
SCASMM Sociodemographic factors and severe maternal morbidity: the risk of being less deprived...
33
SCASMM Sociodemographic factors and severe maternal morbidity: the risk of being less deprived Leslie Marr Reproductive Health Programme Manager November 2014
-
Upload
adelia-dennis -
Category
Documents
-
view
215 -
download
0
Transcript of SCASMM Sociodemographic factors and severe maternal morbidity: the risk of being less deprived...

SCASMMSociodemographic factors and severe maternal morbidity: the risk of being less deprived
Leslie MarrReproductive Health Programme Manager November 2014

A continuous audit of the factors associated with, and the incidence, causes and management of severe maternal morbidity in Scotland, 2003 – 2012
SCOTTISH CONFIDENTIAL AUDIT OF SEVERE MATERNAL MORBIDITY (SCASMM) WHAT WAS IT?
To generate information and provide feedback to clinicians in maternity services in order to improve clinical management, particularly in relation to national guidelines, and to inform service provision.
SCASMM – WHAT WAS ITS PURPOSE?

SCASMM – HOW WAS IT DONE?
•Basic information for 14 severe morbidities, gathered locally by a designated co-ordinator (usually a senior midwife) in each obstetric consultant led maternity unit
•Data analysed by the Reproductive Health Programme (RHP) of Healthcare Improvement Scotland
•Annual reports, including recommendations for practice produced and disseminated.Maternity unit level reports since 2010

CATEGORIES OF SEVERE MORBIDITY
• Major (obstetric) haemorrhage
• Eclampsia
• Renal/liver dysfunction
• Cardiac arrest
• Pulmonary oedema
• Respiratory dysfunction
• Coma
• Cerebrovascular event
• Status epilepticus
• Anaphylaxis
• Septicaemic shock
• Anaesthetic problem
• Pulmonary embolism
• ITU/CCU admission
(Information on interventional radiology collected from January 2010)
Mantel GD, Buchmann E, Rees H, Pattinson RC. BJOG 1998;105:985-90.

SCASMM FORMS

RCOG GUIDELINES

ANNUAL PUBLICATION: SCASMM

healthcareimprovementscotland.org
SCASMM REPORTS ON HEALTHCARE IMPROVEMENT SCOTLAND WEBSITE
SCASMM DEFINITION OF MAJOR OBSTETRIC HAEMORRHAGE (MOH)
One or more criteria:
• Estimated blood loss ≥ 2500 ml
• Transfused 5 or more units of blood
• Received blood products

RATES OF WOMEN WITH MOH AND OTHER MORBIDITIES 2004 - 2012

AGGREGATED RATES OF SEVERE MATERNAL MORBIDITY 2006 -2012

NUMBER OF REPORTED CASES OF ECLAMPSIA IN SCOTLAND, 2003-2012
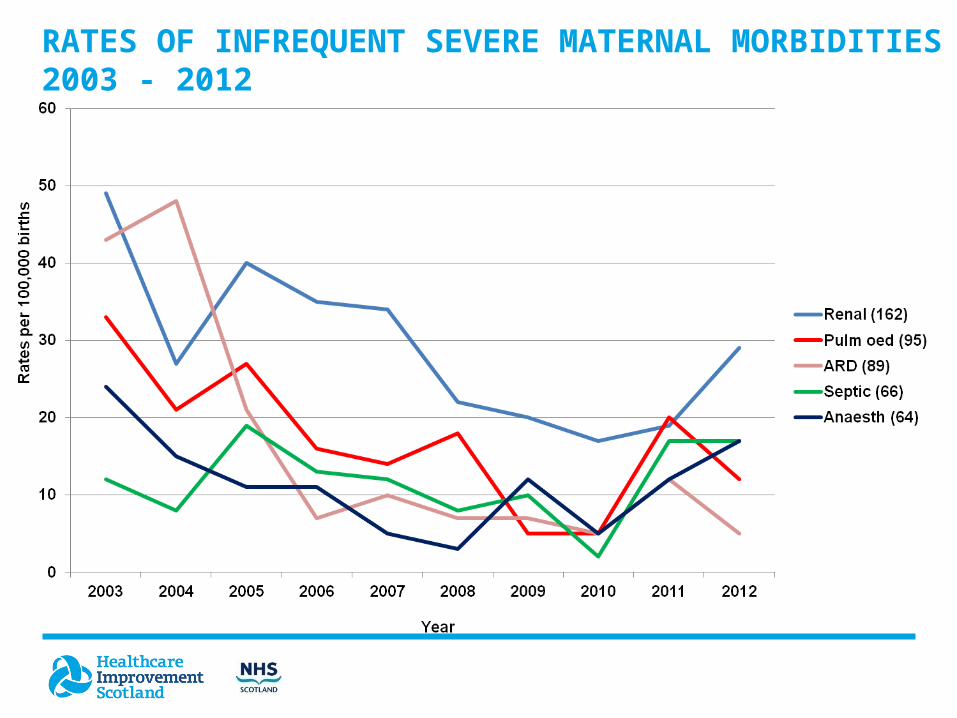
RATES OF INFREQUENT SEVERE MATERNAL MORBIDITIES 2003 - 2012

PERINATAL MORTALITY RATES FOR SEVERE
MATERNAL MORBIDITY 2005-12

MODE OF DELIVERY, ALL BIRTHS (2010-12) AND MOH
(2003-11)

TIME OF EVENT (2012)
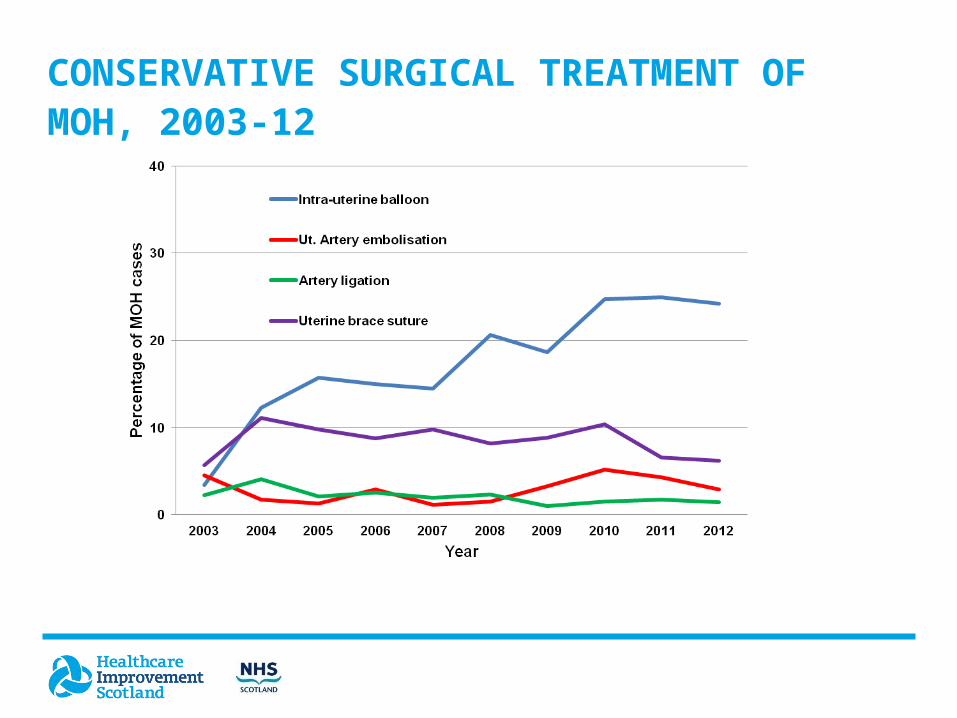
CONSERVATIVE SURGICAL TREATMENT OF MOH, 2003-12
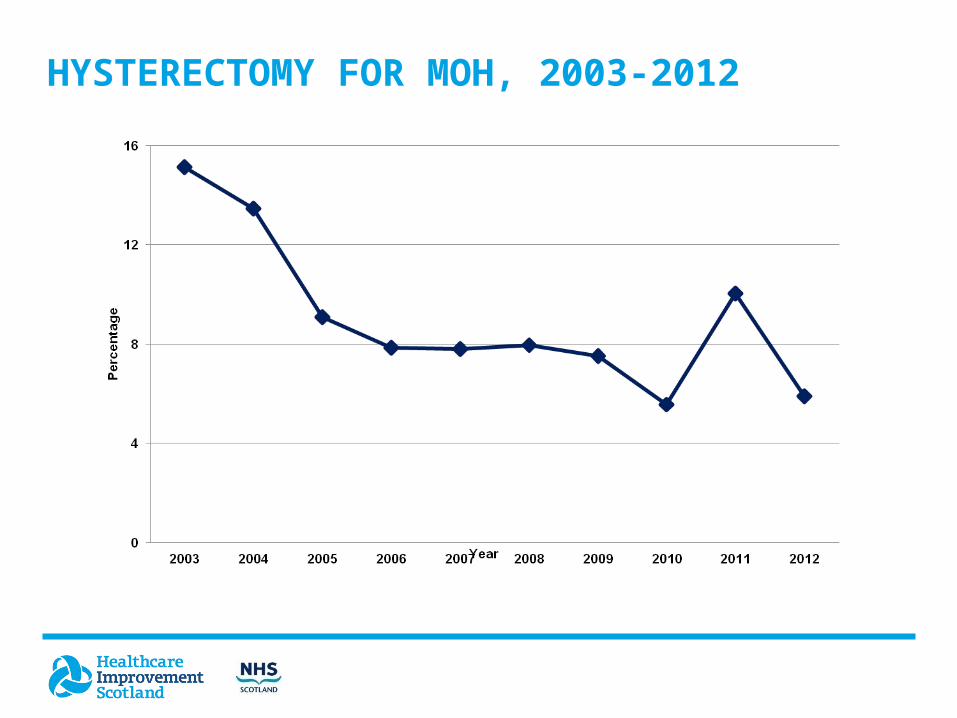
HYSTERECTOMY FOR MOH, 2003-2012

MORBIDITY IN CONTEXT (2006-08)
• Maternal mortality*: 1 in 9,000 births
• Maternal morbidityϮ: 1 in 170 births (1 in 137 in 2012)
• Mortality/morbidityϮ: 1/79
* SML UK dataϮ SCASMM data

DIRECT INVOLVEMENT OF CONSULTANT OBSTETRICIAN AND ANAESTHETIST IN CARE OF
MOH, 2003-2012

PROPORTION OF WOMEN WITH MOH IN 2011 AND
2012 ATTENDED OR NOT ATTENDED BY A
CONSULTANT OBSTETRICIAN IN RELATION TO TIME
OF DAY OR NIGHT

QUALITY OF CARE FOR WOMEN WITH MOH AS
ASSESSED BY MATERNITY UNIT, 2003-2012

SOCIO DEMOGRAPHIC ASSOCIATIONS: DATA COLLECTED FROM JANUARY 2009
Deprivation (SIMD)
Body mass index
Smoking
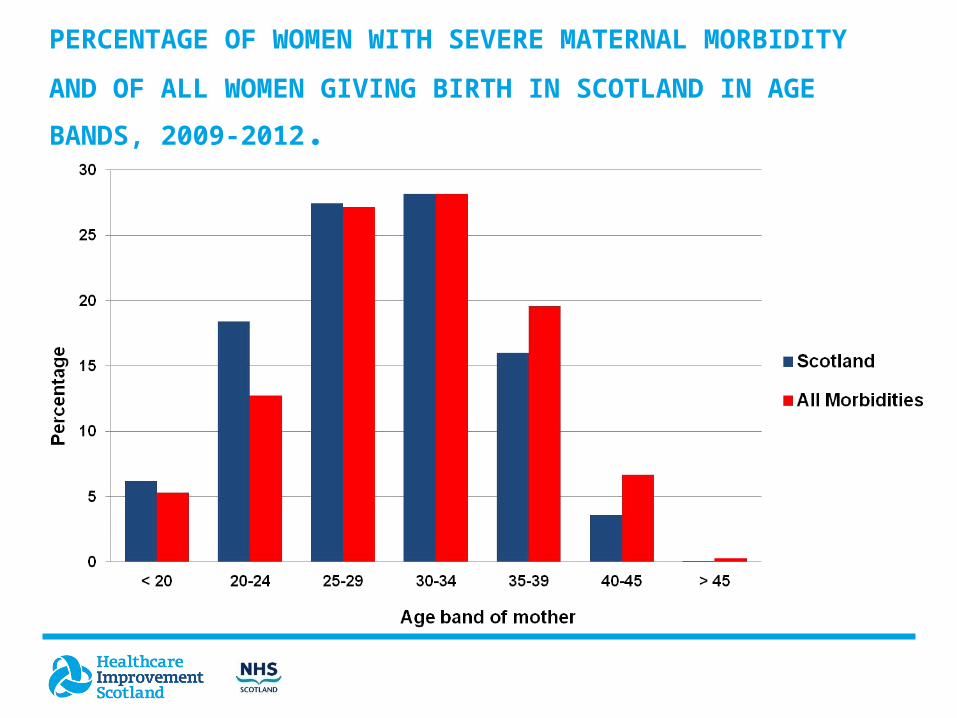
PERCENTAGE OF WOMEN WITH SEVERE MATERNAL
MORBIDITY AND OF ALL WOMEN GIVING BIRTH IN
SCOTLAND IN AGE BANDS, 2009-2012.

OBESITY
Increased risk with BMI >35 (12% of those with severe maternal morbidity, compared with 6.5% of all women giving birth in Scotland )

BODY MASS INDEX OF WOMEN WITH SEVERE
MATERNAL MORBIDITY AND WOMEN GIVING
BIRTH IN SCOTLAND, 2009-2012

BODY MASS INDEX OF WOMEN WITH SEVERE MATERNAL
MORBIDITY AND WOMEN GIVING BIRTH IN SCOTLAND,
2009-2012

SMOKING
At Antenatal booking (where known) reported by :
21% of women with severe maternal morbidity from 2009 – 2012
20.4% of women giving birth in Scotland between 2009 - 2012
However, Women < 20 years of age with severe maternal morbidity were significantly more likely to smoke and come from the most deprived quintile

DEPRIVATION

DEPRIVATION QUINTILE OF WOMEN WITH SEVERE
MATERNAL MORBIDITY AND OF ALL WOMEN GIVING
BIRTH IN SCOTLAND 2009-2012

• Obesity increases the risk of severe maternal morbidity
• Smoking does not appear to influence severe maternal morbidity
• Women in the most and least deprived quintiles are those most likely to experience severe maternal morbidity.
• Further work to assess the impact of maternal age and deprivation on severe maternal morbidity is required
CONCLUSIONS AND FUTURE ANALYSIS

• Chris Lennox – Reproductive Health Programme (RHP) Clinical Advisor, Healthcare Improvement Scotland (HIS)
• Angus K MacFadgen – Statistician
• Naomi Fearns – Clinical Audit Coordinator (RHP) (HIS)
• Kenny Gifford – Administrator (RHP) (HIS)
• Frank Dixon – National Records Scotland
• Kirsten Monteith - Information Analyst, Information Services Division
ACKNOWLEDGEMENTS


















