Effects of Cyclooxygenase Inhibitors in Combination with ...
Click here to load reader

Fax +41 61 306 12 34E-Mail [email protected]
Chronic Inflammation
Dig Dis 2010;28:585–589 DOI: 10.1159/000320278
Role of Cyclooxygenase-2 in Pathogenesis and Prevention of Colorectal Cancer
Ezra Hahn a Sarah Kraus b, c Nadir Arber b, c
a University of Toronto , Faculty of Medicine, Toronto, Ont. , Canada; b The Integrated Cancer Prevention Center,Tel Aviv Sourasky Medical Center, and c Sackler School of Medicine, Tel Aviv University, Tel Aviv , Israel
trials were terminated early due to discovery of significant cardiovascular toxicity, although the exact extent of this tox-icity remains unclear. The exact mechanisms through which NSAIDs exert their cancer preventing effects are currently unknown; inhibition of COX-2 is of great importance, but COX-2 independent pathways exist as well. In addition, the efficacy of NSAID use for cancer prevention can differ sig-nificantly between individuals. Personalized medicine in this field is also greatly anticipated. Combination therapy is un-der extensive research in order to improve efficacy while reducing toxicity profiles. Chemoprevention of colorectal cancer is largely possible, but the ultimate drug and proper patient selection, among other elements of the cancer pre-vention equation, are still needed.
Copyright © 2010 S. Karger AG, Basel
Colorectal cancer (CRC) is a major health concern world-wide. In 2010 alone, more than 1,000,000 new cas-es of CRC and over 500,000 deaths from the disease are predicted [1] . An estimated 75% of the new cases will oc-cur in individuals at average risk [2] . Although screening and surveillance strategies are standard clinical practice in early detection of CRC, their impact is limited due to low adherence to current screening guidelines. Mortality rates from CRC have declined over the last 2 decades, but the number of deaths due to this disease remains alarm-
Key Words
Colorectal cancer � Chemoprevention � Cyclooxygenase-2 � Nonsteroidal anti-inflammatory drugs
Abstract
Chemoprevention of colorectal cancer is a promising sci-ence that has particular importance due to the limited suc-cess of current treatments for most advanced common ma-lignancies. Many chemopreventive agents have been stud-ied including cyclooxygenase (COX) inhibitors. Two isoforms of the COX enzymes are COX-1 and COX-2. COX-1 is constitu-tively expressed in normal tissue, serving an important role in tissue homeostasis, whereas COX-2 is an inducible en-zyme, which is markedly overexpressed at sites of inflamma-tion and colorectal neoplasms. The preventive efficacy of traditional nonsteroidal anti-inflammatory drugs (NSAIDs), which inhibit COX-1 and/or COX-2, has considerable support from animal and epidemiological studies; however, thereare well-documented toxicities associated with NSAID use. These adverse effects are attributed to NSAIDs’ inhibition of COX-1. The development of COX-2 specific inhibitors gave hopes of bypassing the associated traditional NSAID toxici-ties while better targeting tissues sustaining inflammation and neoplasia. The PrsSAP, APC and APPROVe trials demon-strated the efficacy of COX-2 specific inhibitors in preventing the recurrence of sporadic colorectal polyps. However, the
Nadir Arber, MD, MSc, MHA The Integrated Cancer Prevention Center3/3 Floor, Arison Medical Tower , Tel-Aviv Sourasky Medical Center6 Weizmann St., Tel Aviv 64239 (Israel) Tel. +972 3 697 4968, Fax +972 3 697 4867, E-Mail nadir @ tasmc.health.gov.il
© 2010 S. Karger AG, Basel0257–2753/10/0285–0585$26.00/0
Accessible online at:www.karger.com/ddi
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
3:04
:52
PM

Hahn /Kraus /Arber
Dig Dis 2010;28:585–589586
ing. These facts in conjunction with the limited success of current treatments for most advanced common malig-nancies make cancer prevention paramount.
Chemoprevention is an emerging science that pro-vides a promising approach to reduce the incidence of, and mortality from, CRC. Chemoprevention of CRC in-volves the use of a variety of natural or chemical com-pounds that can delay, prevent or even reverse the devel-opment of adenomas or the adenoma to carcinoma pro-cess in the colon. CRC fits the criteria for chemopreventive intervention as it is prevalent, associated with high mor-bidity and mortality, and on average has a 15- to 20-year progression from precursor to malignant lesion, provid-ing a window of opportunity to implement treatment and preventative strategies [3] . Such strategies may be of par-ticular importance to those with a hereditary predisposi-tion to colorectal neoplasia and other high-risk individu-als. Chemoprevention of CRC is an exciting field and many potential compounds and targets have been identi-fied. These agents can essentially be organized mecha-nistically into 3 broad categories [4, 5] : (1) anti-inflam-matory modulators ; (2) signal transduction modulators ; (3) epigenetic modulators.
Agents studied, including folic acid, calcium, estrogen, vitamins, oltipraz, ursodiol, statins and fiber, among oth-ers, have been encouraging, but have only shown mod-est chemopreventive efficacy in clinical trials. The most promising drugs, however, are aspirin and the nonsteroi-
dal anti-inflammatory drugs (NSAIDs). NSAIDs have been extensively studied and much of their effect has been attributed to their potent inhibition of the cyclooxy-genase (COX) enzymes.
The COX enzymes, also known as prostaglandin-en-doperoxide synthases, are central and rate-limiting en-zymes in prostaglandin biosynthesis [6] . COX oxidizes arachidonic acid to prostaglandin G 2 , and subsequently reduces prostaglandin G 2 to prostaglandin H 2 . Further metabolism leads to various prostaglandins that have paracrine and autocrine functions. Soon after their dis-covery in the early 20th century, prostaglandins were found to be important mediators in a variety of physio-logical functions, such as pain, fever, renal function, im-munity and mucosal homeostasis, among others.
Currently, three COX isoforms have been identified: COX-1, COX-2 and COX-3. COX-3, a splice variant of the COX-1 gene, was recently identified and its exact role is yet to be described [7] . COX-1 and COX-2 are located on different chromosomes and are both highly regulated [6] . COX-1 is mapped on chromosome 9q32-q33.2 and isconstitutively expressed in normal tissues, serving as a ‘housekeeper’ of mucosal integrity. It produces prostacy-clins, prostaglandins and thromboxane, which protect gastric mucosa and play a key role in platelet aggregation and renal microvasculature dynamics. In contrast, COX-2, which is mapped on 1q25.2-q25.3, is an immediate ear-ly response gene that is highly inducible by neoplastic and inflammatory stimuli; it is important in inflammation, wound healing, immune regulation, angiogenesis and as-pects of embryonic development.
COX-2 is markedly overexpressed in colorectal neo-plasms [8] . Relative to normal mucosa, COX-2 overex-pression occurs in approximately 40% of colorectal ad-enomas and 85% of human CRCs, making COX-2 an attractive therapeutic target [9] . Indeed, already in the mid-1970s, NSAIDs were hypothesized to inhibit growth of CRC after a significant increase of prostaglandin E 2 was observed in CRC tissue compared to normal sur-rounding mucosa [10] . Of notable importance is the tis-sue specificity achievable with selective COX-2 inhibi-tion – tissues sustaining inflammation or carcinogene-sis.
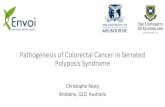
Traditional NSAIDs inhibit COX-1 and or COX-2 [6] . The preventive efficacy of this class of agents is supported by more than 200 animal studies. Most significantly, 60 out of 62 epidemiological studies clearly demonstrated that NSAID consumption prevents adenoma formation and decreases the incidence of, and mortality from, CRC ( fig. 1 ) [5] . However, NSAID consumption is not innocu-
0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6
Mortality
CRC
Adenomas
Fig. 1. Relative risk of colorectal neoplasia in individuals using aspirin, NSAIDs and COX-2 inhibitors (62 epidemiological stud-ies, 1988–2009).
Colo
r ver
sion
ava
ilabl
e on
line
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
3:04
:52
PM

Cyclooxygenase-2 in Pathogenesis and Prevention of Colorectal Cancer
Dig Dis 2010;28:585–589 587
ous. Effects of gastrointestinal toxicity, such as ulcer-ation, bleeding and perforation, are well-known com-plications of NSAID use. It is estimated that of the 60 million Americans consuming NSAIDs, 1–2% will expe-rience a clinically significant upper gastrointestinal event [11] . In 2002, in the United States alone, 260,000 hospital-izations and 26,000 deaths were attributed to NSAID consumption [12] .
Gastrointestinal toxicity, as well as renal toxicity and antiplatelet effects, are attributed to inhibition of COX-1 and prostaglandin biosynthesis [13] . In the early 1990s, pharmaceutical companies began developing COX-2 in-hibitors that do not affect COX-1 activity. COX-2 specific inhibitors, which should have an improved safety profile, are ideal drug candidates for the prevention of CRC, since increased expression of COX-2 is seen from the first ge-netically altered cell, through hyperplasia, dysplasia, car-cinoma and even metastasis, allowing for chemopreven-tive effects throughout the multistep process of CRC car-cinogenesis [14–16] .
Oshima et al. [17] provided direct genetic evidence of the role of COX-2 in colorectal carcinogenesis. APC 716 knockout mice, which have a truncation mutation in their APC gene and develop hundreds of intestinal pol-yps, were used for the experiment. The number of polyps was studied upon knocking out 1 or both of the COX-2 alleles. Compared to control APC 716 mice, the number of polyps was reduced by 34 and 86% upon knocking out one and both COX-2 alleles, respectively. In addition, when both COX-2 alleles were knocked out, there was a reduction of average polyp size.
A proof of concept in humans was achieved in the set-ting of familial adenomatous polyposis patients [18] . Eighty-one patients were selected from London’s St. Mark’s Hospital and Houston’s M.D. Anderson Medical Center for this randomized, double-blind, placebo-con-trolled trial of celecoxib. Patients were selected to receive twice-daily dosages of 400 or 800 mg of drug, or placebo, for 6 months. A 30% reduction of polyp burden was seen in the patients receiving the higher dosage.
Three international, multicenter, prospective, ran-domized, placebo-controlled trials investigating second-ary prevention of CRC were launched in 1999 and 2000 to evaluate the efficacy and safety of the new COX-2 spe-cific inhibitors in preventing the recurrence of sporadic colorectal polyps. These clinical trials demonstrated the potential of chemoprevention as a strategy for reducing cancer incidence, although not without associated side effects. The attractiveness of these drugs partly stems from an ability to engage multiple mechanisms of action
by their potential to influence multiple components of the carcinogenesis pathway, from initiation to progres-sion.
In the Prevention of Colorectal Sporadic Adenoma-tous Polyps (PreSAP) study [19] , sponsored by Pfizer, the effectiveness of celecoxib (400 mg q.d.) in reducing the incidence of sporadic colorectal adenomas was evaluated. It recruited 1,561 patients from 107 sites in 32 countries. Patients were split into a 3: 2 ratio of celecoxib (n = 933) and placebo (n = 628) and stratified for baseline aspirin use (17%). Of the total patients, 89 and 79% underwent a colonoscopy with or without removal of polyps at 1 year and 3 years, respectively. Celecoxib reduced adenoma re-currence by a third after 1 and 3 years (p ! 0.001). The incidence of advanced adenomas (greater than 1 cm, tu-bulovillous or villous histology, high-grade dysplasia, or invasive cancer) was reduced by 51%.
The Adenoma Prevention with Celecoxib (APC) trial [20] , the 2nd study, which was supported by the NCI, en-rolled 2,035 patients from 110 sites in the USA, UK, Can-ada and Australia. Patients were randomized to receive placebo (n = 679), celecoxib 200 (n = 586) or 400 mg (n = 671) b.i.d. A follow-up colonoscopy was conducted in 89 and 76% of the participants after 1 and 3 years, respec-tively. In patients taking celecoxib, polyp recurrence was reduced by 33% for patients taking 400 mg of the drug, and 45% for patients taking 800 mg of the drug (p ! 0.0001). The relative risk of advanced adenomas was even more drastically reduced: by 57 and 66%, respectively, for patients taking the 2 dosages (p ! 0.0001).
In a 3rd study conducted by Merck, the Adenomatous Polyp Prevention on Vioxx (APPROVe) [21] , rofecoxib at 25 mg q.d., was evaluated relative to placebo. 2,547 par-ticipants from 110 sites were recruited. A 25% reduction in polyp recurrence was seen after 1 and 3 years.
However, the APPROVe and the APC studies were ter-minated earlier than planned due to substantial concern of increased cardiovascular (CVS) toxicity [22, 23] , as seen by an increase in CVS events (mainly myocardial infarction, stroke and heart failure). The CVS toxicity seen in the APPROVe trial caused Merck to withdraw ro-fecoxib from the market; this decision was made even be-fore the efficacy of the drug was evaluated. In the APC trial, the CVS toxicity, as evaluated by an independent CVS adjudicating committee, increased from 1.0% (n = 7/679) for placebo to 2.5% (n = 16/685) and 3.4% for cele-coxib (200 and 400 mg b.i.d., respectively; p ! 0.01). These findings caused the NCI to suspend the trial. Lastly, the proportion of all patients experiencing CVS toxicity in the PreSAP trial increased from 1.9% (n = 12/628) for pla-
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
3:04
:52
PM

Hahn /Kraus /Arber
Dig Dis 2010;28:585–589588
cebo to 2.5% (n = 23/933) for celecoxib (400 mg q.d.; p = NS). The CVS toxicity in the PreSAP study was higher in the celecoxib arm, but was not statistically significant. Nevertheless, Pfizer decided to close the trial as well.
Of note is the disparity in CVS toxicity from celecox-ib between the APC and PreSAP trials [3] . A plausible explanation for this discrepancy is the obvious differ-ence in dosages. The APC trial gave celecoxib twice dai-ly, for a total daily dose of 400 or 800 mg. It stands to reason that a greater dose increases the likelihood of an adverse reaction. Another plausible explanation for the discrepancy is that the 400 mg given once daily in the PreSAP trial was less toxic than the 200 mg given twice daily in the APC trial because of the relatively short half-life of celecoxib.
The actual extent of the CVS risk associated with COX-2 selective inhibitors remains unclear [24] . The tri-als mentioned were not designed to study CVS events and it was difficult to control confounding variables. In addi-tion, the number of events was very low. The data also shows that most patients tolerated 3 years of celecoxib use without the related toxicity [25] . Part of the design of the trials was a colonoscopy 1 year after drug use in the study. The polyp recurrence rate reduction was the same after1 and 3 years in all 3 studies. This suggests that use of COX-2 inhibitors for 1 year may be sufficient to prevent polyp recurrence. These trials also found that relative to placebo, the patients taking celecoxib who developed ad-enomas had fewer and smaller tumors; celecoxib did not only reduce tumor number, it reduced the more serious lesions and the overall burden of disease. The discovery of CVS toxicity related to COX-2 specific inhibitors has made development of new agents in this field difficult; indeed, considerable caution must be employed in light of the discovered associated toxicity. However, to ignore po-tential benefit from chemoprevention is to accept a high-er than necessary death rate from CRC.
On the other hand, the gastrointestinal toxicity of ce-lecoxib in the PreSAP and APC trials was recently adju-dicated. There was no significant difference between the drug and placebo for the entire 3-year duration of the study. Surprisingly, low-dose aspirin ( ! 100 mg/day) was associated with a significantly increased gastrointestinal complication rate (HR 2.93; Arber et al., unpubl. data).
The exact mechanisms by which NSAIDs exert their anticancer properties are currently unknown. Inhibition of COX-2 and prostaglandin synthesis is an important step in CRC prevention as COX-2 contributes to tumori-genesis through multiple mechanisms [6] . COX-2 inhibi-tion can reduce proliferation, induce apoptosis, suppress
tumor angiogenesis, prevent immune suppression and inhibit carcinogen conversion. Yet, COX-2 inhibitors work through COX-2 independent pathways as well. Ce-lecoxib can inhibit growth and induce apoptosis in can-cer cells not expressing COX. A variety of non-COX-2 targets for COX-2 inhibitors have been suggested [26–29] : inhibition of nuclear factor- � B, interference of peroxi-some proliferator-activating receptor- � binding to DNA, activation of peroxisome proliferator-activating recep-tor- � , activation of protein kinase G and downregulation of Bcl-XL – an antiapoptotic protein.
Personalized medicine has remained an elusive goal and its utilization in chemoprevention is greatly antici-pated. To illustrate, NSAIDs’ preventive efficacy against CRC carcinogenesis is not fully understood. If COX-2inhibition is the principal mechanism through which NSAIDs work, then these agents should be targeted at tu-mors that overexpress COX-2. In fact, the efficacy of as-pirin differs significantly according to COX-2 expression. Aspirin reduces the risk of CRC in COX-2 expressing cancers, but it is not an effective chemopreventive agent for cancers with weak or absent COX-2 expression [30] . The efficacy and toxicity of NSAID use may be affected by polymorphisms in NSAID targets and metabolizing enzymes [31] . In fact, chemoprevention may not benefit all individuals [32] . As well, the increased metabolizing enzymes, prostaglandin H synthase-2 and uridine di-phosphatidyl glucotransferase polymorphisms, may in-crease chemopreventive efficacy by up to 50% [33, 34] .
An exciting field currently under extensive research is that of combination therapy. This field has the goal of in-creasing the chemopreventive efficacy, which tends to be modest with single compounds in clinical trials, and to decrease the unacceptable toxicity profiles by combining low doses of different agents. In rats with carcinogen-in-duced aberrant crypt foci, a statin and sulindac combina-tion reduced the number of aberrant crypt foci to a great-er degree than each of the drugs alone [35, 36] . Similarly, another study showed that piroxicam in combination with difluoromethylornithine was more effective than ei-ther compound alone [37] . Additionally, curcumin, a tur-meric extract, combined with low doses of celecoxib, po-tentiates the growth inhibitory effect of either drug alone.
When contemplating the use of COX-2 inhibitors, 4 suggestions to consider are [3] : (1) patients should be at high-risk or select moderate-risk for CRC; (2) there should be no Helicobacter pylori infection; (3) patients with CVS risk factors should be excluded; (4) weighing CVS prophylaxis against adverse gastrointestinal side ef-fects may imply using celecoxib with low-dose aspirin.
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
3:04
:52
PM

Cyclooxygenase-2 in Pathogenesis and Prevention of Colorectal Cancer
Dig Dis 2010;28:585–589 589
In the intriguing jigsaw puzzle of cancer prevention, we now have a definite positive answer for the basic ques-tion ‘if ’, but several other parts of the equation – proper patient selection, the ultimate drug, optimal dosage and duration, and best screening modality – are still missing.
Disclosure Statement
The authors declare that no financial or other conflict of inter-est exists in relation to the content of the article.
References
1 World Health Organization: Cancer. http://www.who.int/mediacentre/factsheets/fs297/en/index.html (accessed July 16, 2010).
2 Weir HK, Thun MJ, Hankey BF, et al: An-nual report to the nation on the status of can-cer, 1975–2000, featuring the use of surveil-lance data for cancer prevention and control. J Natl Cancer Inst 2003; 95: 1276–1299.
3 Arber N: Cyclooxygenase-2 inhibitors in colorectal cancer prevention: point. Cancer Epidemiol Biomarkers Prev 2008; 17: 1852–1857.
4 Takayama T, Goji T, Taniguchi T, Inoue A: Chemoprevention of colorectal cancer – ex-perimental and clinical aspects. J Med Invest 2009; 56: 1–5.
5 Kraus S, Arber N: Colorectal cancer chemo-prevention: ready for practice? Eur J Cancer 2009; 45(suppl 1):360–366.
6 Tuynman JB, Peppelenbosch MP, Richel DJ: COX-2 inhibition as a tool to treat and pre-vent colon cancer. Crit Rev Oncol Hematol 2004; 52: 81–101.
7 Chandrasekharan NV, Dai H, Roos KL, et al: COX-3, a cyclooxygenase-1 variant inhibited by acetaminophen and other analgesic/anti-pyretic drugs: cloning, structure, and ex-pression. Proc Natl Acad Sci USA 2002; 99: 13926–13931.
8 Half E, Arber N: Colon cancer: preventive agents and the present status of chemopre-vention. Expert Opin Pharmacother 2009; 10: 211–219.
9 Eberhart CE, Coffey RJ, Radhika A, et al: Up-regulation of cyclooxygenase 2 gene expres-sion in human colorectal adenomas and ad-enocarcinomas. Gastroenterology 1994; 107: 1183–1188.
10 Bennett A, Del Tacca M: Proceedings: pros-taglandins in human colonic carcinoma. Gut 1975; 16: 409.
11 Cryer B: NSAID-associated deaths: the rise and fall of NSAID-associated GI mortality. Am J Gastroenterol 2005; 100: 1694–1695.
12 Grover JK, Yadav S, Vats V, Joshi YK: Cyclo-oxygenase 2 inhibitors: emerging roles in the gut. Int J Colorectal Dis 2003; 18: 279–291.
13 FitzGerald Ga, Patrono C: The coxibs, selec-tive inhibitors of cyclooxygenase-2. N Engl J Med 2001; 345: 433–42.
14 DuBois RN, Radhika A, Reddy BS, et al: In-creased cyclooxygenase-2 levels in carcino-gen-induced rat colonic tumors. Gastroen-terology 1996; 110: 1259–1262.
15 Shiff SJ, Rigas B: The role of cyclooxygen-ase inhibition in the antineoplasic effectsof nonsteroidal antiinflammatory drugs (NSAIDs). J Exp Med 1999; 190: 445–450.
16 Hao XP, Bishop AE, Wallace MH, et al: Early expression of cyclooxygenase-2 during spo-radic colorectal carcinogenesis. J Pathol 1999; 187: 295–301.
17 Oshima M, Murai N, Kargman S, et al: Che-moprevention of intestinal polyposis in the Apcdelta716 mouse by rofecoxib, a specif-ic cyclooxygenase-2 inhibitor. Cancer Res 2001; 61: 1733–1740.
18 Steinbach G, Lynch P, Phillips RK, et al: The effect of celecoxib, a cyclooxygenase-2 inhib-itor, in familial adenomatous polyposis. N Engl J Med 2000; 342: 1946–1952.
19 Arber N, Eagle CJ, Spicak J, et al: Celecoxib for the prevention of colorectal adenomatous polyps. N Engl J Med 2006; 355: 885–895.
20 Bertagnolli MM, Eagle CJ, Zauber AG, et al: Celecoxib for the prevention of sporadic colorectal adenomas. N Engl J Med 2006; 355: 873–884.
21 Baron JA, Sandler RS, Bresalier RS, et al: A randomized trial of rofecoxib for the chemo-prevention of colorectal adenomas. Gastro-enterology 2006; 131: 1674–1682.
22 Bresalier RS, Sandler RS, Quan H, et al: Car-diovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005; 352: 1092–1102.
23 Solomon SD, McMurray JJ, Pfeffer MA, et al: Cardiovascular risk associated with celeco-xib in a clinical trial for colorectal adenoma prevention. N Engl J Med 2005; 352: 1071–1080.
24 Hawk E, Vinder JL: The adenoma prevention with celecoxib and prevention of colorectal sporadic adenomatous polyps trials: step-ping stones to progress. Cancer Epidemiol Biomarkers Prev 2007; 15: 185–187.
25 Bertagnolli MM: Chemoprevention of colo-rectal cancer with cyclooxygenase-2 inhibi-tors: two steps forward, one step back. Lancet Oncol 2007; 8: 439–443.
26 Rao CV, Reddy BS: NSAIDs and chemopre-vention. Curr Cancer Drug Targets 2004; 4: 29–42.
27 Sinicrope FA: Targeting cyclooxygenase-2 for prevention and therapy of colorectal can-cer. Mol Carcinog 2006; 45: 447–454.
28 Arber N, Levin B: Chemoprevention of colorectal neoplasia; the potential for per-sonalized medicine. Gastroenterology 2008; 134: 1224–1237.
29 Grover JK, Yadav S, Vats V, Joshi YK: Cyclo-oxygenase 2 inhibitors: emerging roles in the gut. Int J Colorectal Dis 2003; 18: 279–291.
30 Chan AT, Ogino S, Fuchs CS: Aspirin and the risk of colorectal cancer in relation to the ex-pression of COX-2. N Engl J Med 2007; 356: 2131–2142.
31 Ulrich CM, Bigler J, Potter JD: Non-steroidal ant-inflammatory drugs for cancer preven-tion: promise, perils and pharmacogenetics. Nat Rev Cancer 2006; 6: 130–140.
32 Bigler J, Whitton J, Lampe JW, et al: CYP2C9 and UGT1A6 genotypes modulate the pro-tective effect of aspirin on colon adenoma risk. Cancer Res 2001; 61: 3566–3569.
33 Macarthur M, Sharp L, Hold GL, Little J, El-Omar EM: The role of cytokine gene poly-morphisms in colorectal cancer and theirinteraction with aspirin use in the northeast of Scotland. Cancer Epidemiol Biomarkers Prev 2005; 14: 1613–1618.
34 Lin HJ, Lakkides KM, Keku TO, et al: Pros-taglandin H synthase 2 variant (Val511Ala) in African Americans may reduce the risk for colorectal neoplasia. Cancer Epidemiol Biomarkers Prev 2002; 11: 1305–1315.
35 Agarwal B, Rao CV, Bhendwal S, et al: Lov-astatin augments sulindac-induced apopto-sis in colon cancer cells and potentiateschemopreventive effects of sulindac. Gas-troenterology 1999; 117: 838–847.
36 Reddy BS, Wang CX, Kong AN, et al: Preven-tion of azoxymethane-induced colon cancer by combination of low doses of atorvastatin, aspirin, and celecoxib in F 344 rats. Cancer Res 2006; 66: 4542–4546.
37 Jacoby RF, Cole CE, Hawk ET, et al: Ursode-oxycholate/Sulindac combination treatment effectively prevents intestinal adenomas in a mouse model of polyposis. Gastroenterology 2004; 127: 838–844.
Dow
nloa
ded
by:
Uni
v. o
f Mic
higa
n, T
aubm
an M
ed.L
ib.
141.
213.
236.
110
- 9/
27/2
013
3:04
:52
PM