Schistosoma parasitology kasr el Einy department
26
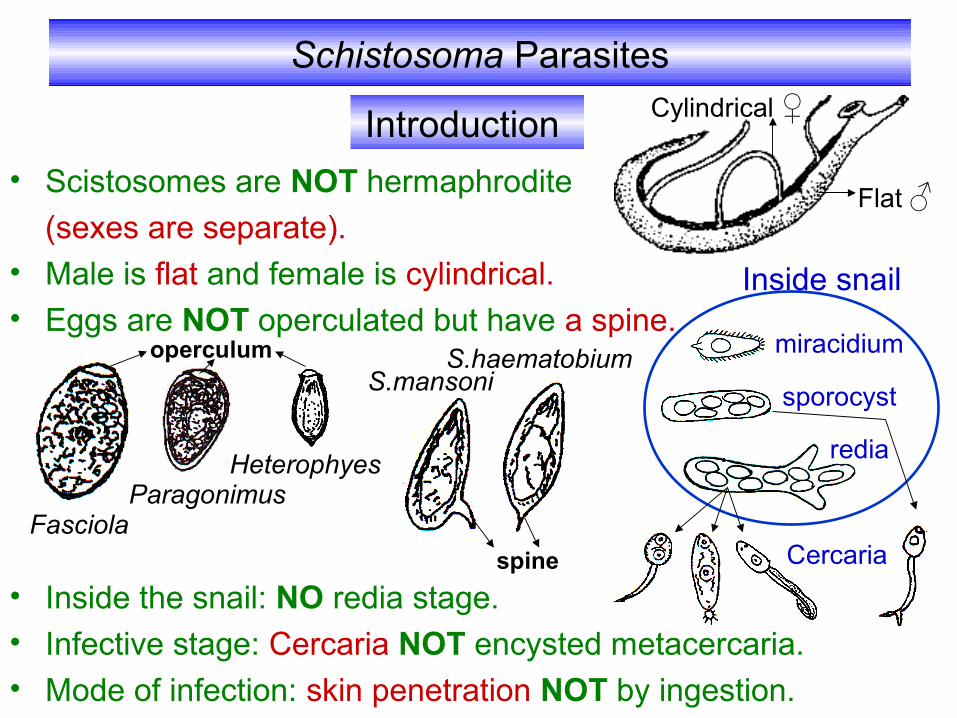
Schistosoma Parasites • Scistosomes are NOT hermaphrodite (sexes are separate). • Male is flat and female is cylindrical. • Eggs are NOT operculated but have a spine. • Inside the snail: NO redia stage. • Infective stage: Cercaria NOT encysted metacercaria. • Mode of infection: skin penetration NOT by ingestion. Introduction Fasciola Paragonimus Heterophyes S.mansoni S.haematobium miracidium sporocyst redia Inside snail operculum spine Flat ♂ Cylindrical ♀ Cercaria
-
Upload
ahmedmohamedkamel -
Category
Documents
-
view
297 -
download
0
Transcript of Schistosoma parasitology kasr el Einy department
Schistosoma Parasites
• Scistosomes are NOT hermaphrodite
(sexes are separate).
• Male is flat and female is cylindrical.
• Eggs are NOT operculated but have a spine.
• Inside the snail: NO redia stage.• Infective stage: Cercaria NOT encysted metacercaria.• Mode of infection: skin penetration NOT by ingestion.
Introduction
FasciolaParagonimus
Heterophyes
S.mansoniS.haematobium
miracidium
sporocyst
redia
Inside snail
operculum
spine
Flat ♂
Cylindrical ♀
Cercaria
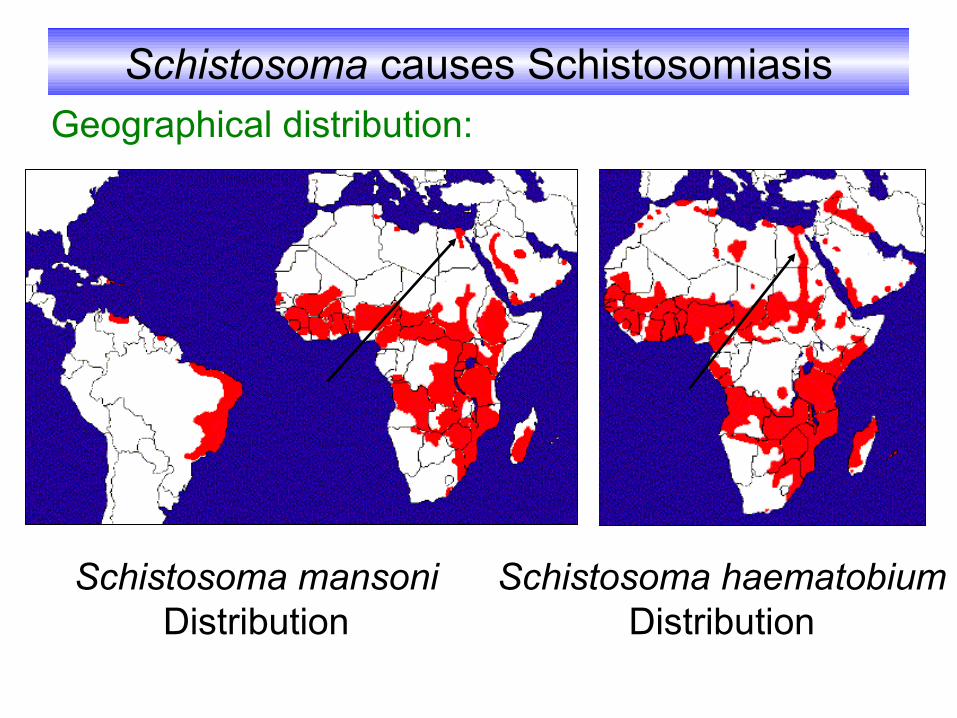
Schistosoma causes SchistosomiasisGeographical distribution:
Schistosoma mansoni Distribution
Schistosoma haematobium Distribution
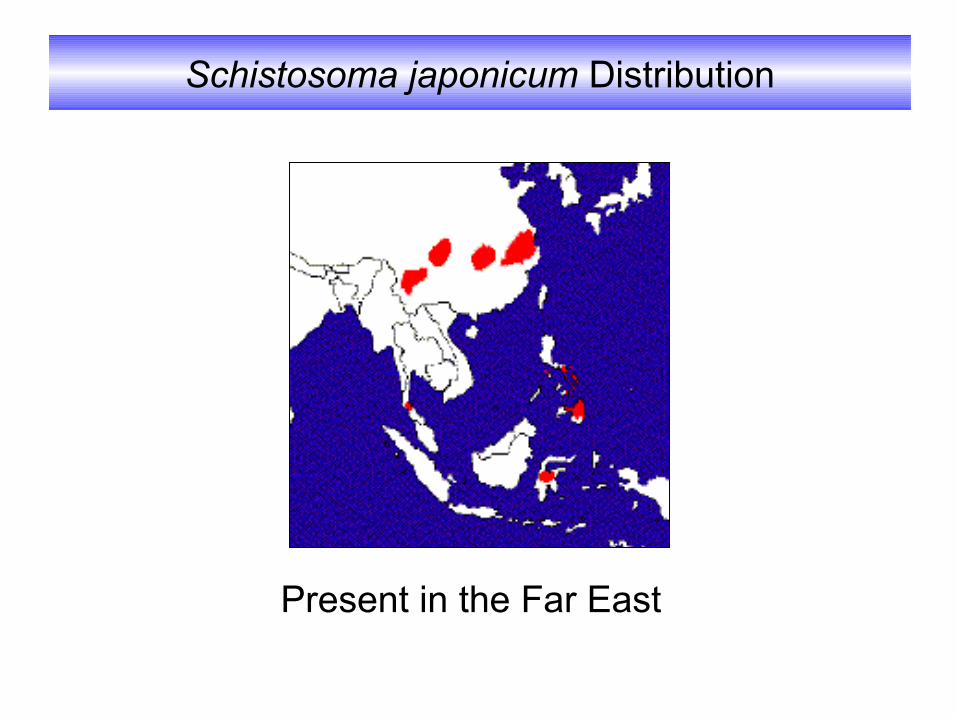
Schistosoma japonicum Distribution
Present in the Far East

Definitive Host Man Habitat
Superior & Inferior mesenteric plexus of
veins
Vesical & pelvic plexus of veins
Where adult S.mansoni live
Where adult S.haematobium live
Blood vesselsThus Schistosomes are
called Blood flukes
Inferior mesenteric plexus of
veinsWhere adult
S.japonicum live

Life Cycle
Infected human
Egg in urine
miracidium
B.truncatusB.alexandrina
Intermediate host
Furcocercous cercaria
Egg in stoolCercaria
penetrate human skin
Fresh water
Definitive host
S.haematobium S.mansoni
Infective stage
Mode of infection
Diagnostic stage

Diagnostic Stage
S.haematobium egg in urine S.mansoni egg in stool
Size:
Shape:
Colour:
Content:
140X60 µ 150X60 µ
Oval, thin shellTerminal spine Lateral spine
Translucent
Miracidium
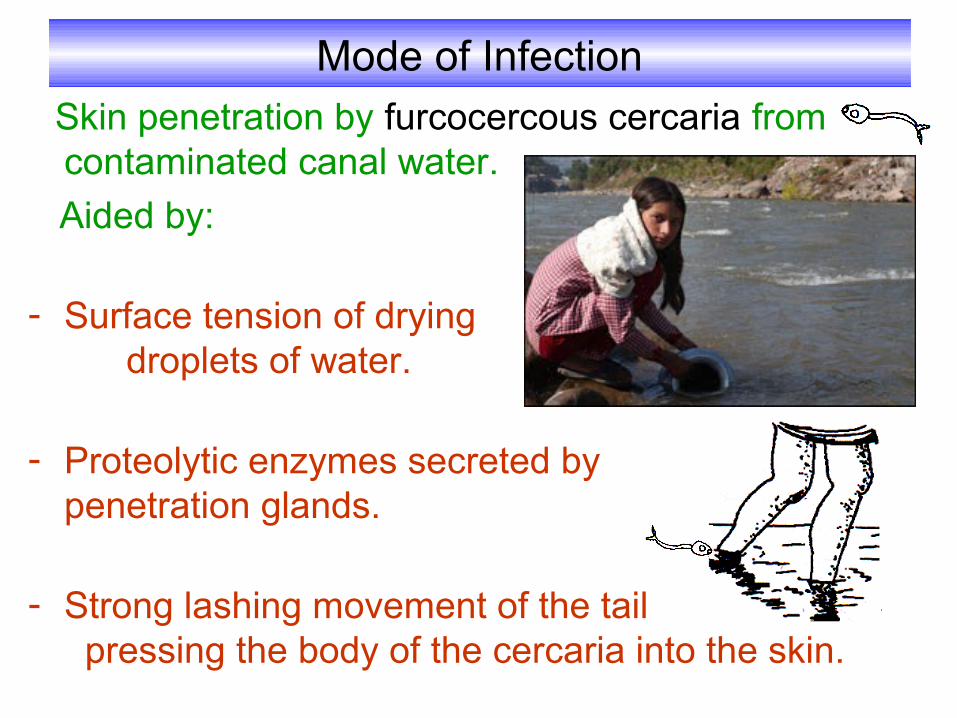
Mode of Infection Skin penetration by furcocercous cercaria from
contaminated canal water.
Aided by:
- Surface tension of drying droplets of water.
- Proteolytic enzymes secreted by penetration glands.
- Strong lashing movement of the tail pressing the body of the cercaria into the skin.
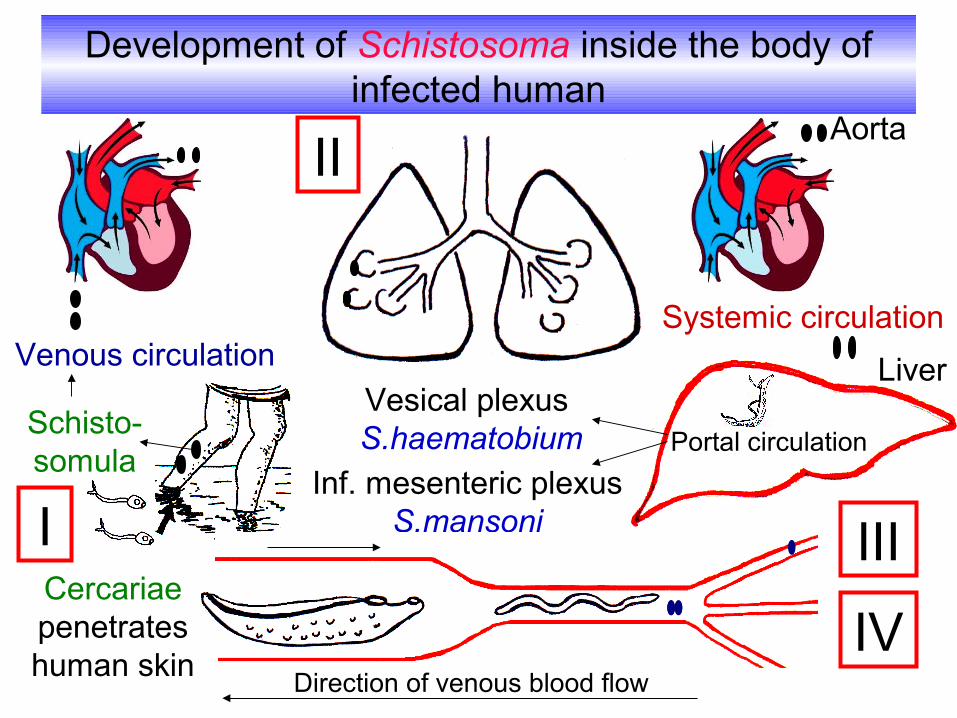
Development of Schistosoma inside the body of infected human
Cercariae penetrates human skin
Schisto- somula
Venous circulationSystemic circulation
Liver
Portal circulation
Vesical plexus S.haematobium
I III
IV
II
Inf. mesenteric plexus S.mansoni
Direction of venous blood flow
Aorta

Pathogenesis and Clinical Picture
There are 4 progressive stages:
Local dermatitis, irritation.
Papular rash.
I- Stage of invasion
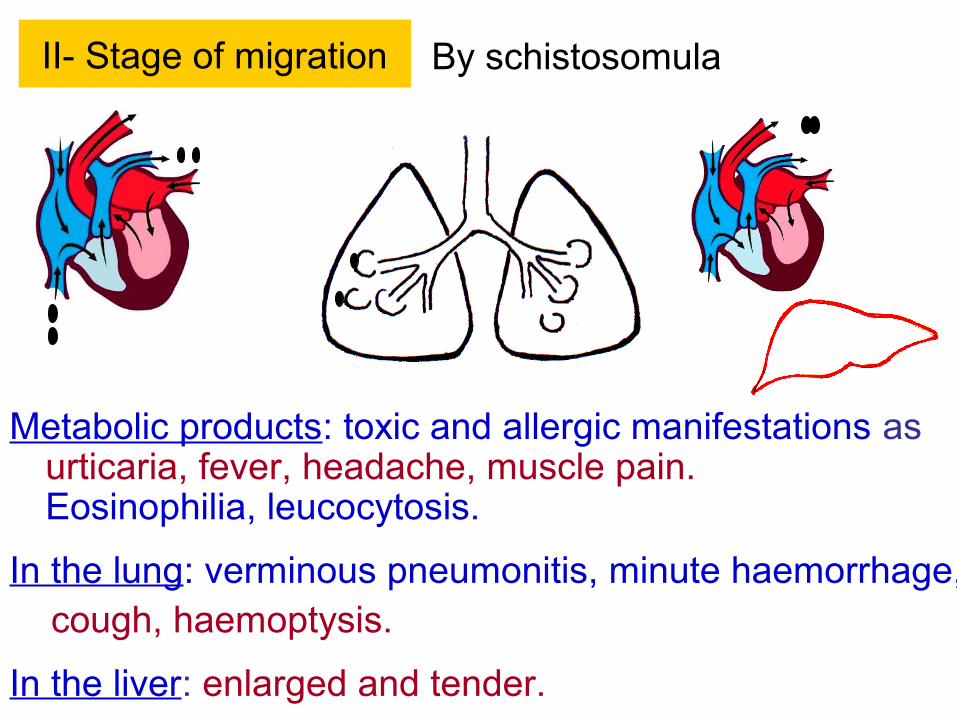
II- Stage of migration
Metabolic products: toxic and allergic manifestations as urticaria, fever, headache, muscle pain. Eosinophilia, leucocytosis.
In the lung: verminous pneumonitis, minute haemorrhage, cough, haemoptysis.
In the liver: enlarged and tender.
By schistosomula

III- Stage of egg deposition and extrusion
The patient may complain of:
Generalized malaise, fever,
rigors, urticaria, abdominal pain
and liver tenderness.
A- Eggs are deposited in the venous plexus
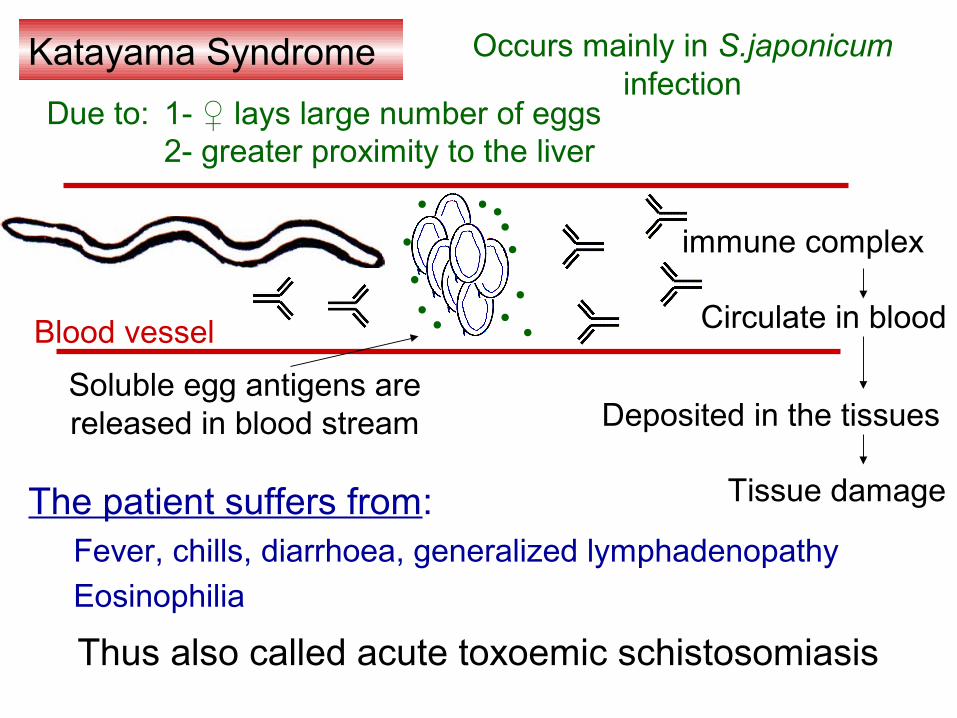
Katayama Syndrome
Blood vessel
Soluble egg antigens are released in blood stream
Occurs mainly in S.japonicum infection
1- ♀ lays large number of eggs2- greater proximity to the liver
immune complex
Deposited in the tissues
Tissue damageThe patient suffers from:Fever, chills, diarrhoea, generalized lymphadenopathy
Eosinophilia
Due to:
Thus also called acute toxoemic schistosomiasis
Circulate in blood
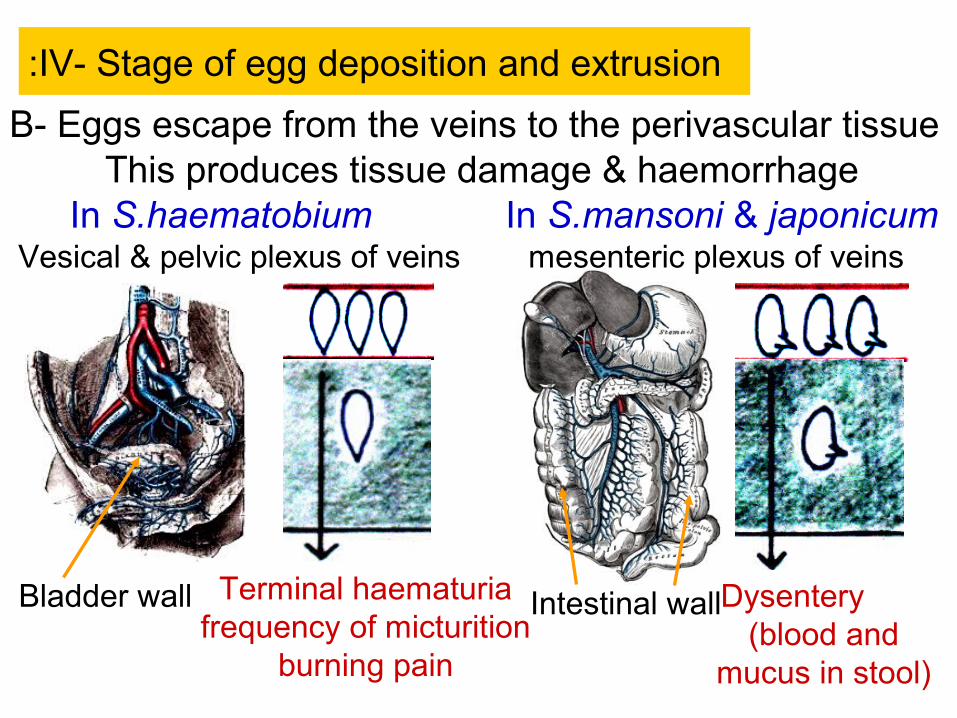
IV- Stage of egg deposition and extrusion:
Terminal haematuria frequency of micturition
burning pain
Dysentery (blood and
mucus in stool)
Vesical & pelvic plexus of veins
Bladder wall
mesenteric plexus of veins
Intestinal wall
This produces tissue damage & haemorrhageIn S.haematobium In S.mansoni & japonicum
B- Eggs escape from the veins to the perivascular tissue
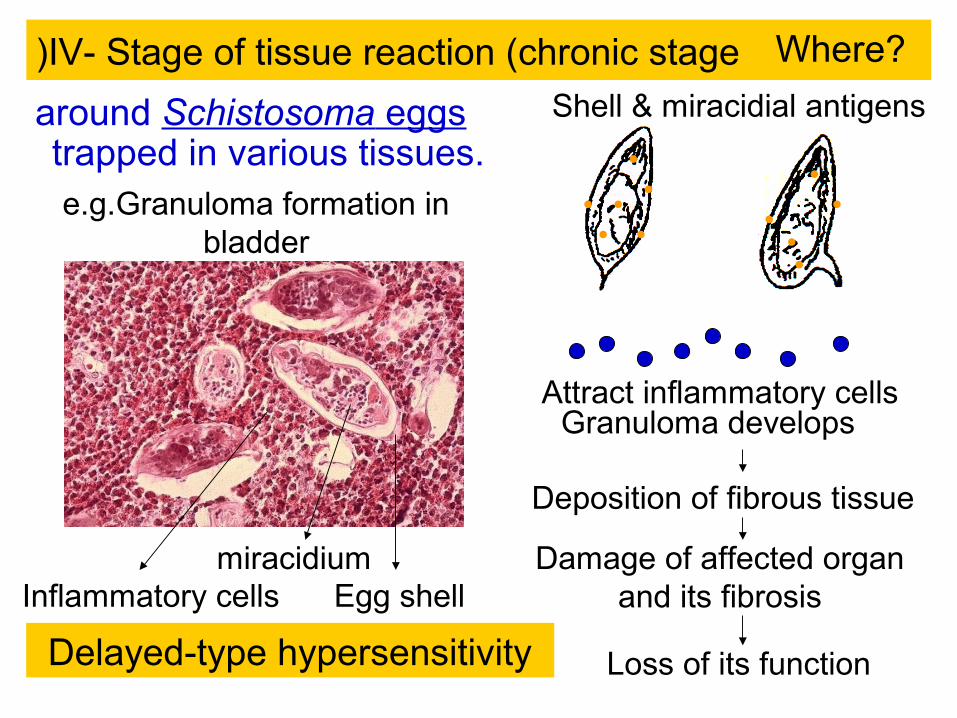
IV- Stage of tissue reaction (chronic stage)
around Schistosoma eggs trapped in various tissues.
Attract inflammatory cells
Deposition of fibrous tissue
Damage of affected organ and its fibrosis
Loss of its function
Egg shellmiracidium
Inflammatory cells
Shell & miracidial antigens
Delayed-type hypersensitivity
e.g.Granuloma formation in bladder
Where?
Granuloma develops

Polyps in the colon Barium enema that shows polyps in the colon
Tissue fibrosis, nodules, papillomata & sandy patches
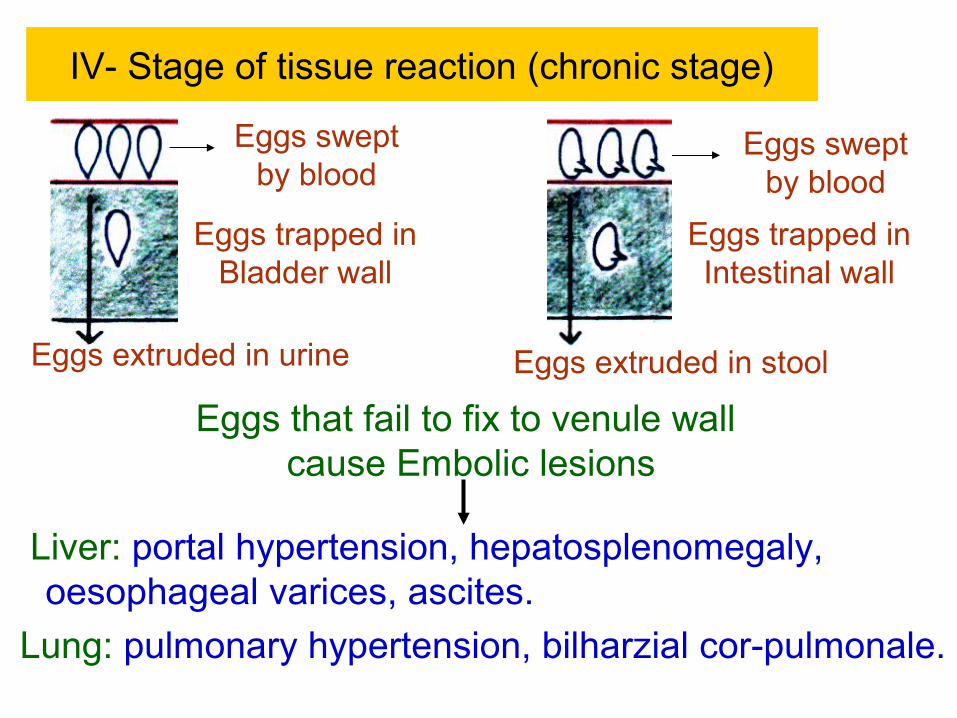
IV- Stage of tissue reaction (chronic stage)
Liver: portal hypertension, hepatosplenomegaly, oesophageal varices, ascites.
Lung: pulmonary hypertension, bilharzial cor-pulmonale.
Eggs swept by blood
Eggs trapped in Bladder wall
Eggs trapped in Intestinal wall
Eggs that fail to fix to venule wall cause Embolic lesions
Eggs swept by blood
Eggs extruded in urine Eggs extruded in stool

Diagnosis
• Direct parasitological methods:Detection of S.haematobium eggs in urine.Test for viability.
Detection of S.mansoni eggs in stool by direct smear method or by concentration method.
Kato thick faecal smear: for egg counting to assess the intensity of infection
Rectal swab
• Blood examination: eosinophilia, leucocytosis, anaemia.
I- Laboratory
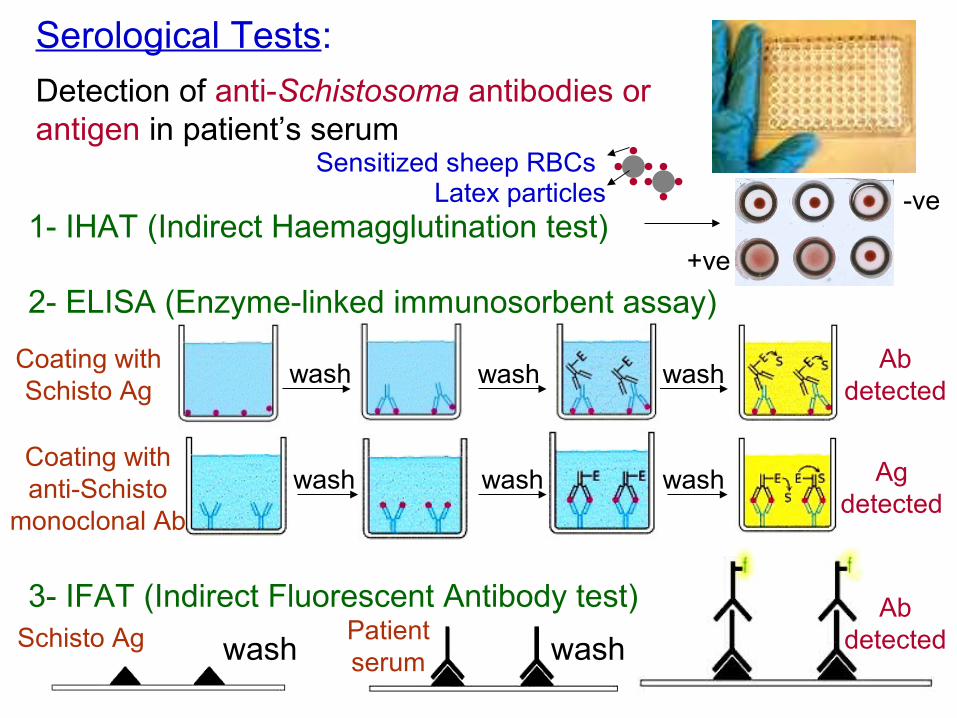
Serological Tests:
1- IHAT (Indirect Haemagglutination test)
Detection of anti-Schistosoma antibodies or antigen in patient’s serum
2- ELISA (Enzyme-linked immunosorbent assay)
3- IFAT (Indirect Fluorescent Antibody test)
wash wash
wash wash washAb
detected
wash wash wash Ag detected
Coating with Schisto Ag
Coating with anti-Schisto
monoclonal Ab
Latex particlesSensitized sheep RBCs
+ve
-ve
Schisto Ag Patient serum
Ab detected

Calcified bladder with hydroureter
Intestinal affection
Stenosed ureters and
hydronephrosis
II- Radiological imaging
S.haematobium infection S.mansoni infection

III- Endoscopyالمناظير
Cystoscopy S.haematobium
Colonoscopy, sigmoidoscopy S.mansoni
Done in chronic cases to detect lesions and take biopsies
Treatment
Praziquantel
Prevention and Control
- Mass treatment.
- Health Education.
- Snail control:
Physical methods
Biological methods
Chemical methods
X
Balanites aegyptica
Copper sulphate

Cercarial Dermatitis (Bather’s itch(
A condition that occurs due to penetration of cercariae of non-human species of schistosomes the skin of man.
Cercariae cannot go beyond the germinal layer.
Clinical picture:
Dermatitis, itching, oedema and secondary bacterial infection.
Treatment:
Antipruritics, antihistamincs,
antibiotics.

M.C.Q.
The major cause of morbidity in schistosomiasis is: a- Migration of adult worms against blood stream. b- Migration of adult worms in the liver. c- Embolic lesions. d- Deposition of eggs in tissues.
Kato technique is used to diagnose: a- Paragonimiasis c- Schistosomiasis haematobium
Bather’s itch occurs frequently with: a- S.haematobium b- S.japonicum
b- Schistosomiasis mansonid- Fascioliasis
b- S.mansonid- non human schistosomes

M.C.Q.
Katayama syndrome:
a- occurs most frequently in S.haematobium infection.
b- consists of pulmonary hypertension and right-sided heart failure.
c- occurs most frequently in S.japonicum infection.
d- occurs in chronic schistosomiasis.

Give reasons for
Terminal haematuria is due to active deposition of eggs by adult female S. haematobium in vesical venous plexuses.
Eggs escape to the perivascular tissue and become extruded to the lumen of the urinary bladder.
Powerful contraction of the bladder at the end of micturition (to squeeze the last drops of urine( leads to haemorrhage (terminal haematuria(.
Occurrence of terminal haematuria in S.haematobium infection
Lumen of urinary bladder
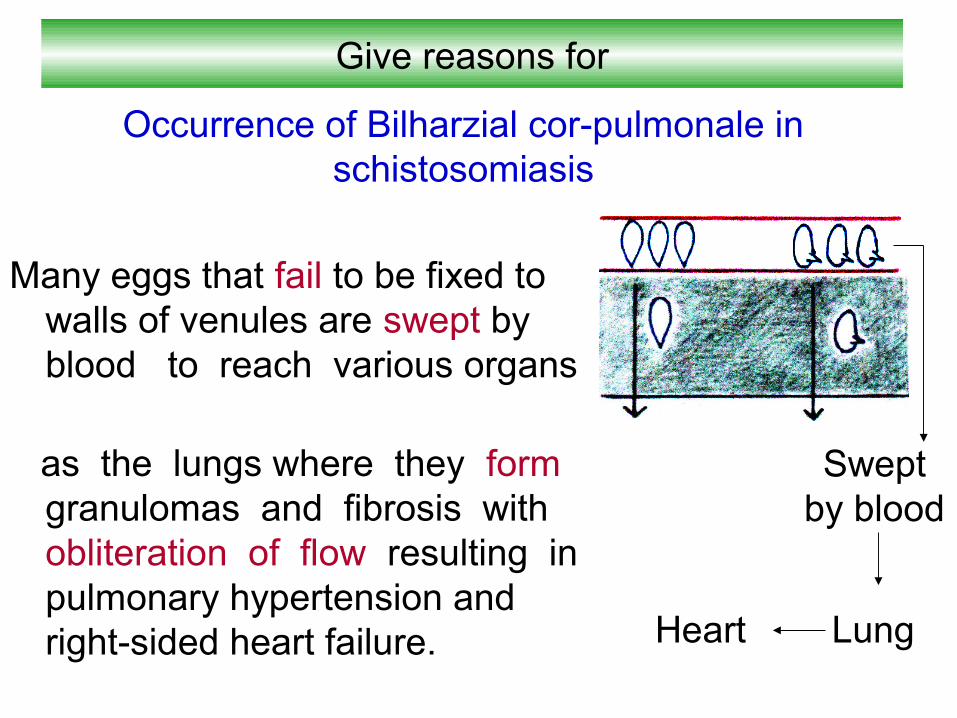
Give reasons for
Many eggs that fail to be fixed to walls of venules are swept by blood to reach various organs
as the lungs where they form granulomas and fibrosis with obliteration of flow resulting in pulmonary hypertension and right-sided heart failure.
Occurrence of Bilharzial cor-pulmonale in schistosomiasis
Swept by blood
Lung Heart