking. It is also important to take
into account the student’s
attention/hyperactivity levels.
NOStudent falls are a common event in
elementary schools. Young students are more likely to fall
than older students. Students who have decreased attention are also more apt to tripping and falling.
Injuries due to Falls?
YESMost typical falls do
not result in significant injuries to students. This can
indicate a gross motor concern with balance or safety responses. Please
also consider consultation with the nurse if the student breaks bones easily.
NOMost student falls do
not result in significant injury.
Scrapes and bruises are common,
especially in young students..
Concern: Functional Mobility

Balance Coordination Strength Endurance Body Awareness Attention
Skills for Functional Mobility

The ability to maintain the line of gravity within the base of support with minimal postural sway.
Able to compile/organize information from◦ vision ◦ vestibular◦ kinesthesia/proprioception ◦ muscle tone
Balance challenged by◦ changing base of support (feet together)◦ Limiting/changing sensory input (uneven
surfaces) ◦ Static/dynamic movements (speed of movement)
Concern: Balance/Postural Stability

Coordination is when movements of several limbs or body parts combined in a well-trained, smooth and efficient way to complete a task.
Coordination difficulties typically stem from cerebellum – may appear clumsy, frustrated, and difficulty learning new skills
Ataxia: lack of coordination seen with existing diagnosis (i.e. MD, CP, MS)
Dyspraxia: altered or decreased coordination
Concern: Coordination/Praxis
Poor Timing Poor Balance
Difficulty sequencing Proprioception difficulties
Ambidextrous Sensory processing difficulties
Low muscle tone Fatigue

Conscious force created through muscle contraction
Stable “core” = solid base of support◦ Solid base of support = more precision/control
NOT muscle tone◦ Tone is unconscious response to a stretch on the
muscle◦ Can be low (hypotonia) – decreased response
Slower reaction time, increased fatigue Associated with Down Syndrome, Autism (?), SMA
◦ Can be high (hypertonia) – increased response Rigid, difficult to move Associated with cerebral palsy, TBI
Concerns: Strength

Understanding what position one’s body is in, where & how one’s body is moving through space & in relation to other objects◦ Processing information from various sensory systems
to build a “body map” Vestibular Difficulties: movement intolerance Tactile Difficulties: Need more/less touch to learn Proprioception Difficulties: Falls frequently; falls out of
chair Poor body awareness may impact
◦ Motor planning◦ Crossing midline◦ Fine motor skills, including handwriting
Concerns: Body Awareness

Student that has difficulty blocking out environmental stimuli to focus on a task.
May appear “wiggly” ◦ If movement is not interfering with academic
progress, allowing movement may assist with learning.
◦ Ergonomic considerations – position/posture in seat, position in classroom
Concerns: Attention

Concern: Handwriting
Explicit Instruction in Handwriting?
YES: Letter formation requires memory, eye-hand coordination, fine
motor muscle coordination, visual
perceptual skills, postural stability
stability, and visual tracking skills.
NO: Students MUST receive explicit
handwriting instruction to
develop efficient legible handwriting. Students must also be provided with opportunities for
repetition and practice.
Knows All Letters – Upper & Lower
Case?
YES: Letter formation requires memory, hand eye coordination, fine
motor muscle coordination, visual
perceptual skills, postural stability,
and visual tracking.
NO: To be an effective writer,
students’ must have knowledge of letters
and their corresponding
forms. Drill and practice to help fill in this educational
gap is appropriate.
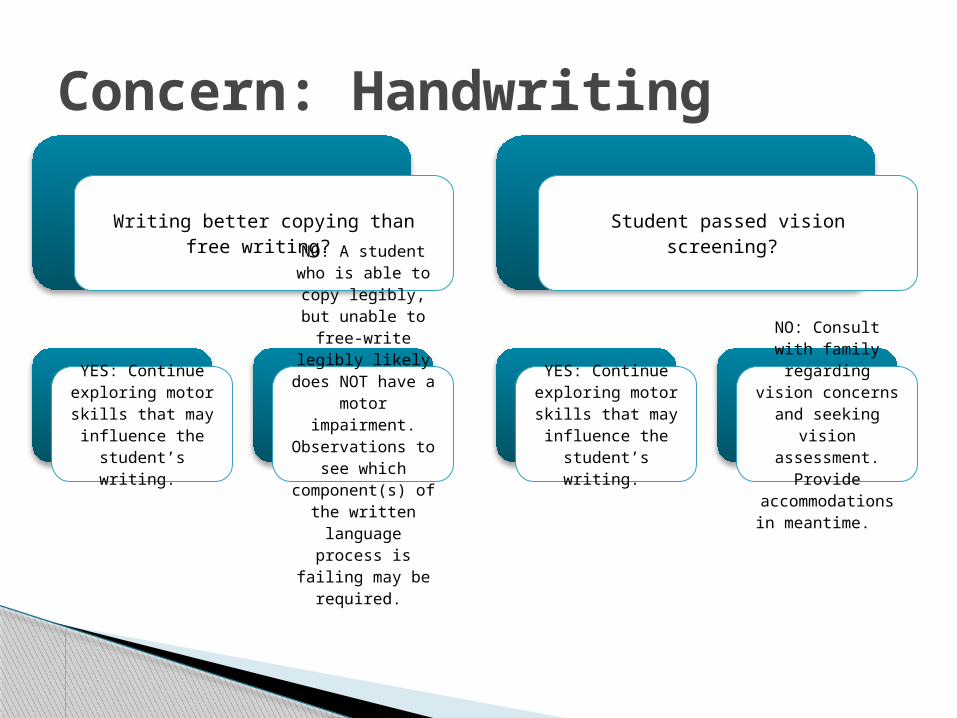
Concern: Handwriting
Writing better copying than free writing?
YES: Continue exploring motor skills that may influence the
student’s writing.
NO: A student who is able to copy
legibly, but unable to free-write
legibly likely does NOT have a motor
impairment. Observations to
see which component(s) of
the written language process is failing may be
required.
Student passed vision screening?
YES: Continue exploring motor skills that may influence the
student’s writing.
NO: Consult with family regarding vision concerns
and seeking vision assessment.
Provide accommodations in meantime.

Concern: Handwriting
Concerns with Grasp?
YES: Implement strategies to
assist, i.e. pencil grasp, short
pencils, mechanical pencil
or soft lead pencils. OT may
consult to provide additional
strategies.
NO: A functional but atypical grasp does not require intervention or
alteration.
Spacing, Orientation, Posture Limiting Legibility?
YES: Implement strategies to
assist, i.e. finger spacing or
highlighted lines, change chair
height.
NO: Motor skills are likely not impacting the
student’s handwriting.
Continue to offer opportunities for instruction and
practice.

Posture Grasp Pre-Writing Skills Visual Motor Skills
Skills Required for Handwriting

Good posture allows for more precise control of hand & fingers for handwriting
90-90-90 Posture is Best◦ Elbows, hips and knees at 90 Degrees◦ Feet flat on floor or foot rest◦ Raise or lower desk heights as needed◦ Computer screen at eye level
Concern: Posture

Concern: Pencil GraspDoes the student have any of these grasp/grip concerns?
Pushes Too Hard/Soft Complains of Hand Grasp Concerns Moves Whole Arm Switches Hands Fatigue or Pain
YESYES YES YES
Initial interventions to try: mechanical pencil, felt or fabric
under paper, or softer lead pencils.
For more suggestions, please consult with OT for Tier II Strategies.
Initial interventions to try: a pencil grip, encourage
play with putty or Playdoh. Consult
with OT regarding additional
suggestions for preventing hand
fatigue.
Initial interventions to try: “The Pencil Grip”, use of golf pencil or broken crayons. Consult with OT regarding
pencil grasp strategies.
This is often seen with younger
students. Encourage them
to keep their forearm on table
and allow opportunities to work on vertical
surfaces.
This is often seen with younger
students. Continue to encourage them to
utilize only one hand. If they have not
developed a preference for one hand, this could
indicate a need for Motor Therapist
Consult.
YES

Concern: Pencil GraspWhat Grasp is Your Student Using?
Dynamic Tripod (Functional)
Dynamic Quadropod (Functional)
Adapted Tripod (Functional)
Five Fingertip (Functional)
Thumb Wrap (Functional)
Fisted/Palmer (NON-Functional)

Difficulty imitating block building patterns Difficulty matching shapes/puzzles Difficulty identifying simple directional
concepts Difficulty tracing a line Difficulty imitating after demonstration Difficulty copying/drawing simple shapes
◦ (i.e. circle, vertical line, horizontal line, cross) Inappropriate pencil pressure
◦ Too light◦ Too Dark
Concern: Pre-Writing

Illegible handwriting Letter reversals Inaccurate letter formation
Concern: Letter Formation

Letters too close together Letters too far apart Letters written over or under the writing line Letters too small Letters too large
Concern: Spacing & Alignment

Visual Spatial Perception◦ Too much/not enough pressure◦ Spacing ◦ Messy/disorganized work
Tracking◦ Difficulty reading and writing across page/pages◦ Turning head while reading◦ Skipping letters/words when copying ◦ Squinting/closing one eye
Shifting Focus◦ i.e. Copying from Black (white) board
Concern: Visual Motor

Difficulty holding or using scissors ◦ OVER THE AGE of FOUR (4) YEARS
Difficulty opening and closing scissors Chopping paper
Concern: Cutting

Difficulty opening and closing fasteners Difficulty dressing Difficulty sequencing steps Difficulty with self feeding
◦ Using utensils, opening/closing containers◦ NOT chewing & swallowing
Difficulty toileting ◦ NOT POTTY TRAINING
Concern: Self-Help

Consult with therapist◦ Describe student and concerns ◦ Describe perceived impact ◦ Describe any attempted strategies
Determine with therapist which strategies may address concerns ◦ Classroom strategies?◦ RtI Plan?
If concerns appear to indicate a motor concern, determine with therapist if assessment is appropriate.
Consult versus Evaluation

Identification of School-
Based Issues
Observe & Document Concerns
Prioritize Concerns
Pre-Referral Strategies
Implementation of
Strategies
Evaluating the Results
Goals
NOT Met
REFER for Evaluation
If strategies NOT working, develop new strategies.
If strategies ARE working, continue 4-6 weeks.
Goals
MET
Pre-Referral for OT & PT

Tier I: Universal Level Support: ◦ Instruction, curriculum, screenings to meet needs
of majority of students in general classroom setting
◦ OT & PT role is to promote universal design for learning, provide minimal input to benefit all students i.e. ergonomics, developmental sequence,
handwriting acquisition, movement breaks for improved learning
◦ NO ROLE AT INDIVIDUAL STUDENT LEVEL
OT & PT in RtI

Tier II: Targeted Level Support◦ Student’s needs not met at universal level. ◦ Consult with team to problem solve specific areas
of concern related to PT & OT◦ Assist teacher in differentiating instruction for
individual student
OT & PT IN RtI

Tier III: Intensive Level ◦ Includes general and special education◦ Instruction is intensive, in small groups or
individual◦ Provide consultative services, work directly with
teachers to provide interventions or embed therapeutic activities into academic activities
◦ Defined, problem-focused, short duration
OT & PT IN RtI

Focus of Intervention
Pre-K & Kindergarten Elementary School
Intense remediation and intervention to promote skills or prevent functional impairments
Early identification of task and environmental adaptations to increase participation
Continued remediation and intervention for skill development or preventing loss of function in early years
Increasing consideration for adaptations
Motor skill acquisition is SLOWING

Focus of Intervention
Intermediate/Middle High School
Increased focus on task and environmental adaptations
New motor skill achievement slows/plateaus
Remediation/accommodations may be necessary considering life skills programs/prevocational programs
Focus is mostly on task and environmental adaptations
Accommodations for impairments may be required in consideration of prevocational programs/life skills.
Service needs may change depending upon post-high school plans.

TYPICALLY SERVICES PROGRESS FROM DIRECT
TO MORE CONSULTATIVE/INTEGRATIV
E METHODS

Direct –◦ Therapist works with student on IEP objectives◦ Therapy may be in group or individual sessions◦ Therapy may be in classroom, lunchroom, PE
class, or “therapy room” (pulled out individually with therapist)
◦ Student needs specialized instruction that ONLY a therapist can provide
◦ Establish/teach a NEW skill that student may use in various other environments and activities
DIRECT VS. CONSULT

CONSULT◦ Therapist works with other professionals -
teachers, EA’s, etc (NOT the student)◦ Provide adaptations, accommodations and
supports to help student meet the IEP objectives ◦ Ensure the student has multiple opportunities
within the school day to practice a particular skill
DIRECT vs. CONSULT

CONSULT (Cont’d)◦ May include observation of and interaction with
student◦ Not treatment or intervention ◦ Does not mean LESS services – often is at least as
time consuming as direct services ◦ Therapist AND others collect data/information to
determine needs and evaluate results of implemented accommodations/adaptations
DIRECT vs. CONSULT

QUESTIONS????