Salivary Glands Anatomy & Inflammation & Tumors
59
Salivary glands By : Mahmoud Abdullah Mashaal Mahmoud Abdelnasser Abotaleb Mahmoud Omar Elkhattab Mahmoud Fathy Saleh Mahmoud Mo'ness Elbialy Supervisor: Prof. Dr. Mohamed Hegazy
-
Upload
- -
Category
Health & Medicine
-
view
276 -
download
2
Transcript of Salivary Glands Anatomy & Inflammation & Tumors

Salivary glandsBy :
Mahmoud Abdullah Mashaal
Mahmoud Abdelnasser Abotaleb
Mahmoud Omar Elkhattab
Mahmoud Fathy Saleh
Mahmoud Mo'ness Elbialy
Supervisor:
Prof. Dr. Mohamed Hegazy

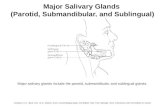
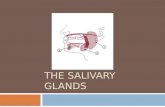
Salivary glands Anatomy

•• A ) parotid gland :
•• -It is the largest gland of the body
•
•- shape :Inverted three sided pyramidApex & base & 3 surfaces & 3 bordersIt has 5 processes : 3 superficial & 2 deep

• - capsule :• - site :• Lies in front & below the parotid compartment• 80% of the gland overlies the masseter muscle• Lies within the investing layer of deep fascia of the
neck called parotid fascia• 1) superficial layer : extend from masseter to
sternocleidomastoid muscle to zygoma• 2) deep layer : from the fascia of posterior belly of
digastric muscle , forming stylomandinular membrane separating the parotid and submandibular glands .
•

Relations

Lateral :1)skin
Anteromedial : (3M)
1)ramus of the mandible
2)masseter
3)medial pterygoid muscle
2) superficial fascia containing ( platysma , branches of great auricular nerve , superficial parotid lNs)
3)parotid fascia
4) deep lN embeded in the gland

Posteromedial:1)mastoid process and 2 muscles atrached ( sternocleidomastoid , posterior belly of digastric )2) styloid process & structures attached to it : 3 muscles ( stylohyoid ,styloglossus , stylopharyngeus ) , 2 ligaments (stylohyoid , stylomandibular)3)carotid sheeth ( ICA, IJV , Lower 4 cranial nerves 9&10&11&12)
•

-borders & extent :• Structures passing through the anterior border :• 1)zygomatic branch of facial nerve• 2)transverse facial vessels• 3)buccal branch if facial nerve• 4)parotid duct• 5)mandibular branch of facial nerve
•• -superior :• From the EAM & TMJ• Structures passing through it :• 1)temporal branch of facial nerve• 2) auriculotemporal nerve• 3)superficial temporal vessels
•

-inferior :
• Posterior belly of digastric & stylohyoid muscle• Structures passing through it:• 1)cervical branch if facial nerve• 2) two devisions of retrandibular vein
•• - structures within the parotid gland :• 1)External carotid artery & its 2 terminal branches :
(maxilary and superficial temporal arteries ) ... Deep• 2)retromandibular vein ... Intermediate• 3) facial nerve and its five terminal branches
( temporal , zygomatic, buccal , marginal mandibular , cervical ) ... Superficial
•
•

Parotid duct : (Stensen's duct )
• - arises from the anterior border of the gland , parallel to the zygomatic arch• -runs superficial to the masseter , then turn 90
degrees to pierce the buccinator muscle at the level of the upper second mollar tooth where it opens into the oral cavity .• - buccal branch of facial nerve runs with the parotid
duct

• Accessory parotid gland :
• Typically found overlying the masseter• Accessory duct lies cranial to the stensen's duct• Have their own blood supply from transverse facial vessels
•
•• Nerve supply• Parasympathetic: glossopharyngeal (secretomotor ) .. otic
ganglion .. auriculotemporal nerve ... Parotid gland• Sympathetic : plexus around the ECA• Sensory : auriculotemporal nerve to the gland , great
auricular nerve from the parotid fascia
•• Arterial supply : ECA inside the gland• Venous drainage : Retromandibular vein• Lymphatic Drainage :• Superficial and deep parotid lymph nodes to the upper deep
cervical lymph nodes
•
•


2 ) Anatomy of submandibuar salivary gland
Site : in the anterior part of the digastric triangle
Extent :
Size : 4 cm long
Anterior : mental foramen
Posterior : angle of the mandible
Superior : mylohyoid line
Inferior : hyoid bone
•

• Parts :
• Facial covering :
• Superficial part is enclosed () 2 layers of deep cervical fascia• Superficial layer is attached to the base of the
mandible ..• Deep layer attached to the mylohyoid line
• A) superficial part : superficial to mylohyoid ms
• B) deep part : deep to mylohyoid ms
• The two parts are connected to each other around the posterior border of mylohyoid ms .
•


A) superficial part :
1) superficial surface (inferolateral surface):
3) medial surface :
* 2 muscles ( mylohyoid & hyoglossus )
* 2 nerves (lingual & hypoglossal )
* Submandibular ganglion
• *Skin• *Superficial fascia (containing platysma , cervical
branch of facial nerve + anterior facial vein + submandibular vein )• *Deep fascia
•• 2) lateral surface:• * Mandible : submandibular Fossa below the
mylohyoid bone• *Facial artery• *Mylohyoid nerve , artery
•

B) deep part :
• - deep to the mylohyoid muscle & superficial to hyoglossus muscle
• - above : lingual nerve , submandibular ganglion• -below : hypoglossal nerve

• Salivary Gland duct (wharton's duct ) :• - 5 cm• - emerge from the anterior end of the deep of the
gland• -runs ()mylohoid & hypoglossususcles• - then () sublingual gland genioglossus• - it opens in the floor of the mouth on the summit of
sublingual papilla at the side the frenulum of the tongue
The lingual nerve ( branch of the mandibular devision of the trigeminal nerve (V) has triple relation to the duct :1st descend lateralThen below the ductThen ascend medial to the duct
NB:NB:

Arterial supply : facial and lingual arteriesVenous drainage : common facial and lingual nerveLymph drainage : submandibuar & upper deep cervical LNsNerve supply :
A) parasympatheticFrom chorda tympani (branch from facial nerve ) pass to the gland through lingual nerve .B) sympathetic :Sympathetic plexus around the facial arteryC) sensory :Lingual nerve
•

Sialadenitis•• Inflammation of salivary gland
•
•

1) acute sialadenitis
Predisposing factors1 - bad oral hygiene2 - Obstruction of salivary duct by food particles foreign body or stone3 - dehydration4 - Debility

route of entry1- Direct : either along duct from mouth (commonest) or from a nearby Focus2- blood borne
Organisms :1- Viral : mumps influenza2- bacterial : staph aureus (commonest), streptococci, pneumococci

•Clinical picture• II. Local->• 1. Pain : early , dull aching, later it is severe
Throbbing.
•• 2. Swelling: elevating the lobule of the ear - red -
warm - edema - tender - fluctuate (late due to thicker parotid fascia)
•• 3. Opening of the duct: red, raised, and edematous,
with discharge.
•• 4. Trismus: restricted movement of
tempromandibular joint.
•
•
•• I. General-» toxemic symptoms (Fever, headache
etc.).
•

1. Leucocytosis
3. US.
• 2. X-ray film may show calcifications or stones
Investigations

• :
• (I) Conservative:
• A) General: rest antibiotic (clindamycin) analgesics a tonics.
• B) Local: hot fomentation, H202 mouth wash, KI as sialogogue.
• C) Observation: Pulse - temperature - swelling
After 3 days conservative treatment, patient either:a. Improves : continue conservative treatment till complete cure.b. Worsens : incision and drainage (Do not wait for fluctuation)
N.B :

2) Surgical treatment:• a. Parotid abscess:
• - A vertical skin incision in front of ear.• - The deep fascia is incised transversely to avoid
injury of the branches of facial nerve.• - A sinus forceps is then introduced closed and
then opened to drain the pus Hilton's method
•• b. Submandibular abscess:• - Skin incision parallel to lower border of the
mandible 1.5 inch below and in front of the angle of mandible to avoid injury of mandibular branch of facial nerve.• - Incise deep fascia• - A sinus forceps is then introduced closed and
then opened to drain the pus ( Hilton's method).

1) Chronic sialadenitis
•Etiology:
•• I. Chronic calcular sialadenitis• 1. Infection: is a good former for stones• 2. Stasis : by sepsis, stricture or FB.
•• II. Chronic non calcular sialadenitis• 1. Oral hygiene is poor.• 2. Obstruction of salivary duct by food particles, F.B.• 3. Imperfect drainage of acute sialoadenitis.
•
•
•

I. Chronic calcular sialadenitis * Site:Stones lie in the gland or in the duct. Submandibular glands to parotid ratio is 50 to 1 because :
A. Secretions of submandibular are more viscid.Parotid secretion is waterySubmandibular secretion is mucoid & viscidB. Its duct opens in floor of mouth -> obstruction by food particles.C. Drainage of submandibular gland is independed.
*Composition: composed of Calcium, Mg phosphate & carbonate.
Pathology:

Complications:
I. Chronic calcular sialoadenitis c. Malignancy.
II. Chronic non calcular sialoadenitis a. Recurrent acute attacks. b. Stone formation. c. Sialactasis: dilatation of the salivary ducts. a. Obstruction and infection may lead to abscess & fistula formation. b. Migration: If small stone.

type of patient :(4) Complications.
• male > female• occurs in middle and old age.
•
• Symptoms• (1) pain :• Dull aching pain if the stone is in the gland or colicky
pain if it is in duct• May refer to tip of the tongue due to irritation of
lingual nerve as it hooks around Submandibular duct• Increases with meal & mastication.
•• (2) Swelling:• The gland is enlarged 6& its size is increased after meal.• Stone in submandibular duct may be felt through floor
of mouth.
•• (3) Discharge: Bloody or even purulent discharge may
be seen coming from duct.
•
Clinical Picture:

Signs
(2) gland is enlarged, tender, cannot be rolled over lower border of mandible (due to capsule of the gland which fix it to the mandible) with preservation of the sulcus ( ) the gland & body of the mandible(3) Bidigital palation: the gland better felt from inside the mouth(4) The duct itself may be palpated with stone in it.
(5) Opening of duct is seen red, raised, discharging blood or pus. A stone may be seen peeping from the duct opening.
• (1) Lemon test: Pain and gland increase in size when the patient is given a lemon to suck.
•

(1) Plain X -Ray. Stones are 100% radio opaque
(3) Neck US.
(2) Sialography.
A radio-opaque material as lipidol is injected in the canulated duct to delineate it and shows sialactasis behind stone.
Investigations:

Treatment:
(A) Stone in the Duct:
• a. Peeping stone from orifice -> meatotomy
•• b. Stone in the duct:• - Under local anesthesia, the duct is underrun by an
anchoring stitch to avoid slippage of stone to the gland)• -Slit duct open from orifice to stone.• -Remove stone, and leave duct opened after
removal of anchoring stitch to allow a better drainage.• c. Recurrent ductal stones or associated with
gland stones: Submandibular sialadenectomy
•• (B) Stone in the gland:• - Submandibular sialadenectomy.• - Total conservative partidectomy
•

Salivary gland tumors Salivary gland tumors

(i)Benign:
B.connective tissue:
Hemangioma-lymphangioma-lipoma-neurofibroma
Pleomorphic adenomas
Monomorphic adenomas
Oncocytoma
• A.epithelial:
(II)Malignant:
A.epthelial:carcinomaB.connective tissue :sarcoma &lymphomas

80% of salivary neoplasms arise in the parotid gland
80% affecting superficial lobe80% are benign80% of benign tumors are pleomorphic adenoma
Rule of 80%

Pleomorphic adenoma(mixed salivary gland tumor)
• Pathology:• Site : common in the parotid gland (80%)• N/E: • Small,firm,incompeletly capsulated mass with lobulated
surface • Cut surface grayish white,occasionally it presents cystic
formation

M/E: there is pleomorphism:
2)stroma: appears blue resembling that of cartilage but now it is found that blue material is a mucinous secretion 3)there are microscopic extensions beyond capsule of the tumor (satellite nodule with projections) and this is responsible for high incidence of recurrence after simple enculation (considered locally malignant tumor )
1)cells: spindle or stellate shaped and arranged in acini,clusters or sheets

Complications :
1)disfigurement
2)malignancy after several years (2-3%)
•

Clinical picture :Patient:
male=female
age at presentation around 40 years
Symptoms :
slowly growing, painless swelling
•
•

• Signs:
• 2)no lymph nodes enlargement
•• 1)single swelling (may be bilateral ) has the
following criteria • a)site : usually in the parotid regin • b)size :usually small • c)shape:hemispherical • d)surface: smooth & lobulated • e)skin over: not attached to the tumor ( freely
mobile)• f)surrounding structures(to eclude malignancy )• facial nerve is free • masseter muscle is not attached • preservation of superficial temporal artery
pulsation• g)special characters:• they fill the space between ramus of mandible and
mastoid process • they may raise lobule of ear• they become more prominent on contraction of
masseter • they become less prominent on opening of the
mouth • h)consistency: firm( never hard )• i)edge: well defined edge • j)tenderness: not tender • k)moblity: freely mobile • l)if the tumor arise in deep lobe: pushing the tonsil
toward midline

Investigations :
1)US,CT&MRI: to assess the extent t deep lobe and the relation to facial nerve
2)isotope scan tcm99 pertechnetate:
All salivary tumors give cold spot except warthin's tumor give hot spot
3)biopsy
•

Treatment :
1)simple enucleation and localized resection
•• 2) superficial parotidectomy:
•• Removal of superficial lobe of the gland +
preservation of facial nerve • Indicated if tumor is in superficial lbe
•• 3)total conservative parotidectomy:• Removal of superficial and deep lobes of gland +
preservation of facial nerve• Indicated for dumbbell parotid tumor & tumor is in
deep lobe or recurrent tumors

Monomorphic Adenoma(adenolymphoma or warthin's tumor)
Incidence: 10% of benign parotid tumors

Pathology :
Site : in lower part of parotid , bilateral in 10%• N.E:small,cystic&completely capsulated mass • Cut section: white areas due to lymphoid tissues
surrounding cystic structures • M/E:• Cells are columnar arranged into cystic spaces with
formation of papillary projections into these cystic spaces which contain mucoid material • Stroma: consist of lymphoid tissues originating
from lymphoid aggregation present in normal parotid gland and support cystic spaces

• Clinical picture :• male>female & age >50y• slowly growing ,painless swelling • as pleomorphic adenoma but not elevating the lobule of ear
& consistency cystic• Complications : not precancerous • Investigations:• As pleomorphic but gives hot spot in isotope scan
•• Signs :
• Symptoms : • Patient :

Treatment :
• Enucleation can be done or superficial parotidectomy

Carcinoma of salivary Carcinoma of salivary glandsglands
Etiology : Predisposing factors : salivary stone &radiation exposure
Precancerous factors : pleomorphic adenoma
•

Pathology :
•
• Site :• - 20% of the parotid tumors are malignant• - 50% of the submandibular tumors are
malignant• - 100% of the sublingual tumors are malignant• N/E :• - large , hard, ill defined ,mass with nodular or
irregular surface• - cut section ; non capsulated with areas of
hemorrhage , necrosis and cyst formation

• 1- Mucoepidermoid (commonest) :
• - arises from duct epithelium • - contains both epidermoid and mucous
secreting epithelium forming cysts • - three grades are described ; low grade ,
intermediate grade , high grade• 2- Epidermoid (squamous cell) carcinoma (rare) :• - arises from duct epithelium• - rare tumor of parotid , more common in
submandibular gland• 3- Adenocarcinoma :• - arises from duct epithelium , arranged in acini• 4- Adenoid cystic carcinoma :• - arises from myoepithelial cells & duct
epithelium cells• - arranged in columns around central cavities of
mucous giving Swiss- cheese pattern• - invade perineural tissues of adjacent nerves
---- painful• - hard & fixed • 5- Acinic cell tumor :• - arises from acini and composed of cells
resemble serous acini• - slowly growing , soft or cystic• - more common in females• 6- Carcinoma ex- pleomorphic adenoma• 7- Undifferentiated
•

• Spread:
•• (1) Direct : - Intrinsic : within gland infiltrating facial nerve• - Extrinsic : to the surroundings ( skin ,
masseter , mandible , oral cavity ) • (2) Lymphatic : to deep cervical L.N.• (3) Blood : to lungs & bones• (4) Perineural invasion (adenoid cystic type) which explains
high rate of recurrence •

Staging TNM :
Primary tumor :
• Tx -----primary tumor cannot be assessed• T1 -----Tumor < 2 cm in greatest dimension• T2 -----Tumor 2-4 cm in greatest dimension• T3 -----Tumor > 4 cm in greatest dimension• T4 -----• T4a ----Tumor invades skin , mandible , ear
canal or facial nerve involvement• T4b ----Tumor invades skull base or
ptergoid plates or carotid artery• Lymph nodes :• Nx -----Regional lymph nodes cannot be
assessed• No -----No regional lymph node metastases• N1 -----Metastases in a single ipsilateral lymph
node < 3cm • N2 -----Metastases in lymph node 3-6 cm • - N2a ----- Metastases in a single
ipsilateral L.N.• - N2b -----Metastases in multiple
ipsilateral L.N.• - N2c -----Metastases in bilateral or
contralateral L.N.• N3 -----Metastases in a lymph node > 6 cm
•• Metastases :• Mx - M0 - M1

• Type of patient :• - Male > female & age > 50 years ( old man )• - Acinic cell carcinoma more common in female• • Symptoms :• - Rapidly growing , painless swelling (painful in adenoid
cystic )• - slow rate of growth in acinic cell tumor•
•
Clinical picture :

Signs :1-Single swelling has the following criteria : 1- Site : usually in parotid region 2- Size : variable (rapidly growing) 3- Shape : irregular 4- Surface : nodular or irregular 5- Skin over : attached to the tumor(not freely mobile) 6- Surrounding structures : - Facial nerve ----- may be infiltrated - Masseter muscle ----- may be attached - Pulsation of superficial temporal a. -----may be absent 7- Special characters : - fill space () ramus of mandible & mastoid process - may raise lobule of ear - become more prominent on contraction of masseter - become less prominent on opening of the mouth 8- Consistency : hard ( soft in acinic cell tumor ) 9- Edge : ill-defined edge 10- Tenderness : slightly tender2- Lymph node : - Enlarged , Hard , Painless , Early Mobile & Later Fixed

Investigations :•• 1- U.S. & CT & MRI• 2- Isotope scan Tc 99 Pertechnetate : cold
spots • 3- Biopsy• 4- Investigation for metastases : esp. for neck
L.N. ---- U.S & CT
•• Complications :
•• 1-Fungation & ulceration• 2-Infection , hemorrhage and fistula formation• 3-Nerve palsy : Facial palsy ----- in parotid tumor • Hypoglossal & lingual nerve injury -----
in submandibular tumor• 4-Disfigurement• 5-Distant metastases
•
•

Differential diagnosis :
Causes of swelling in the parotid region
• • 1- Gland : Inflammation , Tumor , Autoimmune• 2- Lymph node : Preauricular L.N. ,
Lymphadenopathy• 3- Skin : Sebaceous cyst , Preauricular dermoid
cyst • 4- Muscle : Rhabdomyosarcoma • 5- Connective tissue : Lipoma , Fibroma • 6- Nerve : Neurofibroma • 7- Blood vessels : Haemangioma • 8- Mandible : Adamantinoma , Osteoma
•

Treatment : (A)Operable : Radical procedures
(1) Tumor : a. Parotid tumors :
- ( total radical parotidectomy ) - removal of superficial and deep lobes of gland
sacrificing facial nerve - as regard facial nerve :
1- may be grafted using great auricular nerve 2- transposition of hypoglossal nerve then
anastomosing it to peripheral branches of facial nerve
3- facial slings to support facial tissue b. Carcinoma of submandibular gland :
- ( total radical submandibular sialadenectomy )
(2) LNs : a. Negative LNs : elective neck dissection for high
grade tumors b. Positive LNs : block neck dissection
(3) Post-operative radiotherapy : For - High grade tumor with extra glandular
extention or perineural spread

(B)Inoperable : - palliative resection as radiotherapy has minor role ( Relatively radio-resistant )

Copyright @ All data are from Mansoura faculty of medicine General surgery book