Sample Case Presentation Agatha Stanek July 10, 2010.
18
Sample Case Presentation Agatha Stanek July 10, 2010
-
Upload
penelope-taylor -
Category
Documents
-
view
221 -
download
2
Transcript of Sample Case Presentation Agatha Stanek July 10, 2010.
Sample Case Presentation
Agatha Stanek
July 10, 2010

•33 year- old Caucasian female presents to clinic with her younger sister complaining of vomiting, a loss of appetite, and chronic diarrhea over the last 6 days.
•Patient reports dizziness, hair loss, and abdominal pain.
•Decreased cold tolerance
•Rapid weight loss
•Patient confides in physician that she feels lost and like life is not worth living anymore; she has no strength to live.
Case presentationCase presentation
PMHPMH
•Appendicitis treated surgically 10 years ago
•Pernicious anemia x 5 years
• Formally diagnosed with anorexia nervosa at age 19 and treated successfully
•No family history of cancer
•Father died of cardiac arrest 7 years ago•Mother has Crohn disease x 22 years. Crohn disease also runs in father’s side of the family- grandfather had disease.
•Sister of patient has Graves disease
Occupational HxOccupational Hx•Patient recently moved from California to Ottawa where she is now staying with younger sister and her family.
•Upper class citizen who has a successful advertising
company- very stressful
FxFx
•Denies tobacco or alcohol use
•No children•Sister speaks to you outside and reveals that the patient is back in Ottawa after a messy divorce from her husband. She worries that the patient is depressed or she is becoming anorexic again as she has stopped eating.
MedsMeds
Cyanocobalamin, 200 µg IM; monthly. Increased dosage by physician back in the USA.
No allergies
SxSx
• no recent changes in vision, no fevers, chills, dyspnea, cough or night sweats
• changes in menstrual cycle
•Reports aches and pains
•Admits to having one fainting spell 2 weeks ago
•(+) for weight loss of 15 pounds in the last month•Patient is quite tanned, although she reports significant exposure to the sun
ROSROS
VS:BP: 95/75, P 83/min sitting T: 37 °C
BP: 80/60, P 110/min, standing HT: 5 ft- 8 ½ in
RR: 14/min WT: 121 lbs
SKIN:Intact, warm, quite dry
HEENT:•PERRLA•EOMI•Normal funduscopic exam•Dry mucous membrane
PE Results PE Results

NECKThyroid normal, no massesShotty lymphadenopathy??
LUNGSClear; normal vesicular and bronchial sounds
CARDIACRRR
ABDSoft but not tender(-) hepatosplenomegaly
GUNormal pelvic exam
MS/ EXTNormal range of motionMuscle strength throughout
NEUROAlert and orientedNormal gaitCNS II- XII intact

•Anorexia nervosa/ Severe nutritional deficiencies•Depression•Colon disease…•Infection•Pituitary failure/ hypothalamic tumour
Differential DiagnosisDifferential Diagnosis

Laboratory Blood Test Results

UA: •Clear and yellow•SG 1.1016•pH 6.45•(-) blood
Antibody Testing:• (+) 21- hydroxylase•(-) 17-hydroxylase•(-) C-P450
Peripheral Blood Smear:Normal, normocytic erythrocytes
Additional TestsAdditional Tests

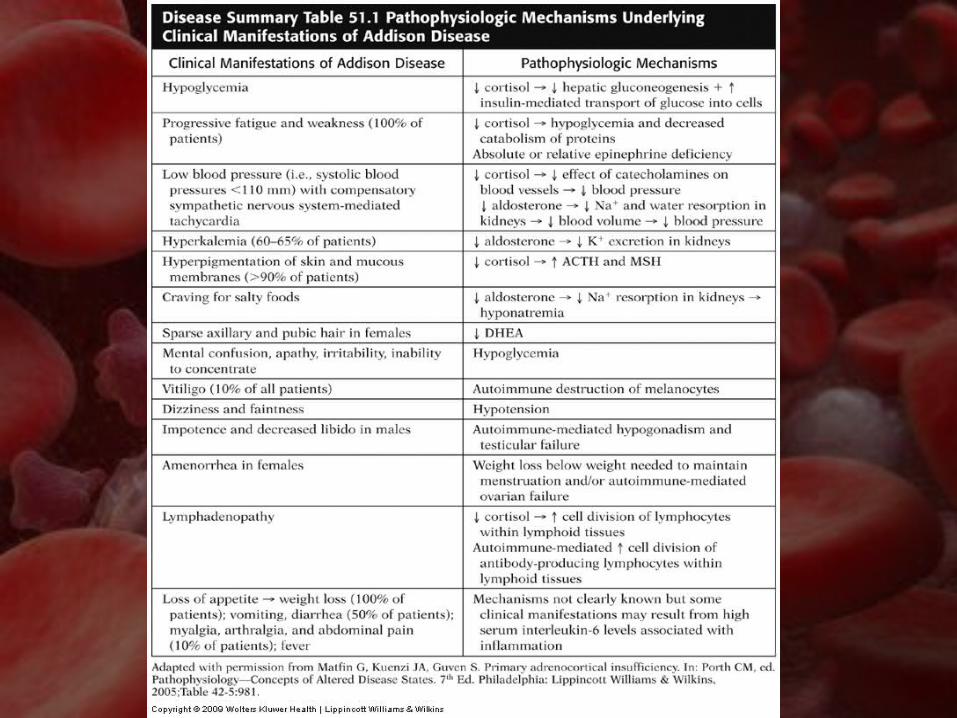
Why are these tests results significant???
Autoimmune Addison disease (AD)-Why autoimmune?
-Why is shotty lymphadenopathy consistent with this diagnosis in this particular patient?
-Why was the patient anemic?
-What other imaging test can confirm this test result? -CT scan: which revealed moderate bilateral atrophy of the adrenal glands.-MRI
Diagnosis Diagnosis

No cure for AD•Glucocorticoid and possibly mineralocorticoid replacement therapy
•Hydrocortisone- daily oral dose of 15-25 mg in 2 doses; 2/3 in the am and 1/3 in the pm.•Proper dose results in normal differential WBC count.
• Fludrocortisone- daily 0.05-0.3 mg orally
•No restrictions on physical activity required
•Diet: include at least 150 meq of Na daily; more if excessive sweating/ diarrhea occur
Treatment Treatment
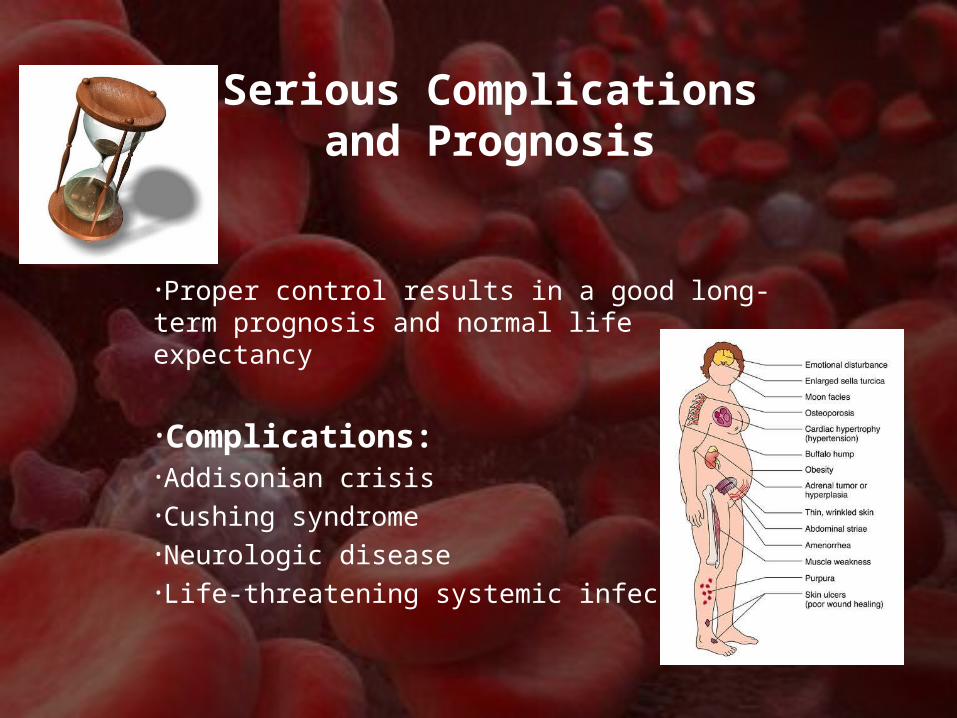
•Proper control results in a good long-term prognosis and normal life expectancy
•Complications:•Addisonian crisis•Cushing syndrome•Neurologic disease•Life-threatening systemic infection?
Serious Complications and Prognosis

Suggest colonoscopy to rule out…
Recommend outpatient therapy- counselling. Referral to nearby psychologist.
Further RecommendationsFurther Recommendations