Russell 1990 Br Heart J
6
Br Heart J 1990;63:195-9 MEASUREMENT Automated non-invasive measurement of cardiac output b y the carbon dioxide rebreathing method: comparisons with dy e dilution a n d thermodilution A E Russell, S A Smith, M J West, P E Aylward, R J McRitchie, R M Hassam, R B Minson, L M H Wing, J P Chalmers Department of Medicine, Flinders Medical Centre, Bedford Park, South Australia A E Russell S A Smith M J West P E Aylward R J McRitchie R M Hassam R B Minson L M H Wing J P Chalmers Correspondence to Professor J P Chalmers, Department of Medicine, Flinders Medical Centre, Bedford Park, South Australia 5042, Australia. Accepted for publication 21 September 1989 Abstract The accuracy and reproducibility of indirect measurement of cardiac output at rest the carbon rebreathing (indirect Fick) method with an automated respiratory analysis system (Gould 9000IV) were compared with simultaneous measurements made in duplicate b y dy e dilution and thermo- dilution in 25 patients having cardiac catheterisation studies. Measurements of cardiac output b y the carbon dioxide rebreathing method were not signifi- cantly different from those obtained with dy e dilution (mean difference - 03 I/min, SD 0 76 , 95 confidence interval - 0 7 to 041). Thermodilution significantly over- estimated cardiac output by a mean of 2- 2 1/min or 39 (SD 15, 95 confidence interval 1- 6 to 2-8) compared with the carbon dioxide rebreathing method and significantly overestimated cardiac out- by 1 9 1/min or 31 (SD 1-2, 9 5 confidence interval 1- 2 to 2-5) compared with dy e dilution. The reproducibility of measurements of cardiac output in individual patients was satisfactory with the dye dilution method bu t wa s poor with carbon dioxide rebreathing and thermodilution. Indirect measurement of resting cardiac output by the Gould 9000IV automated carbon dioxide rebreathing method is more accurate bu t the variability inherent with this method requires that measurements be taken for each determination. Measurement of cardiac output by the thermodilution method by a commer- cially available cardiac output computer was no t satisfactory because not only was there considerable variability between repeat measurements bu t th e method also consistently overestimated cardiac output compared with the dy e dilution method. Although cardiac output is a haemodynamic variable of considerable interest in clinical cardiology an d cardiovascular research, simple an d accurate non-invasive methods fo r its measurement have no t been readily available. In current practice the indicator dilution methods, dye dilution an d thermodilution, have replaced the direct Fick method because of their relative ease an d suitability fo r automation.'2 The invasive nature of these techniques limits their application an d accord- ingly non-invasive methods including elec- trical bioimpedance cardiography,' echo- cardiography,4 5 radionuclide angiography,6 an d the indirect Fick method7 have been developed. These methods ca n be used fo r serial estimations but are limited by technical difficulty or doubts about their accuracy.89 The indirect Fick or carbon dioxide rebreathing method has been available fo r many years an d in general has an accuracy fo r measurement of cardiac output similar to that of other methods. '2 The Gould 9000IV cardiopulmonary exercise system (Gould, Dayton, Ohio) is an automated system fo r respiratory analysis that has removed much of the technical difficulty in performing indirect Fick measurements. It is relatively easy to use an d is ideal f or performing repeated estimates of cardiac output in ambulatory individuals. We compared indirect Fick measurements of cardiac output made by the Gould 9000IV with simultaneous measurements of cardiac output made by dye dilution an d thermodilution an d we obtained a measure of the reproducibility of each method. Previous studies have largely relied upon correlation to compare methods.' 0 1 4 While tw o estimates may be highly correlatedthe estimates may still show poor agreement in individual subjects.'5 16 We used the method of Bland an d Altman'5 to examine the agreement between an d the reproducibility of different methods fo r estimating cardiac output. Patients and methods PATIENTS We studied 25 patients undergoing diagnostic right an d left heart catheterisation fo r valvar heart disease or cardiomyopathy. There were 17 men an d eight women (aged 28-80 years (median = 67). In all but on e a multiple lumen thermistor tipped catheter (Swan-Ganz) wa s placed into the pulmonary artery vi a the right femoral vein. The left heart catheter wa s inserted vi a the right femoral artery. All patients were fully informed of the study 195
-
Upload
otinanai09 -
Category
Documents
-
view
213 -
download
0
Transcript of Russell 1990 Br Heart J

7/27/2019 Russell 1990 Br Heart J
http://slidepdf.com/reader/full/russell-1990-br-heart-j 1/5
Br Heart J 1990;63:195-9
MEASUREMENT
Automated non-invasive measurement of cardiacoutput by the carbon dioxide rebreathing method:
comparisons with dye dilution and thermodilution
A E Russell, S A Smith, M J West, P E Aylward, R J McRitchie, R M Hassam,R B Minson, L M H Wing, J P Chalmers
Department ofMedicine, FlindersMedical Centre,Bedford Park,South AustraliaA E RussellS A SmithM J WestP E AylwardR J McRitchieR M HassamR B MinsonL M H WingJ P Chalmers
Correspondence to
ProfessorJ
P Chalmers,Department of Medicine,Flinders Medical Centre,Bedford Park, SouthAustralia 5042, Australia.
Accepted for publication21 September 1989
AbstractThe accuracy and reproducibility ofindirect measurement of cardiac outputat rest by the carbon dioxide rebreathing(indirect Fick) method with an
automated respiratory analysis system(Gould 9000IV) were compared withsimultaneous measurements made induplicate by dye dilution and thermo-dilution in 25 patients having cardiaccatheterisation studies. Measurements ofcardiac output by the carbon dioxiderebreathing method were not signifi-cantly different from those obtained withdye dilution (mean difference - 03 I/min,SD 0 76 , 95 confidence interval - 0 7 to041). Thermodilution significantly over-estimated cardiac output by a mean of2- 2 1/min or 39 (SD 15, 95 confidence
interval 1- 6 to 2-8) compared with thecarbon dioxide rebreathing method andsignificantly overestimated cardiac out-put by 1 9 1/min or 31 (SD 1-2, 95confidence interval 1-2 to 2-5) comparedwith dye dilution. The reproducibility ofmeasurements of cardiac output inindividual patients was satisfactory withthe dye dilution method but was poorwith carbon dioxide rebreathing andthermodilution.
Indirect measurement of restingcardiac output by the Gould 9000IVautomated carbon dioxide rebreathing
method is more accurate but thevariability inherent with this methodrequires that multiple measurementsbe taken for each determination.Measurement of cardiac output by thethermodilution method by a commer-cially available cardiac output computerwas not satisfactory because not only wasthere considerable variability betweenrepeat measurements but the methodalso consistently overestimated cardiacoutput compared with the dye dilutionmethod.
Although cardiac output is a haemodynamicvariable of considerable interest in clinicalcardiology and cardiovascular research, simpleand accurate non-invasive methods fo r itsmeasurement have not been readily available.
In current practice the indicator dilutionmethods, dye dilution and thermodilution,have replaced the direct Fick method becauseof their relative ease and suitability fo rautomation.'2 The invasive nature of these
techniques limits their application and accord-ingly non-invasive methods including elec-trical bioimpedance cardiography,' echo-cardiography,4 5 radionuclide angiography,6and the indirect Fick method7 have beendeveloped. These methods can be used fo rserial estimations but are limited by technicaldifficulty or doubts about their accuracy.89The indirect Fick or carbon dioxide
rebreathing method has been available formany years and in general has an accuracy fo rmeasurement of cardiac output similar to thatof other methods. '2 The Gould 9000IVcardiopulmonary exercise system (Gould,
Dayton, Ohio) is an automated system fo rrespiratory analysis that has removed much ofthe technical difficulty in performing indirectFick measurements. It is relatively easy to useand is ideal for performing repeated estimatesof cardiac output in ambulatory individuals.We compared indirect Fick measurements of
cardiac output made by the Gould 9000IV withsimultaneous measurements of cardiac outputmade by dye dilution and thermodilution andwe obtained a measure of the reproducibilityof each method. Previous studies havelargely relied upon correlation to comparemethods.'0 14 While two estimates may be
highly correlated the estimates may still showpoor agreement in individual subjects.'5 16 Weused the method of Bland and Altman'5 toexamine the agreement between and thereproducibility of different methods fo restimating cardiac output.
Patients and methodsPATIENTS
We studied 25 patients undergoing diagnosticright and left heart catheterisation fo r valvarheart disease or cardiomyopathy. There were17 men and eight women (aged 28-80 years(median = 67). In all but one a multiple lumenthermistor tipped catheter (Swan-Ganz) wasplaced into the pulmonary artery vi a the rightfemoral vein. The left heart catheter wasinserted via the right femoral artery. Allpatients were fully informed of the study
195

7/27/2019 Russell 1990 Br Heart J
http://slidepdf.com/reader/full/russell-1990-br-heart-j 2/5
Russell, Smith, West, Aylward, McRitchie, Hassam, Minson, Wing, Chalmers
details and then gave written consent toparticipation. The study was approved by thecommittee on clinical investigation of the
Flinders Medical Centre.
CARBON DIOXIDE REBREATHING MEASUREMENTS
(INDIRECT FICK)The Gould 9000IV consists of an infrared
absorption analyser for carbon dioxide, aparamagnetic oxygen analyser, a dry rollingseal spirometer, and a microcomputer with ananalogue to digital converter and a printer. Itprovides measurements of the concentration ofexpired carbon dioxide with resolution to0 01 and an accuracy of ±0 1 whenmeasuring concentrations from 0 to 10 .Minute volume is measured with resolution to0 01 1/min and an accuracy of ±0-025 1/min.These variables have been independentlyvalidated.'7 The analysers and the spirometerwere calibrated before each study according tothe manufacturer's instructions.
With this method t he ca rd ia c output iscalculated by the equation:
Cardiac output = Vco2/(Cvco2 - Caco2)
where Vco2 is th e rate of production of carbondioxide per minute calculated from continuousmeasurements of expired minute volume andthe concentration of carbon dioxide in expiredgas. Cvco2 is the concentration of carbondioxide in mixed venous blood and Caco2 is theconcentration of carbon dioxide in arterialblood. The arteriovenous difference in theconcentration of carbon dioxide is calculatedby th e formula:Cvco2 -Caco2 = 11 02(Pvco20396 -Paco203 )where Pvco2 and Paco2 ar e th e partial pressureof carbon dioxide in venous and arterial bloodrespectively.'120 A haemoglobin concentrationof 150 g/ l and oxygen saturation of 95 wasassumed. The partial pressure of carbon diox-id e in arterial blood was estimated from theconcentration of carbon dioxide in expired gasat the end of expiration. The carbon dioxidetension ofmixed venous blood was estimated ina similar way by using the equilibriumrebreathing procedure described by Collier.The individual respired from an anaestheticbag filled with a mixture of approximately 100%carbon dioxide in oxygen. The volume in thebag was fixed at 1-5 times the mean tidalvolume of th e preceding respirations. Duringthe rebreathing procedure the end tidal con-centration of carbon dioxide was displayed onthe computer screen s o t ha t the operator couldsignal to the computer that a satisfactoryequilibrium had been achieved. Theequilibrium value was used to e st im at e t hemixed venous carbon dioxide tension. Nocorrection was made for differences betweenblood and alveolar tensions.'0 1822 Thecomputer performed all the calculations anddisplayed the estimated cardiac output.
THERMODILUTION MEASUREMENTS
Measurements of cardiac output were takenusing the 7 French pulmonary arterial catheter(Swan-Ganz, 93A-151-7F, American EdwardsLaboratories, Anasco, Puerto Rico) linked to a
9520A cardiac output computer (EdwardsLaboratories, Santa Ana, California). Ten mlof iced 5 dextrose drawn in to a 10 ml plasticsyringe was hand injected into the right atriumvia the proximal lumen of the Swan-Ganzcatheter. The thermodilution cardiac outputwas taken as the value for the second of two orthree injections.
DYE DILUTION MEASUREMENTS
Dye dilution measurements were made with 5or 10 mg of indocyanine green (Cardio-green,HW D Baltimore, Maryland) (the larger dosewas used fo r those with mitral valve disease)injected by hand into the right atrium vi a theproximal lumen of the Swan-Ganz pulmonaryartery catheter. Arterial blood was drawn fromth e proximal aorta through a DC-410photoelectric detector with a SW-367 pump(Waters Instruments, Rochester, Minnesota).Cardiac output was calculated with aCO- 10 cardiac output computer (Waters
Instruments).
EXPERIMENTAL PROTOCOL
Al l measurements of cardiac output were takenat the end of the diagnostic study. The patientsremained supine and breathed room air vi a arespiratory valve connected by a flexible hoseto the spirometer of the Gould 9000IV so thatal l expired gas could be collected and analysed.Indocyanine green was injected at the onset ofcarbon dioxide rebreathing and this injectionwas immediately followed by the two or three
injections of thermodilution indicator. Thissequence was repeated within approximately
10 minutes. In the patients who were not givenindocyanine green, the thermodilutionindicator was injected at the start of the
rebreathing procedure. From the 25 subjectswe obtained 24 duplicate indirect Fickmeasurements with 24 paired thermodilutionreadings, and 19 pairs of measurements fo r dyedilution. This gave 23 comparisons betweenthe carbon dioxide rebreathing and thermo-dilution methods and 18 comparisons betweenthe indirect Fick and dye dilution methods andbetween thermodilution and dye dilution. In17 of th e patients cardiac output was estimatedusing all three methods.
ANALYSIS
For each patient the cardiac output by each ofthe three methods was taken as the mean of thetwo measurements with each method. Thevalues of cardiac output in each subjectobtained by the three methods were comparedby analysis of variance in a repeated measurestwo factor design. Individual comparisonswere made by the Newman-Keuls multiplerange test. Differences between cardiac outputvalues obtained by the three methods wereexamined by the method of Bland and Altmanin which the individual differences between thetwo methods in each individual are plottedagainst the average value obtained from bothmethods in that individual.'5 The mean, stan-
dard deviation, and 95 confidence interval ofthe differences were calculated. We also com-
pared mean values fo r each method with one
196

7/27/2019 Russell 1990 Br Heart J
http://slidepdf.com/reader/full/russell-1990-br-heart-j 3/5
Automated non-invasive measurement of cardiac output by th e carbon dioxide rebreathing method
Table 1 Reproducibility of different methods fo r estimating cardiac output
Dye,/Dye, Fickj/Fick, Thernal,/ Thermal2Comparison (n ) (19) (24) (24)
Mean difference (1/min) between duplicates 0-22 -0-31 -0-39Standard deviation of difference 0 44 1 35 1 11Coefficient of repeatability (2 x SD) 0-88 2 7 2- 2
another using scatter plots.The accuracy of both the carbonrebreathing and thermodilution met}assessed from the mean differenceseach of these methods and dye dilut limits of agreement '5 were calculathe mean difference plus and minus
standard deviation of the difference s
950/ of differences were within that radifferences between the values obtaineindividual fo r the carbon dioxide re tand thermodilution methods were exaa similar fashion.The reproducibility (repeatability)
method was examined by plotting theces between duplicate measurementthe average of the two measuremenmean and standard deviation of the dibetween the two readings were calcithat the coefficient of repeatability'the standard deviation of the differencbe calculated.
ResultsREPRODUCIBILITY OF DIFFERENT METHC
CARDIAC OUTPUT
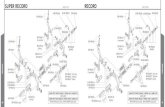
For each method there was no sidifference between the duplicate l
ments (table 1). For dye dilution adifferences were less than 16%/ of tvalue f ig la). For the indirect Fick mcreproducibility was low with only 50
Figure I Differencesbetween the first andsecond estimate of cardiacoutput with each methodplotted against the mean ofthose two measurements bydye dilution (a),thermodilution (b), andindirect Fick (c).
-
E I
I
c
4,
ou
_ -
a
C]
4,
la
4,
.a
a
inL.
4,
21Dye,-Dye2 (i )
.
1 2 3 : 6 7 8
3 Thermal1 -Thermal2 cg
2
0~~~~~~~ 2 3 . *. 6 7 ..
3
.3_3.
3 Fick, -Fick2 Q
2
A1 *
1
-2-
-3
-L
1 2. . - 5 6 7 8.
*
Mean cardiac output (I/min)
dioxidehods wasbetweenion. Theted fromtwice thesuch thatnge. Thed in each
differences being within 20 of the mean value(fig ic). For thermodilution reproducibilitywas such that 70 of the differences werewithin 20 of the mean value (fig lb).
DIFFERENCES BETWEEN METHODS
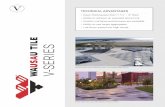
The mean values with the indirect Fick methodand the dye dilution method were not sig-nificantly different, although the limits ofagreement were wide (table 2) with 28 of the
differences being > 20 of the mean value f ig2a). The mean thermodilution value was 310greater than the dye dilution value (p < 0-001)and 390/0 greater than that by the indirect Fickmethod (p < 0-001) (table 2) . For both com-
parisons with thermodilution the range ofdifferences was wide f ig 2).
)reathing Discussionmined in In this study we found no systematic difference
between estimates of cardiac output made by of each the indirect Fick and dy e dilution methods but
differen-measurements
obtained bythe
thermodilutions against method consistently overestimated the cardiac
tS 15 The output compared with measurements obtained
fferences by the other two methods. The reproducibilityulated so of estimates of cardiac output within an
15 (twice individual was significantly worse fo res) could mesurements obtained by carbon dioxide
rebreathing or by thermodilution than it wasfor those obtained by dye dilution. The poorreproducibility of these two methods con-tributed to the wide range of differences seen
)DS FOR between methods.
Several factors contribute to the consider-[gnificant able variation seen between repeatedmeasure- measurements of cardiac output with any oneIll of the method. One important factor is that the car-:he mean diac output is not a tightly regulatedethod the haemodynamic variable such as blood
of the pressure 3 and biological variability betweenmeasurements is considerable.2425 In addition,both thermodilution and dye dilution are
subject to random errors owing to variation inthe dose of indicator and it s rate of injection, tothe pulsatile nature of blood flow, and to
9 10 11 variation in the calculation of the area under theindicator dilution curve.'2426 Thermodilutionis also subject to variation from the placementof the thermistor in the pulmonary artery andfrom physiological variations in the tem-
perature of pulmonary arterial blood with* respiration.'2426 For indirect Fick
1W 11 measurements of cardiac output small randomerrors in the estimation of the arterial andmixed venous carbon dioxide concentrationsfrom the end tidal and the rebreathingequilibrium concentrations of carbon dioxidecan result in relatively large errors in th eestimate of the arteriovenous difference fo rcarbon dioxide concentration.27 28 Thisproblem-seems to be less important when thearteriovenous difference is large such as during
g Tli exercise, when the carbon dioxide rebreathingmethod has been found to be more reliable.72729
Another important source of variation is thatsmall deviations in ventilation and alveolarcarbon dioxide tension can result in largechanges in carbon dioxide transfer and thuscarbon dioxide production.28
197
vI

7/27/2019 Russell 1990 Br Heart J
http://slidepdf.com/reader/full/russell-1990-br-heart-j 4/5
Russell, Smith, West, Aylward, McRitchie, Hassam, Minson, Wing, Chalmers
Table 2 Comparisons of different methodsfor cardiac output
Fick-Dye Thermal-Dye Thermal-FickComparison (n ) (18) (18) (23)
Mean difference -0 28 1-85* 2-16*(1/min) (950° CI) (- 0 66 to 0 07 ) (1 24 to 2 47) (1-52 to 2 79)
Standard deviation of difference 0 76 1-24 1-49Lower limit of agreement - 1-80 - 0-63 -0-82(95 CI) (-245 to -1 15 ) (-1-18 to -008) (4 09 to 6 19
Upper limit of agreement 1-24 4-33 5-14(950oCI) (0 59 t o 1 -8 9) (3-78 to 4-87) (-187 to 0 23
*p < 0-001.
Apparent differences between estimates ofcardiac output by any two methods may stemboth from random variation within eachindividual method (poor reproducibility) orfrom systematic differences between onemethod and another. The dye dilution methodhas been accepted as a gold standard becauseno systematic bias has been found betweendirect (oxygen) Fick and dye dilution estimatesof cardiac output.303' Our results for th e com-parison of indirect Fick and dye dilutionestimates of cardiac output ar e consistent with
such previous observations and with compar-isons of th e indirect Fick method with dyedilution7 12 or with th e direct Fick method. 24The thermodilution method is well establishedin clinical practice and is capable of providingaccurate estimates of cardiac output providedthat appropriate corrections are made forseveral potential errors.'026 The method issubject to overestimation of cardiac output,such as that observed in this study, owing toloss of indicator before and after injection. 26Loss of indicator can be reduced by injection atambient temperature at the expense of a reduc-tion in th e thermistor signal to noise ratio and
thus greater variability in the estimate of car-
diac output.' The thermodilution cardiac out-put computer used in this study uses a com-putation constant to adjust for loss of indicatorwith different Swan-Ganz c at he te rs t ha t isderived from an in vitro study (productliterature). The recommended constant maynot be correct for catheters inserted from thefemoral vein where the longer intravascular
course could result in greater loss of indicator.None the less, an in vitro study using ther-modilution cardiac output computers (includ-in g the model used in this study) obtainedsimilar overestimates of cardiac output underconditions of cold injection and pulsatile flow.'The computer used in the present study alsooverestimated cardiac output when comparedwith invasive Fick measurements in anotherstudy.32 Further evaluation of such devices isneeded before they can be used as a standard fo rcomparison with other methods.' 33
In previous studies comparing differentmethods for estimating cardiac output the
range of differences between estimates has beenwide and a considerable number of differenceswere > 25 of the mean value.7 1222 The rangeof differences seen in the present study issimilar to that reported between direct Fickand indirect Fick 2229 or dye dilution73'estimates. Such observations ar e consistentwith the inherent variability of cardiac outputand of the methods available fo r it s estimation.We found t ha t i nd ir ec t Fick estimates of
resting cardiac output measured by the Gould90001V ar e accurate but that the variability ofestimates is large. Averaging of repeatedmeasurements is required to achieve a reliableestimate of cardiac
outputin
individualsubjects.
Figure 2 Differencesbetween cardiac outputestimates by two differentmethods plotted against themean of those twoestimates; indirect Fickand dye dilution (a);themodilution and dyedilution (b); indirect Fickand thermodilution (c).
3-
2-
1 -
0
._
' 5- A
GoL4.E
3-Q, 2-0
u
av 1z1-0
U 5-
c
4,
~: -1-
.I-
.0
4, 5-uC
4,
3-
2-
1
0
-1
Fick-Dye ( SAS was a British Heart Foundation/Australian National HeartFoundation reciprocal travelling fellow. AER was supported bya scholarship from th e Lions Heart Research Foundation ofSouth Australia.
I -T
1i 3i 4 5 6 7 8 9 10
* 0
Thermal- Dye (
~~~~ 0
0
0 a~~~~
* -0.0 .
2 i l 7 8 lo1
Thermal- Fick0
0
0
0
0
0
0 I-
1 2 3 L 6 7 8 9 10
Mean of cardiac output estimates obtainedby two different methods (I/min)
1 Mackenzie JD, Haites NE , Rawles JM. Method of assessingth e reproducibility of blood flow measurement: factorsinfluencing the performance of thermodilution cardiacoutput computers. Br Heart J 1986;55:14-24.
2 Swan HJC, Ganz W, Forrester J, Marcus H, Diamond G,Chonette D. Catheterisation of the heart in man with useof a flow directed balloon-tipped catheter. N Engl J Med1970;283:447-5 1.
3 Kubicek WG, Karegis JN, Patterson RP, Witsoe DA,Mattson RH. Development and evaluation of animpedance cardiac output system. Aerospace Med1966;37: 1208-12.
4 Williams GA, Labovitz AJ. Doppler estimation of cardiacoutput: principles and pitfalls. Echocardiography 1987;4:355-74.
5 Rawles JM, Haites NE. Doppler ultrasound measurement ofcardiac output. Br J Hosp Med 1984;31:292-7.
6 Jeremy R, Tokuyasu Y, Cheong CY. The reproducibility ofnongeometric analyses of cardiac output and left ven-tricular volume by radionuclide angiography. Am Heart J1985;11O:1020-5.
7 Ferguson RJ, Faulkner JA, Julius S, Conway J. Comparisonof cardiac output determined by CO , rebreathing and dye-dilution methods. J Appl Physiol 1968;25:450-4.
8 Franciosa JA. Application of noninvasive techniques fo rmeasuring cardiac output in hypertensive patients. AmHeart J 1988;116:650-6.
9 Dobb CJ , Donovan KD. Non-invasive methods of measur-ing cardiac output. Intensive Care Med 1987;13:304-9.
10 Hargreaves M, Jennings G. Evaluation of the CO , rebreath-ing method for the non-invasive measurement of restingcardiac output in man. Clin Exp Pharmacol Physiol1983;10:609-1 3.
11 Muiesan G, Sorbini CA, Solinas E, Grassi V, Casucci G,Petz E. Comparison of CO,-rebreathing and direct Fickmethods for determining cardiac output. J Appl Physiol1968;24:424-9.
198
0 ob

7/27/2019 Russell 1990 Br Heart J
http://slidepdf.com/reader/full/russell-1990-br-heart-j 5/5
Automated non-invasive measurement of cardiac output by th e carbon dioxide rebreathing method
12 Franciosa JA, Ragan DO, Rubenstone SJ . Validation of theCO, rebreathing method for measuring cardiac output inpatients with hypertension or heart failure. JLab Clin Med1976;88:672-82.
13 Smith SA, Russell AE, West MJ , Chalmers J. Automatednon-invasive measurement of cardiac output: comparisonof electrical bioimpedance and carbon dioxide rebreathingtechniques. Br Heart J 1988;59:292-8.
14 Kubo SH, Burchenal JEB, Cody RJ. Comparison of directFick and thermodilution cardiac output techniques at highflow rates. Am J Cardiol 1987;59:384-6.
15 Bland MJ, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurement.
Lancet 1986;i:307-10.16 Altman DG. Statistics and ethics in medical research. V-Analysing data. Br Med J 1980;281:1473-5.
17 Eccles RC , Swinamer DL, Jones RL , King EG. Validationof a compact system for measuring gas exchange. CritCare Med 1986;64:807-1 1.
18 Jones NL, Campbell EJM. Clinical exercise testing. 2nd ed.Philadelphia: WB Saunders, 1982:130-46.
19 McHardy GJR. Relationship between the difference inpressure and content of carbon dioxide in arterial andvenous blood. C li n S ci 1967;32:299-309.
20 Gould 9000IV operators manual. Cardiac output. MedicalProducts Division, Dayton OH: Gould, 1983.
21 Collier CR. Determination of mixed venous CO2 concentra-tions by rebreathing. J Appl Physiol 1956;9:25-9.
22 Davis CC, Jones NL, Sealey BJ. Measurement of cardiacoutput in seriously ill patients using a CO 2 rebreathingmethod.Chest 1978;73:167-72.
23 Dobbs WA, Prather JW, Guyton AC . Relative importance
of nervous control of cardiac output and arterial pressure.Am J Cardiol 1971;27:507-12.
24 Levett JM, Replogle RL. Thermodilution cardiac output: acritical analysis and review of the literature. J Surg Res1979;27:392-404.
25 Haites NE, Mowat DHR, McLennan FM, Rawles JM. Howfar is th e cardiac output? Lancet 1984;ii:1025-7.
26 Nadeau S, Noble WH. Limitations of cardiac outputmeasurements by thermodilution. Ca n Anaesth Soc J1986;33:780-4.
27 Wilmore JH, Farrell PA, Norton AC, et al. An automated,indirect assessment of cardiac output during rest andexercise. J Appl Physiol 1982;52:1493-7.
28 Guyton AC . Circulatory physiology: cardiac output and itsregulation. Philadelphia: WB Saunders, 1963:39.29 Clausen JP, Larsen OA, Trap-Jensen J. Cardiac output in
middle-aged patients determined with CO2 rebreathingmethod. J Appl Physiol 1970;28:337-42.
30 Reddy PS, Curtiss EI , Bell B, et al. Determinants ofvariation between Fick and indicator dilution estimates ofcardiac output during diagnostic catheterization. Fick vs.dye cardiac outputs. J Lab Clin Med 1976;87:568-76.
31 Hamilton WF, Riley RL, Attyah AM, et al. Comparison ofth e Fick and dye injection methods of measuring cardiacoutput in man. Am J Physiol 1948;153:309-21.
32 van Grondelle A, Ditchey RV, Groves BM, Wagner WW,Reeves JT. Thermodilution method overestimates lowcardiac output in humans. Am J Physiol 1983;245:H690-2.
33 Shuster AH, Nanda NC. Doppler echocardiographicmeasurement of cardiac output: comparison with a non-golden standard. Am J Cardiol 1984;53:257-9.
199