School-based interventions to prevent HIV, STIs & adolescent pregnancy: What's the evidence?
61
Welcome! School-based interventions to prevent HIV, STIs & adolescent pregnancy: What's the evidence? You will be placed on hold until the webinar begins. The webinar will begin shortly, please remain on the line.
-
Upload
health-evidence -
Category
Education
-
view
86 -
download
0
Transcript of School-based interventions to prevent HIV, STIs & adolescent pregnancy: What's the evidence?
Welcome!School-based interventions to
prevent HIV, STIs &
adolescent pregnancy: What's
the evidence?
You will be placed on hold until the webinar begins.
The webinar will begin shortly, please remain on the line.

Poll Questions: Consent
• Participation in the webinar poll questions is voluntary
• Names are not recorded and persons will not be identified in any way
• Participation in the anonymous polling questions is accepted as an
indication of your consent to participate
Benefits:
• Results inform improvement of the current and future webinars
• Enable engagement; stimulate discussion. This session is intended for
professional development. Some data may be used for program evaluation
and research purposes (e.g., exploring opinion change)
• Results may also be used to inform the production of systematic reviews
and overviews
Risks: None beyond day-to-day living
After Today
• The PowerPoint presentation and audio recording will be made available
• These resources are available at: – PowerPoint:
http://www.slideshare.net/HealthEvidence
– Audio Recording: https://www.youtube.com/user/healthevidence/videos
3

What’s the evidence?
Mason-Jones A, Sinclair D, Mathews C, Kagee
A, Hillman A, & Lombard C. (2016). School-
based interventions for preventing HIV,
sexually transmitted infections, and
pregnancy in adolescents. Cochrane
Database of Systematic Reviews, 2016(11),
CD006417http://www.healthevidence.org/view-
article.aspx?a=school-based-interventions-preventing-
hiv-sexually-transmitted-infections-29881

• Use CHAT to post comments /
questions during the webinar
– ‘Send’ questions to All (not
privately to ‘Host’)
• Connection issues
– Recommend using a wired
Internet connection (vs.
wireless)
• WebEx 24/7 help line
– 1-866-229-3239
Participant Side Panel in WebExHousekeeping

Housekeeping (cont’d)
• Audio
– Listen through your speakers
– Go to ‘Communicate > Audio Broadcast’
• WebEx 24/7 help line
– 1-866-229-3239

Poll Question #1
How many people are watching
today’s session with you?
A. Just me
B. 2-3
C. 4-5
D. 6-10
E. >10

The Health Evidence™ Team
Maureen Dobbins
Scientific Director
Heather Husson
Manager
Susannah Watson
Project Coordinator
Students:
Emily Belita
(PhD candidate)
Jennifer Yost
Assistant ProfessorOlivia Marquez
Research Coordinator
Emily Sully
Research AssistantLiz Kamler
Research Assistant
Zhi (Vivian) Chen
Research Assistant
Research Assistants:
Lina Sherazy
Claire Howarth
Rawan Farran
What is www.healthevidence.org?
Evidence
Decision
Making
inform
Why use www.healthevidence.org?
1. Saves you time
2. Relevant & current evidence
3. Transparent process
4. Supports for EIDM available
5. Easy to use

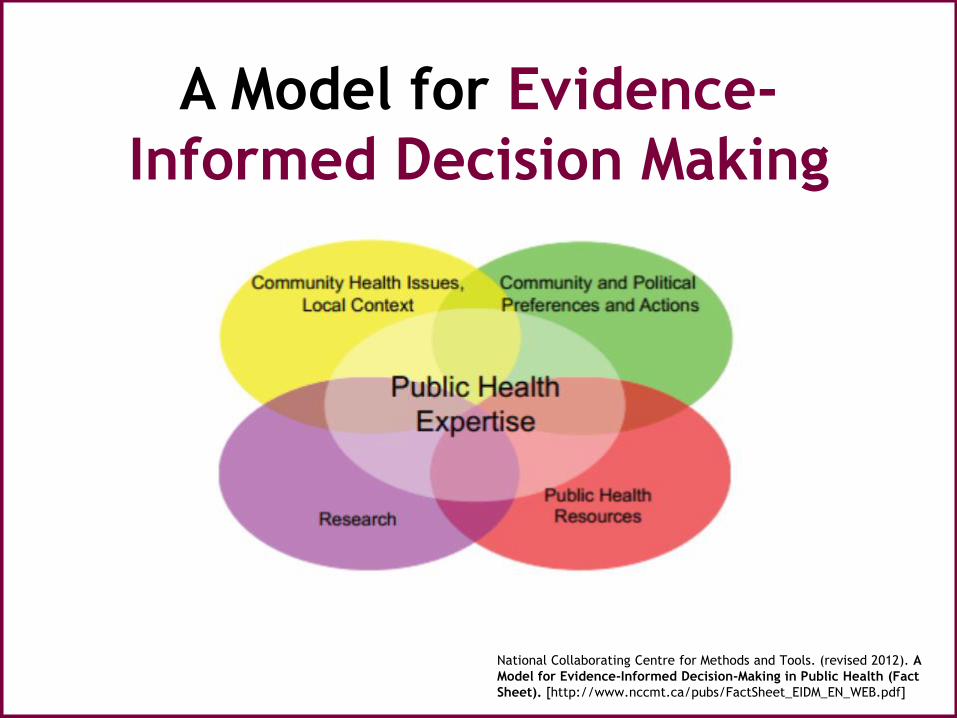
A Model for Evidence-
Informed Decision Making
National Collaborating Centre for Methods and Tools. (revised 2012). A
Model for Evidence-Informed Decision-Making in Public Health (Fact
Sheet). [http://www.nccmt.ca/pubs/FactSheet_EIDM_EN_WEB.pdf]
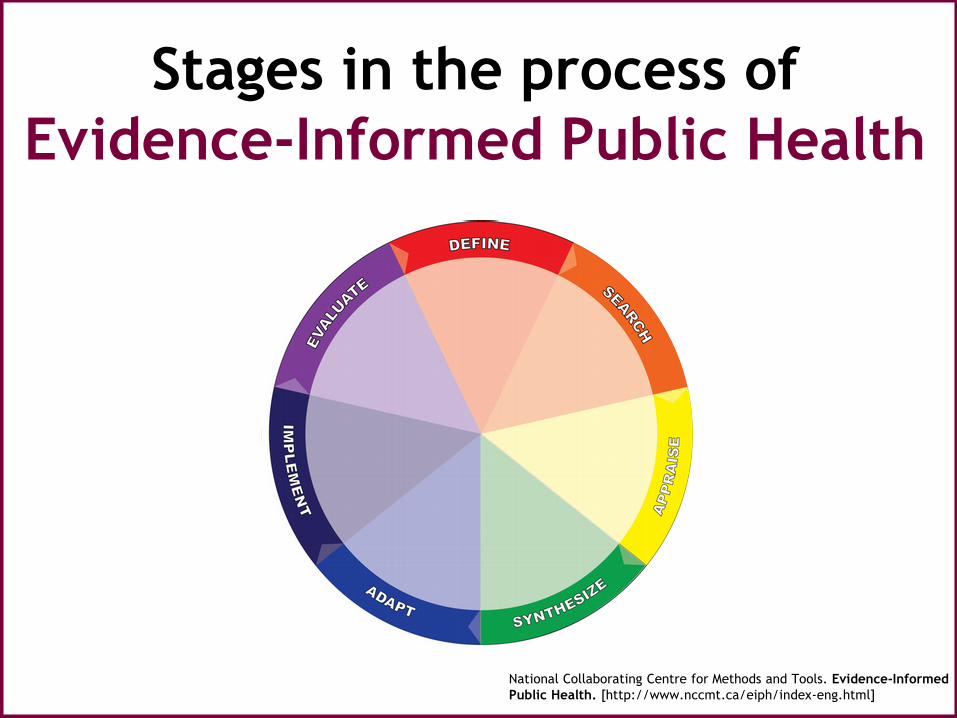
Stages in the process of
Evidence-Informed Public Health
National Collaborating Centre for Methods and Tools. Evidence-Informed
Public Health. [http://www.nccmt.ca/eiph/index-eng.html]
Poll Question #2
Have you heard of PICO(S) before?
A. Yes
B. No
Searchable Questions Think “PICOS”
1.Population (situation)
2.Intervention (exposure)
3.Comparison (other group)
4.Outcomes
5.Setting

How often do you use Systematic Reviews
to inform a program/services?
A. Always
B. Often
C. Sometimes
D. Never
E. I don’t know what a systematic review is
Poll Question #3
Dr. Amanda Mason-Jones
Department of Health Sciences
University of York

The team
• David Sinclair, Liverpool School of Tropical
Medicine, England.
• Cathy Mathews, Health Systems Research Unit,
South African Medical Research Council (MRC).
• Ashraf Kagee, Department of Psychology,
Stellenbosch University, South Africa.
• Alex Hillman, Department of Health Sciences,
University of York, England.
• Carl Lombard, Biostatistics Unit, South African
MRC.

Acknowledgements
• Joy Oliver, South African Cochrane Centre
• Paul Garner & Ann-Marie Stephani, Cochrane
Infectious Diseases Group, Liverpool School of
Tropical Medicine
• Hasci Horvath, HIV/AIDS Collaborative review
group, University of California, San Francisco
• Alan Flisher & Wanjiru Mukoma, University of
Cape Town
• Jimmy Volmink- Stellenbosch University
Altmetric

Media attention

Media attention

Media attention

Research question
• Can school-based sexual and reproductive
health programmes reduce sexually
transmitted infections (such as HIV,
herpes simplex virus, and syphilis), and
pregnancy among adolescents?
Inclusion criteria
• Population- adolescents 10-19 attending school
• Intervention- any that aimed to reduce risk of HIV, STIs and pregnancy
• Comparison- usual practice/other intervention
• Outcome- ‘Biological’ outcomes, HIV, STIs, and pregnancy objectively measured
• Study design-Randomised controlled trials
Search strategySearch dates: 1 Jan 1990-7 April 2016
• MEDLINE
• Embase
• CENTRAL
• WHO International Clinical Trials Registry Platform
• ClinicalTrials.gov
• Conference databases (AIDS, AEGIS)
• NLM GATEWAY)
• Other resources (CDC, CRD, WHO, reference lists, other researchers)
Data collection
• Two reviewers independently reviewed all
studies (titles and abstracts)
• Full text articles were obtained for all
identified as potentially relevant
• Second screening for inclusion/exclusion
• New/ongoing studies were also identified
Data extraction and
management• Data were extracted for all included studies
independently by two authors (location, context, theoretical framework, participants, interventions, quality and results).
• Any discrepancies or disagreements were resolved by looking at the original/supporting papers or contacting the authors
• Trials with multiple publications were managed as one study

Analysis
• Relative risk of the outcome was used
and we reported risk ratios (RR) with 95%
confidence intervals (CIs)
• If odds ratios and CIs were reported this
was used to estimate the design effect
and intraclass correlation coefficient
• Multiple interventions in one trial were
analysed separately
Quality and risk of bias
• The GRADE approach was used to assess
the quality of evidence
• The Cochrane risk of bias assessment tool
for cluster RCTs was used

Results
• 1183 unique references after duplicates
were removed
• 1112 excluded articles
• 71 full-text articles screened
• 8 cluster randomised trials included

Excluded studies
• Reasons for exclusion
– 26 with no biological outcomes
– 10 not school-based
– 12 were not randomised controlled trials
– 11 systematic reviews
– 4 protocol/early reports

Included studies
• Eight cluster randomised trials
• Countries- Chile, England, Kenya, Malawi,
Scotland, South Africa, Tanzania,
Zimbabwe
• 281 clusters
• Cluster size ranged from 18-461
• 55,157 participants
• Follow up from 18 months to 7 years

Type of intervention
• Educational
• Incentive
• Combined incentive plus education

Educational interventions
• Theoretical frameworks focused on changing knowledge, attitudes, behaviours and social norms
• From three one-hour sessions over one year to 36 sessions of 40 minutes over three years
• Used peer educators or teachers/adult facilitators to deliver programmes
• Drama, games, role play, gender roles
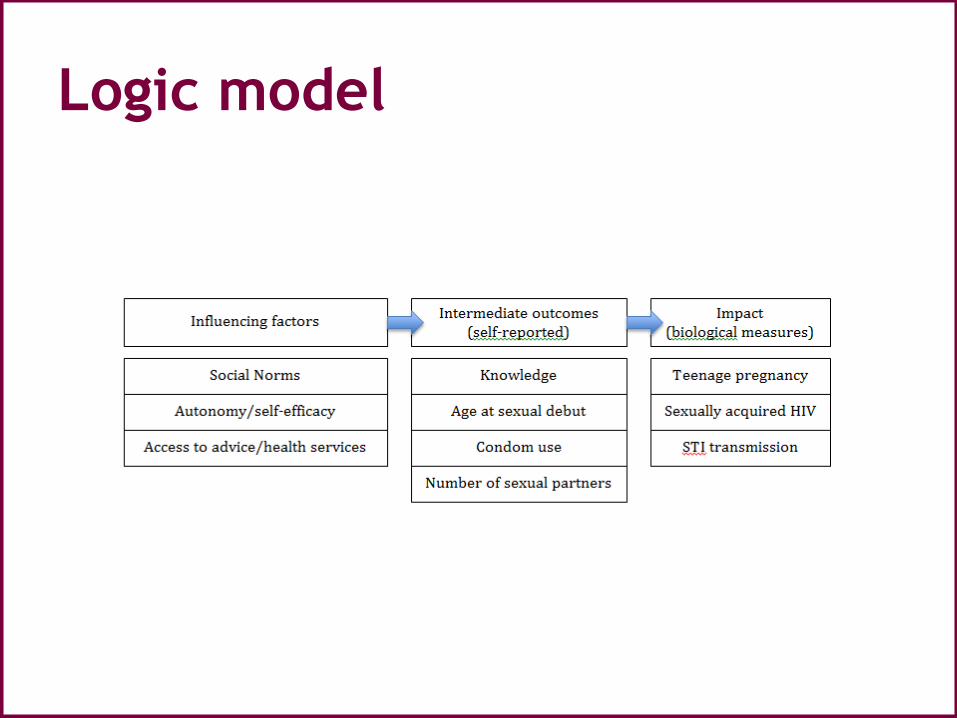
Logic model

Incentive-based interventions
• Theoretical framework based on ‘upstream factors’ that influence sexual health outcomes such as poverty, inequality and school attendance
• Incentives given such as cash (USD1-5 for participant and USD 4-10 for family) or other material transfer (two school uniforms) which were either: – Conditional (e.g. on school attendance)
– Unconditional
Outcome measurement
• HIV, HSV2 and other STIs measured by:
– Dried blood spots
– Blood sera
– Urine tests
• Pregnancy (current) measured by:
– Urine tests
• Pregnancy at follow up measured by:
– Linkage to health service records
– School reports
Comparisons
1. Educational interventions versus no
intervention
2. Incentive programmes versus no
intervention
3. Educational intervention and incentive
versus no intervention

Educational interventions- HSV2
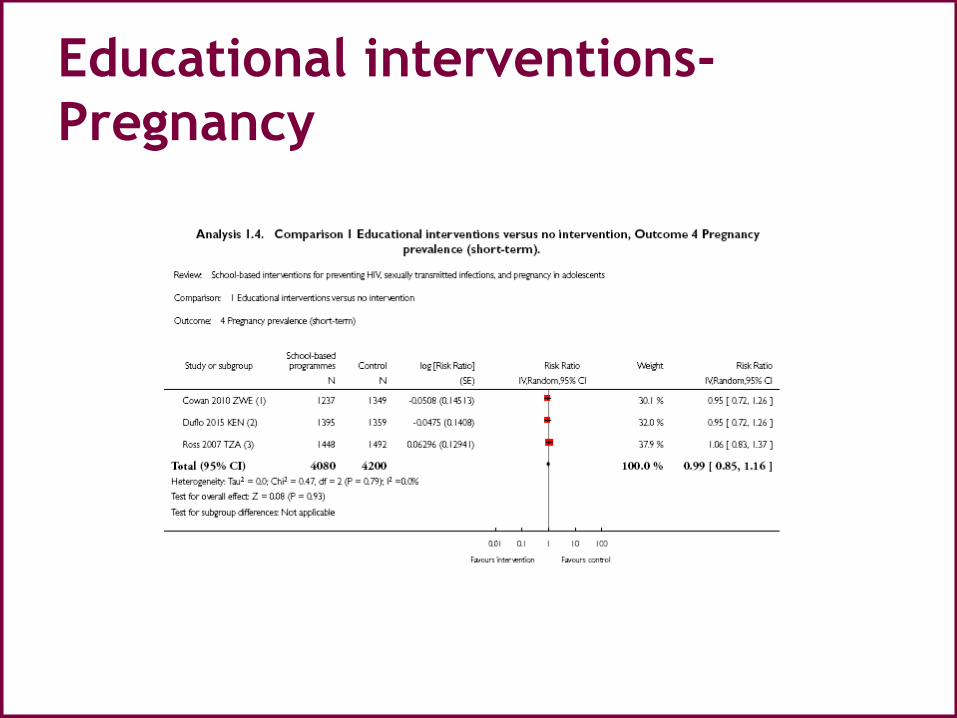
Educational interventions-
Pregnancy
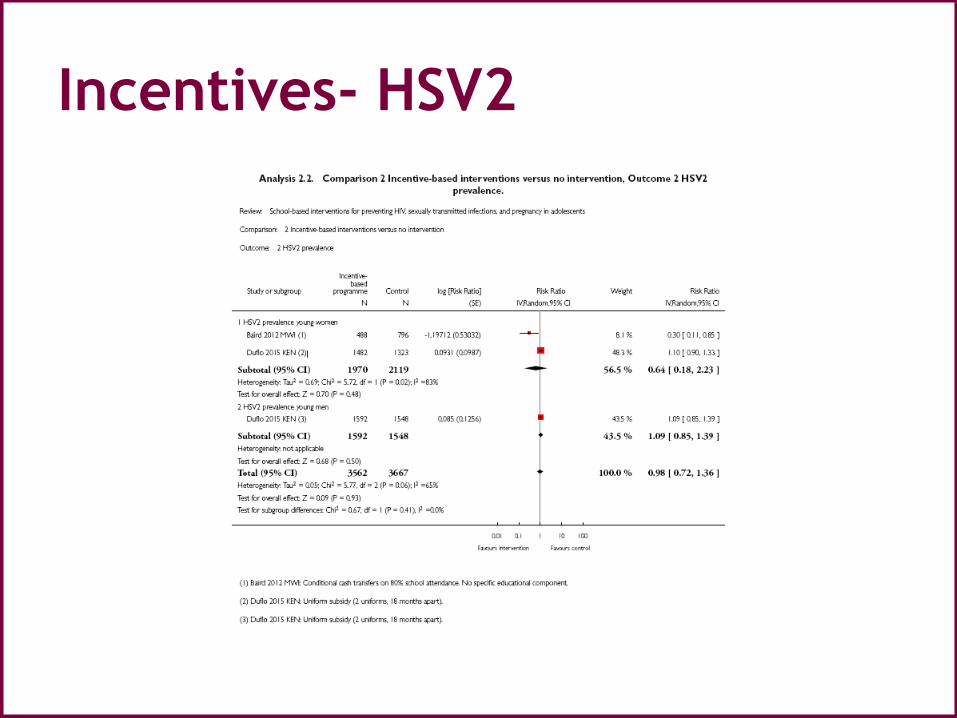
Incentives- HSV2

Incentives- self reported
debut

Incentives- pregnancy

Incentive plus education-
HSV2
Risk of bias
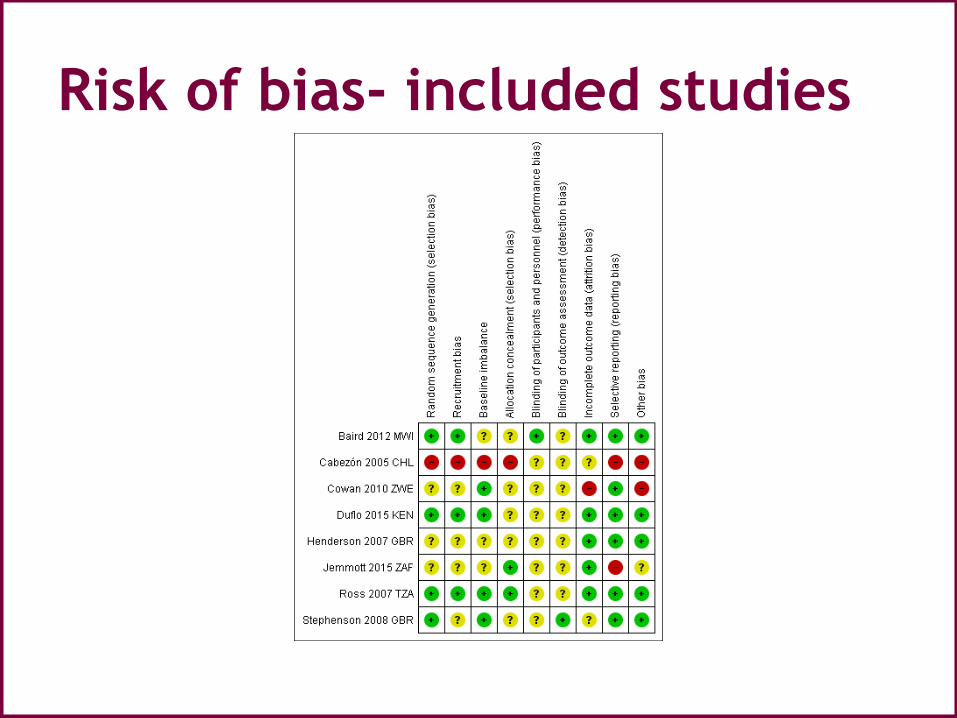
Risk of bias- included studies

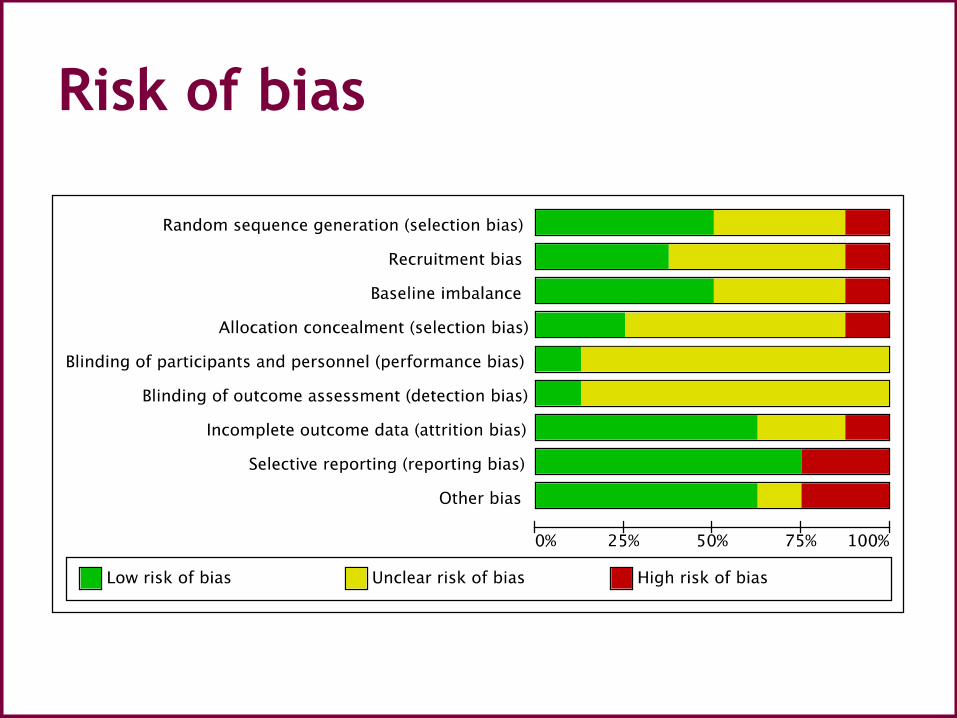
Risk of bias
Risk of bias
• Random sequence generation
• Recruitment bias
• Baseline imbalance
• Allocation concealment
• Blinding
• Incomplete outcome data
• Selective reporting
• Other potential sources of bias

Grade approach
• High certainty: further research is very unlikely to change our confidence in the estimate of effect.
• Moderate certainty: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
• Low certainty: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
• Very low certainty: we are very uncertain about the estimate.

Educational interventions

Incentives
Discussion
• Completeness and applicability
• Quality of the evidence
• Potential biases in the review process
• Agreements and disagreements with
other studies or reviews

Ongoing studies
• 5 ongoing studies
• 4 Cluster RCT/1 Individually randomisedstudy
• South Africa (educational intervention)
• South Africa (incentive plus education)
• South Africa (incentive only)
• Botswana (educational intervention)
• India (educational intervention)

Conclusions
• Implications for practice
– Sexual and relationship health provision
• Implications for research
– Logic model
– Theoretical approaches
– Length of intervention
– Length of follow up
– Outcome measures

A Model for Evidence-
Informed Decision Making
National Collaborating Centre for Methods and Tools. (revised 2012). A
Model for Evidence-Informed Decision-Making in Public Health (Fact
Sheet). [http://www.nccmt.ca/pubs/FactSheet_EIDM_EN_WEB.pdf]
Poll Question #4
The information presented today was
helpful
A. Strongly agree
B. Agree
C. Neutral
D. Disagree
E. Strongly disagree

What can I do now?
Visit the website; a repository of over 5,000 quality-rated systematic reviews
related to the effectiveness of public health interventions. Health Evidence™ is
FREE to use.
Register to receive monthly tailored registry updates AND monthly newsletter
to keep you up to date on upcoming events and public health news.
Tell your colleagues about Health Evidence™: helping you use best evidence to
inform public health practice, program planning, and policy decisions!
Follow us @HealthEvidence on Twitter and receive daily public health review-
related Tweets, receive information about our monthly webinars, as well as
announcements and events relevant to public health.
Encourage your organization to use Health Evidence™ to search for and apply
quality-rated review level evidence to inform program planning and policy
decisions.
Contact us to suggest topics or provide feedback.

Poll Question #5
What are your next steps? [Check all
that apply]
A. Access the full text systematic review
B. Access the quality assessment for the
review on www.healthevidence.org
C. Consider using the evidence
D. Tell a colleague about the evidence

Thank you!
Contact us:
For a copy of the presentation please visit:
http://www.healthevidence.org/webinars.aspx