Routine clotting studies - a bloody waste of resources? Joanne Bratchell Lead Nurse Pre-operative...
19
Routine clotting studies - a bloody waste of resources? Joanne Bratchell Lead Nurse Pre-operative Assessment St George’s Hospital, Tooting Antonia Field-Smith Specialist Registrar in Haematology
-
Upload
crystal-knight -
Category
Documents
-
view
216 -
download
2
Transcript of Routine clotting studies - a bloody waste of resources? Joanne Bratchell Lead Nurse Pre-operative...
Routine clotting studies -a bloody waste of resources?
Joanne BratchellLead Nurse Pre-operative AssessmentSt George’s Hospital, Tooting
Antonia Field-Smith Specialist Registrar in Haematology

Defensive?

Persuasion?
The problem with clotting screens
Do not predict bleeding risk in most patients
Do not accurately reflect in vivo haemostatic response
Designed to detect factor deficiencies in patients with high pre-test probability of bleeding
Low sensitivity and specificity

The clotting cascade

Causes of abnormal clotting screens
Shortened clotting times slow or difficult
venepuncture incorrect volume of
blood in tube inadequate mixing usually not clinically
significant ?increased
thrombotic risk
Prolonged clotting times flawed collection or
prolonged storage anticoagulants heparin
contamination coagulation factor
deficiency inherited acquired
lupus anticoagulant factor inhibitor

Background
Lack of clear NICE guidelines meant clotting screens routinely ordered pre-operatively in our Trust
All evidence available concludes that routine testing in apparently healthy or asymptomatic individuals is unlikely to lead to little if any benefit (Munro et al 1997, ASA 2002, NICE 2003, British Committee Standards in Haematology 2008 )

Aims and Objectives
To determine whether preoperative clotting screens were requested in adherence with Trust guidelines
To determine whether abnormal clotting results affect the clinical management or surgical outcome of elective surgical patients

Methodology
Data collected over 2 week period Included all elective surgery
patients over 18 years of age from 4 care groups attending pre-op clinic
Staff asked to record whether clotting screen requested and why indicated

Results
120/181 (66.2%) patients had clotting screens requested
Only 16 (13.3%) studies requested in line with guidelines
78 (65%) ordered routinely 23/120 (19%) prolonged abnormal
clotting screens

Abnormal results
Causes of abnormal clotting screens in 34 patients out of 120 with clotting screens requested
8
7412
1
11
Warfarin
Borderline raised APTR
APTR >1.3
Factor XI deficiency
Borderline raised INR
Borderline raised TT
Shortened APTR

Outcome
No change to clinical management in patients with abnormal clotting results
Only 5 out of 14 patients with unexplained prolonged clotting times had repeat testing
Perioperative bleeding in 5 patients with prolonged clotting screens All major orthopaedic cases – likely surgical
bleeding

The best way forward?
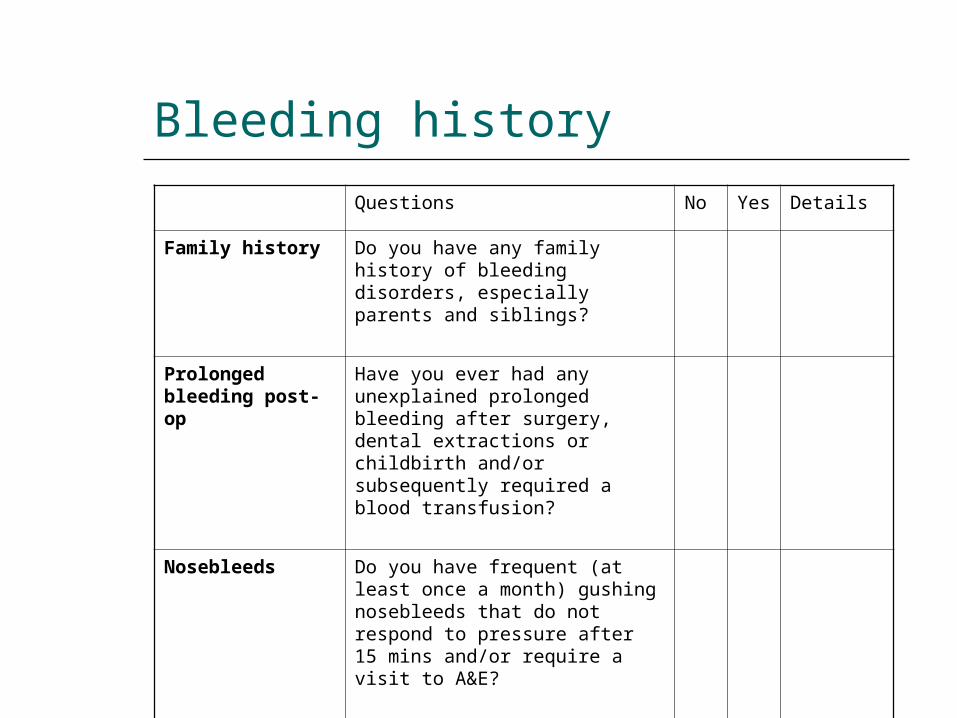
Bleeding history
Questions No Yes Details
Family history Do you have any family history of bleeding disorders, especially parents and siblings?
Prolonged bleeding post-op
Have you ever had any unexplained prolonged bleeding after surgery, dental extractions or childbirth and/or subsequently required a blood transfusion?
Nosebleeds Do you have frequent (at least once a month) gushing nosebleeds that do not respond to pressure after 15 mins and/or require a visit to A&E?

Revised guidelines
Clotting screen
All abnormal results should be repeated
Discuss any persistently abnormal results with Haematology registrar
Positive bleeding history• Family history of bleeding disorder• Prolonged post-op bleeding• Nosebleeds
Refer to haematology
Liver disease
Renal disease eGFR < 30 or on dialysis
Known bleeding disorder Liaise with Haemophilia team
On anticoagulants Not at pre-op visit
Jehovah’s witnesses

Recommendations for practice
Stop ordering routine clotting studies! If positive bleeding history, refer to
haematology All abnormal results should be repeated Refer to haematologist if result remains
abnormal Stop ordering clotting test for warfarin pts
at pre-op visit

Financial implications
Clotting studies at St George’s cost £3.51 a time representing £ thousands per year
In average year, approx £10,500 on pre-op clotting tests
Potential saving of £9000 by adhering to guidelines

Conclusion
Routine clotting studies have no value in the management of elective surgery patients
Limited value to patients and significant cost implications to the Trust
Clotting studies should only be ordered when indicated by medical history or local guidelines

Thank you
Any questions?