
Root Canal Irrigation During Endodontic Treatment
35
Irrigation of Root Canal Assembled by Dr. Osama Asadi, B.D.S
-
Upload
iraqi-dental-academy -
Category
Health & Medicine
-
view
669 -
download
11
Transcript of Root Canal Irrigation During Endodontic Treatment
Irrigation of Root Canal
Assembled by Dr. Osama Asadi, B.D.S
Root Canal Infection
One must know, microorganisms are the main reason for endodontic failure.• Bacterial species present frequently in necrotic root canal are
1) Obligate anaerobes, easily eradicated during root canal treatment.
2) Facultative anaerobes, difficult to eradicate. Such as Steptococci, Enterococci, Lactobacilli.
3) Enterococcus Faecalis, has gain attention in the endodontic literature as it frequently be isolated from root canal in case of failed root canal treatment.

Common Irrigants
Sodium Hypochlorite Chlorhixidine

Sodium Hypochlorite
• Most common irrigant• Used as primay irrigant• Allergies are rare• Concentration (0.25%-5.25%)• Using higher concentration
result in greater effect, but it more toxic.
advantages of NaOCl • Mechanical flushing of debris from the
canal• Dissolvent for vital and necrotic tissue• Antimicrobial action• Lubricating action• Cheap
• Using low concentration hypochlorite (2.5%) and having the same effect as ( 5%) can be obtained by:1. Heating the solution2. Activation with ultrasonic tips3. consuming more volume of solution 4. Instrumentation coupled with irrigation
• It’s still controversial how much time irrigant should be left in canal, but 30 minutes seems reasonable.
Dilution of Sodium Hypochlorite
• 1 Volume of NaOCl + 1 Volume of Saline = ½ concentration
• 1 volume of NaOCl + 2 volume of Saline = 1/3 concentration
Examples:
• 1 cup of 5% NaOCl + 1 cup of Saline = 2 cups of 2.5% NaOCl
• 1 cup of 5% NaOCl + 2 cup of Saline = 3 cups of %1.6 NaOCl
Notice: the higher the concentration, the higher the toxicity.
Chlorhexidine
• Has a broad antimicrobial activity
• Has little toxicity • Concentration ( 0.2% - 2% )• Soluble form: Chlorhexidine
gluconate
Advantages and disadvantages of CHx • Mechanical flushing of debris from the
canal• Can’t dissolve necrotic tissue • Broad spectrum antimicrobial action• Can’t remove smear layer• Cheap
The efficiency of Chx In vitro has shown to be effective, while in vivo it’s still controversial.
Anyway, the effectiveness of Chx as intracanal irragant is overrated, as most supportive studies has been done in vitro, and shown effective against gram positive cocci. These cocci rarely found in primary endodontic infection.
Moreover, randomized clinical trials has found that 2.5% hypochlorite is significantly more effective than 0.2% chlorhexidine.
Smear Layer
• Defined as surface film of debris retained on dentin or another surface after instrumentation.
• It consist of dentin particles, remnant of necrotic or vital pulp tissue, bacterial component and retained irrigants.
• The importance of smear layer in endodntic treatment is still controversial, some researchers suggest removing it, others suggest retaining it as protection to bacterial invasion into dentinal tubules.
• To remove smear layer, we use Chelating agents
Common Chelating agent
• EDTA
• MTAD ( commercially known as BioPure ® and TetraClean ®
• QMix
EDTA
• Colorless soluble product.
• Common Chelating agent
• Effective on removal of smear layer and pose no effect on organic tissue. So irrigation with EDTA alone is not ideal.
• Also pose little or no antimicrobial activity.
• Concentration in edodontics is 17%
• Recommended irrigation time is 1 minutes or so. Irrigation for longer period cause excessive removal of dentin.
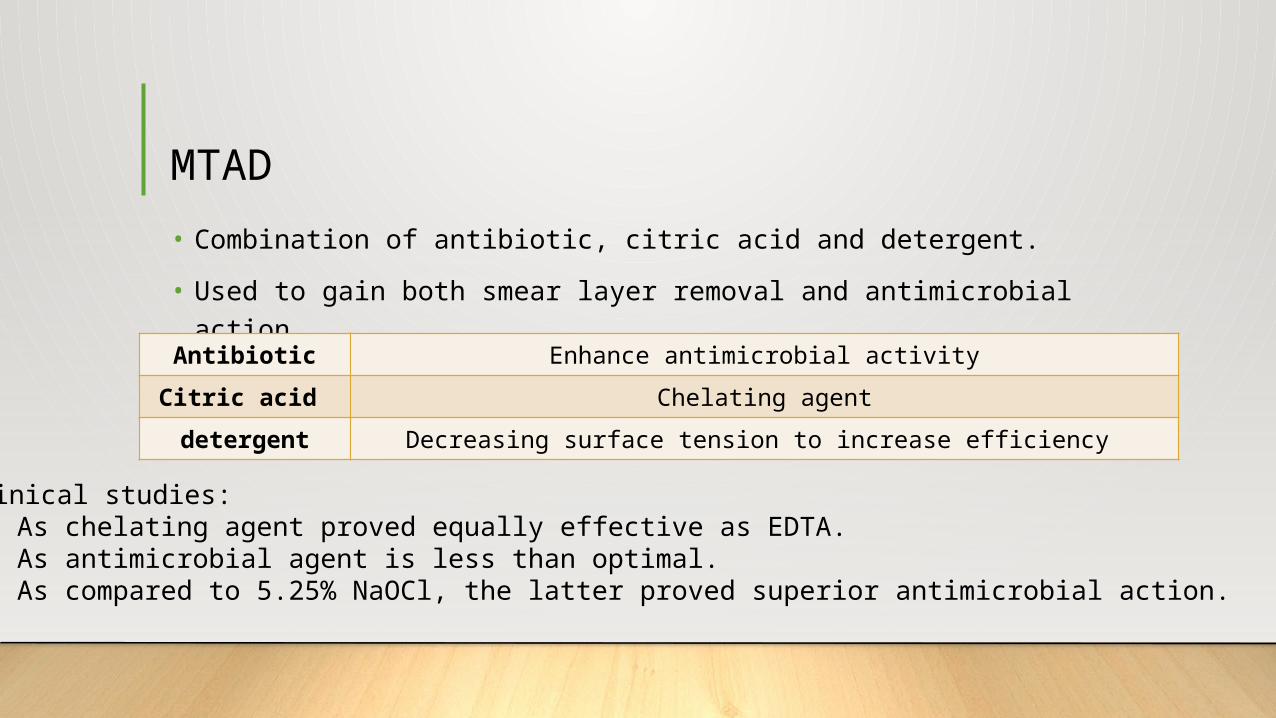
MTAD• Combination of antibiotic, citric acid and detergent.
• Used to gain both smear layer removal and antimicrobial action
Antibiotic Enhance antimicrobial activityCitric acid Chelating agentdetergent Decreasing surface tension to increase efficiency
Clinical studies:• As chelating agent proved equally effective as EDTA.• As antimicrobial agent is less than optimal.• As compared to 5.25% NaOCl, the latter proved superior antimicrobial action.
QMix
• New product introduced in 2011.
• Proved equally effective as EDTA in smear layer removal.
• As for antimicrobial activity, it proved effective. Further clinical studies from independent researchers needed in this matter.
• Lack tissue dissolution capacity, NaOCl irrigation is still required.
Concentration Range of Irrigants
• Sodium hypochlorite ( 0.25% - 5.25% )• Chlorhixidine ( 0.2% - 2% )• EDTA ( 17% )
Interaction between irrigants
• Chx + NaOCl produce change in color and formation of a precipitate. So mixing of both irrigant should be avoided. And drying the canal with paper point before final irrigation with Chx.
• Chx + EDTA produce white precipitate and cancel the chemical action of Chx. Mixing is avoided.
• NaOCl + EDTA mixing take away the tissue dissolving capacity of NaOCl. As no free Chlorine ( the active agent in sodium hypochlorite) was found in the mixture. Mixing is to be avoided.
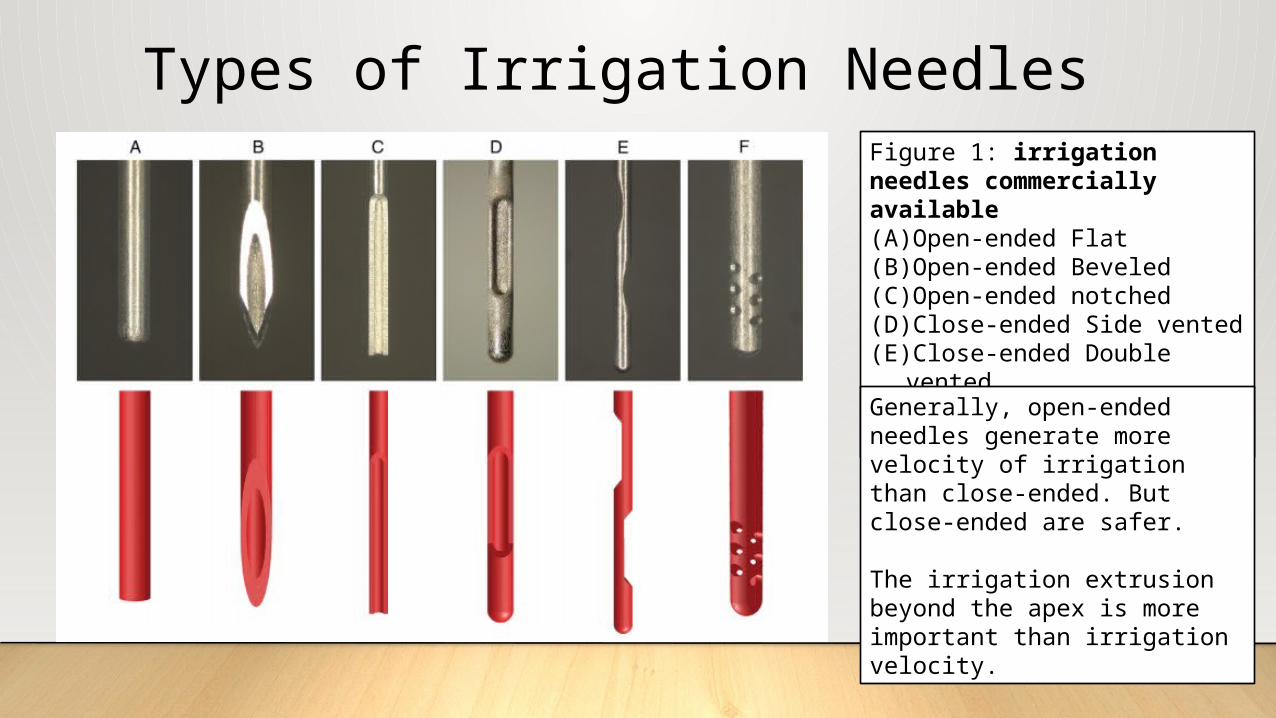
Types of Irrigation NeedlesFigure 1: irrigation needles commercially available(A)Open-ended Flat(B)Open-ended Beveled(C)Open-ended notched(D)Close-ended Side vented(E)Close-ended Double vented(F)Close-ended Multiple
ventedGenerally, open-ended needles generate more velocity of irrigation than close-ended. But close-ended are safer. The irrigation extrusion beyond the apex is more important than irrigation velocity.
Technical tips for irrigation
• The needle should placed loosely in the canal and not bent.
• Deliver the irrigant drop-by-drop and not continuous flushing, especially NaOCl.
• Use index finger to press the needle head, instead of thumb, as less force will be delivered
• The irrigant technically will not go more than 1 mm away from the needle tip.
• Do not mix irrigants.
How much time for each irrigant?
• NaOCl, still controversial, 30 minutes seems reasonable. Plus use files and irrigation synergistically
• EDTA, 1 minute is enough.
• Chlorhexidine, not reported. Use your own clinical judgment.
Does Temperature Affect Irrigant Efficiency?
Heating sodium hypochlorite increase its efficiency, but once delivered into the canal it reaches body temperature. So activation with Ultrasonic or Sonic is still superior.

Irrigation Activation / Agitation
• Root canal poses several irregularities such as isthmuses and ramifications that can not be cleaned with regular irrigation.• Moreover, studies have shown that 30% of root
canal system is not irrigated with regular irrigation.• For the above reasons, activation of irrigation is a necessity.
Different techniques of activation
•Manual agitation•Sonic and Ultrasonic activation•Negative apical pressure•Safety irrigator•Laser activation system
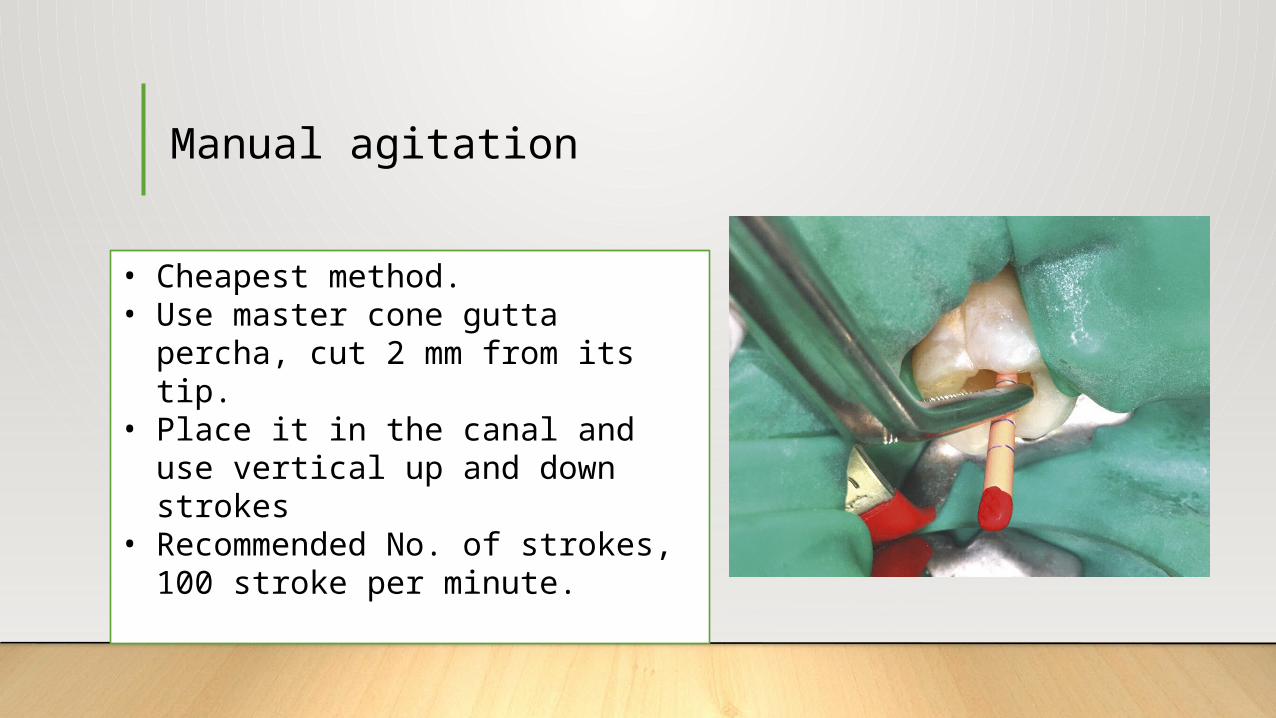
Manual agitation
• Cheapest method.• Use master cone gutta percha,
cut 2 mm from its tip.• Place it in the canal and use
vertical up and down strokes• Recommended No. of strokes,
100 stroke per minute.

Sonic activation
• Commercially know as EndoActivator ®
• Use vibrating movement 1500Hz-6000Hz / Second
• Place the tip into the canal and switched on. Simple as that.
• Less risk of perforation as compared with Ultrasonic system.
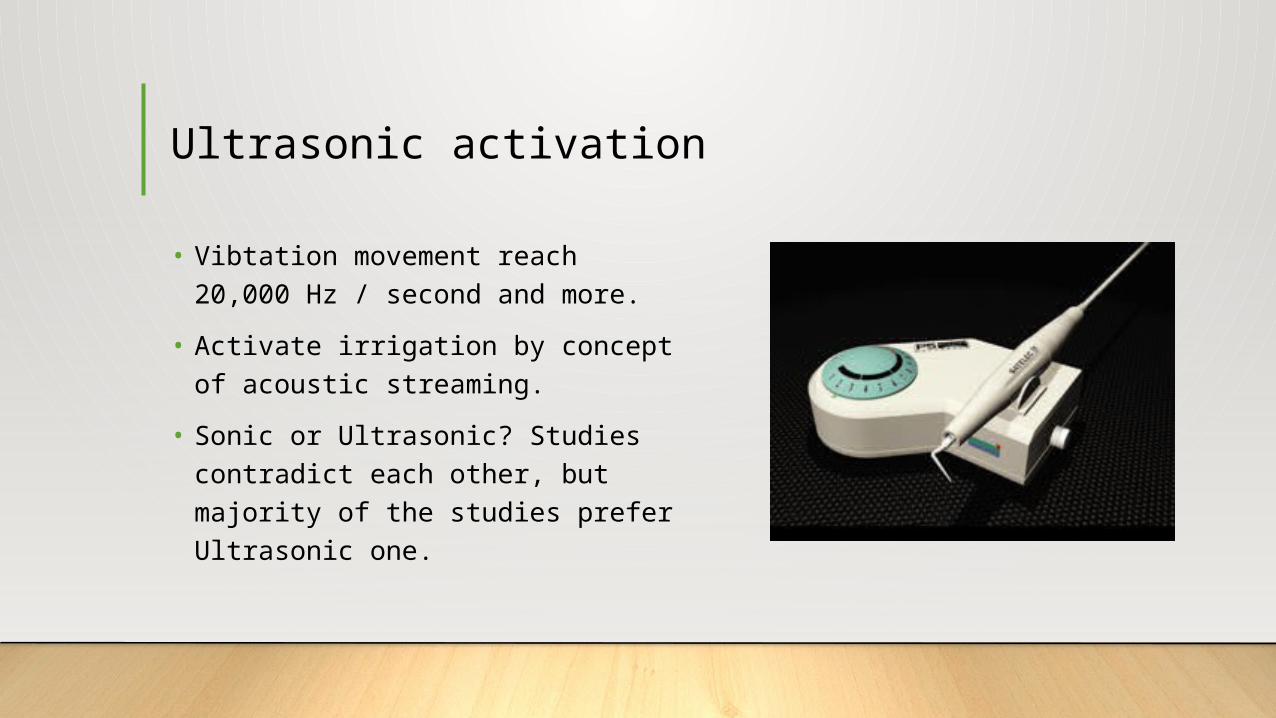
Ultrasonic activation
• Vibtation movement reach 20,000 Hz / second and more.
• Activate irrigation by concept of acoustic streaming.
• Sonic or Ultrasonic? Studies contradict each other, but majority of the studies prefer Ultrasonic one.

Negative apical pressure
• Commercially known as EndoVac ®
• The main advantage of this technique is safety. Many studies have proven that irrigation solution will not extrude to the periapical area.
Safety irrigator
Similar in functionality to EndoVac ® system

• In virto study to test the difference between activation techniques, the results were:
• All techniques were better than regular syringe irrigation without activation
• Manual irrigation is similar to negative apical pressure technique and safety irrigator.
• Ultrasonic proven to be significantly better than all of them.
Laser activation system
• New Modern technique
Several studies indicated that laser is promising for removing smear layer and dentin debris in less time than Ultrasonic
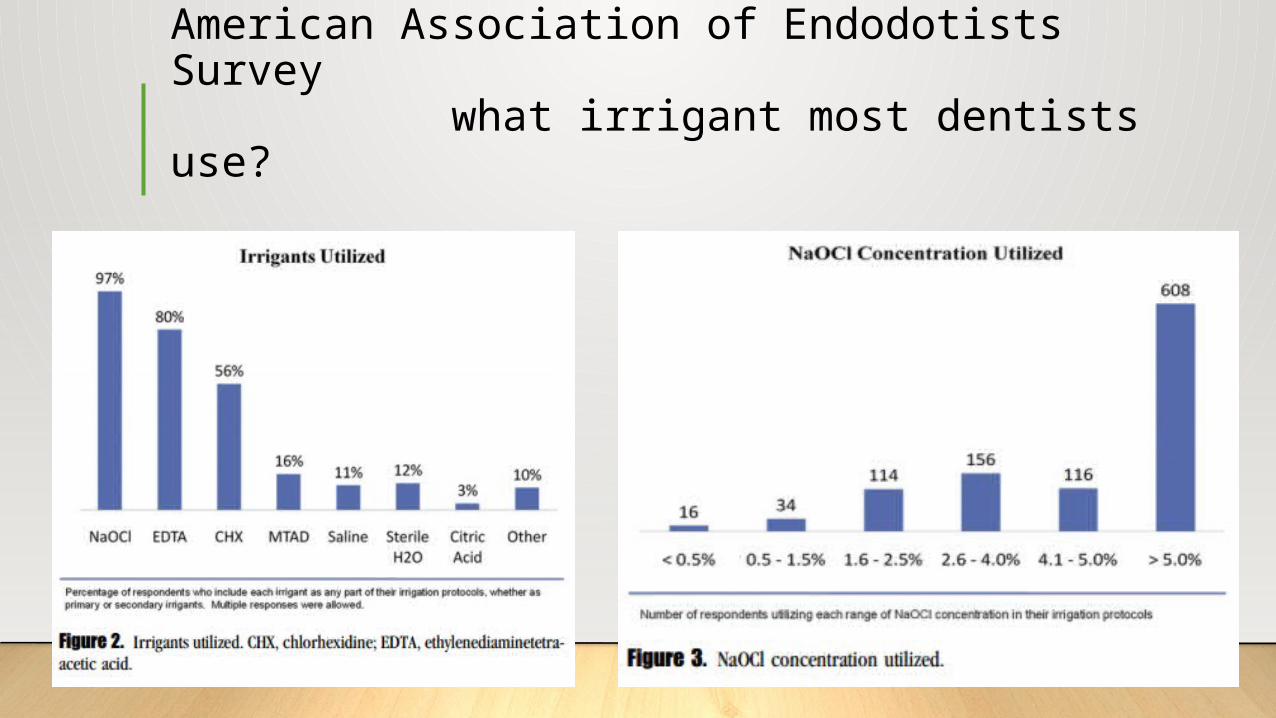
American Association of Endodotists Survey what irrigant most dentists use?
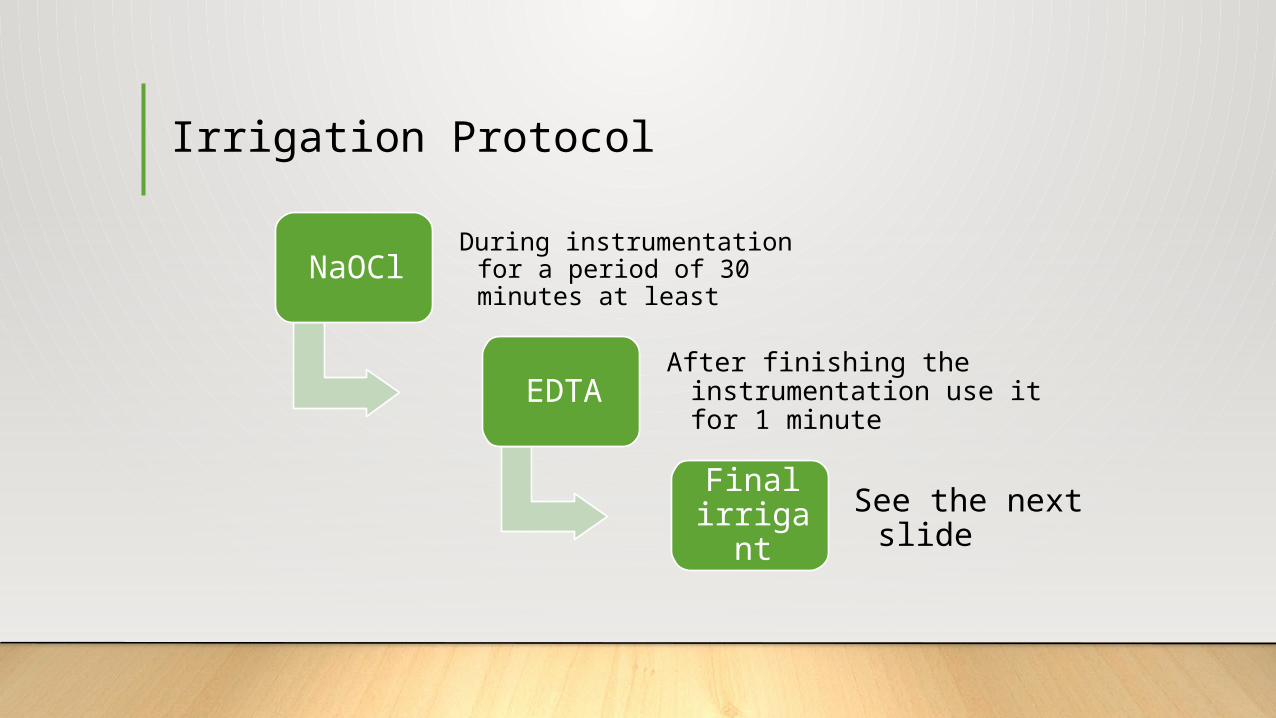
Irrigation Protocol
NaOClDuring instrumentation for a
period of 30 minutes at least
EDTAAfter finishing the
instrumentation use it for 1 minute
Final irrigan
tSee the next slide
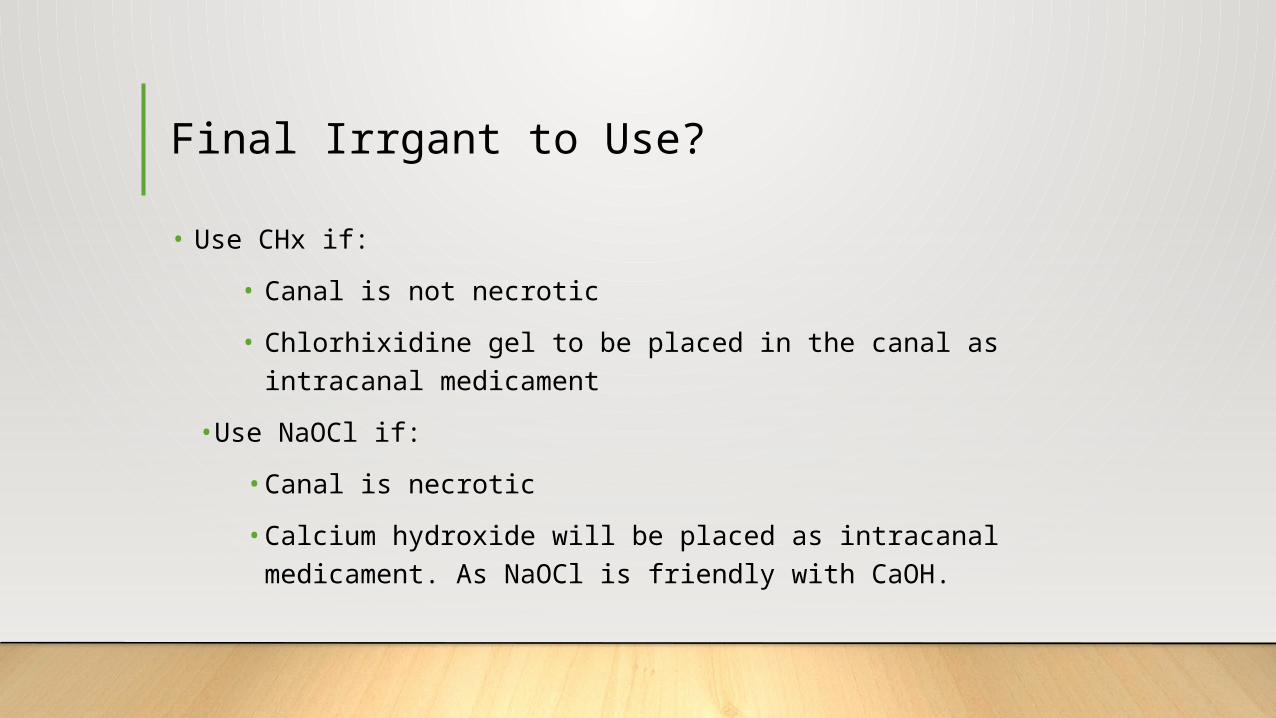
Final Irrgant to Use?
• Use CHx if:
• Canal is not necrotic
• Chlorhixidine gel to be placed in the canal as intracanal medicament
•Use NaOCl if:
• Canal is necrotic
• Calcium hydroxide will be placed as intracanal medicament. As NaOCl is friendly with CaOH.

References
• Cohen Pathways of Pulp, Chapter 6, Cleaning and Shaping of Root Canal System.
• Endodotnics: Principle and Practice. 5th edition, Chapter 16, Cleaning and Shaping.
• Matthias Zehnder, JOE, Volume 32, Number 5, 2006. Root Canal Irrigants
• JOE, Irrigation Trends among American Association of Endodontists Members: A Web-based Survey


















