S tef ana Rosso - McGill Universitydigitool.library.mcgill.ca/thesisfile59292.pdf · S tef ana...
142
Pre ven ti ve Practices of General Practi tioners in Torino, 1 taly S tef ana Rosso Department of Epidemiology and Biostatistics McGill University, Montreal A Thesis submitted to the Faculty of Graduate Studies and RGsearch in partial fulfillment of the requirements for the degree of Master of Science @S. ROSSO, 1989
Transcript of S tef ana Rosso - McGill Universitydigitool.library.mcgill.ca/thesisfile59292.pdf · S tef ana...

Pre ven ti ve Practices of General Practi tioners
in Torino, 1 taly
S tef ana Rosso
Department of Epidemiology and Biostatistics
McGill University, Montreal
A Thesis submitted to the
Faculty of Graduate Studies and RGsearch
in partial fulfillment of the requirements
for the degree of
Master of Science
@S. ROSSO, 1989

ACKNOWLBDGMENTS
The author is grateful to Professors Renddo N. Battista, J. Ivan Williams and
Samy Suissa for their assistance through every stage of this wCJrk and for making
available aIl the necessary resources from the Division of Clinical Epidemiology of the
Montreal General Hospital. The author is also indebted to Dr. Nereo Segnan, who
initiated this study, and to several colleagues from Torino who were involved in its
execution.
Appreciation is expressed to Dr. N.J.B. Wiggin, Ms. Cynthia Palmer and Ms.
Jeannie Haggerty for their valuable and thoughtful comments on earlier drafts of this
manuscript.
i

t
ABSTRACT
This thesis comprises a review of studies on the diffusion of recommended
guidelines on preventive practices and three papers evaluating the preventive practke
patterns of general practitioners in Torino, Italy.
The first paper presents estimates of preventive practices and perceived
effectiveness of preventive interventions. Patterns of practice were found to be
consistently similar to those in other studies.
The second and third papers explore an array of determinants for ten primary
and secondary preventlve interventions.
An analysis of determinants indicates that complex patterns of behaviours are
rather condition-specifie, while the application of techniques is influenced to a varying
extent by organizational and attitudinal factors.
ii

c
Résumé
Cette thèse contient une rewe des études sur le niveau d'intégration
d'activités préventives dans la pratique clinique des médecins, ainsi que trois articles
traitant des pratiques préventives des généralistes à Turin.
Le premier article décrit les pratiques préventives des médecins et leur
perception de l'efficacité de certaines interventions. Nos résultats sont comparables
à ceux ra.pportés par d'autres chercheurs.
Les deuxième et troisième anicles examinent un ensemble de déterminants
pour dix interventions en prévention primaire et secondaire.
Une analyse des déterminants nous indique que les comportements de
pratique varient selon les entités cliniques et que l'utilisation de techniques données
est influencée par les attitudes des médecins et un ensemble de facteurs liés à
l'organisation de leur pratique.
iii

t
, . -~ (;
NOTICE
" The Candidate has the option, subject ta the approval of the Department,
of including as part of the thesis the tex! of an original paper, or papers, suitable for
submission ta learned joumals for publications. In this case, the thesis must still
conform to aIl other requirements explained in Guidelines Concemini Thesis
Preparation, (available at the Thesis Office).
Additional material (experimental and design data as weIl as descriptions of
equipment) must be provided in sufficient detail ta allow a clear and precise
judgement ta be made of the importance and originality of the research reported.
Abstract, full introduction and conclusion must be included, and where more than
one malluscript appears, connecting texts and common abstracts, introduction and
conclusion are required. A mere collection of manuscripts is not acceptable; nor
can reprints of published papers be accepted. "
iv
TABLE OF CONTENTS
Section
Acknowledgments ............................................. i
Abstract ••.•.....•••••..•••.•••.•.......••.•...•....••••...•...•• ii
R ... isumi ...........•......•..........•...............•..........• 111
N . • otlCe ..••••..••..•••••.•••••••••••.•••.••.••.•.••.•.• •••.••.•.••• IV
Table of Contents •......•.••........... 1" •••••••••••••••••••• v
Introouction .....•..•.•....••.•.......•.•...........•.•.....•...• 1
Literatl~re Review ••.......•..•...•..............•.......•...• 3
M ~thods of assessing practice patterns ....•.• 4
Primary preventive interventions ............... 6
Secondary preventive interventions ............ ll
Determinants of preventive practice .......... 13
The Health Care System in Italy ........................ 16
The Current Study ........................................... 0 19
References .........................................•........... 26
Tables ............................................................ 33
Paper 1 : "Preventive Practices of General
Practitioners in Torino, Italy"
Presentation .........•.....................• ,I ........ 39
Paper ..................•.......•.........•.....•........ 40
References ............•.......••..•.........•......... 52
Tables ..•...•..•..•••.••....•..•....•.•....•..•••....... 55
v
.11

Paper 2: "Determinants of Primary Preventive Practices
of General Practitioners in Tarino, Italy"
Presentation ....•........................•........... 63
Paper .......•......••••......•..............•........... M
References ......•.•.. Il •••••••••••••••••••••••• tt •••• 74
Tables ...•.•......••••....•.•.............••• ". " ...... 78
Paper 3: "Determinants of Cancer Barly Detection
Practices of General Practitioners in Torino,Italy"
Presentation ......•... It •••••••••••••••••••••••• 1, ••• 86
Paper ................. Il Il ••••• Il' tt •••••••• Il ••••••••• 87
References ••...•••••. tt. ft ••••••• , •••••••• Il .t' .. , ••• 96
Tables ..•.•••....••••••....•••.•.•••.....••...•.......• w Conclusion .................................................... 103
Appendix ....................................................... 107
vi
,
c
•
INTRODUCTION
The integration of preventive and curative approaches has become a standard
expectation for high quality health care. A key assumption is that the traditional clinical
encounter gives the physician an opportunity to promote health behaviours and to détect
disease early in its asymptomatic stage regardless of the primary reason for the
patient's visit (Easson, 1974; Frei, 1978; Smith, 1979).
From the 192O's l atil relatively recently, all patients weI e offered an
undifferentiated pack~ee of diagnostic procedures and laboratory tests as part of an
annual physical examination. This approach to annua! check-up was critically evaluated
during the 1970's (Frame, 1975) and was shown to be ineffective and mis!eading
because it neither reached appropriate groups at risk nor offered them techniques
proven to be effectivf'.
ln the late 1970's, Breslow and Somers (19n), the Institute of Medicine (IOM,
1978) and the Canadian Task Force on the Periodic Health Examination (1979)
proposed a new approach focused on preventable and serious diseases and on ~ubjects
who were at high risk for these diseases.
Three approaches were used to develop the new strategy.
The first approach was to differentiate primary from secondary prevention. The
object of primary prevention is to identify and modify risk factors in order to reduce
the likelihood of a disease or a disorder developing in a person wherl:as that for
secondary prevention is to identify the presence of disease in a pre-symptomatic stage
when effective therapies are available.
The second approach was to select conditions according to precise criteria of
social relevance, mortality, and morbidity and subsequently assess the effectiveness of
preventive interventions by examining the performance characteristics of early
detection procedures and the efficacy of early treatment.
Finally, effective preventive interventions were arplied to age- and sex-specific
risk groups to enhance the efficiency of the periodic health examination. This
innovative approach to preventive clinicat services bas now replaced the annual check
up as the standard procedure.
The V.S. Preventive Services Task Force, in collaboration with the Canadian Task
1

t
Force on PHE, refined and ~ùopted the above rules in the formulation of its own
recommendations for the integration of preventive interventions into clinical practice
(Goldbloom, 1986; Lawrence, 1987).
The National Institutes of Health (NIH) (Pink, 1984; Jacoby, 1985; Mullan, 1985; Perry, 1980) employed other methods reflecting their own particular concern~ and
perspectivf3 in the making of recomkoendations at "{',onsensus Conferences" ore:anized
by them; so have such other organizations as The American Academy of Pediatrics,
1978; The American College of Physicians, 1981; and The American Hospital
Associatirn, 1981. Problems arise, however, when conflictin~ recommendations for
practices are circulated among physicians.
The implementation of recommendations by physicians is determineti by such
factors as awareness of recommendations, practice structure, and medical training. A
study of these determinants is the subject of t}>js thesis.
The diffusion and implementation of recommendations have been studied mainly in
countries with a fee-for-service system, but their comparison with what happens
within a capitation system could generate new suggestions for increasing the use of
effective strategies in prevention.
These issues were examined in a survey of general practitioners in Torino,
Italy, that estimated the extent to which published guidelines on prevention were
included in GPs' practices within the Italian National Health Service. Associations
between physicians' practice behaviours and their attitudes, knowledge, lifestyles,
organizational models, and socio-demographic characteri5Hcs were a~.~0 investigated as
a means of idp'ltifying strategies for promoting eff~ctive interventions in clinical
practice.
2

c
LITERATURE REVIEW
This review is limited ta articles appearing in print after plJbIication of a set
of recommendations for systematic prev~ntion in primary car,: in the first report of
Th~ C~m~Jmn Task Forr.e on The Periodic Health Examina'~ion (1979). The
bibliographie seareh included M'2DLINE (key words: primary care, praetice
assessment, generai praetice, counselling, early detection), Index Medicus, recent
reviews by Lewis (1988), Bass (1988), and Green (1988), and the bibliographies of
selected articles.
Beca\lse sur.h studies are plagued by variations in subject matter, sampling
techniques, and the questialls posed, a section discussing the methods used in the
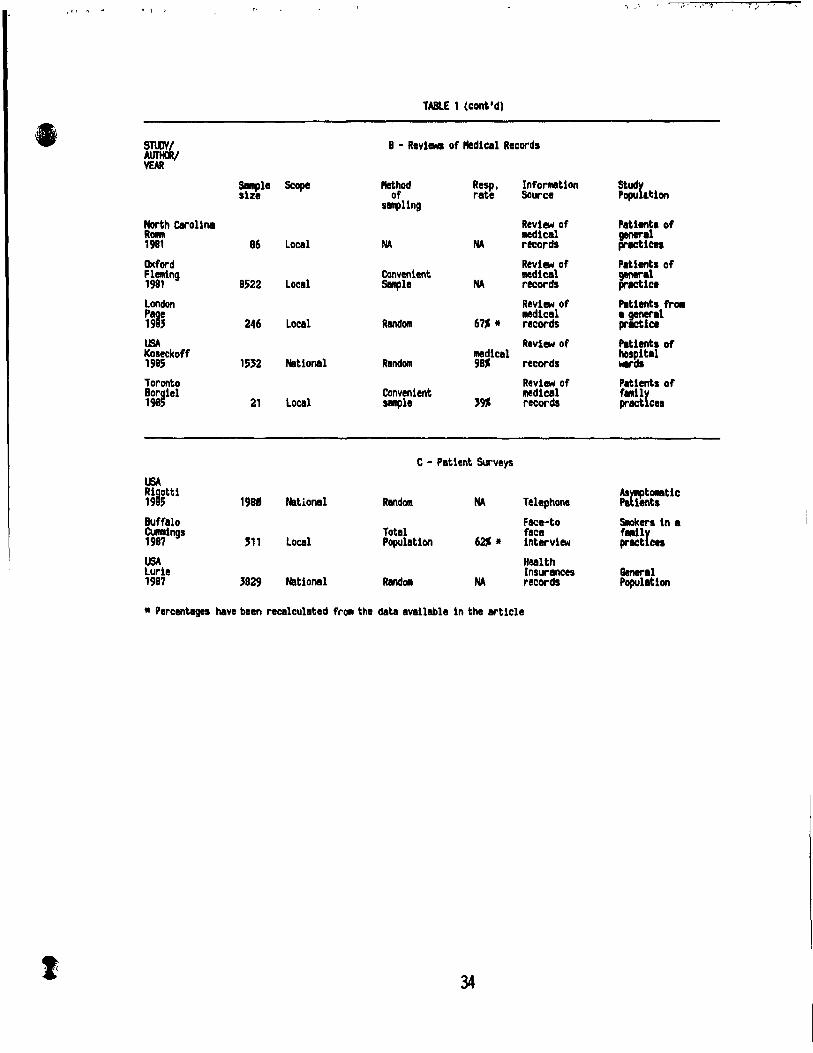
surveys !s inc1uded. Table 1 presents a sytlthesis of the survey methods used ill the
studres eonsidered in this literature review.
The lite rature on the preventive activities of primary care physicians can be
broadly divided inta descriptive articles about the i!nplementation of recommended
practices, and analytic articles concerning the deterrninants of their adoption.
The picture that emerges from this literature review is that the degree ta
which preventive mterventions are implemented varies within individua 1 l'ractices and
is influenced by a complex pattern of organizationai and attitudinal factors inc1uding
method of reimbur~~ment, availability of a given technique, appropriate knowledge
and training, and perceived effectiveness of tde intervention. Tables 2 and 3
summarize the frequencies of implementation of preventive activities in rifferent
studies.
3

1
l
Methods of assessing practice patterns.
The different approaches to ascertaining "what do physicians do about
prevention?" make it very difficult ta compare studies. Even the definition of
preventive practices varies among studies. While it is relatively simple to compare
practices such as "prescription of mammography", what anti-smoking counselling
entails is less clear.
Physicians' counse1ling procedures cover a wide range of activities. Most surveys
asked: "do you counsel patients about [target problem] ?It, but sorne used a proxy
question, such as "do you ask the patient about [target problem] ?" or Hdo you usually
bring up the issue of [target problem] with a11 patients ?" that implied life-style history
taking is the first step in counselling.
Sorne authors (Battista, 1983; Romm, 1981) addressed their questions ta specifie
recommended practices and focused on the type of clinical encounter during which
counselling is carried out and the type of patient groups targeted for the intervention.
Data were gathered by means of structured or semi-structured questionnaires
administered by mail, by telephone, or by trained interviewers during face-to-face
interviews. Most of the studies were local in scope, but sorne were province-wide
(Battista, 1983, 1985).
Physicians overestimate their preventive practices because they have difficulty
in recalling the exact procedure performed in each clinical situation and tend ta give the
desired response. Validation of their estimates is partially possible for reimbursed
procedures, but the reimbursement system seldom covers counselling interventions and
they are not always inc1uded in patient medical records.
Different recording procedures rnake it difficult to compare studies based on
medical records, particularly when physicians claim that the intervention was provided
although not recorded (Lewis, 1988).
Surveys in which patients are asked ta recall what their physicians did or said
provide indirect validation of preventive practices. Although such reports are also
subject to recall problerns, the answers give sorne indication of what the patient retains
frorn the doctor's intervention and are important in understanding the effect of
counsdling on patients (Lewis, 1988).
4

, "
Because several studies found that training and specialization influence
physicians' behaviours and attitudes towards prevention, modifications to continuing
education programs have been suggested. It must always be remembered, however, that
suggested interventions are not alwajs applicable in health systems that differ from
those in which the studies were conducted.
5

\ ' ,"'~'
Primary preventive interventions.
Anti-smoking counselling
Anti-smoking counselling involves giving individuals information about the
effects of smoking on their health and advising them to quit smoking. Counselling can
be supplemented by self-help mate rials and local community programs, but the most
effective strategy is to plan "support or reinforcement" visits during the first months
following cessation of smoking (Kottke, 1988). Recent recommendations issued by the
U.S. Preventive Services Task Force (1988) suggest that aIl patients who smoke,
regardless of the amount they smoke, be exposed to a variety of interventions delivered
by both physicians and other health professionals.
Physicians' consensus about the value of anti-smoking counselling is quite high,
and most physicians claim they provide it. The proportion of physicians reporting anti
smokirJg counselling ranges from 98~ in the Quebec study to a low of 52% in Lewis'
study (American Cancer Society, 1985; Battista, 1983, 1985; Gemson, 1986; Goldstein,
1987; Lewis, 1986; McAlister, 1985; Orleans, 1985; Radecki 1986; Rosen, 1984; Valente,
1986; Wechsler, 1983; Wells, 1984). Similar results wcre found in studies done in
lreland and England where primary care structures differ (Catford, 1984; Daly, 1980).
Other studies showed that 41% of aIl smokers (Cummings, 1987), and 42% of
male smokers to 48% of female smokers (Rigotti, 1985) recalled being counselled by
their physicians. Rates of anti-smoking counselling recorded on medical charts were
61% (Mandel, 1982); 63% (Kosecoff, 1985); and 56 to 72%, depending on patient age,
(Romm, 1981).
Few studies have considered the types of clinical encounter in which counselling
was offered, or whether advice was offered, according to the published guidelines, to
aIl smokers; to "heavy" smokers; or only to smokers with symptoms attributable to
smoking (Battista, 1983, 1985; Wells, 1986). Generally speaking, anti-smoking
counselling is offered more frequently to heavy smokers and to patients with health
problems related to smoking. This finding implies sorne difficulties in fully
implementing the recommendation that counselling be offered to each smoker
regardless of quantity smoked or health status.
Internists and residency-trained family physicians seem to offer anti-smoking
6

; ,1 1.,1.1,_
counselling more frequently than general practitioners do (Attarian, 1987; McAlister,
1985; Valente, 1986; Wechsler, 1983). Physicians who specialize in organ systems
adversely affected by smoking ( i.e. cardiologists, pulmonary specialists and
nephrologists) counsel more than do their colleagues in other specialties (Wells, 1986).
The Wessex study (Catford, 1984), which included an examination of the role of
other professionals, found that 57% of the general practitioners studied thought
counselling about smoking was a responsibility they shared with health yisitors who
provide and support health promotion (Fry, 1986); 65% thought it was a responsibility
they shared with health education officers, whose introduction into the Community Care
Services in Great Britain was intended to reduce length of stay in hospital and to
manage more patients in the community.
A few studies looked at physicians' personal smoking behaviours and found a
negative association between smoking by practitioners and their anti-smoking
counselling practice ( Lewis, 1986; McAlister, 1985;
Maheux, 1987). In a study of physicians' habits and attitudes in Pordenone, Italy, 64% of
current smokers versus 74% of non-smokers and 80% of ex-smokers provided anti
smoking advice to their patients (Franceschi, 1986).
Despite the high importance rating given by physicians to anti-smoking
counselling, only a small minority (3% in Wechsler, 4% in Valente, 12% in Wells and
30% in Goldstein) believe their counselling is effective. This perception of low
effectiveness is corroborSlted by a recent meta-analysis of 39 controlled trials on
smoking cessation interventions. The average success rates for counselling were
13.1% after 6 months, and 3.8% after one year (Kottke, 1988).
~1cohol-abuse counselling
The primary problem in counselling those who abuse alcohol is distinguishing
between prevention of alcoholism and prevention of the long term effeets of a
high/moderate daily alcohol intake (mainly chronic liver damage). While the first
aspect is quite straightforward, no clear recommendations are available as to what
daily intake of alcohol is considered safe, although an intake of two drinks a day is
generally regarded as harmless.
Recommendations for detection and treatment of problem drinking consider
7
.. ). ,

" -
active case finding followed by counselling to reduce alcohol consumption. Interviews,
questionnaire, biomarkers or presence of clinical signs can help physicians in detecting
problem drinking; although no single instruments has shown optimal accuracy,
approaches may be combined sequentially to increase either sensibility or specificity.
There is also good evidence that counselling and monitoring of progress reduce the
amount of alcohol consumed (Canadian Task Force on PHE, 1989).
The proportion of physicians who advise against excessive alcohol intake varies
from 94% in one study (Gems:)n, 1986) to 34% in the INSURE Project, a 3-year
feasibility study to develop and test a clinical model of preventive health services in
primary care, including patient education, as a form of insu rance bene fit (Rosen,
1981). Onlya small minority (3% in Valente), however, viewed their counselling
activities as being effective. Again, internists offer advice egainst alcohol abuse more
often than general practitioners do (Wechsler, 1983).
Validation of results by surveys of patients' health practices showed that 9% of
men and 6% of women who consumed >3 drinks/day had been counselled hy their
physicians (Rigotti, 1985). Medical chart reviews found that data on alcohol
consumptinn were recorded for on1y 18% of patients in one study (Mandel, 1982) and
47% in another (Romm, 1981). Data from a study of the medical records of North
Carolina physicians showed a 57% to 41% compliance with recommendations for alcohol
abuse counselling, depending on patient age groups (Romm, 1981).
Accidents in the home among the elderly
The first ~eport of the Canadian Task Force (1979) stated "An important
proportion of accidents occur at home, where young children and the elderly are
particularly at risk" and recommended "the use of PHE's scheduled for other
purposes to encourage safety in the home and the community". The Report gave no
suggestions about specifie techniques or approaches physicians could use in encouraging
safety in the home.
More recently, sorne authors have proposed a more complex approach and have
suggested precise maneuvers physicians may perform du ring visits. This approach
encompasses a careful history taking about medication and substances affecting balance
8
(
.... i.,
(Kennedy, 1987), a clinical test for early detection of balance impairment (Wolfson,
1985), and a check list for assessing environmental hazards (Tideiksaar, 1986), but
there have been no controlled trials to evaluate the efficacy of such interventions.
Influenza vaccination for the elderly
Studies have demonstrated the efficacy of influenza vaccination for high risk
groups (LaForee, 1987: Recommendation of the Public Health Service Advisory
Committee on influenza practice, 1977; Williams, 1973), and the maneuver has been
included in the Periodic Health Examination, annually, for persans over 65 years of
age.
In New York City (Gemson, 1986), physicians c1aim they offer influenza
vaccine to 68% of their patients over 65. The same study also investigated the
acceptance of a recommendation for a general package of five immunizations published
in the American College of Physicians' "Guide for adult immunization" (1985). The
package included an annual influeIl2.a vaccination for patients over 65; a periodic tetanus
vaccination for aIl patients; and pneumococcal vaccination for elderly 1 chronically m, immuno-suppressed, and asplenic patients. The results showed that younger and board
certified physicians were more likely to agree with these recommendations.
Reviews of medical charts have shown that compliance with recommendations
varies from a low of 3% to 8% (Cohen, 1982; Dietrich, 1984; Lurie, 1987), to a high of
30% (Kosecoff, 1985).
Prevention of unwanted pregnancies
Recommendations for the prevention of unwanted pregnancies cite good evidence
for the effectiveness of contraceptive eounselling in the prevention of second
pregnancies, but there is less evidence for the effectiveness of counselling in
preventing first pregnancies (Canadian Task Force on PHE, 1979, 1988). Th~ impact
of physicians' counselling in reducing unwanted pregnancy rates has not been
demonstrated, but there is sorne evidence that primary health care providers, through
teaching, counselling, and providing contraceptive agents, May be successful in
increasing the level of knowledge, the use of contraceptives, and the postponement of
first intercourse in adolescents (Forrest, 1981; Zabin, 1986).
9

Physicians usually provide information on contraception to prev~nt unwanted
pregnancies. North Carolina physicians recorded offering advice on contraception in
23% of the m~dical records examined (Romm, 1981). In the INSURE project,
approximately 30% of physicians "usually bring this subject up for aIl patients" and 53%
"only for high-risk patients" (Rosen, 1984).
In a patients' survey carried out in a North London practice, where a preventhoe
package of five interventions was offered to women 17-30 years of age, a review of
medical records showed that 86% of the women were counselled on contraception in the
first year and 91% in the second (Page, 1983).
10
(
Lung cancer
Secondary preventive interventions.
- early detection of cancer -
Chest x-ray and sputum cytology are the current screening procedures for lung
cancer. Neither has been declared suitable for inclusion in periodic health examinations
by the Canadian Task Force on The Periodic Health Exan".nation, the U.S. Preventive
Services Task Force or The American Cancer Society.
Nevertheless, the number of physicians ordering chest x-rays for this purpose
ranges from 42% in The American Cancer Society study (1985) to 71% in the Quebec -
New Brunswick study (Battista, 1983, 1985). Internists tend to use chest x-ray more
often than general practitioners - possibly because they see more symptomatic patients
(American Cancer Society, 1985).
Physicians order sputum cytology less frequently; the reported rates vary from
19% of physicians in New York (Gemson, 1986) to 41% in Quebec (Battista, 1983).
Breast cancer
Annual mammography has been widely recommended as an effective early
diagnostic procedure for women 50 years of age and older, but the effectiveness of
mammography for women between 40 and 49 is questionable. The proportion of
physicians recommending mammography for asymptomatic women 50 years of age and
over ranges between 3% (New Brunswick study) and 42% (American Cancer Society,
1985; Albant.s, 1988; Basset, 1986; Battista, 1983, 1985; Cummings, 1983; Gemson,
1986). The low rate in New Brunswick could be due to the scarcity of radiology
centers rather than a negative physician attitude.
Gynecologists reported the regular use of mammography for early detection of
breast cancer in women 50 and over more often than other physicians (American
Cancer Society, 1985; Albanes, 1988).
Radiation hazard (Gemson, 1986) and expensiveness (American Cancer Society,
1985) were the reasons most commonly given for not recommending mammography .
Breast self-examination (BSE) is still controversial and is not included in the
Canadian and U.S. Task Forces' guidelines (Canadian Task Force on PHE, 1986; US
11

Preventive Services Task Force, 1987) although The American Cancer Society (1980)
recommends its performance, monthly, by women over 20. Almost ail physicians in
Quebec (96%) and New Brunswick (m) reported teaching BSE whereas only 48% of
physicians in New York City and 41% of those in the INSURE project adhere to The
American Cancer Society's recommendations.
Cervical cancer
The Papanicolaou smear is a well accepted practice, but there is continuing
discussion about its most effective frequency of use and who is at high risk.
Compliance with the recommendation for its use as an early detection maneuver varies
from 75% in the American Cancer Society study to 92% in the New York City study.
Reviews of medical charts reveal that the procedure was performed for 68% of
patients aged 30 to 39 years (Ro:Dm, 1981).
When types of clinical encounter are considered, orny 52% of physicians in
Quebec perform pap smears du ring visits for non-gynecological problems. Apparently,
a significant number of physicians still use pap smears more often in symptomatic than
asymptomatic patients.
Gynecologists prescribe pap tests more often than general practitioners and
internists; so do female and salaried physicians compared with male and fee-for
service practitioners (Battista, 1983). If only fee-for-service physicians are
considered, higher rates of pap test prescription are associated with better knowledge
and younger age of physicians (Battista, 1986).
12
· :..

Determinants of preventive practice
General conceptual frameworks for the determinants of preventive practices are
being developed (Battista 1986; Green, 1988; Lewis, 1986; Wells 1984).
Green suggests the use of three categories of determinants: predisposing, enabling,
and reinforcing factors. Predisposing factors induce physicians to take action and
inc1ude knowledge, beliefs, and skills. Enabling factors, such as type of
reimbursernent, incentives for preventive activities, availability of techniques and the
means of applying them, favour the introduction of new practice behaviours by
motivated physicians. Reinforcing factors, such as visibility of results, peer support
from colleagues and feed-back from patients, help to sustain new practice behaviours.
Although this classification is stimulating and interesting, the determinants are
not mutually independent and are difficult to put into operational terms.
Physicians' confidence in the effectiveness of an intervention, and their
"perceived self-efficacy" exert significant influences on their behaviour.
Although clinical training and continuing education are important in the diffusion
of preventive practices, the effectiveness of con!inuing medical education prograrns in
changing current practices is controversial (Haynes, 1984; Lomas, 1988). The impact
of training and specific educational programs in improving physicians' performance is
evident in such specialities as family and internaI medicine where better training in
disease prevention is associated with higher rates of use of preventive practices
compared with other speciaities (Attarian, 1987; Dietrich, 1984; Kosecoff, 1985; McPhee, 1986; Radecki, 1986; Wells, 1986; Woo, 1985).
Perceived effectiveness and clinical training are related to what physicians
actually know about the scientific rationale for preventive interventions. Sorne studies
have measured the association between knowledge and practice (Battista 1986), and
have found that it varies across diseases and interventions.
,.i W
Other "limiting factors" or "barrier~" can be grouped into physician-, patient-,
and system-related barriers (Battista, 1986). Time constraints and lack of
inclmtives/reimbursement are physician-re!ated barriers while low compliance,
accl~ssibility to primary care services, and patients' time constraints are patient
re]ated barriers. System-related barriers range from scarcity of resources and the
13
1
availability of a technique under a health insu rance plan to the existence of competing
services offering similar preventive interventions.
Motivation to counsel, perceived risk of smoking, physicians' skill in
counselling, ar.d perceived associated costs and benefits of counselling have been
aggregated in tht. general category of "attitude" and measured as sub-scales of the
"Multi-items Att~tude Scale" tested by Wells et al (1984) for anti-smoking counselling.
This scale has also been used (Lewis et al, 1986) to evaluate smoking and alcohol
abuse counselling, weight control, and exercise promotion. Perceived importance of
preventive practice, physicians' skill, and barriers (costs) were shown to play
differing roles in determining counselling behaviours. The most pervasive
determinants for the majority of counselling and health promotion interventions
appeared to be the physicians' specialties and personal preventive behaviours. Thi!.'
finding bas been ::onfirmed in a study by Maheux (1987) in which physicians' personal
health practices and role model orientation accounted for most of the variation in their
preventive practice behaviours.
Female physicians seem to be more oriented toward prevention, particularly for
gynaecologic cancer and contraception. Sorne authors 5uggest that this may be
attributable to a better doctor-patient relationship for female physicians (Gray, 1982;
Hopkins, 1967; Preston-Whyte, 1983). Gender disapp,~ars as a determinant of
preventive practice behaviours, however, when it is considered in conjunction with
other factors (Maheux, 1987).
Mode of reimbursement has been considered one of the important factors
"facilitating" physicians' preventive practices and various types of health insu rance
plans have been studied with different results (Contandriopoulos, 1980; Lurie, 1987;
McPhee, 1987; Manning, 1984; Pineault, 1976; Rice, 1983). In general, salaried
physicians are more prevention-oriented than fee-for-service physicians (Battista,
1986), but physicians paid on a capitation basis, as in the United Kingdom. are not
(Fleming 1981).
A major problem in evaluating the findings on determinants of preventive and
clinical practice arises when the complex mechanisms of interaction among the
attitudes, characteristics, and practice settings of physicians are considered. Type of
reimbursement has been cited as a main modifying factor in physicians' attitude and
14
.. ; , - ";:--"

c.
, .- "-:r ". '
practices (Battista, 1986). Exploring how determinants are causally linked in a
capitation system, such as that in Italy, is a useful complement to previous analyses.
The picture that emerges from this literature review is that preventive
behavio~rs follow complex patterns and are rather condition-specifie. No group of
systematically adopted interventions is recognizable. Instead, the application of
techniques is influenced by complex and differing patterns of such organizational and
attitudinal factors as method of reimbursement, availability of given techniques,
appropriate knowledge and training, and perceived effectiveness of an intervention: the
adoption of each intervention is made independently from the adoption of similarly
recommended interventions for other conditions.
15
1 ,~ \ i"

THB HEALTH CARE SYSTEM IN IT ALY
Although the National Health Service (tlServizio Sanitario Nazionale -SSN~) in
Italy was only founded in 1978 (Legge 833), health insurance (tlCasse Sociali per
malattiatl ) bas been in existence since 1919 and has been controlled by government since
1966. AIl workers and their families were enroled in health insu rance plans based on
the worker's type of activity, and special plans \Vere provided to the unemployed.
Trade unions participated in the administration of these plans. Although the system
covered the whole ltalian popuiation, persistent inequalities in services and public
concern, during the 1970's, triggered a movement that led to the creation of the SSN and
the enactment of laws concerning prevention.
In 1978, a law was also enacted for the prevention of unwanted pregnancied
("Legy,e per la procreazione responsabile lt). It allowed legal abortior. and led to the
creation of services (tlconsHltori") tailored to preventive activities in family planning,
gynaecological disorders and sexual counselling. Further evidence of a broadening of
the concept of health and an increasing emphasis on health education and promotion is
provided by landmark environmentallegislation during the 1970's.
Until the early 1980's, health promotion stategy relied primarily on mass campaigns
and advertisements, but criticisms of this approach (Morosini, 1984), prompted mainly
by its failure to reach social groups with the greatest needs, led to its reexamination.
The organization of the Italian SSN is based on Lccal Health Authoriti~s
("Unita' Sanitaria Locale" - USL-) whose boards are elected by municipalities. Each
USL provides health services for 50,000 to 200,000 inhabitants and is administered by
the Local Health Authority in accord with national and regional policies. The
administrative resources of USLs are provided, through the Regional Councils, by tl:e
central government according to demographic indicators (population size and
proportions of people in specifie age groups), previous year's budgets, the inflation
rate, and specifie interventions required by the local authorities. The Regional
Councils distribute the funds among the USLs, which are eharged with achieving the
goals defined by central and regional eouncils. AlI public hospital care, family
medicine (encompassing general and paediatric practiee), public health, occupational
medicine, and environmental control faU within the jurisdiction of the USL. Social
16

(
Services, such as home care, bousekeeping help, and "meals on wheelstt for elderly and
disabled people are supported directIy by the municipality which coordinates these
activities with USL administrators.
General practitioneI sare entitled ta provide free and accessible primary care
and ta aet as "gatekeepers" ta specialized and hospital care. Patients who go directly
to specialists have ta pay for their services, themselves. Few exceptions are made ta
this rule since patients may go directly to vaccination centers and clinics ("consultoritt)
specializing in famiiy planning, gynecological disorders and sexual counselling.
Everyone over 14 years of age is enroled in the GP rosters: those under 14 are
enroled in the pediatrician rasters. Before the institution of the SSN, GPs were
allowed any number of patients: subsequent ta its creation, they were invited to reduce
the number, gradually, to an upper limit of 1500. This rule has not been strictly
enforced and a small minority of GPs exceed the limit, slightly. GPs can undertake
other activities within the SSN, provided the number of patients they have is reduced in
accordance with the amount of working professional time they de vote to sueh activities.
GPs are paid on a capitation basis and are limited to a maximum Dumber of
patients according ta the mix of professional activities they engage in, such as hospital
appointments, emergeJlcy wards, and private activity. They run their own practices,
but the sharing of office facilities, nurses, and receptionists' services is inereasingly
common. GPs are responsible for providing, equipping and staffing their practices
from their capitation payments.
Any physician with a degree recognized I~: ille Italian Ministry of Education (i.e.
from a11 Italian Universities and, recently, frOl:' aIl universities of the European
Community Countries - after a language test), can apply for registration on the rosters
of a USL.
As the result of a discussion of the preventive role of GPs in Italy, a generic
statement about the health promotion and preventive activities to be provided by the GPs
was included in the 1985 Contract ("Convenzione per la Medicina Generale") signed by
the Government and the Physicians' Professional Organizations. Despite this
statement, no concrete action for inc1uding precise interventions or maneuvers in
clinical practice has been endorsed.
The Qnly training in prevention received by physicians, in medical sehool, is a
17

course on bygiene, propbylaxis and prevention; no special programs in family medicine
are offered. Physicians who want to specialize in family medicine take a three-year
degree in bygiene and community medicine. A proposaI to reorganize medical school
programs to meet the standards set by the European Corn munit y and the new challenges
ot the Health Reform is being considered by Parliament. It would introduce specifie
courses in medical schools and a four-year degree in corn munit y medicine.
The growing interest among Italian physicians in a more active role in promoting
patient bealth bas become apparent in sorne surveys (ArdigcS, 1982; Piperno, 1980).
The opportunity to introduce a strategy similar to the Periodic Health Examination is
evident in the high annual rate of patient visits, given that about 80% of the practice
population see their GPs once a year (ISTAT, 1980,1983), and sorne authors recognize
this as a favourable premise for the diffusion of preventive interventions by GPs
(Coen, 1983).
Unfortunately, GPs are often more willing to refer their patients to vaccination
centers, "consultori", and tuberculosis prevention services provided within the USL
than they are to carry out the interventions themselves. From a public policy pomt of
view, offering the same maneuver from different points within the same health
organization, with the attendant danger of duplication, may incur significant but
unnecessary costs. Proceeding further in the development of preventive services
separate from primary care, would ooly increase the costs, complexity, and
coordination difficulties of the system.
These problems and increasing concern about costs and monetary constraints
have recently led to a reconsideration of health reform in Italy. The need for a better
understanding of the effectiveness of interventions, the efficiency of proposed
organizational solutions, and the diffusion of innovations among health professionals,
has convinced authorities to fund researcb in primary care. The work reported in this
thesis was undertaken in the context of this new interest in prevention.
18

c
(
THE CURRBNT STUDY
Objectives and justification of the study
Since most reported studies of the diffusion and "penetration" of preventive
practices among physicians were conducted in countries with a fee-for-service or
mixed fee-for-service/salary system, exploring and comparing practice behaviours in a
capitation system could be very enlightening. Since no official recommendations
and guidelines have been published by an Italian organization, the focus of the study was
to estimate the extent to which Italian GPs offer a broad range of preventive
interventions. C\
We also asked questions about specifie preventive strategies addressed locally by
the USL of Torino (the study site), including social services for the elderly, prevention
of disability, and reaction to the introduction of laws making the use of car seat belts
and motorbike crash helmets mandatory
Questions on determinants were selected and included on the basis of results in
other studies. Organizational factors related to the work environment, as cited by
most authors, supplemented by those typical of primary care in Italy, were also
examined.
In addition, we gathered information on preventive interventions having a
potential effect on morbidity and mortality in Italy (Costa, 1984; Rosso, 1984), including
interventions for the elderly and prevention of unwanted pregnancies, sinee they were
targeted by the new social services introduced by the USL and municipality of Torino.
19

j , . "
Specifie aims and research questions
The goal of this research was to answer the following questions:
1) How Many GPs in Torino perform/offer counselling for the following
preventive interventions:
- smoking cessation;
- anti-alcohol abuse;
- accident reduction at home among the elderly;
- flu vaccination for patients over 65 years of age;
- contraception;
- weight control;
- physical exercise;
- oral hygiene;
- the use of crash helmets by motorbikers and seat belts by car
drivers and passengers;
- early detection of lung cancer (chest x-rays and sputum cytology);
- early detection of breast cancer (physical examination, mammography
and breast self- examination);
- early detection of cervical cancer (Papanicolaou smear).
2) How much confidence do the physicians have in the ability of these interventions
to reach the proposed goals?
3) How much agreement is there with the published guidelines of optimal practice?
4) What are the factors influencing physicians' preventive behaviours?
5) How do the organizational features of primary care in Italy affect practice
patterns?
6) Relative to the adequacy of explanatory models emerging from our analyses,
what initiatives can he undertaken to improve physicians' performances.
Sampling Method
The reference population cOl1sisted of physicians who provide primary care. In
the Italian Health Service, this definition includes physicians enroled in the roster of
General and Paediatric practice in each USL. Physicians who offer primary care
exclusively on a private basis outside the SSN form a minority (about 10%) which was
20

,
(
excluded because of problems of accessibility and confidentiality of information.
Pediatricians were excluded because their preventive practices were the subject of a
separate study.
A systematic sample of full- and part-time GPs was drawn from the GP file of
the USL of Torino, after the file had been stratified by sex, age, and maximum number
of patients. Age and sex were selected as variables for stratification since they had
been shown to influence preventive practice behaviours of physicians in other studies
(Battista, 1986; Lurie, 1987; Maheux, 1987). We assumed that practjce size (number of
patients) could affect the amount of time spent by physicians in updating, collaborating
with colleagues, and gaining professional experience in other services.
In May 1986, we systematically selected 1 out of every 5 physicians to obtain a
sample of 225 from 1158 GPs that was proportionate by age, sex, and practice size.
Development of the Survey instrument: Questionnaire
We chose to administer a structured questionnaire during face-to-face
interviews, primar-ily because of the higher response rates achieved with this method in
other studies (Table 1). Other survey techniques were excluded because
confidentiality precluded the use of medical records and a patient survey would be too
expensive.
Ta develop our questionnaire, we first reviewed others used for estimating the
attitudes, knowledge and behaviours of physicians. Most studies asked questions on
limited aspects of practices and their perceived effectiveness; only the Quebec study by
Battista et al. (1983) offered a complete framework for addressing the factors of
interest. Battista's survey was limited to the early detection of four types of cancer,
but its precision made it possible to detect discrepancies from recommended guidelines
based on type and frequency of clinical encounter, and targeted population.
Accordingly, we selected items of interest from the Quebec and New Brunswick
studies and added the interventions ta be used in our survey following the same scheme.
Ta make each interviewas brief as possible, we gathered such information as
address, time-table of patients' visits, practice size, year of graduation, and age from
USL sources. Two general practitioners, who were not included in the sample, helped
us during the formulation of questionnaire items.
21

A pretest, conducted on 10 volunteers not inc1uded in the final sample, enabled us
to optimize subsequent response by: 1) informing physicians that the study was
sponsored by the Physicians' Federation and the USL of Torino within initiatives for
continuing education; 2) guaranteeing the personal involvement of the project director
for soli citation procedures; and 3) allowing the physicians to decide the time and place
for the interview.
The final version of the questiorinaire was sent to officiaIs of the USL of
Torino and the local chapter of the Physicians' Federation (Ordine dei Medici della
Provincia di Torino) for their approval. They granted it without change.
Questionnaire Structure
The first of the questionnaire's nine sections dealt with the management of the
practice. The next seven sections eovered interventions for lung cancer; alcohol
abuse; hypertension; cervical and breast cancer; prevention of disability among the
elderly; prevention of traffie accidents; and unwanted pregnancies. The last section
dealt with the physician's lifestyle - e.g. smoking habits.
Practice behaviors were assessed with questions about the frequency of adoption
of a given intervention scaled on four levels - "Do you adopt this intervention always,
often, seldom, never?" When recommended guidelines suggested such precise patterns
of praetice as frequency of intervention and targeted population, we inc1uded them.
Because we wanted to understand the determina~ts of physicians' practices, we
tried to uncover their attitudes towards prevention with questions on knowledge and
attitudes. Knowledge about prevention was measured by asking physicians to score the
evidenee of association between risk factors and diseases for smoking, alcohol abuse,
and breast and cervical cancer on a four level scale - strong, fair, poor, or no
evidence. Table 4lists the items for each issue. Physicians were also asked to grade
the perceived effectiveness of interventions on a four level seale - very, rather,
somewhat, or never effective.
A list of factors that could hamper the offering of anti-smoking and anti-alcohol
abuse counselling was also presented to physicians with a request that they indicate,
for each item, whether they considered the barriers to be important limiting elements.
22
-

,~. 3! i))iL ,',' '\', }Ji \ 1 t. "
The list includes: lack of training, time constraints for the physician, time constraints
for the patient, lack of monetary incentives, difficult access to the technique,
availability of the technique, lack of reimbursement, and poor compliance from
patients.
In Ita] y , other primary care services offer preventive interventions and patients
have access to them directly, or through their GPs. Physlcians were asked whether
they refer thelr patients to the available centers in the community or carry out
interventions personally, e.g. for flu vaccination in the elderly or contraception advice.
We also asked GPs to rate their satisfaction with the referral services and with
consultant physicians on a four level scale - excellent, good, fair, or poor.
Field work
Interviewers were trained, for the specifie task, before and during the pilot
phase. The training included interview scheduling, making appointments, dealing with
refusais, presenting the questionnaire, and face-to-face interview techniques. Three
interviewers administ(~red the questionnaire to random subsamples of physicians.
A letter introducing the study was sent to each physician two weeks before an
interviewer telephoned to make an interview appointment. Physicians who requested
more information, or declined, were contacted personally by the project director in
order to maximize participation.
Questions missed by interviewers, and mistakes, were identified by a day-by
day checY. of the completed questionnaires. The research assistant contacted the
physicians from whom additional information was needed.
The questionnaires were then sent for key-punching, the entry of data into the
computer, and checking for logical-formal errors (impossible, or out of range values)
and completeness by editing programs.
Most questions were coded using a system that differentiated between "don't
know", "don't remember", and "refuse to answer" categories.
Scale construction
The scales we devised for practice behaviours and their determinants were
analyzed by multtvariate statistical techniques. The questions used to construct the
23

various sC,ales are described below, for each variable studied.
Outcome variables
Patterns of counselling for ,smoking and alcohol abuse were identified by the
type of clinical encounter in which it was done (first visit, periodic check-up, or visit
for symptoms unrelated to the risk factor); frequency (always, often, seldom or
never); and patients targeted (ail patients at risk, at high risk, or only those with
symptoms). An overall score was computed for each type of counselling. The highest
score coincided with the recommended guidelines (aIl smokers during visits for
symptoms not related to the risk factor, and advice repeated more than once).
Adoption of early detection techniques for lung and cervical cancer was assessed
by type of clinical encounter; criteria for defining risk groups (family history, age,
lifestyle); frequency of intervention (once a year, every two years etc.); and follow
up. The highest score indicated compliance with the recommended guidelines.
Mammography and breast examination were to be performed yearly for v!omen aged 50 to S9 years; breast self-examination yearly for women 40 and over.
Che st x-rays and sputum cytology were included, although tlley are not
recommended as early detection techniques. Their scales had bimodal distributions and
were dichotomized.
Scales for measuring adoption of counselling on accident prevention at home
among the elderly, flu vaccination for the elderly, and contraception were based on a
four-level item and were diehotomized for analysis.
Independent variables
Knowledge indexes for smoking, aleohol, cervical and breast cancers were
computed by assigning a positive score for every right answer, and summing positive
scores for each topic. This procedure led to four knowledge indexes. Table 4
displays the criteria used in judging the appro!,riateness of answers.
Seales of barriers to anti-smoking and anti-alcohol abuse cJunselling were
~omputed by summing the barriers considered important by physicians, after chee king
Cronbach's alpha.
In data reduction, "don't know" and "don't remember" (,'ite~ories were assigned
24
(
(
the lowest value (usually zero). While this is appropriate for knowledge indexes,
because it represents a failure in knowledge as well as a wrong answer, it is
questionable for belief scales, since it would indicate a mid- or uncertainty point. In the analysis, we found that the preventive behaviour of physicians in !his category (low
score) was similar to that of physicians with the lowest belief score. We dècided,
therefore, to recode the "don't know" category as low score.
Response rate
We experienced only 16 refusaIs (7.1%). The remaining GPs participated with
great enthusia&îO and without declining to answer any questionnaire items.
Control of information bias
To check the possibility that information bias was introduced by interviewers,
we computed the expected frequencies of answers, by interviewer, from the total
marginal distributions of selected items. Observed-expected difference was tested
with a chi-square statistic. No statistically significant differences among response
patterns by interviewers were detected.
Because the capitation system in Italy does not require recording of the clinicat
encounter and applied interventions, we were unable to validate estimates of practice
patterns given by physicians (probably biased in the direction of overestimation) from
administrative data. The introduction of information bias by physicians waSt
therefore, a possibility.
25
1.
REFERENCES Albanes D, Weinberg GB, Boss L, Taylor PRo A survey of physician's
breast cancer early detection practices. Prev Med 1988;17:643-652.
2. American Academy of Paediatrics, Committee on Stand.ards of Child Health
Care: State of continuity of pediatrie care. Evanston IL: AAP, 1978.
3. American College of Physicians, Medical Practice Committee: Periodic Health
Examination: a guide for designing individualized preventive health eare in the
asymptomatic patient. Ann Intern Med 1981;95:729-732.
4. American CoUege of Physicians, Committee on immunization. Guide for adult
immunization 1985. Philadelphia: American College of Physicians 1985.
5. American Cancer Society. Guidelines for the cancer-related checkup:
recommendations and rational. CA 1980;30:193-240.
6. American Cancer Society. Survey of Physicians' Attitudes and Practices in
Early Cancer Detection. CA. 1985;35(4):197-213.
7. American Hospital Association. AHA Guide to Health Care Field. Chicago,
Illinois: AHA, 1981.
8. Ardigo' A, Barbano F. Medici e socio-sanitari: professioni in transizione.
Angeli, Milano 1982.
9. Attarian L, Fleming M, Barron P, Strecher V. A Comparison of Health
Promotion Practices of General Practitioners and Residency Trained Family
Physicians. 1 Comm Health 1987;12(1):31-39.
10. Bass Ml, Elford RW. Preventive practice patterns of Canadian Primary Care
Physicians. In Battista RN, Lawrence RS, eds. Implementing Preventive
Services. Am 1 Prev Med 1988;4(4)s:17-23.
11. Basset LW, Bunnel DH, Cerny lA, Gold RH. Screening Mammography: Referral
practices of Los Angeles physicians. AJR 1986;147:689-692.
12. Battista RN. Adult cancer prevention in primary care: patterns of practice in
Quibec. Am J Public Health 1983;73(9):1036-1039.
13. Battista RN. Palmer CS, Marchand BM, Spitzer WO. Patterns of preVt"": .<~
practice in New Brunswick. Cao Med Assoc 1 1985;132:1013-10l5.
14. Battista RN, Williams U, MacFarlane LA. Determinants of Primary Medical
Practice in Adult Cancer Prevention. Med Care 1986;24(3):216-224.
26

(
" ,
15. Breslow L, Somers AR. The lifetime health-monitoring program: a practical
approach to preventive medicine. N Bngl j Med 1m;2%:601-608.
.'- i.il
16. Canadian Task Force on the Periodic Health Examination. The periodic health
examination. Can Med Assoc J 1979;121:1193-1254. 17. Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1984 update. Can Med Assoc J 1984;130:1278-1292.
18. Canadian Task Force on the Periodic Health Examination. The periodic he:dth
examination: 2. 1985 update. Can Med Assoc J 1986;134:724-729. 19. Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1987 update. Can Med Assoc J 1988;138:618-626. 20. Canadian Task Force on the Periodic Heaith Examination. The periodic health
examination: 2. 1989 update. Can Med Assac J 1989;141:209-216.
21. Catford jC, Nutbeam D. Prevention in practice: what Wessex General
Practitioners are doing. Br Med J 1984;288:832-834. 22. Coen D. La Prevenzione: promesse, possibilita (ma anche) illusioni.11 Medico
D'Italia 1983;40:14.
23. Cohen DI, Littemberg B, Wetzel C, et al. Improving patients' compliance with
preventive medicine guidelines. Medical Care 1982;20:1040-1045.
24. Contandriopoulos AP. Stimulants 'conomiques et utilisation des services
midicaux. Act Econ 1980;56:264.
25. Costa G, Colombo A, Zanetti R, D'Ambrosio R, Rosso S, Ponti A, Segnan N.
26.
27.
28.
Stato di salute della popolazione a Torino: cause di morte nei residenti - anno
1982 -. Unita' Sanitaria Locale 1/23 Torino. Torino 1984. Cummings KM, Funch DP, Mettlin C, jennings E. Family Physicians' Beliefs
about Breast Cancer Screening by Mammography. j Fam Pract 1983:17(6):1029-
1034. Cummings KM, Giovino G, Sciaudra R, Koenisgsberg M, Emont SL. Physician
advice ta quit smoking. Who gets it and who doesn't? Am J Prev Med 1987;3:69-
75. Daly LE, Bourke G, Herity B, Hickey N. Horgan jM. General Practitioners'
Attitudes ta Aspects of Preventive Medicine. J Irish Med Ass 1980;73(7):260-
264.
27
'B. Dietrich Aj, Goldberg H. Preventive content of adult primary care. Do - generalists and sub-specialists differ? (Audit only). Am J Public Health
1984;74:223-227.
30. Basson EC. The role of the doctor in public education. Health Education,
Theory and Practice in Cancer Control, mcc Technical Report Series, vol. 10,
1974.
31. Fink A, Kosecoff j, Chassin M, Brook RH. Consensus methods: characteristics
and guidelines for use. Am j Public Health 1984;74(9):979-983.
32. Fleming DM, Lawrence MST A. An EVdluation of recorded information about
Preventive Medicine in 38 Practices, J R Coll Gen Pract 1981;31:615-620.
33. Forrest jD, Hermalin A, Henshaw SK. The impact of Family Planning Clinic
Programs on Adolescent Pregnancy. Fam Plann Persp 1981;13:109-106.
34. Frame PS, Carlson 5j. A critical review of perioclic health screening using
specifie sereening criteria. Part 1. Selected diseases of respiratory,
cardiovascular, and central nervous systems. J Fam Pract 1975;2:29-36.
35. Franchesehi S, Serraino D, Talamini R, Candiani E. Personal habits and
attitudes towards smoking in a sample of physicians from north-east of Italy.
Letter to the Editors. Int J Rpidemioll986;15(4):584-585.
36. Frei E, Frechette AL. The future of cancer control. N Engl j Med 1978:298:567.
37. Fry J, Stephen W j. Primary Health Care in the United Kingdom. Int j Health
Services 1986;16(4):485-495.
38. Gemson DH, Elinson j. Prevention in primary care: va riabili t y in physician
practice patterns in New York City. Am j Prev Med 1986;2:226-234.
39. Goldbloom R, Battista RN. The Periodic Health Examination:1. Introduction. Can
Med Assoc j 1986;134:721-723.
40. Golds~ein B, Fischer PM, Richards JW, Goldstein A, Shank jC. Smoking
counseling practices of recently trained Family Physicians. J Fam Pract
1987;24 ( 2): 195-197.
41. Gray j. The effect of the Doctor's Sex on the Dector-Patient Relationship, j R
Coll Gen Praet 1982;32:167.
42. Green LW, Eriksen MP, Schor EL. Preventive Practices by Physicians:
Behaviourial Determinants and Potential Interventions. In Battista RN, Lawrence
1 28

, , ; , ,J )" (.
RS, eds. Implementing Preventive Services. Am J Prey Med 1988;4(4 )s:101-
107.
43. Haynes RB, Davis DK, McKibbon KA, Tugwell P. A critical appraisal of the
efficacy of continuing medical education. lAMA 1984;251:61-64.
44. Hopkins EJ. A study of Patients' Choice of Doctor in an Urban Practice. J R
Coll Gen Pract 1967;14:282.
45. Institute of Medicine. Preventive Services for the WeIl Population. Report of the
Institute of Medicine, National Academy of Science, Healthy People
(appendices), 1-22. Washington, US Department of Health, Education and
Welfare 1978.
46. IST AT. Indagine sullo stato di salute della popolazione: 1980. Roma 1983.
47. IST AT. Indagine sullo stato di salute della popolazione: 1983. Roma 1987.
48. jacoby I. The consensus development program of the National Institutes of
Health - current practices and historical perspectives. Int J of Technology
Assessment in Health Care 1985;1(2):420-432.
49. Kennedy TE, Coppard Le. The prevention of faUs in later life: a report of the
Kellog International Work Group on Prevention of Falls in the Elderly. Danish
Med Bull 1987;34, suppl 4:1-24.
50. Kosecoff l, Fink A, Brook RH et al. General medical care in the education of
internists in university hospital. An evaluation of the teaching hospital, general
medicine group practice program. Ann Int Med 1985; 102:250-257.
51. Kottke TE, Battista RN, DeFriese GH, Brekke ML. Attributes of successful
Smoking Cessation Interventions in Medical Practice: A Meta-analysis of 39
Controlled Trials. JAMA 1988;259(19):2883-2888.
52. LaForce FM. Immunizations, immunoprophylaxis, and chemoprophylaxis to
prevent selected infections. JAMA 1987; 257(18):2464-2470.
53. Lawrence RS, Mickalide AD. Preventive Services in Clinical Practice:
Designing the Periodic Health Examination. JAMA 1987;257(16):2205-2207.
54. Lewis CE, Wells KH, Ware J. A model for predicting the counselling practices
of physicians. J Gen Intern Med 1986;1:14-19.
55. Lewis CE. Disease prevention and health promotion practices of primary care
physicians in the United States. In Battista RN, Lawrence RS, eds. Implementing
Preventive Servir-es. Am J Prev Med 1988;4(4)s:9-16.
56. Lol"las J, Haynes RB. A Typology and critical review of test€<! strategies for
the application of clinical practice Recommendations: from "official" to
"individual "clinical policy. 1[1 E~tt~sta RN, Lawrence RS, eds. Implementing
Preventive Services. Am J Prev Med 1988;4(4)s:n-94.
57. Lurie N, Manning WG, Peterson C, Goldberg GA, Phelps CA, Lillard L.
Preventive care: do we practice what we preach? Am J Public Healtb 1987;
58. Maheux B, Pineault R Beland f. Factors influencing physicinns' orientation
toward prevention. Am J Prev Med 1987;3:12-18.
59. Mandel IG, Franks P, Dickinson JC. Screening guidelines in a family practice
program: A five-year experience. J Fam fract 1982;14:901-907.
60. Manning WG, Leikowitz A, Goldberg GA. A controlled trial of the effect of a
prepaid group practice on use of the services. N Engl J Med 1984;310:1505.
61. McAlister A, Mullen PD, Nixon SA, Dickson C, Gottlieb Nt McCuan R, Green L.
Health Promotion among primary care .,hyslcians in Texas. Texas Medicine
1985;81:55-58.
62. McPhee SJ, Richard RJ, Solkowitz SN. Performance of cancer screening in a
university general internaI medicine practice. J Gen Int Med 1986;1:275-281.
63. McPhee SJ, Schroeder SA. Promoting Preventive Care: changing reimbursement
is not enough. AJPH 1987;n(7):780-781.
64. Morosini PL. Valutazione degli interventi preventivi. Intervento al Convegno per
il Cinquantenario deU' Istituto Supe, iore di Sanità. Roma 1984.
65. Mullan F, J aeoby 1. The town meeting for teehnology - the maturation of
consensus conferences. JAMA 1985;254(8):1068-1072.
66. Orleans CT, George LK, Houpt JL, Bradie KH. Health promotion in primary
care: a survey of U.S. family practitioners. Preventive Medicine 1985;14:636-
647.
67.
68.
Page C. Five preventive activities carried out during general practice
consultations. Br Med J 1983;186:1787-1788.
Perry S, Kalberer JT. The NIH consensus-development program and the
assessment of health-care technologies - the first two years. N Engl J Med
1980;303( 3): 169-172.
30

(
c
69. Pineault R. The effect of prepaid group practice on physicians' utilization
behaviour. Med Care 1976;14:121.
70. Piperno A. Renieri A. Rapporto sul Medico di Base. Salute e Territorio
1980;11:2-9.
71. Preston-Whyte ME, Fraser Re, Beckett JL. Effect of physician's gender on
consultation patterns. J R Coll Gen Pract 1983;33:654.
72. Radecki SE, Mendenhall Re. Patient counselling by primary care physicians:
results of a nationwide survey. Patient Education and Counselling 1986;8:165-
177. 73. Recommendation of the Public Health Service advisory committee on influenza
practices: Influenza vaccine. Morb Mortal Wkl Rep Im;26:193.
74. Rice T. The Impact of changing medicare reimbursement rates on physicians'
induced demande Med Care 1983;21 :803.
75. Rigotti NA, Calkins DR, Gordon NP, Cleary PD. Do Physicians advise patients
about health practices, and does it make a difference? Clinical Research
1985;33:73-85.
76. Romm F J, Fletcher SW, Hulka BS. Periodic health examination: comparison of
recommendations and internists' performance. So Med Journal 1981;74:265-271.
n. Rosen MA, Logsdon DN, Demak MM. Prevention and health promotion in primary
care: baseline results on physicians from the INSURE project on life-cycle
preventive health Services. Prev Med 1984;13:535-548.
78. Rosso S, Segnan N, Colombo A, Costa G, De Maria M, Faggiano F. Stato di
salute della popolazione a Torino:: ~ttivita' sanitaria degli ospedali di Torino.
Unita' Sanitaria Locale 1/23 Torino. Torino 1984.
79. Smith A, Alvarez CA (eds). Cancer control. Advances in Medical oncology,
research and education. England: Pergalu.on Press, 1979.
BO. Tideiksaar R. Preventing faUs: home hazard checklist to help oIder patients
protect themselves. Geriatries 1986;41:26-28.
81. Valente CM, Sobal J, Muncie HL, Levine DM, Antlitz M. Health promotion:
physicians' beliefs, attitudes and practices. Am 1 Prev Med 1986;2:82-88.
82. U.S. Preventive Services Task Force. Recommendations for breast cancer
screening. lAMA 1987;257(16):21%.
31
,1

83. U.S. Preventive Services Task Force. Recommendations for smoking cessation
counselling.jAMA 1988;259(9):2882.
84. Wechsler Ht Levine St Idelson RK. Rohman M, Taylor JO. The physician's role
in health promotion: a survey of primary care practitioners. N Eng J Med
1983;308(2):97-100.
85. Wells KB, Lewis CE, Leake B, Ware JE j r. Do physician preach what they
practice? JAMA 1984;252:2846-2848. 86. Wells KB, Ware JE, Lewis CE. Physicians' attitudes in counselling patients
about smoking. Med Care 1984;22(4):360-365.
87. Wells KB, Lewis CE, Leake B, Schleiter MK, Brook RH. The practices of
general and sub-speciality internists in counseling about smoking and exercise.
Am j Public Health 1986;76(8):1009-1013.
88. Williams MC, Davignon L, Mc Donald jC, et al. Trials of aequos killed
influenza vaccine in Canada 1968-69. Bull WHO 1973;49:333. 89. Wolfson LO, Whipple R, Ammerman P, Kaplan j, Kleinberg A. Falls and the
elderly: gait and balance in the elderly, two functional capacities that link
sensoryand motor ability to faUs. Clinics Ger Med 1985;1:649-659.
90. Woo Bt Woo B, Cook EF, Weisberg M, Goldman L. Screening procedures in the
asymptomatic adult: comparison of physicians' recommendations, patients'
desires, published guidelines, and actual practice. JAMA 1985:254(11):1480-1484.
91. Zabin LS. Evaluation of pregnancy prevention programs for urban teenagers.
Fam Plann Persp 1986;18:119-126.
32

"
TAllE 1 ca.p.rllon of Methodlin !krvtys of Preventive PrllCtica
~ A - Physlc111l ~v'YI
VEAR lnforwtlon st:! ~l. Scope Method Resp. , aize of rate Source Popu atton
JOIe ....,Ung
fMllr Goldste1n Total "'die ne 1978 1116 Local Population 71 •• Telephone PrICt1tloners
Ireland Dall General 198 29S Regional Syst_tic ". MaU PrlCtltloners
l'Iassachussets fMnvi Internai
Wechsler Genera 1985 427 Regional RandOIII 76. Man Practltionerl'
New York State f.nr CuIIIIings Medic ne 19" 2711 Reglonal RandoM 6~ Man PrlCtlt10ners
Quebee Face-to Pri.,.V Battista face Care 198' ·.,11 Regional RandOftl 95_ Intervll!W Physlcl.ns
INSlIIE PriB'y Rosen Convenient Care 1984 61 Regional SMple NA MaU Physic1ans
Wessex Catford General lq84 '8~ Local RandOftl 9". "-11 PrlCtltioners
Merlcan Ceneer prl .. y Society (ACS) Cere 1985 111'5 National RandOftl 91. Telephone Physiciens
_rican ftedical Association (NIA) F·llr Orleans Medie ne 1985 618 National RandOftl 5n "-11 Practltloners
Boston Face~to Patients, Woo Total face Generel 1985 88 Local Population NA lntervil!W Pract1t1oners
New-Brunsw1ek Face-ta Pri ... y Battista fare Cere 1985 265 Regional RandOlll 95. Intervll!W Physiciens
TllCas fMnYi Internai
McAl1ster Genere 1985 442 Regional RandOlll ••• "-11 Practit10ners
Merlcan f'edlcal Association (NIA) Radecki Cllnical 1986 '655 Natlonal RandOIII .~ . MaU Encounters
Le: Mgeles Total A11 State Basset
1986 886 Regional Population 21. Mail ",yslelMS
JIlaryland Pri ... v Valente Care 1986 111411 Regional RandOlll 65. Mail Physiciens
New YorK City FMUYi Internai GeMson Genera 1986 1211 Local SystetIIIItic 9~ Telephone Prectitioners
Pennsylvania Internai Wells fledlc:1ne 1986 628 National RandOIII 7~ • NA Residents
Western USA Pri ... y Lewis Care 1986 281 Local RandOIII 76_ l'eU PhyslclMS
North Ceroline General, Attar1an F.Ur 1987 195 Regional RandOlll 6" ""11 Prect tioners
Pennsylvania Prl ... y Albanès Care 1988 663 Regional RandOll 6'. Mail PhysiclMS
"' ' ~} .. ,)
TABlE 1 (cont'd)
STlIlVI AUTtKRI VEAR
B - Revlews of Medical Records
~le Scope Method Resp. Information Studr slze of rate Source Papu ,tion
5..,11ng
North Cero11na Revlew of Patients 0' ROM ftledieal general 1981 86 Locel NA NA records preetices
OKford Revlew of Patients of Fleming Conventent ftledlcal general 1981 8522 Locel s..,le NA records practlce
London Revlew of Patients 'ra. Paae ftledlcal a~al ln 246 Local Random 67~ • records prlctict
USA Revlew of Patients of Koseckoff IM!dical hosp'ital 1985 1532 National Random 98~ records .... iis
Toronto Review of Patients of Bor~iel Convenient ftledicel fallUr 198 21 locel sample ,~ records preet ces
C - Patient Surveys
USA Riaottl 195 198' National Random NA Telephone
AsmtOMtlc Pa ients
Buffalo Face-to s.okers in a CUmllngs Total face fallnr 1987 '" Local Population 6~ • interview preet ces
USA Health Lurie Insurances General 1987 '829 National Random NA records Population
• Percentage. have been recalculated frOll! the data avaUable ln the rUcle
34

c
STlIlV/ AUTttCII/ VEAR
101008 Goldste1n 1978
Irelend DIIly 19811
PlIIssachussets Wechsler 19S' ~bec Battista 198'
INSlRE Rosen 1984
Wessex C8tford 1984
ACS
1985
N'A Orleans 1985
New Brunswick llettista 1985
Texes McAl1ster 1985
Maryland Val ente 1986
New York City Gealson 1986
Pennsylvania Wells 1986
Western USA Lf!W1s 1986
North Caroline ROIIIIII 1981
USA Koseckoff 1985
USA RigQttt 19~
Buffalo ClMings 1987
A - Physicien S\ryeys _ of Physiciens WlO cOWlSel thelr patients on:
SIIoking Alcohol ebuse
98
94
911 85
98
81
97
88
97
66 59
97 87
97 94
97
52 56
B - Reviews of Medical Records _ of Records reportlng antl-SlCklng and Ilcohol abuse counselllng
72-56-61 57-41-47 (accordlng to Ige groups)
C - Patients SUryeys _ of Patients recalling being counselled by their physiciens
42 (.en) 9 48 (WOMen) 6
41

STIJlVI AU1lOV VEAR
OJebec Blttista 198' New Brumwiclc Blttista 1985
ACS
1985
New York City GeMon 1986
London p;ue 1 ,
New York St.te CunI\Ilngs 198' Los Angeles Basset 1986
Pennsylvania Albanes 1988
IlKford Fllllling 1981
North Caroline ROIIIII 1981
USA Koseckoff 1985
NSPHPC Rigotti 1985
HIE Lurie 1987
, Il,
TABlE , SulMry of results for cancer urlV detectlon practlcel
A - Physicien Survey
_ of P1iïSicians WlO prescribe early detecUon techniques
Luna Cancer Cervical Cancer êhëst sputlIII x-ray cYtology
Breast Cancer mammogrlph~ Breast
lXMIinetlon Breast Pep lelf exaginetion test
77 41 8 99 96 91
77 49 , 98 92 98
58 11 811 98 7S
49 19 211 811 48 92
65 •
8
11
42 69 94
B - Reviews of Medical Records , of Records reportlng early detection techniques
56
85-77-78 68-64-59 (accordlng to age groups)
511
C - Patient surv~s , of Patients screened with early etection techniques
72 69
8
• Percentage has been recalculated frOM the data available in the article
36

.~. l , ; ,i
TMIlE 4 , IteMS for evaluatlng physlclllll' knawledge on association batween rlsk factors end dl_es.
ItelllS on SIIoklng Correct answer ItelS on alcohol abuse Correct An...,.
Lung cancer yes Coronary Hart Disesse yes l1ver Clrrhosis ye. Atherosclerosls yes Esophaglt1s ye. Chronlc Bronch1t1s yes Pancrlltit1s yes 8ladder Cancer yes Psychosis )'1' L .. ynK Cancer yls Pol yneuropathy yes MouthCancer yls Cardiomyopathy yes Pancreas Cancer no Anemia yes Colon Cancer no Esophaglll Cancer yes CerVical Cancer no Pancrlltic Cencer yll ThrOlllboangUtls yes Llver Cencer yes
Stomach Cancer yes 81adder Cancer no !bAth cancer yu
ItelS on cervical 1 teInS on breast cancer Correct answer cancer Correct 1Il5Wer
Dral Contraceptives no Dlet no ""er of sexuel Familial Predisposition yes partners yes Overwelght yes Parity yes low P .. ity yes First sexuel intercourse Dral Contraceptives no at young age yes Late Flrst pregnancy yes POOl' Personal Hygiene yes Early Menarche ylS Law Social Class yes Late Menopause )'II Veneres! Diseases yes 10nlzlng Radiations no Herpes Genitalis yes Cigarette SIIIoking ylS
( 37

PREVENTIVE PRACTICES OF GENERAL PRACTITIONERS
IN TORINO. IT ALY
38
l' '" , \ V'
PRESENTATION
This paper reports the descriptive analysis of the data collected on an array of
preventive practices and attitudes.
Reported practices are compared with published recommendations. We paid
particular attention to the implementation of interventions designated as objects of
special policy by the Local Health Authority of Torino, such as social services for the
elderlyand sexual education for prevention of unwanted pregnancies.
This paper WBS written in collaboration with Dr Nereo Segnan, director of the
Area di Epidemiologia of Torino, Dr Renaldo N. Battista, thesis supervisor, and Drs
Antonio Ponti, Daniela Aimar and Carlo Senore who are researchers at the Ares di
Epidemiologia of Torino. The author of this thesis contributed the literature review,
methods assessment, analysis, and writing of the corresponding sections.
39

, , \'"' - "
PREVENTIVE PRACTICES OF GENERAL PRACTITIONERS
IN TORINO, ITALY
Key wards:
Running head: Preventive Practices in Torino
Primary prevention, secondary prevention, general practice
Nereo Segnan, M.D., M.Sc.* Renaldo N. Battista, M.D., Sc.D.**
Stefano Rosso, M.D.*,** Antonio Ponti, M.D., M.P.H.*
Carlo Senore, M.D* Daniela Aimar, M.Sc.*
* From the Area di Epidemiologia, Unita Sanitaria Locale 1, Torino, Italy
** From the Department of Epidemiology and Biostatistics, McGill University and the Division of Clinical Epidemiology, Montreal General Hospital, Montreal, Canada. Dr. Battista is a Research Scholar of the National Health Research and Development Program, Ottawa, Canada.
Address Reprint requests ta: Dr. Nereo Segnan Area di Epidemiologia, Unita' Sanitaria Locale Tarino l, Via San Francesco da Paola 31, Torino, Italy 10123 Tel.:(l1) - 835386
(11) - 832004
40

~' (,
f. ~,
t ~.
c
"'; ':_l,.-tt{' r~"",t~~"~"" vl.::1~~.~~ .' ,
ABSTRACT
Health care reforms introduced in Italy in the Iate 1970's triggered a profound
rethinking of the role of general practitioners in prevention. Two hundred and
nine general practitioners registered in the Torino area were interviewed to delineate
their beliefs, attitudes, and practice patterns in relation to prevention. An array of
primary and secondary preventive interventions were examined, including influenza
vaccination of the elderly; counselling activities related to smoking, alcohol
consumption, accidents, contraception, safety helmets and seat-belts; and early
detection of hypertension and lung, cervical, and breast cancers. Although progress bas
been made in areas where guidelines for preventive practices are weIl accepted, there
is still room for improvement in their full implementation. Features of the
organization of medical practice in Italy that impede the integration of preventive
interventions are examined and compared with the situation in North America.
41

, ,/
t
INTRODUCTION The raIe of physicians in providing preventive services is now recognized1
-,..
The approach proposed by the Canadian Task Force on the Periodic Health
Examination3 and by Breslow and Somers2 is based on a set of age- and sex-related
health protection packages. Offering ease-finding and primary prevention activities to
patients who consult their physician for episodic care is at the heart of this strategy,
which makes any patient visit an opportunity for prevention6-
7•
Studies of the extent to which preventive activities have been integrated into
clinical practice in the USA8-
16 and Canada'8-22 show that, although sorne
implementation of the preventive strategies is occurring, the full benefits have not been
realized. Few studies have explored the patterns of preventive practice among primary
care physicians in Europe, but one by Pipern023 documents such activities among
general practitioners in Italy.
The organization of the Italian National Health Service (Servizio Sanitario
Nazionale -SSN-) is based on Local Health Authorities ("Unita Sanitaria Locale" -
USL -) whose administrators are elected by the municipal government. The USLs are
population based and each of them provides health services for SO,OOO to 200,000 inhabitants. The Local Health Authorities administer the services according to the
national and regional policies. Resourees for the administration of USL are provided
by the central government to each Region, according to demographic indicators, previous
year budget, inflation rate, and specifie interventions required by the local authorities.
AlI public hospitals, family medicine services, which encompass general and
pediatric practice, public health programs, occupational medicine, and environmental
control activities are under the jurisdietion of the USL. Adults (over 14 years of age)
are enroled in the rosters of GPs while children under 14 years of age are enroled in
the pediatricians' rosters. Patients can freely choose their general practitioners and
pediatricians within the rosters of USL.
Funds for health care are provided by indirect taxation and most medical
interventions are freely provided to aIl citizen;1 with sorne exceptions, sueh 8S dental
treatment.
Physicians with or without a specialization, operating within the SSN, May be:
1) full time general practitioners,
42

2) 3)
part-time general practitioners with hospital duties.
full time hospital physicians.
)iI .,", LU U ' ,
or
Any physician with a degree recognized by the Italian Ministry of Education can
apply for being registered on the rosters of USL as a general practitioner. GPs are
paid on a per capita basis and practiee within the SSN, which aHows tbem a maximum
number of patients that takes into account any other professional commitments they
may have. A general practitioner is allowed a maximum of 1,500 patients; a
pediatrician, BOO, the disparity being due to different workload required by the two
clinical situations.
Before the institution of the SSN, there were no patient quotas for GPs.
Physicians were subsequently invited to gradually reduce the number of patients to the
upper limit mentioned before. This rute was not strictly enforced and there is a smalI
minority of GPs with slightly more than 1500 patients.
GPs provide free and accessible primary care and Act as "gatekeepers" to
consultants and hospital care. Path~nts who go directly to specialists pay for their
services. There are few exceptions to the rule as patients may go directly to
~accination centers and clinics specialized in family planning, gynecological disorders
and sexual counselling called "consultori" without paying.
The object of our survey was to study the attitudes and practice behaviours of
general practitioners about preventive medicine practices recommended by the Canadian
Task Force on the Periodic Health Examination3.24-27 and the US Preventive Services
Task Force28-
31• We colIected information on an array of primary and secondary
pre'/entive interventions inc1uding influenza vaccination of the elderly; counselling
related to smoking, alcohol consumption, accidents, contraception, safety helmets and
seat belts; and early detection of hypertension and cancer of the lu' &, cervix, and
breast. '''le were also interested in gathering data on smoking cessation and anti
alcohol a'lUse interventions other than counselling for which scientific evidence of
effectiveness and c1ear recommendations do not yet eX'lSt.
Tables A.1 and A.2 in Appendix provide a summary of the practices
recommended in the Reports of the Canadian Task Force on The Periodic Health
Examination and methodological guidelines used by the working group3.24-27.
43

!
METHODS
We selected a systematic sample of 225 full- and part-time physicians from the
roster of 1,158 SSN-registered general practitioners in the Torino area after
stratification for sex, age and maximum number of patients allowed - variables
believed to influence preventive behaviour. One in five physicians was sampled. This
method gave us a sample proportionate by age, sex, and practice size. We interviewed
209 of the physicians sampled, as 16 refused (7.1%) to partit.pate in the study. Table 1
illustrates our sampling method and the negligible effects of non-respondents on the
final group of physicians interviewed.
Three trained interviewers asked them questions about:
1) Physicians' patterns of preventive practices including primary preventive
practices (smoking cessation and, anti-alcohol abuse interventions, counselling on
accidents in the home among the elderly, flu vaccination for the elderly, and
contraception) and secondary preventive practices (early detection of long, cervical,
and breast cancers and of hypertension);
2) physicians' perceptions of the effectiveness of these primary and secondary
preventive interventions;
3) specifie features of. the organization of their medical practices including
their mode of reimbursement and the actual structure of their clinical practice; 4)
personal habits of physicians such as smoking.
The questionnaire used in this study consisted of close-ended questions that
forced physicians to make choices. Perceived effectiveness of preventive practices
was rated on a scale ranging from "very effective" to "not effective" and perceived
use of a practice on a similar scale going from "al ways used" to "never used".
A pretest of the questionnaire was conducted on ten physicians not included in the
final sample. Results were examined for information bias. Interviewers did not
introduce any significant bias in collecting and recording answers.
44

RESULTS
O!]!snization of MedicaI Practice
General practitioners in Torino usually run their own medical practice, and they
have to provide offices and support staff. Fifty-six percent had an assistant who, in
20% of cases, was a nurse.
The offices of 50% of physicians were 10cated in buildings where other GPs and
specialists practiseQ~ n% regularly availed themselves of the opportunity to exchange
opinions and discuss cases with other physicians and the specialists operating in the
same facility. Of the physicians who exchange opinions, 21% periodically met with
colleagues and 11% shared office facilities and receptionist services.
Primary prevention
Smoking
Even though 10% of the physicians believed that the risk of contracting lung
cancer is no lower for ex-smokers than for those who continue smoking, aImost aIl
physicians perceived quitting smoking as "very" or "rather important" for promoting
health ('17.6%), and 98% of them claimed to have provided counselling to their patients.
Their advice varied according to patients' smoking habits. Sixt y percent of GPs
counselled aIl their patients smokers, but 37% provided counselling to those whom they
regarded as heavy smokers, i.e. at least 10 cigarettes per day.
Physicians were also questioned about the perceived effectiveness and stated use
of severa! smoking cessation interventions as shown in (Table 2). There was
substantial agreement regarding the effectiveness of mass media advertisir.g (74%) and
regular counselling (72%). Various types of psychotherapy (individual - 56%; psychotherapy in clinics - 43%; and group therapy - 41%) were considered effective to
varying degrees. Although psychotherapy as a whole had considerably high credibility,
the lack of adoption may be explained by the lack of payment for this technique by the
SSN. Acupuncture is not covered by the SSN, but was perceived as effective and was
used. In addition, it must be emphasised that from 15% to 36% of GPs admitted to
having no knowledge or opinions about the interventions discussed, except for mass
media advertising and counselling.
45

Counselling practice appeared ta be influenced by the physician's own smoking
habits. Seventy-four percent of non-smokers compared to 47% of smoking physicians
and 58% of ex-smokers counselled their patients who smoke to quit. This finding was
confirmed by several studies32-
33 although no relationship was found by other
studiesll,34. It is WOI th noting that the percentage of physicians who smoke is quite
high (36.8%) in comparison to other western countries, and approaches the proportion
of smokers in Torino (38.4% between 25 and 74 years of age). Similar findings have
been reported in Pordenone, ltaly35.
The most important limiting factors in implementing smoking cessation
intelventions were perceived to be the low patient compliance (rated important by 67%
of GPs) and the cost of the techniques (rated important by 47% of GPs). Restrictive
legislation and increasing the price of cigarettes are perceived as moderately effective
strategies by 48.3% and 30.6% of physicians, respectively.
AlcoJtol
A distinction can be made between alcohol abuse and a moderate intake of
:0 alcoholic beverages, but general practitioners in the Torino area fail ta agree on the
level of alcohol consumption considered safe (Table 3). The results are comparable with
those from a survey oi health care workers in England36.
Contrary to the opinions expressed regarding the effectiveness of measures to
help smokers quit, 77% of physicians main tain that psychotherapy is the most effective
treatment for alcohol abuse and 61% recommend it. Smaller perceJtage~ of physicians
belil'!ved in the effeetiveness of regular eounselling proviced by physicians and
Alcoholics Anonymous (Table 4). Although 53% of GPs considered Alcoholics
Anonymous ta be effective, ùnly 19% of them recommended it because of the
difficulties associated with recmrmending practices not eovered by the SSN.
Forty-seven percent of physicians said they do not use available techniques
considered effective b cause the SSN does not reimburse patients for such treatment.
Forty-one percent of GPs feel they have insufficient professional training in counselling.
Health education and mass media advertising were considered important factors which
ean fac:ilitate the physicians' in",;l ve!1tion against alcohol abuse, but 85% of GPs
believed specialized treatment centers to be particularly useful (Table 5). In
46

(
(
addition, most physicians (81%) regarded a tightening of controls on drinkina and
driving as a more effective measure than increasing the price of alcohol and restricting
sales.
Accidents in the home among the elderly
Only half of the G Ps surveyed believed advice to elderly patients to he useful in
preventing accidents at home, while 10% feU they had insufficient knowledge to form
an opinion on the tapie. This finding was supported by the fact that ooly 4'71 of the
GPs offered such advice, and 27% of those who did, did so with difficulty. Most
physicians (96%) were aware of the difficulty of modifying the living conditions of
their eIderIy patients, and 57% maintained that their patients failed to follow anyadvice
that was not strietly medieal (Table 6).
Plu vaccination for the eiderly
Seventy-seven percent of GPs believed flu vaccination to be effective for people
over 65 years of age, ooly 18% of GPs directly vaccinate them. Physicians frequently
refer patients to vaccination centers within the SSN.
Contraception
Most GPs (92%) considered it useful to provide information on contraceptives
and sexual education, but ooly 34% of them took the initiative to provide them. Many
GPs (82%) referred patients to specialized clioies (consultori) where advice and
assistance js provided for sueh matters as contraception, pregnancy and the prevention
of cancers specifie to wornen. Sorne patients were referred to specialists who
practice in other public rnultispecialized services or have hospital appointments.
Other Preventive Measl!.es
Most physicie.l1S maintained that the measures listed in Table 7 were extremely
effective, with the exception of vitamin A for the prevention of lung cancer.
At the tirn ~ of the survey, two legislative bills were tabled making the wearing
of safety helmets by motorcyclists, and seat belts by car drivers compulsory. The bill
on safety helmets was subsequently enacted into law. However, 58% of GPs did not
47

,1 consider il their responsibility to recommend the use of safety helmets and seat belts.
Secondary prevention
Luna cancer Although 57% of GPs believed chest X-rays to be effective in the early detection
of lung cancer, only 30% ordered them and 19% prescribed chest X-rays only for
patients who smoke at least 20 cigarettes per day and are 45 years of age or older.
Gynecoloaica1 cancers
Prevention of gynecologica! cancers is shared by G Ps with others in the National
Health System. Of the GPs surveyed, 18% maintained that such preventive activity i8
the duty of gynecologists, while 11 % believed it should be the responsibility of the
"consultorio". The working relations between GPs, cHoic physicians, and specialists
are often rather difficult, and 45% of GPs reported that they did not get enough
....ooperation from such colleagues.
Cancer of the cervix
Virtually all physicians (99%) consider the PAP test effective, but we uncovered
differences in the frequency with which it is performed relative to the age of the
patient (Table 8). Most physicians performed PAP tests frequently on women over 35
years of age, but oo1y 16% of thpm gave women under 35 the test.
Breast cancer
The physicians interviewed considered the mammogram to be more of a diagnostic
technique than an early detection measure for asymptomatic women. Oo1y 10% used
mammography as a screening procedure in the age group at risk (50-59 years of age).
A physical examination of the breast, in the absence of breast related symptoms, was
carried out by ooly 21% of physicians.
Physicians seemed to regard breast self examination (8SE) as a more important
secondary preventive measure, and 95% believed regular BSE to be a 'Iseful early
detection technique. Of the 87% of physicians who recommended it to their patients,
66% recommended that it begin at age 20. There was, however, some doubt about how
48
, ,

c
well the technique was taught to patients since only 25% of GP's make any follow-up
effort to ensure it is being performed properly.
Rather than teaching their patients BSE, 21% of GPs gave them literature on the
subject or referred them to a gynecologist or to a "consultorio".
Hypertension
It was common practice for GPs to take the patient's blood pressure during
routine examinations, but 5% of physicians stated that they only did so when certain
symptoms were present. Seventy-one percent of GPs took the patient's blood pressure
on the first visit only, 23% took it du ring every clinical encounter, and 6% invited
patients to return for periodic monitoring.
Twenty-eight percent of GPs began drug treatment of high blood pressure in
asymptomatic patients over 40 years of age when the diastolic reading was between 90
and 95,64% percent began treatment when the diastolic reading was between 95 and 100, and 7% when it exceeded 100.
DISCUSSION
The raIe of the primary care physician in providing preventive services has been
emphasized in North America in the pa st decade. Two recent reviews assessed the
penetration of preventive activities into the clinical practice of primary care physicians
in the U.S.A.37 and Canada38• Bath concluded that, even though progress has been
achieved in some areas where there are weIl accepted guidelines, such as smoking
counselling and early detection of cervical cancer, there is considerable room for
improvement in the implementation of the sets of guidelines promulgated by the
Canadian Task Force on the Periodic Health Examination3.24-27 and by the U.S.
Preventive Services Task Force2s-
31•
The health care reforms du ring the late 1970s in Italy have triggered a profound
rethinking, not only of the Italian health care system but, of the respective roles of
general practitioners and specialists in primary care. The high response rate of GPs,
their level of interest during interviews, and the strong beliefs they expressed about the
effectiveness of preventive activities can be viewed as signs of their growing interest
49

, ' , ~r
in playing a more active role in promoting their patients' health. Indeed, a similar
survey of physicians' attitudes towards the prevention of gynecological tumours
conducted in Italy by Mossetti et al. 38, about ten years ago, had a 13% response rate, and
demonstrated a lack of knowledge and poor utilization of early diagnostic techniques.
Our findings indicate a need for additional incentives for physicians in carrying
out their new role. The physicians we interviewed confirmed their beHef in the
efficacy of the various preventive activities they were asked to judge and they tended to
overestimate the effectiveness of early detection of cancer and other diseases. The
most effective measures were, in fact, entrusted to consulting specialists23• With
regard to primary prevention, the practices considered most effective by GPs were
either not yet targets for counselling during clinical encounters (e.g. the use of crash
helmets and seat belts), or seen as being the responsibility of the consultant
gynecologist (e.g. counselling about contraceptive methods).
Interventions for such problems as smoking or drug and alcohol abuse were
delivered with only moderate confidence in their effectiveness. Attitudes regarding
smoking cessation are illustrative. Although the majority of physicians are firmly
persuaded that smoking cessation is very important in promoting individual health, only
60% of physicians comply with published guidelines, counselling all smokerst
regardless of the number of cigarettes they claimed to smoke daily. Consistent with
other studies32-n , smoking habits of physicians influence their counselling behaviours.
Another factor that influenced GPs' decisions to prescribe particular preventive
maneuvers was the coverage of medical interventions for those enrolled in the SSN.
Sorne interventions, such as psychotherapy, are partially reimbursed by the SSN and
GPs may be reluctant to prescribe procedures that result in an expense for the patient,
their effectiveness notwithstanding. Indeed the cost of procedures was often claimed by
GPs as a limiting factor in recommending them.
In general, interest in preventive practices appears to be oriented toward early
detection mea~ures as primary preventive activities are ooly beginning to receive
attention by primary care physicians in Italy, and the rates of usage of screening
techniques are, in general, higher tban those for adoption of primary preventive
interventions. Although the Reform of the National Health Service in 1978 clearly
emphasized the role of GPs in prevention, no follow-through action has been
50

(
· (
undertaken. The duties of GPs are still being viewed in the traditional perspective of
diagnosis and treatment. Preventive measures involving "medical" too18 are considered
more appropriate than counselling on the use of seat belts and crash helmets or on how
elderly patients may avoid domestic accidents.
In North America, practice guidelines have been provided by the Canadian Task
Force on the Periodic Health Examination, the U.S. Preventive Services Task Force,
and other recommending bodies such as the American Cancer Society and the Consensus
Development Conferences of the National Institutes of Health. In Europe. practice
guidelines have been formulated mainly by the International Union Against Cancer of the
World Health Organization. Although a reformulation of practice recommendations
May not he necessary, an Italian organization could be set up to summarize the state of
the evidence supporting preventive interventions and to ensure its adequate diffusion to
practising clinicians.
Appropriate incentives for preventive practices should be considered in order to
accelerate physicians' involvement in the emerging worldwide reorientation towards
disease prevention and health promotion.
51

1.
REFERENCES Frame PS, Carlson SJ. A critical review of periodic health screening using
specifie screening criteria. Part 1. Selected diseases of r~spiratory,
cardiovascular, and central nervous systems. J Fam Pract 1975;2:29-36. 2. Breslow L, Samers AR. The lifetime health-monitoring program: a practical
approach to preventive medicine. N Engl J Med 1977;296:601-608. 3. Canadian Task Force on the Periodic Health Examination. The periodic health
examination. Can Med Assoc J 1979;121:1194-1254. 4. Roemer MI. The value of medical care for health promotion. Commentary. Am
J Publk Health 1984:74:243-248. 5. Frei E, Frechette AL. The future of cancer control. N Engl J Med
1978;298:567.
6. Basson EC. The role of the doctor in public education. Health Education,
Theory and Practice in Cancer Control, UIeC Technical Report Series, vol. 10,
1974.
7. Smith A, Alvarez CA (eds). Cancer control. Advances in medical oncology,
research and education. England: Pergamon Press, 1979. 8. Romm F J, Fletcher SW t Hulka BS. Periodic health examination: comparison of
recommendations and internists' performance. Sa Med Journal 1981;74:265-271. 9. Radecki SE, Mendenhall RC. Patient counselling by primary care physicians:
results of a nationwide survey. Patient Education and Counselling 1986;8:165-177.
10. Gemson DH, Elinson J. Prevention in primary care: variability in physician
practice patterns in New York City. Am J Prev Med 1986:2:226-234. 11. Lurie N, Manning WG, Peterson e, Goldberg GA, Phelps CA, Lillard L.
Preventive care: do we practice what we preach? Am J Public Health
1987;77:801-804. 12. Wu B, Cook EF, Weisberg M, Goldman L. Screening procedures in the
asymptomatic adulte Comparison of physicians' recommendations, patients'
desires, published guidelines and actual practice. JAMA 1985;254:1480-1484.
13. McPhee SJ, Richard RJ, 50lkowitz SN. Performance of cancer screening in a
university general internai medicine practice. J Gen Int Med 1986;1:275-281.
52

~ ~, '!~."4j , l' • .. 'l r t,t·· ' ..
14. Val ente CM, Sobal J, Muncie HL, Levine DM, Antlitz M. Health promotion:
, physicians' beliefs, attitudes and practices. Am J Prev Med 1986;2:82-88.
(
15. Orleans CT, George LK, Haupt JL, Brodie KH. Health promotion in primary
care: a survey of US family practitioners. Prev Med 1985;14:636-647.
16. Battista RN. Adult cancer prevention in primary care: patterns of practice in
Qu6bec. Am J Public Health 1983;73(9):1036-1039.
17. Battista RN, Palmer CS, Marchand BM, Spitzer WO. Patterns of preventive
practice in New Brunswick. Can Med Assoc J 1985;132:1013-1015.
18. Battista RN, Spitzer WO. Adult cancer prevention in primary care: contrasts
among primary care practice settings in Qu'bec. Am J Public Health
1983;73(9):1040-1041 19. Elford W. Patterns of preventive practice of Southern Alberta Family
Physicians. Department of Family Medicine, University of Calgary, 1987.
20. Ho A, Herbert C, Farrall J. Periodic health screening: what members of the
Department of Family Practice at the Vancouver General Hospital are doing.
University of British Columbia, Department of Family Medicine, 1986.
21. Borgiel A, Williams j, Anderson G, Bass M, Spasoff R, Dunn E, Lamont C.
22.
23.
24.
25.
26.
27.
28.
Assessing the quality of care in family physicians' practices. Cao Fam Phis
1985;31:853-862. Audunnson G. Preventive infrastructure in family medicine; Master's thesis.
Department of Family Medicine, University of Western Ontario.
Piperno A. Renieri A. Rapporto sul Medico di Base. Salute e Territorio
1980;11:2-9. Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1984 update. Can Med Assoc j 1984;130:1278-1292.
Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1985 update. Can Med Assoc J 1986;134:724-729.
Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1987 update. Can Med Assoc J 1988;138:618-626.
Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1989 update. Can Med Assoc J 1989;141:209-216.
U.S. Preventive Services Task Force. Recommendations for breast cancer
S3
1
,".
screening. JAMA 1987;257(16):2196.
29. U.S. Preventive Service Task Force. Recommendations for prevention of
sexually transmitted diseases. JAMA 1987; 258(6):814.
30. U.S. Preventive Services Task Force. Recommendations for automobile
occupant protection counselling. JAMA 1988;259(1 ):76.
31. V.S. Preventive Services Task Force. Recommendations for smoking cessation
counselling. JAMA 1988;259(19):2882.
32. Battista RN, Williams JI, McFarlane L. Determinants of preventive practices in
fee-far-service primary carel Am J of Prev Med (Submitted for Publication).
33. Cummings KM, Giovino G, Sciandra R, Koenisgsberg M, Emont SL. Physician
advice to quit smoking. Who gets it and who doesn't? Am J Prev Med 1987;3:69-
75.
34. Maheux B, Pineault R, Beland F. Factors influencing physicians' orientation
toward prevention. Am J Prey Med 1987;3:12-18.
35. Francheschi S, Serraino D, Talamini R, Candiani E. Personal Habits and
attitudes towards smoking in a sample of physicians from north-east of Italy.
Letter to the Editors. Int J Epidemiol 1986;15(4):584-585.
36. Anderson P, Cremona A, Wallace P. What are the safe levels of alcohol
consumption? Brit Med J 1984;289:1657-1658.
37. Lewis CE. Oisease prevention and health promotion practices of primary care
physicians in the United States. In Battista RN, Lawrence RS, eds. Implementing
Preventive Services. Am J Prev Med 1988;4(4)s:9-16.
38. Bass MJ, Elford RW. Preventive practice patterns of Canadian primary care
physicians. In Battista RN, Lawrence RS, eds. Implementing Preventive
Services. Am J Prev Med 1988;4(4 )s:17-23.
39. Mossetti C, Sismondi GP, Panero M. Il compartamento dei medico nell'azione
preventive antitumorale, dati relativi ad un questionario inviato ai medici della
Provincïa di Torino. Minerva Gynaecologica 19n:29:107.
54

(
TABLE 1 - Number of patients allowed, and proportions ot physicians, by. and sex, for an GPs, those in sample and those interviewed.
Number of patients Age Sex "all GPs % sample " interviewed allowed
<=500 <40 M 21.7 21.8 22.8 <=500 =>40 M 15.2 15.1 14.9
501-1499 <40 M 3.0 3.1 2.5 501-1499 =>40 M 3.9 3.5 3.3
=>1500 <40 M 14.1 13.8 14.3 =>1500 =>40 M 26.2 26.7 25.5 any all F 15.9 16.0 16.7
(N=l158) (N=225) (N=209)
55

, ~ "
TABLE 2 - Perceived effectiveness of smoking cessation intenentions -Physicians' response C%)
Actual Use Perceived Effectiveness
Type of intervention Yes Effective Not Don't Effective know
Interventions that GPs ean perform by themselves
Regular counselling 98.1 71.8 27.8 0.4
One-time counselling 90.0 34.5 65.1 0.4
Nicotine gum 26.3 20.6 47.4 32.0
* "Nicoprivetl 28.2 15.8 63.6 20.6
Interventions that G Ps can prescribe and are only partially reimbursed by the SSN to the patients
Individual psychotherapy 26.3 56.0 25.4 18.6
Psychotherapy in clinics 8.6 42.6 29.2 28.2
Group therapy 7.7 41.2 29.7 29.1
Acupuncture 43.1 39.7 45.5 14.8
Hypnosis 19.1 37.8 31.1 31.1
Auriculotherapy 34.4 31.6 42.1 26.3
Specialized clinies 2.9 23.4 40.7 35.9
Mass media advertising Not 73.5 25.0 1.5 Applicable
Audiovisuals/Print 25.4 65.6 33.0 1.5
* Smoking cessation medieation used in Italy , 56

(
T ABLB 3 - Daily alcohol intake considered safe
Alcohol intake per day
o drinks/ day 1-2 drinks/day 3-4 drinks/day 5-6 drinks/day more than 6/ day
Physicians in agreement (%)
1.4 47.4 43.1 6.2 1.9
TABLE 4 - Perceived use and effectiveness of alcohol abuse treatment
Physicians' response (%)
Treatment Actual Use Perceived Effectiveness
Yes Effective Not Oon't know Effective
Interventions that GPs can perform by themselves
Repeated 97.1 58.8 41.2 0.0 counselling
Pharnnacotherapy 53.1 36.9 56.0 7.1 One-time coun,elling 82.8 30.7 68.5 0.8
Interventions that GPs can prescribe and are only partially reimbursed by the SSN ta the patients
Psychotherapy 61.2 76.6 20.5 2.9 Alcoholics Anonymous 18.7 53.1 19.6 27.3
Acupuncture 12.9 14.3 48.4 37.3
57

, ,r,
TABLE 5 - Factors perceived as facllitating the prevention of alcoholism
Physicians' response (%)
Useful Not useful Don't know
Specialized centers 84.7 12.9 2.4
Monitoring level of alcohol in drivers 81.4 17.7 0.9
Mass media campaign 78.0 22.0 0.0
Healtb Education 63.1 36.3 0.6
Taxation 25.4 73.7 0.9
Restrictions on sales 18.2 81.3 0.5
TABLE 6 - Problems encountered by 56 physicians who counsel the elderly on accidents at home
Problem
Impossible to modify living condition
Patient does not follow advice that is not strictly medical
Physician's limited time
Inadequate professional training
Patient's limited time
Physicians' response (%) (N=56)
58
YES NO
96.4
57.1
35.7
28.6
14.3
3.6
42.9
64.3
71.4
85.7

(
c
~ '( • 1
TABLE7- Perceived effectiveness of other primary preventive measures
Physicians' response (%) Preventive measure
Effective hot effective
Crash helmet for motorcyclists 100
Seat belts in cars 94.8 4.7
Weight control 94.7 4.8
Physical exercise 91.4 8.6
Controlled use of drugs 89.4 10.6
Oral hygiene 88.3 11.2
Vitamin A for the prevention of lung cancer 18.2 50.7
TABLE 8 - Use of PAP tests
Physicians' response (%)
Frequency of PAP test prescription Never more than 1 one per every 2 every 3
per year year years years Age of women
<35 16.3 4.4
35-70 1.5 11.8
30.5
69.5
27.1
11.3
59
11.3
2.0
Don't know
0.5
0.5
0.5
31.1
every 5 no years answer
7.0
0.5
3.4
3.4
.. \i'\
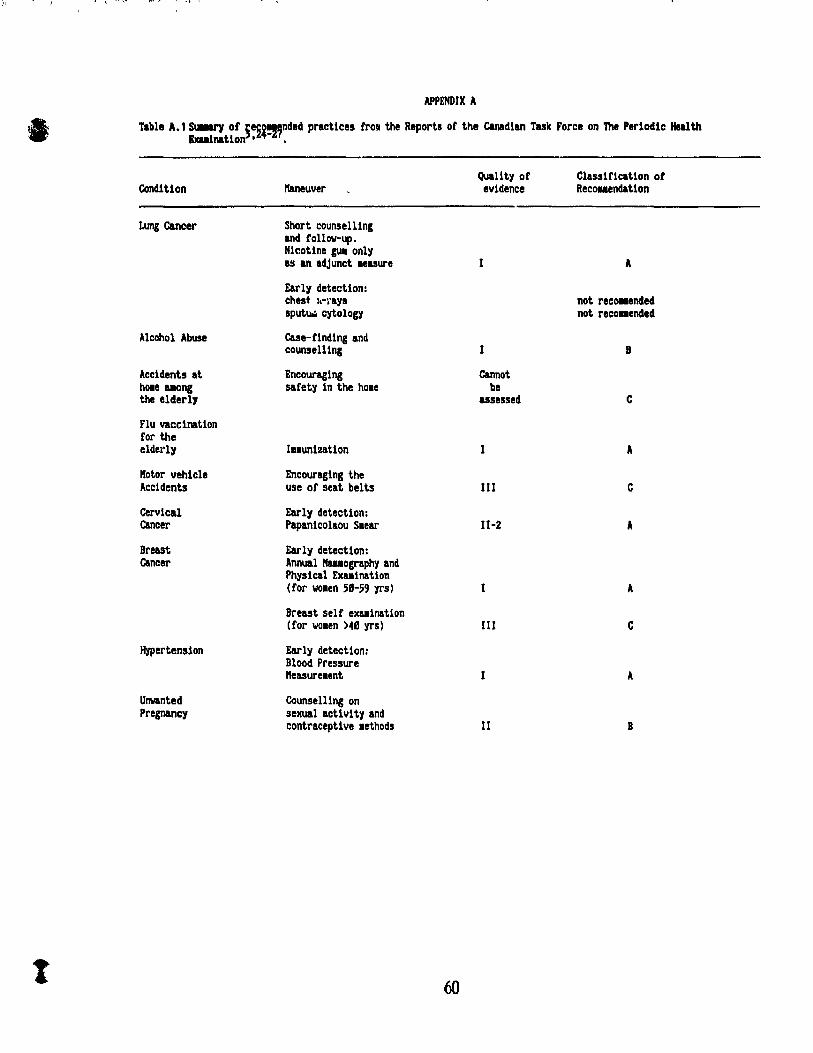
APPENDIX A
\1 Table A. 1 ~ of §e~~!nnded practices fraI the Reports of the C&nadian Tuk Force on 'Ille Perlodlc Health Exuinatlon • ,
Qual1tyof Classification ot Condition lfaneuver evidence Recouendation
Lung cancer Short counaelling and follow-up. Nicotine gu. only as an adjunct leasure 1 A
Early detection: chest I.-\'ays not recOlUnded sputUiO cytology not reco .. ended
Alcohol Abuse Case-rlndlng and counselling B
Accidents at Encouraging Cannot hOle IIIOng safety in the hOle be the elderly assessed C
Flu vaccination for the elderly IHunization A
Kotor vehicle Encouraging the Accidents use or seat belts III C
Cervical Early detection: Cancer Papan1colaou Slear 11-2 A
Breast Early detect10n: cancer Annual lfauography and
Physical EXlllnatlon (for wOlen 58-59 yrs) A
Breast self exaalnatlon (for wOlen >48 yrs) III C
Hypertension Early detecUon: Blood Pressure "easureaent A
Ull\/anted Counselllng on pregnancy sexual actlvlty and
contraceptive lethods Il B
t 60

c
------~~----------~,~,,~L .... ,;,~ ... ,~,i, ........ I".W.ni.J~1I'I
Table A.2 Summary of the grades of quality of evidence and classification of recommendations25
•
Quality of evidence
1: Evidence obtained from at least one properly randomized controlled trial. 11-1: Evidence obtained from well-designed controlled trials without
randomization. 11-2: Evidence obtained from well-designed cohort or case-control analytic
studies, preferably from more than one c~nter or research ,roup. 11-3: Evidence obtained from comparison be1.ween times or places with or
WithOl ~ the intervention. Dramatic results in uncontrolled experiments (such as the results of treatment with penicillin in the 19408) could also be included in the category.
III: Opinions of respected authorities, based on clinical experience, descriptive studies m' reports of expert committees.
Classification of Recommendations.
A:
B:
C:
D:
E:
There is good evidence to support the recommendation that the condition be specifically considered in a periodic health examination. There is fair evidence to support the recommendation that the condition be specifically considered in a periodic health examination There is poor evidence regarding the inclusion of the condition in a periodic health examination, but recomm.!ndations may be made on other grounds. There is fair evidence to support the recommendation that the condition be excluded from consideration in a periodic health examination. There is good evidence to support the recommendation that the condition be excluded from consideration in a periodic health examination.
61

1
DETERMINANTS OF PRIMARY PREVENTIVE PRACTICES OF
GENERAL PRACTITIONERS IN TORINO, IT ALY.
62

PRESENT A TION
Guided by the results of the study reported in paper 1, we selected an array of
primary and secondary preventive techniques according to their availability and adoption
in practice. We also focused on sorne traditional Medical procedures for comparison
with other studies, although such alternative approaches as acupuncture for smoking
cessation or Alcoholics Anonymous were also available and used in Torino.
The results of the previous analysis indicated that physicians tend to
overestimate the effectiveness of severai techniques, and entrust the most effective to
consulting specialists or other services. When patterns of adoption were examined, no
homogenous behaviours emerged and cornpliance to published guidelines V8ried among
physicians.
In paper 2, we explore the determinants of a set of primary preventive practices
of General Practitioners in Torino, ItaIy. Scales were constructed to measure
practices, leveis of knowledge and attitudes of GPs with respect to primary preventive
practices. An overall scale did not have an acceptable levei of internaI consistt:ncy,
signifying tlu:.t physicians' preventive behaviours vary across interventions.
Accordingly, we analyzed the determinants of each primary preventive practice.
Paper 2 was written by the author of this thesis, supervised by Drs Renaldo N.
Battista, Nereo Segnan, J. Ivan Williams and Dr Samy Suissa, and in collaboration with
Dr. Antonio Ponti.
63

o
1
DBTBRMlNANTS OF PRIMARY PREVENTIVE PRACTICBS OF
GBNERAL PRACTITIONBRS IN TORINO. IT ALY
Key words:
Running head: Primary Preventive Practices in Torino
Primary prevention, general practice, patterns of practice.
Stefano Rosso, M.D.*,** Renaldo N. Battista, M.D., Sc.D.**
Nereo Segnan, M.D., M.Sc.* J. Ivan Williams Ph.D.**
Samy Suissa Ph.D.*· Antonio Ponti, M.D., M.P.H.*
* From the Area di Epidemiologia, Unita' Sanitaria Locale 1, Torino, Italy
** From the Department of Epidemiology and Biostatistics, McGill University and the Division of Clinical Epidemiology, Montreal General Hospital, Montreal, Canada. Dr. Battista is a Research Scholar of the National Health Research and Development Program, Ottawa, Canada. Dr. Suis sa is a Research Scholar of the Fonds de la recherche en sant' du Qu'bec.
Address Reprint requests to: Dr. Stefano Rosso Area di Epidemiologia, Unita' Sanitaria Locale Torino l, Via San Francesco da Paola 31, Torino, ltaly 10123 Tel.:(l1) - 835386
(11) - 832004
64

ABSTRACT We conducted a studyof general practitioners in Torino, Italy, to determine
their patterns of preventive practice. A set of primary and secondary preventive
interventions and their determinants were examined. Seales were constructed to
encompass praetice behaviors, knowledge, beliefs, and barriers. Organizational
aspects of health care in Italy, and physicians' lifestyle were considered in the
analysis.
In this article we explore the determinants of primary preventive interventions,
including anti-smoking and alcohol abuse counselling, counselling for prevention of
accidents at home among the elderly, flu vaccination for the elderly, and counselling on
contraceptive use.
The explanatory factors were grouped in cognitive, socio-demographic, and
organizational. Different patterns emerged for each maneuver. Cognitive factors
played an important role, but their importance varied for each intervention. Smoking
behavior of physicians was found to be the major predietor of anti-smoking
counselling.
The importance of better understanding determinants of practice behaviors is
emphasized for implementing strategies to enhanee the diffusion of effective
preventive techniques.
Key words: cancer prevention, primary prevention, general practice, patterns of
practice.
65
t
INTRODUCTION
The evo1ution of health care and monetary constraints in recent yean have
underscored the raie of prevention in primary care. A new èpproach wap proposed in
the 1ate seventies by Breslow and Sorners 1 , the Institute of Medicine- and the Canadian
Task Force on ~e Periodic Health Examination:!. Scientific evidence for the
prevention of several important health problems was reviewed. The loal was the
diffusion of recomrnended practices during patient visits for periodic or epiaodic caret
The proeess of implementation is neithel' complete nor uniform"-18• Sorne
practices, such as the prescription of Papanicolaou test for early detection of cervical
cancer, have received wide acceptance into Medical practice whereas others such as
counselling on accidents at home among the elderly have yet to be widely adopted.
We need a better understanding of the factors influencing integration of
preventive activities into medical practice. As most of the studies on diffusion of
preventive activities in primary care were conducted in countries with a fee-for
service or mixed fee-for-service 1 salary system-a- 51, we decided to explore practice
behaviors in a capitation system.
The Italian National Health Service (Servizio Sanitario Nazionale -SSN-),
founded in 1978, is based on Local Health Authorities whose administrators are elected
by the municipal government. Primary care, public health and hospitals are under their
jurisdiction. General Practice is done mainly by general practitioners, but it can also
include internists and surgeons devoting part of their time to primary caret General
practitioners are paid on a capitation basis for an allowed number of patients that
varies according to their professional commitments.
The object of our survey was ta study the attitudes and behaviors of primary
care physicians in Torino, Italy, with respect to primary preventive practices based on
recommendations from the Canadian Task Force on the Periodic Health
Examination3•20
-a :! and the U.S. Preventive Services Task Forcea4
-27
•
METHOns
A systematic sample of 225 general practitioners was drawn from the files of
66
;"

1
the Local Health Authority of Torino. The sample was stratified by qe, sex and
practice size, as measured by the maximum number of patients allowed under the
capitation system. Sixteen physicians refused to be interviewed (7.1").
Information was collected on items encompassing reported patterns of
preventive practice, perceived effectiveness of interventions, knowledge of the
diseases associated with smoking and alcohol abuse, and perceived barriers to the
implementation of specific preventive interventions in their medical practice. Also we
documented several practice features such as size of practice, group or solo activity,
type of training of physicians, and their personal health habits such as smoking.
The data were coUected through face-to-face interviews by three trained
interviewers and results were based on physicians' reports.
In the analysis of the data we created scales for anti-smoking and alcohol abuse
eounselling, knowledge, and barriers. Factor analysis28-28 was used to reduce items
to scale scores for counselling behaviors and barriers. Oo1y the items with factor
loadings of 0.4 on the principal factor were retained. Cronbach's alpha2ti1-
30 was used
to assess the internaI consistencyof each scale previously delineated through factor
analysis. The correlation matrices of each scale's items are presented in Appendix A
(Tables A.1-A.2). The total and partial scores for each scale were standardized using
Z-score transformation « score - mean ) / scale's standard deviation ).
Outcome variables.
The anti-smoking and alcohol abuse counselling seales were constructed by
eombining different items, including the type of clinical encounter during which
counselling was done (first visit, periodic check-up, visit for symptoms unrelated to
the risk factor), frequency of given counselling (always, often, seldom or never) and
the patients targeted by the intervention (a11 patients, high risk group only or
symptomatic patients).
The internaI consistency coefficient for the anti-smoking counselling items was
0.64. Alcohol abuse counselling items had an internaI consistency coefficient of 0.67.
Factor analysis showed a major scale factor for both scales, scores were normally
distributed, and the scales were left as continuous variables.
The questions on counselling for accidents in the elderly at home and giving of
67

J'f ,~ ~:- ,~ ~ 1 T q. v ... ' l • L ~ , '
a
contraception advice had four response categories (always, often, seldom or never
performed), and they were subsequently dichotomized for analysis.
Physicians were asked if they carried out flu vaccination for the elderly. A
score of 1 was assigned if the answer was positive and zero if patients were referred
to other services.
Determinants.
Knowledge of diseases caused by smoking and alcohol consumption was assessed
with two distinct seales. Physicians were requested to rate the evidence pertaining to
the associations between smoking and alcohol abuse with diseases on a four point scale
(strong, fair, poor, no evidence).
Physicians' self-confidence in the effectiveness of their interventions refers to
the doctors' beHefs that these interventions will reach the desired goals. Physicians
were asked to grade their confidence in the effectiveness of interventions on a four
level scale (very effective, rather effective, somewhat effective and never effective).
A "don't know" category was also included. For aIl practices, except counselling for
accident at home in the elderly, the frequencyof "don't know" was less than 5%. A
"don't know" response was recoded as a lack of perceived effectiveness (never
effective). Perceived effectiveness scores for anti-smoking and alcohol abuse
counselling were normally distributed. Perceived effectiveness scores for counselling
for prevention of accidents at home among the elderly, influenza vaccination, and
counselling on contraceptive use were bimodally distributed. Consequently we
dichotomized them.
GPs were also asked what problems they had encountered in implementing
smoking cessation and alcohol abuse interventions. Barrier scales were cons:tructed
including the following items: lack of knowledge, time constraints, time cost for the
patient, lack of monetary incentives, ove raIl cost of the procedure, accessibility, and
patients' compliance. The barrier scale for anti-smoking counselling had a borderline
internaI consistency coefficient of 0.60. It was normally distributed and was used in
the analysis as a eontinuous variable. The barrier seale for alcohol abuse counselling
had alow alpha and a skewed distribution. The variable was dichotomized into alow
score (physicians who had c1aimed none or one barrier) and high score (physicians who
68

had claimed 2 or more barriers).
The possibility of "collaborating" with other colleagues was thought to he
important in improving preventive practices7,31. Measurement of the level of
"collaboration with other colleagues" is based on two questions that elicit different
degrees of interaction with peers. The first question asks if there are other
physicians practising in the same office, and the second question focuses on the level of
collaboration with colleagues. Scores are: 0 (neither collaborate nor sbare office
facilities); 1 (share office facilities); 2 (attend occasional professional meetings); 3
(attend periodic professional meetings); 4 (manage common patients occasionally); 5 (sbare medical records and manage common patients). The scale showed a bimodal
distribution and for this reason was dichotomized in "solo" (scores 0 to 1) (64.1") and
"group" practice (scores 2 to 5) (35.~). Group practice is defined as physicians who
have periodic working meetings with other colleagues for discussing common
management of their patients or clinical cases.
We classified practitioners according to their main activity: full-time
practitioners (59.8%); internists devoting part of their time to primary care (25.8%): and surgeons devoting part of their time to primary care (14.4%).
Gender and number of years since graduation were also incorporated in the
analyses.
The distributions of variables included in the analysis are presented in Appendix
B (Tables B1-B5).
Analysis
For the continuous outcome variables (anti-smoking and anti-alcohol abuse
counselling), we used multiple linear regression analysis3a- n • A stepwise selection
procedure was applied in order to select the best fitting model using several variables
including knowledge, beliefs, barriers, daily intake of alcohol considered damaging and
number of years since graduation. A multiple-partial F test32 was used for
comparison of models when adding categorical variables (gender, categoryof
practitioners, collaboration with other colleagues, and smoking behavior). We
reassessed the significance of the first set of variables after inclusion of significant
categorical variables and analyzing residuals.
For the dichotomous outcome variables (flu vaccination for the eiderly,
69

, ,
•
t
<"
counselling for accidents at home among the elderly and counselling on contraceptive
use), multiple logistic regression analysis was used with a stepwise selection
procedurcl4-
3!1.
First order interactior .. terms were also considered in both analyses. Higher order
interaction terms were excluded because of difficulty in interpreting the models.
RESULTS
Different patterns of determinants emerged for each preventive practice. A
summary of the important predictors is given in Table 1, where determinants are
classified as cognitive, socio-demographic, and organizationaI. We presented summary
statistics for each model and measures of association such as partial correlation
coefficients for multiple linear regression models and adjusted odds ratios for logistic
models. Multiple regression models cou Id only explain between 7 to 10% of the
variance in practice behaviors, and logis tic models showed a limited goodness of fit.
The principal findings are discussed below for each intervention.
Anti-smoking counselling.
Our GPs claimed they gave repeated counselling in a high proportion (98%) of
their patients, but only 60% of them counselled aIl their patient smokers in accord an ce
to recommendations3•27
• The principal detenninants of anti-smoking counselling were
perceived effectiveness of counselling, smoking habits of physician, and category of
practitioners with partial correlation coefficients ranging from 0.13 to 0.23.
Physicians who are non-smokers have the highest adjusted score. Although
important differences exist in the adjusted mean scores between smokers and non
smokers (13% of the scale's overall range) and between ex-smokers and non-smokers
(7% of the scale's overall range) only the first comparison is significant (Table 2).
Intemists devoting part of their time to primary care had a higher counselling
score than full-time OPs or surgeons with part-time commit ment to primary care
(Table 2).
Younger physicians appeared to counsel their patients more frequently than their
70

) i, '. ;# .
oider colleagues, although number of years since graduation had borderline
significance. Most of the lowest scores were from a minority of oIder physicians.
When these outliers were removed from the analysis, number of years since graduatbn
was no longer a significant predictor of practice.
Perceived effectiveness of anti-smoking counselling was also an important
determinant, contributing about 15% of the variance explained by the model.
Alcohol abuse counselling.
Counselling for preventing alcohol abuse was reported by 97% of GPs, although
the intervention was considered less effective tban anti-smoking counselling. Levelof
knowledge, and number of years since graduation were important determinants of this
practice. Younger physicians with a better training (higher knowledge score)
counselled their patients more on alcohol-abuse. The poor fit of the model (R-square
of 0.08) however, underscores the need for a better theoretical model that would
include other determinants, and more precise measurements.
Counselling for accidents at home among the elderly.
About half of the physicians (47%) reported they counselled elderly patients on
prevention of accidents at home. GPs can refer their patients to social services
directly supported by the local community, and 36% of them reported to have referred
their elderly patients because of the presence of environmental hazards at home which
could result in faIls and injuries.
Factors associated with this type of counselling were, the perceived
effectiveness of counselling (50.7% of GPs perceive counselling as very or rather
effective), and a good working relationship with social services which offer support
and help to the elderly. Only 17.7% of interviewed physicians had a good working
relationship with social services and referred their patients to them.
Flu vaccination.
Eighteen percent of physicians directly administered flu vaccine to the elderly.
The remaining physicians frequently referred patients to vaccination centres within the
SSN.
71

~ .... ~ , ,,'
In the logistic regression, perceived effectiveness of the flu vaccination among
patients over 6S years of age was only marginally related to practice. Physicians who
perceived flu vaccination as very or rather effective (78.0%) were three times more
likely to carry it out.
Counselling on contraceptive use.
Although the majority (92%) of GPs considered contraception effective in
preventing unwanted pregnancies, ooly 34% of them actually counsel their patients.
Many of them (82%) refer their patients to specialized services.
Pemale physicians in group practice were the mostly likely to provide such
advice.
DISCUSSION
Patterns of preventive practices result from the interaction of several factors,
and various classifications of determinants have been proposed. Green et al.38
classified the factors into three categories, predisposing, enabling, and reinforcing
factors. The three sets are not mutually independent and are difficult to put in
ope rational terms. We preferred to classify them in cognitive, socio-demographic, and
organizational factors as proposed by Battista et a1.37-
38• Nevertheless, as noted in
other studies9• 39-41 ,determinants work differently for each preventive practice and a
more efficient theoretical framework is needed.
Smoking counselling has been studied by several authors8• 37-43 a.nd similar
patterns of determinants have been recognized. Other studies have documented that
internists seem to be more oriented towards counselling 13-14. 31 .44-45.
Younger physicians offer both anti-smoking and alcohol abuse counselling more
often than their oIder colleagues~ thus reflecting a change in the training received in
more recent years.
Recommendations for the inclusion of counselling on accidents in the home
72

among the elderly have only recently been considered by the US Preventive Services
Task Forcelt ... Even though the prevention of home accidents is recognized by our
physicians to be an important public health issue, this intervention is DOt yet part of
their usual medical practice.
Perceived effectiveness of flu vaccination for the elderly was the oo1y
significant predictor of its use, whereas other studies have also found that younger and
board-certified physicians were more likely to meet these immunization guidelineslt7•
Gender and group practice were found to be the key factors associated with
contraception counselling.
The analysis of the se data is the first attempt to investigate the determinants of
physicians' primary preventive practices in Italy and to compare them with studies in
other countries.
Our study showed that in general, prevention is carried out by physicians at a
comparable level with similar determinants. Local organizational features, such as
availability of other primary care services, are also important factors modulating the
level of preventive care offered by physicians.
Any attempt at improving physicians' performance in preventive care should take
these factors into account, and consider physicians' involvement in prevention in the
broader context of public health efforts.
73

1.
REFERENCES Breslow L, Somers AR. The lifetime health-monitoring program: a practical
approach to preventive medicine. N Engl J Med 19n;296:601-608.
2. Institute of Medicine. Preventive Services for the Well Population. Report of the
Institute of Medicine, National Academy of Science, Healthy People
(appendices), 1-22. Washington, US Department of Health, Education and
Welfare 1978. 3. Canadian Task Force on the Periodic Health Examination. The periodic health
examination. Can Med Assoc J 1979;121 :1194-1254.
4. Battista RN. Adult cancer prevention in primary care: patterns of practice in
Qu'bec. Am J Public Health 1983;73(9):1036-1039.
5. Battista RN, Palmer CS, Marchand BM, Spitzer WO. Patterns of preventive
practice in New Brunswick. Can Med Assoc J 1985;132:1013-1015.
6. Catford JC, Nutbeam D. Prevention in practice: what Wessex General
Practitioners are doing. Br Med J 1984;288:832-834.
7. Gemson OH, Elinson J. P~evention in primary care: variability in physician
practice patterns in New York City. Am J Prev Med 1986;2:226-234.
8. Goldstein B, Fischer PM, Richards jW, Goldst'!in A, Shank je. Smoking
counseling practices of recentIy trained Family l">hysicians. J Fam Pract
1987;24( 2) :195-197.
9. Lurie N, Manning WG, Peterson C, Goldberg G/. t Phelps CA, Lillard L.
Preventive Care: do we practice what we prea(;h? Am J Public Health 1987;
10. Orleans CT, George LK, Houpt JL, Brodie KH.Health promotion in primary
care: a survey of U.S. Family Practitioner:i. Preventive Medicine 1985;14:636-
647. 11. Rigotti NA, Calkins DR, Gordon NP, Cleary PD.Do Physicians advise petients
about health practiccs, and does it make a difference? Clinical Research
11985;33:73-85. 12. Romm F J, Fletcher SW, Hulka BS. Periodic health examination: comparison of
recommendations and internists performance. So Med journal 1981;74:265-271.
13. Val ente CM, Sobal J, Muncie HL, Levine DM, Antlitz M. Health promotion:
physicians' beliefs, attitudes and practices. Am J Prev Med 1986;2:82-88.
74

'e
14. Wechsler H, Levine S, Idelson RK, Rohman M, Taylor JO. The physician's role
in health promotion: a survey of Primary Care Practitioners. N Bill J Med
1983;308 ( 2) :fJI-1 00. 15. Wells m, Lewis CE, Leake B, Ware JB Jr. Do physician preach what they
prar.ticû JAMA 1984;252:2846-2848.
16. Blford W. Patterns of preventive practice of Southern Alberta Family
Physicians. Department of Family Medicine, Univ~rsity of Calgary, 1987.
17. Ho A, Herbert C, Farrall J. Periodic health scrr,t,;;ng: what members of the
Department of Family Practice at the Vancouver General Hospital are doing.
University of British Columbia, Department of Family Medicine, 1986.
18. Borgiel At Williams J, Anderson G, Bass M, Spasoff R, Dunn E, Lamont C.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
Assessing the quality of care in family physicians' practices. Can Fam Phys
1985;31 :853-862.
Audunnson G. Preventive infrastructure in family medicine; Master's thesis.
Department of Family Medicine, University of Western Ontario.
CSlladian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1984 update. Calll Med Assoc J 1984;130:1278-1292.
Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1985 update. C8IIl Med Assoc J 1986;134:724-729.
Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1987 update. Can Med Assoc J 1988;138:618-626.
Canadian Task Force on the Periodic Health Examination. The periodic health
examination: 2. 1989 update. Can Med Assoc J 1988;141:209-216.
U.S. Pr~ventive Services Task Force. Recommendations for breast cancer
screening. JAMA 1987;257(16):2196.
U.S. Preventive Service Task Force. Recommendations for prevention of
sexually transmitted diseases. JAMA 1987; 258(6):814.
U.S. Preventive Services Task Force. Recommendations for automobile
occupant protection counselling. JAMA 1988;259(1):76.
U.S. Preventive Services Task Force. Recommendations for smoking cessation
counselling. JAMA 1988;259(9):2882.
Zeller RA, Carmines EG. Measurement in the Social Sciences: The Link
75

between Theory and Data. Cambridge University Press, London 1980. - 29. SPSS Ine. Statistical Package for the Social Sciences. User's Guide 2nd ed.
McGraw-Hill, New York 1986.
30. Nunnally JC. Psychometrie Theory. 2nd ed. McGraw-Hill, New York 1978.
31. Radecki SE, Mendenhall RC. Patient counselling by primary care physicians:
results of a nationwide survey. Patient Education and Counselling 1986;8:165-
rn. 32. Kleinbaum DG, Kupper LL, Muller JŒ. Applied Regression Analysis and Other
Multivariable Methods. 2nd ed. PWS-KENT Publishing Company, Boston MA
1987. 33. Statistical Analysis System. Raleigh, NC: SAS institute INc., 1979.
34. Bishop YMM, Fienberg SE, Holland PW. Discrete multivariate analysis: Theory
and practice. MIT Press, Cambridge, Mass 1975.
35. BMDP Statistical Software. Departments of Biomathematics University of
California, Los Angeles. University of California Press, 1981.
Rf 36. Green LW, Eriksen MP, Schor EL. Preventive Practices by Physicians: \
Behaviourial Determinants and Potential Interventions. In Battista RN, Lawrence
RS, eds. Implementing Preventive Services. Am J Prey Med 1988;4(4)s:101-
107.
37. Battista RN, Williams IJ, MacFarlane LA. Determinants of primary medical
practice in adult cancer prevention. Med Care 1986;24(3):216-224.
38. Battista RN, Williams JI, McFarlane L. Determinants of preventive practices in
fee-for-service primary care. Am J Prev Med (Submitted for Publication).
39. Cummings KM, Giovino G, Sciandra R, Koenisgsberg M, Emont SL. Physician
advice to quit smoking. Who gets it and who doesn't? Am J Prev Med 1987:3:69-
75.
40. Maheux B, Pineault R Beland f. Factors influencing physicians' orientation
toward prevention. Am J Prey Med 1987;3:12-18.
41. Lewis CE, Wells KB, Ware J. A model for predicting the Cot.mse1l~ Practices
of Physicians. J Gen Intern Med 1986;1:14-1<).
42. Attarian L, Fleming M, Barron P, Strecher V. A CompArison of health promotion
practices of general practitioners and reside.ne)' trained famHy physicians. J , 76

Comm Health 1987;12(1):31-39.
43. Wells KB, Ware JE, Lewis CE. Physicians' attitudes in counsellinl patients
about smoking. Med Care 1984;22(4):360-365.
44. McAlister A, Mullen PD, Nixon SA, Dickson C, Gottlieb N, McCuan R, Green L.
Health promotion among primary care physicians in Texas. Texas Medicine
1985;81 :55-58.
45. Wells KB, Lewis CE, Leake B, Schleiter MK, Brook RH. The practices of
general and subspeciality internists in counseling about smoking and exercise.
Am J Public Health 1986:76(8):1009-1013.
46. Hindmarsh], Estes EH, Scatartige C. Falls in the elderly: etiology and
intervention. Unpublished draft for the US Preventive Services Task Force ju1y
1987 meeting.
47. American College of Physicians, Committee on immunization. Guide for adult
immunization 1985. Philadelphia: American College of Physicians 1985.
48. Pineault R. The effect of prepaid group practice on physicians' utilization
behaviour. Med Care 1976;14:121.
49. Contandriopoulos AP. Stimulants iconomiques et utilisation des services
midicaux. Act Eeon 1980;56:264.
50. Rice T. The impact of changing Medicare reimbursement rates on physicians'
induced demand. Med Care 1983;21 :803.
51. Manning WG, Leikowitz A, Goldberg GA. A controlled trial of the effect of a
prepaid group practice on use of services. N Engl J Med 1984;310:1505.
77

•
TAIlLE 1
P.·Ual correlation coefficients (r) and adJusted odds ratios (or) for use of pri .. y preventive interventions (Logistic regres.ion 95_ Confidence intervals of odds ratios in parenthesis)
Prift8r~ 2[eventlve interventions Predietor variables
Alcohol Counselling for Anti-SIIIOking abuse accidents at home Flu Contraception counselling counse1l1ng among the elderly Vaccination counsell1ng
Perceived (or) 27.1 (or) '.1 effeetiveness (r) 1.14. (2.2,81.8) (1.9,111.')
Knawledge (r) Il.19**
Vers slnee graduation (r)-I.l'· (r)-II.2I··
SIoking behavior of physiciens (reference category -non SIIIOkers- ) (r)-1.2'··
Gender of (or) Il.' physicien (1.1,1.6) (reference category -female-)
C8tegory of Practitloners (reference category Gps full-Unie ) (r) Il.18.
Good vs poor (reference category) working relation with (or) 6.11 sociel services (2.4,15.9)
Group vs solo (referenee cetegory) (or) 1.8 practice (1.1,'.')
SUmmary statistlcs for IIIOdels
R-square Il.''''' Il.118''' AdJusted R-square .11.111 Il.117
P- value for Goodness of fit Chi-square 8.98 8.93 1.111
'p<8.B5 "p<8.B1 "·p<8 . .,B\
78
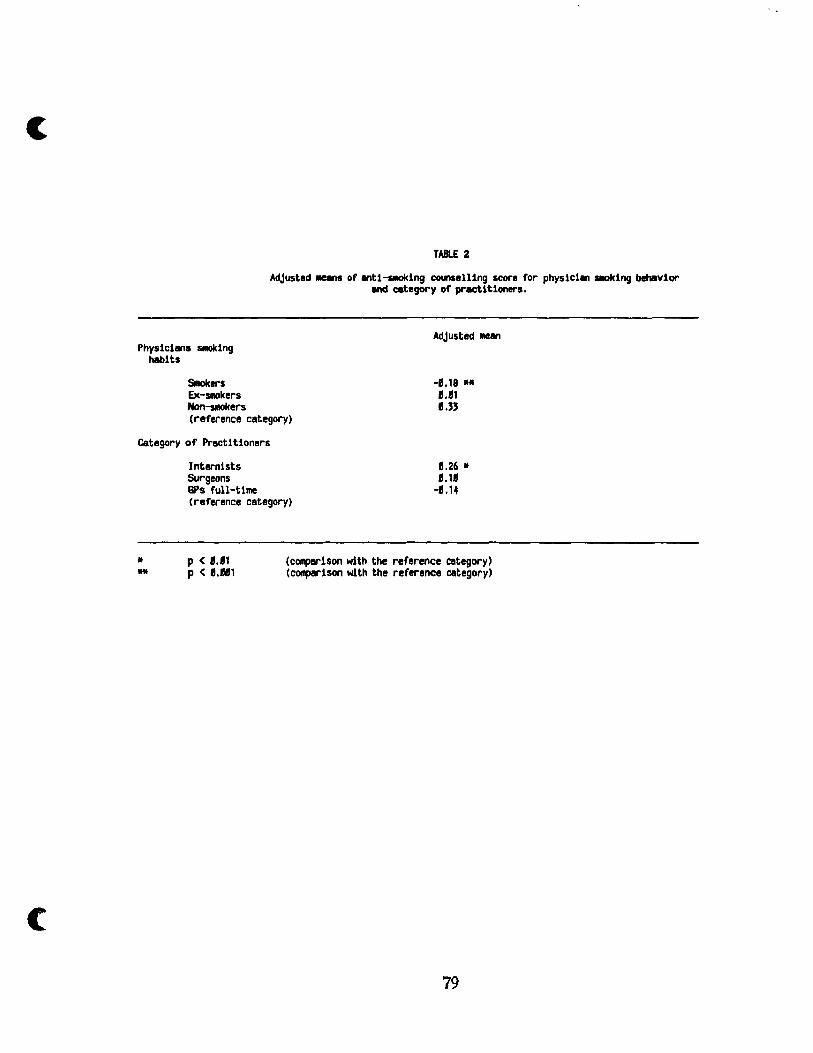
(
TABlE 2
Adjusted MeanS of entl-SIOklng counselling score for physicien SIOklng behavlor end category of practtt1oners.
AdJusted Man Physiciens SIOklng
habits
SIIokers Ex-SIIOkers Non-SIIOkers (reference category)
-8.18 .. 8.81 8."
Category of Practltloners
* ..
Internists Surgeons GPs full-Ume (reference category)
8.26 * 8.18
-8.14
p < 8.81 P < Il.11111
(comparlson with the reference category) (comparlson with the reference category)
79

'f"" " , ft '<.--~-.f,·--
APPOOIX A
o Correlation Matrices of Scale ft.
TABLE Il.1
Antl-SMoklng Counselling Items
2 , 4
CcMJnselllng durlng lst visU 1.1111
2 CcMJnsel11ng during ~al check-ups Il.'11 1.1111
, Counselllng durlng vls1ts for problems not related to s.oklng Il.'4 8.54 1.811
4 Targeted population (ail SIOkers. heavy s.okers. smokers with l~tOlllS) 8.119 8.22 Il.32 1.1111
Correlation ~, fI.'1I17 Correlation standard error Il. 1484
Antl-IIlcohol Abuse Counselling Items
2 , 4 5
Counselling durlng lst vlslt 1.1111
2 Counselling during general check-ups Il.411 1.111
, Counselling durlng vls1ts for problems not related to alcohol abuse ".," Il.56 1.1111
4 Targeted population for one-Ume counselling (ail drlnkers. heBvy drlnkers. drinkers wl th symptoms) Il.17 Il.16 Il.25 1.1I1l
Targeted population for repeBted counselling Il.27 Il.14 Il.22 Il.49 Lell
Correlation mean Il.29611 Correlation standard error Il.14'5
80

i. ; • 1 li J
TAIlLE A.2
Antl-SMoklng Counselllng Barriers
2 , 4 5 6 7
1 Lack of training 1.11.
2 Physicl .. 's tille constralnts Il.24 1.1111
, Patient's tille constralnts Il.1' Il.'7 1.1111
4 Lack of IIOnetary lncenUves Il.15 Il.27 Il.11 , .11
5 Accessibil1ty 1.17 Il.17 •• 14 1.19 1.1111
6 Costs for patients Il.2' Il.21 Il.2' Il.14 1.117 LIli
7 Avallab1Uty of te.:hnique 1J.28 1J.19 1J.15 Il.87 8.16 Il.'9 1.811
Correlation Mean Il.1928 Correlation standard error Il.118486
c 81

1
, ; .
Standardized scores
1.' - 1.2 1.1- 1.1 Il.9 - 1.8 Il.7 - 1.6 Il.~ - 1.4 Il.' - '.2 Il.1 - 1.1
Il.11 - -11.1 -11.2 - -II.' -11.4 - -11.5 -1!.6 - -11.7 -11.8 - -11.9 -1.11 - -1.1 -1.2 - -1.' -1.4 - -1.5 -1.6 - -1. 7 -1.8 - -1.9 -2.11 - -2.1 -2.2 - -2.' -2.4 - -2.5
Standardized scores
1.9- 1.5 1.4 - 1.11 Il.9 - Il.5 Il.4 - Il.' Il.11 - -11.4
-II.~ - -11.9 -1.11 - -1.4 -1.~ - -1.9 -2.11 - -2.4 -2.~ - -2.9
APPENlIX 8
DISTRIBUTHW CE VARIABLES INl.t.ŒD IN ANAlVSIS
TABLE B.l
Distribution of standlrdized Anti-SMoklng Counselling Scores
Frequencv
42 Il
14 17 Il
21 18 7
14 22 2 1~ 9 2
12 6 , 2 2 1
Distribution of standardized Alcohol Abuse Counselling Score'
Frequency
18 17 41 24 29 49 19 11 7 1
82

(
Rank of knowledge scores (Highest to lowest)
1 2 , 4 5 6 7 8 9 l'
Rank of 1Cnow1edge Scores (Hlghest to lowest)
1 2 , 4 5 6 7 8 ,
TAIlLE B.Z
Distribution of SIIoIcing Knawledge Scores
Frequency
4 29
" ., '8 15 11 14 8 8
Distribution of Alcohol Abuse Knowledge Scores
Frequency
8 64 '2 ., 22 24 12 , 1
83

o
~~ c-~ t'"""'~~ - - ~ v Of' "
Rank of IIrrlers scores (Hlghest to l~st)
1 2 , 4 5 6 7 8
TABlE B.'
Diltribution of Anti-SIoklng Counselling Barriers
Frequency
TABLE 8.4
Perceived Effectiveness of Anti-Smoking and Alcohol Abuse Counselling
Very Effective Rather Effective SeldOil Effective Hever Effective
Don't know
Vears
< 5 5 - 7 8 - 18
11 - 1; 16 - 28 21 - 25
26 - " " - '5 '6 - 48 41 +
Frequency Antl Smoking Counselllng Alcohol Abuse Counselling
67
" 48 11
TABLE B.5
Vears Since Graduation
Frequency
2 44 46
" " 15
" 2' 15 7
84
19 58 59 48
15
(
DETERMINANTS OF CANCER EARLY DETECTION PRACTICBS
OF GENERAL PRACTITIONERS IN TORINO, ITALY.
85
il : ,-," , ,

o PRESENT A TION OF THE ARTICLE
In paper 2, the determinants of primary preventive interventions were examined
and classified as cognitive, sociodemographic, and organizational. Different patterns
of determinants emerged for each intervention.
In paper 3, we explore the determinants of early detection practices for lung,
cervical, and breast cancer. Scales were constructed to measure practices,
knowledge, beliefs, and barriers and the determinants were analyzed separately for
each early detection technique.
Paper 3 was written by the author of this thesis, under the supervision of Drs.
Renaldo N. Battista, Nereo Segnan, J. Ivan Williams, and Samy Suissa, and in
collaboration with Dr. Antonio Ponti.
86

c
Key wards:
DETERMINANTS OF CANCER EARLY DETECTION
PRACTICBS OF GENERAL PRACTITIONERS
IN TORINO, IT ALY
Running head: Cancer Prevention Practices in Torino
Cancer prevention, general practice, patterns of practice.
Stefano Rosso, M.D.*,** Renaldo N. Battista, M.D., Sc.D.**
Nereo Segnan, M.D., M.Sc.* J. Ivan Williams Ph.D.**
Samy Suissa Ph.D. ** Antonio Ponti, M.D., M.P.H.*
* From the Area dl Epidemiologia, UnHa' Sanitaria Locale 1, Torino, Italy
i !,
** From the Department of Epidemiology and Biostatistics, McGill University and the Division of Clinical Epidemiology, Montreal General Hospital, Montreal, Canada. Dr. Battista is a Research Scholar of the National Health Research and Development Program, Ottawa, Canada. Dr. Suissa is a Research Scholar of the Fonds de la recherche en sant6 du Qu6bec.
Address Reprint requests to: Dr. Stefano Rosso Area di Epidemiologia Unita' Sanitaria Locale Torino If Via S. Francesco da Paola 31, Torino, Italy 10123 Tel.:(l1) - 835386
( 11) - 832004
87

ABSTRACT
We surveyed general practitioners in Torino, Italy, to ascertain their patterns of
primaryand secondary preventive practices and their determinants. Scales were
constructed encompassing practice behaviors, knowledge, beHefs and barriers.
Organizational aspects of health care in Italy, and physicians' lifestyle were also
considered in the analysis.
In this article we focus on early detection of lung (chest x-rays and sputum
cytology), breast (mammography, physical examination, and teaching of breast self
examination), and cervical (Papanicolaou smear) cancers.
The explanatory factors were grouped as cognitive, socio-demographic, and
organizational. Different patterns emerged for each maneuver. Cognitive factors
(perceived effectiveness and knowledge) are important predictors of use of early
detection techniques. The availability of other primary care services is an important
factor in the early detection of gynecological cancers. Given the importance of
cognitive determinants, continuing education programs are warranted in changing
patterns of early detection practices.
Key words: Cancer prevention, early detection, general practice, patterns of
practice.
88

INTRODUCTION
A planned approach for the use of early detection techniques was proposed in the
late seventies by the Canadian Task Force on the Periodic Health Examination as weIl
as others1-
3• It is based on age- and sex-specific health protection packages. In
Europe, practice guidelines have been formulated mainly by the International Union
Against Cancer4•
The Italian National Health Service (Servizio Sanitario Nazionale -SSN-),
founded in 1978, is based on Local Health Authorities whose administrators are elected
by the municipal government. Primary care, public health and hospitals are under their
jurisdiction.
General Practice is done mainly by general practitioners, but sorne internists and
surgeons devote part of their time to primary care. General practitioners are paid on a
per capita basis for an allowed number of patients based on their professionsl
commitments. GPs provide free and accessible primary care and act as "gatekeepers"
within the SSN. However, patients May go directly to vaccination centers and
"consultori" or clinics specialized in family planning, gynecological disorders and
sexual counselling.
The diffusion of preventive practices has been studied in countries that have
fee-far-service or mixed fee-for-service 1 salary systems. We explored patterns of
primaryand secondary preventi'.re practice in a group of italian primary care physicians
reimbursed on a capitation basis.
In this article we present the analysis of the determinants of early detection of
lung, breast and cervical cancers.
MBTHODS
We interviewed 225 general practitioners practising in Torino, Italy. They
were systematically selected after stratification by age, sex and maximum number of
patients allowed. Sixte en physicians (7.1%) refused to be interviewed.
Information was coUected on reported patterns of preventive practice, perceived
effectiveness of interventions, knowledge of the risk factors associated with the three
89

r r
f.
i' <
(
c
cancers under study and perceived barders to the implementation of specifie preventive
interventions in their medical practiee. Also, specifie features of physicians' practice
setting, their specialty, and their health behaviors were documented.
The data were collected through face-to-face interviews by three trained
interviewers and results were based on physicians' reports.
We used factor analysis5-
6 to reduce items to seale scores for deteetion
practices, and Cronbach's alpha to assess the internai consistency of each scales - 7•
Outcome variables.
There was no internaI consistency between the items on che st x-rays and sputum
cytology and on mammography, physical examin3.tion performed by physicians and
teaching of breast self-examination. Consequently we analyzed the determinants
separately for each intervention.
Most of the outcome variables, except the teaching of breast self-examination,
had bimodal distributions and they were subsequently dichotomized.
Patterns for the teaching of breast self-examination were delineated through
two questions on the targeted patients and the follow-up strategy of thcse patients.
Items were eombined in a seale with six levels.
We analyzed prescription of mammography, as a dichotomous variable, assigning
a score of one to physicians who prescribed mammography as an early detection
technique (annually for women 50 to 59 years of age, women with low parity, and
women with family history of breast cancer) (31.5%), or a score of zero if physicians
prescribed mammography in already symptomatic women (68.5%).
Twenty one percent of GPs performed breast examination in a11 asymptomatic
women during visits not for gynecological disorders. In the analysis this group of
physicians was given a score of one.
The scale for prescription of Papanicolaou test for early detection of cervical
cancer was based on questions pertaining to th\~ age groups screened, the periodicity of
Pap test prescription, and follow-up of patients. These items had an interna!
~onsistency coefficient (alpha) of 0.74 (see correlation matrix in Appendix A) and
factor analysis fitted the items into a single dimension. As the resulting seale had a
bimodal distribution, it was subsequently dichotomized for analysis, with 66.S% of the
90
,J ,l , ,

1 GPs in the high score group.
Adoption of chest x-rays and sputum cytology for lung cancer early detection
were dichotom;zed for analysis.
Determinants.
Knowledge of risk factors for breast and cervical cancer was assessed with
separate scales. Physicians indicated on a four level scale their knowledge of the
existing evidence about risk factors for breast and cervical cancer (strong, fair, poor,
no evidence).
Physicians' confidence in the effectiveness of an intervention is referred to as
"perceived effectiveness" or "self-efficacy belief". Physicians were asked ta grade
their beliefs on the effectiveness of interventions on a four level scale (very effective,
rather effective, somewhat effective and never effective). A "don't know" category
was also included. For aIl the interventions there were very few "don't know" answers
(below 1%). They were recorded as lack of perceived effectiveness (never
~ffective). This variable was continuous in the lung and breast cancer detection
models, while it was dichotomized in the ce:vical cancer detection model (it was
skewed towards positive values) (89.0% of Gl's).
Information on practice organization allowed us to differentiate between GPs
who have a solo (64.1%) or group practice) (35.9%). We also asked physicians about
their perceived role in preventing gynecological cancer and their professional
relationship with gynecologists and "consultori".
We c1assified practitioners according to their specialty: full-time practitioners
(59.8%); internists devoting part of their time ta primary care (25.8%); and surgeons
with sorne primary care practice (14.4%).
The distributions of variables inc1uded in the analysis are presented in Appendix
B (Tables BI-B3).
Analysis
We used multiple linear regression ta examine the continuous outcome variable
"teaching of breast self-examination", and the best-fitting model was identified through
a stepwise selection procedures- e • For the dichotomous ontcome variables (chest x-
91
c
,C
rays, sputum cytology, mammography, breast examination, and pap-test), logistic
regression was used with a stepwise selection procedure 10-11.
First order interaction terms were also considered in both analyses. Higher
order interaction terms were excluded bec.ause of difficulty in interpreting the models.
RESULTS
Different patterns of determinants emerged for each preventive practice. In
Table 1 we present a summary of the results with meaS'Jres of association, such as
partial correlation coefficients for multiple linear regression models, and odds ratios
for logistic models. Summary statistics for each model are also presented.
The multiple regression model could only explain alx..lt 7% of the variance in
practice behavior , while the logistic models showed a limited goodness of fit.
Lung Cancer.
There are no effective screening techniques available for the early detection of
lung cancer; nevertheless 30.6% of GPs in our sample used che st x-ray Emd 12% sputum
cytology for this purpose.
Perceived effecti"eness of early detectior. was the most important predictor of
the use of che st x-ray. Male physicians were more likely to prescribe radiograms for
early detection of lung cancer than their female colleaguet ev en after adjusting for
speciality and years since graduation.
None of the studied variables could explain the use of sputum cytology.
Breast Cancer.
Only 10% of our physicians used mammography as a screening procedure in
asymptomatic women 50 to 59 years of age as recommended.
The use of mammography seems to be influenced mostly by the degree of
perceived effectiveness of the procedure. Alsot younger GPs order mammogram more
often than their older colleagues. Full time G Ps and surgeons devoting part of their
92

, 1
t
time as general practitioners prescribe mammograms as an early detection technique
more often than their internist colleagues.
Physicians in our study were less likely (21%) to carry out breast examination
than physicians in other studies 13,14,16,19, where rates of adoption ranged from 77%
to 99%. A possible explanation could be their preference to send patients to
gynecologists or to "consultori". Female physicians are more likely to carry out breast
examination in asymptomatie patients than male. Aiso a better knowledge of breast
cancer risk factors is associated with greater integration of the procedure into the
usual medicai practice.
Most GPs in our sample (87%) teach BSE to their patients, but only 25% of them
follow patients to ensure it is being performed properly. About 21% of the physicians
refer patients to a gynecologist or a "consultorio".
Belief in the effeetiveness of the procedure is the most important determinant
of this maneuver, with a partial correlation coefficient of 0.23. Physicians who teach
BSE and follow their patients (high score) are more likely to c1aim an active role for
General Practitioners in preventing gynecological cancers (69.0% of GPs).
Cervical Cancer.
The Papanicolaou smear is a weIl accepted practice, but GPs in our sample tend
to prescribe it more for women after age 35 than for younger women21• Determinants
of early detection of cervical cancer were found to be the qge of physicians, and
perceived effectiveness of the Pap test.
DISCUSSION
Since the introduction of the concept of integration of preventive activities in
primary care, determinants of this integration have been assessed. No single
explanatory model has emerged, rather the patterns of determinants seem to be
condition and maneuver specifie. The results of our study eonfirm this finding.
We c1assified determinants as cognitive, socio-demographic and organizational
as proposed elsewhere22-
23• In general, cognitive factors (perceived effectiveness
and knowledge) played the most important role in determining patterns of early
93

(
(
detection practice (Table 1), in agreement with other studies 12 • 1 &. 2,. •
A similar pattern of determinants (mainly cognitive and organizational factors)
was also found in our analysis of primary preventive practices2Q, underscoring the role
of continuing education programs in modifying practice patterns.
However, a note of caution must be introduced as the causallink between
education and beHefs is not yet weIl understood. Other factors such as positive
feedback from patients and peers can encourage the process of implementation of new
techniques:!5.
Demographic factors such as seniority in the profession and gender of
physicians play an important, Etlbeit lesser, role in shaping practice behaviors. F emale
physicians seem to be more sensitized to the problem of breast cancer than their male
colleagues. As suggested in the literature, a better doctor-patient relationship for
women physicians could explain their higher involvement in early detection of
gynecological cf.ncers26-
28•
The higher use of chest x-ray by male GPs, as found in our study, was not
confirmed in other studies22• 23.
Recently graduateci GPs are more likely to pre scribe mammography and Pap
test. A greater emphasis on these techniques in medical schools in recent years could
explain these findings, also reported in other studies 12.15.22-24.
Beyond these cognitive and demographic determinants, organizational factors
influence practice behaviours. Type of activity or specialization and perceived role of
physicians in prevention of gynecological cancers appear to be important predictors of
use of mammography and teaching of BSE. Surveys showed that gynecologists are
more apt to follow preventIve guidelines about mammography than other
specialists 17.34. In our sample, surgeons including gynecologists and obstetricians do
mammogram for early detection of breast cancer more often than full-time GPs and
internists.
Sorne authors23 have found other organizationaIfreatures to be important
determinants of preventive practices such as greater accessibility of the practice and
practice volume. The introduction of monetary incentives in fee-for-service settings
has also been proposed for improving physicians performances22-
23• 30-33. In a
capitation system such as in Italy, cognitive factors seem to carry a lot of weight in
94

-
• shaping practice patterns.
,
In this context, a strateg'f for improving physicians' preventive practices should
include reorientation of continuing education programs towards preventive m,!dicine, the
introduction of appropriate inr,entives, and a better coordination of GPs' actïvities with
other primary care services.
95

(:
(
REFERENCES
1. Frame PS, Carlson SJ. A critieall'eview of periodic health sereening using
specifie screening criteria. Part 1. Seleeted diseases of respiratory,
cardiovascular, and central nervous systems" J Fam Pract 1975;2:29-36.
2. Breslow L, Somen; AR. The lifetime health-monitoring program: a praetieal
approaeh to preventive medicine. N Engl ] Med 1977;296:601-608.
3. Canadian Task Force on the Periodic Health Examination. The periodie health
examination. Can Med Assoc J 1979:121:1193-1254.
4. Basson EC. The role of the doctor in public education. Health Education,
Theory and Practh:e in Cancer Control, UIeC Teehnical Report Series, vol. 10,
1974. 5. Zeller RA, Carmines EG. Measurement in the Sociai Sciellc~s: The Link
between Theory and Data. Cambridge University Press, London 1980.
6. SPSS Ine. Statistical Package for the Social Sciences. User's Guide 2nd ed.
McGraw" Hill, New York 1986.
7. Nunnally JC. Psychometrie Theory. 2nd ed. MeGraw-Hill, New York 1978.
8. Kleinbaum DG, Kupper LL, Muller KE. Applied Regression Analysis and Other
Multivariable Methods. 2nd ed. PWS-KENT PubUshing Company, Boston MA
1987. 9. Siatistieal Analysis System. Raleigh, Ne: SAS institute INc., 1979.
10. Bishop YMM, Fienberg SE, Rolland PW. Discrete multivariate analysis: Theory
and praetiee. MIT Pre~s, Cambridge, Mass 1975.
11.
12.
13.
14.
15.
BMDP Statistical Software. Departments of Biomathematics University of
California, Los Angeles. University of California Press, 1981.
Basset LW, Bunnel DH, Cerny JA, Gold RH. Screening m~mmography: Referral
practiees of Los Angeles physicians. A]R 1986;147:689-692.
Battista RN. Adult cancer prevention in primary care: patterns of practiee in
Qu'bec. Am J Public Health 1983;73(9):1036-1039.
Battista RN, Palmer CS, Marchand BM, Spitzer WO. Patterns of preventive
practice in New Brunswick. Can Med Assoc] 1985;132:1013-1015.
Cummings KM, Giovino G, Sciandra R, Koenisgsberg M, Emont SL. Physieian
96

advice to QUit smoking. Who gets it and who doesn't? Am J Prey Med 1987;3:69-
1 75.
t
16. Gemson DH, Elinson J. Prevention in primary care: variability in physilCÏan
practice patterns in New York City. Am J Prev Med 1986;2:226-234.
17. American Cancer Society. Survey of physicians' attitudes and practices in early
cancer detection. CA. 1985;35(4): 197-213.
18. Rosen MA, Logsdon DN, Demak MM. Prevention and health promotion in primary
care: Baseline results on physicians from the IN SURE Project on Lifecycle
Preventive Health Services. Prev Med 1984;13:535-548.
19. Canadian Task Force on the Periodic Healtl. ~xamination. The periodic health
examination: 2. 1984 update. Can Med Assac J 1984;130:1278-1292.
20. American Cancer Society. Guidelines for the cancer-related checkup:
recommendations and rational. CA 1980;30:193-240.
21 Segnan N, Battista RN, Rosso S, Ponti A, Senore C, Aimar D. Preventive
practices of general practitioners in Torino, Italy (Personal Communication)
22. Battista RN, Williams U, MacFarlane LA. Determinants of primary medical
practice in adult cancer prevention. Med Care 1986;24(3):216-224.
23. Battista RN, Williams JI. McFarlane L. Determinants of preventive practices in
fee-for-service primary care. Am J Prev Med (Submitted for Publication).
24. Woo B, Woo B, Cook EF. Weisberg M, Goldman L. Screening procedures in the
asymptomatic adult: comparison of physicians' recommendations, patients'
desires, published guidelines, and actual practice. JAMA 1985;254(11):1480-1484.
25. Green LW, Eriksen MP, Schor EL. Preventive practices by physicians:
26.
27.
28.
Behaviourial determinants and potential interventions. In Battista RN, Lawrence
RS, eds. Implementing Preventive Services. Am J Prev Med 1988;4(4)s:101-
107.
Gray J. The effect of the doctor's sex on the doctor-patient relationship, J R
Coll Gen Pract 1982;32:167.
Hopkins EJ. A study of patients' choice of doctor in an urban practice. J R Coll
Gen Pract 1%7;14:282.
Preston-Whyte ME, Fraser RC, Beckett JL. Effect of a principal's gender on
consultation patterns. J R Coll Gen Pract 1933;33:654.
97

(
'19. Rosgo S, Battista RN, Segnan N, Williams JI, Suissa S .. Dete11llinants of
primary preventive praetiee of general practitioners in Torino, Italy. (Personal
Communica tio!\).
30. Pineault R. The Effeet of prepaid group practice on physicians' utilization
behaviour. Med Care 1976;14:121.
31. Contandriopoulos AP. Stimulants iconomiques et utilisation des ser'lkes
midicaux. Act Eeon 1980;56:2.64.
32. Rice T. The impact of changing Medicare reimbursement rates on physicians'
indueed d'~:;land. Med Care 1983;21:803.
33. Manning ~~I G, Leikowitz A, Goldgerg GA. A Controlled trial of the effect of a
prepaid group practiee on use of the services. N Engl J Med 1984;310:1505.
34. Albanes Dt Weinberg GB, Boss L, Taylor PRo A survey of physician's
breast cancer early detection practices. Prev Med 1988;17:643-652.
98

o
t
TABLE 1
Prilal correlation coefficient.s (r) end adJusted oads ratios (or) for lise of orly dltecUon techniques (Logistlc r~gression 95_ Confidence int.ervals of odds rat:Js ln parenthesls)
Predictor variables
Perceived effectiveness
Knowledge
Vears since graduation
Sender of physicien (reference category
MIe - )
SUrgeons
GPs full-tlme
Internists (reference category)
Chest X-ray
(/Ir) 1.6 (1.2.2.1 )
(or) Il .• (8.2,1.11)
Role of GPs 1n Preventlng gynecologlcal cancers
Summary statlstics for models
R-square AdJusted R-square
p- value for GIlodness of fit Chi-square Il.1l4
·p<8.fl5 "p<lI.el '''p<8.881
(Oi') 2.11 (1.5.~.1I)
(or) Il.95 (8.95.11.98)
(or) 2.6 (8.9.7.2)
(or) 2.4 (1.1.5.5)
1.1'
fl.89
Earlv detectlon technlgue~
Breast examlnatlon
(or) 1.2 (1.11.1.4)
(or) 2.7 (1.2.5.9)
Il .• '
Teaching of BSE
(r) Il.15'
Il.118''' 8.117
Pep telt
(or) '.2 (1.'.8.4)
(or) Il.95 (11.96.11.97)
Il.11'

APPENlIX A
CMRELATlIIi MTRIX IF SCALE ITE/'IS
TABLE A.1
Cerviral Cancer DetectIon Scores
2 4
Pep test prescription 1.""
2 Follow-up of patients Il.51 1.118 , Repeated advice for earj" detection Il.61 Il.44 U.
4 Targeted population ( '5 yrs J'.52 Il.22 Il.'6 1.1111
5 Targeted popula~lon ~ '5 yrs 8.65 8.43 Il.62 Il.54 1.118
Corrplation llletln 8.4900 Correlat1on standard error ".1~19
(
100

Standardlzed scores
1.4 - 2.2 11.7 - ", lU - 8.6
-11.6 - lU -1.' - -8.7 -1.~ - -1.4
Rank of Knowledge scores (Highest to lowest)
l 2 , 4 5 6 7 8 9
HI 11
Rank of Knowledge scores (Highest to lowest)
1 2 , 4 5 6 7 8 9
-------------------------------------------~------...
APPOOIX 8 Distribution of Vcrlables Included in Analysis
TABLE B.1
Distribution of standardized Breast Cancer Detection Scores (Teachlng of Bre8st Self-Examlnatlon)
Frequency
19 19 27 91 26 27
TABLE 8.2 Distribution of Breast Cancer Knowle1ge scc"es
Frequency
, 8 7 9
25 37 29 59 26 11 5
Distribution of Cervical cancer Knowledge scores
Frequency
101
12 41 '4 5' 29 24 6 5 5
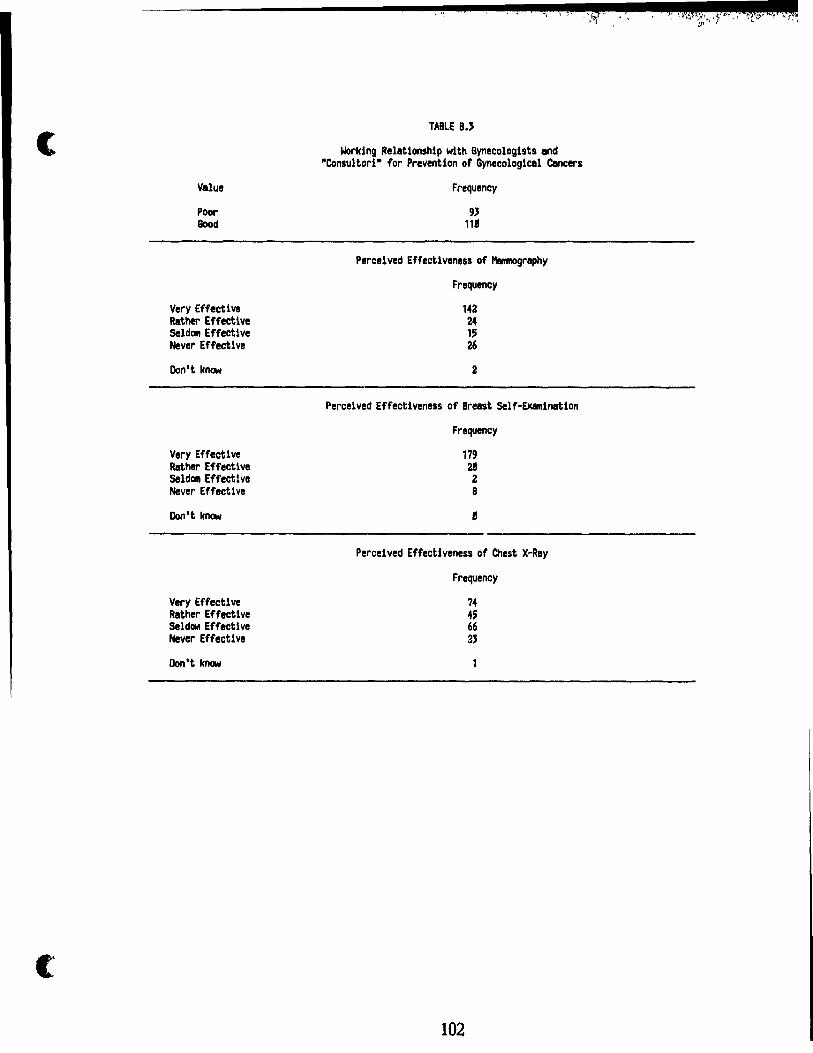
(
(
Value
POOl' Good
Very Effective Rather Effective Seldom Effective Hever Effective
Don't know
Very Effective Rather Effective Seldom Effective Never Effective
Don't know
Very Effective Rather Effective SeldOlft Effective Never Effective
Don't know
~; , ,!
TABLE B.'
Working Relationshlp with Gynecologlsts and ·Consultorl- for Prevention of Gynecologiesl Cancers
Frequency
9J lUI
Percelved Effectiveness of Mamnography
Frequency
142 24 15 26
2
Percelved Effectiveness of Breast Self-EXamlnatlon
Frequency
179 28 2 8
8
Perceived Effectiveness of Chest X-Ray
Frequency
102
,§.. i

.. .... -,.
CONCLUSION
Interest in prevention has grown, in recent years, not only among health
professionals but also among lay communities.
Environmental pollution and hazards, and the need for better health habits and strategies
for more efficient primary care services pose formidable challenges. Meeting their
increasing complexity, successfully, requires nrw and integrated approaches to
prevention.
Part of the challenge for improving health rests in physicians' practices, as
documented by the increasing portion of time allocated to preventive activities in family
medicine, general internaI medicine and other primary care practices.
There is now an evident and growing need for scientific methods for evaluating
the evidence of ef:ectiveness, and for sound policies for implementing effective
interventions in the most approp.iate and efficient way. Among the approaches put
forward, du ring recent decades, are those of the Canadian Task Force on Periodic
Health Examination, the U.S Preventive Services Task Force, and the National
Institutes of Health Consensus Conferences.
Different strategies have been proposed for diffusing and implementing
interventions, and it has been suggested that the capitation system is more successful in
inducing physicians to adopt preventive strategies. The more stable and dfdfined
population of patients in the capitation, vis-a-vis the fee-for-service system
makes it easier for physicians to have positive feed-back from their preventive
activities.
Our study documents preventive practices and their determinants in a sample of
general practitioners in Torino, Italy, where a capitation system was introduced with
the National Health Service, in 1978. During the debate on The Health Reform, and
since its adoption, the role of general practitioners and primary care physicians has
been widely discussed.
Although specifie bills created other preventive services in occupational hazards,
family planning, psychiatrie care, and drug addiction, The Health Reform also included
them in primary care without guidelines for their integration into GPs preventive
practices.
103

Although still general in nature, proposaIs about the implementation ~f preventive
strategies by GPs have subsequently appeared in such official reports and laws as the
General Practitioners' Contract in 1985 (Convenzione per la Medicina Generale) and
the Reports of the Piedmont Region on Organization of Health and Social Services
(Piano Socio-Sanitario della Regione Piemonte - anni 1983, 1986).
The organization described in our study is in effect throughout Italy and,
although sorne local differences may exist, the general findings of our study portray the
characteristics and behaviours of G Ps in most italian settings.
Our study indicates that the Italian capitation system is not clearly superior, if
physicians' attitudes are not taken into account, because estimates of the proportion of
physicians c1aiming to adopt practices are analogous to those found in other studies. On
the other hand, the SSN was created only recently and comparisons with data gathered
before its institution would be required to determine whether improvements have been
achieved. A comparison of our results with those of a similar survey conducted before
the institution of the SSN (Mossetti, 19n), showed an improved interest in prevention
and a better knowledge of preventive techniques, but the methods employed and the
selection bias in this earlier survey make its findings questionable.
Factors influencing preventive practice cannot be limited to type of
reimbursement. A complex pattern of determinants emerges from several studies
(Battista, 1986; Lurie, 1987; Maheux, 1987), and various classifications of determinants
and models have been proposed. The findings from these studies indicate that there are
separate patterns of determinants for each condition and intervention, but the precision
of the proposed models is quite poor and explain, at most, 20% of the variance.
In general, the main problems affecting the results of these studies are the
inadequacy of the measurement tools and the conceptualization of models. Nevertheless,
some factors appear consistently although with different weights.
Cognitive indicators, such as knowledge and perceived effectiveness, appear as
factors in both primary and secondary preventive interventions, in our study. Reviews
of other studies reveal a wealth of approaches in current use for improving physicians'
knowledge and attitudes towards prevention, but many are inadequately tested.
Recommendations, from these reviews, suggest the incorporation of elements from
different types of educationa} interventions (Haynes, 1984; Lomas, 1987).
104

• ....
In Italy, there is no official organization that provides specifie recommendations
in preventive strategies. Although a complete reformulation of practice
recommendations may not be necessary, assessing priorities, summarizing the state of
existing evidence, and supporting preventive interventions and their adequate diffusion
to practising c1i~icians, should be the initial tasks undertaken when responsibility for
them is assumed by sorne existing or yet-to-be-created organization.
Another issue that needs to be addressed is the integration of general practice
into other primary carl'. services, ·as illustrated by our findings on the way GPs oiten
refer their patients to other services and consultant specialists. The role of GPs as
gatekeepers for preventive interventions requires reconsideratio~ on the basis of an
understanding of whether it is more effective and efficient to keep sorne interventions
in general practice or to assign them to specialists with spedfic training.
Although prevention has evolved diff ~rently in various countries, the role of
physicians has become preeminent despite differing organizational solutions. Our study
is one of several that demonstrate the need for better integration of preventive
interventions in primary care, including the orientation of medical schools toward
prevention and the reformulation of continuing education programs .
105

c
(
t
1.
2.
REFERENCES
Battista RN, Williams n, MacFarlane LA. Determinants of primary medical
practice in ad1'lt cancer prevention. Med Care 1986;24(3):216-224.
Haynes RB, Davis OK, McKlbbon KA, Tugwell P. A critical appraisal of the
efficacy of continuing medical education. JAMA 1984;251:61-64.
3. Lomas J, Haynes RB. A taxonomy and critical review of tested strategies for the
application of clinical practice recommendations: from "official" to "individual"
clinical policy. In: Battista RN, Lawrence RS, eds. Implementing Preventive
Services. Am J Prev Med 1988;4(4)(suppl):77-94.
4. Lurie N, Manning WG, Peterson C, Goldberg GA, Phelps CA, Lillard L.
Preventive care: do we practice what we preach? Am J Public Health 1987;
5. Maheux B, Pineault R, Beland F. Factors influencing physicians' orientation
toward prevention. Am J Prev Med 1987;3:12-18.
6. Mossetti C, Sismondi GP, Panero M. TI comportamento deI medico nell'azione
preventiva antitumnrale, dati relatjvi ad un questionario inviato ai medici della
Provincia di Torino. Minerva Gynaecologica 1977;29:107.
106

o
APPENDIX
t 107

r, ~ •
: ~~ '.
.. il':,
LETTER dF PRESENTATION SENT TO PHYSICIANS. '
c ~.\ f NIZIO SANITARIO NAZIONALE Hb! jlONE PIEMONTE
SIIIa
Societ6 Italiana di Medicina Generale Sezione di Torino
(
U.B.L. TORINO 1-23
Alea di F.pidemiologia Alea dl Educazione Sanitaria
l' . 1 ~
( , J\)~" l '-..1
Tonno ••
Al Dr.
Egregio Collega,
col patrocinio dell'Ordine dei Medici della Provincia di Torino è
in corso un'indagine rispetto al ruolo che 11 medlco di Medicina Genera le svolge nel campo della prevenzione primaria e secondaria, ed agli ostacoli che eventualmente incontra.
Dall'elenco dei Medici dl Medicina Generale convenzionati con il SerVIZlO Sanitario Nazionale operanti a Torino è stato estratto a caso un campione di 225 colleghi, tale che sia assicurata all'indagine dal punto di vista statistico adeguata potenza e precIsione.
Il tuo no~e è compreso tra quello dei colleghl chiamati a partecipare aH' indagine, e non pua essere sosti bn to a pena dl ridurre la validltà dej risultatl. Ci permettiamo qUlndi dl chledere la tua gentile, personale collaborazione per una intervlsta della durata di circa 1 ora.
Il nostrO collaboratore che avrà )'incarico dl inter~istarti si met terà ln contat~o telefonicamente con te nel proSSlml giornj per stabillre ]'appuntam~nto.
Grazle u cordlaJi salutl
Dr. NJ~}t~ Respnnsah1]e dell'Area di Epidemiologia
'1
..1 '- -'~./ ~/VL---
Dr. Glùf'C':,pe Ventngl la
Respons~r,le RegIonale della Società ItaJ18w. j' :.'edlclna Generale
qi . , !f
f" .. :!'
.'
1
~.
.- ~ c ,-

;, : " .~ , , ..
.. r'~
-:.
- "
o SURVEY QUESTIONNAIRE,
INDAGlNE SULLA PREVENZIONE IN IlEDICINA GENERALE
condotta da:
- Area di Educazione Sanitaria. USL'Torino 1-23
- Area di Epide.iologia, USL Torino 1-23
- Societl ltali~ di Medicina Generale, Sezione di Torino
con il patrocinio dell' Ordine dei ledici della provincia di Torino
QUe4ta .i.n.d.a~e ha f..i.n.i.. de4 C/lil.ti.. vi... 5i.. fJ/LflgantJ i.. CoLl.~ di.
/l.i..potti:.OA.e a.ttIl.aVeMO i.. qUe4UonOA.i.. i.n.f-OIlJna]A.oni.. il p.i.ù po.1.1i..bue
ac~ate .1ulie ~o~o opLnLoni.. e ~a ~~o con~eta p~ati..ca œnbu~ato
l1.i..~e.
1 ï utte ~e domande .1,(, 11.i..f-e.JliAcono ~a p~ati..ca i.n. conven~i..on e
con U Se/l.vi..~o SanJ...tOA.-t.O Na~on~e.
Le mf-olllTlap_on-t. Il.e~«ate nu qUe4ti..onall.i..o .1MannO cOMuiell.ai~
conf-ui.enJA-aAA.. e non veIl.Il.anno .ut ~cun. modo -1.Me nute m f,olllTla nu
mi..naUva.
Aprile 198h
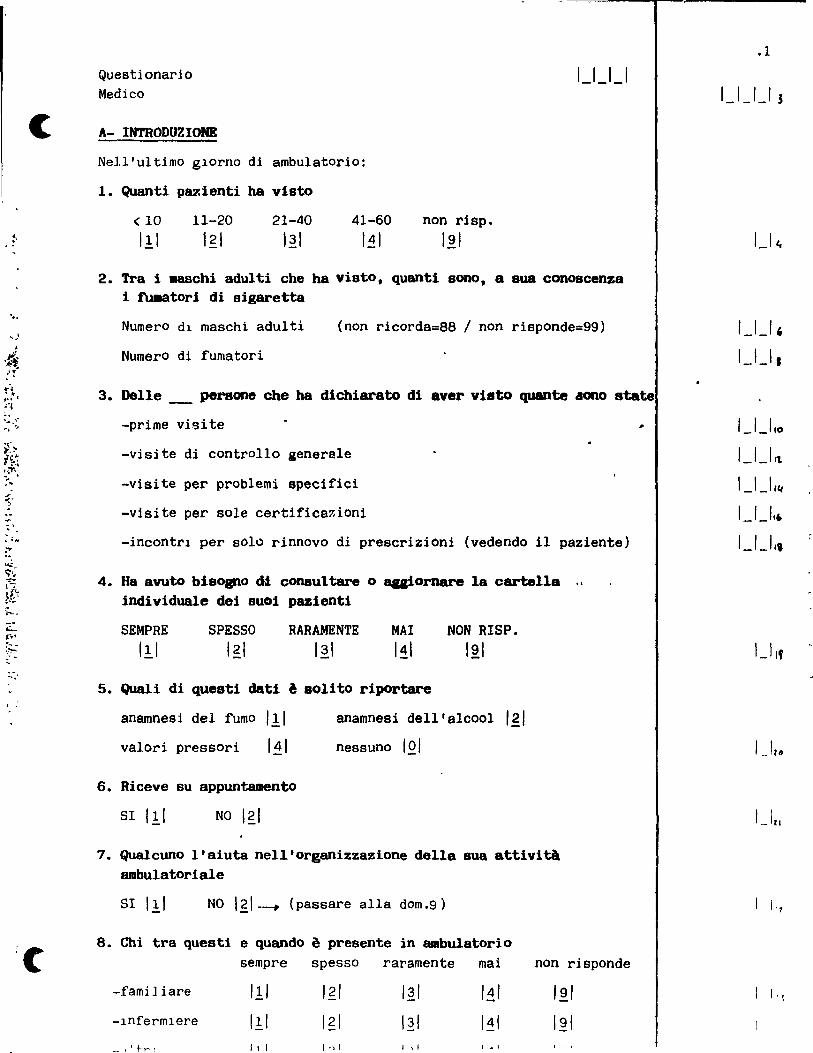
:. , .
' ..
-:J. )
--,
-~ ..
:C
Questionari0 Medico
A- INTRODUZIONE
Nell'ultimo g~orno di ambulatorio:
1. Quanti pazienti ha visto
< 10
III 11-20
I~I 21-40
I~I 41-60
I~I
1-'_'-'
non risp.
'~I
2. Tra i I18schi adul ti che ha visto, quanti S0l10, a sua conoscenza i tu.atori di sigaretta
Numero dl rnaschi adulti (non ricorda=88 / non risponde=99)
Numero di fumatori
3. Delle _ pers one che ha dichiarato di aver visto quante aono state
-prime visite ,
-visite di controll0 generale
-visite per problemi specifici
-visite per sole certificar,ioni
-incontrl pel' solo rinnovo di prescrizioni (vedendo il paziente)
4. Ha avuto bisogno dt consultare 0 agiornare la cartella .. indi viduale dei suOi pazienti
SEMPRE III
SPESSO I~I
RARAMENTE 121
MAI I~I
NON RISP. 12\
5. Quali di quest! clati a soUto riportare
anamnesi del fumo III valori pressori
6. Riceve su appuntamento
SI III NO I~I
anamnesi dell'alcool Igi
nessuno IQ/
7. Qualcuno l'aiuta nell'organizzazione della sua attivltà ambulatoriale
SI Il/ NO I~I--.. (passare alla dom.9)
8. Chi tra questi e quando è presente in ambulatorio sempre spesso raramente mai non risponde
-famiJiare I!I I~I I~I I~I 12/ -lnfermlere Il:1 I~I I~I I~I 12/ ~., ~ 1 t r l 111 ") 1 1,1 1 • 1
.1
1-' -'_, J
,-,-' , 1_1-' 1
'-'-'10 I_I_/'t
1-' -' II(
'_'-"6 I_'-"i
1_11'

.2
9. Ha un associ ato
0 SI III NO I~I 1 -' If,
10. Nel suo a.bulatorio praticano altri .edici
SI Il.! NO 121-. (passare alla Sez.FUMO) 1-' 11
11. Si tratta di: medi c i genori ci III specialisti I~I entrambi I~I 1-' t\
12. Esiste uno sf;8IIbio di opinioni/esperienze
" SI III NO I~I 1 -' l.'/ Se sl: si no
,* -gestione in comune di una parte di assisti ti III 121 1_1 ~o >-.lot
~
'It ~ . ~ . -incontri periodici per la discussione dei ,u i. 1
problemi incontrati III I~I i -' sr t.
-scambio di opinioni occasionale III 121 J 1 -' JI
-al tro (speci f. ) ............................ III 121 1_1 CJ
PRESENTARI TABEI.I.! 1 e 2
.. B- FUIIO
1. Quali di queste I18.lattie lei ritiene steno causste da! ru.o di sigaretta
sl prob.si ;:.
veros.no no non sO 1 r" Ca polmone .111 Igi I~I I~I I~I 1 -'fil ~ ..
- Coronaropatie III Igl I~I I~I I~I 1 Ilç " 1 <'
AteroBclerosi I!I Igi I.~I 1.11 I~I 1 1 ~f, --Bronchite cronica III Igi I~I I~I I~I 117
1
III Igi Ca vescica I~I I~I I~I 1 39.
Ca l-aringe III I~I I~I 141 I~I ln
Ca bocca I!I 121 I~I I~I I~I 1 tu
Ca pancreas III I~I I~I I~I I~I l't' Ca colon III I~I I~I I~I I~I l,
Ca collo utero III I~I I~I I~I I~I 1 l '1\
r, Tromboangioite .. oblitt:!rante III I~I I~I I~I I~I

"
-'-.
..
(
2. In occasione di quali visite si inforas sulle abi tudini (ü fUIIO dei suoi assistiti
sempre spesBo raramente mai non rie.
-prime visite Il.1 Igl I~I I~I I~I
-in vislte generali I!I Igl I~I I~I I~I
-in vlsi te pel' problemi legati al fumo I!I Igi I~I I~I I~I
-in visite per problemi partieolal'i non asso-ti al fumo Il.1 Igi I~I I~I I~I
-altro (specifjcare ) I!I Igi I~I 111 I~I ....................... 3.Quali tecniche specifiche per far cessare l'abitudine al ru.o lei
conosce · ........................................... . · ........................................... . · ........................................... .
Presentare Tabella 3
4. Se non adotta 0 suageriace tecniche che ritiene utili. quali SODO i proble.i che glielo i~iBConO
-inadeguata formazione
-insufficienza di tempo deI medico
-insufficienza di tempo deI paziente
-assenza di incentivi
-carenza di spazilmezzi nell'ambulatorio
-terapie non mutuabili
-non di sp10nibilità della tecniea
-searso interesse e/o rispondenza presso gli assistiti
-altro (speLif.) ...••••.•.••••••.•••
CITATO SUGGERITO
III 111 111
111 111 111
111
5. Se eonsiglia ai suoi assistiti di smettere di fumare. questo avviene con: -tuttI i SUOI assistiti fumatori Il.1
-solo con i fortl fumatori I~I (specificare ..•..•••.. )
,.
6. Ritiene che smettere di fumare possa comportare eCCetti indesiderati
iii
.3
1 _.14<,
1_141
IJ <'1
,_, '-S
1_1 t"
I_I_I~, ~
1_1-' s~
'_1-' ss " " "
~ .. :~.'
'.
,-' ~t ,1
1-' '1
1_1 ~~ ,1
1-' Sl/
1 Ibo
1 161 -l 'l
16 ;
1 ~I,
(1

,
"
................................... 7. C'è qualche condizione di età e/o salute per la quale gli eCCetti
citati sconslgliano un suo intervento
slili no~~1
~ Se si, specificare
................................... B. Ri tiene che il rischio di _.alarsi di tuIIOre deI polllOne sI
modificht negli ex-cu.abOri
si,semprelll
non so Isl T
81,80]0 per pIccoli 0 recenti fumato~l
no I~I_ (passare aU a dom.10) t
9. Dopo quanti ann! ri Uene che il rischio di tuIIOre al polllOne di un
ex fuma tore eguagll quello di una persona che non ha llI8i fullato
10. Che cosa di quanto indicato potrebbe Cacili tare la sua opera di prevenzione dei danni da ru.o
l'
molto ~~ poco inutile non so utile utile utile
-opuscoli di educazione sanitaria da distribuire
-campagne mass media
-aumento del prezzo delle
III III
sigarette III 1
-leglslazjone più restrittival!1
-altro (specificare)
I~I
Igi
I~I
i~1
I~I
I~I
I~I
I~I
Il. Se dovesse utilizzare, in appoggio ai suoi consigli,materiale illustrativo da distribuire ai suoi assistiti,preferirebbe che questo ma teriale avesse una impostazione tendent~ prevalentemente a: -
-spaventare 0 Intlmorlre IJ fumatore SUI dannl da fumol!i
-presentare lInon fumatore come una persona socj~lmente 'in' o posltiva I~I non sol~1
. -'
1_1 Tt;
1 1 ln
1 1 1'71
1_1_ls,
1 l 'l" _.'_ a .. ,
1_1 g.;
1_-'\1(,
1 _ Ill?
1 1 ~

· .r ... ;
. " . !,Jo .' · ' . --, · '. ,---.,: ..
-.'
1. ~_
c
12. Ri ti ene che la diagnosi precoce deI tuIIore pol.anare truite Rx
torac0 ai suoi assistiti fumatori sia:
eff1cacel.!1 abbastanza efficacelgl poco efficacel~1
inefficacel~1 non sol~1
13. Prescrive un Rx torace ai suoi assistiti tu.atori asintOMatici per la diagnosi precoce deI tumore polmonare e con quale periodismo
PERIODISMO si •
6mes. lanno 2aa altro,specificare
-a tutti I fumatori UJ Igi I~I I~I · ......... -a tutti I fumatori con più di 45 annl 111 12 1
_1 I.~I I~I · ......... -a chi fuma più di 20 sigarette ad ogni età 111 Igi I~I I~I · .............
-a chi fuma più di 20 sigarette e con più di 45 anni 111 Igi I~I I~I · .........
-altro (specificare) 111 Igi I.~I I~I · .......... . ......... " .....................
rio. mal 111
14. Prescrive un esame citologico dell'escreato ai suoi aasistiti fUmatori per la diagnosi precoce del tuIIOre pollllOll8re e con quale pe-riodismo PERIODlSMO
51,
-a tutti i fumatori
-a tutti i fumatori con più dl 45 anni
-a chi fuma più di 20 sigarette ad Qgni età
-a ChI fuma plÙ di 20
sigarette e con p~ù dl 45 anni
-altro (specificare)
no, mal III
6mesi
111
111
111
III
, 1 "0 2aa
. I~I . . Igi 121
Igi 121
I~I
altro,specific.
I~I .. ............
I~I · ................
111 .................
1 ~ 1 ••••••••••
1 ~ 1 ................ ..
15. Ritiene che l'assuozione di vitamina A e/o Beta carotene sia efficace per prevenire i tumori deI polmone
effIcace Il.1 abbastanza efflcace I~I poco efficace I~I
1 .1
• S
1 1 <iz
1 1,1'S
1 J 7,*
IJ~~
1 1 fC,
1_191
IJ ~"
1111
l,.,."
1 1,01
1 i.)


(
>.
(
3. Qu8le livello giornalieco di consuma di alcool rltlene che sarebbe raccomandabile non superare per un adulto sano con nor.ale attività fisica, secondo la sua opinione
-0 ml di alcool asscluto III -25 ml di alcool assoluto (1 bicchiere di vino a pasto) Igl
-50 ml di alcool assoluto (2 bicchieri di vino 8 pasto) I~I
-75 ml di alcool assoluto (3 bicchieri di vino a pasto) 111 -100 ml di alcool assoluto (1 litro di vino al giorno) I~I
-altro (specificare) ..•.•••••••....•••••••••••••••.••• 161
-non so I~I
4. Quali _alattie. a suo parere causate dall"abuso di bevande alcoliche. rl1eva plù f"requenteMnte tra i 8uoi pazientl (elencare le prime tre)
· ........................................... , .............................................. · ........................................... .
5. Quali tecniche specifiche lel con08ce per far ce8S&re 11 consUllO di alcool
• ••••••• 0 ••••••••••••••••••••••••
· ............................... . · ............................... .
Presentare tabella 4
6. Che cosa di quanta indicato potrebbe facili tare la aua opera nel C8llpo della prevenzione dell' alcolisllO
-opuscoli di educaz.sanitaria da distribuire
-indicazione di centri specif. pp.r prevenzlone e cura
-campagne mass-media
-restrizione vendita
- tassaz l one
-controllo alcolemia de! guidatore
-altro (specif.)
III
III III
III
I.?I
Igl
,~,
181
.7
IJ It~
I-'-'In ,_,-' 119
1 1 IIJI
'-'-'ru I_I-'"s
'_'-',n
1 .I,\~
1 111.0
1 1""
'. "

,-,.
7. Se non adotta tecniche che ritiene utili, oppure se le adotta .eno frequente.ente di quanto potrebbe,quali sono i aotivi che glielo illpediscono
-inadeguata farmazione
-insufficienza di tempo deI medico
-insufficlenza di t~mpo del paziente
-assenza di incentivi
-earenza di spazi/mezzi nell'ambulatorio
-terapie non mutuabili
-altro(specificare) .••••••••••••.•••••• ..................................... ,
D- IPIRTENSIONI
CITATO
III
111
III
III
III
I.!: 1
Iii
SUGGERITO
1. NeU' ul tiao giorno di a.bulatorio a quanti paienti ha .isurato la presaione (se 0, passare alla dom.3)
2. A quanti su richiesta deI paz lente
3. Control la la pressione indipendente.8nte da .alattie legate aU' ipertenoione slili nol~1 ~ (passare alla dam.S)
4. Se sl, a quali assisti ti e con quale perlodisllO
-a tutti
-solo ad aleuni gruppi di assiste
· ............... . · ............... . · ............... .
solo lD visita
IQI
IQI
IQI IQI
invito a tornare agni 3ms 6ms la aitro
III
Il.1
I.!.I
III
I.~I I~I I~I
Igi I~I I~I
I~I I~I I~I
I~I I~I I~I
quando vengano in ambulatorio
151
5. Nell'ultiao giorno di a-bulatorio quanti assistiti in trattamento faraacologico per ipertensione ha visto
6. Incontra difficoltà nel pratic~e il follow-up dei pazienti ipertesi sil.!.1 nolgl
Se sl, quali
.H
1-' Ill~ l'Ill' '-'14 , 'J ,tl~
'-"119 'J 's,-"s,
'-'-'IH I_'-'IH
Il'''
1 lin

C
'.
' .
. " . . t,.)~
.117 ~7~ ._.
(
7. Consiglia ai suoi pazienti ipertesi in trattamento far-acologico:
SEMPRE SPESSO RARAMENTE MAI
-automisurazione da parte deI paziente a domicilio III Igi I~I 111
-automisurazione con apparec- III Igi I~I 111 chi automatici in farmacla
B.Nel suo ambulatorio chi misura più frequente.ente la pressione arteriosa
un infermlerelll lei stessolgl solo lei 131
9. Registra i valori riscontrati
sempre I.!I solo se al di fuori della nor~a 1 g 1
solo se riscontro variazioni significativel~1 mail~1
. 10. A partire da quali valori lI8X e/o ain di pre.Bione arterioaa
diastolica e/o sistolica ritiene utile ini.iare un tratta.ento f8I'118cologico in un adulto aaschio con pin di 40 anni
MAX MIN 1_1_1_1 1_1_1_1
E- TUIIORI FEIDIINILI
1. Ritiene che l'orienta.ento delle donne rispetto alla prevenzione dei tuaori deI collo dell'utero e della ~lla debba essere svolto prevalente.ente da:
medico di base I.!I ginecologo 1 g 1
consultorio I~I altro(specif.)I!I •••••••••••••••••••••
UTERO
2. Quali considera fattori di rischio di K collo utero SI PROB.SI VEROS.NO NO NON SO
- C'ontraccetti vi in usa I.! 1 Igl I~I I~I I~I
-numero partners sessuali I.! 1 Igi I~I I~I I~I
-numero fi g] i I.! 1 Igl I~I I~I I~I
-precocità rapporti sessuali I.! 1 I~I 131 111 I~I
-igiene intlma 111 Igi I~I 111 I~I
-cl asse soclal e I.! 1 Igi I~I I~I I~I
-malattle veneree I.! 1 Igi I~I 111 I~I
-herpes genitale ! 1:. 1 Igl I~' I~I I~'
.9
1 _I,,,~
1-' It~
'_'_IJI1I#
IJJJm
1-' I?~ ,. l'~l'
1_1,,,,
l ,~~ I,Q
1 : ~I,
l'~,'

'. -. ..; ~-' t~' :-: ;'. r
.... •
; .
, ,~~ - ~--~~'~~~~-.--------------.... -----IWOŒLLA
10. Quali dei se~enti elementi considera fattori di riBchio per il K della .aDMDella
SI PROB. SI VEROS. NO NO NON SO
-dieta
-familiari tà
-obesità
-contraccettivi orali in uso
-nu1l1 pari tà
-prima gravldanza dopo j 30 anni
-menarca precoce
-menopausa tardiva
-radiazioni
-fumo
I.~ 1
I!I I!I
I!I I!I
III I!I
I.~I
I!I I!I
I~I
I~I
Igi Igi Igi
Il. Pratica l'esaae obiettivo della ...-ella
I~I
I~I
i~1
I~I
I~I
I~I
I~I
I~I
I~I
I~I
-solo sulla base dei sintomi dichiarati dall'assistita I!I (passere alla dom.13)
-anche indipendentementa dalla denuncia di sintomi p come pratica a sé Igl
-mai (passare alla dom.13) I~I
12. La fa per quali assistite almano 1 intervallo oeeasiovOlta/an più lungo nalmente
-tut te le assistite con più di 18 aa
-solo al'euni gruppi di età (speci fi ~. ) .............................
-solo nelle donne a rischio
111
III
1.11
I~I
I~I
I~I
13. Considera la .ammografia eseguita periodicamente una tecnica che riduce la probabili tà di IIIOrire per K della mammella in tutte le donne per alcune claBsi di età
SI 111
PROB. SI
121 VEROS.NO NO
I~I I~I 1 1 (pas sare alla
NON SO
181 !
dom.15)
.11
lJ Iqs
IJ i'lV
1_1100
IJ/.#, 1_ll.ot
I-'z-J 1:..11.01,
1-' lA
1-' z.c;
1_1~7
1 l" v
1 17,,,
1 Jl"

.
.'
- -'-
(
3. Considera il Pap-test una tecnica che riduce il rischio di .orire per tuaore deI collo dell'utero
SI
III PROB.SI
Igl VEROS.NO
I~I NO
I~I NON SO
I!! 1
4. Lo consiglia aIle sue pazienti
SI, a tutte le donne sesualmente attive I!I a tutte le donne in dcterminate classi di età 12\
alle donne ad alto ~ischlO 13\
solo a chi chiede consiglio 111 solo aIle donne sintomatiche
NO (passare alla sez.MAMMELLA)
perché ............. ' ............................... . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . .. . . . . . . . .
5. A. quante sue 88sistite ha consigliato il Pap-test nelle ultiae due setti.ane
6. Ritiene soddisf'acente il sua rapporto con 10 specialista e/o la struttura deI consultorio
SI III NO Igi Se no, perché .•••..••••••..•••••.•.••.••••••••.•••••••••.••••••
7. Richiede che le donne cui consiglia il Pap-test ritornino con il risultato dell'esame
SI Il ~ NO 121
8. Ripete regolarmente l'invito a sottoporsi all'esame
SI III 1 No 12\
9. Con quaie periodicità 10 consiglia
< 1 volta 1 volta agni 2aa ogni 3aa agni 5aa
l'anno l'anno a più
(35 ANNI I.~I Igi I~I I~I 121 35-70 ANNI III Igl I~I I~\ 15' _1
.10
IJ,l~
. "

'.
.. . , . : ~
0" .... :,
". "
14. Da che età a che età consiglierebbe l'esame .••..•.••.........
15. Prescrive la mammograCia aIle Bue pazienti
SI I!I NO 1 g 1 __ (passare alla dom.1 7 )
16. La prescrive :
-a tut te le assistite nell'ambito delle età citate III
-solo aIle donne a rischio Igl -solo in presenza di sintomi
Con quale periodismQ (in anni) (se tutte / donne a rischio)
17. Considera l'autipalp~zione esegulta periOdicamente una tecnica che riduce la possiblll tà di ~rire per Je della .ammella per alcune classi di età
SI PROB.SI VEROS.NO NO NON SO Igl I~I 141 lai r r (passare alln dom.19)
III
18. Da che età a che età la consiglierebbe •.•••••••.•••••••••••••.•
19. Prescrive l'autopalpazione alle Bue pazienti
SI I!I NO 1 g 1-+ (passare alla dom. 24)
20. La prescrive:
-a tutte le assistite nelJ'ambito delle età cltate III -solo aIle donne a rischio
Con quale periodismo (in settimane)
21. Nel caso lei insegni l'autoesame deI seno rlc~iama la sua 8Ssistita per verificare la correttezza della tecnica
SEMPRE SPESSO RARAMENTE MA!
I~I
NON INSEGNA
IQI l (passare alla dom.23)
l " • r
,_,_ 1 1
111( .. lb
1 1. 10
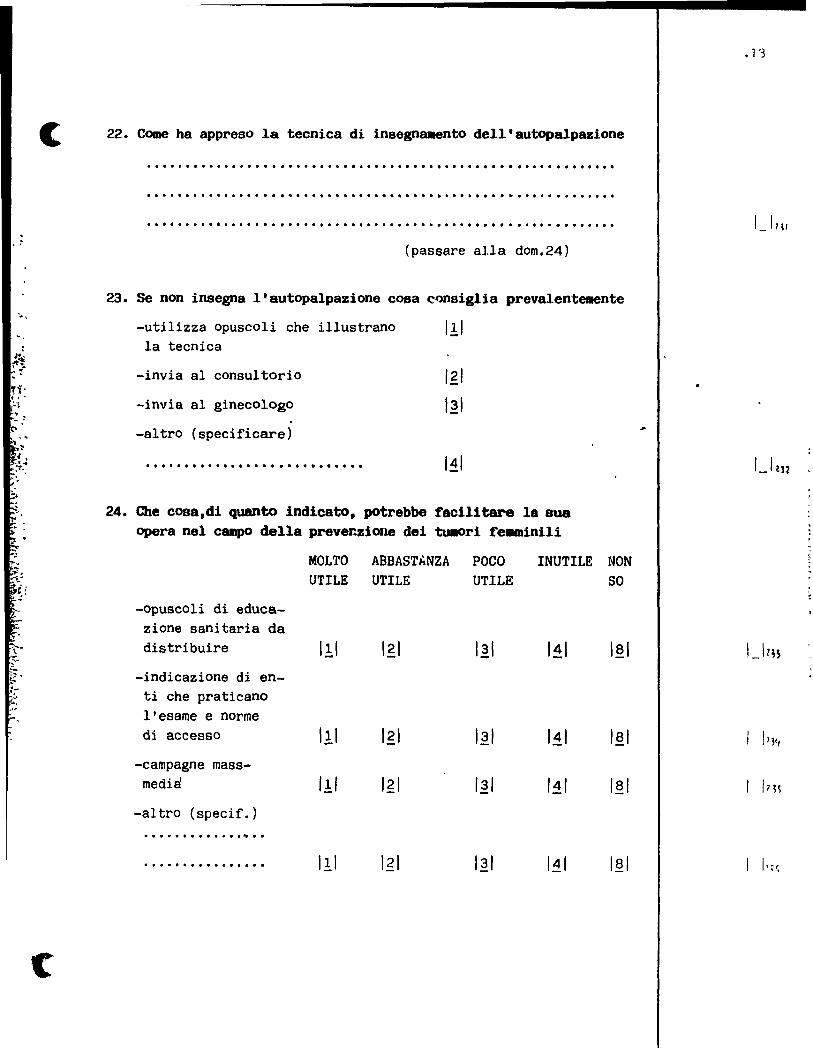
. . .
"
c
22. Come ha appreso la tecnica di insegnamento dell'autopalpazione
· ............................................................ . · ............................................................ . · ............................................................. .
(passare alla dom.24)
23. Se non insegna l'autopalpazione cosa cQnsiglia prevalenteaente
-utilizza opuscoli che illustrano I!I la tecnica
-invia al consultorio
-invia al ginecologo
-altro (specificare)
· ........................... .
121
I~I
I.~I
24. Che cosa,di quanto indicato, potrebbe facilitare la sua opera nel campo della prever~iœle dei tu.ori fe.minili
MOLTO ABBASThNZA POCO INUTILE NON
-opuscoli di educazione sanitaria da distribuire
-indicazione di enti che praticano l'esame e norme di accesso
-campagne massmedia
-altro (specif.) ............. ,. ... ................
UTILE UTILE UTILE SO
I!I
I~I I~I
I~/ /4/ I~I
I!I I~/ I~I
.1'3

o
~ .. "
, .-~.
F- ADOLESCENTI
INCIDENTI
1. Ritiene efficace l'uso di caschi per i motociclisti nella prevenzi~ ne dei danni da incidenti stradali
MOLTO EFFIC. III
ABBAST.EFFIC. Igi
POCO EFFIC.
I~I
INEFFIC.
I~I L
(passare
NON so lai r
a dom.3)
2. Si accerta dell'uso deI casco da parte dei suoi pazienti IIIOtociclisti
SEMPRE III
SPESSO Igi
RARAMENTE MAI
I~I I~I
3. Rltlene efficace l'uso delle cint~ di sicurezza per aIl automobilisti nella prevenzlone dei danni da incidenti atradali
MOLTO EFFICCACE III
ABBAST.EFFIC. POCO EFFIC. INEFFIC. NON 50 Igl I~I 141 lai
T 1" (passare a dom.S) 4. SI accerta dell'U8o delle cinture di
pazienti autoaobilistl slcurezza da parte dei suoi
SEMPRE III
SPESSO Igi
RARAMENTE I~I
MAI I~I
5. Lei pensa che rlentri tra i suoi cOlipiti quello raccOll8lldare l'uso di caschi e cinture di sicurezza
SI III NO 121 NON 50 lai ~ - l -
(passare alla Sez.5essualità)
6. Cosa potrebbe influlre negativamente sull'ascolto delle sue raccOliandazioni
-non seguono le mie indicazioni su argomenti non sanitari
-per i costi che comporta 1'acquisto di un casco
-altro (specificare)
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
citato suggeri to
I!I Igi
I!I
• l 11
1 Il~'
1_12140
1 l 'I,l
1 1 •

. . .
'.
.~ , .. " ,
, "
-1. 1
1
c
SESSUALITA'
1. Ritiene utile una sua attività di inforaazione sulla contraccezione al fine di prevenire gravidanze indesiderate
MOLTO UTILE
Il:1 ABBAST • UTILE
Igl POCO UTILE
12.1 NON UTILE
141 NON 50 lai r r (passare alla 5ez.ANZIANI
2. Fornisce questa indicazione di sua iniziativa
5EMPRE III ~
(passare
SPE5S0 RARAMENTE
121 I~I r alla dom.4)
3. La foroisce su richiesta
SI III NO Igl
MAI
I~I
4. Invia al consultorio/spec1a11sta
SI I!I NO Igi
5. Incontra ostacoli nel fornira queste 1nf'ol'll8Zioni SI Il:1 NO Igl Se sl, quaIi: -inadeguata formazione
-difficoltà ad affrontare l'argomento con le pazienti per resistenze cultural! e ps!cologiche
-altro (specif.) ••••••••••••••••••••••••• ......... -............................. .
G- ANZIANI
VACClNO ANTIINFLUBNZALE
I!I
1. Ri tiene' che la vaccinazione antinfluenzale nelle persone > 65 énrii sia efficace nella prevenzione delle cOMplicanze polmonari
SI
III PROB.5I . I~I
VERSO.NO
I~I
2. La esegue direttamente SI III NO I~I
NO NON 50 141 lai T r
(passare alla Sez.successiva)
3. Consiglia il ricorso a tale vaccinazione negli anziani (>65 aa) SEMPRE SPESSO RARAMENTE MAI III I~I 131 141 - T
(n"::JiL C"..,. ..... C'lI .... 1',.,. C" __ ........ -..-.. ...... ___ .! _,
,
• 1 ~
1._1 Zl"
1 1 tl.S
1 I.!

,
0
, .
.:
4.I~pazienti seguono la sua indicazione
SEMPRE SPESSO RARAMENTE MAI III I~I I.~I I~I
5. Quali problemi si presentano ai suoi pazienti nel rispondere a questa sua indicazi~ne
cltato suggeri to
-costo deI vaCCIno
-accesslbJ]ltà servlzio vaccInale
-altro (sppclflcarp)
.................................... ~ .............................. , ... .
INCIDENTI
6.A suo parere le indicazioni del medico di base possono avere una utilità nel prevenire incident1 degli anziani in a.bito domestico
MOLTO UTILE
III ABBAST • UTILE
Igl POCO UTILE
I~I INUTILE NON SO
141 I~I (passare alla Sez.success.
7. Lei di solito dA indicazioni in questo senso
SEMPRE III
SPESSO Igl
RARAMENTE I~I
8. Incontra problemi nel Cornirle
SI III NO Igi
9. Se sl, quali
-formazione inadeguata 1
-tempo deI medico
-tempo del paziente
-il paziente non segue conslgli non sanitari
-impOSSIbllltà dl modificare la sltuazlone dl vita
-a)tro (specjfirare)
..... , ....................... .
MAI I~I-.(passare alla Sez.successiva)
citato suggerito
Il.1 Igi
I!I Igi
I!I Igl
I!I Igi
I!I Igi
Il.1
10. Le è capitato di segnalere ai Servizi Sociali }'esistenza di casi a particolare rischio dl Incidentj domestjci
,F
, 1
in
: '!~
l',
'"
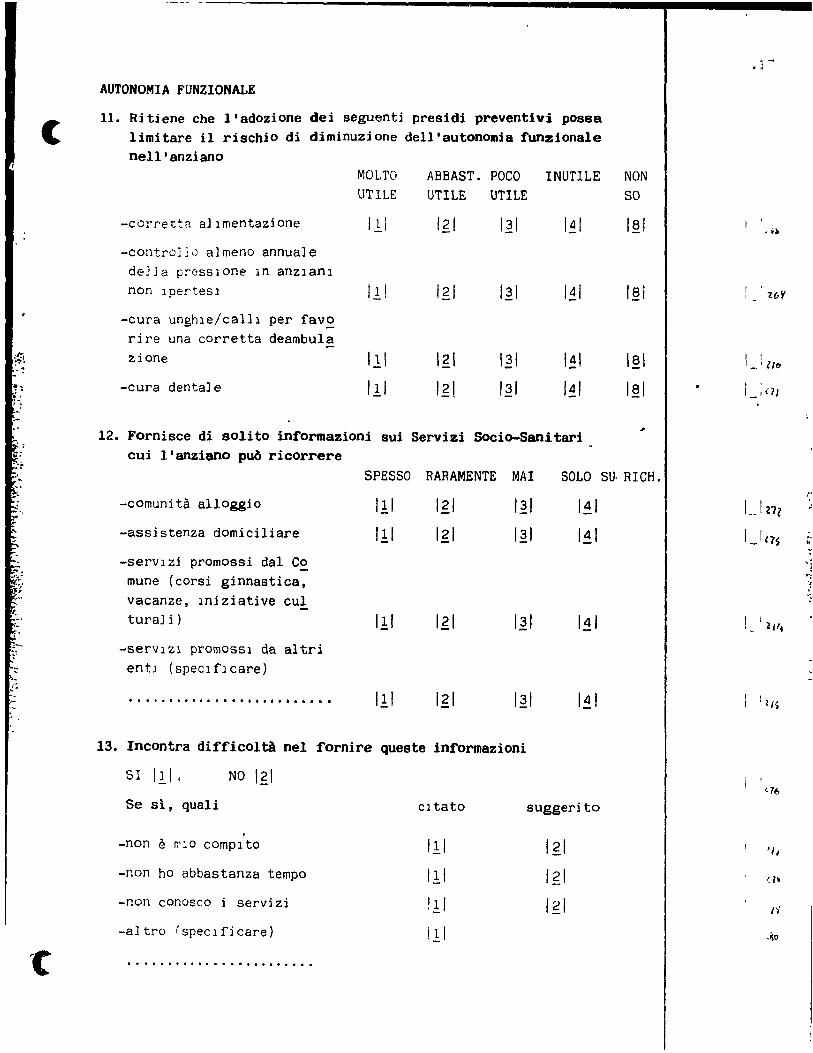
,',
.'
" "
(
AUTONOMIA FUNZIONALE
Il. Ritiene che l'adozione dei seguenti pres1d1 preventivi possa limitare il rischio di diminuzione dell'autonomia ~unzionale nell'anziano
MOLTO
UTILE ABBAST. POCO INUTILE NON UTILE UTILE SO
-cOrretta allmentazione
-contrO]~0 a]meno annuale de]Ja preSSlone ln anzlanl non Ipertesl
-cura unghle/calll per fav~ rire una corretta deambula zione
-cura dentale
Il,1 I~I
I~I
I~l
I~I
12. Fornisce di solito in~ormazioni sui Servizi Socio-Sanitari cui l'anziano puô ricorrere
18' -'
SPESSO RARAMENTE MAI SOLO SU· RICH.
-comunità alloggio
-assistenza domiciliare
-servlzi promossi dal C~ mune (corsi ginnastica, vacanze, Iniziative cul turaJi)
-serVIZ1 promOSSl da altri entl (speclflcare)
......... , .................. .
III
III
III
III
I~I
13. Incontra di~ficoltà nel fornire queste in~ormazioni
SI III 1 NO 1 ,g 1
Se si, quali cltato
. -non è ~lO complto
-non ho abbastanza tempo
-non conosco i servizi
-altro (speclficare)
... , ..... , ............. .
I~I
suggeri to
.] -
•••
1 1 ,_ l/l.
1 'Ig
1 1
'-1"
'l,
1)'

''\ ; ' .. ,. f.
o H- FARMACI
1. Ha incontrato nella sua attività il problema di abuso di autoprescrizione di farmaci
SEMPRE III
SPESSO Igl
RARAMENTE I~I
MAI I~I
2. Esiste nella sua attività il prrblema dell'errata interpretazione delle sue indicazioni circa il dosaggio e le modalità di assunzione dei farmaci
SEMPRE III
SPESSO Igl
RARAMENTE
I~I MAI
I~I
3. Control la la corretta assuozione dei tarmaci che prescrive
SEMPRE I!I
SPESSO Igi
RARAMENTE I~I
MAI I~I
4. Si informa sui tarmaci assuoti contemporaneamente a quelli da lei prescritti
SEMPRE III
SPESSO Igl
RARAMENTE MAI
I~I I~I
5. Ritiene che le sue raccomandazioni e controlli possano avere un ruolo di prevenzione nell'abuso di farmac!
MOLTO UTILE III
ABBAST.UTILE Igi
POCO UTILE
I~I INUTILE
I~I NON 50 I!;! 1
,Ji
. ~81
, 1
_ 12S"
, I~)

(
1 ,.
--,
c
1- ABlTUDINI PERSONALI
1. Lei {'uma
slgarette (speCl ficare numero f! anni
(speclflcare numero e anni
pIpa (specificare annl dl fumo)
di fumo)
di fumo)
III
I..?I
1.21
I~I
121
ex fuma tore (spPclflcarp numero p anni dalla cessazione)
mai fumato
2. Lei {'uma in ambula~;orio
anche davant! al paZlentl
solo fuori dalla sa] a in CUl vIsi to
solo se non vi sono pazlenti
mai
3. Nella sua sala d'attesa ~ permesso tumare
SI III NO Igl
4. Sulla sua automobile sono montate le cinture di sicurezza
SI III NO 121
5. Quando le usa
mal 11:.1 solo in città Igl solo fuori città I~I
sempre 141
1 1 1 1 1 1 1 1 tg!. l~ 1«,)

In mol te delle domande formulatel~ Je ahblamo chiesto di quantificare le
risposte, anche se non disponeva dl datl oggettivi.
Per Questa ragione le sue stlme non .",ClrantlO completamente esatte.
Da un punto di vlsta scientlflCo vaJldare Je risposte di indagini svol-
te, come questa, tramlte questlonarlo, dà una misura della affidabilità
dell'indaglne, attraverso una venfIea su dati oggettlvi.
Un metodo lndiretto dl valldazlone C'onslste nel chledere alla persona
intervistata qual è la sua stlma dell'errore che pua essere stato intro-
dette.
Lei precedentem~nte mi ha detto di aver visto nell'ultimo giorno di am-.. bulatorio assistiti: quaI è il numero minimo e il numero massimo
dl persane che è sicuro di aver visto?
non mena di
non più di
ANALOGAMENTE: Lei mi ha cetto di aver misurato, nell'ultimo giorno di
ambulatorio, la pressione a assistiti: QuaI è il numero minlma e
il numero massimo di assistiti cui è sicuro di averla misurata?
non meno dl
non più di
I._I-'!o~
1 i 1 ~ol

,
.~ .
.--,-~--------------------~~~------~--....
In una seconda fase di questo studlO ci proponiamo di valutare l' effic!,
c: cia dei consigli del medico genera)e nel facilitare la cessazione della
abitudine al fumo tra i proprl asslstiti.
Questo progetto è concepito facendo riferimento ad altri analoghi con
dotti nei paesi anglosassoni e verrà definito nei dettagli in relazione
al contrlbuto de] colleghi che co]laboreranno ad esso.
Sarebbe interessato a partecipare ad un intervento di educazione 8anit!,
ria sul fuma in cui le verrebbe richiesto di seguire nel tempo (orient!,
tivamente 4-5 volte in un anno) un gruppo di suoi assistiti fumatori
SI I!I NO Igl
Se SI
Posso farla contattare nei prossimi mesi dai responsabili della studio
(SIMG e Area di Epidemiologia) per fornirle magaiori informazionl sulla
ricerca e concordare la sua eventuale partecipazione?
SI I!I NO Igi
• ?1
1_'W9
·c
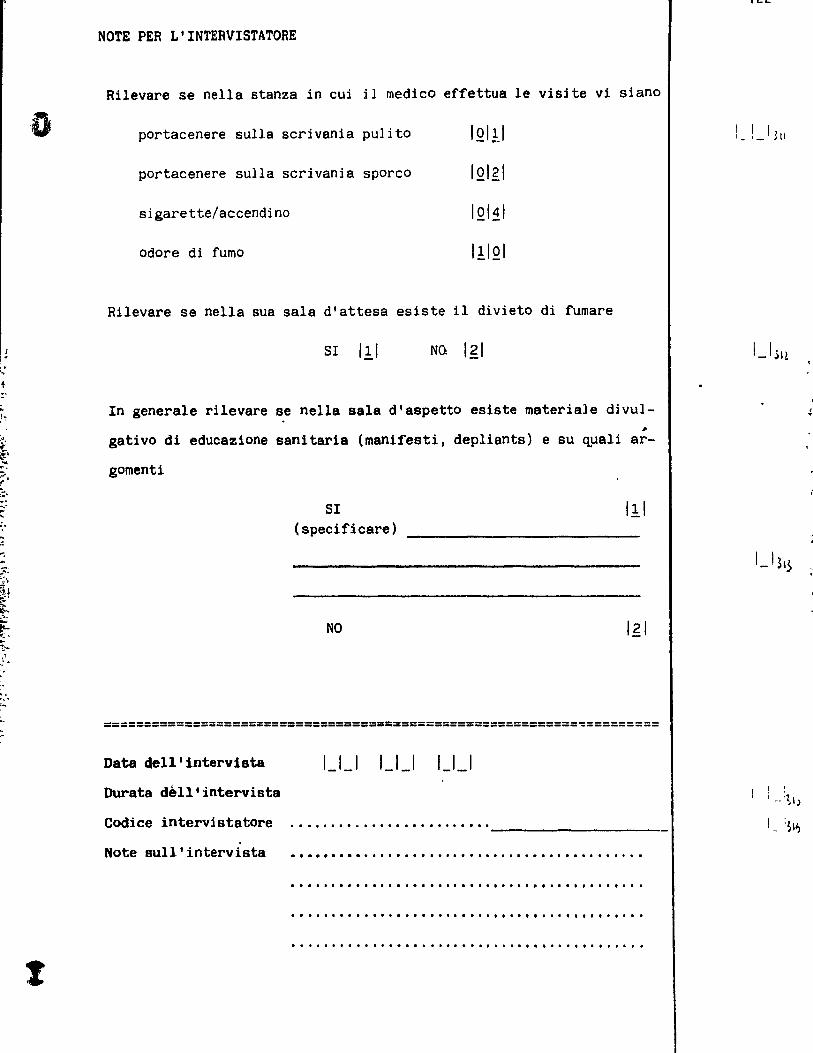
'''. r
-,-" ,
" "." ...
t
NOTE PER L'INTERVISTATORE
Rilevare se nella stanza in cui il medico effettua le visite vi siano
portacenere sulla scd vania pulito IQI11
portacenere sulla scrivania sporco IQI,g1
sigarette/accendino IQI~I
odore di fumo I!IQI
Rilevare se nella sua sala d'attesa esiste il divieto di fumare
SI III NO Igl
In generale rilevare se nella sala d'aspetto esiste materiale divu]-
gativo di educazione sanitar1a (manifesti, depliants) e su quali ar
gomenti
SI (specificare)
NO
I!I
===========================================================~=========
Data dell'intervista 1_1_1 1_1_1 1_1_1
Durata dell'intervista
Codice intervistatore ......................... ------------------------. Note sull'intervista · .......................................... .
.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . · .................................... , .. , .. . · ............................................ .
.....
1. ! _1 ~II
'-' ~\.$

l ,
(
. ~
~
-:
.[
TABELLA 1 INTERVENTI PREVENTIVI
Con riferillnto I9li iftttr\l!llti/colPOrt.t!llti 'uUa i""'caU:
Quanto 11 rlt1.nl UTILI
nel proluovere 11 silute
di un adulto
Quanto li ri ti.1II PREPARATO
ptr dlrl indiclzioni/conti-
gli/prllcrizioni in IIrito
Quinto SUCCESSO rititnt di
pot", aVlrl Ml dltlrlinar.
un cilbillinto dll11 Ibitu·
dini dli ,uoi Il,i,titi
Riti.nt SUD cDIPito
INTERVEMIRE lU quelti pro
blt.i Inchl prltlO un paZllntl
lino chi non 911.10 richieda
"plIe! tuente
ELIHIHAZIOHE COHTROLLO
FUHO PESO
REGOLARE
ESERCIZIO FISICO
!1!2!3!~!8! !1!2!31~!8! !1!2!3!.!8!
!1!2!3!4!8! !1!2!3!4!8! !1!2!3!.!8!
! 1 !2!3!4!8! !1 !2!3!4!8! !1!2!3!4!8!
SI NO SI NO SI NO
IGlENE ORALE
!1!2!3!4!8 1
,
!1!2!3!t!8!
!1!2!3!4!8!
SI NO
N.B. 1: ~LTO utlle/prep~rato/succe,so 2: M8ASTAHZA IJhle !Ct. 3, POCO uhl, ~r.':,
4 NOH IJt11e ICC. 8, NON 50
2.
---. -.
-,
:' -:,: ~
r~ .. ' ~ -J
,.~ '~ ;,i
' '!' ~
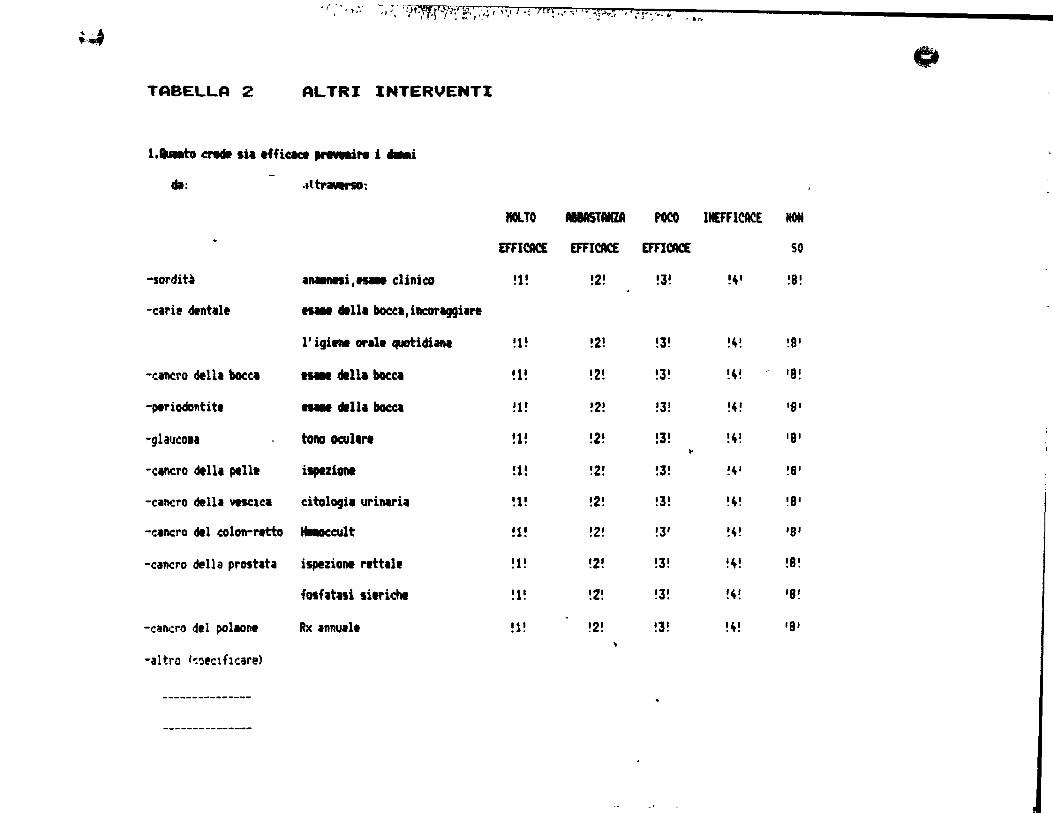
.. ," ~.'.wo!J
~ -.. , .. " J ~ J. 4 - ~~irJ-.'-l"'l'51l "Ir ",!*t ldl .. ~,,;I''''''V''''1'~ II_~ .. ~._ .. .. ~ ~" ' ... , . l : _,' 1 ,_~..J • '. ,~. t .. ~ , ~ ~
TABELLA 2 ALTRI INTERVENTI
l.au.to a"8dI sia effic.ce """'N i ... i dl: .tltr ..... :
ItOlTO MMSTANZA POCO
EFFICACE EfFICACE EfFICACE
-sordit~ InMllfti,~ clinico !1! !2! !J!
-c;rif dentall .... d1Ua bocca,illCOl'aggiare
l'igi.nt oral. quatidiana !1! !2! !J!
-cintra della bocCI .... 411111 bocct ~1! !2! !J!
-~riadontit. .... dlilallacct !1! !2! !J!
-glaIJCOI. toRO ocullr. !1! !2! !J! .. -Cintra dtlll ptll. i.,.ziOM !1! !2! !3!
-canero della YelC1Ca citologia urinaria !1! !2! !J!
-canero ~l colon-rttto Hlllaccuit !1! !2! !3'
-canero della prost.t; ispezion. r.ttal, !1! !2! !J!
fosfatlli litrichl !1! !Z! !3!
-canero deI pollOnt Rx InnUlI. !1! !2! !J! ..
-altro (~~,r.lflr.are)
---------------
---------------
Ci
INEfFICACE HON
SO
!~I !8!
!4~ !8'
!4! 'B!
!4! 11P
!4! 'B' !~, !8'
!4! !S'
!4! '8'
!4! !B!
!4! '8!
!4! 'S'

l
TABEllA 3 FUHO
C Quanto • eDftYinto IuIll di l'"~ hl Idottlt. I1111D URI l, 4Ulli clli 1. hl Idottltf/con~1911ltt
-tlf ~.!rYlno '101b iMipel\de,,~ell ,~f dl !pUa chi o If 111oth/.:nr'i\g!11
ptftl. oggi dtlll loro utllit' (posliblli plÙ l'l'post,) .
SEhPRE fOf<TI IN F~ESEN:~ vi S' .. j Su
FU"ATÎJR! MALIlT"I~ R" .-,.,.. ... P'" .. t. J 1 ~
-FI~.a:otlrlPil (nlcoprlvl) Il'2'3'4'8' SI ! 11 (doe succ) NO '2 1 (Ilt)
·l~/or'lzlonl '111 IIdil '1!2!3!4!8! (Mn li IPPlica)
-PIJbb llCl shcl/'ud1ovi Il vi Il!2!3!4!8' SI ! l! (dol IUCe) 110 !2! 'aIt' t
• -Inv!to/rICCOIlndlzlOftf dt1
, ' . -,
IICleo uni tlntUi !1!2!3!~!8! SI ! l' (dol tuce) MO !21 (lit' , ,
Il
:
-Invltl/riCCOI,ndIZ10ftl dl! . HdlCO 1'1pttuti !1!2!3!~!1' SI !1! (dol _el 110 !2! (lit),
,'J: -, ,~
c
-Go .. , 1111 nlcotinl !1!2!3!4!1! SI !l! (dol MC' MO !2! 'Ilt) .:::: .. -., ... -Plicot,ripil in cilnici !1!Z!3!4!1! SI !1! 'dol _e' MO !2! (lit)
;;. il
.. ..1
-Pll~ot,rlPll di gruppo !1!2'3!4!1' SI !l' (dol _e' MO !Z~ 'lit) ~ .~
·Pll~ot,rlPll indiYldulle ! 1 !2!3!4!8! SI Il! tdDI suce) MO :2! (11t) .~
'1
-Ipncli !1!2!3!4!1! SI !a! (411 suce) MO !Z! 'ait' .~ ~
-~opunturl !1!2!3!~!'! SI !1! (dol suce' MO !Z! (ait', '''; , •
-Rlcovlrro 10 clinlcht
IpWihzZltt !1!2!3!4!8' SI 'l' (dol suce) NO !2' (Ilt, 1
-AU~lcolctlr.pll '1'2'3'4!8' SI '1! (dot luccl NO !2! (Ilt)
-Hlt-e :sper.:heue) .
... -...... _----_ ... _-- '1'2'3'1t'8' SI 'li (dol syec) NO 12 1 (alt)
--------------- ___ w .... __ •• ___
-N,a, 1 MLTO uh 1. 2 A6SASTANZA IJh le 3 POCO 'Jhl, 4 INllTILE 8, NON 50

1/;. 1:'~-;~:ït~·~r·-r~A~d/:I':tt7/:,·{y.~,.",·'\~''''-!:'~t \1~ _"'.::. ï."~~
!J TABELLA 4 ALCOOL Cl
e. rU"t.t. all. tIeIidw sotta ildieah:
.'8uRto t eowilto I)_li di 1111 hl _ttatt 0 CllMiglim o 51 l, .. _tt.t. QI. MDtt., 1 -dMt 'iel'Vana I.na ... volt. i ... i ..... teeaat. ... i. 4UIli easi 10 fa / ha fatto
.. 110 dit ,.... .... UI 1.0 uti1iü ~i~ili pi~ ritpDltl) .
5BfI[ FGITI III PlESt-:NlA Dl SU &"R1 .... IMT.I .. niE (dl alcool) RIatIESn CASt RIeta
-Pucottripii !112IJ I 4!8! 51 ! 1! <doit. succ.) HO !21 (ilt)
-Invito/raccoaaftdlzlonl
dtl Mdico UftI bntta 1112IJ!4 18! SI !1! <".succ.) NO !2! (ilt)
-IftYltl/racCDllft6azloni
dll 1141CO ripttutl '112'3!418! SI !1! (daI.succ.) 110 !2! (ait)
~lcaoli,tl IftOnili !1 12!J!4 I BI 51 !1! (",succ.) NO !2! (lit)
-f Il'IIICOUripia !112!3!4!8! 51 !t! (".suce.) NO !2! (ait)
-Agopuftturi '1!2!314!81 SI Il! (a. suee. ) NO !2! (lIt)
-Altre (speciflcare)
i '11:'314181 SI 111 (dol. suce.) NO '2 1 (alt) : ----------------- ~
-----------------. -----------------
~
(4 E 1101 ta 'Jtlle 2 abbi5tanza utIle 3- pGCo utile ft IfllJhle 8- non 50
-.1 • ..... 2· : ... :-K .. -:r....C_.!...cJ.., .. '.I.'1:.!i .... t~J~.§.~"'''".,. 4& J •.. :\) n~., , .. ,.