Role of Endoscopy in Iron Deficiency anemia
47
Giant Brunner gland adenoma manifesting as iron deficiency anemia and intussusception Prof. P. Kar, Rajiv Singla DEPARTMENT OF MEDICINE MAMC, Delhi
Transcript of Role of Endoscopy in Iron Deficiency anemia
Giant Brunner gland adenoma manifesting as irondeficiency anemia and intussusception
Prof. P. Kar, Rajiv SinglaDEPARTMENT OF MEDICINEMAMC, Delhi

History43 yrs/femaleR/o AssamPresented to MOPD with chief complaint of Pain in abdomen x 6 months. Easy fatigability x 6 months. Generalised weakness x 6 months.

No h/o Nausea/Vomitting/DiarroheaNo h/o feverNo h/o Jaundice.No h/o TB/DM/HTN.No h/o blood in vomitus/stool.No h/o wt. loss/decrease appetite.No h/o bone pains.No h/o abdominal distension.No h/o any chronic drug intake.

PAST HISTORY
History of similar complaints on and off for last 6-7 years present.
History of multiple blood transfusions for same complaints present
History FAMILY HISTORY
No significant family history.
PERSONAL HISTORYUpper middle income groupNon-smoker Non alcoholicVegetarian, but diet adequate
MENSURAL HISTORYRegular cycles, no excessive bleeding
GPE GC fair P = 74/min BP = 110/70 mm of Hg Pallor + RR = 14/min No Icterus No cynosis No clubbing JVP not raised No Peadal Oedema
SYSTEMIC EXAMINATION
CHEST B/L clear A/E equal
CVS S1 S2 are normal No MURMUR present
CNS WNL
P/A Soft non tender No organomeagly Bowl sounds + No Free Fluid

INVESTIGATIONSHb = 7.4TLC = 7300DLC = 74/24/1/1P/C = 2.23 lacP/S = microcytic hypochromic RBC
with few target cells.RBS = 98BU/S.Cr = 23/0.9Na+/K+ = 143/4.2T.Bil = 0.4AST/ALT = 23/25T.Pro/S.Alb = 6.8/3.4

S.Ferritin = 23.3 mcg/dl
Stool for occult blood= positive
Chest X-ray = WNL

Provisional Diagnosis Iron deficiency anemia due to GI blood loss

UGIE
Esophagus - No varicesStomach - Normal Duodenum - Polypoidal mass with pedunclated stalk in 2nd and 3rd part of duodenum was found

Barium Enteroclysis :
S/O a pedunclated Polypoidal filling defect witin the third part of Duodenum extending upto Duodeno-Jejunal junction.
M R Abdo with MR Enteroclysis :
A peduncalted polypoidal soft tissue mass in third and fourth part of duodenum with stalk extending upto the Ampulla of Vater
?? Adenoma.

DIAGNOSIS :-
Iron deficiency Anemia with GI Blood Loss due to Duodenal Adenoma
Course Patient was offered surgery, but patient
refused. Went back to Assam Had severe abdominal pain and was
diagnosed to have intussuception Was operated on emergency basis.

OPERATIVE FINDINGS Duodeno- duodenal intususception reaching upto
the Duodeno- jejunal junction, Could be reduced partially.
Longitudinal duodenotomy revealed a long stalk like structure and a polypoidal mass at the tip of it as an initiator of the intussusception.
Polyp was excised with clearance of more than three centimeters.
Polyp-size = 4x3x2 cm greeish white in colour.


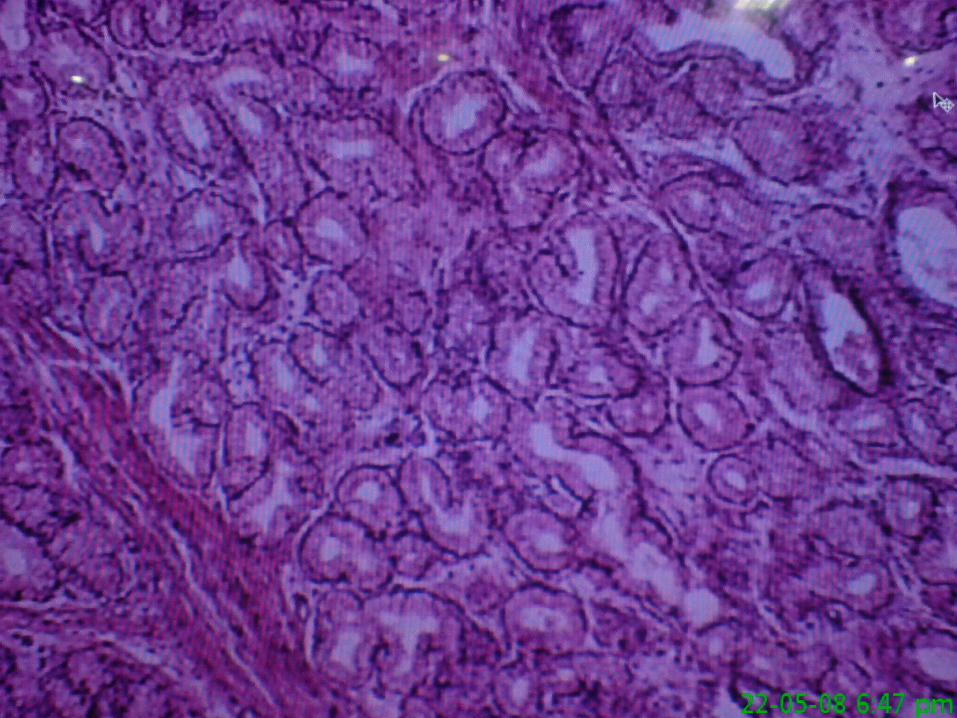
HISTOPATHOLOGICAL EXAMINATION Shows normal intestinal villi with sheets of
proliferated benign looking submucosal glandular structures. Focal areas shows small collections of chronic inflammatory cells.
S/o Brunner gland Adenoma (BRUNNEROMA)

AFTER SURGERY
HB = 11.4TLC = 7900DLC = 78/20/2P/C = 2.22 lacStool for Occult Blood = Negative

Final Diagnosis Brunner Gland Adenoma with iron
deficiency anemia
Role of Endoscopy in Iron Deficiency anemia
The role of fecal occult blood test in IDABrunner Gland Tumor

IRON DEFICIENCY ANEMIA ETIOLOGY:
• INCREASED IRON REQUIRMENT (JUVENILE AGE, PREGNANCY, LACTATION)
• DECREASED IRON INTAKE/ABSORBTION• CHRONIC BLEEDING
• MENORRHAGIA • GI LOSS• URINARY LOSS• EPISTAXIS• HEMOPTYSIS
Four per cent of referrals for endoscopy are initiated because of iron-deficiency anemia (IDA) Moses PL, Smith RE. Endoscopic evaluation of iron deficiency anemia. Postgrad Med 1995;98:213-24.


VALUE OF UGI ENDOSCOPY
Esophagogastroduodenoscopy (EGD) demonstrates pathology in 27% to 60% of individuals with IDA
strong correlation between a positive history of upper gastrointestinal tract symptoms and consequent lesions identified on EGD
More controversial is whether EGD is necessary in individuals without upper gastrointestinal symptoms
VALUE OF UGI ENDOSCOPY
Diseases important to diagnose, such as gastric cancer (up to 7% of cases causing IDA) or peptic ulcers (7% to 21%), cannot be ruled out on the basis of whether upper gastrointestinal symptoms are present.
Given the low risk of EGD presently, the expected benefit-to-risk ratio of EGD favours this procedure even in the absence of symptoms.

VALUE OF SMALL BOWEL BIOPSY
Trials have convincingly demonstrated that IDA may be the only manifestation of celiac sprue in absence of the classical findings of celiac sprue.
Prevalence of celiac sprue has been shown to be as high as 6% in a population of patients with IDA, emphasizing the need for small bowel biopsy in IDA even when other features of small bowel disease are not present.
On the other hand, the cost effectiveness of small bowel biopsy in IDA has not yet been calculated.

VALUE OF COLONOSCOPY Because colorectal cancer is the most life-
threatening disease among the common causes of IDA, colonoscopy is highly recommended, at slightest suspicion, as the initial procedure.
Anywhere from 16% to 30% of gastrointestinal lesions causing IDA can be identified by colonoscopy
Barium studies with or without sigmoidoscopy are less superior methods of examining the colon
VALUE OF COLONOSCOPY Classically, it is the patients with carcinoma of the
right colon who present with IDA, but carcinomas in the rectum and other parts of the colon may represent patients with IDA and no symptoms referable to the lower bowel.
Vascular malformations (angiodysplasia) have been associated with IDA in 3% to 9% of patients.
Other pathological lesions identified by colonoscopy include neoplastic polyps (5% to 15%), and much less commonly, colitis and colonic ulcerations.

CONCURRENT LESIONS A number of studies have identified patients with
concurrent lesions in the upper and lower tract. The frequency of such findings ranged from 1% to 17%,
with only one study quoting a frequency greater than 10% The data suggest that the older the population being
investigated, the greater the chance of identifying concurrent lesions.
Impossible to be certain which lesion is the major contributor to blood loss; therefore, both lesions often have to be treated.
No consensus on whether EGD is necessary after a lesion is found oncolonoscopy in a patient with IDA without symptoms referableto the upper gastrointestinal tract.
SITE-SPECIFIC SYMPTOM CORRELATION
In their prospective study of 100 patients, Rockey and Cello (28) found that symptoms do predict the location of the lesions underlying IDA. For example, in their article, the positive predictive values of history for predicting lesions in the upper and lower tract were 82% and 86%, respectively.
However, other investigators have been unable to confirm such a correlation and thus do not recommend the use of symptoms to direct the initial investigation (26-30).
Certainly, there is universal agreement that a lack of symptoms does not rule out disease and should not deter gastrointestinal investigation.

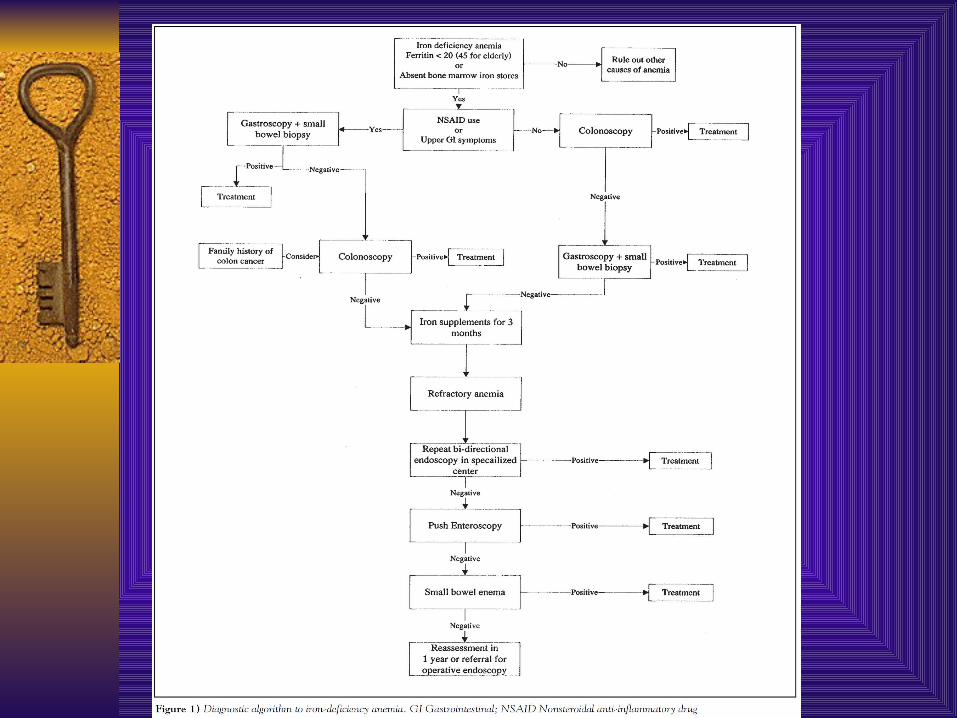
Assessment of Obscure GI Bleed In 7% to 47% of cases of IDA, the etiology of the anemia
remains unexplained after colonoscopy, gastroscopy and small bowel biopsy.
Several observations have been made about IDA of obscure origin by long term follow-up studies. – enteroclysis (small bowel enema) has a low yield if there are no
symptoms referable to the small bowel. – In about two-thirds of patients with IDA of obscure origin, the
anemia resolves by itself after a course of oral iron supplementation
– a high yield of finding a bleeding lesion can be expected from repeating colonoscopy and gastroscopy in a specialist unit
– enteroscopy shows a cause for obscure IDA in about 10% to 50% of cases
With the advent of enteroscopy, laparoscopy combined with intraoperative endoscopy is less often necessary
THE ROLE OF FECAL OCCULT BLOOD TEST IN IDA
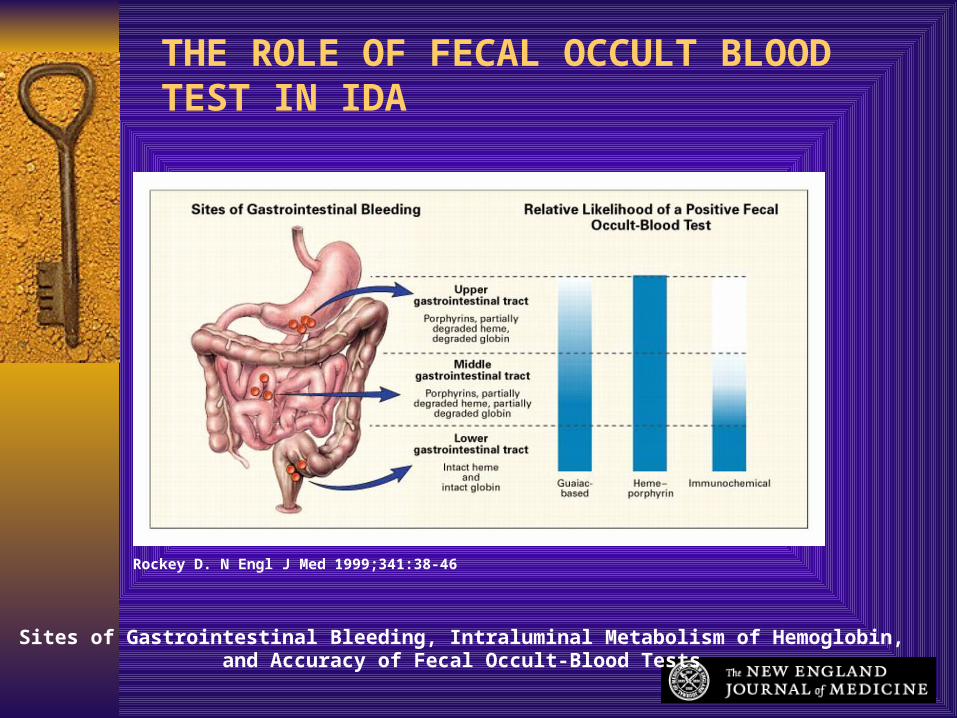
Rockey D. N Engl J Med 1999;341:38-46
Sites of Gastrointestinal Bleeding, Intraluminal Metabolism of Hemoglobin, and Accuracy of Fecal Occult-Blood Tests
THE ROLE OF FECAL OCCULT BLOOD TEST IN IDA
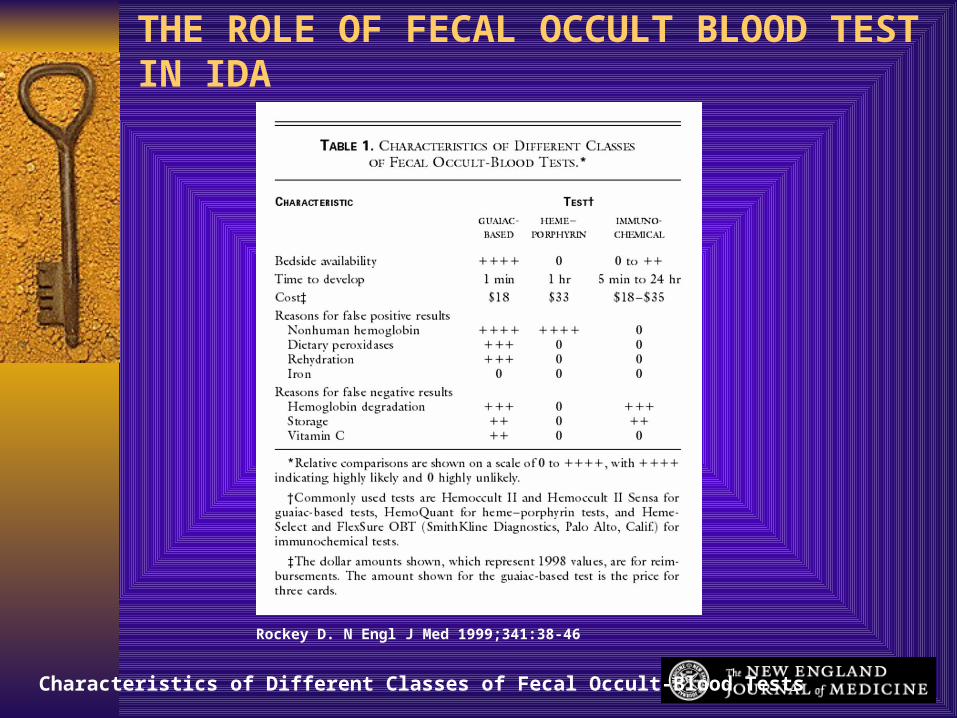
Rockey D. N Engl J Med 1999;341:38-46
Characteristics of Different Classes of Fecal Occult-Blood Tests
THE ROLE OF FECAL OCCULT BLOOD TEST IN IDA
THE ROLE OF FECAL OCCULT BLOOD TEST IN IDA Intuitively, fecal occult blood tests (FOBTs) appear to be
helpful in IDA to determine whether there is a bleeding lesion in the bowel
However, the literature does not support this hypothesis, chiefly because the pretest probability of the presence of a gut lesion in IDA is almost as high as the sensitivity of the FOBT
Accordingly, it is not surprising that most studies do not show any correlation in IDA between a positive FOBT and the presence or absence of a lesion in the bowel.
FOBT similarly is not helpful in determining the location of the bleeding lesion in the gut
FOBT is used best for screening (healthy individuals for colorectal cancer) rather than determining whether IDA is due to a bowel lesion
An approach to iron-deficiency anemia. Can J Gastroenterol Vol 15 No 11 November 2001

Brunner Gland Adenoma

Brunner Gland Adenoma Brunner’s gland adenoma (BGA) is a very rare benign
tumour of the duodenum. Less than 30 cases reported till date
BGA has a tendency to be predominant in the fifth or sixth decade of life with equal gender distribution
Clinical presentation is variable. Majority of cases are asymptomatic or present with non
specific, vague symptoms such as abdominal pain or discomfort, nausea or bloating.
BGA is usually an incidental finding during imaging studies or EGDS

Brunner Gland Adenoma In symptomatic patients, the most common clinical
presentations are gastrointestinal bleeding (37%) and obstructive symptoms (37%)[5].
Gastrointestinal bleeding manifests in the majority of cases as chronic loss of blood with iron deficiency and anaemia[6].
Less frequently, when erosion or ulceration of the tumour occurs, patients can present with melena or haematemesis.
These findings are usually described in BGA occurring beyond the fi rst portion of the duodenum, probably because these lesions are subjected to more stress and vascular damage from gastrointestinal motility[
Brunner Gland Adenoma Aetiology and pathogenesis of BGA still remain to be
elucidated. Due to the “anti-acid” function of Brunner’s glands, it has
been postulated that an increased acid secretion could stimulate these structures to undergo
A second hypothesis suggests that this lesion is of inflammatory origin due to the presence of a dense inflammatory cell infiltration. Since lymphocytes are usually present in the normal submucosa of the intestinal tract, the presence of inflammatory foci in the BGA is not sufficient to sustain the “inflammatory hypothesis”.
Finally, it has been suggested that H pylori infection may play a rolein the pathogenesis of BGA.
Brunner Gland Adenoma The duodenal bulb is the most frequent
localizationof BGA (57%) In the majority of cases, these lesions develop into
a polypoid mass, usually pedunculated (88%), being 1 to 2 cm in size while few cases reaching several centimetres as the ”giant BGA” have been reported
On the other hand, lesions < 1 cm are referred to as Brunner’s gland hyperplasia

Brunner Gland Adenoma Diagnosis can be obtained by histological
examination of the excised mass. Traditional endoscopy of pinching biopsies
is usually negative since the biopsy forceps are unable to reach the tumoral tissue localized completely in the submucosa layer
Brunner Gland Adenoma Endoscopic or surgical removal of BGA has been
suggested to prevent the development of complications (haemorrhage, severe anaemia, obstruction or intussusception).
Endoscopic polypectomy represents the ideal approach, which is more cost-effective and less invasive of the abdominal surgery [22, 23]. However, the success depends on site and size of the BGA and presence of a peduncle.