Role of neoadjuvant chemotherapy in the management of advanced ovarian yolk sac tumor
6
UNCORRECTED PROOF 1 Role of neoadjuvant chemotherapy in the management of advanced 2 ovarian yolk sac tumor Yan Q1 Lu a , Jiaxin Yang a , Dongyan Cao a , Huifang Huang a , Ming Wu a , Yan You b , Jie Chen b , 4 Jinhe Lang a , Keng Shen a, ⁎ a Q2 Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, People's Republic of China b Q3 Department of Pathology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, People's Republic of China 7 8 HIGHLIGHTS 9 10 • This was the first series of applying NACT in OYST with the largest number of advanced patients. 11 • The tumor status and general condition of the patients were improved significantly after NACT. 12 • Patients treated with NACT showed less peri-operative morbidities and better optimal cytoreduction rate, which was the independent prognostic factor. 13 14 15 abstract 16 article info 17 Article history: 18 Received 23 December 2013 19 Accepted 20 February 2014 20 Available online xxxx 21 Keywords: 22 Alpha-fetoprotein 23 Endodermal sinus tumor 24 Neoadjuvant therapy 25 Prognosis 26 Objective. The aim of the study was to identify the role of neoadjuvant chemotherapy (NACT) in the treatment 27 of the patients with advanced stage ovarian yolk sac tumor (OYST). 28 Methods. The comparative study was based on 53 cases with advanced stage OYST registered at Peking Union 29 Medical College Hospital from 1995 to 2010. Twenty one cases were treated with NACT followed by interval 30 debulking surgery (IDS). Thirty two cases were treated with primary debulking surgery (PDS). Data on patient 31 characteristics, treatment and survival were analyzed and compared between two groups to assess the outcome 32 of NACT. 33 Results. After NACT, the overall status of the patients was improved significantly. Patients in NACT had better 34 optimal cytoreduction rate and less peri-operative morbidities. Seven patients (13.2%) suffered from relapse. 35 There was a significantly better PFS for patients with ovarian tumor size N 20 cm in the NACT than those 36 underwent PDS. Residual disease N 2 cm was the independent risk factor of relapse. 37 Conclusions. NACT is the better treatment option for some patients with advanced stage OYST, especially for 38 those with unresectable tumors and poor general condition. 39 © 2014 Published by Elsevier Inc. All rights reserved. 40 41 42 43 44 Introduction 45 Ovarian yolk sac tumor (OYST) is a rare malignancy that primarily 46 occurs in young women and adolescents. It accounts for 20% of 47 malignant ovarian germ cell tumor (MOGCT) representing about 1% of 48 all ovarian malignancies [1]. Before the advent of combination 49 chemotherapy, OYST was almost universally fatal. Current therapy of 50 surgery followed by post-operative cisplatin-based chemotherapy has 51 dramatically improved the prognosis [2–5]. As a highly aggressive 52 malignancy that shows early dissemination and metastasis, approxi- 53 mately 30% to 40% of OYST is International Federation of Gynecology 54 and Obstetrics (FIGO) stage III or IV [1]. Because patients with advanced 55 stage or complex ovarian tumors were transferred to our institution 56 from peripheral hospitals, more than half of our patients presented 57 with extra-pelvic disease. To our knowledge, we reported herein the 58 largest series of patients treated for advanced stage OYST. Some 59 advanced stage patients did not appear to be suitable for performing 60 optimal cytoreductive surgery at the initial presentation, which encour- 61 aged us to explore an alternative treatment. 62 It has been reported that neoadjuvant chemotherapy (NACT) prior 63 to surgery is a better alternative option in some patients with advanced 64 stage epithelial ovarian cancer (EOC) [6]. Though the benefits to survival 65 still remain controversial, studies have mostly confirmed the effect of 66 NACT to increase the feasibility of optimal cytoreduction [7–11]. The 67 post-operative rates of adverse effects and mortality tended to be less 68 after interval debulking than after primary debulking [9–11]. Though 69 widely documented in EOC, the role of NACT in MOGCT has not been 70 investigated yet. The aim of our study was to evaluate the outcome of Gynecologic Oncology xxx (2014) xxx–xxx ⁎ Corresponding author at: No.1 Shuaifuyuan, Dongcheng District, Beijing 100730, People's Republic of China. Fax: +86 10 65212507. E-mail address: [email protected] (K. Shen). YGYNO-975407; No. of pages: 6; 4C: http://dx.doi.org/10.1016/j.ygyno.2014.02.029 0090-8258/© 2014 Published by Elsevier Inc. All rights reserved. Contents lists available at ScienceDirect Gynecologic Oncology journal homepage: www.elsevier.com/locate/ygyno Please cite this article as: Lu Y, et al, Role of neoadjuvant chemotherapy in the management of advanced ovarian yolk sac tumor, Gynecol Oncol (2014), http://dx.doi.org/10.1016/j.ygyno.2014.02.029
Transcript of Role of neoadjuvant chemotherapy in the management of advanced ovarian yolk sac tumor

1
2
3Q1
4
5Q26Q37
8
9
10
11
12
1314
1 5
1 6
17181920
2122232425
39
4041
42
43
44
45
46
47
48
49
50
51
52
53
54
Gynecologic Oncology xxx (2014) xxx–xxx
YGYNO-975407; No. of pages: 6; 4C:
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r .com/ locate /ygyno
Role of neoadjuvant chemotherapy in the management of advancedovarian yolk sac tumor
PRO
OFYan Lu a, Jiaxin Yang a, Dongyan Cao a, Huifang Huang a, Ming Wu a, Yan You b, Jie Chen b,
Jinhe Lang a, Keng Shen a,⁎a Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, People's Republic of Chinab Department of Pathology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, People's Republic of China
H I G H L I G H T S
• This was the first series of applying NACT in OYST with the largest number of advanced patients.• The tumor status and general condition of the patients were improved significantly after NACT.• Patients treated with NACT showed less peri-operative morbidities and better optimal cytoreduction rate, which was the independent prognostic factor.
⁎ Corresponding author at: No.1 Shuaifuyuan, DongcPeople's Republic of China. Fax: +86 10 65212507.
E-mail address: [email protected] (K. Shen).
http://dx.doi.org/10.1016/j.ygyno.2014.02.0290090-8258/© 2014 Published by Elsevier Inc. All rights re
Please cite this article as: Lu Y, et al, Role of n(2014), http://dx.doi.org/10.1016/j.ygyno.20
Da b s t r a c t
a r t i c l e i n f o26
Article history:27
28
29
30
31
32
33
34
ECTEReceived 23 December 2013Accepted 20 February 2014Available online xxxx
Keywords:Alpha-fetoproteinEndodermal sinus tumorNeoadjuvant therapyPrognosis
Objective.The aimof the studywas to identify the role of neoadjuvant chemotherapy (NACT) in the treatmentof the patients with advanced stage ovarian yolk sac tumor (OYST).
Methods. The comparative studywas based on 53 caseswith advanced stage OYST registered at Peking UnionMedical College Hospital from 1995 to 2010. Twenty one cases were treated with NACT followed by intervaldebulking surgery (IDS). Thirty two cases were treated with primary debulking surgery (PDS). Data on patientcharacteristics, treatment and survival were analyzed and compared between two groups to assess the outcomeof NACT.
Results. After NACT, the overall status of the patients was improved significantly. Patients in NACT had betteroptimal cytoreduction rate and less peri-operative morbidities. Seven patients (13.2%) suffered from relapse.
35
36
37
38
RThere was a significantly better PFS for patients with ovarian tumor size N20 cm in the NACT than thoseunderwent PDS. Residual disease N2 cm was the independent risk factor of relapse.
Conclusions. NACT is the better treatment option for some patients with advanced stage OYST, especially forthose with unresectable tumors and poor general condition.
© 2014 Published by Elsevier Inc. All rights reserved.
R55
56
57
58
59
60
61
62
63
64
65
66
UNCO
Introduction
Ovarian yolk sac tumor (OYST) is a rare malignancy that primarilyoccurs in young women and adolescents. It accounts for 20% ofmalignant ovarian germ cell tumor (MOGCT) representing about 1% ofall ovarian malignancies [1]. Before the advent of combinationchemotherapy, OYST was almost universally fatal. Current therapy ofsurgery followed by post-operative cisplatin-based chemotherapy hasdramatically improved the prognosis [2–5]. As a highly aggressivemalignancy that shows early dissemination and metastasis, approxi-mately 30% to 40% of OYST is International Federation of Gynecologyand Obstetrics (FIGO) stage III or IV [1]. Because patients with advanced
67
68
69
70
heng District, Beijing 100730,
served.
eoadjuvant chemotherapy in14.02.029
stage or complex ovarian tumors were transferred to our institutionfrom peripheral hospitals, more than half of our patients presentedwith extra-pelvic disease. To our knowledge, we reported herein thelargest series of patients treated for advanced stage OYST. Someadvanced stage patients did not appear to be suitable for performingoptimal cytoreductive surgery at the initial presentation, which encour-aged us to explore an alternative treatment.
It has been reported that neoadjuvant chemotherapy (NACT) priorto surgery is a better alternative option in some patients with advancedstage epithelial ovarian cancer (EOC) [6]. Though thebenefits to survivalstill remain controversial, studies have mostly confirmed the effect ofNACT to increase the feasibility of optimal cytoreduction [7–11]. Thepost-operative rates of adverse effects and mortality tended to be lessafter interval debulking than after primary debulking [9–11]. Thoughwidely documented in EOC, the role of NACT in MOGCT has not beeninvestigated yet. The aim of our study was to evaluate the outcome of
the management of advanced ovarian yolk sac tumor, Gynecol Oncol

T
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
t1:1Table 1t1:2Comparison of patients profile between the NACT and PDS groups.
Variables NACT (N = 21) PDS (N = 32) P value t1:3
Mean age (years) 23 25 0.313 t1:4
Ovarian tumor size t1:5
N20 cm 16 (76%) 4 (12%) b0.001 t1:6
≤20 cm 5 (24%) 28 (88%) t1:7
AFP level t1:8
N3.5 × 104 ng/mL 10 (48%) 4 (12%) 0.005 t1:9
≤3.5 × 104 ng/mL 11 (52%) 28 (88%) t1:10
Pleural effusion t1:11
Present 9 (43%) 9 (28%) 0.268 t1:12
Absent 12 (57%) 23 (72%) t1:13
Ascites t1:14
N100 mL 20 (95%) 24 (75%) 0.071 t1:15
≤100 mL 1 (5%) 8 (25%) t1:16
Histology t1:17
Pure OYST 14 (67%) 23 (72%) 0.686 t1:18
Mixed OYST 7 (33%) 9 (28%) t1:19
Stage t1:20
III 13 (62%) 27 (84%) 0.063 t1:21
IV 8 (38%) 5 (16%) t1:22
2 Y. Lu et al. / Gynecologic Oncology xxx (2014) xxx–xxx
UNCO
RREC
NACT and to identify the role of NACT in the treatment of the patientswith advanced stage OYST.
Materials and methods
Patient population
In total, 127 consecutive cases of OYST registered at Peking UnionMedical College Hospital from 1995 to 2010. Eighty cases (63%) wereclassified to have stage III or IV diseases according to the FIGO stagingsystem. Among them, 53 patients who had both debulking surgeryand chemotherapy with intact records at our institution were eligiblefor this comparative study. Twenty one patients had NACT followedby interval debulking surgery (IDS) and adjuvant chemotherapy. Thirtytwo patients underwent primary debulking surgery (PDS) followed byadjuvant chemotherapy. The information of patient's age, clinicalmanifestation, imaging finding, tumor marker, histology, treatmentmodality, outcome of the treatment and results of follow-up werecollected from the medical records and clinical database.
Diagnosis
Physical examination, detection of serum alpha-fetoprotein (AFP)and computerized tomography (CT) scans of chest, abdomen and pelviswere performed before and after treatment to evaluate the tumorstatus. Of the 21 patients in the NACT group, eleven were clinicallydiagnosed as OYST owing to the distinctive characteristics of youngage, large ovarian mass, massive ascites and extraordinarily elevatedAFP with the exclusion of pregnancy, liver disease and other factors.The diagnosis was confirmed by the post-operative pathology in all ofthese 11 cases. The other 10 patients of the NACT group had undergonelaparotomic or laparoscopic biopsy and the pathology revealed OYST.The patients of the PDS group were diagnosed by surgical pathology.The histology was confirmed by at least two pathologists based on thedistinctive Schiller–Duval bodies and immunohistochemical stain forAFP.
Treatment protocol
Cisplatin-based combination chemotherapy was the standardtreatment for NACT. The inclusion criteria of NACT candidates were asfollows:(1) extensive metastasis on the surface of intra-abdominaland pelvic organ, (2) massive malignant ascites, (3) fixed big tumorspredicting the patients to have surgically non-resectable disease; and(4) patients with severe medical co-morbidities or poor general condi-tion leading to their inability to tolerate the debulking surgery in a shortterm. Patients received 1–3 cycles of NACT depending on the responseand tolerance. IDS was performed when patients responded well toNACT. The evaluation criteria of good response toNACTwere as follows:(1) relieving of the abdominal distension due to the reduction of theascites, (2) favorable AFP decline on a common logarithmic scale,(3) a 50% ormore decrease in ovarian tumor size, and (4) improvementof general status to tolerate the debulking surgery.
In patients who desired fertility preservation, unilateral salpingo-oophorectomy was performed. In patients not requiring fertilitypreservation, total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed. Peritoneal cytological study, resectionof macroscopic lesions, omentectomy, and dissection or sampling ofthe retroperitoneal lymph nodes were performed regardless of preserv-ing fertility or not.
After debulking surgery, standard combination chemotherapy wasadministrated as adjuvant therapy. After AFP dropped to the levelwithin the normal range (b20 ng/mL at our institution), 2 additionalcycles of chemotherapy were given to consolidate the remission.All the patients received standard combination chemotherapy ofPEB (cisplatin/etoposide/bleomycin) or PVB (cisplatin/vinblastine/
Please cite this article as: Lu Y, et al, Role of neoadjuvant chemotherapy in(2014), http://dx.doi.org/10.1016/j.ygyno.2014.02.029
bleomycin) regimen. PEV regimen (cisplatin/etoposide/vincristine)was used after the total bleomycin dosage accumulated to 250 mg/m2
(according to the regulation of State Food and Drug Administration ofChina). Standard chemotherapy was considered to be the effectivePEB/PVB regimen with full dose, adequate cycles and strict adherence.The administration of the chemotherapy regimen was described in S1of the Supplementary materials.
OO
F
Evaluation of treatment
Optimal cytoreduction was considered to be achieved when thelargest residual tumor was ≤2 cm. The definition of none residualdisease was no macroscopic residual disease left at the completion ofcytoreduction. Serum AFP was closely monitored after surgery andeach cycle of chemotherapy, and chemotherapy was consideredsatisfactory when AFP declined on a common logarithmic scale. ChestX ray and ultrasonography of abdomen and pelvis after each cycle ofchemotherapy and CT scans after the whole therapy were obtained toevaluate the tumor response. A complete remission (CR) was definedas the disappearance of all clinical, radiographic, and biochemicalevidence of disease.
D P
R
Follow-up
Patient follow-up included clinical examination, blood markermeasurements and imaging at least every month during the first yearfollowing treatment and at gradually increasing intervals thereafter.Recurrence was defined as the return of disease after CR was achieved.
E
Statistical analysis
Progression free survival (PFS) was calculated from the date of thediagnosis to the date of the first event, defined as a relapse or death.Kaplan–Meier survivalwas applied in theunivariate analysis to evaluatethe prognostic factors for PFS. A multivariate Cox proportional hazardregression model was constructed to determine the independent prog-nostic factors. Only factors that were significant in the univariate analy-sis were subsequently incorporated into themultivariatemodel. P valuebelow 0.05 was considered statistically significant.
the management of advanced ovarian yolk sac tumor, Gynecol Oncol

T
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
t2:1
t2:2
t2:3
t2:4
t2:5
t2:6
t2:7
3Y. Lu et al. / Gynecologic Oncology xxx (2014) xxx–xxx
UNCO
RREC
Results
Patient characteristics
Table 1 compares the patient profile between the NACT and PDSgroups. Themeanovarian tumor size in theNACT groupwas significant-ly larger than that in the PDS group (20.7 ± 5.7 vs. 16.7 ± 4.7 cm, P =0.009). The median serum AFP level was significantly higher in theNACT than that in the PDS group (3.6 × 104 vs. 2.2 × 104 ng/mL, P =0.044). There were more patients in the NACT group who presentedwith extra-abdominal disease consistent with stage IV disease thanthat in the PDS group, but the difference was not significant (38% vs.16%).
Results of NACT
Fifteen patients (71%) experienced three cycles of NACT, 5 patients(24%) experienced two cycles and 1 patient (5%) experienced onecycle. The mean number of NACT cycles was 2.7 ± 0.6. The mean num-ber of total chemotherapy cycles in theNACT and PDS groupswas 5.8±0.9 and 6.1 ± 1.2, respectively. The mean number of chemotherapy cy-cles for serum AFP to decline to the normal range in the NACT and PDSgroups was 3.7 ± 0.7 and 3.8 ± 1.0, respectively. No significant differ-ences were observed between the two groups.
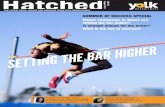
Table 2 compared the tumor status before and after NACT accordingto the evaluation criteria of response. The mean ovarian tumor sizedecreased significantly after NACT (20.7 ± 5.7 vs. 17.0 ± 3.3 cm, P =0.016) and the mean shrinkage was 15.3%. In the 15 patients thatexperienced three cycles of NACT, the mean tumor size at the initialpresentation and after each cycle was 22.7 ± 5.2, 19.1 ± 3.4, 18.4 ±3.1 and 18.2 ± 3.0 cm, respectively. The shrinkage between each cycletended to be less and less (15% vs. 3.3% vs. 1.0%). The median serumAFP level declined significantly after NACT (3.3 × 104 vs. 6.6 × 102 ng/mL, P b 0.001). The number of chemotherapy cycles for AFP to decreasemore than 101 was one in 7 patients, two in 12 patients and three in 2patients. When NACT was completed, the chest X ray showed thatpleural effusion disappeared in 6 patients and deceased to variabledegree in the remaining 3. IDS found that 15 (71%) patients had ascites≤100 mL. The change of pleural effusion and ascites in patients treatedwith NACT was shown in Fig. 1.
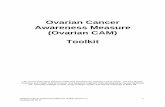
As shown in Fig. 2, the surgical pathology revealed OYST andmetas-tasis in 12 (57%) patients (Figs. 2A and B), degenerated residual tumorconsistent with post-chemotherapy alterations in 6 (29%) patients(Fig. 2C), and only necrosis or chronic inflammation without tumorsigns in 3 (14%) patients (Fig. 2D).
Results of surgery
The overall rate of optimal cytoreduction with residual disease ≤2cm was 89%. The difference was of no significance between the NACTand PDS groups (95% vs. 84%, P= 0.384). However, the rate of patientswith nonresidual disease was 81% in the NACT group, whichwas signif-icantly higher than that in the PDS group (44%, P = 0.007).
Peri-operative parameters and post-operative complications be-tween the NACT and PDS groupswere compared in Table 3. Themedianamount of surgical blood loss in the NACT group was significantly lessthan that in the PDS group (200 vs. 450 mL, P = 0.018). The PDS
266
267
268
269
270
271
272
273
Table 2Tumor status before and after NACT (N = 21).
Variables Before NACT After NACT P value
Mean ovarian tumor size (cm) 20.7 ± 5.7 17.0 ± 3.3 0.016Median AFP level (ng/mL) 3.3 × 104 6.6 × 102 b0.001Presence of pleural effusion — n (%) 9 (43) 3 (14) 0.040Ascites N100 mL — n (%) 20 (95) 6 (29) b0.001
Please cite this article as: Lu Y, et al, Role of neoadjuvant chemotherapy in(2014), http://dx.doi.org/10.1016/j.ygyno.2014.02.029
ED P
RO
OF
group had more transfusion rate, longer median operation time andprolonged mean hospital course, but the differences were not signifi-cant. The rates of post-operative complications were of no significancebetween the two groups.
Results of long term follow-up
The median follow-up was 46 months (range: 6–189 months).Recurrence was observed in seven patients (13.2%). The median timeto recurrence was 10 months (range: 3–18 months). There was no sig-nificant difference of recurrence rate between theNACT and PDS groups(14.3% vs. 12.5%). The median PFS time could not be calculated becauseit had not yet been reached. Two patients died of the recurrent diseaseduring the period of follow-up. One was in the NACT group and theother was in the PDS group. The difference was of no significance(4.7% vs. 3.1%). Details of the recurrent cases were described in S2 ofthe Supplementary materials.
It was noted that ovarian tumor size and serum AFP level were sig-nificantly higher in the NACT group than that in the PDS group. Asshown in Fig. 3, there was a significantly better PFS for patients withovarian tumor size N20 cm in the NACT group than that in the PDSgroup (P = 0.016). No difference in PFS was found for patients withAFP N3.5 × 104 ng/mL between the NACT and PDS groups (P= 0.165).
Prognostic factors
Kaplan–Meier univariate analysis was performed with PFS as theend point, and included the following variables: treatment group, initialovarian tumor size, initial serum AFP level, FIGO stage, pleural effusion,ascites, histologic type, residual tumor and operation type (classified byfertility sparing or radical surgery). Tumor size N20 cm, AFP N3.5×104 ng/mL, FIGO stage IV and residual diseaseN2 cmwere the risk fac-tors of relapse (S3 in the Supplemental materials). However, NACT didnot significantly influence the PFS (P= 0.838). The further Cox propor-tional hazard regression model proved that residual disease N2 cmwasthe only independent risk factor for prognosis (P = 0.017) (S4 in theSupplemental materials).
Discussion
The results of the present study demonstrated that the tumor statusand general condition of the patients were improved significantly afterNACT. Patients treatedwithNACT followed by IDS shown better optimalcytoreduction rate, less peri-operativemorbidities and similar PFS com-pared with those underwent PDS. And the optimal cytoreduction ratewas proved to be the independent prognostic factor by the survivalanalysis.
Before the initiation of NACT, the diagnosis of OYST should be madefirstly by either pathology or clinical manifestation. Although pathologywas the golden standard, diagnosis could also be made clinically. In ourseries, the diagnosis prior to surgery in 11 patients of the NACT groupwas mainly dependent on the clinical features, radiology examinationand extraordinarily elevated serum AFP level. AFP plays key role in thedifferential diagnosis. Immature teratoma, embryonal carcinoma andpolyembryoma also produce AFP, but the level is much lower thanYST [12]. Talerman et al. [13] reported that patients with tumors com-posed of or containing YST elements had serum AFP levels measuredin 100s or 1000s of ng/mL, whereas slightly elevated AFP up to 60 ng/mL was noted in a few patients with pure embryonal carcinoma.Kawai et al. [14] reported that in 46 cases with MOGCT, AFP wasabove 1000 ng/mL in 23 of 25 cases with pure or mixed OYST (92%),while only in 1 of 17 cases with immature teratoma (6%). Elevation ofAFP level above 1000 ng/ml strongly suggested the presence of YST. Inrare cases, especially in children and menopausal and postmenopausalwomen, AFP might exceed 1000 ng/mL in other types of MOGCT[15–17]. However, in our series, the post-operative pathology
the management of advanced ovarian yolk sac tumor, Gynecol Oncol

TED P
RO
OF
274
275
276
277
278
279
280
281
282
283
Fig. 1. CT scans of pleural effusion and ascites in patients treatedwith NACT. (A) Pleural effusion at the initial presentation. (B) Pleural effusion disappeared after NACT. (C)Massive ascitesat the initial presentation. (D) Ascites diminished after NACT.
4 Y. Lu et al. / Gynecologic Oncology xxx (2014) xxx–xxx
C
confirmed the OYST in all of those 11 cases. The pre-operative histologyof OYST was usually acquired by biopsy. Petrakakou et al. [18] reportedthat paracentesis of ascitic fluid in the diagnosis of OYST was still chal-lenging and required the correlation of cytology with the remainingclinical and laboratory data.
UNCO
RRE
Fig. 2. Surgical pathology images of patients treated with NACT. (A) Yolk sac tumor with SchillThe yolk sac component is positive (AFP, ×100). (C) Scattered yolk sac tumor residual consistemation without tumor signs (H and E, ×100).
Please cite this article as: Lu Y, et al, Role of neoadjuvant chemotherapy in(2014), http://dx.doi.org/10.1016/j.ygyno.2014.02.029
Patientswith advanced stageOYSTusually have bulky tumor burdenand massive ascites with or without pleural effusion, whose generalcondition is too poor to tolerate PDS. Those featureswere exactly the se-lection criteria the present studymade for NACT candidates. The surviv-al analysis proved that in the subgroup of patients with ovarian tumor
er–Duval body (H and E, ×200). (B) Immunohistochemical staining for alpha-fetoprotein.nt with post-chemotherapy alterations (H and E, ×200). (D) Necrosis and chronic inflam-
the management of advanced ovarian yolk sac tumor, Gynecol Oncol

T
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347348349Q4350351352353354355356357358359360361362
t3:1 Table 3t3:2 Peri-operative parameters and post-operative complications between the NACT and PDSt3:3 groups.
Parameter NACT (N = 21) PDS (N = 32) P valuet3:4
Blood loss (mL) 200 450 0.018t3:5
Transfusion needed — n (%) 3 (14) 8 (25) 0.494t3:6
Transfusion (unit) 3.3 ± 1.1 3.2 ± 1.0 0.910t3:7
Operation time (min) 120 130 0.121t3:8
Hospital stay (days) 11 ± 1.9 13 ± 2.7 0.062t3:9
Post-operative complications— n (%)t3:10
Bowel obstruction 1 (4.8) 5 (16) 0.384t3:11
Urinary tract infection 3 (14) 3 (9.4) 0.671t3:12
Lung infection 0 1 (3.1) 1.000t3:13
Wound infection 2 (9.5) 1 (3.1) 0.555t3:14
Thromboembolism 1 (4.8) 0 0.396t3:15
Total 7 (33) 10 (31) 0.874t3:16
5Y. Lu et al. / Gynecologic Oncology xxx (2014) xxx–xxx
ORREC
size N20 cm, the PFS in the patients treated with NACT followed by IDSwas significantly better than that in the patients treated with PDS. Thisfinding suggested that advanced stage OYST with ovarian tumor sizeN20 cm was recommended to be selected as the inclusion criteria forNACT.
The effects of NACT with PEB or PVB combination chemotherapywere favorable. The tumor size and serum AFP level decreased signifi-cantly. The ascites and pleural effusion were controlled very well. In 3patients, IDS pathology did not even find the signs of tumor left. The op-timal effects of NACT were prospected to be the improvements of pa-tient general status to tolerate the debulking surgery and to achievethe optimal cytoreduction. The optimal number of NACT cycleswas rec-ommended to be nomore than three. This recommendation was basedon two reasons. Firstly, three cycles were enough for the patients toachieve the optimal effects of NACT. Secondly, it was estimated thatthe volume of remaining tumor and necrosis tissue would no longershrink with NACT more than three cycles. Because in the 15 patientstreated with three cycles of NACT, the tumor size tended to decreaseless and less between each cycle (15% vs. 3.3% vs. 1.0%). The shrinkagebetween the second and third cycle was of no significant difference(P = 0.189). At this step of treatment, IDS, rather than furtherNACT, should be performed to resect the remaining lesions. Moreover,NACT did not increase the number of overall chemotherapy cycles,thus the drug toxicity would not be aggravated.
NACT followed by IDS was associated with better optimal rate, butthe difference was not significant compared with PDS, likely due tothe limited population. However, the improvement of NACT to therate of nonresidual disease was significant. The peri-operative morbid-ities seemed better in the NACT group than that in the PDS group, butnot significant in all parameters. And the post-operative complicationswere similar between the two groups. Since the overall status of
UNC 363
364365366367368369370371372373374375376377378379380381382383384385386387
Fig. 3. Kaplan–Meier curves of progression free survival in patients with ovarian tumorsize N20 cm. Gray line: NACT group. Black line: PDS group.
Please cite this article as: Lu Y, et al, Role of neoadjuvant chemotherapy in(2014), http://dx.doi.org/10.1016/j.ygyno.2014.02.029
ED P
RO
OF
patients in NACT seemed to beworse than that in the PDS, no significantdifference might actually reflect the improvements due to NACT.
Due to the rarity of OYST, identifying prognostic factors has beenquite challenging. It has been a consensus that standard PEB regimenis the most decisive prognostic factor [3,19]. Most reports suggestedthat the absence of bulky residual disease was a good prognostic factorfor OYST [20–25]. Tong et al. [23] reported that in 76 cases of OYST,patients with residual tumors ≤2 cm showed a significantly better5-year survival than those with residual tumors N2 cm (66.7% vs.7.9%, P b 0.0001), but there was no difference between patients withnone residual tumor and residual tumor ≤2 cm (71.2% vs. 66.7%,P N 0.05). The results were similar to ours. The survival analysis failedto prove that NACT had a significant impact on PFS. However, thepatients in the NACT group had better optimal cytoreduction rate.Therefore, it was estimated that NACT might improve the prognosisby increasing the optimal cytoreduction rate.
The limitations of our study include the non-randomized nature andthe small size of population. Prior to surgery, specific selection criteriafor NACT candidates and optimal number of chemotherapy cycles stillneed to be validated.
With the development of value-basedmedicine in gynecological on-cology, individualization treatment will be emphasized more and morein clinical decision making. The results of the present study proved thefact that NACT followed by IDS might be an alternative option for pa-tients with advanced stage OYST, especially for those with surgicallynon-resectable tumors and those with poor general condition leadingto their inability to tolerate the primary debulking surgery.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ygyno.2014.02.029.
Conflict of interest statement
The authors have declared no conflicts of interest.
References
[1] Dallenbach P, Bonnefoi H, Pelte MF, Vlastos G. Yolk sac tumours of the ovary: an up-date. Eur J Surg Oncol 2006;32:1063–75.
[2] Williams S, Blessing JA, Liao SY, et al. Adjuvant therapy of ovarian germ cell tumorswith cisplatin, etoposide, and bleomycin: a trial of the Gynecologic Oncology Group.J Clin Oncol 1994;12:701–6.
[3] Gershenson DM. Management of ovarian germ cell tumors. J Clin Oncol2007;25:2938–43.
[4] Kang H, Kim TJ, KimWY, et al. Outcome and reproductive function after cumulativehigh-dose combination chemotherapy with bleomycin, etoposide and cisplatin(BEP) for patients with ovarian endodermal sinus tumor. Gynecol Oncol2008;111:106–10.
[5] de La Motte Rouge T, Pautier P, Rey A, et al. Prognostic factors in women treated forovarian yolk sac tumour: a retrospective analysis of 84 cases. Eur J Cancer2011;47:175–82.
[6] Vergote I, Trope CG, Amant F, et al. Neoadjuvant chemotherapy is the better treat-ment option in some patients with stage IIIc to IV ovarian cancer. J Clin Oncol2011;29:4076–8.
[7] Kuhn W, Rutke S, Spathe K, et al. Neoadjuvant chemotherapy followed by tumordebulking prolongs survival for patients with poor prognosis in International Feder-ation of Gynecology and Obstetrics Stage IIIC ovarian carcinoma. Cancer2001;92:2585–91.
[8] Loizzi V, Cormio G, Resta L, et al. Neoadjuvant chemotherapy in advanced ovariancancer: a case–control study. Int J Gynecol Cancer 2005;15:217–23.
[9] Lee SJ, Kim BG, Lee JW, et al. Preliminary results of neoadjuvant chemotherapy withpaclitaxel and cisplatin in patients with advanced epithelial ovarian cancer who areinadequate for optimum primary surgery. J Obstet Gynaecol Res 2006;32:99–106.
[10] Hou JY, Kelly MG, Yu H, et al. Neoadjuvant chemotherapy lessens surgical morbidityin advanced ovarian cancer and leads to improved survival in stage IV disease.Gynecol Oncol 2007;105:211–7.
[11] Vergote I, Trope CG, Amant F, et al. Neoadjuvant chemotherapy or primary surgeryin stage IIIC or IV ovarian cancer. N Engl J Med 2010;363:943–53.
[12] Aggarwal P, Kehoe S. Serum tumour markers in gynaecological cancers. Maturitas2010;67:46–53.
[13] Talerman A, Haije WG, Baggerman L. Serum alphafetoprotein (AFP) in patients withgerm cell tumors of the gonads and extragonadal sites: correlation between endo-dermal sinus (yolk sac) tumor and raised serum AFP. Cancer 1980;46:380–5.
[14] Kawai M, Furuhashi Y, Kano T, et al. Alpha-fetoprotein in malignant germ cell tu-mors of the ovary. Gynecol Oncol 1990;39:160–6.
[15] Nakakuma K, Tashiro S, Uemura K, Takayama K. Alpha-fetoprotein and human cho-rionic gonadotropin in embryonal carcinoma of the ovary. An 8-year survival case.Cancer 1983;52:1470–2.
the management of advanced ovarian yolk sac tumor, Gynecol Oncol

388389390391392393394395396397398399400
401402403404405406407408409410411412
413
6 Y. Lu et al. / Gynecologic Oncology xxx (2014) xxx–xxx
[16] Takemori M, Nishimura R, Yamasaki M, et al. Ovarian mixed germ cell tumor com-posed of polyembryoma and immature teratoma. Gynecol Oncol 1998;69:260–3.
[17] Mann JR, Raafat F, Robinson K, et al. The United Kingdom Children's Cancer StudyGroup's second germ cell tumor study: carboplatin, etoposide, and bleomycin are ef-fective treatment for children with malignant extracranial germ cell tumors, withacceptable toxicity. J Clin Oncol 2000;18:3809–18.
[18] Petrakakou E, Grapsa D, Stergiou ME, et al. Ascitic fluid cytology of yolk sac tumor ofthe ovary: a case report. Acta Cytol 2009;53:701–3.
[19] de La Motte Rouge T, Pautier P, Duvillard P, et al. Survival and reproductive functionof 52women treatedwith surgery and bleomycin, etoposide, cisplatin (BEP) chemo-therapy for ovarian yolk sac tumor. Ann Oncol 2008;19:1435–41.
[20] Kawai M, Kano T, Furuhashi Y, et al. Prognostic factors in yolk sac tumors of theovary. A clinicopathologic analysis of 29 cases. Cancer 1991;67:184–92.
UNCO
RRECT
Please cite this article as: Lu Y, et al, Role of neoadjuvant chemotherapy in(2014), http://dx.doi.org/10.1016/j.ygyno.2014.02.029
[21] Nawa A, Obata N, Kikkawa F, et al. Prognostic factors of patients with yolk sac tu-mors of the ovary. Am J Obstet Gynecol 2001;184:1182–8.
[22] Umezu T, Kajiyama H, Terauchi M, et al. Long-term outcome and prognostic factorsfor yolk sac tumor of the ovary. Nagoya J Med Sci 2008;70:29–34.
[23] Tong X, You Q, Li L, et al. Prognostic factors of patients with ovarian yolk sac tumors:a study in Chinese patients. Onkologie 2008;31:679–84.
[24] Cicin I, Saip P, Guney N, et al. Yolk sac tumours of the ovary: evaluation of clinico-pathological features and prognostic factors. Eur J Obstet Gynecol Reprod Biol2009;146:210–4.
[25] Lee CW, SongMJ, Park ST, et al. Residual tumor after the salvage surgery is themajorrisk factors for primary treatment failure in malignant ovarian germ cell tumors: aretrospective study of single institution. World J Surg Oncol 2011;9:123.
ED P
RO
OF
the management of advanced ovarian yolk sac tumor, Gynecol Oncol