
Sa1 2017 COPD March Internal Medicine...
24
Strange - COPD 3/11/17 1 What is new in COPD? Charlie Strange, MD Professor of Pulmonary and Critical Care Medicine Medical University of South Carolina Dr. Strange is a grant recipient from the NIH, Alpha-1 Foundation, Baxalta, CSL Behring, Grifols, BTG, and Pulmonx in COPD. He is a consultant for Astra Zeneca, CSL Behring, and Grifols for COPD. Previous Definition of COPD Chronic Bronchitis Emphysema Airflow Obstruction Asthma Am J Respir Crit Care Med. 1995;152:S77. COPD
-
Upload
phungtuong -
Category
Documents
-
view
214 -
download
1
Transcript of Sa1 2017 COPD March Internal Medicine...

Strange - COPD 3/11/17
1
What is new in COPD?Charlie Strange, MD
Professor of Pulmonary and Critical Care Medicine
Medical University of South Carolina
Dr. Strange is a grant recipient from the NIH, Alpha-1 Foundation, Baxalta, CSL Behring, Grifols, BTG, and Pulmonx in COPD. He is a consultant for Astra Zeneca,
CSL Behring, and Grifols for COPD.
Previous Definition of COPD
Chronic Bronchitis Emphysema
Airflow Obstruction
Asthma
Am J Respir Crit Care Med. 1995;152:S77.
COPD

Strange - COPD 3/11/17
2
Current Definition of COPD
Chronic Bronchitis Emphysema
Airflow Obstruction
Asthma
Vestbo, J et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: GOLD Executive Summary. Am J Respir Crit Care Med 2013, 187(4):347-365.
.
COPD
Since 2009 COPD is now the #3 Cause of Death in the US
US Bureau of Health Statistics, 2011

Strange - COPD 3/11/17
3
Current Definition of the Asthma-COPD Overlap Syndrome (ACOS)
Chronic Bronchitis Emphysema
Airflow Obstruction
Asthma
Vestbo, J et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: GOLD Executive Summary. Am J Respir Crit Care Med 2013, 187(4):347-365.
.
ACOS
Model-based COPD Prevalence by County, 2011

Strange - COPD 3/11/17
4
Underdiagnosis of COPD in the United States
Age in Years
25-44 45-54 55-64 65-74 >75
Per
cen
tage
22.9%20.7%
14.0%
7.2%
5.2%
Diagnosed with COPD
GOLD stage II or higher
Mannino DM, MMWR 2002; 51:1-16
Diagnosis of COPD
SYMPTOMS
coughcoughsputumsputumdyspneadyspnea
EXPOSURE TO RISKFACTORS
tobaccotobaccooccupationoccupation
indoor/outdoor pollutionindoor/outdoor pollution
SPIROMETRYSPIROMETRY

Strange - COPD 3/11/17
5
Spirometry
0 1 2 3 4 5 6Seconds
VolumeLiters
4
3
2
1
0
FEV1FVCRestriction
Normal
Obstruction
Spirometry Interpretation
FEV1/FVC <0.70 FEV1/FVC > 0.70FVC < 80% Predicted
ObstructionFEV1
RestrictionFVC
Severe<50%
Moderate<70%
Mild<80%
VerySevere<30%
Moderate50-80%
Mild>80%
Severe30-50%
IV III II IGOLD Stage

Strange - COPD 3/11/17
6
Age
FEV 1(L)
NormalSusceptible Smoker
SymptomsQuit
Average Smoker
5
4
3
1
2
7525 50
FEV1 in the Framingham, Copenhagen City, and Lovelace Cohorts
Lange P, et al. NEJM 2015; 373:111
Strange - COPD 3/11/17
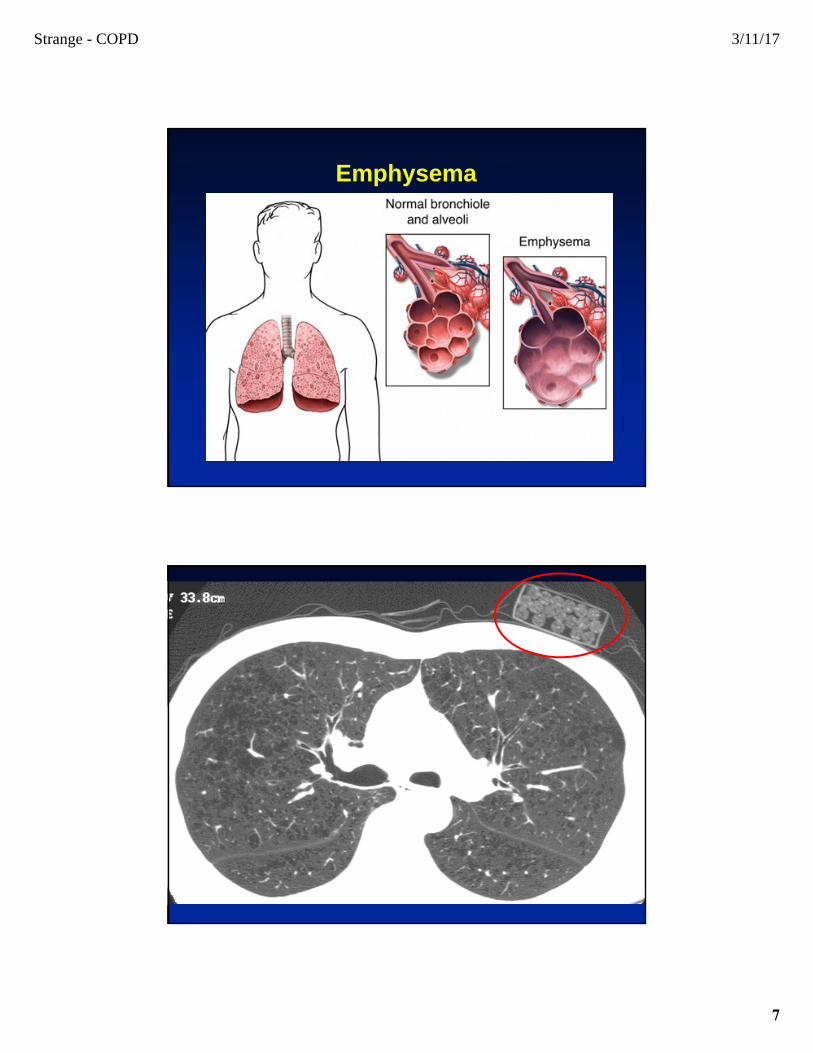
7
Emphysema

Strange - COPD 3/11/17
8
Risk Factors for COPD
Smoking Tobacco in any formMarijuanaPassive smoking
Ambient air pollution (eg. uranium)Hyperresponsive airwaysAlpha‐1 antitrypsin deficiencyHIVMarfan Syndrome, Ehler’s DanlosCutis laxaHypocomplementemic urticarial vasculitisCrack cocaine, IV RitalinPrematurity
What is Alpha-1?
• Alpha-1 Antitrypsin (AAT) Deficiency is a genetic disease in which a deficiency of AAT produces COPD and liver disease from retained misfolded AAT.
ZZZ

Strange - COPD 3/11/17
9
You’re Not Just Identifying a Patient—You’re Discovering an Entire Family at Risk for Lung
Disease•The model
shown is based on an actual family that has been tested for Alpha-1
Alpha-1 family tree of disease
Pi MZ Pi ZZ
Pi ZZ Pi ZZ Pi ZZ Pi ZZPi MZ Pi MZuntested untestedPi MS Pi MM
untested Pi MSPi MZPi MZ Pi MZ Pi MZ Pi MZPi ZZ Pi ZZ Pi ZZ
Pi MMPi MSPi MZPi ZZuntested
Pi MZ
Pi MZPi MZ
Alpha-1 Foundation CRC Research Registry:
www.alphaoneregistry.org

Strange - COPD 3/11/17
10
lobal Initiative for Chronic
bstructive
ung
isease
lobal Initiative for Chronic
bstructive
ung
isease
GOLD
GOLD
www.goldCOPD.com
Step Care Model of COPD Therapy
(1) Smoking Cessation
(2) Bronchodilator TherapyIpratropium and/or Beta2-Agonist
(3) Exacerbation PreventionRegular Inhaled LAMA/LABA/Corticosteroid
(4) Targeted Therapy of ExacerbationsA. Infectious Antibiotic for 7-10 daysB. Excess mucus Mucolytic/ expectorant for 2-8 wksC. Neither Corticosteroid boost for 3-14 days
(5) Expectant TherapyA. Pulmonary Rehabilitation ProgramB. NutritionC. Influenza and Pneumococcal VaccinationD. Oxygen
(6) Treat HyperinflationLung Transplant or Volume Reduction Surgery
Strange - COPD 3/11/17
11
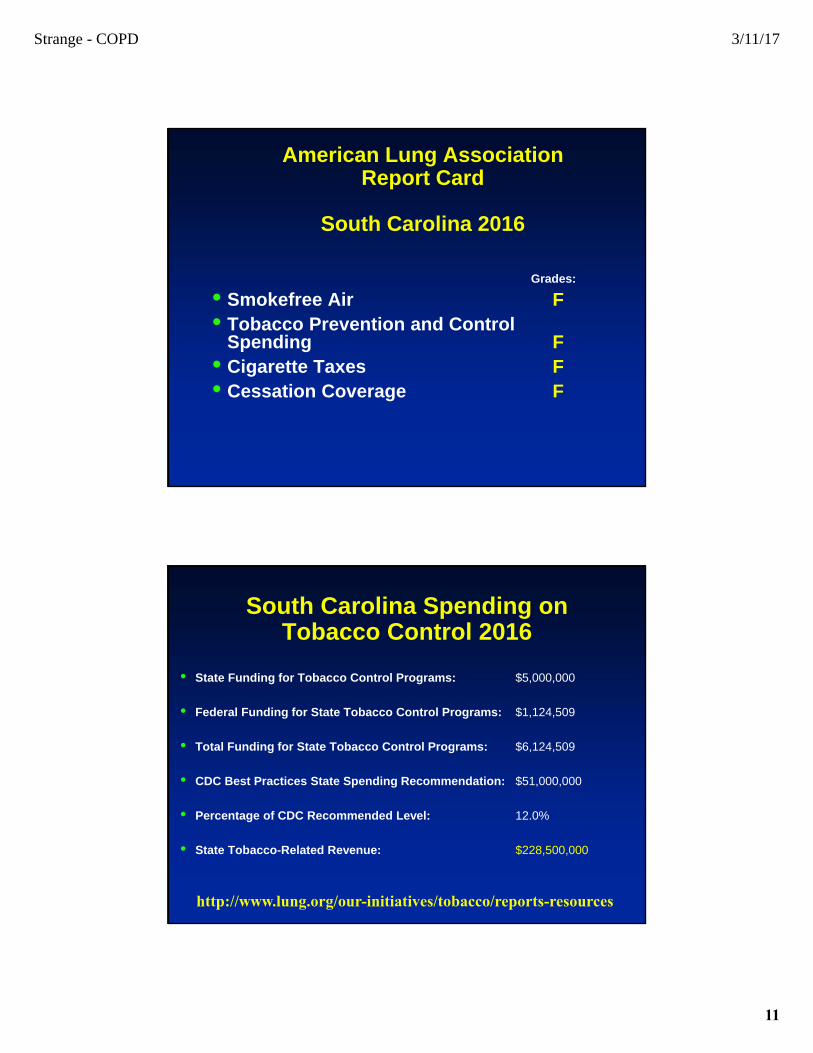
American Lung Association Report Card
South Carolina 2016
Grades:
• Smokefree Air F• Tobacco Prevention and Control
Spending F• Cigarette Taxes F• Cessation Coverage F
South Carolina Spending on Tobacco Control 2016
• State Funding for Tobacco Control Programs: $5,000,000
• Federal Funding for State Tobacco Control Programs: $1,124,509
• Total Funding for State Tobacco Control Programs: $6,124,509
• CDC Best Practices State Spending Recommendation: $51,000,000
• Percentage of CDC Recommended Level: 12.0%
• State Tobacco-Related Revenue: $228,500,000
http://www.lung.org/our-initiatives/tobacco/reports-resources

Strange - COPD 3/11/17
12
GOLD COPD
C D
A B
Spirometry(GOLD Class)
Exacerbations
Symptoms(mMRC/CAT)
0-1/<10 ≥ 2/≥10
Hospitalizations
1
2
3
4
≤10
≥2≥1
Classes of Medications
SABA= Short acting beta agonists (eg. albuterol)SAMA= Short acting muscarinic antagonists (eg. ipratropium)
LABA = Long acting beta agonistsLAMA= Long acting muscarinic antagonists
ICS= Inhaled corticosteroids
LTA= Leukotriene antagonists (eg. montelukast)
PDE4 inhibitors (roflumilast)
Strange - COPD 3/11/17
13
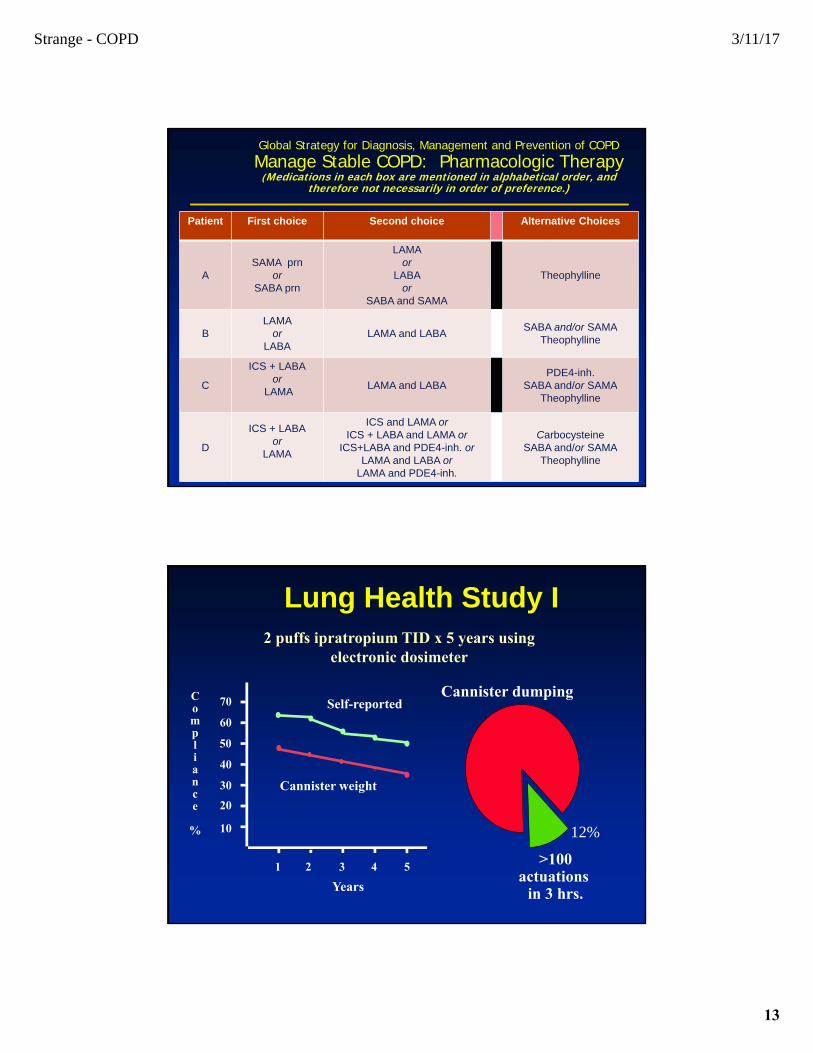
Global Strategy for Diagnosis, Management and Prevention of COPDManage Stable COPD: Pharmacologic Therapy
(Medications in each box are mentioned in alphabetical order, and therefore not necessarily in order of preference.)
Patient First choice Second choice Alternative Choices
ASAMA prn
orSABA prn
LAMAor
LABA or
SABA and SAMA
Theophylline
BLAMA
orLABA
LAMA and LABASABA and/or SAMA
Theophylline
C
ICS + LABAor
LAMALAMA and LABA
PDE4-inh.SABA and/or SAMA
Theophylline
D
ICS + LABAor
LAMA
ICS and LAMA orICS + LABA and LAMA or
ICS+LABA and PDE4-inh. orLAMA and LABA or
LAMA and PDE4-inh.
CarbocysteineSABA and/or SAMA
Theophylline
Lung Health Study I2 puffs ipratropium TID x 5 years using
electronic dosimeter
Compliance
%
1 2 3 4 5
10
20
30
40
50
60
70 Self-reported
Cannister weight
Cannister dumping
>100actuations
in 3 hrs.Years
12%

Strange - COPD 3/11/17
14
Currently Available Single Agent Bronchodilators
Albuterol 0.18 mg 2.5 mg 28(Ventolin, Proventil, Proair)
Levoalbuterol (Xopenex) 0.09 mg 0.63-1.25 mg 14-28Ipratroprium (Atrovent) 0.36 mg 0.5 mg 28
Salmeterol (Serevent) 0.42 mg 0.50mg BIDOladaterol (Striverdi) 2. 5mcg QDIndacaterol (Arcapta) 75 mcg QDFormoterol (Foradil, Perforomist) 12 mcg BID 20 mcg BIDAformoterol (Brovana) 15 mcg BID
Tiotroprium (Spiriva) 0.18 mg QDAclidinium (Tudorza) 0.4 mg BIDUmeclidinium (Incruze) 62.5 mcg QDGlycopyrolate (Seebri) 44 mcg QD
Drug MDI2 Puffs
DPI / Mist
NebulizerDose
MDI to Equal Neb
Management of ExacerbationsObjective Strategy
Acute
Relieve dyspneaSABA +/- short acting
anticholinergic
Reduce airway inflammation
Systemic corticosteroids
Improve lung function
Systemic corticosteroids
Eradicate infections Antibiotics
Maintenance Reduce risk of new
exacerbation
Smoking cessation
Pharmacotherapy •LAMA•LABA
•LAMA/LABA•LABA/ICS
Immunizations•Influenza
•Pneumonia
Pulmonary rehab
Self-management supportAnzueto A. Am J Med Sci. 2010]

Strange - COPD 3/11/17
15
LAMA/LABATiotropium/Olodaterol Boeringher
IngelheimStiolto Respimat®
Vilanterol/Umeclidiniumbromide
GlaxoSmithKline Anoro Ellipta®
Glycopyronium/Indacaterol Novartis Pharmaceuticals
Ultibron Breezhaler®
Glycopyrronium/formoterol
fumarate
AstraZeneca Bevispi Aerosphere®
Fluticasone propionate/ Salmeterol
GlaxoSmithKline, Elpen
Advair Diskus®, Advair HFA®
Budesonide/Formoterol AstraZeneca Symbicort®
Mometasone/Formoterol Merck Dulera® for asthma, investigational COPD
Fluticasone furoate/ Vilanterol
GlaxoSmithKline Breo Ellipta®
ICS /LABA
Exacerbation Rates on LAMA/LABA vs ICS (N=3358)
Wedzicha JA. NEJM 2016.
Strange - COPD 3/11/17
16
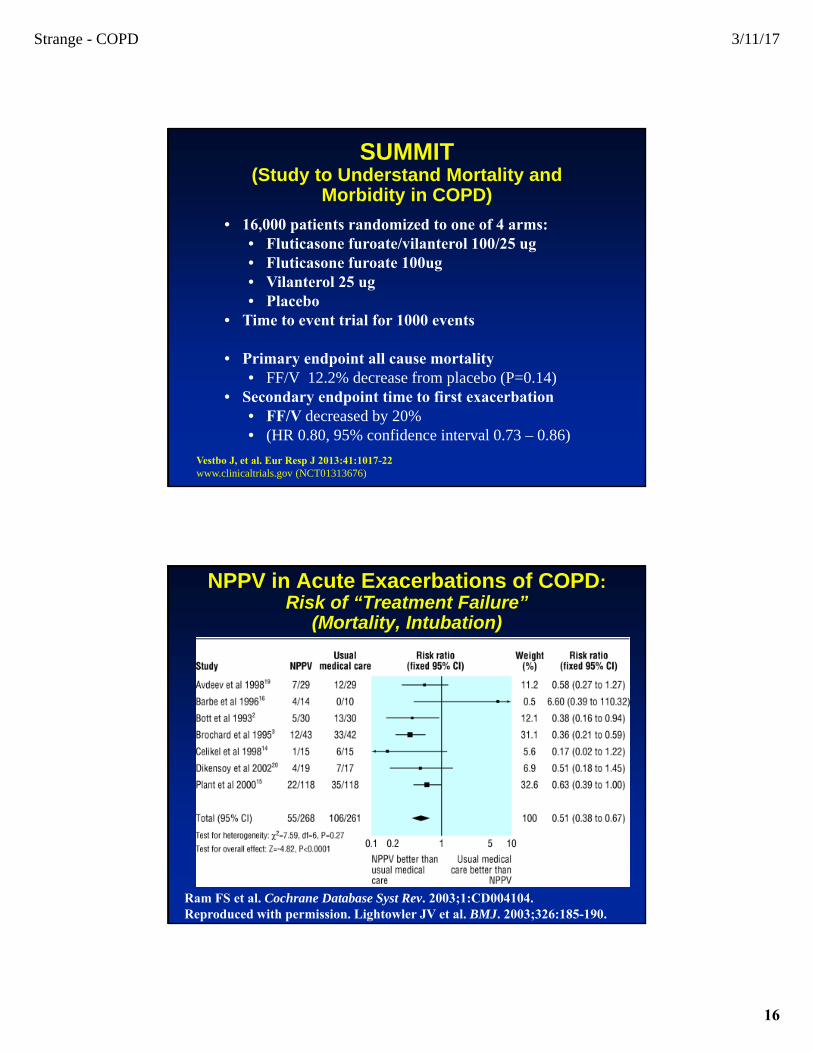
SUMMIT(Study to Understand Mortality and
Morbidity in COPD)
• 16,000 patients randomized to one of 4 arms:• Fluticasone furoate/vilanterol 100/25 ug• Fluticasone furoate 100ug• Vilanterol 25 ug• Placebo
• Time to event trial for 1000 events
• Primary endpoint all cause mortality • FF/V 12.2% decrease from placebo (P=0.14)
• Secondary endpoint time to first exacerbation• FF/V decreased by 20% • (HR 0.80, 95% confidence interval 0.73 – 0.86)
Vestbo J, et al. Eur Resp J 2013:41:1017-22www.clinicaltrials.gov (NCT01313676)
NPPV in Acute Exacerbations of COPD:Risk of “Treatment Failure”
(Mortality, Intubation)
Ram FS et al. Cochrane Database Syst Rev. 2003;1:CD004104.Reproduced with permission. Lightowler JV et al. BMJ. 2003;326:185-190.
Strange - COPD 3/11/17
17
GoldSealMirage
IQ
SoftFitSimplicity
Spectrum
Breeze
PhantomTotal face mask
Oxygen• Improved mortality in individuals with resting pO2
<55 mmHg• 24 hours/day is better than 12 hours per day
• Improved exercise and quality of life in individuals who have O2 desaturation <88% when given oxygen with exercise. No change in other outcomes.
• No data that oxygen improves mortality with O2 sats >88% despite intermittent desaturations <88%.

Strange - COPD 3/11/17
18
Manage Stable COPD Rehabilitation
All COPD-patients benefit from exercise training programs, improving with respect to both exercise tolerance and symptoms of dyspnea and fatigue (Evidence A).
Progressive Hyperinflation Reduces Inspiratory Capacity
Cooper CB. Am J Med. 2006;119:S21.
Normal Mild Moderate Severe
COPD
VT
FRC/EELV
ICHypotheticalDyspneaThreshold
IC
IRV
ERV
RV
TLC

Strange - COPD 3/11/17
19
Zephyr-Endobronchial Valves (EBV)
Intrabronchial Valves (IBV)
PneumRx®
Elevair™ Endobronchial
Coil
InterVapor -Bronchoscopic Thermal Vapor
Ablation (BTVA)
PulmonX
Spiration
PneumRx
Uptake
Tis
sue
com
pre
ssio
n
Mechanism of Action
Flo
w r
egu
lati
on
Product
BTVA uses heated water vapor to produce a thermal reaction leading to an initial localized inflammatory response followed by permanent fibrosis and atelectasis with subsequent reduction in lung volume.
Image
Coils are delivered to the lung in a straight configuration through a bronchoscope. Once deployed, LVRC reduces the diseased lung volume by coiling up thereby compressing the diseased tissue and allowing expansion of the healthier areas
One-way valves prevent air from entering the blocked emphysematous segment, while allowing the venting of expired gas and bronchial secretions, leading to atelectasis of the isolated segments with subsequent reduction in lung volume.

Strange - COPD 3/11/17
20
The RePneuⓇ Lung Volume Reduction Coil (LVRCⓇ)
Self actuating Nitinol implant
LV
RC
Pro
ced
ure
Courtesy of Dr. Gaetan Deslee

Strange - COPD 3/11/17
21
Disease Management Programs for COPD
761 COPD patients entered into program with 1.5 hour orientation + spirometry
Randomized to program vs controlMonthly nurse telephone calls for 1 year.
Prednisone use, tiotroprium use, antibiotic courses all P<0.05 different between groups
COPD Hospitalization (p<0.0001)
COPD Hosp or ER Visits (p<0001)
Rice KL, et al. Am J Respir Crit Care Med. 2010

Strange - COPD 3/11/17
22
Patient Centered Care and Self-Efficacy
Hospice
Pulmonary Rehabilitation
RT
Specialist
PCP
Patient(Home &
Community)
SNF
Acute Rehab
LTACHospital
EDUC
Patient/caregiver Education
Problem solving skill mastery
Social participation
Pulmonary Pulmonary
MUSC Medical Center
Number of Discharges
168
Number of Readmissions
34
Readmissions Rate
20.2%
Excess Readmissions
Ratio
0.9929
Chronic Obstructive Pulmonary Disease (COPD)
Figures are calculated from publicly available data in CMS's FY 2016 IPPS Final Rule Impact File notice, Estimated amounts may differ from actual final figures.

Strange - COPD 3/11/17
23
Symptom Status Update
Patients With Moderate and Severe COPD Record Daily Respiratory Symptoms
• Breathlessness (Modified Borg Scale)
• Sputum Quantity, Color, and Consistency
• Peak Flow Measurements
• Presence of Temperature Over 100°F
• Presence of Any Cough, Wheeze, Sore Throat or Nasal Congestion
Current Guidelines Based on ATS/ERS Guidelines
HGE Exacerba on Treatment Severity Score
None Mild (any FEV1)
Mild‐Moderate
(FEV1 > 50%)
Moderate‐Severe
(FEV1 < 50%)
Severe (any FEV1)
Score
0‐1 1‐1.9 2‐2.9 2‐2.9 >3
Ac on 1 Con nue present care
Increase albuterol
Increase albuterol
Increase albuterol
Increase albuterol
Ac on 2 No changes needed
Increase ipratropium
Increase ipratropium
Increase ipratropium
Increase ipratropium
Ac on 3 Add albuterol or ipratropium if on solo BDA therapy
Increase albuterol +/‐ ipratropium
Increase both albuterol and ipratropium
Increase both albuterol and ipratropium
Ac on 4 +/‐ Prednisone +/‐ Prednisone Prednisone
Ac on 5: If purulent mucous add an bio c
Symptom Deviation ScoreSymptom Deviation Score Suggested Treatment Based on Score
Suggested Treatment Based on Score
Time to TreatTime to Treat

Strange - COPD 3/11/17
24
COPD CO-PILOT: First Prospective Randomized TrialPA-SCOPE: Impact of Early Telemedicine AECOPD Intervention on Daily Dyspnea Score
PA-SCOPE: Impact of Early Telemedicine AECOPD Intervention on Daily Peak Flow
05
1015202530
Mild Moderate SevereFre
q.
of
Exa
cerb
atio
n
Exacerbation Severity
Frequency of Exacerbation v. Exacerbation Severity
Call Center
Standard of Care
*
* P<0.001
Criner G, 2016
Conclusions
• The COPD world has many new options for therapy, some of them pharmacologic
• New inhalers improve convenience
• Large unmet need in compliance with medications
• Much more focus on integrated care will drive COPD therapy


















