Salivary Gland Tumors Slide Seminar
47
Salivary Gland Tumors Slide Seminar Arghavan Etebarian DDS, MSc February 2021
Transcript of Salivary Gland Tumors Slide Seminar

Salivary Gland Tumors Slide Seminar
Arghavan Etebarian DDS, MSc
February 2021

Case 1 –video 1 attached
A 15 yrs. old young lady
with a parotid mass
https://www.dropbox.com/s/l9tqx9ya6wgmmeq/1.mp4?dl=0
To see video #1, please find the attached video or, click
the below link to open it in the browser:

What is your diagnosis?
• A. Cystadenocarcinoma
• B. Metastatic squamous cell carcinoma
• C. Mucoepidermoid carcinoma
• D. Low grade salivary duct carcinoma

Mucoepidermoid carcinomaIntermediate grade
• 3 cell types
• No myoepithelial cells
• Solid and cystic spaces
• Sialomucin

PAS + Mucicarmine

Cystic low grade MEC

Intermediate cells and foci of epidermoid cells
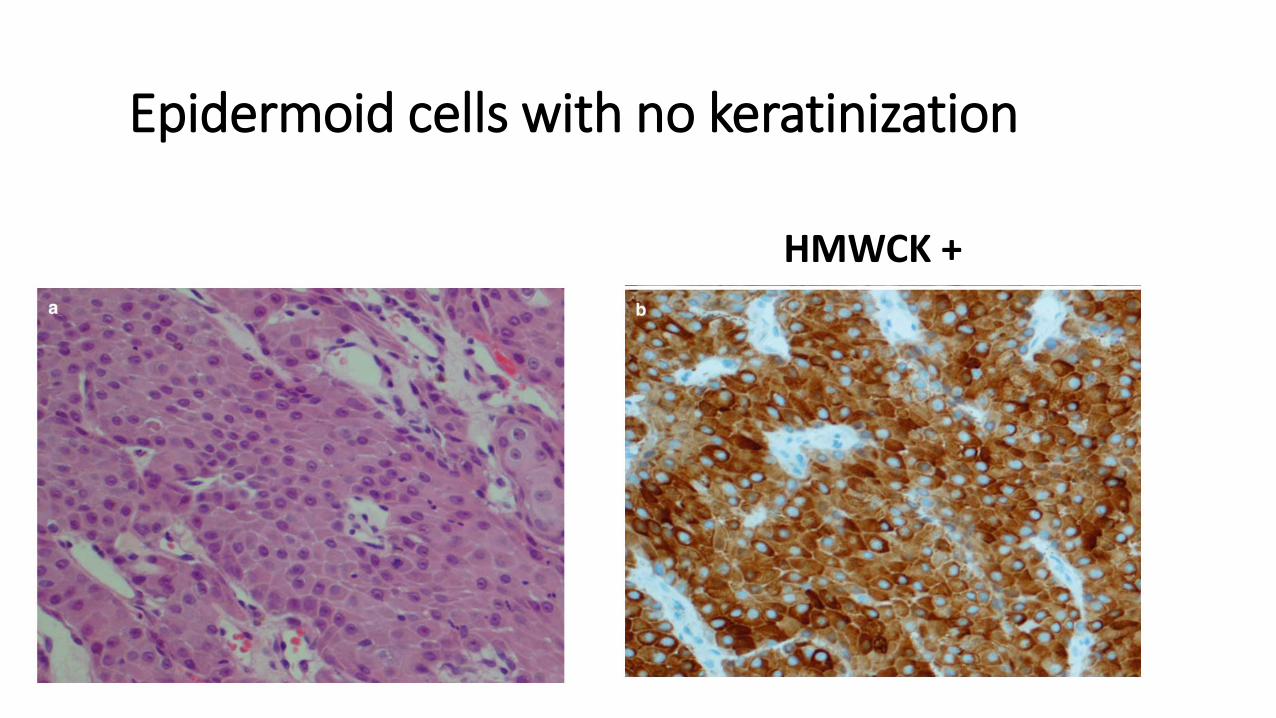
Epidermoid cells with no keratinization
HMWCK +

Clear cells (PAS+, diastase sensitive)

High grade MEC Cellular anaplasia

MEC or Metastatic skin SCC ? CK7+ BER-EP4+

Two-level grading is more practical to use!

IHC panel for MEC• CK7 (Strong +)• CK14 (Scattered +)• P63 +( striated ductal phenotype, basal cells origin, Exclude Metastatic RCC)• MUC1, MUC4, MUC5AC +
• Myoepithelial markers-> Negative
• Mucicarmine staining
Prognosis for MEC
Correlate strongly with clinical stageTumor site
Adequacy of surgical procedure
Adjuvant therapy
• Importance of early diagnosis
Tumor size Tumor invasion Vascular/ perineural invasion Surgical margins

Case 2- video 2 attached
A 44 yrs. old woman with a submandibular
masshttps://www.dropbox.com/s/nkpxhabnkjeh2p5/2.mp4?dl=0
To see video #2, please find the attached video or, click
the below link to open it in the browser:

What is your diagnosis?
• A. Salivary duct carcinoma
• B. Adenoid cystic carcinoma
• C. Basal cell adenocarcinoma
• D. Polymorphous adenocarcinoma (PAC)

Sieve-like pattern
of small malignant basaloid cells
2 cell types: luminal and abluminal
3 growth patterns
Adenoid cystic carcinoma

1. Cribriform ( glandular)
-Numerous pseudocyst (punched out)-Some true cysts

2. Tubular ADCC
Inner epithelialOuter myoepithelial

3.Solid ADCC
Cellular atypia

Perineural and intraneuralinvasion
Centered around a vessel

Infiltrative borders
Pseudopapillarygrowth pattern
PAC?
-Ki67>10%
-GFAP+

Differential diagnosisfor ADCC

ADCC
A high grade malignancy and
histological grading is of less importance!
Clinical staging
Case 3- video 3 attached
A 55 yrs. old woman with a parotid mass
https://www.dropbox.com/s/73puz6564xbcrqw/3.mp4?dl=0
To see video #3, please find the attached video or, click
the below link to open it in the browser:

What is your diagnosis?
• A. Mucoepidermoid carcinoma
• B. Acinic cell carcinoma
• C. Secretory carcinoma
• D. Metastatic thyroid carcinoma

Acinic cell carcinoma
• 4 cell types
• 4 patterns: Solid, Microcystic, Papillary-cystic, Follicular

1. Acinar cells (PASD+)

2. Vacuolated cells (PAS -)( papillary cystic- microcystic variant)

3. Clear cells (PAS -) Rare!

4. Non-specific glandular cells

Prominent lymphocytic infiltrationGerminal center formation

1. Solid pattern
-Uniform basophilic acinar cells
-Necrosis !?-Mitotic figures: unusual

2. Microcystic patternMucinous, proteinaceous material

3. Papillary-cystic patternACC or metastatic PTC ?

4. Follicular patternMetastatic follicular thyroid carcinoma ?

• Well-differentiated ACC associated with lymphoid stromaMicrocystic growth pattern + dense lymphoid stroma
Low Ki-67 labelling index
Thin pseudocapsule
• High grade transformation (dedifferentiation) Conventional low-grade ACC + high grade ACC
High Ki-67 labelling

ACC diagnosis and treatmentDOG1 staining for ACC diagnosis (acinar differentiation) MUC3 positive in ACC ( not in MEC, ADCC)Always negative for P63 ( MEC is always +)
• Histological grade is stronger predictor of survival than TNM stage.• Surgical resection -> excellent results• Best survival rate of all salivary gland carcinomas

MASC 2010
SC 2017

PAS stain in ACC and MASC

S100 – in ACC S100 + in MASC

DOG1 + in ACC(apical and membranous)
Mammaglobin + in MASC

In SC ( no other salivary gland tumor!)
ETV6-RET ETV6-MET
Positive ETV6-NTRK3 gene fusion
100 % specific90.7% sensitive

Immunohistochemistry
Plays a limited, even though important rolein diagnosing salivary gland tumors
Assist the final diagnosis! CK7+/CK20-

Strongly recommended!

Thank you and have a lovely day