Roentgenological study of the superior and posterior mediastinum
17
ROENTGENOLOGICAL STUDY OF THE SUPERIOR AND POSTERIOR MEDIASTINUM” SAMUEL BROWN, M.D., AND HAROLD G. REINECKE, M.D. CINCINNATI, OHIO I N a previous communication1 our study was confined to the soft structures of the neck. In the present paper we shaI1 deaI chiefly with the structures of the superior and posterior mediastinum. It is our experience, based on a Iarge number of examinations, that no study of the superior and posterior mediastinum is compIete unIess both the anteroposterior and IateraI views are made. Of the two the IateraI view often renders more vaIuabIe information than the anteroposterior view. In the Iatter severa dense structures such as the sternum, spine, heart, and great bIood vesseIs are superimposed, thus ob- scuring to more or Iess degree the soft structures of the mediastinum. We aIso find that a true IateraI view is of greater vaIue than the obIique view. This is due to the fact that a knowIedge of the norma reIationship between the various structures in a true anteroposterior and IateraI positions is more readiIy acquired. Thus a deviation from the norma in the reIationship of the structures is more easiIy recognized. The mediastinum is that portion of the chest which is not occupied by the Iungs and pIeurae. It is bounded in the front by the sternum and behind by the dorsa1 spine. The IateraI boundaries are formed by the pIeura1 sacs. The mediastinum is divided into a superior and an inferior portion by an imaginary pIane which corresponds to a horizonta1 Iine drawn from the Iower part of the body of the fourth dorsa1 vertebra to the junction between the manubrium and the gIadioIus. The inferior portion is subdivided by the anterior and posterior Iayers of the peri- cardium into an anterior, middIe, and ‘Am. J. Roentgenol ff Rad. Tberapy, 20: 208-212. 1928. posterior mediastinum. The anterior mediastinum is in front of the pericardium. The middIe mediastinum is within the pericardia1 sac, and the posterior medi- astinum is behind the pericardium and in front of the dorsa1 vertebrae. In this communication we are interested in the roentgenoIogica1 consideration of the supe- rior and posterior mediastinum. The position of the mediastina1 struc- tures is essentiaIIy due to the equiIibrium between the two pIeura1 cavities and the position of the diaphragm. Any change of the position of the diaphragm or any dis- turbance of the equaIity of pressure between the two pIeura1 cavities wiII pro- duce a disIocation of the mediastina1 structures. Both IocaI or genera1 causes may be responsibIe for a change in the position of any of the structures. The IocaI causes wiI1 receive our specia1 attention and the structures deaIt with wiI1 be the trachea, esophagus and aorta. The position of the trachea, esophagus and aorta as reveaIed in the anteropos- terior view is famiIiar to a11 roentgenoIo- gists. Any deviation of these structures from their norma course in a IateraI direc- tion and the significance which that impIies is fuIIy appreciated by aI1. How- ever, the significance of the exact position of these structures as seen in the Iateral view and their deviations in the antero- posterior direction is very much Iess understood by the average student of roentgenoIogy of the thorax. We shaI1, therefore, make a detaiIed description of these structures in the foIIowing few paragraphs. In the IateraI view of the thorax, the trachea (Fig. I A and B) is recognized on the roentgenogram by its greater trans- parency in the shape of a narrow coIumn *Submitted for pubIication October II, 1930. 452
-
Upload
samuel-brown -
Category
Documents
-
view
215 -
download
2
Transcript of Roentgenological study of the superior and posterior mediastinum

ROENTGENOLOGICAL STUDY OF THE
SUPERIOR AND POSTERIOR MEDIASTINUM”
SAMUEL BROWN, M.D., AND HAROLD G. REINECKE, M.D.
CINCINNATI, OHIO
I N a previous communication1 our study was confined to the soft structures of the neck. In the present paper we shaI1
deaI chiefly with the structures of the superior and posterior mediastinum.
It is our experience, based on a Iarge number of examinations, that no study of the superior and posterior mediastinum is compIete unIess both the anteroposterior and IateraI views are made. Of the two the IateraI view often renders more vaIuabIe information than the anteroposterior view. In the Iatter severa dense structures such as the sternum, spine, heart, and great bIood vesseIs are superimposed, thus ob- scuring to more or Iess degree the soft structures of the mediastinum.
We aIso find that a true IateraI view is of greater vaIue than the obIique view. This is due to the fact that a knowIedge of the norma reIationship between the various structures in a true anteroposterior and IateraI positions is more readiIy acquired. Thus a deviation from the norma in the reIationship of the structures is more easiIy recognized.
The mediastinum is that portion of the chest which is not occupied by the Iungs and pIeurae. It is bounded in the front by the sternum and behind by the dorsa1 spine. The IateraI boundaries are formed by the pIeura1 sacs. The mediastinum is divided into a superior and an inferior portion by an imaginary pIane which corresponds to a horizonta1 Iine drawn from the Iower part of the body of the fourth dorsa1 vertebra to the junction between the manubrium and the gIadioIus. The inferior portion is subdivided by the anterior and posterior Iayers of the peri- cardium into an anterior, middIe, and
‘Am. J. Roentgenol ff Rad. Tberapy, 20: 208-212. 1928.
posterior mediastinum. The anterior mediastinum is in front of the pericardium. The middIe mediastinum is within the pericardia1 sac, and the posterior medi- astinum is behind the pericardium and in front of the dorsa1 vertebrae. In this communication we are interested in the roentgenoIogica1 consideration of the supe- rior and posterior mediastinum.
The position of the mediastina1 struc- tures is essentiaIIy due to the equiIibrium between the two pIeura1 cavities and the position of the diaphragm. Any change of the position of the diaphragm or any dis- turbance of the equaIity of pressure between the two pIeura1 cavities wiII pro- duce a disIocation of the mediastina1 structures. Both IocaI or genera1 causes may be responsibIe for a change in the position of any of the structures. The IocaI causes wiI1 receive our specia1 attention and the structures deaIt with wiI1 be the trachea, esophagus and aorta.
The position of the trachea, esophagus and aorta as reveaIed in the anteropos- terior view is famiIiar to a11 roentgenoIo- gists. Any deviation of these structures from their norma course in a IateraI direc- tion and the significance which that impIies is fuIIy appreciated by aI1. How- ever, the significance of the exact position of these structures as seen in the Iateral view and their deviations in the antero- posterior direction is very much Iess understood by the average student of roentgenoIogy of the thorax. We shaI1, therefore, make a detaiIed description of these structures in the foIIowing few paragraphs.
In the IateraI view of the thorax, the trachea (Fig. I A and B) is recognized on the roentgenogram by its greater trans- parency in the shape of a narrow coIumn
*Submitted for pubIication October II, 1930.
452

New SERIES VOL. X, No. 3 Brown & Reinecke-Mediastinum American ~ournat of surgery 453
which bisects the superior mediastinum puImonary artery there is often seen a into two aImost equa1 parts. The anterior ring-Iike shadow due to the origin of the part is in front of the trachea and is major branches of the bronchi. In front
:IG. I A. Anterior view. Trachea and bronchi injected with IipiodoI. Notice close reIationship which exists
FIG. I B. LateraI view. Trachea bisects superior medi-
between trachea on right and arch of aorta on Ieft. astinum into two equa1 parts. Notice its crossing of arch of aorta. BeIow arch, trachea is in front of descending aorta.
bounded in front by the sternum. The posterior part is behind the trachea and is bounded behind by the dorsaI vertebrae. The width of the trachea varies with the age and habitus of the individua1. It is usuaIIy wider in broad-chested individuals and narrower in individuaIs of sIender buiId. OccasionaIIy the trachea1 rings are readiIy made out. The course of the trachea from above downward is usuaIIy straight with a slight in&nation toward the spine. Above, the trachea is con- tinuous with the cervicaI portion through the superior aperture of the thorax. BeIow, the trachea is crossed on the Ieft side by the arch of the aorta and beIow the arch by the puImonary artery. These vesseIs obscure the trachea to a greater or Iesser degree depending upon the con- dition of their waIIs. In case of diIatation of the aorta the trachea may be found dis- pIaced to the right. This is best observed in the anteroposterior view. BeIow the
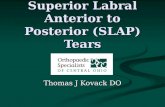
FIG. 2. LateraI view. EsophageaI diverticulum dis- pIacing trachea forward.
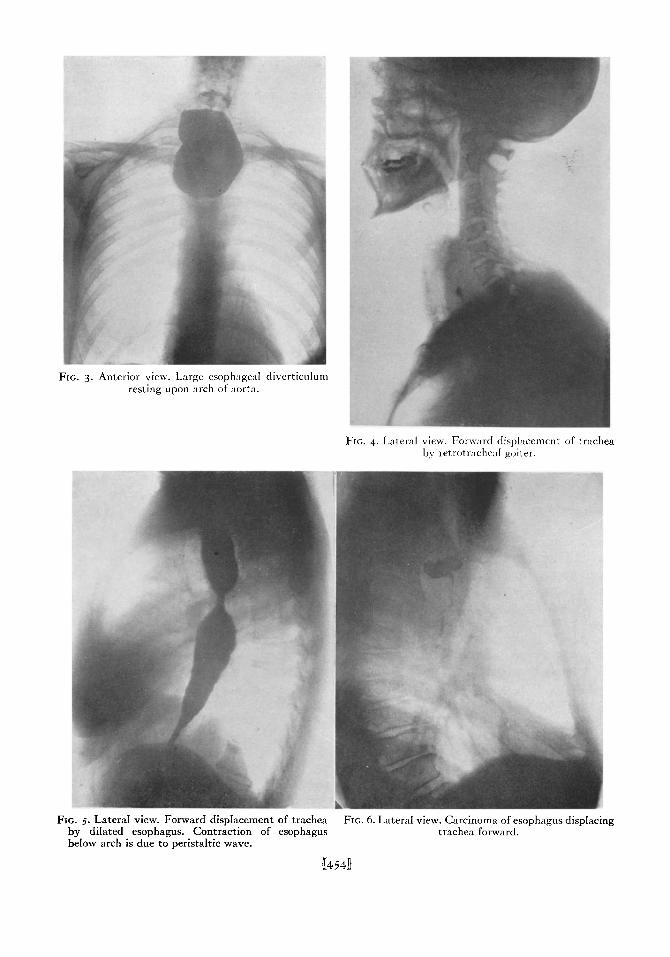
FIG. 3. Anterior view. Large esophageal divcrticuIum resting upon arch of aorta.
FIG. 4. Lateral view. Forward disphtcemcnt of trachea by retrotrache:d goiter.
FIG. 5. LateraI view. Forward dispIacement of trachea FIG. 6. LateraI view. Carcinoma of esophagus dispIacir by diIated esophagus. Contraction of esophagus trachea forward. below arch is due to peristaltic wave.
‘g
u454ll

NEW SERIES VOL. X, No. 3 Brown & Reinecke-Mediastinum American Journal of Surgery 455
of the trachea and above the arch of the aorta there is an area of reIatively greater density. Its course is paraIle1 to the trachea and its width is about the same as that of the trachea and is due to the blood vesseIs arising from the aorta and the veins entering the heart. In front of this area the region is more transparent, which is due to the apices of the Iungs.
Under abnorma1 conditions the trachea is often found to be dispIaced forward as a result of the presence of esophagea1 divertic- ula (Figs. 2, 3). Retrotracheal goiter can onIy be recognized in the IateraI view (Fig. 4) by showing the forward displacement of the trachea. In the anterior view it is impossibIe to determine its true position. The knowIedge of the true positidn of a goiter enabIes the surgeon to pIan the operation accordingIy. Forward dispIace- ment of the trachea may resuIt from diIatation of the esophagus (Fig. 5), but this is usuaIIy of a temporary nature and depends upon the presence of food above the obstruction. However, there may be permanent dispIacement as a resuIt of a Iarge tumor of the esophagus (Fig. 6). The distance between the spine and trachea indicates the size of the tumor. In this case the waIIs of the trachea are not involved but onIy dispIaced. OccasionaIIy, in addition to the forward dispIacement there is aIso narrowing of the Iumen of the trachea as we11 as distortion of its waI1 (Fig. 7). The subject of this illustration complained more of dyspnea than of dysphagia. An interesting case of forward dispIacement of the trachea as a resuIt of retrotrachea1 tumor due to metastasis is represented by Figure 8. This patient com- pIained of difFicuIty in breathing. The anterior view faiIed to show anything abnorma1 in the chest. The IateraI view immediateIy determined the true cause of the diffIcuIty.
Fistulous communication between the trachea and esophagus is best demon- strated in the IateraI view as shown in a case of carcinoma of the esophagus iIIus- trated in Figure g. The greatest usefuIness
of the IateraI view, we find, is in cases of aneurysm. As a rule an aneurysm is repre- sented by a dense shadow in the anterior
FIG. 7. Lateral view. Carcinoma of esophagus with forward dispIacement of trachea and distortion of posterior ~111 of trachea.
view of the superior mediastinum. Its exact origin and its reIation to the other mediastina1 structures are impossibIe to determine in this view aIone. However, by studying both the anterior and IateraI views it is possibIe to come to a definite concIusion. The anterior view (Fig. IO A)
shows a Iarge circumscribed shadow above the arch of the aorta. In the IateraI view (Fig. IO B) the shadow occupies the pos- terior portion of the superior mediastinum. The trachea is dispIaced forward. EvidentIy the aneurysm is originating from that part of the aorta which is behind the trachea, nameIy, the upper end of the descending aorta. Postmortem examination of this case confirmed the x-ray finding. The next case (Figs. I I A and B) is just the opposite. The anterior view aIso shows a dense shadow occupying the superior medias- tinum, but the IateraI view reveals pos- terior dispIacement of the trachea with the

FIG. 8. LateraI view. Forward dispkement of trachea FIG. g. LateraI view. Tracheoesophageal fist&. and depression of esophagus by metastatic tumor in superior mediastinum.
FIG. IO A. Anterior view. Large circumscribed shadow FIG. IO B. LateraI view. Shadow is behind trachea, which occupying region of superior mediastinum. is displaced forward. EvidentIy, if an aneurysm, it
must originate from posterior end of arch or descend- ing aorta. Postmortem examination confirmed this finding.
tK456ll

FIG. I I A. Anterior view. Large shadow occupying FIG. I I B. Lateral view. Shadow is in front of trachea. region of superior mediastinum. Latter is dispIaced backwards. EvidentIy, if an
aneurysm, it must originate from ascending aorta.
FIG. 12 A. Anterior view. Aorta shows moderate FIG. 12 B. LateraI view. DiIatation of arch is confined diIatation of arch. to inferior surface. Trachea is depressed and dis-
pIaced forward. Confirmed by postmortem.
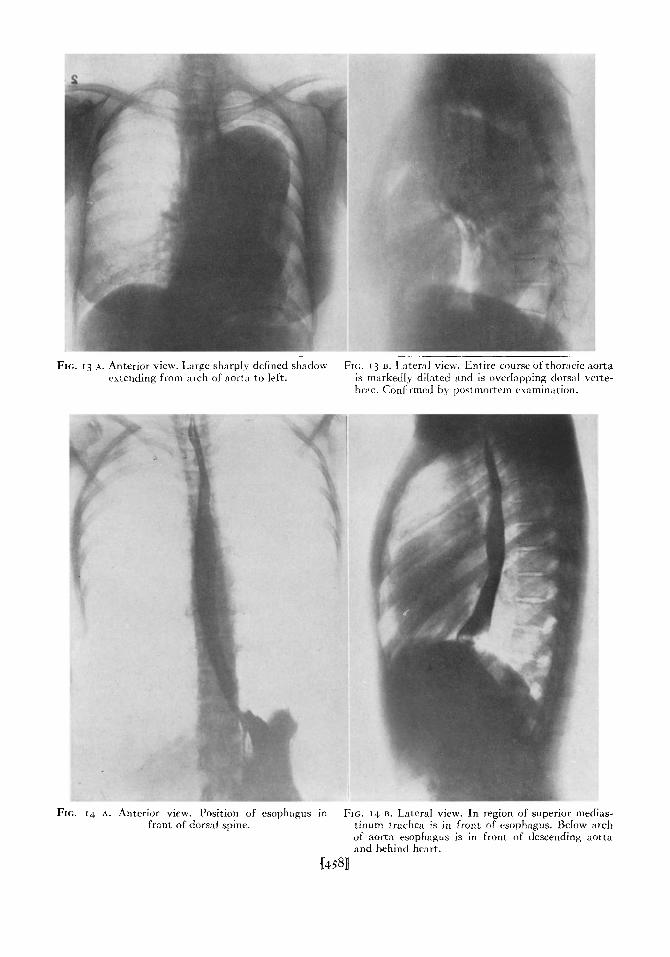
FIG. r3 A. Anterior view. Large sharpIy defined shadox FIG. 13 u. Lateral view. Entire course of thoracic aorta extending from arch of aorta to Ieft. is m:~rkedIy dilated and is ovcrhlpping dorsal verte-
hrx. Confirmed by postmortem examination.
FIG. rh A. Anterior view. Position of esophagus in FIG. 14 B. Lateral view. In region of superior medias- front of dors:d spine. tinum trachea is in front of esophagus. BeIow arch
of aorta esophagus is in front of descending aorta and behind heart.
U493D

FIG. 15. LateraI view. Upper end of esophagus is FIG. 16. Lateral view. Compression of esophagus as displaced forward by enlarged gland. result of enlarged heart.
FIG. 17. Lateral view. Compression of lower end of FIG. 18. LateraI view. Esophageal distortion as resu esophagus by left ventricuIar hypertrophy. of diaphragmatic hernia.
%4594
It

FIG. 19. LateraI view. Esophageal perforation into posterior mediastina1 structures due to carcinoma.
FIG. 20. Lateral view. Benign esophageal stricture in woman, aged twenty-four. No history of injury. Esophagoscopic examination and subsequent treat- ment confirmed benign nature of lesion.
FIG. 21. Lateral view. Esophageal stricture at cardiac FIG. zz. Lateral view. Carcinoma of esophagus below end of esophagus. Benign in origin. Transparent area middIe third. is due to pIug of food.
U4Wl

NEW SERIES VOL. X, No. 3 Brown & Reinecke-Mediastinum American journal of surgery 461
density occupying the anterior haIf of the superior mediastinum. EvidentIy its origin must be the ascending or anterior portion of the arch. In this case it appears that we are deaIing with two aneurysms as shown in the IateraI view. One is arising from the ascending portion and the other from the transverse arch. The dispIacement of the arch downward and backward is shown quite distinctIy. Aneurysms may aIso arise from the concave or inferior aspect of the arch of the aorta. This is again best shown in the IateraI view (Figs. 12 A and B).
The anterior view shows a slight diIatation of the aorta on the left side beyond the arch. In the Iateral view there is shown a buIging arising from the inferior surface of the arch which depresses the anterior wall of the trachea and the Ieft bronchus. This partia1 obstruction resuIted in a bronchiectasis. AI1 the x-ray findings were confirmed by postmortem examination. An extreme case of marked dilatation of the aorta is iIIustrated in Figures 13 A and B. The IateraI view shows that diIatation invoIves the whoIe of the thoracic aorta. The Ieft bronchus is dispIaced downward and forward by the marked buIging of the concave surface of the arch.
Behind the trachea and paraIIe1 to it is the esophagus (Figs. 14 A and B) which cannot be recognized unIess it is rendered visibIe by an opaque medium. The course of the esophagus from above downward is aImost straight. Above, it is continuous with the cervica1 portion of the esophagus through the superior aperture of the thorax. Throughout its whoIe course it is in front of the spine with the exception of its Iower extremity which deviates toward the Ieft before it passes through the esophagea1 orifice in the diaphragm. In the region of the superior mediastinum it is in front of the bodies of the dorsa1 vertebrae. In the region of the posterior mediastinum the esophagus is behind the pericardium and in front of the descending aorta. It is never found to rest against the spine under normaI conditions notwithstanding the
teachings of severa anatomists to the contrary. The esophagus is crossed by the arch of the aorta on the left side. In
FIG. 23. LateraI view. Carcinoma of cardiac end of esophagus on posterior wal1.
this region its contour is often found to be depressed by the arch of the aorta.
Under abnorma1 conditions the esopha- gus may be found to be displaced as shown in Figure 15, where the dispIacement is forward and is due to enIarged trachea1 gIands. Depression of the anterior waI1 of the esophagus as a resuIt of cardiac enIarge- ment is shown in Figure 16. LocaIized depression by enIargement of the Ieft ventricIe is shown in Figure 17. The esoph- agus is occasionaIIy found to have a zigzag and distorted appearance when associated with a diaphragmatic hernia as shown in Figure 18. Perforation of the esophagus with extravasation of opaque medium into the mediastina1 tissues is best iIIustrated in the IateraI view (Fig. 19). This was primariIy due to a carcinoma. CicatriciaI strictures are aIso best shown

;. 24 A. Diaphragmatic hernia through esophageal FIG. 24 D. EsophagenI divcrticuIum of Iower end of orifice. esophagus.
:G. 25. LateraI view. SmaII diverticuIum of cardiac end of esophagus.
FIG. 26. Anterior view. Cardiospasm. Fundus stomach is normal.
U462ll

FIG. 28. Anterior view. Deviation of cardiac end of esophagus to Ieft as resuIt of maIignant growth. Confirmed by operation.
FIG. 27. Anterior view. MaIignant tumor of stomach encroaching upon cardiac end of stomach, thus producing obstruction of esophagus. Appearance cIoseIy resembIes simpIe spasm.
FIG. 2g A. Anterior view. Displacement of descending FIG. 2g B. Lateral view. Aorta is seen to overIap doa aorta to Ieft due to diIatation. vertebrae.
U463ll

464 Amcric,tn Journal of Surgery Brown & Reinecke-Mediastinum 1>EcnMmEn, ,030
in the IateraI view. Figure 20 shows a stricture in the middle of the esophagus. Figure 21 shows a stricture at the cardiac
FIG. 30. Ant&x view. Displnccmcnt of lower end of esophagus to left due to aneurysm of descending aorta.
end of the esophagus due to a caustic burn. EvidentIy the cIear space between the opaque medium and cardiac end is due to ingested food which faiIed to pass the narrow opening of the stricture. MaIignant strictures or deformities in the contour of the esophagus can also be demonstrated in the IateraI view to their greatest advantage. Figure 22 shows deformity of the esophagus beIow its upper haIf. Figure 23 shows a deformity of the posterior waI1 of the esophagus at the cardiac end. Diver- ticuIi of the Iower end of the esophagus can readiIy be demonstrated in the ante& posterior or IateraI views. The differen- tiation between a diverticulum of the Iower end of the esophagus and a dia- phragmatic hernia through the esophagea1 orifice is often difflcuIt to make. A carefu1
study of the severa characteristics associ- ated with diverticuIa and diaphragmatic hernia has helped us in arriving to a correct diagnosis. Diaphragmatic hernia (Fig. 24
A) through the esophagea1 orifice presents the foIIowing differentia1 points:
I. The part of the stomach above the diaphragm consists of the fundus and cardiac end of the stomach.
2. The expansion of the hernia1 sac is equaIIy distributed on both sides of the spine.
3. The size of the hernia varies with the position of the patient. It is Iarger in the prone and smaIIer in the erect position.
4. The fundus is absent in the left hypochondriac region.
5. The stomach beIow the diaphragm is smaI1.
EsophageaI diverticuIum of the Iower end of the esophagus (Fig. 24 B) presents the foIIowing points :
I. The sac arises and communicates with the esophagus.
2. The sac is found to be Iocated to one side of the spine.
3. The size of the sac remains the same in any position.
4. The fundus of the stomach is found in the region of the Ieft hypochondrium.
5. The stomach is of normaI size and shape.
Figure 25 shows a smaI1 diverticuIum which was best shown in the IateraI view. Cardiospasm of the esophagus shouId aIways in&de, if possibIe, an examination of the stomach in order to excIude a lesion of this organ. In the demonstrations of cardiospasm there is no specia1 advantage in taking a IateraI view. An anterior view (Fig. 26) wiI1 show the existing condition without any diffIcuIty. Figure 27 to a11 appearances resembIes a typica case of cardiospasm. However, a study of the stomach wiI1 show that the Iumen is encroached upon by a mass which extends toward the cardiac end producing an organic obstruction. The position of the cardiac end of the stomach shouId aIways be watched. Any marked deviation from

FIG. 31 A. Anterior view. Dense shadow on left side FIG. 31 B. LateraI view. Anterior and posterior medi- of heart in case of Hodgkin’s disease. Contirmed by astina1 gIands are enlarged. biopsy.
FIG. 32 A. Anterior view. Heart is displaced to left FIG. 32 B. LateraI view. Region beIow arch of aorta is and superimposed upon heart shadow is another obscured by dense shadow. Diagnosis of tumor of shadow presumed to be aorta. posterior mediastinum was confirmed by postmortem
examination.
646433
FI (12. 33 *. LateraI view. Ovoid transparent area is FIG. 33 B. LnteraI view. After barium injection tra seen to be located between he:trt :md aorta. parent shadow proved to be due to diaphragma
hernia.
IIS-
rtic
FIG. 34 A. Anterior view. Dense shadow on right side FIG. 34 B. LateraI view. Spinal tuberculosis with abscess of heart. extending into posterior mediastinum.

NEW SERIES VOL. X. No. J Brown & Reinecke-Mediastinum American journal O( surgery 467
the normaI shouId Iead one to suspect the of the traches more or Iess prevents dis- possibiIity of an organic Iesion (Fig. 28). pIacement to this side. Figure 29 A shows The x-ray diagnosis of carcinoma of the marked dispIacement of the descending
FIG. 35 A. Anterior view. Dense shadow on right side of heart.
esophagus was confirmed by operation in this case.
The descending aorta is Iocated in front of the spine. Under norma conditions but very Iittle of it is seen in the antero- posterior view. Wh enever the aorta is observed in the anteroposterior view it is either diIated or dislocated. In the IateraI view its whoIe course can readiIy be seen in most individuaIs. Above, it is continuous with the arch of the aorta. BeIow, it is Iost from view below the diaphragm. In its downward course is foIIows the dorsa1 spine very closely. A deviation in the course of the spine wiII reflect upon the course of the aorta. Whenever the aorta is found to over-rap the bodies of the dorsa1 vertebrae in a true Iateral view it is either displaced or dilated. Deviation of the aorta usuahy takes place to the Ieft side, since this is the point of Ieast resist- ance. On the right side the firm structure
FIG. 35 B. Lateral view. Tuherculous abscess originating from spine.
aorta to the Ieft. Figure 29 B shows the IateraI view with the descending aorta overIapping the entire dorsal spine. An aneurysm arising from the descending aorta is best demonstrated with an opaque medium in the esophagus. The dispIace- ment of the lower end of the esophagus to the Ieft in Figure 30 was due to an aneurysm.
Demonstration of enIarged gIands or tumors in the posterior mediastinum is greatIy assisted by Iateral views. Figures 31 A and B show a case of Hodgkin’s disease. Figures 32 A and B show a case of Iymphosarcoma. Postmortem examination confirmed the x-ray findings. A rather unusua1 transparent shadow Located be- tween the posterior surface of the peri- cardium and the descending aorta (Figs. 33 A, B) proved to be due to a diaphrag- matic hernia. It is needIess to say that the anterior view failed to show anything abnorma1. Occasionahy abnorma1 shadows

468 A m&can Journal of Surgery Brown & Reinecke-Mediastinum DECEMBER. ,930
in the neighborhood of the posterior mediastinum cannot be expIained unIess a study of the thorax is made in the IateraI position. Figures 34 A and B and Figures 35 A and B show the exact nature of the shadows to be due to tubercuIous spinal abscesses and that they are only encroach- ing upon the mediastinum, not originating from it.
CONCLUSIONS
I. A study of the superior and posterior mediastinum shouId incIude both an antero- posterior and IateraI views.
2. The advantages of the IateraI view over the anteroposterior view are shown by many iIIustrations.
3. The latera view enables one to deter-
mine the position of the trachea in reIation to the thoracic waIIs. Any deviation from its norma course and the probabIe cause can be determined with a high degree of accuracy.
4. The origin of aneurysms can be accurateIy determined by studying the Iocation of the aneurysm in reIation to the trachea.
5. Lesions affecting the esophagus can be studied with greater advantage in the IateraI view.
6. AbnormaI changes in the descending aorta are best recognized in the IateraI view.
7. The exact origin of abnorma1 shadows encroaching upon the mediastina can be determined in the IateraI view.
REFERENCES OF DR. DE VRIES*
I. DUFFIELD, W. L. New York State J. Med., 8: 20, 7. PRIMROSE. J. A. M. A. 75: 12-16, Igzo.
‘909. 2. ALBRECT, quoted by DuffxeId.
8. GRAWITZ. V&bows Arch. f. patb. Anat., gz: 39,
3. KEYES. Urology. N. Y., AppIeton, 1923. 1883.
4. EISENDRATH. Surg. Gynec. Obst., 13: 467-474, 1912. 9. STOERK. Bed. klin. Wcbnscbr., 16: 773, 1908. 5. BUGBEE. J. Ural., 5: no. 4. 1921. IO. FRASER. Surg. Gynec. Obst., 23: 645-656, rgr6. 6. WELLS. Arch. Surg., 356-365, 5: 1922. I I. MORRIS. Human Anatomy. PhiIa., BIakiston, 1925.
* Continued from p. 492.