Scabies
79
Scabies & Pediculosis
-
Upload
oliyad-tashaaethiopia -
Category
Health & Medicine
-
view
319 -
download
10
description
Transcript of Scabies

Scabies & Pediculosis

Infestation Infestation is the presence of animal parasites on or in the body, is common in tropical countries and less so in temperate ones. Infestations fall into two main groups:
1 those caused by arthropods; and
2 those caused by worms.


Mechanisms of skin injury by arthropods Mechanical trauma Injection of irritant, cytotoxic or pharmacologically active substances Injection of potential allergens Invasion of the host's tissues Reactions to retained mouthparts Secondary infection

HISTORY
2500 yrs Sarcoptes scabiei is derived from the
Greek words
sarx (the flesh)
koptein (to smite or cut) and the
Latin scabere (to scratch). first ascribed to the mite by Giovan
Cosimo Bonomo in 1687.Over 300 million people worldwide
are infected

EPIDEMOLOGY women & children
urban areas,
winter
Prevalence 4 – 100%

Transmission
◦ directly by close personal contact, sexual or
◦ indirectly via fomites
factors◦ overcrowding,◦ delayed treatment of primary cases, and
◦ public awareness


highly host-specific an arthropod a member of the
class Arachnida, subclass Acari, order Astigmata, and family Sarcoptidae.
Too small to be seen by the naked eyeAdult female measures ~
0.4 - 0.3 mm, & the smaller male 0.2 - O.15
mm

body is creamy white & is marked by transverse corrugations,
ovoid
four-pairs of legs - anterior two pairs end in elongated
peduncles tipped with small suckers, In the female, the rear two pairs of legs
end in long bristles, whereas in the male bristles are present on the third pair and peduncles with suckers on the fourth.
crawl at a rate of 2.5 cm/min, burrow through the stratum corneum at the rate of about 2 mm per day(0.5 - 5 mm/day)
At temperatures below 20°C, S scabiei are immobile, although they can survive

number - <20 & with crusted scabies can be thousands to millions
live mites can survive for up to a week in the environment, feeding on the sloughed stratum corneum
cannot fly or jump

Pathogenesis
F (within 20 min) burrows into the stratum corneum (traverses at a rate of 0.5 - 5 mm/day)
avoid areas with a high density of pilosebaceous follicles

Mating takes place once, and the female is fertile for the rest of her life (1 mo),
Copulation in a small burrow---------the male, falls off the skin & perishes--------- Fertilized female enlarges the burrow using proteolytic enzymes to dissolve the stratum corneum of the epidermis ----- begins egg laying (3 eggs a day each)
Six-legged larvae emerge from the eggs after 3-4 days
90% of the hatched mites die

Escape from the burrow by cutting through its roof------then dig short burrows called moulting pouches & transform into nymphs-------------After further moult into larger nymphs , adult males and females develop(in 2-3 weeks)


Clinical features IP- 2-6 weeks
immediate symptoms –in re infection
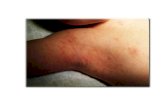
Triad`sPruritic papular lesions, Excoriations, andBurrowsSite- The circle of Hebra ~ an imaginary
circle intersecting the main sites of involvement - axillae, elbow flexures, wrists & hands, & crotch

Cont...... Pruritis
○ accentuate at night & exacerbated by a hot bath or shower
Primary lesions of scabies - burrows, papules, pustules,
nodules, occasionally urticarial papules and plaques
interdigital webbing of the hands,
flexural aspect of the wrists, behind the ears, axilla, waist, ankles, feet, buttocks & belt area
penile & scrotal in men, areola, nipples & genital area in women

Distribution of lesions

◦In very young children, infants, elderly and immunocompromised hosts, a widespread eczematous eruption primarily on the trunk is common , scalp & face can also be affected.

Contd... P/E The burrow
◦ pathognomonic sign and represent the intraepidermal tunnel created by the moving female mite. ◦ a 1-10 mm tunnel ◦ serpiginous, greyish-white thread-like elevations
◦ At the end of it a vesicle/pustule containing
the mite may be noted, especially in infants & children
at entry, slight scale

In infants, commonly located on the palms & soles : F
To identify burrows quickly:
apply a drop of India ink or gentian violet to the infested area, remove it with alcoholThin threadlike burrows retain the ink

Contd... Erythematous Papules & Vesicles (filled with serous
fluid) rarely contain mites and most likely are due to a hypersensitivity reactionPapules= on the shaft of the penis &
scrotum in men & on nipples in women
Vesicles= on the palms & soles

Animal Scabies: Zoonotic scabies◦ affect humans who come in close
contact with the animal◦ incubation period is shorter, the
symptoms are transient◦ usually manifests with vesicles &
papules with atypical distribution◦ Burrows are usually absent◦ runs a self-limited course, require no
treatment Mites from animals are not a
source of human infestation, but they can produce bite reactions
Asymptomatic infestation◦ not uncommon ◦ considered ‘carriers’


Secondary scabies lesions
With rubbing- secondary infection, - the host immune response against the mites and their products. Excoriations, Lichenification, widespread eczema, honey-colored crusting, postinflammatory hyperpigmentation, erythroderma, and frank pyoderma

DDx
Atopic dermatitis Insect bites Contact dermtitis Autosensitization ('id' reaction)
Drug eruptions PPE

VariantsVariants
Nodular scabies in 7-10% of patients with active scabies Pink, tan, brown, or dull red nodules (2-20 mms)
May or may not itch Persist on the scrotum, penis, and vulva and In neonates unable to scratch, pinkish-brown nodules may
develop usually sterile
Intralesional steroids, tar, or excision are methods of treatment

DDxNodular scabies
Papular urticaria (insect bites)
Prurigo nodularis
Secondary syphilis

Bullous scabies
Mimics BP both clinically & histologically (contain many eosinophils)
Vesicles and bullae-, particularly on the palms & fingers
Immunofluorescent

In immunocompromised / debilitated patients, including those with:
neurologic disorders, Down syndrome, organ transplants, graft-versus-host disease, adult T-cell leukemia, leprosy, or AIDS and institutionalized populations
Risk factors for profound infestation -an inability to mount an immune response, perceive pruritis, and/or physically scratch the skin
Crusted scabies (Norwegian/hyperkeratotic scabies)

* marked thickening and crusting of the skin.
* Hyperkeratotic, crusted/scaling lesions teem with mites
* large areas with prominent scalp lesions,
hands and arms are usual locations * Swollen & crusted finger tips; &
dystrophic nails * Pruritis- minimal/absent

Contd...The rest of the skin usually appears diffusely xerotichighly contagiousSevere fissuring & scaling of the genitalia & buttocks may be presentOral agent should be used in conjunction with a topical agent

DDxCrusted scabies
Psoriasis
Seborrheic dermatitis

Complications
Secondary impetiginization
Lymphangitis & septicemia ~ particularly in crusted scabies
Post-streptococcal glomerulonephritis
'post-scabietic pruritus‘◦ represent the body's response to dead mites that are
eventually sloughed off (within 4 wks) along with natural epidermal exfoliation
◦ Tx- antihistamines or a short course of topical or oral corticosteroids

Scabies and HIV frequent
unusual features
head and neck
occur with minimal or no pruritis but with an extensive papulosquamous eruption( i.e.,hyperkeratotic,
Crusted scabies- soles
- should arouse suspicion of underline HIV
difficult to eradicate
Oral ivermectin (200 1Micg/kg weekly) is the most effective

Diagnosis
Mainly clinicalPruritus with typical lesions & distribution
Contact Hx
Microscope
○Skin scrapings obtained from the finger webs, wrists, or ankles is most likely to be positive
○In Norwegian scabies, scraping of the thick scales will often yield several viable mites(100)
○Excoriated lesions are often negative

Dermoscopy PCR
Biopsy

Contd...H/pH/p
A patchy to diffuse infiltrate with eosinophils is noted in the reticular dermis
On transection, a scabies mite may occasionally be seen within the epidermis
fragments of the adult mite exoskeleton
serve as a clue to the Dx when mites, scybala or eggs are not identified

Treatment
Age cost severity ? previous treatment status
In infants with extensive involvement, several re treatments a week apart occasionally be required
second application of topical medication.......
Treat simultaneously all household contacts (even with no symptoms)

Contd...

Medications 1) 1) Permethrin
5% cream applied for 8 -14 hrs
standard first line topical scabicide
MoA= produce nerve paralysis & death in ectoparasites by causing delayed repolarization by disrupting Na+ current~ ovicidal
2) Benzyl benzoate(BBL)
Derivatives of balsam of peru12.5% & 25% emulsion
lotion overnight application for three consecutive nights or left to the skin for 48hrs
MOA= ?kills the adult scabies mite with yet unclear action
exerts toxic effects on the nervous system of the parasite, resulting toxic to mite ova, though its exact mechanism of action is unknown.

Contd...3) Precipitated sulfur
◦ 6-10% precipitated sulfur ointment in a petrolatum base (for children 2.5%)
◦ Applied to the entire body for three successive nights~ 2wks
MOA= kills adult scabies mite
interact with cysteine, present in the stratum corneum, to form hydrogen sulfide---
safe in preg and neonates
Efficacy = as high as 92%
4) ivermectin Structurally similar to macrolide antibiotics,
MoA= blocks neurotransmission across nerve synapses that utilize glutamate or GABA(y-aminobutyrica cid) --- cause paralysis of peripheral motor function in insects
Age specific

Contd...Ivermectin
dosage- 200 micg/kg; often the dose is repeated in 10 to 14 days
LINDANE 1% lotion or cream applied only in a thin
coat to dry skin should not be applied
immediately after bathing
M/A= ?? Inhibits inositol in scabies mite to produce CNS excitation & death of the parasite
Inhibits GABA
C/I= children < 2 yrs of age, pregnant & lactationWeight --

Follow-up visits
In 2 weeks is important to ascertain success or failure of therapy
Any new lesions
'post-scabietic pruritus‘ body's response to dead mites- till 4th week after treatment.
steroids

Prevention

Pediculosis
Phthiraptera family Order Anoplura-blood-sucking (***solenophages)
ectoparasites of mammals
Pediculus capitis, the head louse Pediculus humanus, the clothing or body louse
& Pthitrus pubis, the pubic or crab louse
ingest blood, & produce skin lesions by mechanical puncture( stylet, haustellum) & injecting toxic secretions

Pediculosis Capitis
Head lice
in school-aged children, 3-12yr, 10%of children : F
affect all levels of society & all ethnic groups◦ Prevalence= 6 to 12 million infestations/year
◦ incidence is low among African Americans
◦ spread by close physical contact◦ sharing of head gear, combs, brushes, & pillows

Etiology & Pathogenesis
is 1 to 2 mm long, elongated, greyish white flattened dorsoventrally, & wingless three pairs of sharp clow- grasp hairs and for feeding feed approximately five times each day
5 - 10 eggs a day can travel up to 23 cm/min The larva, called a nymyh/instar, looks like a miniature
adult louse 1 - 2 days (4 days) away from the scalp (Nits up to 10 days) 30 days *Head lice do not carry or transmit any human disease. hatches in 8 to 10 days, and reaches maturity in
approximately 18 days. Nits are .8mm, with operculum



Clinical findings
Louse - occipital and retro auricular regions◦ <20 but in 5% >100
Itching or can be asymptomatic◦ a result of hypersensitivity reaction to the
saliva & faecal matter produced by the louse during feeding
◦ Sensitization - 3-8month
hemorrhagic crust Excoriations, lymphadenopathy, &
conjunctivitis(redness &swelling) may be observed

Contd...Diagnosis
Identification of live adult lice, immature nymphs, and/or viable-appearing eggs
Live nits(egg cases) placed in close proximity to the scalp(parietal & occipital)
Have proteinaceou sheath
◦ cemented to the hair shaft with chitinous material secreted by the female accessory glands
C0MPLICATIONS
Excoriation ----- Secondary bacterial infections

DDx
Seborrheic
piedra
Delusion parasitosis
Artifacts on the hair
Hair casts (pseudonitis)

Pediculosis corporis (Body/clothing lice)
EPIDEMIOLOGY
low of socio-economic
in urban public hospitals
No predilection for race, age, or sex
contaminated clothing or bedding

ETIOPATHOGENESIS
Body Iouse/P. humanus var humanus
lifespan -18 days 270 to 300 ova
2-4mm
3 day,with out meal comes to the surface only for meal

CLINICAL FEATURES
linear excoriations primarily
Occasionally, a macula ceruleae (Iiterally, sky-blues pot)◦ a blue to slightly slate-colored macule.............bruise-like lesion (~1.5 cm) & often with a central punctum 2nd to altered blood pigments in clothing binds (waistband, buttocks & thighs) & is asymptomatic to slightly pruritic

Contd...
Diagnosis examining the lining of
the clothing seams for the presence of nits
By shaking out the clothing over a sheet of newsprint,
Nits that contain an unborn louse fluoresce white.
Nits that are empty fluoresce gray.

DDx Scabies
AD
ACD
Drug reaction
Viral exanthem
Systemic cause of pruritus

COMPLICATIONS
Excoriation
secondary infection with S. aureus, S. pyogenes & other bacteria (impetigo & furunculosis)
act as vectors for R.prowazekaii (epidemic typhus), Bartonella quintana (trench fevers or endocarditis) & Borrelia recurrentis (relapsing fever)

Pediculosis pubis (Pubic Lice)
EPIDEMIOLOGY
most often are a sexually transmitted disease
~ 30 % of patients have another concurrent STI
from one sexual exposure with an infested partner is more than 90%
contaminated clothing, towels, or beddings

ETIOPATH0GENESIS
Pthiridae
crab - naming
second and third pairs of -to cling on to hair (pincer like claws)
light brown
0.8 to 1.2 mm in length
ambulate up to 10 cm/day
lifespan of 2 wks
25 ova
away from the human host for up to 36 hrs
dog

CLINICAL FEATURES
Pruritus
Maculae ceruleae (sky-blue spots, (tache bleu), on inner thighs or sides of trunk
Bullous lesion
adult organisms on the body ( ~ 10 - 25 or more) pubic hair, any hair bearing site can be affected,
eyelashes ((phthiriasis palpebrarum○ in hirsute ~ short hairs of the thighs, trunk, & perianal
area
nits near the base of the hair the duration of infestation can be approximated by the
distance of the nit from the skin surface

Contd...
Diagnosis louse in the pubic area
coexisting STI
microscopic examination Empty nits may
indicate a prior infestation
COMPLICATIONS excoriation
Secondary infection -lymphadenitis & fever
. generalized exanthem (pityriasis rosealike pediculid).

DDx Scabies Extensive excoriation Contact dermatitis
White piedra Trichosporon cutaneum
Trichomycosis pubis
Hair casts

Treatments
PYRETHRIN (SYNERGIZED/SYNTHETIC= PERMETHRIN/PIPERONYL BUTOXIDE) 1%, 5% SHAMPOO
Block Na+ channel repolarization
Topically for 10min, repeat a wk later for body louse
100% cidal- 10min
PERMETHRIN 1% CREAM
◦ Topically 8 -12 hrs repeat in 7 -10 days
◦ Currently treatment of choice for body louse

MALATHION 0.5% LOTION
◦ Organophosphate cholinesterase inhibitor
◦ Topically for 8-12hrs (20-30min)
LINDANE SHAMPOO 1%
◦ Organochloride acts as GABA inhibitor
◦ Topically for 5-10min, not to be repeated

Contd...
Ivermectin, oralInhibit GABA release & cause respiratory paralysis
250micro gm/kg a week apart
not ovicidal
Wet combing Occlusive or
suffocation Boiling of clothing(65 *C), bedding, &
other possible fomites is ovicidal & lousicidal
cotimoxazole acctylcholincsterase
inhibiting insecticides
Robi comb, Tea tree oil and lavender oil

Eye tx
thick layer of petrolatum twice a day for 2 weeks (interere respiratory function –block)
mechanical removal cryotherapy flurescein 10-20% mercuric oxide physiostigmine ointment!!!!!!!!! Oral ivermectin argon laser photo therapy aqueous pediculicide

Contd...
Patients with HIV/AIDS◦have more severe infestations with p. pubis &
◦unresponsive to conventional therapy

References
EMEDICINERook'sTextbook of Dermatology

THANK U!

Malathion, carbaryl and permethrin preparation are probably the treatments of choice now. They kill lice and eggs effectively;
malathion has the extra value of sticking to the hair
and so Lotions should remain on the scalp for at least 12 h, and are more effective than shampoos. The application should be repeated after 1 week so that any lice that survive the first application and hatch out in that interval can be killed.protecting against reinfection for 6 weeks.

Intralesional steroids, tar, or excision are methods of treatment for this troublesome condition, termed nodular scabies.
Sensitization
majority of mites are found on the hands and wrists,
Children have often gathered mites
and ova under the nails when scratching.

Permethrin 5% cream (Elimite) is the most widely used medication for scabies. It is a synthetic pyrethroid that is lethal to mites and has low toxicity for humans.
Lindane (y-benzene hexachloride) is also effective, with a low incidence of adverse effects when used properly. Because of
the availability of less toxic agents, lindane is rarely used as a first-line agent. In much of the world, benzyl benzoate and 10% precipitated sulfur in white petrolatum are used to treat scabies. The
scabicide should be thoroughly rubbed into theskin from the neck to the feet, with particular attention given to the creases, perianal areas, umbilicus, and free nail edge and folds. It is washed off 8 to 10 h later. Clothing and bedlinen are changed and laundered thoroughly.
Crotamiton (Eurax) has a lower cure rate than other available agents. When used, it should be applied on 5 successive nights and washed off 24 h after the last use.

it usually takes 2-6 weeks
before the host's immune system becomes sensitized to the mite or its by product
'post-scabietic pmritus'.
body's response to dead mites
second application of topical medication is performed in order to reduce the potential for reinfestation from fomites as well as to ensure killing of any nymphs that may have hatched as a result of thesemi-protective environment within the egg that allowed them to survive

Lotions should remain on the scalp for at least 12 h, and are more effective than shampoos. The application should be repeated after 1 week so that any lice that survive the first application and hatch out in that interval can be killed. A systemic antibiotic may be needed to deal with severe secondary Infection a head louse repellent, containing 2% piperonal, is available over the counter and may be worth a trial for those who are repeatedly reinfested. Systemic ivermectin therapy is reserved for infestations resisting the treatments listed

th e head and body lice
may be variants within a single species,
but are thought by most biologists to
represent two distinct species that can
hybridize or interbreed under special circumstances.

peri pilar keratin casts
('pseudonits'; hair muffs) [21,221 or dried globules of
cheap hair lacquer.
The acctylcholincsteraseinhibiting
insecticides malathion and carbaryl (carbaril)
Robi comb, co-trimoxazole, Tea tree oil and lavender oil
prophylaxis

Treatment failure Evidence
the presence of adult organisms should be suspected if live lice are still present 12 to 24 hours after
treatment
Failure to follow instructions changing formulations, dilution of the pediculicide subtheraputic doses or duration
Neglecting to treat sexual contacts
Treating only the pubic area in hairy individuals
Re-infestation