SAR PPT 1-Program_07

of 36
Transcript of SAR PPT 1-Program_07
PowerPoint
ACUTE RADIATION SYNDROME1This lecture is directed to medical professionals who may be involved in the management of radiation injuries starting from the first few hours or days after an exposure of undefined severity (i.e. those handling the emergency situation may not know the extent and severity of the accident). Experience has shown that the complete management of emergency care involves, in addition to occupational physicians, other professionals such as haematologists, oncologists, plastic surgeons, dermatologists, vascular surgeons, psychiatrists and consultants in other medical specialties. The principal aim of this module is to provide guidelines for carrying out prompt diagnostic measures and emergency treatment.
The most important radiation effectsEarly(deterministic only)LocalRadiation injury ofindividual organs:functional and/ormorphologicalchanges withinhrs-days-weeksCommonAcute radiation syndrome
LateDeterministicRadiation dermatitisRadiation cataractaTeratogenic effects
StochasticTumours LeukaemiaGenetic effects
2Radiation effects may appear - early (i.e. within three months) or - late (beyond 3 months, usually in years).Early effects result from high dose radiation to partial body or whole body. They are all of deterministic type. Among the local effects the most frequent is the radiation induced skin injury. Acute exposure of the whole body is early expressed in the rather general symptoms of the acute radiation syndrome (ARS) or acute radiation disease. It leads to death - without treatment - in 3-6 weeks if the radiation absorbed in the whole body dose is above 5 Gy. The LD50/60 dose is about 3.5 Gy when there is no possibility of specialized treatment. However, with specialized haematological treatment and provision of sterile conditions, the effects of doses even twice as high can be cured and the patient can be saved. Note: The table refers to equivalent dose in sieverts, understanding that the biological effect depends on both the absorbed dose and type of radiation (i.e. its ionizing capability). However, in by far most of the cases accidental overexposures are caused by beta-, gamma- or X rays having a radiation weighing factor of unity. In these cases 1 Gy = 1 Sv, while in case of neutron irradiation the absorbed neutron energy (kerma) may be 2-5-times lower (depending of the energy of neutrons) of the threshold values given in the above table!Among the late effects we can distinguish deterministic effects, such as dermatitis, cataracta or teratogenic effects. They develop if the cumulative absorbed dose is above of a cumulative threshold dose required for the given effect. Thus, teratogenic damage may only develop if the absorbed dose in the foetus is above 0.1 Gy. The stochastic late effects are cancer and genetic (hereditary) effects, usually appearing after many years.Forms of radiation injury depending on conditions of radiation exposureAcute total external radiation exposureAcute radiation syndromeAcute local external irradiation or external contaminationLocal radiation injury Acute total external radiation exposure with external or internal contaminationAcute radiation syndrome coexisting local or internal radiation injury Combined exposure of radiation and non-radiation factorsCombined radiation injuryChronic external or internal radiation exposureChronic radiation syndrome3Forms of radiation injury depending on conditions of radiation exposure. After acute total external radiation exposure developing acute radiation syndrome, after acute local external irradiation or external contamination local radiation injury, after acute total external radiation exposure with external or internal contamination acute radiation syndrome coexisting local or internal radiation injury, after combined exposure of radiation and non-radiation factors combined radiation injury, after cronic external or internal radiation exposure chronic radiation syndrome. Early deterministic effects after whole body irradiation< 0.1 Gy no detectable difference in exposed or non-exposed patients0.10.2 Gy detectable increase in chromosome aberrations, but no clinical signs or symptoms0.12 Gy sperm count decreases to minimum about day 45 0.3 Gy detectable temporary sterility for man0.5 Gy detectable bone marrow depression with lymphopenia4Below 0.1 Gy, whole body (WB), there is no detectable difference in exposed vs non-exposed patients.Detectable increase in chromosome aberrations by cytogenetic dosimetry is found in whole body doses greater than 0.1-0.2 Gy but still there are no clinical signs or symptoms.Sperm count decreses to minimum about day 45 at doses more than 0.12 Gy WB.Bone marrow depression with lymphopenia can be detected at doses 0.5 Gy WB.Exposure levels at which healthy adults are affected_________________________________________________________________Health effects Acute dose, Gy_________________________________________________________________ Blood count changes 0.50 Vomiting (threshold) 1.00 Mortality (threshold) 1.50 LD50/60 (minimal supportive care) 3.2-3.6 LD50/60 (supportive medical treatment) 4.8-5.4 LD50/60 (autologous bone marrow or > 5.4 stem cell transplant)___________________________________________________________________________Source: NCRP Report 98 "Guidance on Radiation Received in Space Activities", NCRP, Bethesda (MD) (1989)5Human Dose ResponseThe LD50/30 or LD50/60 is defined as the dose necessary to cause death in 50% of an irradiated population in 30 and 60 days, respectively.For an exposed worker population, the dose for 5% mortality may differ from the dose for 95%mortality by only 2-3 Gy. Therefore, an increase in dose by only a factor of 2 may represent the difference between total survival of an irradiated population and essentially total mortality.LD50/60 may increase above 5.4 Gy with advanced therapy modalities.
Factors decreasing LD50/60Coexisting trauma combined injury
Chronic nutritional deficit
Coexisting infection
Contribution of high LET radiation6As with many other clinical phenomena, a patient's response to radiation may not conform to the anticipated. Therefore, the relationship between a particular radiation dose level and an expected effect should be considered approximate at best. Individual response to and ability to recover from radiation injury is related to: total dose and quality of radiation dose rate portion of the body exposed comparative intrinsic genetic cellular radiosensitivity uniformity of exposure age and health of the victim presence of coexisting injuries or illnesses
Acute radiation syndrome (ARS)Acute radiation syndrome threat Discharged medical irradiatorsIndustrial radiography unitsCommercial irradiatorsTerrorist detonationNuclear fuel processingNuclear reactors Combination of clinical syndromes occuring in stages hours to weeks after exposure as injury to various tissues and organs is expressed
7A radiological accident is defined as an unforeseen event involving overexposure or contamination of persons/the environment by radioactive material. Acute radiation syndrome (ARS) is defined as a combination of clinical syndromes occuring in stages during a period of hours to weeks after exposure, as injury to various tissue and organs is expressed.The latest major nuclear and radiological accidents have contributed to the diagnosis, monitoring and treatment of radiation injuries:Explosion of the vapour at the Chernobyl Nuclear Power Plant in April 1986 resulted in the hospitalization of 237 patients identified as overexposed persons. 134 of them developed ARS. Of these 134 exposed persons, 28 eventually died of ARS associated injury with extensive radiation burns. In September 1987, a shielded radioactive caesium-137 source (50.9 TBq) was removed from the protective housing of an abandoned teletherapy machine in Goinia, Brazil. Subsequently, the source was ruptured. As a result, many people incurred large doses of radiation by both external and internal contamination. Four of the casualties ultimately died, and 28 people developed local radiation injuries. In 1989, a radiological accident occurred at an industrial sterilization facility in San Salvador, El Salvador. The accident occurred when the cobalt-60 source became stuck in the open position. Three workers were exposed to high radiation doses and developed ARS. The immediate acute effects were limited by specialized treatment. Nonetheless, two of the men were so seriously injured that their legs had to be partly or completely amputated. The most highly exposed worker died 6.5 months later, his death attributed to residual lung damage and other injuries .
Clinical forms of acute radiation syndrome Haematopoietic syndrome (HPS)Gastrointestinal syndrome (GIS) Neurovascular syndrome (NVS)8Acute radiation syndrome (ARS) is a complex of acute injury manifestations that occur after a sufficiently large portion of a person's body is exposed to a high dose of ionizing radiation. Such irradiation initially injures all organs to some extent, but the timing and extent of the injury manifestations depend upon the type, rate, and dose of radiation received. The percentage of the body that is injured, the dose homogeneity, and the intrinsic radiosensitivity of the exposed individual also influence manifestations. Different ranges of whole body doses produce different manifestations of injury.The three main ranges that produce the most characteristic manifestations are referred to as the haematological, gastrointestinal, and neurovascular syndromes. These syndromes are, as a rule, produced only with total-body or nearly total-body irradiation by photon or mixed photon/neutron radiation. High-dose injuries to smaller percentages of the body produce local injury effects but may not cause ARS.
Critical organs or tissues after acute whole body radiation exposureDose, GyCritical organ or tissueMortality, per cent Time of death, days1 2 Bone marrow 2 4 540 60 4 6 5030 40 6 10 9510 20 10 30 Gastrointestinal tract1007 14 > 30 Neurovascular system1001 59Three main syndromes are distinguished following an acute whole body exposure. These are listed in the above table and are usually referred to as BM, GIT and NV syndromes. There are also symptoms of BM syndrome in acute whole body exposure above 10 Gy; however, in this dose range the symptoms of the GIT syndrome dominate the clinical picture.The primary cause of death in BM syndrome is infection (following loss of cellular immunity), in GIT syndrome - the severe loss of fluids and intestinal bleeding, in CV syndrome - oedema of brain.Phases of acute radiation syndrome Initial or prodromal phase Latent phase Manifest illness phase Recovery phase10ARS has been broken down into three subsyndromes, which are dose and time profile dependent. The three syndromes described follow a similar clinical pattern that can be divided into three phases: an initial or prodromal phase occurring during the first few hours after exposure, a latent phase, which becomes shorter with increasing dose; and the manifest phase of clinical illness. The time of onset and degree of the transient incapacitation of the initial phase, the duration of the latent period, as well as the time of onset and severity of the clinical phase and ultimate outcome are all, to a variable extent, dependent upon total dose and individual radiation sensitivity.
Haematopoietic syndrome
Normal bone marrow cells
Bone marrow damaged by radiation injury 11Patients who have received doses of radiation in the potentially low to mid-lethal range (2-6 Gy) will have depression of bone-marrow function with cessation of blood-cell production leading to pancytopenia.Bone marrow contains three cell renewal systems whose time cycles, cellular distribution patterns and post-irradiation responses are quite different: the erythropoietic (red cell), the myelopoietic (white cell), and the thrombopoietic (platelet). A pluripotential stem cell gives rise to these three cell lines in the bone marrow. Each cell renewal system consists of a stem cell compartment for the production of erythrocytes, leukocytes (lymphocytes, granulocytes, monocytes, etc.), or platelets, a dividing and differentiating compartment, a maturing (non-dividing) compartment, and a compartment containing mature functional cells.The stem cell lines of the bone marrow are among the most radiosensitive tissue of the body. This is because of their high mitotic rate and their high nuclear-to-cytoplasmic ratio.
Even at ionizing radiation doses of 2.5 Gy and higher, a small percentage of the surviving stem cell population is capable of continuously expanding progeny. The surviving stem cells must perform the "double duty" of replenishing their own populations while reproducing committed stem cells and differentiated precursor blood line cells.While this replenishment occurs, the counts of the shorter lived cell populations drop to a nadir and then recover, assuming the patient is surviving. The severity and duration of the nadir depend upon the severity of the dose received, the patient's inherent ability to repair bone marrow damage, and the effect of therapy received - whether it enhances or inhibits the repair process.Phases of haematopoietic syndrome (HPS)Prodromal phase symptoms nausea and vomiting lasts only a few hours, with time of onset from later than one hour to about 24 hours after exposure
Latent phase lasts up to a month. Relatively asymptomatic except for some fatigue and weakness
Manifest illness phase characterizes by neutropenic fevers, systemic and localized infections, sepsis, and haemorrhage12Patients injured with doses in the haematopoietic range will experience prodromal symptoms of nausea and vomiting which, compared with those for the other syndromes, are less severe and easier to control. They last only a few hours, with time of onset from later than an hour to about 24 hours after exposure. There is usually a lack of central nervous system syndrome signs, very little change in blood pressure, and only mild watery diarrhoea. Fatigue, malaise, anorexia, and drowsiness may be observed but are not consistently correlated to dose received as are the onset and severity of nausea and vomiting.The prodromal phase is followed by the latent phase that lasts up to a month and is relatively asymptomatic except for some tiredness and weakness.The latent phase is followed by the manifest illness phase, characterized by neutropenic fevers, systemic and localized infections, sepsis, and haemorrhage.
Threshold doses for symptoms of the prodromal phase ARSanorexia, nausea and vomiting (1 Gy) diarrhea (4 6 Gy),malaise, weakness and fatigue (1 2 Gy),headache (4 6 Gy),dizziness (6 8 Gy), fever (8 10 Gy) 13Threshold doses for symptoms of the prodromal phase ARS: anorexia, nausea and vomiting (0,5 1 Gy) diarrhea (4 6 Gy),malaise, weakness and fatigue (1 2 Gy),headache (4 6 Gy),dizziness (6 8 Gy), fever (8 10 Gy)Central mechanism: activation of chemoreceptor trigger zone of vomiting centre by biological activity substances from irradiated tissues biogenic amines, regulatory peptides and other bioregulators
Peripheral or reflex mechanism: irritation peripheral emetic receptors from peripheral zones located, mainly, in digestive tractPathogenesis of emetic syndrome14Pathogenesis of emetic syndrome includes central and peripheral mechanisms.Central mechanism: activation of chemoreceptor trigger zone of vomiting centre by biological activity substances from irradiated tissues biogenic amines, regulatory peptides and other bioregulators.Peripheral or reflex mechanism: irritation peripheral emetic receptors from peripheral zones located, mainly, in digestive tract
Characteristic of symptoms of prodromal phase of ARS depending on doses1 2 Gy2 4 Gy 4 6 Gy> 6 GyInitiation2 hours1 2 hours0,5 1 hours5 20 minutesVomitingunitaryrepeatedfrequentlyrepeatedunrest-rainedDiarrhea+ + + +Duration
1 3 hoursto 1 daysto 2 daysmore than 2 3 days15Characteristic of symptoms of prodromal phase of ARS depending on doses (see table).Haematological response to 1 Gy whole body radiation exposure
16Cytogenetic injury to bone marrow cells and nucleated blood cells can occur at ionizing radiation doses as low as 0.25 Gy, but clinical depression of cell counts is usually not noted until a dose of 0.5 Gy. Platelets After exposure to ionizing radiation, platelet counts generally drop in concert with neutrophil counts, but an abortive count rise is not usually observed. Platelet counts drop to zero or near zero with doses that exceed 5 Gy.With the changes in blood counts, the patient suffers damage to the immune and haematostatic systems. In the week preceding and during the neutrophil and platelet count nadir, the function of remaining cells is altered. Not only are few neutrophils and platelets left, but the remaining cells may not function since they are at the end of their life span due to either senescence or radiation damage.If, during the 15-day recovery period from the nadir of neutropenia, the patient survives neutropenic fever, complications of sepsis, and uncontrollable haemorrhage, recovery following the nadir period can be expected. Thus, the therapeutic goal in the management of such a patient is to lessen the severity of thrombocytopenia and neutropenia while minimizing and treating infectious damages.Haematological response to 3 Gy whole body radiation exposure
17Red blood cells . After exposure to ionizing radiation, there is usually no depression or only a very mild depression of red blood cells unless there is concomitant haemorrhage.Granulocytes Doses greater than 2 Gy cause an initial paradoxical rise in counts, a rise that lasts only hours or days and is followed by a precipitous drop. This is caused by prompt demargination of white cells into the circulation. Any blood cell count (BCC) taken during this paradoxical rise may be misinterpreted as evidence of infection.Doses of 2 to 5 Gy cause a second abortive rise, which interrupts the precipitous drop in counts for several days and possibly as long as a week. This second abortive rise is caused by the products of final differentiation and entry into circulation of marrow PMN (polymorphic nucleated cell) precursor cells, which do not need to undergo further mitotic divisions. The extent and duration of this second rise varies; but classically, it lasts for approximately a week with a rise from about 50% to about 75% of normal. Then the neutrophil count continues dropping to a nadir of near zero to 20% of normal at around 25-35 days after exposure.
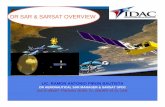
Lymphocytes changes5-6 GyTime after exposure, daysLymphocytes, per cent of normal18The first detectable sign of whole body exposure is a decrease in blood lymphocytes. This decrease appears a few hours or days after irradiation and is related to the dose received, but also to the volume of irradiated bone marrow. This is due to the direct effect of ionizing radiation on lymphocytes, but also to the radiation induced death of proliferating haematopoietic cells that are not able to ensure the renewal of blood cells.
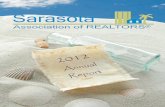
Leukocytes changesNormal5-6 GyNeutrophils, per cent of normalTime after exposure, days19The function of the myelopoietic marrow cell renewal system is mainly to produce mature granulocytes, i.e. neutrophils, eosinophils, and basophils, for the circulating blood. Of these, the neutrophils, because of their role in combating infection, are the most important cell type in this cell line. The stem cells and those developing stages within the dividing and differentiating compartment are the most radiosensitive. These include the myeloblast, progranulocyte and myelocyte stages. As with the erythropoietic system, cell stages within the maturing (non-dividing) compartment and the mature functional compartment, i.e. granulocytes, are not significantly affected by radiation doses within the mid-lethal range. 3-7 days are normally required for the mature circulating neutrophil granulocyte to form from its stem cell precursor stage in the bone marrow. An ionizing radiation dose of 2 Gy or less usually causes a very gradual depression of counts to 50% or less with a nadir at more than 40 days. Doses greater than 2 Gy cause an initial paradoxical rise in counts, a rise that lasts only hours or days and is followed by a precipitous drop. This is caused by prompt demargination of white cells into the circulation. Any CBC taken during this paradoxical rise may be misinterpreted as evidence of infection. Doses greater than 5 Gy usually cause the precipitous drop to continue relentlessly to a nadir of zero or near zero in 3-4 weeks. Doses of 2-5 Gy cause a second abortive rise, which interrupts the precipitous drop in counts for several days and possibly as long as a week. This second abortive rise is caused by the products of final differentiation and entry into circulation of marrow PMN (polymorphic nucleated cell) precursor cells, which do not need to undergo further mitotic divisions. The extent and duration of this second rise varies; but classically, it lasts for approximately a week with a rise from about 50% to about 75% of normal. Then the neutrophil count continues dropping to a nadir of near zero to 20% of normal at around 25-35 days after exposure. Recovery of myelopoiesis lags slightly behind erythropoiesis and is accompanied by rapid increases in numbers of differentiating and dividing forms in the marrow. Prompt recovery is occasionally manifest and is indicated by increased numbers of band cells in the peripheral blood.
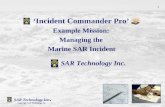
Thrombocytes changesNormal5-6 GyPlatelets, per cent of normalTime after exposure, days20The thrombopoietic cell renewal system is responsible for the production of platelets (thrombocytes) for the peripheral circulating blood. Platelets along with granulocytes constitute two of the most important cell types in the circulation, the levels of which during the critical phase after mid-lethal doses markedly influence the survival or non-survival of irradiated persons. Platelets are produced by megakaryocytes in the bone marrow. Both platelets and mature megakaryocytes are relatively radioresistant; however, the stem cells and immature stages are very radiosensitive. During their developmental progression through the bone marrow, megakaryocytic precursor cells undergo nuclear division without cell division. The transit time through the megakaryocyte proliferating compartment in humans ranges from 4 to 10 days. Platelets have a lifespan of 8-9 days. Although platelet production by megakaryocytes may be reduced by a high dose of ionizing radiation, the primary effect is on stem cells and immature megakaryocyte stages in the bone marrow. As with the erythropoietic and myelopoietic systems, the time of beginning depression of circulating platelets is influenced by the normal turnover kinetics of cells within the maturing and functional compartments. Early platelet depression, reaching thrombocytopenic levels by 3-4 weeks after mid-lethal range doses, occurs from killing of stem cells and immature megakaryocyte stages and from maturation depletion of maturing and functional megakaryocytes. Regeneration of thrombocytopoiesis after sublethal irradiation normally lags behind both erythropoiesis and myelopoiesis. Supranormal platelet numbers which overshoot the preirradiation level have occurred during the intense regenerative phase in human nuclear accident victims. The mechanism of the prompt rapid recovery of platelet numbers after acute sublethal irradiation may be explained by the response of the surviving and regenerating stem cell pool to a human feedback stimulus from the acute thrombocytopenic condition. and marked increases in size of megakaryocytes contribute to the intense platelet production and eventual restoration of steady state levels. Blood coagulation defects with concomitant haemorrhage constitute important clinical sequalae during the thrombocytopenic phase of bone marrow and gastrointestinal syndromes.
Erythrocytes changes1 Gy3 Gy21The function of this cell renewal system is to produce mature erythrocytes for the circulation. The transit time from the stem cell stage in the bone marrow to the mature red cell ranges from 4 to 7 days, after which the life span of the red cell is approximately 120 days. The immature forms, i.e. erythroblast and proerythroblast, undergo mitosis as they progress through the dividing and differentiating compartment. Because of their rapid proliferating characteristics, they are markedly sensitive to cell killing by ionizing radiation. Cell stages within the maturing (non-dividing) and functional compartments, i.e. normoblast, reticulocyte, and red cell, are not significantly affected by mid-lethal to lethal range doses. The death of stem cells and of those within the next compartment is responsible for the depression of erythropoietic marrow and, if sufficiently severe, is responsible together with haemorrhage for subsequent radiation induced anaemia. Because of the relatively slow turnover rate, e.g. approximately 1% loss of red cell mass per day, in comparison with leukocytes and platelets, evidence of anaemia is manifest subsequent to the depression of the other cell lines, provided that significant haemorrhage has not occurred. The erythropoietic system has a marked propensity for regeneration following irradiation from which survival is possible. After sublethal exposures, marrow erythropoiesis normally recovers slightly earlier than granulopoiesis and thrombopoiesis and occasionally overshoots the base-line level before levels at or near normal are reached. Reticulocytosis, occasionally evident in peripheral blood smears during the early intense regenerative phase occurring after maximum depression, often closely follows the temporal pattern of marrow erythropoietic recovery. Although anaemia may be evident in the later stages of the bone marrow syndrome, it should not be considered a survival limiting sequalae.
Basic syndromes of manifest illness phasepancytopeniahaemorrhagesystemic and localized infectionssepsis, feversvomiting, diarrhea toxemia alopeciakaheksia etc.22Basic syndromes of manifest illness phase is pancytopenia, haemorrhage, systemic and localized infections, sepsis, fevers, vomiting, diarrhea, toxemia, alopecia, kaheksia etc.
Gastrointestinal syndrome
Irradiated gastrointestinal mucosa
Develops after an irradiation in doses 10 30 Gy23Generally, exposure to a dose range of 10-30 Gy is fatal since that dose range causes reproductive death of the mucosal crypt stem cell.Loss of these cells eliminates the bowel's ability to replenish the short lived mucosal cells that normally slough off during routine GI function. Since the rate of cell turnover is highest in the small intestine, radiation injury is usually most severe in that part of the tract. Additionally, there is, to a degree, disruption of neural control of the gut, abnormal release of intestinal neurohormonal peptides, oedema of the submucosa, and engorgement and stasis of the submucosal blood vessels.Pathogenesis of the gastrointestinal syndromeDepletion of the epithelial cells lining lumen of gastrointestinal tract
Intestinal bacteria gain free access to body
Haemorrhage through denuded areas
Loss of absorptive capacity
24Denuding of sections of bowel, in turn, causes a host of pathophysiological sequelae. They include invasion of lumenal bacteria into the circulation, loss of fluid and electrolytes, loss of absorptive capability, significant gastrointestinal haemorrhage and loss of blood, and dysfunctional bowel motility, resulting in severe bloody diarrhoea, anaemia, ileus, severe electrolyte disturbances, and malnutrition.
Phases of gastrointestinal syndromeProdromal period: severe nausea and vomiting, watery diarrhoea and cramps. Occurs within hours after exposure
Latent (subacute) phase: asymptomatic for hours to days, severe tiredness, weakness
Manifest illness: return of severe diarrhoea, vomiting with fever; progression to bloody diarrhoea, shock and death without aggressive medical intervention25Prodromal period: Within 30 minutes to 2 hours of exposure, patients receiving radiation doses of 8-30 Gy may experience severe prodromal symptoms of anorexia, nausea, vomiting, and occasionally watery diarrhoea with abdominal cramps, which increase in intensity for 4-8 hours and may be difficult to control with antiemetic medications. These symptoms are usually accompanied by listlessness, drowsiness, and fatigue. Occasionally, prodromal symptoms include parotid gland pain, metallic taste sensation, mild hypotension, and tachycardia. The prodromal symptoms continue but diminish over the first 48 hours after exposure.Latent (subacute) phase: Patient is asymptomatic for hours to days but markedly tired and weak.Then ensues the course of manifest illness: return of severe diarrhoea and then vomiting and diarrhoea with fever, progressing to bloody diarrhoea, shock, and death.
Systemic effects of gastrointestinal syndrome Malabsorption malnutrition
Fluid and electrolyte shifts dehydration, acute renal failure, cardiovascular collapse Gastrointestinal bleeding anaemia
Gastrointestinal infectious sepsis
Paralytic ileus vomiting, abdominal distention26The simultaneous invasion of a host of potentially pathological bacteria into the bloodstream quickly overwhelms the victim's ability to fight such infections. Malabsorption leads to malnutrition; paralytic ileus causes vomiting and abdominal distension; fluid and electrolyte shifts result in dehydration, acute renal failure, and cardiovascular collapse. Gastrointestinal bleeding leads to anaemia. Sepsis, septic shock, and eventually death ensue.Neurovascular syndromeDevelops after an irradiation in doses 30 Gy and above Prodromal phase: Burning sensation within minutes of exposure; nausea and vomiting within first hour; loss of balance, confusion with prostration; hypotension, hyperpyrexia
Latent phase:Apparent improvement lasting several hours, may be lucid and in no pain but weak
Manifest illness phase:Rapid onset, watery diarrhoea, respiratory distress, gross CNS signs, wide pulse pressure, hypotension27Acute radiation doses of 30 Gy and above cause death within 72 hours and usually between 24 and 48 hours, well before the damage to the gastrointestinal or bone marrow systems becomes clinically apparent. Doses in this range cause significant direct effects as well as free radical overload of the cells and basement membranes of the microcirculation system. This leads to, among other damage, massive loss of serum and electrolytes through leakage into the extravascular space, circulatory collapse, oedema, increased intracranial pressure, and cerebral anoxia.In less than an hour and possibly within minutes of exposure, patients receiving these doses begin experiencing prodromal symptoms: a burning sensation within minutes and severe nausea and usually projectile vomiting within an hour. The symptoms, which are severe and may last more than 24 hours, also include diarrhoea that is occasionally bloody, cutaneous oedema and erythema, hypotension, hyperpyrexia, disorientation, prostration, loss of co-ordination, and possibly seizures.Following the prodromal phase, there may be a brief latent phase of apparent clinical improvement; but this will last only for hours to days. Finally, the victim will succumb to a complex of gross CNS dysfunction and total cardiovascular collapse, leading to a relatively prompt and inevitable death.
Radiation-induced early transient incapacitation For high radiation doses (in excess of 30 Gy), early transient incapacitation occurs on average within 5 to 10 minutes after acute whole-body irradiation. Lowering the dose the median time of ETI occurrence increases up to 12 to 15 minutes. Exposure to doses of ionizing radiation (of the order of 50 Gy) results in an immediate precipitous decline in cerebral blood flow (CBF) which is followed by a partial recovery at 2030 minutes, and subsequent slower secondary decrease in CBF thereafter, accompanied by parallel changes in systemic blood pressure.28For high radiation doses (in excess of 10 Gy), early transient incapacitation (ETI) occurs on average within 5 to 10 minutes after acute whole-body irradiation. Lowering the dose the median time of ETI occurrence increases up to 12 to 15 minutes. Exposure to doses of ionizing radiation (of the order of 25 Gy) results in an immediate precipitous decline in cerebral blood flow (CBF) which is followed by a partial recovery at 2030 minutes, and subsequent slower secondary decrease in CBF thereafter, accompanied by parallel changes in systemic blood pressure. These data indicate that radiation adversely affects the ability of the brain to regulate its blood supply.
Possible mechanisms of radiation-induced early transient incapacitation Several generalizations have emerged from non-human experimental studies:
early transient incapacitation is qualitatively very similar for many behavioral tasks
the frequency of incapacitation within a population increases as a function of radiation dose
incapacitation can be elicited by both trunkonly and headonly irradiation
neutrons are less effective in producing early transient incapacitation than are gamma rays
the activity of certain brain enzymes involved in neurotransmitter metabolism is also considerably affected during early transient incapacitation29Performance decrement has been evaluated for numerous behavioral takes after whole-body and partial-body irradiation for various radiation qualities and dose rates. Several generalizations have emerged from non-human experimental studies.(1) Early transient incapacitation is qualitatively very similar for many behavioral tasks. (2) The frequency of incapacitation within a population increases as a function of radiation dose. (3) Incapacitation can be elicited by both trunkonly and headonly irradiation.(4) Neutrons are less effective in producing early transient incapacitation than are gamma rays. The relative biological effectiveness for incapacitation of neutron to gamma has been estimated between 0.23 and 0.62. (5) The activity of certain brain enzymes involved in neurotransmitter metabolism is also considerably affected during ETI.
The frequency of incapacitation produced by a given radiation dose is proportional to the demands or stress of the task being performed. Current combat casualty criteria are based on the incapacitating dose levels for both physically demanding tasks and undemanding tasks. They do not include combat ineffectiveness due to partially degraded performance that may result from slower reaction to the task, task stress, or prodromal effects of acute radiation sickness. Prognosis of gastrointestinal and neurovascular syndromes SymptomsRadiationdose (Gy)Life threateninginjuriesDeath of patients16202530Loss of consciousnessNeurovascular damage 5-12 days 2-5 days30Radiation doses in this range are uniformly fatal regardless of therapy attempted; therefore, aggressive medical support with vasopressors, fluids, steroids, and the like will bring only temporary improvement and may only serve to prolong suffering. Thus, therapy should be palliative in nature, and the clinician caring for such a patient is encouraged to be generous with any palliative measure such as opiates or tranquillizers.
Acute radiation syndrome at a non-uniform irradiationNon-uniform it is considered an irradiation at which difference of the absorbed dozes on a body exceeds 10 - 15 %
At small differences of dozes the clinical picture of non-uniform defeat differs from the classical form of sharp radiation sickness a little
Features of a clinical picture are shown at factor of non-uniformity more than 3 and the maximal dose of an irradiation from above 10 Gy31Acute radiation syndrome at a non-uniform irradiation:- non-uniform it is considered an irradiation at which difference of the absorbed dozes on a body exceeds 10 - 15 %;- at small differences of dozes the clinical picture of non-uniform defeat differs from the classical form of sharp radiation sickness a little;- features of a clinical picture are shown at factor of non-uniformity more than 3 and the maximal dose of an irradiation from above 10 Gy.
Features of radiation injuries at a non-uniform irradiationDecrease in efficiency of biological action of radiation on critical systems of organism
Infringement characteristic for "classical" form ARS of periodicity and time dependence of its basic symptoms
Prevalence in a clinical picture of disease of the symptoms reflecting infringement of functions of bodies and fabrics, undergone to an irradiation 32Features of radiation injuries at a non-uniform irradiation:- decrease in efficiency of biological action of radiation on critical systems of organism;- infringement characteristic for "classical" form ARS of periodicity and time dependence of its basic symptoms; - prevalence in a clinical picture of disease of the symptoms reflecting infringement of functions of bodies and fabrics, undergone to an irradiation.Features of radiation injuries at a non-uniform irradiation(continued)Opportunity of development at same struck several radiating syndromes Reduction the role of haematological syndrome with growth of non-uniform irradiation Increase with growth of non-uniform irradiation the role of oropharingeal and intestinal syndromes, a local radiation injury of skin Updating of clinical current of haematological and gastrointestinal syndromes 33- opportunity of development at same struck several radiating syndromes; - reduction the role of haematological syndrome with growth of non-uniform irradiation; - increase with growth of non-uniform irradiation the role of oropharingeal and intestinal syndromes, a local radiation injury of skin; - updating of clinical current of haematological and gastrointestinal syndromes.
Summary of lectureAcute radiation syndrome is a complex of acute injury manifestations occurring after extensive exposure to high dose of ionizing radiation Phases of acute radiation syndrome: prodromal, latent, manifest illness, recovery Different ranges of whole body doses produce different manifestations of injury Dose ranges producing the most characteristic manifestations: haematological, gastrointestinal, cardiovascular /central nervous system syndromes 34Acute radiation syndrome is a complex of acute injury manifestations occurring after extensive exposure to high dose of ionizing radiation Phases of acute radiation syndrome: prodromal, latent, manifest illness, recovery Different ranges of whole body doses produce different manifestations of injury Dose ranges producing the most characteristic manifestations: haematological, gastrointestinal, cardiovascular /central nervous system syndromes
Summary of lecture(continued)Radiation doses in cardiovascular/central nervous system syndrome range uniformly fatal regardless of therapy Doses in gastrointestinal syndrome range, which also produce life-threatening pulmonary effects, usually fatal Doses in the haematopoietic syndrome range are survivable. Therapeutic goal: lessen the severity of thrombocytopenia and neutropenia while minimizing and treating infection 35Radiation doses in cardiovascular/central nervous system syndrome range uniformly fatal regardless of therapy Doses in gastrointestinal syndrome range, which also produce life-threatening pulmonary effects, usually fatal Doses in the haematopoietic syndrome range are survivable. Therapeutic goal: lessen the severity of thrombocytopenia and neutropenia while minimizing and treating infection
Lecture is endedTHANKS FOR ATTENTIONIn lecture materials of the International Atomic Energy Agency (IAEA), kindly given by doctor Elena Buglova, were used