Roche Translating excellence in science into customer benefit249e4cde-cb09-4d49... · Roche...
39
Roche Translating excellence in science into customer benefit Cheuvreux Pan Europe Forum, London May 16, 2011 Dr. Stefan Frings, Global Head Medical Affairs Oncology Dr. Karl Mahler, Head of Investor Relations
Transcript of Roche Translating excellence in science into customer benefit249e4cde-cb09-4d49... · Roche...

RocheTranslating excellence in science into customer benefit
Cheuvreux Pan Europe Forum, LondonMay 16, 2011
Dr. Stefan Frings, Global Head Medical Affairs OncologyDr. Karl Mahler, Head of Investor Relations

2
This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as ‘believes’, ‘expects’, ‘anticipates’, ‘projects’, ‘intends’, ‘should’, ‘seeks’, ‘estimates’, ‘future’ or similar expressions or by discussion of, among other things, strategy, goals, plans or intentions. Various factors may cause actual results to differ materially in the future from those reflected in forward-looking statements contained in this presentation, among others:
1 pricing and product initiatives of competitors;2 legislative and regulatory developments and economic conditions; 3 delay or inability in obtaining regulatory approvals or bringing products to market; 4 fluctuations in currency exchange rates and general financial market conditions; 5 uncertainties in the discovery, development or marketing of new products or new uses of existing products,
including without limitation negative results of clinical trials or research projects, unexpected side-effects of pipeline or marketed products;
6 increased government pricing pressures; 7 interruptions in production 8 loss of or inability to obtain adequate protection for intellectual property rights; 9 litigation;10 loss of key executives or other employees; and11 adverse publicity and news coverage.
Any statements regarding earnings per share growth is not a profit forecast and should not be interpreted to mean that Roche’s earnings or earnings per share for this year or any subsequent period will necessarily match or exceed the historical published earnings or earnings per share of Roche.
For marketed products discussed in this presentation, please see full prescribing information on our website –www.roche.com
All mentioned trademarks are legally protected

3
Performance update and strategy
Update on oncology portfolio
Summary and short term news flow

4
Pharmaceuticals Division 9,727 8,712 -10 -2 +1
Diagnostics Division 2,518 2,408 -4 +6 +6
Roche Group 12,245 11,120 -9 0 +2
2010 2011 ExcludingCHF m CHF m CHF local Tamiflu1
change in %
Q1 2011: Group sales Supporting full-year guidance, strong currency impact
1 local currency

5
Roche: Focused on medically differentiated therapies
Generics
Differentiation
Focus
MedTech
OTC
Prem
ium
for
inno
vatio
n
DiaPharma

6
Key Pharmaceuticals & Diagnostics productsA risk-diversified portfolio of drugs and BUs
Sale
s (C
HF
bn)
* 2010 sales
0
5
10
15
20
25
30
35
'03 '04 '05 '06 '07 '08 '09 '10
2 with > than CHF 6 bn
1 with > than CHF 5 bn
11 with > than CHF 1 bn
MabThera/Rituxan
Xeloda
NeoRecormonCellCept
Herceptin
Avastin
Pegasys
Clinical Chemistry
Immunochemistry
Tarceva
Lucentis
>C
HF
6bn*
>C
HF
1bn*
>C
HF
5bn*
Diabetes Care
Molecular DxBoniva

7% Sales Lost calculated by subtracting given year sales (‘10, ’11, ‘12, ‘13) from full year sales from year prior to LOE.Data excludes sales lost impact of products with LOE prior to 2010.Source: Evaluate Pharma
Roche: Limited exposure to patent expiries in the short and medium term
40%
35%
30%
25%
0%
20%
10%
15%
5%
2010 2011 2012 2013
Business impact from biosimilars 2014/15 and beyond?

8
Long patent protection Biosimilars facing high hurdles
Long primary patent protection of our key biologics
Patents US EUROW/EM
Avastin 2019 similar
Lucentis 2019 marketed by Novartis
Rituxan/ MabThera 2018 earlier
Herceptin 2019 earlier
Pegasys 2018 similar
Biosimilars outlook
US: recent healthcare legislation opens pathway for biosimilars
FDA in the process of developing guidelines
Data exclusivity for biologics 12 years
ROW/EM: investment in countries with strong IP regulations (China)
Brand awareness important
EU: legal and regulatory hurdles likely to remain high for biosimilars

99
A leading pipeline12 NMEs in late-stage development
2007 2008 2009 2010
Number of NMEs
2
4
10Metabolic
Oncology
Inflammation
ocrelizumab
dalcetrapib
pertuzumab
taspoglutide
Actemra
CNS
ocrelizumab
12Virology
1 LIP decision made, phase III start pending
dalcetrapib
aleglitazar
Glycine reuptake inh
ocrelizumab MS
lebrikizumab1
HCV pol inh1
pertuzumab
BRAF inhibitor
T-DM1
Hedgehog inh
GA101(CLL, NHL)
MetMAb1
dalcetrapib
aleglitazar
Glycine reuptake inh
ocrelizumab
pertuzumab
BRAF inhibitor
T-DM1
Hedgehog inh
GA101 (CLL)
taspoglutide

1010
Creating medical value and improving patient care Six NMEs in late-stage development have PHC approach
NMEs = new molecular entities PHC = Personalised HealthcareNot all products available in all countries; some products in development
Periostin(lebrikizumab)
BRAF V600(BRAF inh)
HER2(T-DM1)
HCV load, genotype(HCV pol inh)
Met(MetMAb)
HER2/3(Pertuzumab)
Diagnostics
Companion Diagnostics

We need to stay above industry success rates
11
Success (+) Failure (-)
2008 2009 2010 2011 (Jan-Mar)
(+) (-) (+) (-) (+) (-) (+) (-)
Phase II 6 6 7 1
Phase III 21 2 20 1 10 6 4 0
Total 27 2 26 1 17 6 5 0
Ph III success rate 91% 95% 62% 100%
Based on IR up-dates
Industry ph III success rate 63%1 64%2
Roche
KMR Group, 1)= 2006-2008, 2)= 2007- 2009,

Key clinical trials since October 2010 18 positive studies in 6 months
12
Compound Indication StudyMetMAb 2nd/3rd line NSCLC Randomised Phase II, ESMO 2010
Avastin front line Ovarian Cancer ICON7 Phase III, ESMO 2010
Ocrelizumab RR Multiple Sclerosis Randomised Phase II, ECTRIMS 2010
Mericitabine (RG7128) Hepatitis C PROPEL randomised Phase IIb, interim data AASLD 2010
Vemurafenib (BRAF inh) Metastatic Melanoma BRIM2 Phase II, Melanoma Research Congress 2010
GA101 Non-Hodgkin's Lymphoma Randomised Phase II, ASH 2010
Glycine Reuptake inh. (GlyT-1) Schizophrenia Randomised Phase II, ACNP 2010
Pertuzumab Neoadjuvant HER2+ Breast Cancer NEOSPHERE randomised Phase II, SABCS 2010
Lebrikizumab Asthma Randomised Phase II, data in house
Dalcetrapib CV risk reduction Dal-VESSEL, Dal-PLAQUE safety data in house
T-DM1 1st line HER2-positive breast cancer Randomised Phase II, Apr 2011
Vemurafenib (BRAF inh) Metastatic Melanoma BRIM3 Phase III interim analysis, Jan 2011
Tarceva Advanced NSCLC EURTAC Phase III interim analysis, Jan 2011
Avastin Relapsed Ovarian Cancer OCEANS Phase III, Feb 2011
Lucentis Diabetic macular edema (DME) RISE and RIDE, 2 Phase III studies, Feb-Mar 2011
Vismodegib (Hedgehog inh) Basal Cell Carcinoma (mBCC) Pivotal Phase II, Mar 2011
Pivotal studies in Q1 2011

13
Performance update and strategy
Update on oncology portfolio
Summary and short term news flow

14
Managing franchisesAdding benefits to key medicines; developing better ones
GA101MabThera/Rituxan MabT/Rituxan s.c.Anti-CD20oncology
T-DM1pertuzumabHerceptin Herceptin s.c.Anti-HER2
Avastin anti-PIGF anti-EGFL7Anti-angiogenesis

15
Roche Group Pipeline today
Status as of March 31, 2011
phase I (36 NMEs)
phase II (18 NMEs + 8 Als)
phase III(8 NMEs + 27 Als)
Registration(6 Als)
NMEAdditional Indication
OncologyInflammation/ImmunologyVirologyMetabolic/CardiovascularCNSOphthalmologyOthers
RG-No Roche Genentech managedCHU Chugai managedEVO Evotec
RG105 MabThera is branded as Rituxan in US and Japan
RG1569 Actemra is branded as RoActemra in EU
* submitted in the EU** submitted in the US
anti-glypican Mab liver cancerRG7686
Mab Beta7 ulcerative colitisRG7413
anti-factor D Mab geographic atrophyRG7417
mGluR2 antag (2) depressionRG1578
anti-Abeta Mab Alzheimer‘sRG7412triple reuptake inh depressionRG7166
ABCA1 inducer dyslipidemiaRG7273
anti-oxLDL Mab sec prev CV eventsRG7418
GABA-A a5 inv ago cogn. disordersRG1662
anti-IL-17 Mab RARG4934
EGFR Mab solid tumorsRG7160CIF/MEK inh solid tumorsRG7167Raf & MEK dual inh solid tumorsRG7304
anti-PLGF Mab solid tumorsRG7334
MDM2 ant (2) solid & hem tumorsRG7112
MEK inh solid tumorsRG7420
PI3 K/mTOR inh solid & hem tumorsRG7422
PI3 kinase inh solid tumorsRG7321
anti-EGFL7 Mab solid tumorsRG7414
dulanermin cancerRG3639
AKT inhibitor solid tumorsRG7440
MEK inh solid tumorsRG7421
CD22 Mab ADC hem. malignanciesRG7593
CRTH2 antag asthmaRG7185
BRaf inh(2) BRAF mut. melanoma RG7256
nucleoside pol inh (9) HCVRG7432
anti-Her3 Mab m. epithelial tumorsRG7597
antiangiogenic solid tumorsRG7594
IAP ant (2) solid tum & lymphomaRG7459
FGFR3 Mab multiple myelomaRG7444
Cat S antag CV risk in CKD RG7236
GIP/GLP-1 dual ago type 2 diabetesRG7685
ALK inhibitor NSCLCCHU- solid tumorsCHU
vismodegib operable BCCRG3616MetMab mNSCLCRG3638
pertuzumab HER2+ EBC RG1273
vismodegib advanced BBCRG3616
topoisomerase I inh gastric cancerCHUnavitoclax (ABT-263) sol & hem tumRG7433
oxelumab (OX40L Mab) asthmaRG4930lebrikizumab (anti-IL13) asthmaRG3637
rontalizumab (IFN alpha Mab) SLERG7415
mericitabine (polymerase inh) HCVRG7128 danoprevir (protease inh) HCVRG7227
mGluR5 antag (2) TRDRG7090NMDA receptor antag TRDEVO
ocrelizumab RMSRG1594
anti-LT alpha Mab RARG7416
gantenerumab (A-beta) Alzheimer‘sRG1450
P selectin Mab ACS/CVDRG1512
anti-M1 prime Mab asthmaRG7449
pertuzumab HER2+ mBC 2nd lineRG1273
GA101 NHL & CLLRG7159
T-DM1 HER2+ EBCRG3502
Avastin ovarian cancer 1st lineRG435*Avastin BC combo Xeloda 1st lineRG435*
EPOCH chemo induced anemiaCHU
Tarceva NSCLC EGFR mut 1st lineRG1415*
Actemra sJIARG1569Rituxan ANCA assoc vasculRG105**
11 beta HSD inh metabolic diseasesRG4929
- solid tumorsRG7604
- prostate cancerRG7450
- hematological malignanciesRG7596
Xolair chronic idiopathic urticariaRG3648
Rituxan NHL fast infusionRG105
Avastin HER2+ BC adjRG435Avastin BC combo Herceptin 1st lineRG435Avastin NSCLC adjRG435
GRI schizophrenia negative sympt. RG1678
Avastin HER2-neg. BC adj RG435
Avastin relapsed ovarian caRG435Avastin high risk carcinoidRG435Avastin glioblastoma 1st lineRG435
Avastin triple-neg. BC adjRG435
aleglitazar CV risk reduction in T2DRG1439dalcetrapib atherosc. CV risk red.RG1658
Lucentis diabetic macular edemaRG3645Lucentis AMD high doseRG3645
pertuzumab HER2+ mBC 1st lineRG1273
Herceptin HER2+ BC subcut.RG597Herceptin HER2+ adj BC (2yrs)RG597
GA101 iNHLRG7159vemurafenib met. melanomaRG7204
Tarceva NSCLC adj RG1415
Actemra early RARG1569
T-DM1 HER2+ mBC 1st l.RG3502
GA101 CLLRG7159
Actemra RA DMARD IR H2HRG1569
Avastin mCRC TML RG435
T-DM1 HER2+ adv. mBCRG3502
Actemra sc formulation RARG1569
Tarceva NSCLC EGFR mut 1st lineRG1415
Actemra ankylosing spondylitisRG1569
MabThera NHL sc formulationRG105
ocrelizumab PPMSRG1594
GRI schizophrenia subopt. controlRG1678
Avastin mBC 2nd lineRG435
Activase extended time window AISRG3626
MetMab mBCRG3638
SGLT2 inh type 2 diabetesRG72011
1 Ph3 in Japan
vemurafenib met. melanoma 2nd/3rd l.RG7204

Major themes of our oncology franchise
• Managing existing franchises and expanding to new areas
• Subcutaneous delivery of monoclonal antibodies– Herceptin s.c., MabThera s.c.
• Antibody drug conjugates (‘armed antibodies’)– T-DM1, many more to come
• Personalized health care/targeted agents– Vemurafenib, vismodegib, MetMab, PI3k, etc
• Glyco-engineered antibodies– GA101 (anti-CD20), GA201 (anti-EGFR)
16

Mutated BRAF: an important therapeutic target
1. Garnett MJ, et al. Cancer Cell 2004;6:313–319; 2. Davies H, et al. Nature 2002;417:949-54 3. Libra M, et al. Cell Cycle 2005;4:1382-4. 4. Wan PTC, et al. Cell 2004;116:855–867
5. McCubrey JA, et al. Biochim Biophys Acta 2007;1773:1263–1284.
020406080
100
Onc
ogen
icBR
AF(%
)
• Oncogenic BRAF is frequently identified in cancer1-3
• Highest incidence of BRAF mutations is in melanoma1-3
• 90% of BRAF mutations in cancer result in substitution at position V6001
– All mutations tested result in constitutive activation of BRAF kinase4
• 90% of BRAF mutations at V600 in melanoma result in substitution V600E5
0
10
20
30
40
50
60
Freq
uenc
y of
m
utat
ion
G46
3E
G46
3V
G46
5A
G46
5E
G46
5T
G46
8A
G46
8E
E58
5K
G59
6R
F594
L
V600
EV
599D
G59
6V
0
10
20
30
40
50
60
Freq
uenc
y of
m
utat
ion
G46
3E
G46
3V
G46
5A
G46
5E
G46
5T
G46
8A
G46
8E
E58
5K
G59
6R
F594
L
V600
EV
599D
G59
6V
18
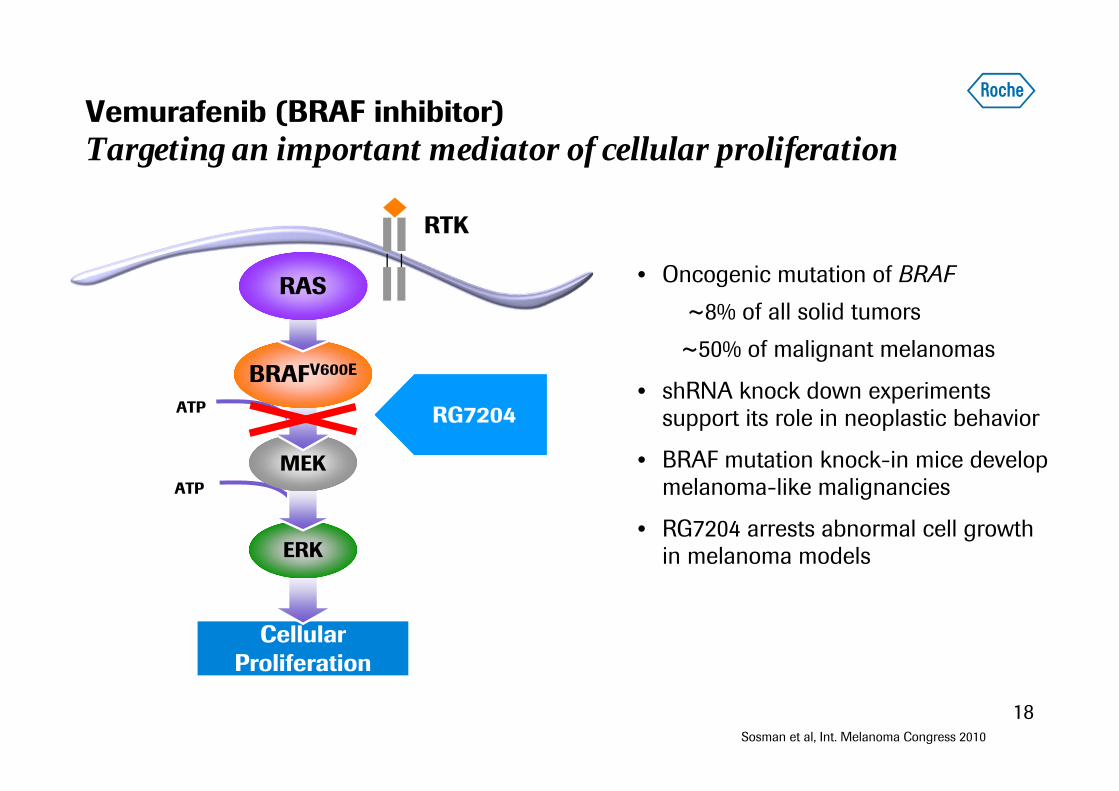
Vemurafenib (BRAF inhibitor)Targeting an important mediator of cellular proliferation
CellularProliferation
RTK
Raf
RG7204ATP
ATP
ERK
MEK
BRAFV600E
RAS • Oncogenic mutation of BRAF~8% of all solid tumors~50% of malignant melanomas
• shRNA knock down experiments support its role in neoplastic behavior
• BRAF mutation knock-in mice develop melanoma-like malignancies
• RG7204 arrests abnormal cell growth in melanoma models
Sosman et al, Int. Melanoma Congress 2010

19
BRIM2Tumor regression occurred in majority of patients
*** 7 patients had 100% tumor shrinkage, 3 of which had confirmed CR; 1 patient had unconfirmed CR and 3 patients had non-target lesions present • 122 patients had baseline and ≥ 1post-baseline scan with measurable disease
RECIST 30% Decrease
***
Sosman et al, Int. Melanoma Congress 2010

2020
Vemurafenib meets overall survival endpointin Phase III
Patient PopulationSecond- and Third line Malignant Melanoma
BRAF mutation positive
First-line Malignant MelanomaBRAF mutation positive
Phase/Study Phase II BRIM2 Phase III BRIM3
# of Patients N=132 N=675
Design • Single ARM: RG7204 • ARM A: RG7204• ARM B: dacarbazine
Primary Endpoint • Best overall response rate assessed by IRC using RECIST criteria • Overall survival
Status• Presented at Int. Melanoma Congress 2010 • FPI Q1 2010; fully recruited in Dec 2010
• Met OS and PFS endpoints in Jan 2011
Filing dossier submitted in US and EU
21
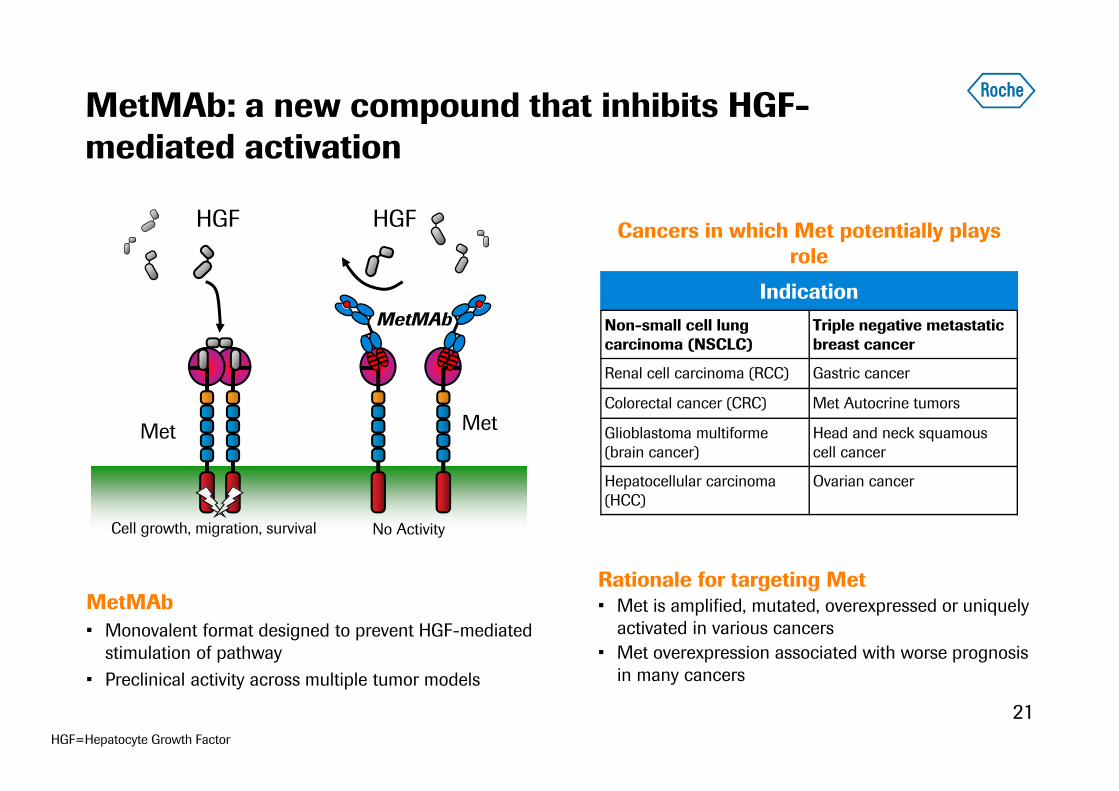
MetMAb: a new compound that inhibits HGF-mediated activation
MetMAb• Monovalent format designed to prevent HGF-mediated
stimulation of pathway • Preclinical activity across multiple tumor models
HGF=Hepatocyte Growth Factor
MetMAb
Met
α α
HGF HGF
Met
No ActivityCell growth, migration, survival
IndicationNon-small cell lung carcinoma (NSCLC)
Triple negative metastatic breast cancer
Renal cell carcinoma (RCC) Gastric cancer
Colorectal cancer (CRC) Met Autocrine tumors
Glioblastoma multiforme (brain cancer)
Head and neck squamous cell cancer
Hepatocellular carcinoma (HCC)
Ovarian cancer
Rationale for targeting Met• Met is amplified, mutated, overexpressed or uniquely
activated in various cancers• Met overexpression associated with worse prognosis
in many cancers
Cancers in which Met potentially plays role

22
MetMAb + Tarceva in lung cancerEfficacy analysis in overall population
23 patients from the erlotinib+placebo arm crossed over to MetMAb.
PFS HR=1.09 OS HR=1.09
Median PFS and OS are consistent with previously reported findings in similar disease setting.
Early analysis of all patients2nd/3rd line mNSCLC
Spigel et al, ESMO 2010

23
Diagnostic companion testUnderstanding the biology of Met signalling
NSCLC: Intensity of Met staining on tumor cells scored on 0–3 scale1+ 2+ 3+
Spigel et al, ESMO 2010
• Phase III in NSCLC with prospective testing of Met receptor over-expression
• Estimated that about one-half of NSCLC patients have Met high tumours
• Met IHC assay will be a companion test for the approval for MetMAb in NSCLC
‘Met high’ definition: ≥50% tumor cells with a staining intensity of 2+ or 3+

24
MetMAb + Tarceva in lung cancerNew example of Personalised Healthcare approach
PFS HR=0.56 OS HR=0.55
• 54% patients had ‘Met High’ NSCLC• 12/23 patients from the Tarceva+placebo arm who crossed over to MetMAb were Met High.• Updated analysis to be presented at ASCO
Early analysis of Met High Patients 2nd/3rd line mNSCLC
Spigel et al, ESMO 2010

25
MetMAb development planNSCLC and triple-negative mBC
Patient Population 2nd and 3rd line Metastatic Non-small Cell Lung Cancer
1st and 2nd line Triple Negative Metastatic
Breast Cancer
Phase Phase III Phase II
Patients Over-expressing Met Receptor N=180
Design • ARM A: Tarceva plus MetMAb• ARM B: Tarceva plus placebo
Prospective Met status testing.
• ARM A: Avastin and paclitaxel plus MetMAb
• ARM B: Avastin and paclitaxel plus placebo
• ARM C: paclitaxel plus MetMAb
Primary end-point • Overall survival • Progression-free survival
Status • Expect FPI in 2011 • Expect FPI Q1 2011

26
HER2-positive breast cancerImproving the standard of care
2010 2016
Early (adjuvant) BC
Herceptin + chemotherapy
Herceptin Subcutaneous+ chemotherapy
Herceptin & pertuzumab + chemotherapy
2012 2013 2014 20152011
1st linemBC
Herceptin + chemotherapy
T-DM1& pertuzumab(MARIANNE)
Herceptin & pertuzumab + chemotherapy(CLEOPATRA)
2nd linemBC
Xeloda + lapatinib
T-DM1 (EMILIA)
Timelines refer to the expected dates of first filing
27
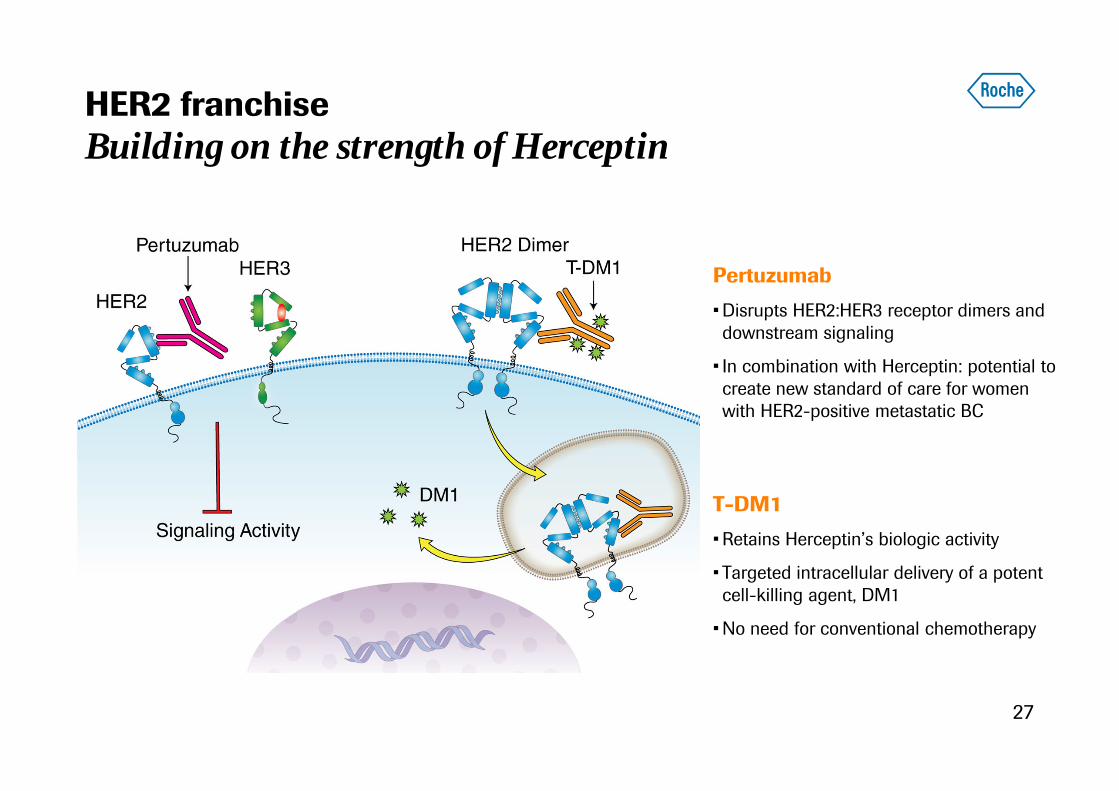
HER2 franchiseBuilding on the strength of Herceptin
T-DM1
• Retains Herceptin’s biologic activity
• Targeted intracellular delivery of a potent cell-killing agent, DM1
• No need for conventional chemotherapy
Pertuzumab
• Disrupts HER2:HER3 receptor dimers and downstream signaling
• In combination with Herceptin: potential to create new standard of care for women with HER2-positive metastatic BC

2828
16.8%
24.0%
45.8%
29.0%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Herceptin +
docetaxel
Herceptin &
pertuzumab +
docetaxel
Herceptin &
pertuzumab
pertuzumab +
docetaxel
path
olog
ical
com
plet
e re
spon
se
ITT population summary
p = 0.0141
p = 0.0198
p = 0.003
Herceptin & pertuzumab in neoadjuvant HER2+ BCAn encouraging result from NEOSPHERE trial
SABCS 2010

29
First line HER2-positive metastatic BCHerceptin and pertuzumab: CLEOPATRA trial
Primary endpoint:
• Progression-free survival
Herceptin + docetaxel
Herceptin & pertuzumab+ docetaxel
HER2-positive mBC(N=808)
• Enrolment completed Q2 2010• Expect PFS data 2011• Filing in 2011

30
Herceptin & pertuzumab in adjuvant settingPotentially increasing the cure rate
Herceptin & pertuzumab+ chemotherapy
Herceptin+ chemotherapy
HER2-positive early breast cancer
N=~4000
Primary end-point: • 3 year Disease Free Survival
Chemotherapy: FEC x 3 →TH x 3 or AC x 4 → TH x 4 or TCH x 6; Total duration of Herceptin treatment=1 yearFEC = 5-fluorouracil, Epirubicin, Cyclophosphamide; TH=Taxotere, Herceptin; AC=cyclophosphamide, doxorubicin; TCH=Taxotere, Carboplatin, Herceptin
• FPI: H2 2011• Follow-up: 3 years (median)• Expect data 2016

31
Second line HER2-positive metastatic breast cancerT-DM1 to demonstrate benefit over standard of care
Second-line1
HER2-positive Metastatic Breast Cancer
Phase IIIEMILIA
N=980
• ARM A: T-DM1• ARM B: Xeloda plus lapatinib
Co-primary endpoints: • Progression-free survival• Overall survival
• FPI Q1 2009• Expect PFS data 2012
• Trial recruiting well.• Filing for accelerated approval expected in 2012, with mature PFS data.• OS data to be provided within 1.5 years thereafter.
1 Patients must have received prior treatment which included both: a taxane, alone or in combination with another agent, and trastuzumab in the adjuvant, locally advanced, or metastatic setting
Patient Population
Second-line1
HER2-positive Metastatic Breast Cancer
Phase/StudyPhase IIIEMILIA
# of Patients N=580
Design • ARM A: T-DM1• ARM B: Xeloda plus lapatinib
Primary Endpoint
• Progression-free survival
Status • FPI Q1 2009• Expect data early 2012

32
Redefining HER2 blockade: pertuzumab and T-DM1 Increasing the efficacy and tolerability in first line
Herceptin+ chemotherapy
Efficacy
Tole
rabi
lity
T-DM1
Herceptin& pertuzumab
+ chemotherapy
T-DM1& pertuzumab
33
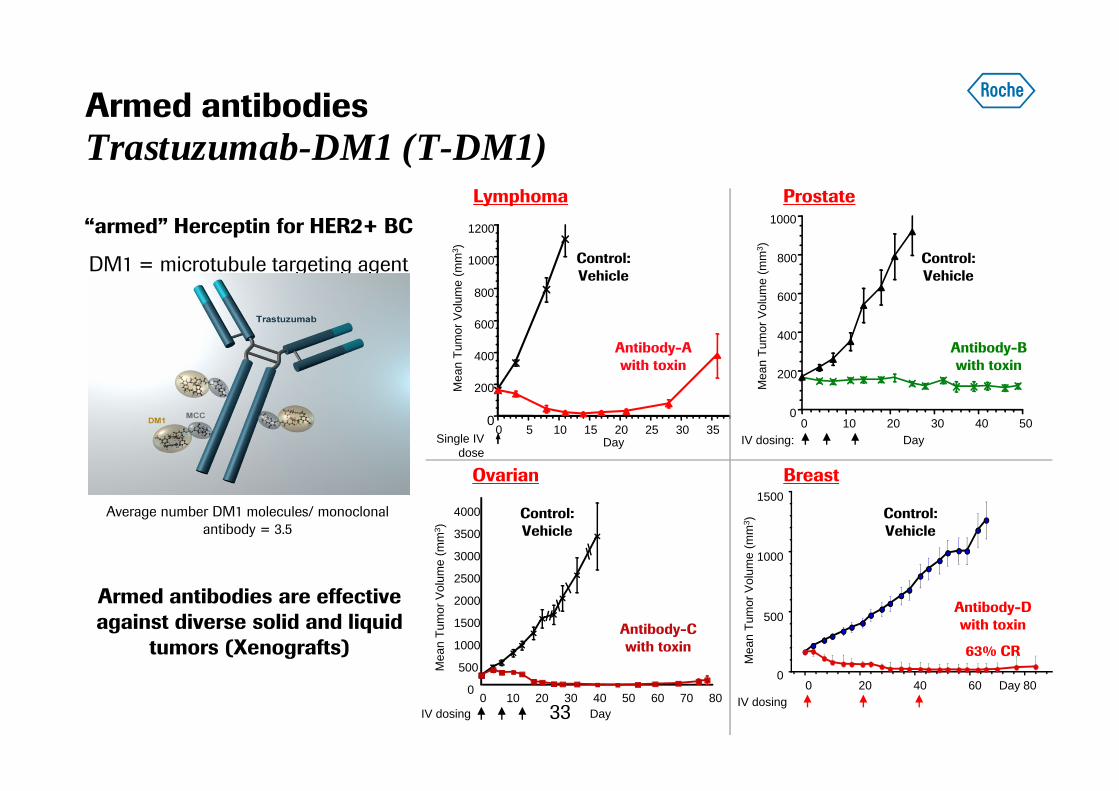
Armed antibodiesTrastuzumab-DM1 (T-DM1)
Average number DM1 molecules/ monoclonal antibody = 3.5
“armed” Herceptin for HER2+ BC
DM1 = microtubule targeting agent
0
200
400
600
800
1000
1200
0 5 10 15 20 25 30 35DaySingle IV
doseM
ean
Tum
or V
olum
e (m
m3 )
Control: Vehicle
Antibody-A with toxin
Lymphoma Prostate
0
200
400
600
800
1000
0 10 20 30 40 50DayIV dosing:
Mea
n Tu
mor
Vol
ume
(mm
3 )
Control: Vehicle
Antibody-B with toxin
0
500
1000
1500
2000
2500
3000
3500
4000
0 10 20 30 40 50 60 70 80
Mea
n Tu
mor
Vol
ume
(mm
3 )
DayIV dosing
Ovarian
Control: Vehicle
Antibody-C with toxin
Breast
0
500
1000
1500
0 20 40 60 80Day
Mea
n Tu
mor
Vol
ume
(mm
3 )
IV dosing
Control: Vehicle
Antibody-D with toxin
63% CR
Armed antibodies are effective against diverse solid and liquid
tumors (Xenografts)

34
TargetScreen Pre-Early Early Stage
ResearchLate StageResearch Early Dev Phase I Phase II/III
ARCNew ADC Linker/drugNew TAP screenNew VAP ScreenRNAi Conjugate
Antibody drug conjugate portfolio
As of March 3, 2010
T-DM1
NME-8
NME-7
NME-14
NME-11
NME-15
NME-16
LSR
LSR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
ESR
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early
Pre-Early Pre-Early
Pre-EarlyPre-Early
Pre-Early
Ovarian
Melanoma
NHL
Kidney
Lung
Pancreatic
Multiple Myeloma
Prostate
Colon
Breast
LSR Go Ed Go IND Submission

ASCO 2011: Key submissionsPersonalised Healthcare becoming reality
Vemurafenib (BRAF inh.)BRIM 3; 1st line met. melanoma
Tarceva EURTAC; EGFR-mutated 1st line NSCLC
MetMAb2nd/3rd line NSCLC; final PFS and OS data
AvastinOCEANS; relapsed ovarian cancer
35
Patient selection crucial for the
success of the trials

36
Performance update and strategy
Update on oncology portfolio
Summary and short term news flow

2011: Major clinical news for late-stage NMEs 7 Phase III and 10 Phase II studies
Compound Indication Study
BRAF inh 1st line met melanoma BRIM3
Lucentis Diabetic macular edema RIDE RISE
Avastin Relapsed ovarian cancer OCEANS
Pertuzumab + Herceptin 1st line HER2+ mBC CLEOPATRA
Herceptin Early HER2+BC sc HANNAH
Actemra Early RA Head-to-Head against Humira1
Hedgehog Pathway Inh. Advanced BCC Pivotal study
T-DM1 1st line HER2+ mBC PFS data
GA101 Relapsed indolent NHL Head-to-Head against MabThera/Rituxan
MetMab NSCLC 2nd / 3rd line Final data
Lebrikizumab Asthma MILLY; MOLLY
Mericitabine Hepatitis C PROPEL final data; JUMP-C
Dalcetrapib Atheroclerosis CV risk red. dal-VESSEL; dal-PLAQUE
1 Read-out likely early 2012
Phas
e II
Phas
e III
37

3838
Outlook for 2011
Barring unforeseen events; LC=Local Currency; * vs. 2010: CHF 0.8 bn
Sales growth (in LC) Group & Pharma (excl. Tamiflu): low single-digitDiagnostics: significantly above market
Core EPS growth target (in LC)
High single-digit
Genentech synergies 2011+ : CHF 1.0 bn*
Debt Aim to return to net cash position by 2015
Dividend outlook Grow dividend in-line with Core EPS growth
Operational Excellencesavings
2011 : CHF 1.8 bn2012+ : CHF 2.4 bn

39
We Innovate Healthcare