ROLE OF FDG-PET/CT STUDY IN THE DETECTION OF BONE MARROW DISEASE IN PATIENTS WITH AGGRESSIVE...
1
ROLE OF FDG-PET/CT STUDY IN THE DETECTION OF BONE MARROW DISEASE IN PATIENTS WITH AGGRESSIVE NON- HODGKIN LYMPHOMA (NHL) AND HODGKIN LYMPHOMA (HL) Figure 1. PET scan transaxial view in a patient with negative BMb upstaged by FDG-PET a) FDG-PET uptake at the sacral level confirmed to be pathological at MRI b) The same patient after chemotherapy Figure 2. a) Patient negative at BMb with a solitary bone marrow disease localizations at PET b) Patient negative at BMb with polyostotic bone marrow disease at PET. PET/CT BMb + BMb - To t SOLITARY LOCALIZATION Single focality 2 6 2 (FP) 10 POLYOSTOTIC DISEASE Multiple focalities 10 9 19 Tot 12 17 29 Table 2. Bone disease patterns at FDG-PET/CT and BMb results. BACKGROUND OBJECTIVE METHODS RESULTS CONCLUSIONS E. Pelosi 1-3 , D. Deandreis 1 , D. Penna 1 , A. Chiappella 2 , P. Pregno 2 , M. Racca 1 , F. Carra' 1 , A. Douroukas 3 , U. Vitolo 2 , G. Bisi 1 . 1) SCDU Medicina Nucleare, ASO S. Giovanni Battista, Torino, Italy 2) SCDO Ematologia, ASO S. Giovanni Battista, Torino, Italy 3) Centro PET IRMET, Torino, Italy PET + PET - BMb + 12 12 24 BMb - 15 + 2 FP 78 95 29 90 119 Table 1. Accordance/Discordance between PET e BMb in the evaluation of bone marrow disease. In patients affected by lymphoma, bone marrow disease evaluation is considered one of most important step in the diagnostic iter. At this moment bone marrow biopsy (BMb) is considered the gold standard in this field, even if it presents some limitations. The aim of this study was to evaluate the usefulness of FDG-PET/CT, comparing it with BMb, in the detection of bone marrow disease in patients with HL and aggressive NHL and its therapeutic impact in this subset of patients. Between April 2004 and April 2006, 119 consecutive patients with lymphoma were referred for disease staging. In all patients the clinical stage was assessed according to the Ann Arbor classification including bilateral bone marrow biopsy and whole body FDG PET/CT scan. The range of time interval between c.e. CT, BMb, and PET/CT scan was of 2 weeks at maximum. Sensitivity, specificity, accuracy, positive and negative predictive value in bone disease evaluation were calculated for either PET and BMb. An analysis of bone disease presentation at FDG-PET scan was also performed dividing it in 2 patterns groups: solitary (single FDG focal uptake) and polyostotic localisation (2 or more focal FDG uptakes). These patterns were then correlated with BMb results. 1) FDG-PET/CT: sensitivity 69.2%, specificity 97.5%, accuracy 88.2%, positive and negative predictive value respectively 93.1% and 86.7% BMb: sensitivity 61.5%, specificity 100%, accuracy 87.4%, positive and negative predictive value respectively 100% and 84.2% 2) Correlation between FDG- PET patterns of disease at presentation (solitary and polyostotic localizations) and BMb findings are showed in Table 2. Our study demonstrates that the diagnostic role of BMb and FDG-PET in the evaluation of bone marrow disease is complementary. FDG-PET, in fact, improves BMb sensitivity especially when in presence of a solitary bone marrow disease localization. Our proposal is to perform FDG-PET/CT before bone marrow biopsy, to eventually address the biopsy site. 3) In 9 patients the therapeutic protocol was changed on the basis of FDG-PET findings. a b
description
a. b. ROLE OF FDG-PET/CT STUDY IN THE DETECTION OF BONE MARROW DISEASE IN PATIENTS WITH AGGRESSIVE NON-HODGKIN LYMPHOMA (NHL) AND HODGKIN LYMPHOMA (HL). - PowerPoint PPT Presentation
Transcript of ROLE OF FDG-PET/CT STUDY IN THE DETECTION OF BONE MARROW DISEASE IN PATIENTS WITH AGGRESSIVE...

ROLE OF FDG-PET/CT STUDY IN THE DETECTION OF BONE MARROW DISEASE IN PATIENTS WITH AGGRESSIVE NON-HODGKIN LYMPHOMA (NHL) AND HODGKIN LYMPHOMA (HL)
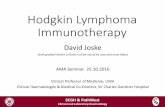
Figure 1. PET scan transaxial view in a patient with negative BMb upstaged by FDG-PET a) FDG-PET uptake at the sacral level confirmed to be pathological at MRI b) The same patient after chemotherapy
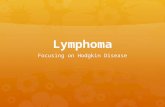
Figure 2. a) Patient negative at BMb with a solitary bone marrow disease localizations at PET b) Patient negative at BMb with polyostotic bone marrow disease at PET.
PET/CT BMb+
BMb- Tot
SOLITARY LOCALIZATIONSingle focality
2 62 (FP) 10
POLYOSTOTIC DISEASEMultiple focalities
10 9 19
Tot 12 17 29
Table 2. Bone disease patterns at FDG-PET/CT and BMb results.
BACKGROUND
OBJECTIVE
METHODS
RESULTS
CONCLUSIONS
E. Pelosi1-3, D. Deandreis1, D. Penna1, A. Chiappella2, P. Pregno2, M. Racca1, F. Carra'1, A. Douroukas3, U. Vitolo2, G. Bisi1.
1) SCDU Medicina Nucleare, ASO S. Giovanni Battista, Torino, Italy2) SCDO Ematologia, ASO S. Giovanni Battista, Torino, Italy3) Centro PET IRMET, Torino, Italy
PET + PET -BMb + 12 12 24BMb - 15 + 2 FP 78 95
29 90 119Table 1. Accordance/Discordance between PET e BMb in the evaluation of bone marrow disease.
In patients affected by lymphoma, bone marrow disease evaluation is considered one of most important step in the diagnostic iter. At this moment bone marrow biopsy (BMb) is considered the gold standard in this field, even if it presents some limitations.
The aim of this study was to evaluate the usefulness of FDG-PET/CT, comparing it with BMb, in the detection of bone marrow disease in patients with HL and aggressive NHL and its therapeutic impact in this subset of patients.
Between April 2004 and April 2006, 119 consecutive patients with lymphoma were referred for disease staging. In all patients the clinical stage was assessed according to the Ann Arbor classification including bilateral bone marrow biopsy and whole body FDG PET/CT scan. The range of time interval between c.e. CT, BMb, and PET/CT scan was of 2 weeks at maximum.Sensitivity, specificity, accuracy, positive and negative predictive value in bone disease evaluation were calculated for either PET and BMb. An analysis of bone disease presentation at FDG-PET scan was also performed dividing it in 2 patterns groups: solitary (single FDG focal uptake) and polyostotic localisation (2 or more focal FDG uptakes). These patterns were then correlated with BMb results.
1) FDG-PET/CT: sensitivity 69.2%, specificity 97.5%, accuracy 88.2%, positive and negative predictive value respectively 93.1% and 86.7%BMb: sensitivity 61.5%, specificity 100%, accuracy 87.4%, positive and negative predictive value respectively 100% and 84.2%
2) Correlation between FDG-PET patterns of disease at presentation (solitary and polyostotic localizations) and BMb findings are showed in Table 2.
Our study demonstrates that the diagnostic role of BMb and FDG-PET in the evaluation of bone marrow disease is complementary. FDG-PET, in fact, improves BMb sensitivity especially when in presence of a solitary bone marrow disease localization. Our proposal is to perform FDG-PET/CT before bone marrow biopsy, to eventually address the biopsy site.
3) In 9 patients the therapeutic protocol was changed on the basis of FDG-PET findings.
a
b