
Rocky Mountain Spotted Fever. Rocky Mountain Spotted Fever: First recognized in 1896 in the Snake...
19
Rocky Mountain Rocky Mountain Spotted Fever Spotted Fever
-
Upload
josephine-hutchinson -
Category
Documents
-
view
216 -
download
0
Transcript of Rocky Mountain Spotted Fever. Rocky Mountain Spotted Fever: First recognized in 1896 in the Snake...

Rocky Mountain Rocky Mountain Spotted FeverSpotted Fever

Rocky Mountain Spotted Rocky Mountain Spotted Fever:Fever:
First recognized in 1896 in the Snake River First recognized in 1896 in the Snake River Valley of Idaho and was originally called Valley of Idaho and was originally called "black measles" because of the "black measles" because of the characteristic rash.characteristic rash.
Howard T. Ricketts established the identity Howard T. Ricketts established the identity of the infectious organism that of the infectious organism that causes this disease, causes this disease, Rickettsia Rickettsia rickettsii. rickettsii.
He and others described the He and others described the epidemiologic features of the disease, epidemiologic features of the disease, including the role of tick vectors. including the role of tick vectors.
Sadly, Dr. Ricketts died of typhus (another Sadly, Dr. Ricketts died of typhus (another rickettsial disease) in Mexico in 1910. rickettsial disease) in Mexico in 1910.

Epidemiology:Epidemiology:
A bit of a misnomer, this disease has A bit of a misnomer, this disease has been identified in almost all of the been identified in almost all of the continental US, with perhaps the continental US, with perhaps the exception of Maine and Vermontexception of Maine and Vermont Most cases reported in south Atlantic, Most cases reported in south Atlantic,
southeastern and south central statessoutheastern and south central states 54% of cases were from NC, TN, OK, SC 54% of cases were from NC, TN, OK, SC
and Arkand Ark


Transmission:Transmission:
Vector=tickVector=tick Wood tick, dog tick and Lone Star tickWood tick, dog tick and Lone Star tick
Both dog and Lone Star ticks are found in Both dog and Lone Star ticks are found in NCNC
Wood tick is primarily in western US, and Wood tick is primarily in western US, and Rocky Mountain areaRocky Mountain area
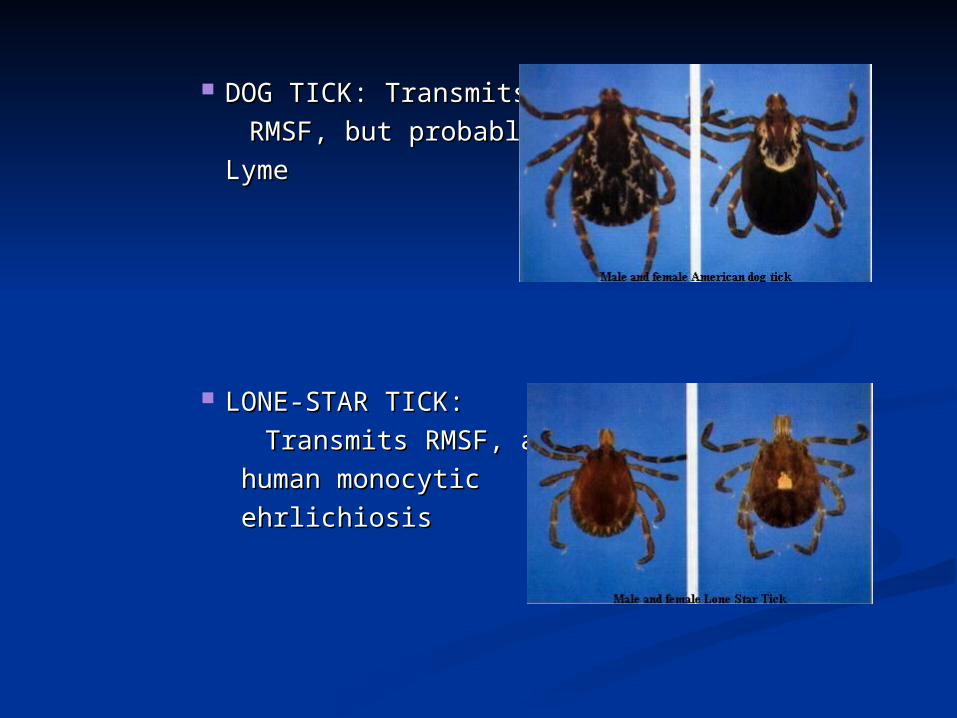
DOG TICK: Transmits DOG TICK: Transmits
RMSF, but probably not RMSF, but probably not
LymeLyme
LONE-STAR TICK:LONE-STAR TICK:
Transmits RMSF, andTransmits RMSF, and
human monocytichuman monocytic
ehrlichiosisehrlichiosis

Two-thirds of RMSF cases occur in Two-thirds of RMSF cases occur in children younger than 15 yearschildren younger than 15 years
Males are infected more commonly Males are infected more commonly (1.7-2.2:1)(1.7-2.2:1)
Caucasians are more common than Caucasians are more common than African-AmericansAfrican-Americans
Peak months of infection are April-Peak months of infection are April-OctoberOctober


R. rickettsii organisms are released R. rickettsii organisms are released through saliva during a feedingthrough saliva during a feeding Usually 12-24 hrs of attachment is Usually 12-24 hrs of attachment is
requiredrequired Incubation period is 2-14 daysIncubation period is 2-14 days Once organisms enter the body, they Once organisms enter the body, they
multiply within endothelial cell multiply within endothelial cell linings of small blood vessels linings of small blood vessels

Signs and Symptoms:Signs and Symptoms: EARLY:EARLY:
Fever, nausea, vomiting, severe headache, Fever, nausea, vomiting, severe headache, anorexia and malaiseanorexia and malaise
LATE:LATE: Rash, joint pain and diarrheaRash, joint pain and diarrhea
Classic triad=fever, rash and headacheClassic triad=fever, rash and headache Rash: appears between day 2 to 5 of illnessRash: appears between day 2 to 5 of illness
Blanching, erythematous macules arouond Blanching, erythematous macules arouond ankles feet, later wrists and hands; palms and ankles feet, later wrists and hands; palms and soles often involvedsoles often involved
Petechiae on day 6Petechiae on day 6 10-15% of infected patients are without rash10-15% of infected patients are without rash



Important points:Important points:
Only 40-60% of those infected have a Only 40-60% of those infected have a history of tick bitehistory of tick bite
RMSF may be clinically RMSF may be clinically indisginguishable from Human indisginguishable from Human Monocytic ehrlichiosis Monocytic ehrlichiosis

Laboratory tests:Laboratory tests:
Hyponatremia (20%)Hyponatremia (20%) Thrombocytopenia (33%)Thrombocytopenia (33%) Anemia, increased LFTs or BUN Anemia, increased LFTs or BUN
(25%)(25%) CSF: monocytic pleocytosis, CSF: monocytic pleocytosis,
increased proteinincreased protein

Diagnosis:Diagnosis:
Largely clinicalLargely clinical Suspect if classic triadSuspect if classic triad Acute and convalescent titers (> 3 wks Acute and convalescent titers (> 3 wks
apart)apart) Immunofluorescence assayImmunofluorescence assay PCRPCR Isolation of Isolation of R rickettsiiR rickettsii from clinical from clinical
specimenspecimen

Treatment:Treatment:
Should be started immediatelyShould be started immediately Doxycycline, usually 7-10 daysDoxycycline, usually 7-10 days
100 mg PO BID for adults100 mg PO BID for adults 4 mg/kg/day div BID for children4 mg/kg/day div BID for children Discontinue 72 hrs after defervescenceDiscontinue 72 hrs after defervescence Teeth staining if < 9 years old; probably Teeth staining if < 9 years old; probably
requires 5-6 courses before staining requires 5-6 courses before staining appearsappears

Prevention:Prevention: Protective clothingProtective clothing RepellantsRepellants
Avoid DEET if under 12 monthsAvoid DEET if under 12 months Full body examinationsFull body examinations

To remove attached ticks, use the following procedure:To remove attached ticks, use the following procedure: 1. Use fine-tipped tweezers or shield your fingers with a tissue, paper towel, 1. Use fine-tipped tweezers or shield your fingers with a tissue, paper towel,
or rubber gloves (Figure 17). When possible, persons should avoid removing or rubber gloves (Figure 17). When possible, persons should avoid removing ticks with bare hands. ticks with bare hands.
2. Grasp the tick as close to the skin surface as possible and pull upward 2. Grasp the tick as close to the skin surface as possible and pull upward with steady, even pressure (Figure 18). Do not twist or jerk the tick; this may with steady, even pressure (Figure 18). Do not twist or jerk the tick; this may cause the mouthparts to break off and remain in the skin. cause the mouthparts to break off and remain in the skin. (If this happens, (If this happens, remove mouthparts with tweezers. Consult your health care provider if remove mouthparts with tweezers. Consult your health care provider if infection occurs.)infection occurs.)
3. Do not squeeze, crush, or puncture the body of the tick because its fluids 3. Do not squeeze, crush, or puncture the body of the tick because its fluids (saliva, body fluids, gut contents) may contain infectious organisms.(saliva, body fluids, gut contents) may contain infectious organisms.
4. After removing the tick, thoroughly disinfect the bite site and wash your 4. After removing the tick, thoroughly disinfect the bite site and wash your hands with soap and water.hands with soap and water.
5. Save the tick for identification in case you become ill. This may help your 5. Save the tick for identification in case you become ill. This may help your doctor make an accurate diagnosis. Place the tick in a plastic bag and put it doctor make an accurate diagnosis. Place the tick in a plastic bag and put it in your freezer. Write the date of the bite on a piece of paper with a pencil in your freezer. Write the date of the bite on a piece of paper with a pencil and place it in the bag.and place it in the bag.

Resources:Resources:
Center for Disease Control and Center for Disease Control and Prevention. Rocky Mountain spotted Prevention. Rocky Mountain spotted fever. Available at: fever. Available at: http://www.cdc.gov/ncidod/dvrd/rmsfhttp://www.cdc.gov/ncidod/dvrd/rmsf
Pickering, L. Red Book; 26Pickering, L. Red Book; 26thth edition. pp. edition. pp. 532-534.532-534.
Razzaq, S. Rocky Mountain Spotted Razzaq, S. Rocky Mountain Spotted Fever: A Physician’s Challenge. Fever: A Physician’s Challenge. Pediatrics in Review. Vol. 26, No. 4 April Pediatrics in Review. Vol. 26, No. 4 April 2005. pp. 125-129.2005. pp. 125-129.


















