SARS Timeline Nov 16 ‘02 Feb 11 ‘03 Feb 28 March 11 March 12 March 19 March 27 April 5 April 9...
23
SARS Timeline Nov 16 ‘02 Feb 11 ‘03 Feb 28 March 11 March 12 March 19 March 27 April 5 April 9 April 14 April 17 April 28 First cases Hong Kong WHO Sequence retrospectively and Vietnam issues of suspected Recognized, report out- travel agent, a Guangdong, breaks in advisories coronavirus, China hospital established workers China Acute coverup India respiratory WHO admitted; reported in issues SARS SARS Guangdong global made top by China alert priority Vietnam MOH contain- Reported First ing virus First in U.S. and SARS in (WHO) SARS Europe Africa case – Vietnam
-
date post
19-Dec-2015 -
Category
Documents
-
view
215 -
download
1
Transcript of SARS Timeline Nov 16 ‘02 Feb 11 ‘03 Feb 28 March 11 March 12 March 19 March 27 April 5 April 9...

SARS Timeline
Nov 16 ‘02 Feb 11 ‘03 Feb 28 March 11 March 12 March 19 March 27 April 5 April 9 April 14 April 17 April 28
First cases Hong Kong WHO Sequence
retrospectively and Vietnam issues of suspected
Recognized, report out- travel agent, a
Guangdong, breaks in advisories coronavirus,
China hospital established
workers China
Acute coverup India
respiratory WHO admitted;
reported in issues SARS SARSGuangdong global made top
by China alert priority Vietnam
MOH contain-
Reported First ing virus
First in U.S. and SARS in (WHO)
SARS Europe Africa
case –
Vietnam

Case Distribution of SARS Worldwide
ERSI, May 2003
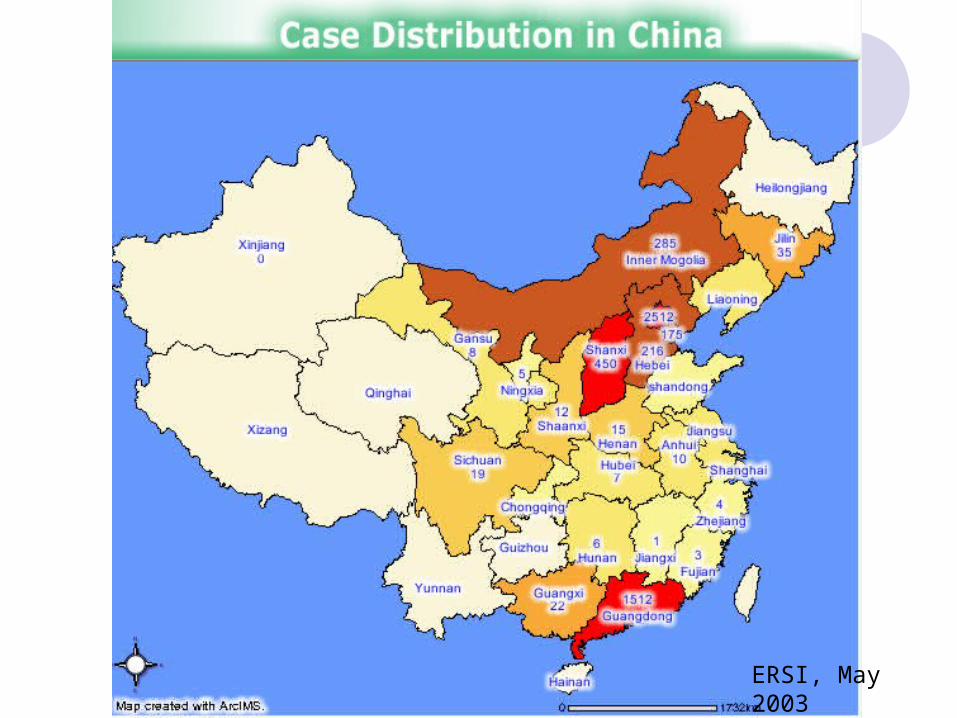
ERSI, May 2003

Hotel MHong Kong
Guangdong Province,
China A
A
H,JA
H,J
Hong Kong SAR
95 HCW
>100 close contacts
United States
1 HCW
I, L,M
I,L,M
K Ireland
0 HCWK
Singapore
34 HCW37 close contacts
C,D,E
C,D,E
B
B
Vietnam
37 HCW
21 close contacts
F,G
Canada
18 HCWF,G
11 close contacts
Effect of Travel and Missed Cases on the SARS EpidemicSpread from Hotel M, Hong Kong

SARS Hotspots (as of May 28, 2003)
# Probable Cases # Deaths
China 5322 321Hong Kong 1728 269Taiwan 596 76Singapore 206 31Canada 148 26United States 65 0Vietnam 63 5Philippines 12 2Other Countries 62 4
Total 8202 734

0
50
100
150
200
250
4,22
4,24
4,26
4,28
4,30
5,02
5,04
5,06
5,08
5,10
Number of SARS Cases Reported over Time (China)

Symptoms of SARS
• Cough• High fever• Severe pneumonia• Difficult to distinguish from other
respiratory diseases in early stages

1.6
7.2
29.2
18.7
21.5
18.016.1 16.5
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
0- 10- 20- 30- 40- 50- 60- 70-
( 1/1,000,000)
Incidence Difference across Different Age Groups (China)
CDC, 2003

0.0 0.0 0.93.0
5.0
10.0
17.6
28.026.3
0.0
5.0
10.0
15.0
20.0
25.0
30.0
0- 10- 20- 30- 40- 50- 60- 70- 80-
Fatality Rates of Different Age Groups
CDC, 2003


Etiology

SARS DiagnosticsKey Messages
• SARS diagnostic assays are sensitive and specific, but may not provide definitive diagnosis early in the illness
• Changes in the quantity, type, and timing of specimens collected may improve detection of SARS-CoV infection
• Rapid and accurate diagnosis of other respiratory pathogens associated with SARS-like illness may help rule out SARS-CoV infection and calm public fears
• Interpretation of test results must take into consideration possibility of false positives and negatives; a clear strategy to minimize such possibilities and to confirm test results are essential
CDC, 2003
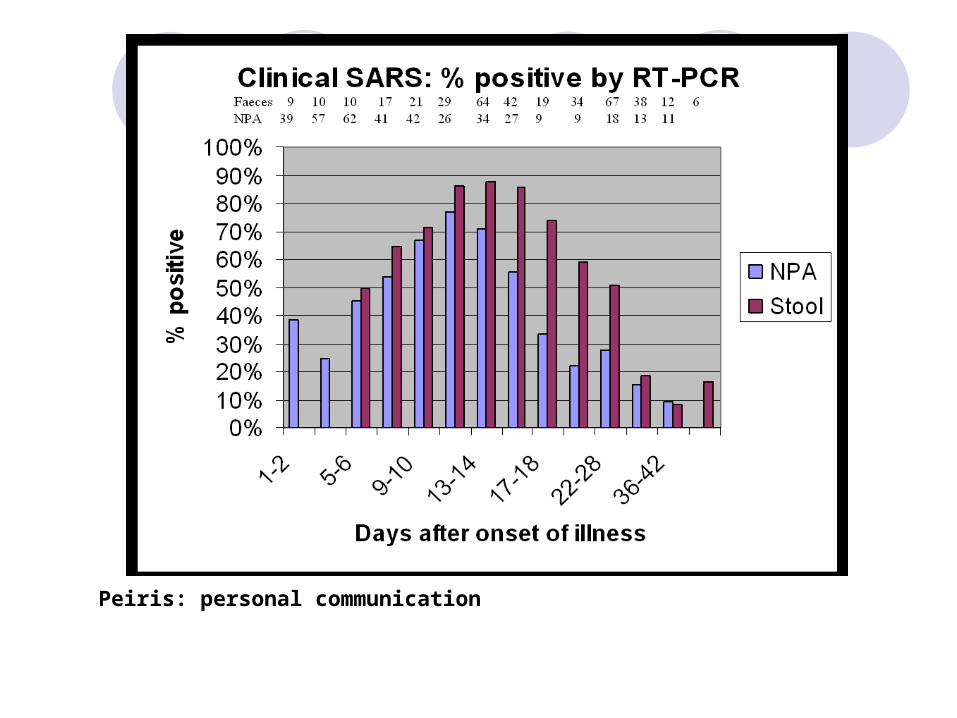
Peiris: personal communication

Prevention of SARS


Definitions of Quarantine Isolation
• Separation and restricted movement of ill persons with contagious disease
• Often in a hospital setting• Primarily individual level, may be populations
Quarantine• Separation and restricted movement of well persons
presumed exposed to contagion• Often at home, may be designated residential facility• Applied at the individual or community level
May be voluntary or mandatory
CDC, 2003

A collective action for the common good predicated on aiding individuals infected or exposed to infectious agents while protecting others from the dangers of inadvertent exposure
Public good Civil liberties
Modern Quarantine
Meeting needs of individuals infected and exposed is paramount
CDC, 2003

Key Issues to Consider
• Surveillance• Clinical evaluation • Infection control measures• Patient isolation• Engineering controls• Exposure evaluation• Staffing needs and personnel policies• Access controls• Supplies and equipment• Communication
CDC, 2003

SARS Mysteries
Origin of SARS – animal reservoirs?
Is coronavirus the etiologic agent?
• Cases without antibody
• Non-cases with antibody

SARS Mysteries (continued)
What proportion of exposed persons
develop clinical disease and death?
• Proportion of exposed, infected and asymptomatic
Are there asymptomatic carriers?
• Reports of cases without known source of exposure

SARS Mysteries (continued)
What causes “super shedders”?• Host characteristics; e.g., age
• Agent characteristics – “virulent strain”
Is pathology caused by the virus or the
response to the virus?
• AIDS patients appear to be resistant to SARS

SARS Mysteries (continued)
Will SARS reappear in the fall?
• SARS is transmitted through the respiratory route. These diseases, like influenza, tend to have a season cycle with resurgence in the late fall, winter and early spring

Will SARS Re-emerge?
Potential sources of re-emergence
• Animal reservoir
• Humans with persistent infection
• Unrecognized transmission in humans
• Laboratory exposure
SARS most likely to recur outside U.S.
• Well-established global surveillance is important to recognition of first case










![[XLS]imprintartservices.comimprintartservices.com/data/Data 1/Billing Sheets/Billing... · Web viewBONICA MAY May,2011 April Overview Bonica April April,2011 March,2011 Feb, 2011](https://static.fdocuments.us/doc/165x107/5ad1bcb47f8b9a05208bf050/xls-1billing-sheetsbillingweb-viewbonica-may-may2011-april-overview-bonica.jpg)