
Robotic Surgery - Report · Searches were conducted without language restriction. The Intuitive...
117
Technology Overview: da Vinci Surgical Robotic System July 2004 Rebecca Tooher & Clara Pham Australian Safety and Efficacy Register of New Interventional Procedures – Surgical (ASERNIP-S) © 2004 Intuitive Surgical
Transcript of Robotic Surgery - Report · Searches were conducted without language restriction. The Intuitive...

Technology Overview: da Vinci Surgical Robotic System
July 2004
Rebecca Tooher & Clara Pham
Australian Safety and Efficacy Register of New Interventional Procedures – Surgical
(ASERNIP-S)
© 2004 Intuitive Surgical
2
The ASERNIP-S Programme
Under the auspices of the Royal Australasian College of Surgeons, ASERNIP-S (Australian Safety and Efficacy Register of New Interventional Procedures – Surgical) conducts systematic reviews, accelerated systematic reviews and overviews of new and emerging surgical techniques and technologies. ASERNIP-S is supported by the Australian Government Department of Health and Ageing.
Acknowledgements
We would like to thank Professor Anthony Costello, Mr Patrick Cregan, Associate Professor James Tatoulos and Professor Julian Smith for their expert clinical review of this document. Philippa Middleton and Wendy Babidge provided editorial assistance, and Rebecca Morgan assisted in the literature search.
This report should be cited in the following manner: Tooher, R, Pham, C. The da Vinci surgical robotics system: Technology overview ASERNIP-S Report No. 45. Adelaide, South Australia: ASERNIP-S, (July 2004).(ISBN:0909844658) Copies of these reports can be obtained from: ASERNIP-S The Royal Australasian College of Surgeons PO Box 553, Stepney, SA 5069 AUSTRALIA Ph: 61-8-8363 7513 Fax: 61-8-8362 2077 E-Mail: [email protected] http://www.surgeons.org/asernip-s
This report was ratified by:
The ASERNIP-S Management Committee on
July 8, 2004
The Executive of the Council of the Royal Australasian College of Surgeons
in July 2004

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
3
Table of Contents
Executive summary………………………………………………………………5
1. Introduction .................................................................................................... 9
Background and purpose ...................................................................................................9
The da Vinci surgical robotic system............................................................................. 10
Purported benefits of robotic surgery ....................................................................... 13
Suggested drawbacks of robotic surgery ................................................................... 13
Intuitive Surgical, Inc. .................................................................................................. 14
Regulatory status of the da Vinci surgical system .................................................... 15
Centres using the da Vinci surgical system ............................................................... 16
2. Literature search............................................................................................17
Search strategy.................................................................................................................. 17
Search results .................................................................................................................... 17
3. Applications of da Vinci system ....................................................................18
Urological .......................................................................................................................... 18
Laparoscopic Radical Prostatectomy......................................................................... 19
Pyeloplasty ..................................................................................................................... 20
Other applications ........................................................................................................ 21
Cardiovascular .................................................................................................................. 22
Coronary artery bypass grafting.................................................................................. 23
Atrial septal defect repair............................................................................................. 26
Mitral valve repair ......................................................................................................... 27
Vascular applications.................................................................................................... 27
Thoracic ............................................................................................................................. 28
General Surgery ................................................................................................................ 29
Cholecystectomy........................................................................................................... 30
Fundoplication .............................................................................................................. 31
Gastric surgery .............................................................................................................. 32
Nephrectomy and kidney transplantation................................................................. 33
Other applications ........................................................................................................ 34
Gynaecological .................................................................................................................. 35
Paediatric............................................................................................................................ 36

4
4. Discussion .................................................................................................... 37
Key findings .......................................................................................................................37
Efficacy and safety ........................................................................................................37
Benefits of robotic surgery using the da Vinci system.............................................38
Limitations of robotic surgery using the da Vinci system .......................................39
Technical difficulties with the robotic system...........................................................40
Cost and resource use issues ...........................................................................................42
Training and learning curve issues..................................................................................43
5. Conclusions .................................................................................................. 46
References ........................................................................................................ 48
Appendix A – Centres publishing results of da Vinci robotic-assisted surgery
Appendix B – Excluded studies
Appendix C – Typical operating room set-up
Appendix D – Study design and results tables

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
EXECUTIVE SUMMARY 5
Executive Summary
Background The da Vinci surgical robotic system has recently been introduced into the Australian health care system (to the private Epworth Hospital in Melbourne), and has generated considerable interest from clinicians, patients and the wider community.
The da Vinci surgical robotic system The da Vinci surgical robotic system is a master-slave telemanipulation system, in which the operating surgeon (master) directs robotic surgical arms (slave) from a computer-video console. The da Vinci system consists of three or four robotic arms, one holding the videoscope which provides binocular vision of the operative field, and the others holding instrument adapters to which specialised robotic instruments are attached. The instruments all have articulated elbow and wrist joints, enabling a range of movement which mimics the natural motions of open surgery. The surgeon directs the robotic arms using master handles which sit below the video console and transmit the exact motions of the surgeon’s hands to the robotic arms. The computer console is able to filter hand/arm tremor and provides some tactile feedback, but the majority of tactile feedback is provided indirectly via the video monitor and the tensile feedback available from the robotic arms.
Robotic surgery may offer potential benefits to patients arising from the use of minimally invasive surgery, benefits to the operating surgeon in terms of improved ergonomics and potential for better surgical performance, and benefits to the health system and society resulting from shorter hospital stay and convalescence times. However, the system is expensive, costing at least A$3 million for initial set-up, with ongoing costs for servicing and maintenance, and additional costs for training. Other drawbacks include the lack of direct tactile feedback available with the current system, and a range of practical issues with the robotic set-up.
Aims of the overview This technology overview provides information regarding the use of the da Vinci surgical robotic system for all types of surgery, and addresses cost and resource use issues, legal, regulatory and company issues, surgical training and other policy issues. Rather than making recommendations regarding the uptake and use of the da Vinci robotic system, this overview presents information to assist decision-makers in formulating their own evidence-based recommendations.
EXECUTIVE SUMMARY 6
Methods A systematic search of electronic databases (MEDLINE, EMBASE, PubMed and Cochrane Library) using Boolean search terms was conducted, from 1996 to April 2004. Other relevant internet databases were also searched. We also checked the reference lists of other health technology assessments of robotic surgery. Searches were conducted without language restriction. The Intuitive Surgical website was also searched for product information and relevant trials.
Articles were obtained on the basis of the abstract containing safety and efficacy data on robotic-assisted surgery using the da Vinci surgical robotic system, in the form of randomised controlled trials (RCTs), other controlled or comparative studies, case series and case reports. As there was limited time to complete this overview, we restricted our inclusion criteria to published articles in the English language. Animal studies were excluded. Studies focusing on cost or training issues were used for background. In the case of duplicate publications, the latest and most complete study was included.
Results There were 67 included studies in the following surgical specialty areas: urological (18 studies); cardiovascular (19 studies); general surgery (19 studies); thoracic surgery (7 studies); gynaecological (2 studies); paediatric surgery (2 studies). There were eight comparative studies and 59 case series or case reports. Five of the comparative studies used concurrent controls (Level III-2) and three used historical controls (III-3). One randomised trial comparing robotic surgery and laparoscopic surgery was identified (Cadiere 2001). However, it used the clinical prototype for the da Vinci system, the Mona robot, and was not included in the literature review because technical problems identified in that study were subsequently addressed in the version of the robotic system which is currently available (i.e. the Mona robot was considered to be substantially different to the da Vinci system).
Safety and efficacy of robotic-assisted surgery using the da Vinci system At the present time there is insufficient evidence to determine the safety or efficacy of robotic surgery compared with conventional open or laparoscopic surgery for any surgical application. Small sample sizes and short durations of follow-up characterise the majority of studies. However, some trends were evident in nine comparisons of robotic with open or laparoscopic surgery in the included studies: operative times are generally longer using the robotic system, reflecting increased set-up times and learning curve issues; length of hospital stay
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
EXECUTIVE SUMMARY 7
may be shorter, but is influenced by hospital protocols; and rates of complications appeared to be similar.
The vast majority of included studies were case series or case reports, primarily providing information regarding the feasibility of using the robotic system for different surgical applications and documenting a variety of robotic-related and procedure-related complications.
Feasibility of robotic surgery applications The feasibility of the system has been shown in the following procedures:
- urological: laparoscopic radical prostatectomy, laparoscopic pyeloplasty, laparoscopic cystectomy, laparoscopic cystoprostatectomy, sacrocolpopexy, laparoscopic adrenalectomy
- cardiac: coronary artery bypass grafting, atrial septal defect repair, mitral valve repair, aorto-femoral bypass grafting, laparoscopic aortic reconstruction
- thoracic: thymectomy, pericardial cyst resection, mediastinal mass evaluation and extirpation, thymomectomy
- general: cholecystectomy, fundoplication, gastric surgery, laparoscopic live-donor nephrectomy, kidney transplantation, pancreatic tumour resection, Heller myotomy, suture rectopexy, inguinal hernia repair
- gynaecological: tubal reanastomosis, laparoscopic hysterectomy
- paediatric: fundoplication, cholecystectomy, splenectomy, urachus resection, lymphadenectomy, hernia repair, mediastinal mass investigation, bilateral salpingo-oophorectomy
Benefits, limitations and technical difficulties of robotic surgery A number of benefits of robotic surgery were noted by authors of the included studies. The 3D visualisation, freedom of instrument movement and intuitiveness of the surgical motion were able to the restore hand-eye coordination that is usually lost in laparoscopic surgery, enabling laparoscopic approaches to be used in some cases where it is usually not possible. The moving camera, motion scaling and tremor elimination were regarded as particularly beneficial for procedures requiring precise dissection and identification of anatomic planes. Although there is a significant learning curve for robotic surgery, some authors found that it was shorter than for laparoscopic surgery as skills learned in open surgery were easier to transfer.
Limitations of robotic surgery included: problems adjusting to the robotic system (primarily related to the learning curve and lack of experience); problems with the robotic set-up, in particular the additional time required to set-up the robotic system and the size of the equipment; and problems with

EXECUTIVE SUMMARY 8
communication between the operating surgeon and the rest of the surgical team, particularly the surgical assistant, introduced by the robotic set-up. Technical difficulties encountered in the included studies were related to the malfunction of the system, or collision of the robotic arms either with the patient or with each other, or problems with the instrumentation.
Costs and resource use Only four studies were identified which reported any data regarding cost and resource use issues related to the robotic surgical system. Three reported only direct costs, and none considered potential savings accruing to the patient or society. One study compared robotic and open cardiac surgery and found that although operative costs were significantly higher for robotic surgery, these were offset to some extent by lower postoperative costs, resulting in no significant cost difference overall.
Training and the learning curve The importance of a comprehensive staged training program was emphasised in several studies, and a number of such programs have been developed in the United States. It was noted that training must include the entire surgical team, with particular emphasis on the surgical assistant.
The learning curve (or a volume effect) was evident in many of the included studies, and appeared to be related to increased complications and conversions to open or conventional laparoscopic procedures. As experience with the robotic system increased, operative times, complications and conversions all tended to decrease.
Conclusions Robotic surgery offers some benefits over conventional laparoscopic or open surgery, however, there is a significant learning curve and substantial costs involved both in the initial purchase and ongoing servicing and maintenance of the system. Frequent hardware and software updates can be expected, as with any computer-based equipment. The evidence available at the present time is insufficient to allow any useful comparisons of robotic surgery with open or laparoscopic surgery in terms of safety or efficacy, and high quality randomised trials and thorough economic evaluations are required. Those contemplating the purchase of a da Vinci surgical robotic system should consider whether sufficient procedures can be done to overcome the learning/volume effect and offset the start-up and fixed costs associated with the system.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 1 - INTRODUCTION 9
1. Introduction
“Heartfelt thanks to space-age surgeon” The Weekend Australian, March 27 2004
Background and purpose The da Vinci surgical robotic system has attracted considerable media attention since it was introduced to the private Epworth Hospital in Melbourne in December 2003. As the headline above highlights, the robotic system is seen as the future of surgical technology. Surgeons, patients and hospitals alike are attracted by the promise of “cutting-edge” surgery. However, the very considerable costs involved (at least A$3 million) must be balanced against the possible benefits for patients and surgeons.
This technology overview aims to provide information regarding the use of the da Vinci surgical robotic system for all types of surgery, and to address cost and resource use issues, legal, regulatory and company issues, and other policy issues. The issue of surgical training and learning curves with the da Vinci robot will also be considered. This overview is not a systematic review of robotic surgery using the da Vinci system, and although a systematic approach has been used to identify and synthesize relevant evidence regarding key safety and efficacy outcomes for different surgical applications, the overview does not seek to compare robotic-assisted surgery to conventional surgery with regard to safety and efficacy (as a systematic review typically would do). Rather, the technology overview takes a broader approach and documents both the scientific literature regarding the da Vinci surgical robotic system and other important issues regarding the status and evolution of surgical robotics, which may be important in deciding whether to introduce the da Vinci robot into the Australian health care system, or under which conditions this should be done. Rather than making recommendations regarding the use and uptake of the da Vinci robotic system, this overview presents information to assist decision-makers in formulating their own evidence-based recommendations.

SECT ION 1 - INTRODUCTION 10
The da Vinci surgical robotic system The da Vinci surgical robotic system is a master-slave telemanipulation system. A master-slave system consists of a remote console where the operating surgeon (master) directs the robotic surgical arms (slave) via a telerobotic videoscopic link (Figure 1).
Figure 1: Typical set-up of robotic system in operating room
© 2004 Intuitive Surgical
Elements of the system1
Surgeon console
1 Much of the description of the system provided here is based on Ballantyne & Moll 2003.
The console provides the computer interface between the surgeon and the surgical robotic arms. The surgeon controls the robotic arms through the use of master handles (see Figure 2) which are located in “virtual 3D space” below the visual display. The surgeon’s hand movements are digitised and transmitted to the robotic arms which perform the identical
surgeon console (master)
rroobboottiicc aarrmm ccaarrtt ((ssllaavvee))
mobile video cart
Figure 2: Surgeon console
© 2004 Intuitive Surgical

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 1 - INTRODUCTION 11
movements in the operative field. Foot controls are used to activate electrocautery and ultrasonic instruments, and for repositioning the master handles as necessary. The surgeon views the surgical field through the binocular visual display in the hood of the console. The robotic arms are deactivated whenever the surgeon’s eyes are removed from the display. At the present time the surgeon console and the robotic arm cart are connected via a data cable, and FDA approval in the United States requires that the operating surgeon (at the console) is in the same room as the patient (Ballantyne & Moll 2003). However, telesurgery in which the patient and surgeon are not in the same room is possible, although limited at present by the relatively slow speeds for data transfer currently available.
Master handles In addition to providing direction to the robotic arms, the master handles are also used to control other aspects of the video display system and robotic arms, such as endoscope selection and motion scaling ratio. The master handles filter tremor in the surgeon’s hands and arms, and provide a degree of tactile feedback. However, the majority of tactile feedback is provided indirectly via the video monitor (i.e. visually) and the tensile feedback available through the robotic arms.
Robotic arm cart The robotic arm cart is placed beside the patient on the operating table. It holds three or, more recently, four robotic arms on a central tower. One arm holds the videoscope (Figure 4) and the others are used to attach the instrument adapters which are connected to robotic instrumentation through reusable trocars. Stereoscopic vision is supplied via 30° or 0° specialised 3D scopes which provide the surgeon at the console with binocular vision of the operative field.
Figure 3: Master handles
© 2004 Intuitive Surgical
© 2004 Intuitive Surgical
Figure 4: Video arm
SECT ION 1 - INTRODUCTION 12
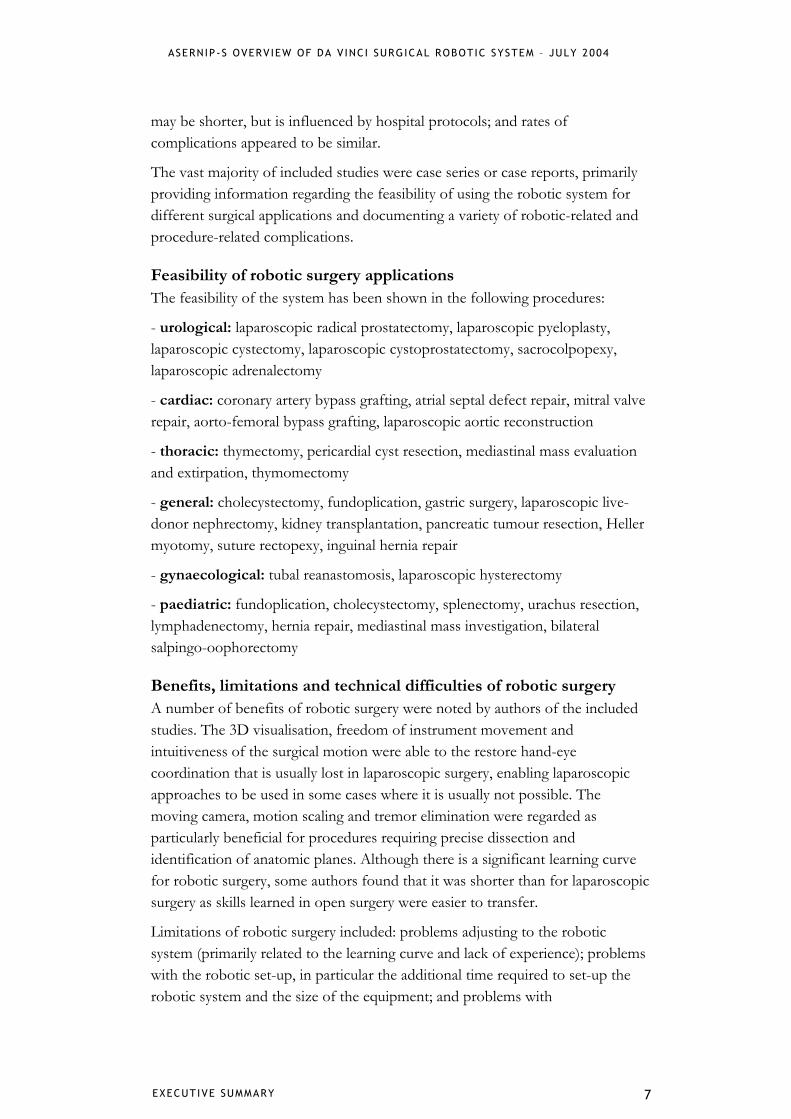
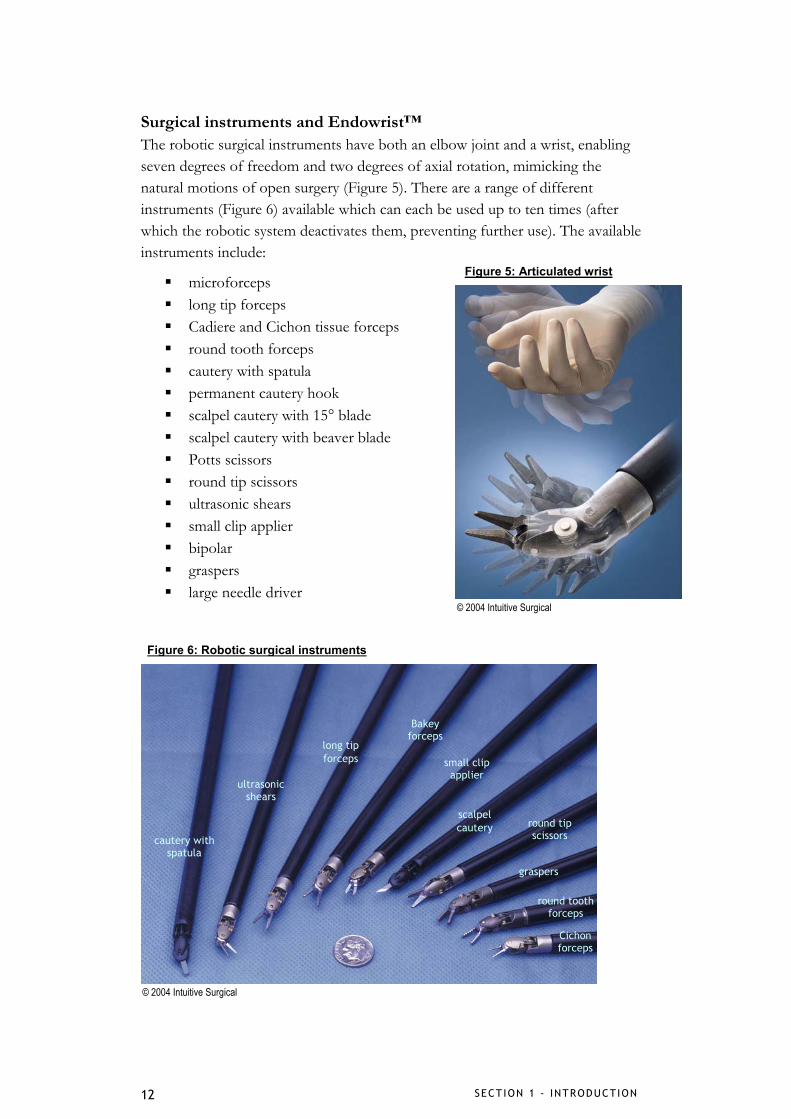
Surgical instruments and Endowrist™ The robotic surgical instruments have both an elbow joint and a wrist, enabling seven degrees of freedom and two degrees of axial rotation, mimicking the natural motions of open surgery (Figure 5). There are a range of different instruments (Figure 6) available which can each be used up to ten times (after which the robotic system deactivates them, preventing further use). The available instruments include:
microforceps long tip forceps Cadiere and Cichon tissue forceps round tooth forceps cautery with spatula permanent cautery hook scalpel cautery with 15° blade scalpel cautery with beaver blade Potts scissors round tip scissors ultrasonic shears small clip applier bipolar graspers large needle driver
Figure 5: Articulated wrist
© 2004 Intuitive Surgical
cautery with spatula
ultrasonic shears
long tip forceps
Bakey forceps
small clip applier
scalpel cautery round tip
scissors
graspers
round tooth forceps
Cichon forceps
Figure 6: Robotic surgical instruments
© 2004 Intuitive Surgical
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 1 - INTRODUCTION 13
Purported benefits of robotic surgery The purported benefits of the da Vinci surgical robotic system are obtained in three key areas:
1) benefits conferred to patients as a result of minimally invasive surgery compared with open approaches (i.e. less blood loss, better cosmesis, fewer complications, shorter convalescence) – the robotic system may allow minimally invasive approaches to be used where conventional laparoscopic approaches would not be possible.
2) benefits conferred to the operating surgeon as a result of the ergonomic set-up of the surgeon console, and expected benefits in surgical performance as a result of the precision of the robotic instrumentation and computer system – in particular the ability to view the surgical field in three dimensions and use natural hand and arm movements (unlike conventional laparoscopic surgery where the laparoscopic instruments are subject to a fulcrum effect) and the ability of the system to filter hand/arm tremor.
3) benefits conferred to the health system as a result of shorter hospital stay and less patient morbidity, and benefits conferred on society by shorter convalescence for patients (for example resulting in fewer lost days from work).
Suggested drawbacks of robotic surgery Suggested drawbacks of robotic surgery also focus on three key areas:
1) the cost of the system – both the initial cost of the equipment (US$1-1.5 million or around A$3 million) and the ongoing costs of supporting the system. As the robotic instruments are only partly reusable ongoing costs could be substantial. Furthermore specialised training in the use of the robotic system is required which may add further costs (cost issues will be explored in more detail on p.43).
2) practical issues with the robotic set-up – the surgeon console, robotic arm cart and video cart may take up considerable space in the operating room and take additional time to prepare, and in addition to the robotic system, a patient-side surgical assistant is still required to assist the operating surgeon at the console.
3) technical issues with the robotic system – the primary technical concern appears to be the lack of tactile feedback available with the current system. Other issues include the possibility of system breakdown and some lack of flexibility with the surgical robotic arms.
SECT ION 1 - INTRODUCTION 14
Intuitive Surgical, Inc.
Company history The information summarised here is publically available from the Intuitive Surgical website (www.intuitivesurgical.com). The da Vinci surgical robotic system is manufactured in Sunnyvale, California by Intuitive Surgical, Inc. The company was formed by Frederic Moll, Robert Younge and John Freund in 1995, to commercialise initial research in surgical robotics undertaken at the Stanford Research Institute (SRI International), and the Massachusetts Institute of Technology. Since that time Intuitive Surgical has developed relationships with IBM Corporation, Johnson & Johnson (Heartport, Inc and Ethicon Endo-Surgery), Olympus Optical, and Medtronic, Inc. Intuitive Surgical was listed on the US stock exchange in June 2000 and trades on the NASDAQ index of high technology stocks (ticker symbol ISRG). The company currently holds the rights to more than 130 patents, with 70 patents pending. From around 2000 Intuitive Surgical was involved in ongoing litigation with Computer Motion Inc., manufacturer of the ZEUS and AESOP surgical robots, over patents issues. These matters were settled in June 2003 and Computer Motion merged with Intuitive Surgical.2 Impending litigation with Brookhill-Wilk (owner of other robotic surgery patents) was settled in January 2004.
Financial status3 Intuitive Surgical’s financial report for 2003 is available from the company’s website (www.intuitivesurgical.com). In 2003 Intuitive Surgical had a full year revenue of US$91.7 million (an increase of 27% from the previous year) with recurring revenue for 2003 of US$29.9 million. A gross margin of 55.2% was reported (excluding non-routine charges associated with settling litigation and acquiring Computer Motion). Around one third of the total operating budget of US$55.9 million was spent on research and development (US$16.2 million). Sales of da Vinci units have increased each year for the past three years; however, sales of services (i.e. for servicing existing systems) have nearly doubled in the last year and appear to be an increasing proportion of Intuitive’s total sales. It may be noted that the company’s initial public offering (IPO) on the stock exchange was oversubscribed, indicating a degree of confidence from the market for the potential for their systems and business; the additional cash reserves generated should be of assistance in funding their ongoing research and development programme.
2 This technology overview is limited to the da Vinci surgical robotic system as it is currently available and does not consider Intuitive Surgical’s other products. 3 Assistance in interpreting the Intuitive Surgical financial report was provided by Business Diagnosis and Solutions, Queensland.
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 1 - INTRODUCTION 15
Regulatory status of the da Vinci surgical system The United States Federal Drug Administration (FDA) has approved the da Vinci surgical system for use in:
thoracoscopic cardiotomy procedures (Nov 02: K022574) general laparoscopic surgery (Jul 00:K990144)
- gallbladder - gastroesophageal reflux - gynaecologic surgery
thoracoscopic surgery (Mar 01:K002489) - IMA harvesting for coronary artery bypass - lung surgery
laparoscopic radical prostatectomy (May 01:K011002) surgical assistance (Jul 97: K965001)
The da Vinci system is not yet cleared for any cardiac procedure in the United States. However, a multicentre study of totally endoscopic coronary artery bypass (TECAB) has been undertaken for FDA approval.
Initial FDA approval in 2000 was supported by a small randomised trial of 22 patients in Mexico comparing robotic-assisted and conventional laparoscopic Nissen fundoplication. The study used the clinical prototype for the da Vinci system – the Mona robot. This study proved the feasibility of the system in a clinical setting but showed that robotic surgery could be significantly longer than conventional laparoscopic surgery (76 mins vs 56 mins). There was one complication in each group and length of stay was similar in both groups. A number of technical problems became apparent which have since been addressed in the current da Vinci system.
In Europe the da Vinci system has full regulatory clearance and is entitled to affix the CE mark4 to the system until August 2006, when the clearance will need to be renewed.
In Australia the da Vinci surgical robotic system is listed on the Therapeutic Goods Administration (TGA) Australian Register of Therapeutic Goods (ARTG) (Class IIb) and is distributed in Australia by Device Technologies Australia, P/L.
4 The “Conformité Européene” (CE) mark may be placed on manufactured goods to signify that the product complies with relevant product directives, may legally be placed on the market, may be traded freely within the European Union, and is subject to regulatory control (and could be withdrawn from market if it fails to comply).

SECT ION 1 - INTRODUCTION 16
Centres using the da Vinci surgical system5 According to the Intuitive Surgical website, there are 210 da Vinci units in hospitals around the world, including 148 in the United States, 47 in Europe and 15 in the rest of the world. To our knowledge, the private Epworth Hospital in Melbourne is the only Australian hospital using the system, although Device Technologies Australia appears to have a second robotic system on loan from Intuitive which may be accessed by surgeons in Sydney. The Epworth Hospital has performed 40 robot-assisted radical prostatectomies to date (Epworth Hospital, Vic: personal communication, 2004). Cardiac procedures have also been performed since March 2004; however, actual numbers have not been given and from press releases we estimate that at least one coronary artery bypass graft, five mitral valve repairs, and at least one single vessel small thoracotomy and one multi-vessel small thoracotomy have been performed.
5 Appendix A tabulates the centres worldwide which have published results of robotic-assisted surgery using the da Vinci system (located in our literature search as detailed below).
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 2 – METHODOLOGY 17
2. Literature search
Search strategy A systematic search of MEDLINE, EMBASE, PubMed and Cochrane Library using Boolean search terms was conducted, from 1996 to April 2004. The York (UK) Centre for Reviews and Dissemination databases, Clinicaltrials.gov, National Research Register, relevant online journals and the Internet were searched in March and April 2004. We also checked the reference lists of other health technology assessments of robotic surgery. Searches were conducted without language restriction. The Intuitive Surgical website was also searched for product information and relevant trials.
Articles were obtained on the basis of the abstract containing safety and efficacy data on robotic-assisted surgery using the da Vinci surgical robotic system, in the form of randomised controlled trials (RCTs), other controlled or comparative studies, case series and case reports. As there was limited time to complete this overview, we restricted our inclusion criteria to published articles in the English language. Animal studies were excluded. Studies focusing on cost or training issues were used for background. In the case of duplicate publications, the latest and most complete study was included.
Search results Our searches retrieved 154 abstracts. We included 67 (accounting for 16 duplicate publications) and excluded 71 (see Appendix B).
The included studies were in the following surgical specialty areas: urological – 18 studies cardiovascular – 19 studies general surgery – 19 studies thoracic surgery – 7 studies gynaecological – 2 studies paediatric surgery – 2 studies
Study design details and key outcomes are tabulated in Appendix D. There were eight comparative studies and 59 case series or case reports. Five of the comparative studies used concurrent controls (Level III-2) and three used historical controls (III-3). One randomised trial comparing robotic surgery and laparoscopic surgery was identified (Cadiere 2001). However, it used the clinical prototype for the da Vinci system, the Mona robot, and was not included in the literature review because technical problems identified in that study were subsequently addressed in the version of the robotic system which is currently available (the results of this study are described on p.15).

SECTION 3 – L ITERATURE REV IEW 18
3. Applications of da Vinci system
Urological We found eighteen studies reporting urological applications of the da Vinci surgical robotic system. The most common use is in laparoscopic radical prostatectomy (10 studies; 351 patients). The robotic system has also been used for laparoscopic pyeloplasty (2 studies; 17 patients), cystectomy (2 studies; 4 patients), cystoprostatectomy (1 study; 17 patients), adrenalectomy (2 studies; 3 patients) and sacrocolpopexy (1 study; 5 patients) (see Table 1). Appendix C shows typical operating room set-up for urological surgery.
Table 1: Urological Studies (18)
Study Indication Level N Follow-up Menon 2002 prostatectomy III-2 30 robotic
30 control NS
Menon 2003a prostatectomy IV 100 NS Wolfram 2003* prostatectomy IV 81 NS Bentas 2003a* prostatectomy IV 40 up to 23
months Ahlering 2003 prostatectomy IV 45 3-6 months Rassweiler 2001 prostatectomy IV 6 1 month Pasticier 2000 prostatectomy IV 5 1 month Gettman 2003 prostatectomy IV 4 NS Kaouk 2003 sural nerve graft during
prostatectomy IV 3 NS
Abbou 2001 prostatectomy IV 1 7 days
Gettman 2002 pyeloplasty III-3 6 robotic 6 control
3 months
Bentas 2003b pyeloplasty IV 11 median 21 months
Menon 2004 cystectomy IV 3 NS Beecken 2003 cystectomy IV 1 5 months
Menon 2003b cystoprostatectomy IV 17 NS Di Marco sacrocolpopexy for
vaginal vault prolapse IV 5 4 months
Desai 2002 laparoscopic adrenalectomy
IV 2 NS
Young 2002 adrenalectomy for adrenal incidentaloma
IV 1 NS
NOTE: NS – not stated; * same centre but no patient cross-over

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 19
Laparoscopic Radical Prostatectomy (LRP)
Technique In this application the robotic system is connected to the instruments used for laparoscopic radical prostatectomy (scope, forceps, needle drivers, scalpel, electrocautery). Port placement generally consists of a 12mm port on the upper left side of the umbilicus for the binocular endoscope and two 8mm ports around 10 to 12cm from the midline (lateral border of the rectal sheath). The assistant’s role includes exposing the operative field, suction and irrigation for haemostasis, and application of clips and electrocautery. The prostate is removed through the umbilical port. In the Vattikuti Institute Technique (VIT) (Ahlering 2003) the initial incision is just above the pubic symphysis. The endopelvic fascia is incised using the da Vinci hook or spatula and da Vinci long tip forceps are used to grasp the cut end of the posterior bladder neck in the midline and gradually dissect it away from the prostate. The proponents of VIT argue that it combines the virtue of a large working space with those of an extraperitoneal dissection (Ahlering 2003).
Results Key results from the ten studies of robotic LRP are shown in Table 2. In the single comparative study (Menon 2002), operative time was over twice as long using the robotic system as conventional open surgery (288 mins vs 138 mins); however, there was a shorter length of stay, less blood loss and fewer transfusions. In the other studies, operative times of around 240 minutes for the robotic system appear typical, although there is a wide range and there is evidence of a learning, or at least a volume, effect, in that operative times appear shorter in larger series and in later series from the same centre. For example, at the J.W. Goethe University (Frankfurt) Department of Urology, mean operative time for the first 40 patients was 558 minutes (Bentas 2003a) whereas for the next 81 patients it was 250 minutes (Wolfram 2003). Ahlering (2003) reported results for five cohorts of patients allowing the learning/volume effect to be tracked. Mean operative time gradually decreased from 350 minutes for the first cohort (patients 1 to 5) to 162 minutes for the fifth cohort (patients 36 to 45). Length of stay appears to vary more widely and this may be attributable to different hospital protocols for discharge in European hospitals compared with US hospitals.
A number of complications were reported in almost all studies. We have calculated an overall complication rate based on all reported complications divided by the number of patients. In doing so, we have made the assumption that each patient only experienced one complication unless it was otherwise stated in the relevant paper. Complication rates between 4% and 33% were
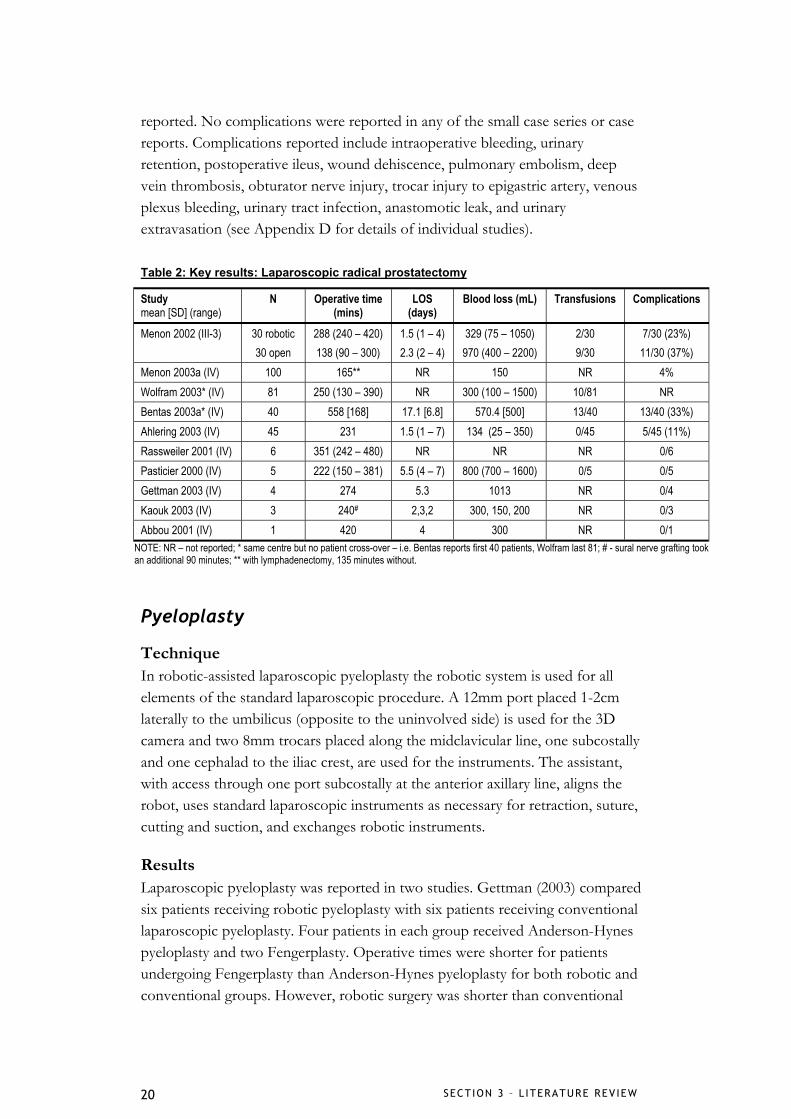
SECTION 3 – L ITERATURE REV IEW 20
reported. No complications were reported in any of the small case series or case reports. Complications reported include intraoperative bleeding, urinary retention, postoperative ileus, wound dehiscence, pulmonary embolism, deep vein thrombosis, obturator nerve injury, trocar injury to epigastric artery, venous plexus bleeding, urinary tract infection, anastomotic leak, and urinary extravasation (see Appendix D for details of individual studies).
Table 2: Key results: Laparoscopic radical prostatectomy
Study mean [SD] (range)
N Operative time (mins)
LOS (days)
Blood loss (mL) Transfusions Complications
Menon 2002 (III-3)
30 robotic 30 open
288 (240 – 420) 138 (90 – 300)
1.5 (1 – 4) 2.3 (2 – 4)
329 (75 – 1050) 970 (400 – 2200)
2/30 9/30
7/30 (23%) 11/30 (37%)
Menon 2003a (IV) 100 165** NR 150 NR 4% Wolfram 2003* (IV) 81 250 (130 – 390) NR 300 (100 – 1500) 10/81 NR Bentas 2003a* (IV) 40 558 [168] 17.1 [6.8] 570.4 [500] 13/40 13/40 (33%) Ahlering 2003 (IV) 45 231 1.5 (1 – 7) 134 (25 – 350) 0/45 5/45 (11%) Rassweiler 2001 (IV) 6 351 (242 – 480) NR NR NR 0/6 Pasticier 2000 (IV) 5 222 (150 – 381) 5.5 (4 – 7) 800 (700 – 1600) 0/5 0/5 Gettman 2003 (IV) 4 274 5.3 1013 NR 0/4 Kaouk 2003 (IV) 3 240# 2,3,2 300, 150, 200 NR 0/3 Abbou 2001 (IV) 1 420 4 300 NR 0/1
NOTE: NR – not reported; * same centre but no patient cross-over – i.e. Bentas reports first 40 patients, Wolfram last 81; # - sural nerve grafting took an additional 90 minutes; ** with lymphadenectomy, 135 minutes without.
Pyeloplasty
Technique In robotic-assisted laparoscopic pyeloplasty the robotic system is used for all elements of the standard laparoscopic procedure. A 12mm port placed 1-2cm laterally to the umbilicus (opposite to the uninvolved side) is used for the 3D camera and two 8mm trocars placed along the midclavicular line, one subcostally and one cephalad to the iliac crest, are used for the instruments. The assistant, with access through one port subcostally at the anterior axillary line, aligns the robot, uses standard laparoscopic instruments as necessary for retraction, suture, cutting and suction, and exchanges robotic instruments.
Results Laparoscopic pyeloplasty was reported in two studies. Gettman (2003) compared six patients receiving robotic pyeloplasty with six patients receiving conventional laparoscopic pyeloplasty. Four patients in each group received Anderson-Hynes pyeloplasty and two Fengerplasty. Operative times were shorter for patients undergoing Fengerplasty than Anderson-Hynes pyeloplasty for both robotic and conventional groups. However, robotic surgery was shorter than conventional

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 21
surgery for both types of pyeloplasty. Mean operative times for Anderson -Hynes and Fengerplasty were 140 and 78 minutes for robotic surgery and 235 and 100 minutes for conventional surgery. Hospital stay was 4 days for all patient groups. There were no conversions to open and all patients were successfully treated. Blood loss was minimal (less than 50mL in all cases) and there were no postoperative complications.
Bentas (2003b) reported a series of 11 patients receiving robotic-assisted laparoscopic pyeloplasty via a transperitoneal approach. Mean operative time was 197 minutes and length of hospital stay 5.5 days. There were no conversions and blood loss was reported as negligible. No complications were reported apart from one patient with mild flank pain.
Other applications Menon (2003b) used the robotic system for 17 patients receiving nerve-sparing radical cystoprostatectomy for transitional cell carcinoma of the bladder. Mean operative time was 140 minutes and blood loss was less than 150mL. Three complications were reported, one incomplete operation due to lens malfunction, one re-exploration and one port-site haematoma.
DiMarco (2004) reported five patients receiving robotic-assisted sacrocolpopexy. Mean operative time was 222 minutes and hospital stay one night. One patient experienced persistent vaginal bleeding for two days postoperatively. There were no vaginal prolapses and no robot-related complications.
Beeken (2003) used the robotic system for a laparoscopic radical cystectomy and intra-abdominal formation of orthotopic ileal neobladder. The procedure was thought to be curative as there were clear margins and no lymph node metastases and after five months the patient was tumour free with a functioning neobladder. There were no intraoperative or postoperative complications. Menon (2004) reported three patients receiving radical cystectomy and urinary diversion with preservation of uterus and vagina. All three had successful tumour removal with clear margins and all lymph nodes removed were negative. Mean operative time was 160 minutes and mean blood loss less than 100mL.
Desai (2002) reported two patients receiving laparoscopic adrenalectomy. Neither were converted to the conventional laparoscopic or open procedure; however, the second patient experienced capsular tear of the adrenal gland due to robotic retraction and manipulation. There were no other complications reported. Young (2002) reported one patient receiving robotic-assisted adrenalectomy for adrenal incidentaloma. The adrenal oncocytoma was removed with clear margins, the postoperative course was “uneventful” and the patient
SECTION 3 – L ITERATURE REV IEW 22
was discharged within 24 hours. Robotic dissection took 55 minutes of a total 100 minutes of operative time.
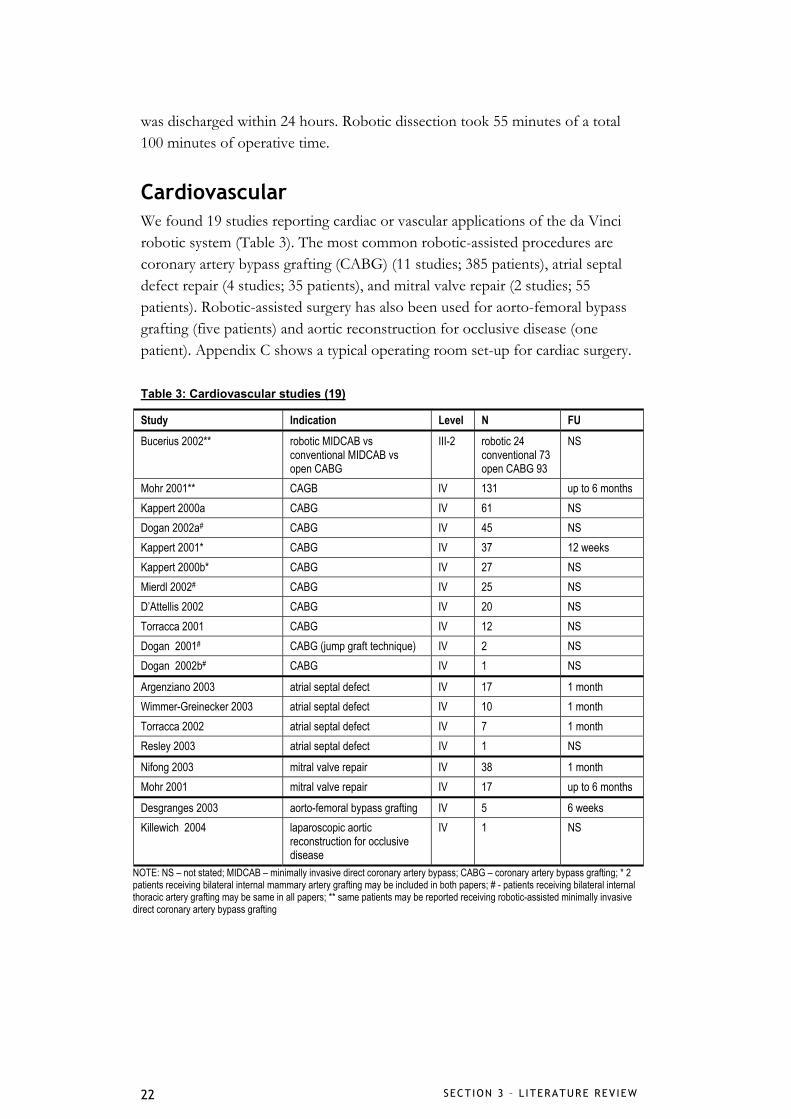
Cardiovascular We found 19 studies reporting cardiac or vascular applications of the da Vinci robotic system (Table 3). The most common robotic-assisted procedures are coronary artery bypass grafting (CABG) (11 studies; 385 patients), atrial septal defect repair (4 studies; 35 patients), and mitral valve repair (2 studies; 55 patients). Robotic-assisted surgery has also been used for aorto-femoral bypass grafting (five patients) and aortic reconstruction for occlusive disease (one patient). Appendix C shows a typical operating room set-up for cardiac surgery.
Table 3: Cardiovascular studies (19)
Study Indication Level N FU Bucerius 2002** robotic MIDCAB vs
conventional MIDCAB vs open CABG
III-2 robotic 24 conventional 73 open CABG 93
NS
Mohr 2001** CAGB IV 131 up to 6 months Kappert 2000a CABG IV 61 NS Dogan 2002a# CABG IV 45 NS Kappert 2001* CABG IV 37 12 weeks Kappert 2000b* CABG IV 27 NS Mierdl 2002# CABG IV 25 NS D’Attellis 2002 CABG IV 20 NS Torracca 2001 CABG IV 12 NS Dogan 2001# CABG (jump graft technique) IV 2 NS Dogan 2002b# CABG IV 1 NS
Argenziano 2003 atrial septal defect IV 17 1 month Wimmer-Greinecker 2003 atrial septal defect IV 10 1 month Torracca 2002 atrial septal defect IV 7 1 month Resley 2003 atrial septal defect IV 1 NS
Nifong 2003 mitral valve repair IV 38 1 month Mohr 2001 mitral valve repair IV 17 up to 6 months
Desgranges 2003 aorto-femoral bypass grafting IV 5 6 weeks Killewich 2004 laparoscopic aortic
reconstruction for occlusive disease
IV 1 NS
NOTE: NS – not stated; MIDCAB – minimally invasive direct coronary artery bypass; CABG – coronary artery bypass grafting; * 2 patients receiving bilateral internal mammary artery grafting may be included in both papers; # - patients receiving bilateral internal thoracic artery grafting may be same in all papers; ** same patients may be reported receiving robotic-assisted minimally invasive direct coronary artery bypass grafting

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 23
Coronary artery bypass grafting
Procedure The robotic system is used for a number of different elements of the coronary artery bypass grafting (CABG) procedure, often depending on the experience of the centre with the robotic system. In some cases, the robotic system is used only for harvesting of the internal thoracic artery (ITA) or the anastomosis of the ITA to the left anterior descending coronary artery. In other cases, both the left internal mammary artery (LIMA) harvesting and the CABG procedure are performed using the da Vinci telemanipulation system. A port for the 3D camera is placed in the forth or fifth left intercostal space at the level of the midclavicular line. Two ports for the robotic instrumentation are made in the third or fourth intercostal space (right instrument) and in the fifth or sixth intercostal space (left instrument) both at the level of the anterior axillary line.
Results Key results for robotic-assisted coronary artery bypass grafting are shown in Table 4. One study compared robotic minimally invasive direct coronary artery bypass (MIDCAB) with conventional MIDCAB and also with conventional CABG via a median sternotomy. Length of hospital stay was significantly shorter for the robotic group (8.9 days) than either the conventional MIDCAB group (15.9 days) or the conventional CABG group (16.3 days). There was no significant difference in ICU stay.
Results from the remaining case series and reports are difficult to compare as the operative approach and extent of robotic-assistance differs between and within the studies. This variability is clearest in the total operative times reported, so to facilitate comparison Table 5 shows times for ITA takedown, anastomosis, cardiopulmonary bypass and aortic cross-clamping separately. These times reflect robotic-assisted surgery, whereas total operative times include both conventional and robotic-assisted elements of the procedure. Robotic-assisted left internal mammary artery (LIMA) harvesting ranged from 25 minutes to around 50 minutes, right internal mammary artery (RIMA) harvesting between 45 and 55 mintues, and bilateral internal mammary artery (BIMA) harvesting was around 88 minutes in two patients and 102 in one patient (Kappert 2000a&b). Anastomosis times were only reported by Kappert and ranged from 7 minutes in six TECAB patients to 31 minutes in 29 off-pump CABG patients. Cardiopulmonary bypass times (CBT) between 109 and 197 minutes were reported in five studies and cross-clamp times between 38 and 126 minutes were reported in seven studies (See Table 5).
Length of stay ranged from around six to sixteen days; however, ICU stay was more consistent at around 24 hours in most studies. Conversions to open

SECTION 3 – L ITERATURE REV IEW 24
surgery ranged from none to 75% (6/8 totally endoscopic CABG operations on the beating heart). More complex surgeries appeared to have higher conversion rates, perhaps reflecting learning-curve issues. This appears to be the case with the high conversion rate noted above in the series reported by Mohr (2001). Similarly, though Dogan (2002a) reported a conversion rate of 24% (11/45), 10 of these occurred in the first 20 patients, with only one occurring in the last 25 patients.
Table 4: Key results: Coronary artery bypass grafting
Study mean [SD]
N LOS (days)
ICU stay (hours)
Conversions Complications
Bucerius 2002** (III-2)
MIDCAB-R: 24 MIDCAB: 73
open CABG: 93
8.9 15.9 16.3
16.3 20.9 29.7
NR NR
Mohr 2001** (IV) MIDCAB: 81 ITA anastomosis: 15
TECAB: 27 on beating heart: 8
10.7 NR 9.4 NR
20.1 NR 15.5 NR
0/81 0/15
5/27 (18.5%) 6/8 (75%)
10/81 (12%) 1/15 (7%) 2/27 (7%) 5/8 (63%)
Kappert 2000a (IV) MIDCAB: 37 Dresden: 17 TECAB-1: 6 TECAB-2: 1
NR 21 [8] 21 [6] 22 [23]
42
2/61 (3%) 3/61 (5%)
Dogan 2002a# (IV) single vessel: 37 double vessel: 8
8.6 15.4
24 74
11/45 (24%) 15/45 (33%)
Kappert 2001* (IV) on-pump: 8 off-pump: 29
6 21 1/37 (3%) 5/37 (14%)
Kappert 2000b* (IV) 27 7 [1] 20 [24] NR 1/17 (6%) Mierdl 2002# (IV) 25 NR NR NR 3/25 (12%) D’Attellis 2002 (IV) 20 12 47 2/16 (12.5%) 14/16 (88%) Torracca 2001 (IV) LIMA harvest: 12 < 7 NR 1/12 (8%) 2/12 (17%) Dogan 2001# (IV) 2 NR 24 0 0 Dogan 2002# (IV) 1 NR 24 0 1/2
NOTE: NR – not reported; NA – not applicable; CABG – coronary artery bypass grafting; MIDCAB - minimally invasive direct coronary artery bypass; MIDCAB-R – robotic-assisted MIDCAB; ITA – internal thoracic artery; TECAB – totally endoscopic coronary artery bypass grafting; Dresden – CABG using the Dresden technique; LIMA – left internal mammary artery; CBT – cardiopulmonary bypass time; * 2 patients receiving bilateral internal mammary artery grafting may be included in both papers; # - patients receiving bilateral internal thoracic artery grafting may be same in all papers; ** same patients may be reported receiving robotic-assisted minimally invasive direct coronary artery bypass grafting

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 25
Table 5: Operative times: Coronary artery bypass grafting
IMA takedown (mins) Study mean [SD]
N Operative time
(mins) LIMA RIMA BIMA AT
(mins) CBT
(mins) CCT
(mins)
Bucerius 2002** (III-2)
MIDCAB-R: 24 MIDCAB: 73
open CABG: 93
NR NR NR NR NR NR NR
Mohr 2001** (IV) MIDCAB: 81 ITA anastomosis: 15
TECAB: 27 on beating heart: 8
217 [75] 16 [11] 347 [95]
NR
25 - 40 NR NR NR
NA NA NR NR NA
Kappert 2000a* (IV)
MIDCAB: 37 Dresden: 17 TECAB-1: 6 TECAB-2: 1
145 [64] 280 [80] 264 [94]
480
51 [17] 50 [17] 39 [12]
48
NA NA
47 [17] 54
NA NA
89 [16] 102
12 [1] 28 [5] 7 [6] 48
NR NR NR NR
NA 40 [11] 70 [6]
98 Dogan 2002a# (IV) single vessel:37
double vessel: 8 252 [54] 378 [60]
NR NR NR NR 136 [32] 197 [63]
61 [16] 99 [55]
Kappert 2001* (IV) on-pump: 8 off-pump: 29
280 174
50 [17] 35 [8]
54 42 [1]
NA NA
28 [5] 31 [10]
NR NR
70 [6] NA
Kappert 2000b* (IV)
27 240 [79] 40 [13] 45 [15] 87 [18] NR NR 38 [10]
Mierdl 2002# (IV) 25 492 [129] NR NR NR NR 171 [68] 83 [36] D’Attellis 2002 (IV) 20 NR NR NR NR NR 109 [14] NA Torracca 2001 (IV) LIMA harvest: 12 median 44
(38 – 90) NA NA NA NA NA NA
Dogan 2001# (IV) 2 348, 450 NR NR NR NR 139,168 100,126 Dogan 2002# (IV) 1 330 NR NR NR NR 194 96
NOTE: NR – not reported; CABG – coronary artery bypass grafting; MIDCAB - minimally invasive direct coronary artery bypass; MIDCAB-R – robotic-assisted MIDCAB; ITA – internal thoracic artery; TECAB – totally endoscopic coronary artery bypass grafting; Dresden – CABG using the Dresden technique; LIMA – left internal mammary artery; RIMA – right internal mammary artery; BIMA – bilateral internal mammary arteries; CBT – cardiopulmonary bypass time; CCT – cross-clamp time; AT – anastomosis time; * 2 patients receiving bilateral internal mammary artery grafting may be included in both papers; # - patients receiving bilateral internal thoracic artery grafting may be same in all papers; ** same patients may be reported receiving robotic-assisted minimally invasive direct coronary artery bypass grafting
Overall complication rates were calculated by dividing all reported complications by the number of patients (see Table 4). Complications reported included transient atrial fibrillation, stroke atelectasis, graft occlusion, ITA injury, myocardial infarction, reperfusion injury, hypovoloemic shock, pain, and bleeding. The variability in rates of complications may be an artefact of reporting, in that some studies reported problems encountered with the robotic system as complications, whereas in other studies such issues were considered in the discussion. It is possible there was some under-reporting of such complications or difficulties encountered intraoperatively. With the exception of the D’Attelis (2002) series, complication rates seem to be closely related to conversion rates and the degree of experience with the robotic system for complex applications such as minimally invasive heart surgery. Mortality was
SECTION 3 – L ITERATURE REV IEW 26
reported in three studies. D’Attelis (2002) reported no in-hospital mortality but one patient died from low cardiac output after six months. Torracca (2001) reported no mortality. Mohr (2001) reported three patient deaths: one from unknown cause in a MIDCAB patient, one from haemorrhagic stroke in a patient who received robotic-assisted ITA anastomosis, and one patient who received beating-heart TECAB who died from severe anterior myocardial infarction.
Atrial septal defect repair
Procedure The robotic system is used for the intrathoracic portion of atrial septal defect repair. The endoscopic camera is placed through a 12mm port in the fourth intercostal space in the midclavicular line and two instrument ports are placed in the third and sixth intercostal spaces in the anterior axillary line. A pericardiotomy is made using the long-tip forceps and cautery attachments of the robotic system. Pericardial stay sutures are placed, the right atrium is explored, and the fossa closed with a double layer of primary suture. The assistant, working through a port in the fifth intercostal space in the posterior axillary line, provides cardiotomy suction and other assistance as required.
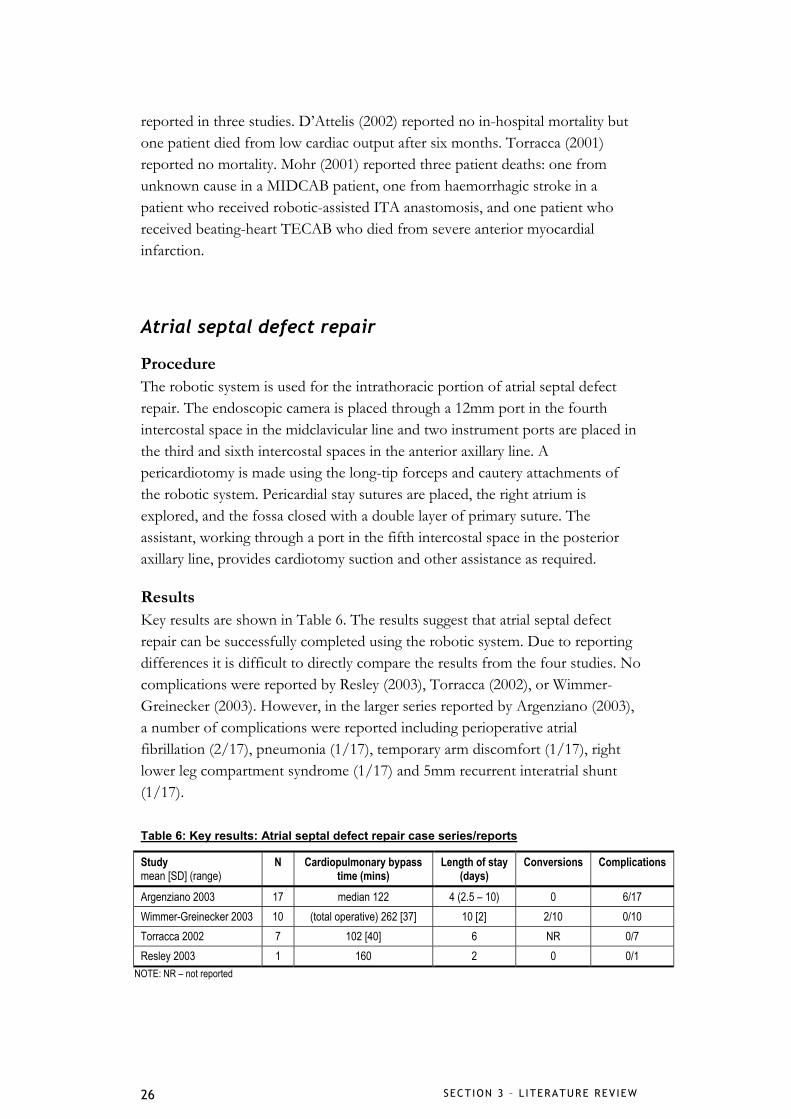
Results Key results are shown in Table 6. The results suggest that atrial septal defect repair can be successfully completed using the robotic system. Due to reporting differences it is difficult to directly compare the results from the four studies. No complications were reported by Resley (2003), Torracca (2002), or Wimmer-Greinecker (2003). However, in the larger series reported by Argenziano (2003), a number of complications were reported including perioperative atrial fibrillation (2/17), pneumonia (1/17), temporary arm discomfort (1/17), right lower leg compartment syndrome (1/17) and 5mm recurrent interatrial shunt (1/17).
Table 6: Key results: Atrial septal defect repair case series/reports
Study mean [SD] (range)
N Cardiopulmonary bypass time (mins)
Length of stay (days)
Conversions Complications
Argenziano 2003 17 median 122 4 (2.5 – 10) 0 6/17 Wimmer-Greinecker 2003 10 (total operative) 262 [37] 10 [2] 2/10 0/10 Torracca 2002 7 102 [40] 6 NR 0/7 Resley 2003 1 160 2 0 0/1
NOTE: NR – not reported
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 27
Mitral valve repair
Procedure In robotic-assisted mitral valve surgery the robotic system is used for valve repair. After the mitral valves have been exposed the right and left robotic arms are inserted via a right trocar in the fourth intercostal space posterior and lateral to a left atriotomy and parallel to the right superior pulmonary vein, and a left trocar placed 6cm cephalad and medial to the right trocar. The 3D high resolution endoscope is placed into the medial portion of a 3-5cm intercostal mini-thoracotomy made for initial valve inspection. The assistant changes instruments and supplies and retrieves operative material via the remaining portion of the mini-thoracotomy. The left atrium is closed under direct vision.
Results Robotic-assisted mitral valve repair was reported in two studies. Mohr (2001) reported mean operative time of 201 [53] minutes, and Nifong (2003) reported a time of 306 [6] minutes for the first 19 patients in their series, and 264 [6] minutes for the last 19 patients. Length of stay was about half as long in Nifong (2003) (around 4 days) as Mohr (2001) (around 10 days) probably reflecting difference in hospital protocol between the United States and Europe. ICU stay was similar in both studies. Eight of 17 (47%) patients in the Mohr (2001) series experienced complications, including mitral insufficiency, postoperative confusion, reintubation for respiratory insufficiency, pneumothorax, and minor residual regurgitation. By comparison there were only three complications in 38 patients in the Nifong series (8%), including one re-exploration, one haemolysis and one fatal stroke at 20 days postoperatively.
Vascular applications Desgranges (2004) reported five patients receiving robotic-assisted aorto-femoral bypass grafting. Aortic anastomoses were successful in four of the five patients, three via mini-laparotomy and one via total laparotomy. In these four patients no robotic related complications were noted. However, in one patient anastomosis could not be performed due to external conflict of the robotic arms and this patient was converted to open laparotomy using conventional techniques. Killewich (2004) reported a case of robotic-assisted laparoscopic aortic reconstruction for occlusive disease. The procedure was successful with the patient returning to normal activity after 2.5 weeks. The operative time of eight hours was considerably longer than the author’s normal operative time; however, no complications were experienced.
SECTION 3 – L ITERATURE REV IEW 28
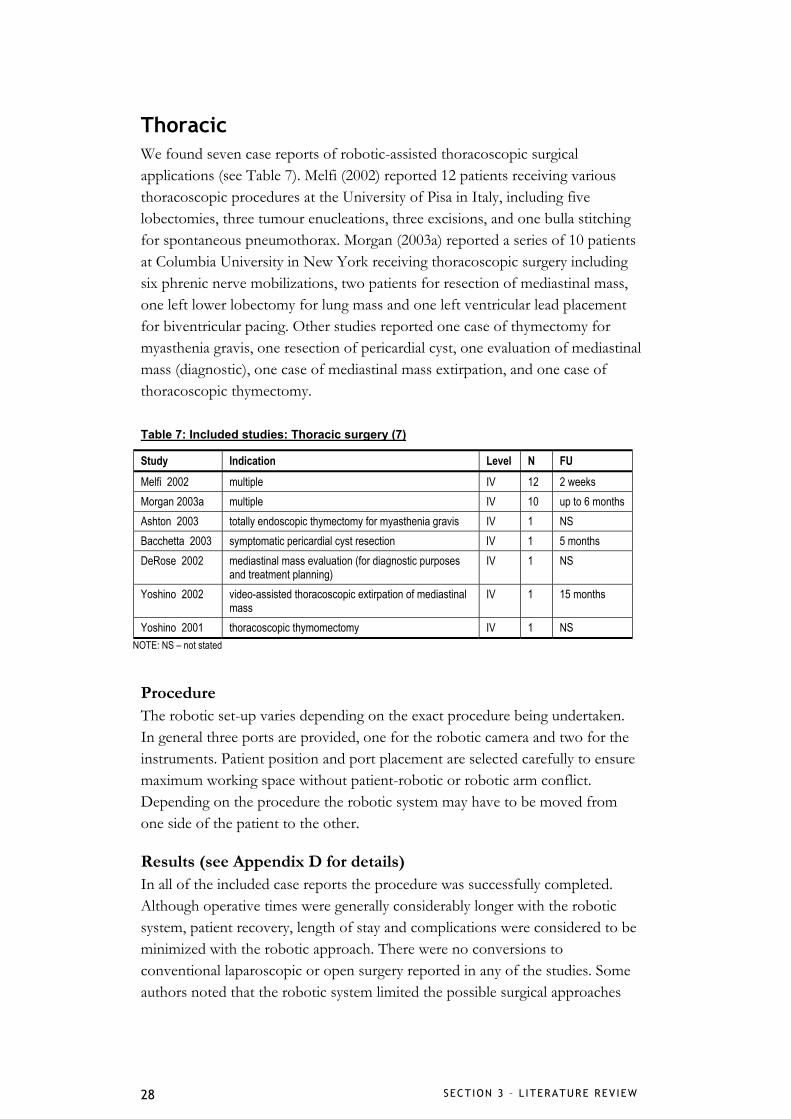
Thoracic We found seven case reports of robotic-assisted thoracoscopic surgical applications (see Table 7). Melfi (2002) reported 12 patients receiving various thoracoscopic procedures at the University of Pisa in Italy, including five lobectomies, three tumour enucleations, three excisions, and one bulla stitching for spontaneous pneumothorax. Morgan (2003a) reported a series of 10 patients at Columbia University in New York receiving thoracoscopic surgery including six phrenic nerve mobilizations, two patients for resection of mediastinal mass, one left lower lobectomy for lung mass and one left ventricular lead placement for biventricular pacing. Other studies reported one case of thymectomy for myasthenia gravis, one resection of pericardial cyst, one evaluation of mediastinal mass (diagnostic), one case of mediastinal mass extirpation, and one case of thoracoscopic thymectomy.
Table 7: Included studies: Thoracic surgery (7)
Study Indication Level N FU Melfi 2002 multiple IV 12 2 weeks Morgan 2003a multiple IV 10 up to 6 months Ashton 2003 totally endoscopic thymectomy for myasthenia gravis IV 1 NS Bacchetta 2003 symptomatic pericardial cyst resection IV 1 5 months DeRose 2002 mediastinal mass evaluation (for diagnostic purposes
and treatment planning) IV 1 NS
Yoshino 2002 video-assisted thoracoscopic extirpation of mediastinal mass
IV 1 15 months
Yoshino 2001 thoracoscopic thymomectomy IV 1 NS NOTE: NS – not stated
Procedure The robotic set-up varies depending on the exact procedure being undertaken. In general three ports are provided, one for the robotic camera and two for the instruments. Patient position and port placement are selected carefully to ensure maximum working space without patient-robotic or robotic arm conflict. Depending on the procedure the robotic system may have to be moved from one side of the patient to the other.
Results (see Appendix D for details) In all of the included case reports the procedure was successfully completed. Although operative times were generally considerably longer with the robotic system, patient recovery, length of stay and complications were considered to be minimized with the robotic approach. There were no conversions to conventional laparoscopic or open surgery reported in any of the studies. Some authors noted that the robotic system limited the possible surgical approaches
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 29
which could be used (Ashton 2003, DeRose 2003). However, Yoshino (2002) felt that the robotic system allowed closed-chest procedures to be carried out more safely and easily than conventional thoracoscopic procedures, and Morgan (2003) reported that complex thoracoscopic surgery could be carried out by less experienced surgeons when using the robotic system than with conventional surgery.
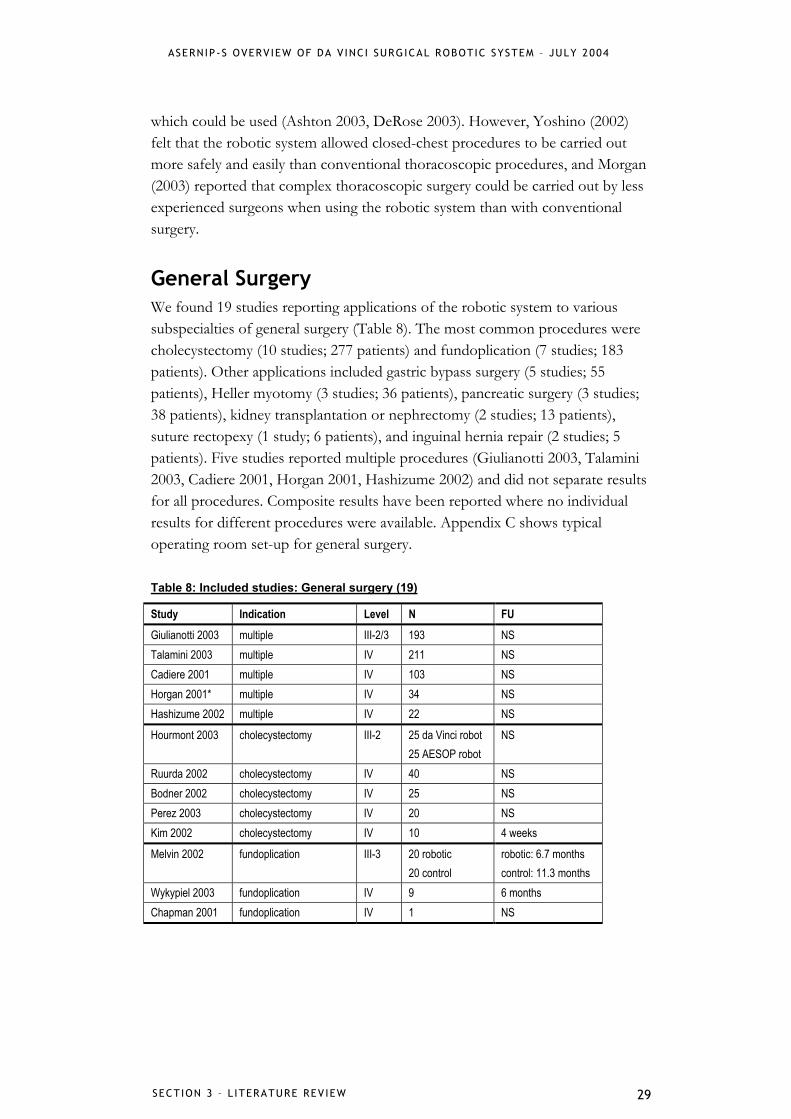
General Surgery We found 19 studies reporting applications of the robotic system to various subspecialties of general surgery (Table 8). The most common procedures were cholecystectomy (10 studies; 277 patients) and fundoplication (7 studies; 183 patients). Other applications included gastric bypass surgery (5 studies; 55 patients), Heller myotomy (3 studies; 36 patients), pancreatic surgery (3 studies; 38 patients), kidney transplantation or nephrectomy (2 studies; 13 patients), suture rectopexy (1 study; 6 patients), and inguinal hernia repair (2 studies; 5 patients). Five studies reported multiple procedures (Giulianotti 2003, Talamini 2003, Cadiere 2001, Horgan 2001, Hashizume 2002) and did not separate results for all procedures. Composite results have been reported where no individual results for different procedures were available. Appendix C shows typical operating room set-up for general surgery.
Table 8: Included studies: General surgery (19)
Study Indication Level N FU Giulianotti 2003 multiple III-2/3 193 NS Talamini 2003 multiple IV 211 NS Cadiere 2001 multiple IV 103 NS Horgan 2001* multiple IV 34 NS Hashizume 2002 multiple IV 22 NS
Hourmont 2003 cholecystectomy III-2 25 da Vinci robot 25 AESOP robot
NS
Ruurda 2002 cholecystectomy IV 40 NS Bodner 2002 cholecystectomy IV 25 NS Perez 2003 cholecystectomy IV 20 NS Kim 2002 cholecystectomy IV 10 4 weeks
Melvin 2002 fundoplication III-3 20 robotic 20 control
robotic: 6.7 months control: 11.3 months
Wykypiel 2003 fundoplication IV 9 6 months Chapman 2001 fundoplication IV 1 NS
SECTION 3 – L ITERATURE REV IEW 30
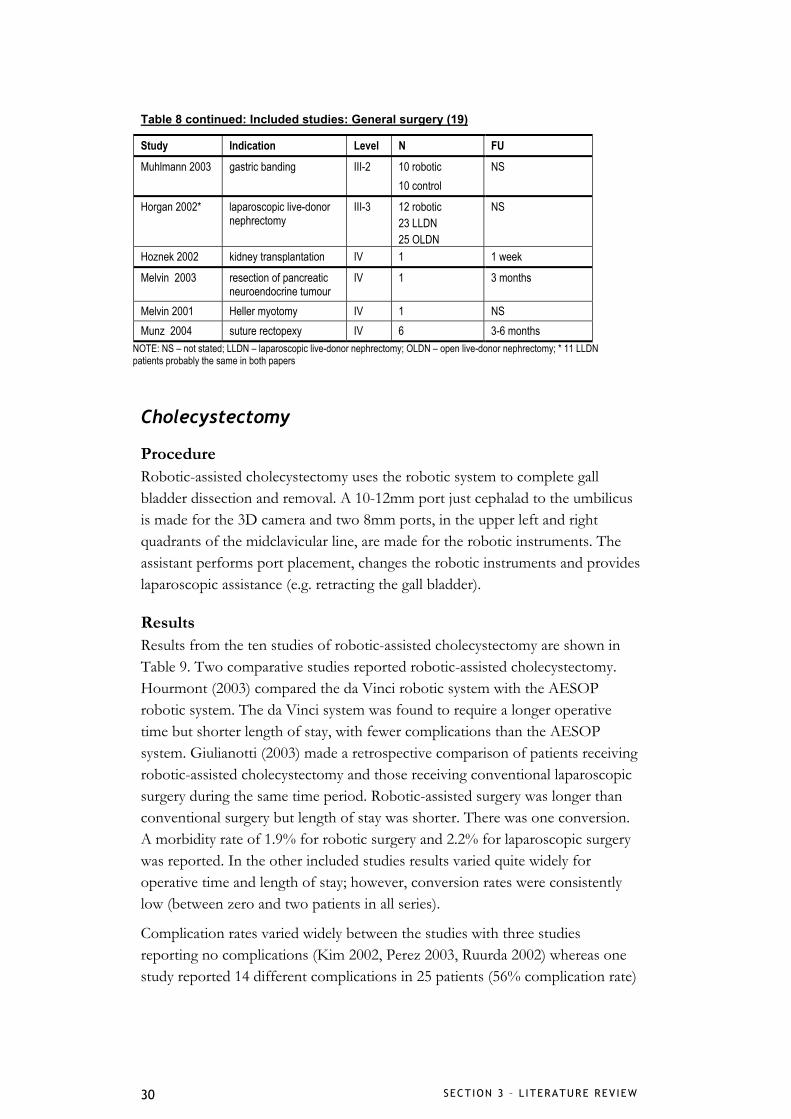
Table 8 continued: Included studies: General surgery (19)
Study Indication Level N FU Muhlmann 2003 gastric banding III-2 10 robotic
10 control NS
Horgan 2002* laparoscopic live-donor nephrectomy
III-3 12 robotic 23 LLDN 25 OLDN
NS
Hoznek 2002 kidney transplantation IV 1 1 week
Melvin 2003 resection of pancreatic neuroendocrine tumour
IV 1 3 months
Melvin 2001 Heller myotomy IV 1 NS Munz 2004 suture rectopexy IV 6 3-6 months
NOTE: NS – not stated; LLDN – laparoscopic live-donor nephrectomy; OLDN – open live-donor nephrectomy; * 11 LLDN patients probably the same in both papers
Cholecystectomy
Procedure Robotic-assisted cholecystectomy uses the robotic system to complete gall bladder dissection and removal. A 10-12mm port just cephalad to the umbilicus is made for the 3D camera and two 8mm ports, in the upper left and right quadrants of the midclavicular line, are made for the robotic instruments. The assistant performs port placement, changes the robotic instruments and provides laparoscopic assistance (e.g. retracting the gall bladder).
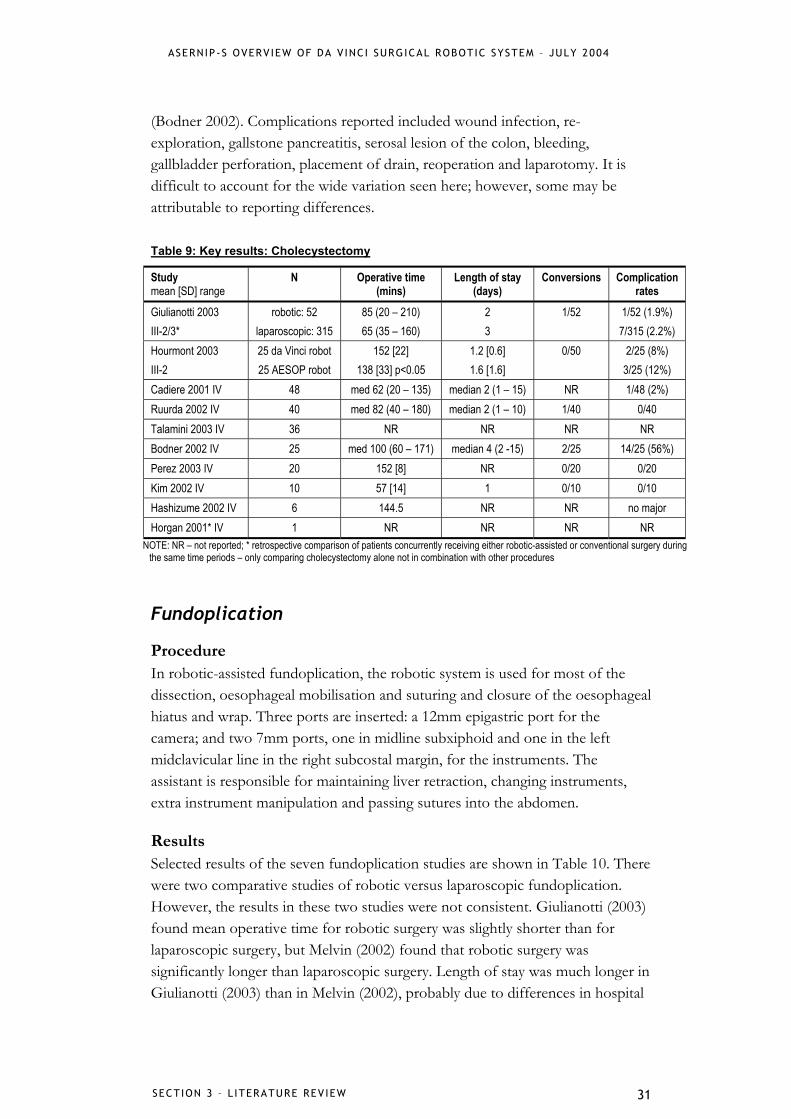
Results Results from the ten studies of robotic-assisted cholecystectomy are shown in Table 9. Two comparative studies reported robotic-assisted cholecystectomy. Hourmont (2003) compared the da Vinci robotic system with the AESOP robotic system. The da Vinci system was found to require a longer operative time but shorter length of stay, with fewer complications than the AESOP system. Giulianotti (2003) made a retrospective comparison of patients receiving robotic-assisted cholecystectomy and those receiving conventional laparoscopic surgery during the same time period. Robotic-assisted surgery was longer than conventional surgery but length of stay was shorter. There was one conversion. A morbidity rate of 1.9% for robotic surgery and 2.2% for laparoscopic surgery was reported. In the other included studies results varied quite widely for operative time and length of stay; however, conversion rates were consistently low (between zero and two patients in all series).
Complication rates varied widely between the studies with three studies reporting no complications (Kim 2002, Perez 2003, Ruurda 2002) whereas one study reported 14 different complications in 25 patients (56% complication rate)
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 31
(Bodner 2002). Complications reported included wound infection, re-exploration, gallstone pancreatitis, serosal lesion of the colon, bleeding, gallbladder perforation, placement of drain, reoperation and laparotomy. It is difficult to account for the wide variation seen here; however, some may be attributable to reporting differences.
Table 9: Key results: Cholecystectomy
Study mean [SD] range
N Operative time (mins)
Length of stay (days)
Conversions Complication rates
Giulianotti 2003 III-2/3*
robotic: 52 laparoscopic: 315
85 (20 – 210) 65 (35 – 160)
2 3
1/52 1/52 (1.9%) 7/315 (2.2%)
Hourmont 2003 III-2
25 da Vinci robot 25 AESOP robot
152 [22] 138 [33] p<0.05
1.2 [0.6] 1.6 [1.6]
0/50 2/25 (8%) 3/25 (12%)
Cadiere 2001 IV 48 med 62 (20 – 135) median 2 (1 – 15) NR 1/48 (2%) Ruurda 2002 IV 40 med 82 (40 – 180) median 2 (1 – 10) 1/40 0/40 Talamini 2003 IV 36 NR NR NR NR Bodner 2002 IV 25 med 100 (60 – 171) median 4 (2 -15) 2/25 14/25 (56%) Perez 2003 IV 20 152 [8] NR 0/20 0/20 Kim 2002 IV 10 57 [14] 1 0/10 0/10 Hashizume 2002 IV 6 144.5 NR NR no major Horgan 2001* IV 1 NR NR NR NR
NOTE: NR – not reported; * retrospective comparison of patients concurrently receiving either robotic-assisted or conventional surgery during the same time periods – only comparing cholecystectomy alone not in combination with other procedures
Fundoplication
Procedure In robotic-assisted fundoplication, the robotic system is used for most of the dissection, oesophageal mobilisation and suturing and closure of the oesophageal hiatus and wrap. Three ports are inserted: a 12mm epigastric port for the camera; and two 7mm ports, one in midline subxiphoid and one in the left midclavicular line in the right subcostal margin, for the instruments. The assistant is responsible for maintaining liver retraction, changing instruments, extra instrument manipulation and passing sutures into the abdomen.
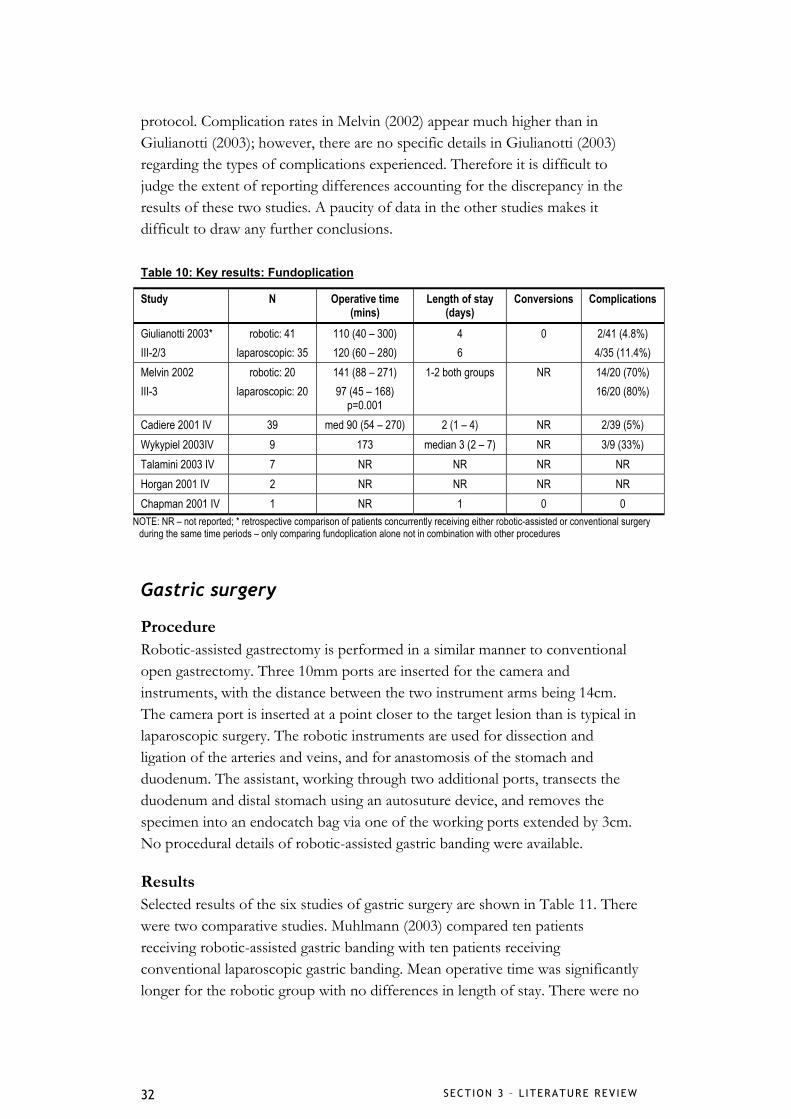
Results Selected results of the seven fundoplication studies are shown in Table 10. There were two comparative studies of robotic versus laparoscopic fundoplication. However, the results in these two studies were not consistent. Giulianotti (2003) found mean operative time for robotic surgery was slightly shorter than for laparoscopic surgery, but Melvin (2002) found that robotic surgery was significantly longer than laparoscopic surgery. Length of stay was much longer in Giulianotti (2003) than in Melvin (2002), probably due to differences in hospital
SECTION 3 – L ITERATURE REV IEW 32
protocol. Complication rates in Melvin (2002) appear much higher than in Giulianotti (2003); however, there are no specific details in Giulianotti (2003) regarding the types of complications experienced. Therefore it is difficult to judge the extent of reporting differences accounting for the discrepancy in the results of these two studies. A paucity of data in the other studies makes it difficult to draw any further conclusions.
Table 10: Key results: Fundoplication
Study N Operative time (mins)
Length of stay (days)
Conversions Complications
Giulianotti 2003* III-2/3
robotic: 41 laparoscopic: 35
110 (40 – 300) 120 (60 – 280)
4 6
0 2/41 (4.8%) 4/35 (11.4%)
Melvin 2002 III-3
robotic: 20 laparoscopic: 20
141 (88 – 271) 97 (45 – 168)
p=0.001
1-2 both groups NR 14/20 (70%) 16/20 (80%)
Cadiere 2001 IV 39 med 90 (54 – 270) 2 (1 – 4) NR 2/39 (5%) Wykypiel 2003IV 9 173 median 3 (2 – 7) NR 3/9 (33%) Talamini 2003 IV 7 NR NR NR NR Horgan 2001 IV 2 NR NR NR NR Chapman 2001 IV 1 NR 1 0 0
NOTE: NR – not reported; * retrospective comparison of patients concurrently receiving either robotic-assisted or conventional surgery during the same time periods – only comparing fundoplication alone not in combination with other procedures
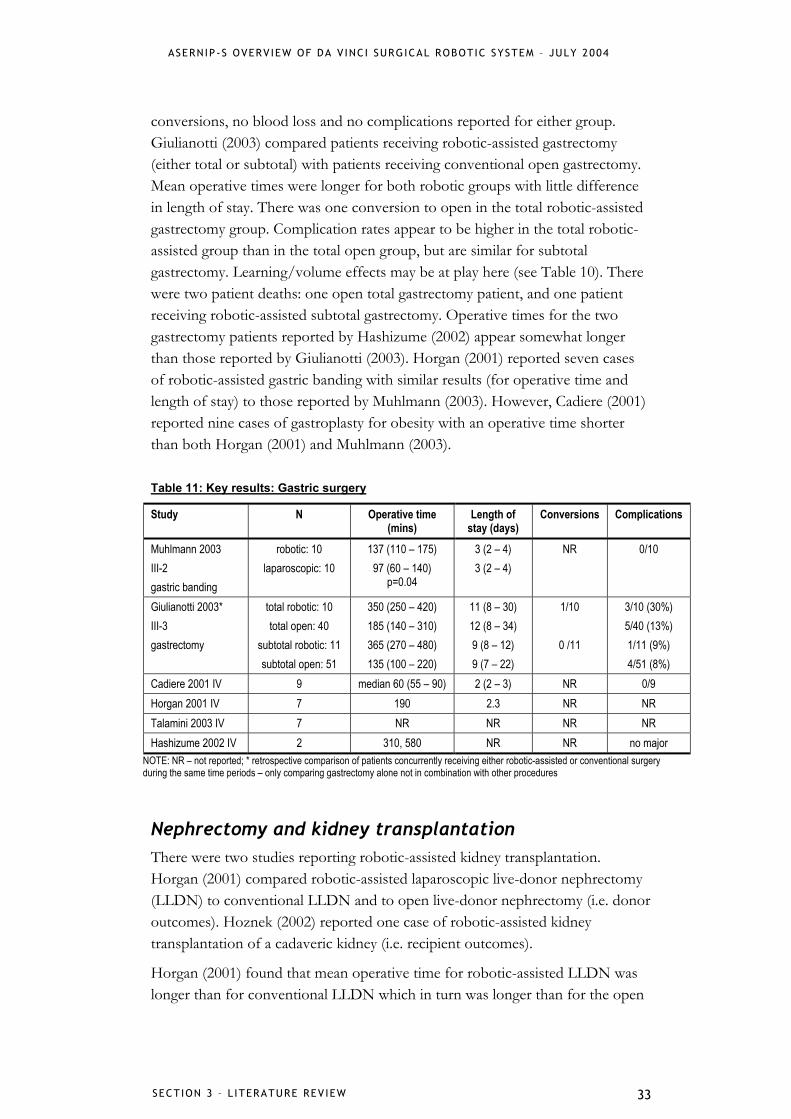
Gastric surgery
Procedure Robotic-assisted gastrectomy is performed in a similar manner to conventional open gastrectomy. Three 10mm ports are inserted for the camera and instruments, with the distance between the two instrument arms being 14cm. The camera port is inserted at a point closer to the target lesion than is typical in laparoscopic surgery. The robotic instruments are used for dissection and ligation of the arteries and veins, and for anastomosis of the stomach and duodenum. The assistant, working through two additional ports, transects the duodenum and distal stomach using an autosuture device, and removes the specimen into an endocatch bag via one of the working ports extended by 3cm. No procedural details of robotic-assisted gastric banding were available.
Results Selected results of the six studies of gastric surgery are shown in Table 11. There were two comparative studies. Muhlmann (2003) compared ten patients receiving robotic-assisted gastric banding with ten patients receiving conventional laparoscopic gastric banding. Mean operative time was significantly longer for the robotic group with no differences in length of stay. There were no
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 33
conversions, no blood loss and no complications reported for either group. Giulianotti (2003) compared patients receiving robotic-assisted gastrectomy (either total or subtotal) with patients receiving conventional open gastrectomy. Mean operative times were longer for both robotic groups with little difference in length of stay. There was one conversion to open in the total robotic-assisted gastrectomy group. Complication rates appear to be higher in the total robotic-assisted group than in the total open group, but are similar for subtotal gastrectomy. Learning/volume effects may be at play here (see Table 10). There were two patient deaths: one open total gastrectomy patient, and one patient receiving robotic-assisted subtotal gastrectomy. Operative times for the two gastrectomy patients reported by Hashizume (2002) appear somewhat longer than those reported by Giulianotti (2003). Horgan (2001) reported seven cases of robotic-assisted gastric banding with similar results (for operative time and length of stay) to those reported by Muhlmann (2003). However, Cadiere (2001) reported nine cases of gastroplasty for obesity with an operative time shorter than both Horgan (2001) and Muhlmann (2003).
Table 11: Key results: Gastric surgery
Study N Operative time (mins)
Length of stay (days)
Conversions Complications
Muhlmann 2003 III-2 gastric banding
robotic: 10 laparoscopic: 10
137 (110 – 175) 97 (60 – 140)
p=0.04
3 (2 – 4) 3 (2 – 4)
NR 0/10
Giulianotti 2003* III-3 gastrectomy
total robotic: 10 total open: 40
subtotal robotic: 11 subtotal open: 51
350 (250 – 420) 185 (140 – 310) 365 (270 – 480) 135 (100 – 220)
11 (8 – 30) 12 (8 – 34) 9 (8 – 12) 9 (7 – 22)
1/10
0 /11
3/10 (30%) 5/40 (13%) 1/11 (9%) 4/51 (8%)
Cadiere 2001 IV 9 median 60 (55 – 90) 2 (2 – 3) NR 0/9 Horgan 2001 IV 7 190 2.3 NR NR Talamini 2003 IV 7 NR NR NR NR Hashizume 2002 IV 2 310, 580 NR NR no major
NOTE: NR – not reported; * retrospective comparison of patients concurrently receiving either robotic-assisted or conventional surgery during the same time periods – only comparing gastrectomy alone not in combination with other procedures
Nephrectomy and kidney transplantation There were two studies reporting robotic-assisted kidney transplantation. Horgan (2001) compared robotic-assisted laparoscopic live-donor nephrectomy (LLDN) to conventional LLDN and to open live-donor nephrectomy (i.e. donor outcomes). Hoznek (2002) reported one case of robotic-assisted kidney transplantation of a cadaveric kidney (i.e. recipient outcomes).
Horgan (2001) found that mean operative time for robotic-assisted LLDN was longer than for conventional LLDN which in turn was longer than for the open

SECTION 3 – L ITERATURE REV IEW 34
procedure (166 mins, 110 mins, 95 mins respectively). However, mean length of stay was shorter for robotic-assisted LLDN than conventional LLDN which was in turn shorter than the open procedure (1.9 days, 2.5 days, 5.1 days respectively). There were no conversions of robotic-assisted patients to either the conventional laparoscopic or open operation. There did not appear to be major differences in any of the safety measures such as blood loss, transfusions, complications or mortality (see Appendix D for details). Hoznek (2002) reported a single case of recipient transplantation using the robotic system. The procedure was successful; however, the authors noted that operative times were longer using the robotic system because the robot obscured the operative field, limiting the access and vision of the surgical assistant. Problems were also experienced with communication between the operating surgeon and assistant due to distance and angles of vision between them.
Other applications Munz (2004) reported six cases of robotic-assisted suture rectopexy. All operations were successful with no significant blood loss and resumption of normal diet within 24 hours. There were no major complications or mortality. Three to six months postoperatively five patients were healthy with no recurrence of rectal prolapse and one patient was experiencing some faecal soiling but with improved symptoms compared with preoperatively. The set-up time for the robotic system averaged 28 minutes (approximately twice as long as conventional set-up). Cadiere (2001) reported three cases of intrarectal procedures with robotic assistance. Median operative time was 65 minutes (range 60 to 79) and length of stay one day (range 1 to 2). There were no complications.
Three studies reported cases of robotic-assisted Heller myotomy (Horgan 2001, Talamini 2003, Melvin 2001); however, Talamini (2003) combined results of various procedures and did not report results of Heller myotomy separately. Horgan (2001) reported a mean operative time for nine patients of 140 minutes with a length of stay of 1.3 days. There were no robotic-related complications. Melvin (2001) reported one case of robotic-assisted Heller myotomy which was completed successfully with no complications and return to normal diet within 24 hours.
Giulianotti (2003) compared 13 patients receiving robotic-assisted pancreatic surgery (pancreatoduodenectomy and left pancreatectomy) with 67 patients receiving open pancreatic surgery. Mean operative times were longer for robotic surgery (490 mins versus 270 mins for pancreatoduodenectomy and 250 mins versus 170 mins for left pancreatectomy), but length of stay was similar in both groups. There were four complications (pancreatic fistulas) in the robotic-
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 3 – L ITERATURE REV IEW 35
assisted groups (complication rate 31%) compared with 21 complications in the open group (complication rate 31%).
Cadiere (2001) reported three patients receiving robotic-assisted inguinal hernia repair. Median operative time was 60 minutes (range 50 to 79) and length of stay one day. No complications were reported.
Talamini (2003) combined the results of 211 patients receiving a variety of different robotic-assisted procedures at four different US centres (see Appendix D for details). Mean operative time was 188 [83] minutes and median length of stay was one day (range 0 to 37 days). Five patients were converted (1%), three due to technical reasons (i.e. too difficult for robotic or laparoscopic approach) and two due to surgeon difficulty with complex robotic-assisted procedures early in the learning curve. Overall there were eight technical complications (4%) including three system malfunctions, four tip dislodgements and one slipped trocar. There were also eight surgical complications including three patients with bleeding, one subcutaneous haematoma, one Clostridium difficile colitis, one case of atelectasis and one case of fever. There were no intraoperative deaths, but one patient died postoperatively, not from robotic-related causes.
Hashizume (2002) combined the results of 22 patients receiving a variety of robotic-assisted general surgical procedures at one Japanese hospital. Mean operative time for all 22 patients was 238 [120] minutes, with robotic time averaging 130 [102] minutes. Mean length of stay was 17 [10] days (similar to conventional surgery in Japanese hospitals). There were no major complications reported. However, several robotic-related problems did occur. In two cases the robotic instrument (forceps) broke and in one case there was a power failure because the da Vinci power source had been incorrectly used. The authors also found that the robotic instruments did not provide sufficient force for effective coagulation and haemostasis and that the surgical assistant needed to hold the tissue with standard laparoscopic forceps to ensure success.
Gynaecological We found two studies reporting gynaecological applications of the robotic system. Schwarzler (2002) reported five patients receiving robotic-assisted tubal reanastomoses. Mean operative time was 189 [41] minutes and length of stay was 3.5 days. There were no conversions and all five procedures were successful. There were no complications reported. Cadiere (2001) reported 28 patients receiving robotic-assisted tubal reanastomoses. Median operative time was 125 minutes (range 108 to 244) and length of stay one day (range 1 to 2). There were no complications. Cadiere (2001) also reported two cases of robotic-assisted

SECTION 3 – L ITERATURE REV IEW 36
laparoscopic hysterectomy. Operative time was 120 minutes and length of stay three days. Complications were not reported.
Paediatric We found two studies reporting multiple applications of the robotic system for paediatric surgery. Luebbe (2003) reported 20 cases of paediatric surgery, including Nissen fundoplication (10), cholecystectomy (3), splenectomy (2), urachus resection (1), unilateral iliac and retroperitoneal lymphadenectomy (1), incisional biopsy of retroperitoneal presacral mass (1), incisional biopsy of hepatic mass (1), Gortex patch repair of Morgagni diaphragmatic hernia, and biopsy of benign infracarinal mediastinal mass (1). Mean operative time for these 20 patients was 208 minutes (range 58 to 573), and mean length of stay was 3 days (range 1 to 16). There were two conversions in splenectomy patients. There were four complications: a right-side pneumothorax in the patient receiving Morgagni hernia repair, two cases of postoperative dysphagia, and one superficial wound infection, all in patients receiving fundoplication. There was no mortality. The authors reported a number of robotic system malfunctions including instrument malfunction, vision system problems, and collisions of the robotic arms due to poor trocar placement or robotic cart positioning.
Gutt (2002) reported 14 cases of robotic-assisted paediatric surgery, including laparoscopic anterior partial fundoplication (8), Nissen fundoplication (3), cholecystectomy (2), and bilateral salpingo-oophorectomy (1). Mean operative time for fundoplication was 146 minutes, for cholecystectomy 150 and 105 minutes, and for salpingo-oophorectomy 95 minutes. Hospital stay for fundoplication was five to six days, and for cholecystectomy was two days. There were no conversions or complications reported. The authors note that the use of robotic-assisted surgery in paediatric patients is limited by the availability of instruments adapted for use in small children.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 4 – D ISCUSS ION 37
4. Discussion
Key findings
Efficacy and safety Table 12 summarises the key findings of the nine comparisons of robotic surgery with conventional laparoscopic or open surgery in the included studies. In six comparisons, mean operative time was longer than conventional surgery (in some cases up to twice as long). However, in two comparisons operative time for robotic-assisted surgery was shorter, though probably not significantly so. Length of stay was shorter in five studies but similar in four. Blood loss and transfusions were similar in two comparisons, but for robotic laparoscopic radical prostatectomy, there was around a third less blood loss and transfusions in the robotic-assisted group compared to open surgery. Rates of complications appeared similar.
Table 12: Key efficacy and safety results from nine comparisons of robotic vs conventional surgery
Comparison Operative time LOS Conversions Blood loss Complications robotic LRP vs open
prostatectomy Menon 2002, III-2
robotic longer (around 2 times)
robotic shorter
NR
around one third less in robotic
7/30 robotic vs 11/30 conventional
laparoscopic pyeloplasty Gettman 2002, III-3
robotic shorter similar NR blood loss minimal both
groups
no complications
MIDCAB and CABG Bucerius 2002, III-2
NR robotic shorter
NR NR NR
laparoscopic cholecystectomy Giulianotti 2003, III-2/3
robotic longer (by 20 mins)
robotic shorter
1 NR 1/52 robotic vs 7/315 conventional
laparoscopic fundoplication Giulianotti 2003, III-2/3
similar (robotic 10 mins shorter)
robotic shorter
0 NR 2/41 robotic vs 4/35 conventional
laparoscopic fundoplication Melvin 2002, III-3
robotic longer (significant)
similar NR NR 14/20 robotic vs 16/20 conventional
laparoscopic gastric banding Muhlmann 2003, III-2
robotic longer (not significant)
similar 0 NR no complications any group
robotic vs open gastrectomy Giulianotti 2003, III-2/3
robotic longer (around 2 times)
similar 1 NR 3/10 robotic total vs 5/40 open total subtotal similar
LLDN and OLDN Horgan 2002, III-3
robotic longer robotic shorter
0 NR similar across all groups
NOTE: NR – not reported; LRP – laparoscopic radical prostatectomy; MIDCAB – minimally invasive direct coronary artery bypass; CABG – coronary artery bypass grafting; LLDN – laparoscopic live-donor nephrectomy; OLDN – open live-donor nephrectomy
SECT ION 4 – D ISCUSS ION 38
Overall, in the included studies, across all surgical specialties, a wide range of procedural complications were reported. In some reports high rates of complications may have reflected the typical difficulties experienced when introducing a new surgical procedure (for discussion of these see Technical difficulties with the robotic system below). There may also have been some discrepancies in reporting of complications between studies in that some included technical complications related to the robotic system together with procedural complications whereas other studies did not. At the present time, the available evidence does not provide sufficient information to make a judgement about the relative safety or efficacy of robotic surgery compared with conventional laparoscopic or open surgery as, in general, study sample sizes are small and lengths of follow-up short.
Benefits of robotic surgery using the da Vinci system The robotic system was generally well received in the majority of included studies. In general, the authors reported that the use of the robotic system enabled laparoscopic approaches to be used, in some cases for procedures which would normally not be possible to perform laparoscopically. The 3D visualisation, freedom of instrument movement and intuitiveness of the surgical motion were regarded as benefits of the system, which were able to restore the hand-eye coordination that is usually lost in laparoscopic surgery (Menon 2002, Bentas 2003, Cadiere 2003, Bodner 2002, Wykypiel 2003, Muhlmann 2003, Hashizume 2002).
The precision of the system was seen as a major advantage by several authors. Cadiere (2003) suggests that short gastric vessels were easier to dissect as dissecting tools could always come perpendicular to the vessels. The moving camera, motion scaling and tremor elimination of the system were regarded as particularly beneficial in complex procedures that require precise dissection and identification of anatomic planes such as LLDN, Heller myotomy and gastric banding (Horgan 2001, Muhlmann 2003).
Shorter learning curves were noted by some authors. Desgranges (2003) noted a shorter learning time for surgeons not experienced in laparoscopic suturing as the robotic system enables “natural” hand-eye coordination and thus skills learned under direct vision can be more easily applied in the laparoscopic setting. Wykypiel (2003) also noted that the learning curve appeared to be rapid for surgeons experienced in laparoscopic antireflux procedures.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 4 – D ISCUSS ION 39
Limitations of robotic surgery using the da Vinci system A number of robotic-related complications or problems were reported, including problems adjusting to the 3D visualisation system, difficulty with lack of tactile feedback (which sometimes caused difficulties in tying sutures without breakage), and lack of specialised instruments (particularly for paediatric patients) (Rassweiler 2001, Gettman 2002, Menon 2002, Desai 2002, Bodner 2002, Luebbe 2003, Gutt 2002). Kim (2002) reported that the surgical assistants experienced some difficulty in correctly inserting instruments, causing slight delays in operative times. This problem appeared to be due to a lack of experience and training with the robotic system. Cadiere (2003) also found that the narrow field of vision provided by the optical system meant that dissection had to be interrupted to reposition the optics.
Robotic set-up also provided challenges in many types of surgery. Set-up times for the robotic system of between 30 and 45 minutes (up to double the time required for conventional laparoscopic surgery) added to overall operative times (Muhlmann 2003, Munz 2004), and some authors regarded the equipment as cumbersome (Bodner 2002, Hoznek 2002). Several authors noted that patient set-up and port placement were very important to avoid conflict of the robotic arms, either with each other, or with the patient, and to ensure procedural success (D’Attellis 2002, Desgranges 2004, Kappert 2001, Mohr 2001).
Communication between the operative team was also noted to be very important particularly between the operating surgeon at the robotic console and the assistant who must anticipate the need to change instruments and take responsibility for the condition of the patient (Dogan 2002). Giulianotti (2003) noted that patient positioning is crucial because postural changes during different steps of the operation may be required. Hoznek (2002) reported that operative times were longer with robotic than with standard surgery because the robotic system obscures the operative field limiting the access and vision of the surgical assistant, and that distance and angles between the operating surgeon and surgical assistant also made communication difficult.
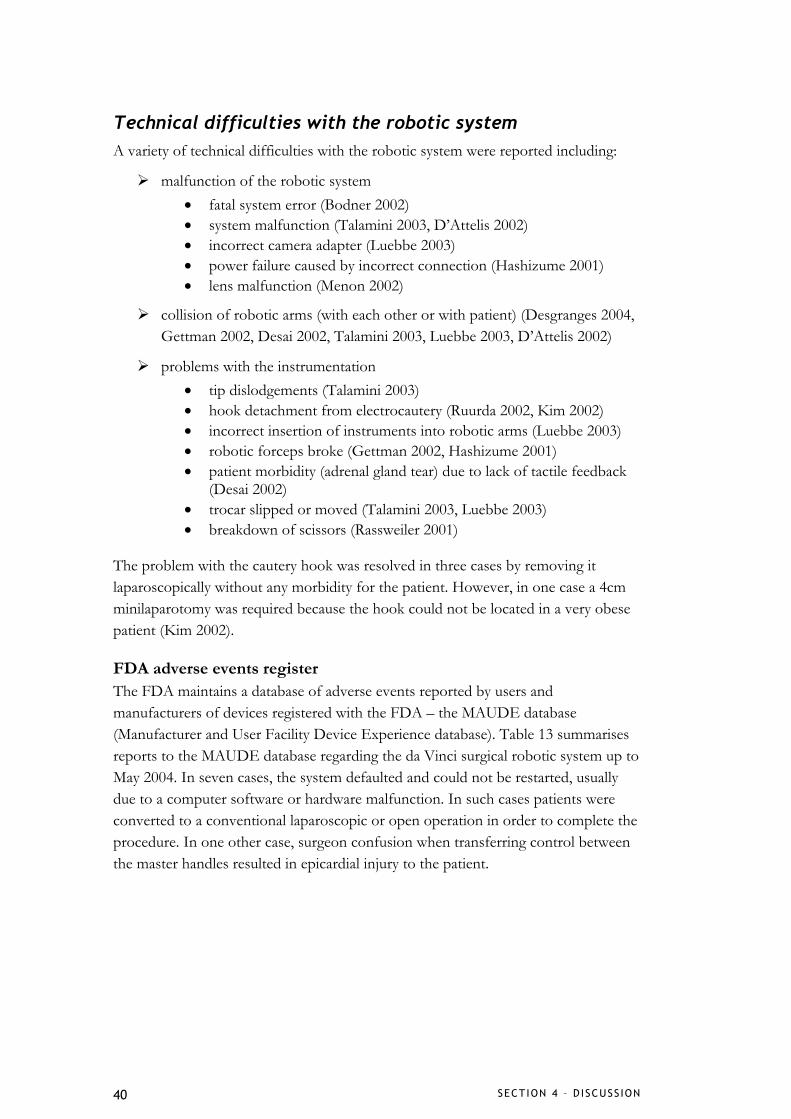
SECT ION 4 – D ISCUSS ION 40
Technical difficulties with the robotic system A variety of technical difficulties with the robotic system were reported including:
malfunction of the robotic system • fatal system error (Bodner 2002) • system malfunction (Talamini 2003, D’Attelis 2002) • incorrect camera adapter (Luebbe 2003) • power failure caused by incorrect connection (Hashizume 2001) • lens malfunction (Menon 2002)
collision of robotic arms (with each other or with patient) (Desgranges 2004, Gettman 2002, Desai 2002, Talamini 2003, Luebbe 2003, D’Attelis 2002)
problems with the instrumentation • tip dislodgements (Talamini 2003) • hook detachment from electrocautery (Ruurda 2002, Kim 2002) • incorrect insertion of instruments into robotic arms (Luebbe 2003) • robotic forceps broke (Gettman 2002, Hashizume 2001) • patient morbidity (adrenal gland tear) due to lack of tactile feedback
(Desai 2002) • trocar slipped or moved (Talamini 2003, Luebbe 2003) • breakdown of scissors (Rassweiler 2001)
The problem with the cautery hook was resolved in three cases by removing it laparoscopically without any morbidity for the patient. However, in one case a 4cm minilaparotomy was required because the hook could not be located in a very obese patient (Kim 2002).
FDA adverse events register The FDA maintains a database of adverse events reported by users and manufacturers of devices registered with the FDA – the MAUDE database (Manufacturer and User Facility Device Experience database). Table 13 summarises reports to the MAUDE database regarding the da Vinci surgical robotic system up to May 2004. In seven cases, the system defaulted and could not be restarted, usually due to a computer software or hardware malfunction. In such cases patients were converted to a conventional laparoscopic or open operation in order to complete the procedure. In one other case, surgeon confusion when transferring control between the master handles resulted in epicardial injury to the patient.
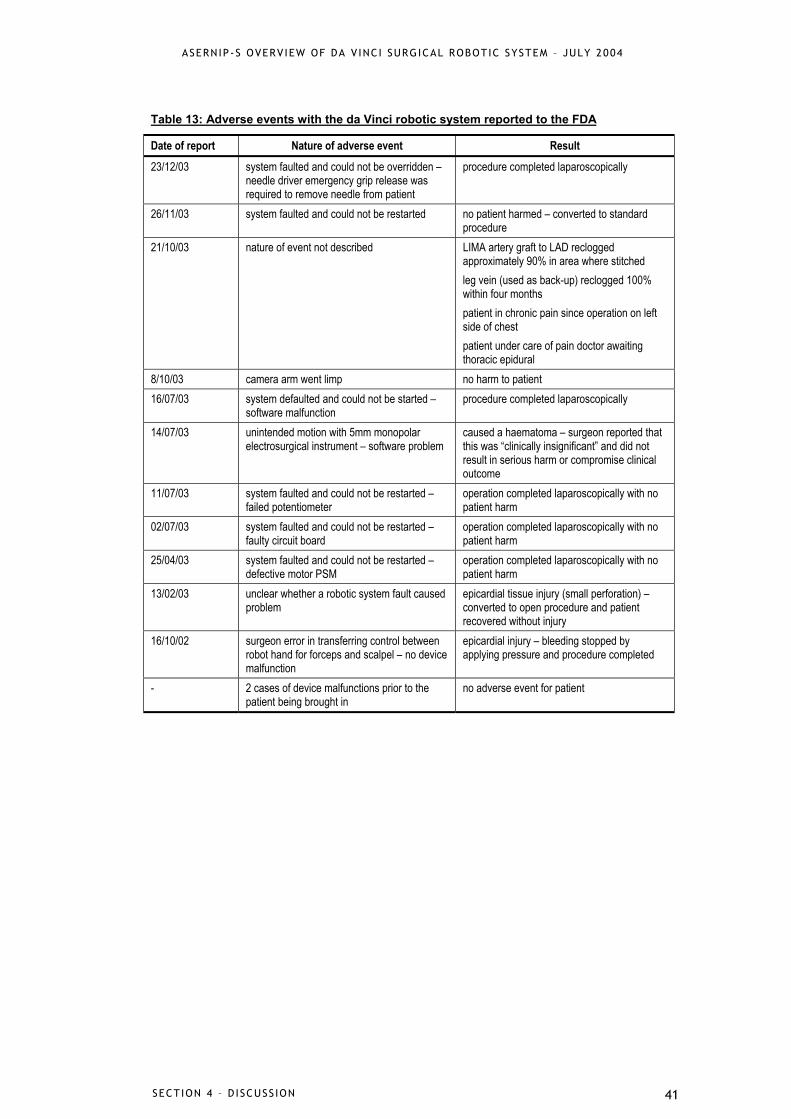
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 4 – D ISCUSS ION 41
Table 13: Adverse events with the da Vinci robotic system reported to the FDA
Date of report Nature of adverse event Result 23/12/03 system faulted and could not be overridden –
needle driver emergency grip release was required to remove needle from patient
procedure completed laparoscopically
26/11/03 system faulted and could not be restarted no patient harmed – converted to standard procedure
21/10/03 nature of event not described LIMA artery graft to LAD reclogged approximately 90% in area where stitched leg vein (used as back-up) reclogged 100% within four months patient in chronic pain since operation on left side of chest patient under care of pain doctor awaiting thoracic epidural
8/10/03 camera arm went limp no harm to patient 16/07/03 system defaulted and could not be started –
software malfunction procedure completed laparoscopically
14/07/03 unintended motion with 5mm monopolar electrosurgical instrument – software problem
caused a haematoma – surgeon reported that this was “clinically insignificant” and did not result in serious harm or compromise clinical outcome
11/07/03 system faulted and could not be restarted – failed potentiometer
operation completed laparoscopically with no patient harm
02/07/03 system faulted and could not be restarted – faulty circuit board
operation completed laparoscopically with no patient harm
25/04/03 system faulted and could not be restarted – defective motor PSM
operation completed laparoscopically with no patient harm
13/02/03 unclear whether a robotic system fault caused problem
epicardial tissue injury (small perforation) – converted to open procedure and patient recovered without injury
16/10/02 surgeon error in transferring control between robot hand for forceps and scalpel – no device malfunction
epicardial injury – bleeding stopped by applying pressure and procedure completed
- 2 cases of device malfunctions prior to the patient being brought in
no adverse event for patient
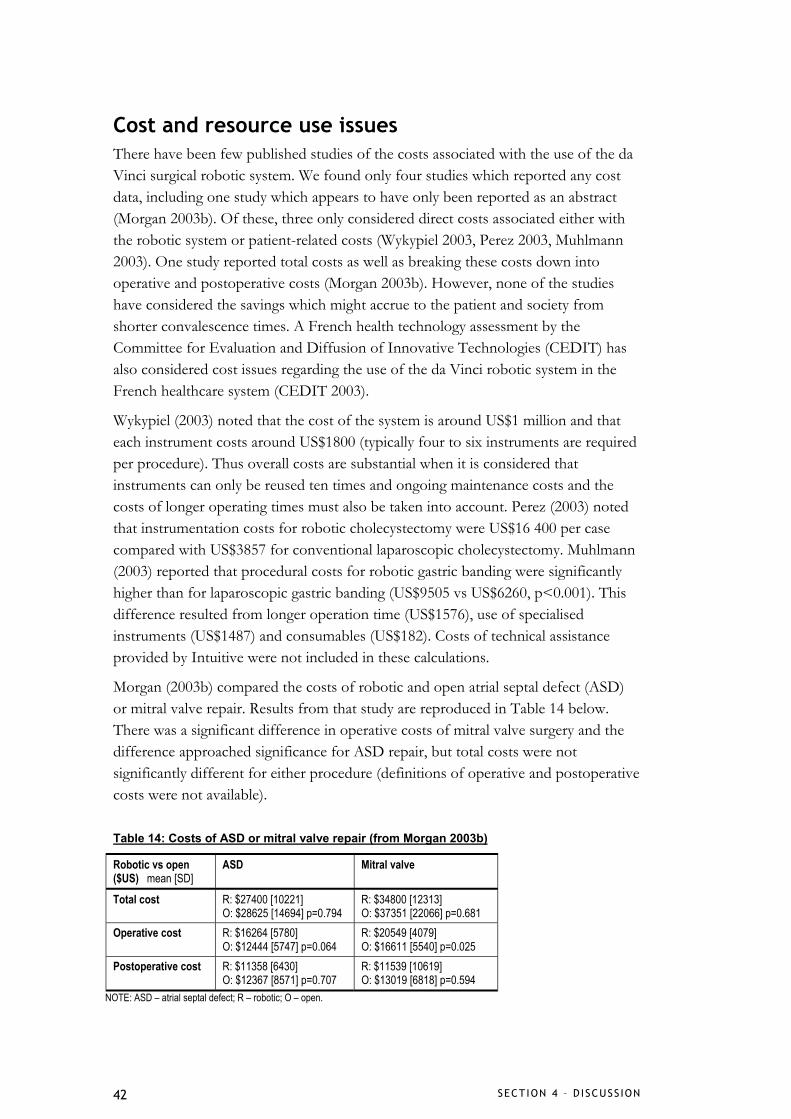
SECT ION 4 – D ISCUSS ION 42
Cost and resource use issues There have been few published studies of the costs associated with the use of the da Vinci surgical robotic system. We found only four studies which reported any cost data, including one study which appears to have only been reported as an abstract (Morgan 2003b). Of these, three only considered direct costs associated either with the robotic system or patient-related costs (Wykypiel 2003, Perez 2003, Muhlmann 2003). One study reported total costs as well as breaking these costs down into operative and postoperative costs (Morgan 2003b). However, none of the studies have considered the savings which might accrue to the patient and society from shorter convalescence times. A French health technology assessment by the Committee for Evaluation and Diffusion of Innovative Technologies (CEDIT) has also considered cost issues regarding the use of the da Vinci robotic system in the French healthcare system (CEDIT 2003).
Wykypiel (2003) noted that the cost of the system is around US$1 million and that each instrument costs around US$1800 (typically four to six instruments are required per procedure). Thus overall costs are substantial when it is considered that instruments can only be reused ten times and ongoing maintenance costs and the costs of longer operating times must also be taken into account. Perez (2003) noted that instrumentation costs for robotic cholecystectomy were US$16 400 per case compared with US$3857 for conventional laparoscopic cholecystectomy. Muhlmann (2003) reported that procedural costs for robotic gastric banding were significantly higher than for laparoscopic gastric banding (US$9505 vs US$6260, p<0.001). This difference resulted from longer operation time (US$1576), use of specialised instruments (US$1487) and consumables (US$182). Costs of technical assistance provided by Intuitive were not included in these calculations.
Morgan (2003b) compared the costs of robotic and open atrial septal defect (ASD) or mitral valve repair. Results from that study are reproduced in Table 14 below. There was a significant difference in operative costs of mitral valve surgery and the difference approached significance for ASD repair, but total costs were not significantly different for either procedure (definitions of operative and postoperative costs were not available).
Table 14: Costs of ASD or mitral valve repair (from Morgan 2003b)
Robotic vs open ($US) mean [SD]
ASD Mitral valve
Total cost R: $27400 [10221] O: $28625 [14694] p=0.794
R: $34800 [12313] O: $37351 [22066] p=0.681
Operative cost R: $16264 [5780] O: $12444 [5747] p=0.064
R: $20549 [4079] O: $16611 [5540] p=0.025
Postoperative cost R: $11358 [6430] O: $12367 [8571] p=0.707
R: $11539 [10619] O: $13019 [6818] p=0.594
NOTE: ASD – atrial septal defect; R – robotic; O – open.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 4 – D ISCUSS ION 43
The French CEDIT report estimated the costs likely to be associated with the use of a da Vinci surgical robotic system for cardiac surgery in the French healthcare system in 2002 (Table 15).
Table 15: Estimated costs of robotic cardiac surgery in the French healthcare system in
Item Cost estimate in euros capital outlay (including warranty, shipping, installation, training) 1.1 – 1.2 million maintenance contract 100,000 per year total annual operating costs of already installed system 230,000 first year operating costs (including purchase of new system) 1.3 million total annual additional cost incurred (annuity for depreciation, operating costs including financial charges)
365,000
Training and learning curve issues
Training In the United States a number of robotic training programs have been developed by different centres including the University of California, Irvine (UCI), the Brody School of Medicine at East Carolina University (ECU), North Carolina, the University of Southern California and St Luke’s Roosevelt Hospital, New York. The UCI program has been described in detail in Chitwood (2001). The UCI curriculum consists of five levels of training, starting with lectures regarding the technical aspects of the robotic system and its limitations, and then working through practice in the inanimate and animal laboratories, to practice on cadavers, and observation of robotic-assisted procedures, before finally graduating to the clinical setting. A similar staged program is described by Boehm (2003). Training courses typically last two to five days.
Bonatti (2004) describes training in robotic-assisted totally endoscopic coronary artery bypass (TECAB) which also uses a staged approach where the trainee works through the various elements of a full TECAB procedure (i.e. internal thoracic artery takedown, pericardial lipectomy and pericardiotomy, anastomoses) practicing the earlier stages many times before completing a full TECAB.
Several aspects of training appear to be particularly important. The whole operating room team must be trained – doctors, nurses, anaesthetic and other staff – with a focus on team cohesion in the operative setting (Hashizume & Sugimachi 2003, Chitwood 2001, Boehm 2003). The training of the surgical assistant is also very important as this is a key point of contact with the patient for the operating surgeon (Boehm 2003). Previous experience with minimally invasive techniques is also expected to shorten learning curves and improve outcomes (Boehm 2003, Hashizume & Sugimachi 2003).
SECT ION 4 – D ISCUSS ION 44
Learning curve It is clear there is a significant learning curve when transferring conventional laparoscopic or open skills into the robotic-assisted environment. A learning or volume effect was evident in a number of the included studies (where patient results were divided into cohorts of early and late experience) and could be inferred by comparing operative times from many of the small case series with larger series for the same procedure (where operative times are generally shorter for larger series). In addition to those results outlined in the literature review, we found two additional studies which had focused on learning curve issues specifically.
Chitwood (2001) compared a number of aspects of cholecystectomy, mitral valve repair, and Nissen fundoplication in both an experimental setting (i.e. in an animal body part) and in a clinical setting. Their experience was split into two groups representing the first 50% of procedures and the second 50%. For experimental cholecystectomy they found that robotic set-up, port placement, duct/artery dissection, gall bladder dissection and total procedure time were significantly shorter in the second group. However, in the clinical setting only duct artery dissection and total robotic and procedure time were significantly shorter. In experimental mitral valve repair they found that robotic set-up time and total band time were significantly shorter for the second group. However, in the clinical setting only draping, suture and knot tying were shorter, although the number of sutures/bands per procedure was higher suggesting more bands were placed in less time after more experience. In fundoplication hiatal dissection, suture placement and total procedure time were significantly shorter in the second group. In the clinical setting only total robotic and procedure time was significantly shorter. Chitwood (2001) suggest that as their experience increased the complexity of the surgery increased and the surgeons became more efficient hence the reduction in total robotic and procedure times.
Bonatti (2004) calculated surgical learning curves for their experience with internal thoracic artery (ITA) takedown, total endoscopic coronary artery bypass (TECAB) and ITA anastomosis. Operative times decreased from 180 minutes to 50 minutes for ITA takedown (p<0.001) and from 9 hours to 6 hours for TECAB (p=0.028). However, there was no significant learning curve effect for ITA anastomosis. The authors suggest that much of the primary learning occurred during the ITA takedown phase and that may account for the lack of learning curve for anastomosis. Also, training in anastomosis was completed in pig hearts prior to the clinical setting probably reducing the clinical learning curve further. The learning curve effect seen with the full TECAB was thought to reflect the cumulative learning curves of the phased training program (see p.44) and what the authors call “a potentiating effect” when each of the previous training phases is mastered.
An interesting area of development in this regard is the possibility of using telemetry within the da Vinci surgical system to reconstruct the surgeon’s movements during a
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 4 – D ISCUSS ION 45
procedure using flight path analysis. Such a process has been described and could be used to measure expertise objectively and monitor surgical learning curves (Verner 2003).

SECT ION 5 - CONCLUS IONS 46
5. Conclusions Surgical robotics offers a number of advantages over conventional laparoscopic and open surgery and these benefits were evident in the studies of the da Vinci surgical robotic system included in this overview. The use of the robotic system enabled minimally invasive approaches to be used where otherwise an open approach would have to be used. This led to shorter lengths of hospital stay and less blood loss (in those studies where it was reported). However, these benefits were not as clear in comparisons of conventional laparoscopic and robotic surgery. There may be some complex surgeries where a laparoscopic approach, whether robotic-assisted or not, may be so technically difficult that an open approach is preferred (for example some gastric surgeries).
A number of complications were experienced in many of the included studies, some related to the use of the robotic system, and others procedural. A relationship between the number of complications and the number of patients requiring conversion to the laparoscopic or open procedure was noted, and it was suggested that this may reflect the steep learning curve for robotic-assisted surgery. This learning curve was most evident in the consistently longer operative times reported in most studies (in case series, many authors commented on this in comparison to their experience with conventional surgery, even though a formal comparison was not made). Set-up times with the robotic system were a key element of the learning curve which appeared to shorten with experience; however, there may be some upper limit to set-up time efficiency which cannot be improved with the current da Vinci system. If the learning curve can be overcome (or if a centre performs a sufficient number of robotic-assisted surgeries) it may be reasonable to expect that operative times could approach those of conventional laparoscopic surgery.6
The initial cost of the da Vinci system is substantial, and ongoing maintenance and equipment costs are also significant. As with any computer-based technology, frequent software and hardware upgrade could be expected to add to ongoing costs.7 In addition to the costs of the system, the cost of training (both the operating surgeons and the operating room team) must also be considered. In the initial stages a high level of technical support from the manufacturer will probably be needed to ensure that system problems do not affect patient safety.
At the present time there is insufficient evidence to make many useful comparisons of robotic-assisted and conventional laparoscopic surgery, particularly in regard to the cost-effectiveness of robotic-assisted surgery.
6 If the robotic system is used more routinely it may be possible that some elements of the set-up will be in place and that the operating room itself will evolve to incorporate the surgical robot. 7 The average useful life of the da Vinci system has been estimated to be five years, with components lasting four to seven years (Hartford Hospital, 2003)

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
SECT ION 5 - CONCLUS IONS 47
There is also scarce information about the long-term (or even medium-term) efficacy of robotic-assisted surgery. In addition, little consideration has been given in the literature to the acceptability of robotic surgery to patients. Given the substantial costs involved, high quality randomised trials are required to determine the efficacy and safety of robotic-assisted surgery, and thorough economic analyses should also be conducted. Those contemplating the purchase of a da Vinci surgical robotic system should consider whether sufficient procedures can be done to overcome the learning/volume effect and offset the start-up and fixed costs associated with the system.
REFERENCES 48
References
Abbou C, Hoznek A, Salomon L, Olsson L, Lobontiu A, Saint F, Cicco A, Antiphon P, Chopin D. Laparoscopic radical prostatectomy with a remote controlled robot. Journal of Urology 2001; 165(6 Pt 1): 1964-1966.
Ahlering T, Skarecky D, Lee D, Clayman R. Successful transfer of open surgical skills to a laparoscopic environment using a robotic interface: initial experience with laparoscopic radical prostatectomy. Journal of Urology 2003; 170(5): 1738-1741.
Argenziano M, Oz M, Kohmoto T, Morgan J, Dimitui J, Mongero L, Beck J, Smith C. Totally endoscopic atrial septal defect repair with robotic assistance. Circulation 2003; 108(Suppl II): II-191-II-194.
Ashton R, McGinnis K, Connery C, Swistel D, Ewing D, DeRose J. Totally endoscopic robotic thymectomy for myasthenia gravis. Annals of Thoracic Surgery 2003; 75(2): 569-571.
Autschbach R, Onnasch JF, Falk V, Walther T, Kruger M, Schilling L, Mohr F. The Leipzig experience with robotic valve surgery. Journal of Cardiac Surgery 2000; 15(1): 82-87.
Bacchetta M, Korst R, Altorki N, Port J, Isom O, Mack C. Resection of a symptomatic pericardial cyst using the computer-enhanced da Vinci Surgical System. Annals of Thoracic Surgery 2003; 75(6): 1953-1955.
Ballantyne G, Moll F. The da Vinci telerobotic surgical system: the virtual operative field and telepresence surgery. Surgical Clinics of North America 2003; 83(6): 1293-1304.
Beecken W, Wolfram M, Engl T, Bentas W, Probst M, Blaheta R, Oertl A, Jonas D, Binder J. Robotic-assisted laparoscopic radical cystectomy and intra-abdominal formation of an orthotopic ileal neobladder. European Urology 2003; 44(3): 337-339.
Bentas W, Wolfram M, Jones J, Brautigam R, Kramer W, Binder J. Robotic technology and the translation of open radical prostatectomy to laparoscopy: the early Frankfurt experience with robotic radical prostatectomy and one year follow-up. European Urology 2003a; 44(2): 175-181.
Bentas W, Wolfram M, Brautigam R, Probst M, Beecken W, Jonas D, Binder J. Da Vinci robot assisted Anderson-Hynes dismembered pyeloplasty: technique and 1 year follow-up. World Journal of Urology 2003b; 21(3): 133-138.
Beohm D, Arnold M, Detter C, Reichenspurner H. Incorporating robotics into an open-heart program. Surgical Clinics of North America 2003; 83(6): 1369-1380.
Bodner J, Schmid T, Wykypiel H, Bodner E. First experiences with robotic-assisted laparoscopic cholecystectomies. European Surgery - Acta Chirurgica Austriaca Supplement 2002; 34(3): 166-169.
Bonatti J, Schachner T, Bernecker O, Chevtchik O, Bonaros N, Ott H, Freidrich F, Laufer G. Robotic totally endoscopic coronary artery bypass: Program development and learning curve. Journal of Thoracic & Cardiovascular Surgery 2004; 127(2): 504-510.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
REFERENCES 49
Bucerius J, Metz S, Walther T, Falk V, Doll N, Noack F, Holzhey D, Diegeler A, Mohr F. Endoscopic internal thoracic artery dissection leads to significant reduction of pain after minimally invasive direct coronary artery bypass graft surgery. Annals of Thoracic Surgery 2002; 73(4): 1180-1184.
Cadiere G. Evaluation of telesurgical (robotic) NISSEN fundoplication. Surgical Endoscopy 2001; 15(9): 918-923.
Cadiere G, Himpens J, Germay O, Izizaw R, Degueldre M, Vandromme J, Capelluto E, Bruyns J. Feasibility of robotic laparoscopic surgery: 146 cases. World Journal of Surgery 2001; 25(11): 1467-1477.
CEDIT. Robotic surgery using telemanipulators. Paris: Committee for Evaluation and Diffusion of Innovative Technologies - Assistance Publique Hôpitaux de Paris, 2002. Available online: http://cedit.aphp.fr/english/f_pub_cedit_menu.html. Accessed April 5, 2004.
Chapman W, Young J, Albrecht R, Kim V, Nifong L, Chitwood W. Robotic Nissen fundoplication: alternative surgical technique for the treatment of gastroesophageal reflux disease. Journal of Laparoendoscopic & Advanced Surgical Techniques.Part A 2001; 11(1): 27-30.
Chitwood W, Nifong L, Chapman W, Felger J, Bailey B, Ballint T, Mendleson K, Kim V, Young J, Albrecht R. Robotic surgical training in an academic institution. Annals of Surgery 2001; 234(4): 475-484.
D'Attellis N, Loulmet D, Carpentier A, Berrebi A, Cardon C, Severac-Bastide R, Fabiani J, Safran D. Robotic-assisted cardiac surgery: anesthetic and postoperative considerations. Journal of Cardiothoracic & Vascular Anesthesia 2002; 16(4): 397-400.
DeRose J, Swistel D, Safavi A, Connery C, Ashton R. Mediastinal mass evaluation using advanced robotic techniques. Annals of Thoracic Surgery 2003; 75(2): 571-573.
Desai M, Gill I, Kaouk J, Matin S, Sung G, Bravo E. Robotic-assisted laparoscopic adrenalectomy. Urology 2002; 60(6): 1104-1107.
DesgrangesP, Bourriez A, Javerliat I, Van Laere O, Melliere D, Becquemin J. Robotically assisted aorto-femoral bypass grafting: lessons learned from our initial experience. European Journal of Endovascular Surgery 2004; In press.
Di Marco D, Chow G, Gettman M, Elliott D. Robotic-assisted laparoscopic sacrocolpopexy for treatment of vaginal vault prolapse. Urology 2004; 63(2): 373-376.
Dogan S, Aybek T, Andressen E, Byhahn C, Mierdl S, Westphal K, Matheis G, Moritz A, Wimmer-Greinecker G. Totally endoscopic coronary artery bypass grafting on cardiopulmonary bypass with robotically enhanced telemanipulation: report of forty-five cases. Journal of Thoracic & Cardiovascular Surgery 2002a; 123(6): 1125-1131.
Dogan S, Aybek T, Khan MF, Neidhart G, Auch-Schwelk W, Moritz A, Wimmer-Greinecker G. Totally endoscopic bilateral internal thoracic artery bypass grafting in a young diabetic patient. Medical Science Monitor 2002b; 8(12): CS95-CS97.
Dogan S, Aybek T, Westphal K, Mierdl S, Moritz A, Wimmer-Greinecker G. Computer-enhanced totally endoscopic sequential arterial coronary artery bypass. Annals of Thoracic Surgery 2001; 72(2): 610-611.
REFERENCES 50
Gettman M, Hoznek A, Salomon L, Katz R, Borkowski T, Antiphon P, Lobontiu A, Abbou C. Laparoscopic radical prostatectomy: description of the extraperitoneal approach using the da Vinci robotic system. Journal of Urology 2003; 170(2 Pt 1): 416-419.
Gettman M, Peschel R, Neururer R, Bartsch G. A comparison of laparoscopic pyeloplasty performed with the daVinci robotic system versus standard laparoscopic techniques: initial clinical results. European Urology 2002; 42(5): 453-457.
Giulianotti P, Coratti A, Angelini M, Sbrana F, Cecconi S, Balestracci T, Caravaglios G. Robotics in general surgery: personal experience in a large community hospital. Archives of Surgery 2003; 138(7): 777-784.
Gutt C, Markus B, Kim Z, Meininger D, Brinkmann L, Heller K. Early experiences of robotic surgery in children. Surgical Endoscopy 2002; 16(7): 1083-1086.
Hashizume M, Sugimachi K. Robot-assisted gastric surgery. Surgical Clinics of North America 2003; 83(6): 1429-1444.
Hartford Hospital. Acquisition of a da Vinci surgical system. Office of Health Care Access Certificate of Need Application. Docket number 03-30049, Filed August 7, 2003. Accessed at: www.ocha.state.ct.us/CONFiles/CONDecisions/03-30049.pdf. Accessed on 03/06/04.
Heller K, Gutt C, Schaeff B, Beyer P, Markus B. Use of the robot system Da Vinci for laparoscopic repair of gastro-oesophageal reflux in children. European Journal of Pediatric Surgery 2002; 12(4): 239-242.
Horgan S, Vanuno D. Robots in laparoscopic surgery. Journal of Laparoendoscopic & Advanced Surgical Techniques.Part A 2001; 11(6): 415-419.
Horgan S, Vanuno D, Sileri P, Cicalese L, Benedetti E. Robotic-assisted laparoscopic donor nephrectomy for kidney transplantation. Transplantation 2002; 73(9): 1474-1479.
Hourmont K, Chung W, Pereira S, Wasielewski A, Davies R, Ballantyne G. Robotic versus telerobotic laparoscopic cholecystectomy: duration of surgery and outcomes. Surgical Clinics of North America 2003; 83(6): 1445-1462.
Hoznek A, Zaki SK, Samadi D, Salomon L, Lobontiu A, Lang P, Abbou C. Robotic assisted kidney transplantation: an initial experience. Journal of Urology 2002; 167(4): 1604-1606.
Kaouk J, Desai M, Abreu S, Papay F, Gill I. Robotic assisted laparoscopic sural nerve grafting during radical prostatectomy: initial experience. Journal of Urology 2003; 170(3): 909-912.
Kappert U, Cichon R, Gulielmos V, Schneider J, Schramm I, Nicolai J, Tugtekin S, Schueler S. Robotic-enhanced Dresden technique for minimally invasive bilateral internal mammary artery grafting. Heart Surgery Forum 2000a; 3(4): 319-321.
Kappert U, Cichon R, Schneider J, Gulielmos V, Ahmadzade T, Nicolai J, Tugtekin S, Schueler S. Technique of closed chest coronary artery surgery on the beating heart. European Journal of Cardio-Thoracic Surgery 2001; 20(4): 765-769.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
REFERENCES 51
Kappert U, Schneider J, Cichon R, Gulielmos V, Matschke K, Tugtekin S, Schuler S. Wrist-enhanced instrumentation: moving toward totally endoscopic coronary artery bypass grafting. Annals of Thoracic Surgery 2000b; 70(3): 1105-1108.
Killewich L, Cindrick-Pounds L, Gomez G. Robot-assisted laparoscopic aortic reconstruction for occlusive disease: A case report. Vascular & Endovascular Surgery 2004; 38(1): 83-87.
Kim V, Chapman W, Albrecht R, Bailey B, Young J, Nifong L, Chitwood W. Early experience with telemanipulative robot-assisted laparoscopic cholecystectomy using da Vinci. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 2002; 12(1): 33-40.
Luebbe B, Woo R, Wolf S, Irish M. Robotically assisted minimally invasive surgery in a pediatric population: Initial experience, technical considerations, and description of the da Vinci surgical system. Pediatric Endosurgery & Innovative Techniques 2003; 7(4): 385-402.
Melfi F, Menconi G, Mariani A, Angeletti C. Early experience with robotic technology for thoracoscopic surgery. European Journal of Cardio-Thoracic Surgery 2002; 21(5): 864-868.
Melvin W, Needleman B, Krause K, Ellison E. Robotic resection of pancreatic neuroendocrine tumor. Journal of Laparoendoscopic & Advanced Surgical Techniques.Part A 2003; 13(1): 33-36.
Melvin W, Needleman B, Krause K, Schneider F, Ellison E. Computer-enhanced vs standard laparoscopic antireflux surgery. Journal of Gastrointestinal Surgery 2002; 6(1): 11-16.
Melvin W, Needleman B, Krause K, Wolf R, Michler R, Ellison E. Computer-assisted robotic heller myotomy: initial case report. Journal of Laparoendoscopic & Advanced Surgical Techniques.Part A 2001; 11(4): 251-253.
Menon M, Hemal A, Tewari A, Shrivastava A, Shoma A, Abol-Enein H, Ghoneim M. Robot-assisted radical cyctectomy and urinary diversion in femal patients: technique with preservation of the uterus and vagina. Journal of the American College of Surgeons 2004; 198(3): 386-393.
Menon M, Tewari A, Peabody J, The VIP Team. Vattikuti Institute prostatectomy: technique. Journal of Urology 2003a; 169(6): 2289-2292.
Menon M, Hemal A, Tewari A, Shrivastava A, Shoma A, El Tabey N, Shaaban A, Abol-Enein H, Ghoneim M. Nerve-sparing robot-assisted radical cystoprostatectomy and urinary diversion. BJU International 2003b; 92(3): 232-236.
Menon M, Tewari A, Baize B, Guillonneau B, Vallancien G. Prospective comparison of radical retropubic prostatectomy and robot-assisted anatomic prostatectomy: the Vattikuti Urology Institute experience. Urology 2002; 60(5): 864-868.
Mierdl S, Byhahn C, Dogan S, Aybek T, Wimmer-Greinecker G, Kessler P, Meininger D, Westphal K. Segmental wall motion abnormalities during telerobotic totally endoscopic coronary artery bypass grafting. Anesthesia & Analgesia 2002; 94(4): 774-780.
Mohr F, Falk V, Diegeler A, Walther T, Gummert J, Bucerius J, Jacobs S, Autschbach R. Computer-enhanced "robotic" cardiac surgery: experience in 148 patients. Journal of Thoracic & Cardiovascular Surgery 2001; 121(5): 842-853.

REFERENCES 52
Morgan J, Thornton B, Hollingsworth K, Colletti N, Kohmoto T, Kherani A, Vigilance D, Cheema F, Garrido M, Naka Y, Rose E, Smith C, Oz M. Does robotic technology make minimally invasive cardiac surgery too expensive? A hospital cost analysis of robotic and conventional techniques. Heart Surgery Forum 2003a; 6(2): 114.
Morgan J, Ginsburg M, Sonett J, Morales D, Kohmoto T, Gorenstein L, Smith C, Argenziano M. Advanced thoracoscopic procedures are facilitated by computer-aided robotic technology. European Journal of Cardio-Thoracic Surgery 2003b; 23(6): 883-887.
Muhlmann G, Klaus A, Kirchmayr W, Wykypiel H, Unger A, Holler E, Nehoda H, Aigner F, Weiss HG. DaVinci robotic-assisted laparoscopic bariatric surgery: Is it justified in a routine setting? Obesity Surgery 2003; 13(6): 848-854.
Munz Y, Moorthy K, Kudchadkar R, Hernandez J, Martin S, Darzi A, Rockall T. Robotic assisted rectopexy. American Journal of Surgery 2004; 187(1): 88-92.
Nifong L, Chu V, Bailey B, Maziarz D, Sorrell V, Holbert D, Chitwood W. Robotic mitral valve repair: experience with the da Vinci system. Annals of Thoracic Surgery 2003; 75(2): 438-442.
Pasticier G, Rietbergen J, Guillonneau B, Fromont G, Menon M, Vallancien G. Robotically assisted laparoscopic radical prostatectomy: feasibility study in men. European Urology 2001; 40(1): 70-74.
Perez A, Zinner M, Ashley S, Brooks D, Whang E. What is the value of telerobotic technology in gastrointestinal surgery? Surgical Endoscopy 2003; 17(5): 811-813.
Rassweiler J, Frede T, Seemann O, Stock C, Sentker L. Telepresence surgery: First experiences with laparoscopic radical prostatectomy. Minimally Invasive Therapy & Allied Technologies 2001a; 10(6): 261-270.
Rassweiler J, Frede T, Seemann O, Stock C, Sentker L. Telesurgical laparoscopic radical prostatectomy: Initial experience. European Urology 2001b; 40(1): 75-83.
Resley J, Fitzgerald D, Albus R, Massimiano P. Pericardial patch closure of an atrial septal defect using endoscopic robotic technology. Perfusion 2003; 18(6): 365-367.
Ruurda J, Simmermacher R, Borel R, Broeders I. Robotic surgery in a routine procedure an evaluation of 40 robot-assisted laparoscopic cholecystectomies. European Surgery - Acta Chirurgica Austriaca Supplement 2002; 34(3): 170-172.
Schwarzler P, Fessler S, Marth C. Robot-assisted laparoscopic surgery in gynaecology: First experiences and review of the literature. European Surgery - Acta Chirurgica Austriaca Supplement 2002; 34(3): 180-182.
Talamini M, Chapman S, Horgan S, Melvin W. A prospective analysis of 211 robotic-assisted surgical procedures. Surgical Endoscopy 2003; 17(10): 1521-1524.
Torracca L, Ismeno G, Franze V, Alfieri O. The use of robotic technology in the LAST operation. Italian Heart Journal 2001; 2(12): 900-903.
Torracca L, Ismeno G, Quarti A, Alfieri O. Totally endoscopic atrial septal defect closure with a robotic system: experience with seven cases. Heart Surgery Forum 2002; 5(2): 125-127.

ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
REFERENCES 53
Verner L, Oleynikov D, Holtmann JZL. Measurements of the level of surgical expertise using flight path analysis from the da Vinci robotic surgery system. Studies in Health Technology and Informatics - Medicine Meets Virtual Reality 2003; 94: 373-378.
Wimmer-Greinecker G, Dogan S, Aybek T, Khan MF, Mierdl S, Byhahn C, Moritz A. Totally endoscopic atrial septal repair in adults with computer-enhanced telemanipulation. Journal of Thoracic & Cardiovascular Surgery 2003; 126(2): 465-468.
Wolfram M, Brautigam R, Engl T, Bentas W, Heitkamp S, Ostwald M, Kramer W, Binder J, Blaheta R, Jonas D, Beecken W. Robotic-assisted laparoscopic radical prostatectomy: the Frankfurt technique. World Journal of Urology 2003; 21(3): 128-132.
Wykypiel H, Wetscher GJ, Klaus A, Schmid T, Gadenstaetter M, Bodner J, Bodner E. Robot-assisted laparoscopic partial posterior fundoplication with the DaVinci system: Initial experiences and technical aspects. Langenbecks Archives of Surgery 2003; 387(11-12): 411-416.
Yoshino I, Hashizume M, Shimada M, Tomikawa M, Sugimachi K. Video-assisted thoracoscopic extirpation of a posterior mediastinal mass using the da Vinci computer enhanced surgical system. Annals of Thoracic Surgery 2002; 74(4): 1235-1237.
Yoshino I, Hashizume M, Shimada M, Tomikawa M, Tomiyasu M, Suemitsu R, Sugimachi K. Thoracoscopic thymomectomy with the da Vinci computer-enhanced surgical system. Journal of Thoracic & Cardiovascular Surgery 2001; 122(4): 783-785.
Young J, Chapman W, Kim V, Albrecht R, Ng P, Nifong L, Chitwood R. Robotic-assisted adrenalectomy for adrenal incidentaloma: Case and review of the technique. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 2002; 12(2): 126-130.

APPENDIX A 54
NOTE: First authors of included papers are shown in bold.
Appendix A – Centres publishing results of da Vinci robotic-assisted surgery
United States
Group Specialties Authors UNITED STATES Mayo Clinic, Department of Urology, Rochester, Minnesota
urology DiMarco, Chow, Gettman, Elliott
Cleveland Clinic, Section of Laparoscopic and Minimally Invasive Surgery, Urological Institute, Cleveland, Ohio
urology Kaouk, Desai, Abreu, Papy, Gill, Matin, Sung, Bravo
Vattikuti Urology Institute, Henry Ford Hospital, Detroit, Michigan
urology Menon, Hemal, Tewari, Shrivastava
University of Illinois at Chicago Medical Centre, Minimally Invasive Surgery Centre Chicago, Illinois
urology Horgan, Vanuno, Sileri, Cicalese, Benedetti
Case Western Reserve University School of Medicine, Department of Urology, Cleveland, Ohio
urology Menon, Tewari, Peabody
University of California Irvine, Department of Urology, Orange, California
urology Ahlering, Skarecky, Clayman
Ohio State University Medical Center, Department of Surgery, Columbus, Ohio
general Melvin, Needleman, Krause, Ellison, Schneider, Wolf, Michler
The Brody School of Medicine, East Carolina University, Department of Surgery, Greenville, North Carolina
general cardiac
Young, Chapman, Kim, Albrecht, Ng, Nifong, Chitwood, Chu, Bailey, Maziarz, Sorrell, Holbert, Wixon, Elbeery, Moran, Lust
Hackensack University Medical Center, Minimally Invasive and Telerobotic Surgery Institute, Hackensack, USA
general Hourmont, Chung, Pereira, Wasielewski, Davies, Ballantyne
Brigham and Women’s Hospital, Harvard Medical School, Department of Surgery and Division of Minimally Invasive Surgery, Boston, Massachussettes
general Perez, Zinner, Ashley, Brooks, Whang
New York Presbyterian Hospital – Weill Cornell Medical Center, Department of Cardiothoracic Surgery, New York
thoracic Bacchetta, Korst, Altorki, Port, Isom, Mack
College of Physicians and Surgeons, Columbia University, New York St Luke’s Roosevelt Hospital Center
thoracic Morgan, Ginsburg, Sonett, Morales, Kohmoto, Gorenstein, Smith, Argenziano, Oz, Dimitui, Mongero, Beck, Smith Ashton, McGinnis, Connery, Swistel, Ewing, DeRose, Safavi
University of Texas Medical Branch, Division of Minimally Invasive Surgery, Department of Surgery, Galverston, Texas
vascular Killewich, Cindrick-Pounds, Gomez
Iowa Methodist Medical Center, Des Moines, Iowa
paediatric Luebbe
Blank Children’s Hospital, Des Moines, Iowa
paediatric Wolf, Irish
INOVA Fairfax Hospital, Department of Cardiovascular Surgery, Falls Church Virginia
cardiac Resley, Fitzgerald, Albus, Massimiano
Johns Hopkins University School of Medicine, Department of Surgery, Baltimore, Maryland
multiple Talamini
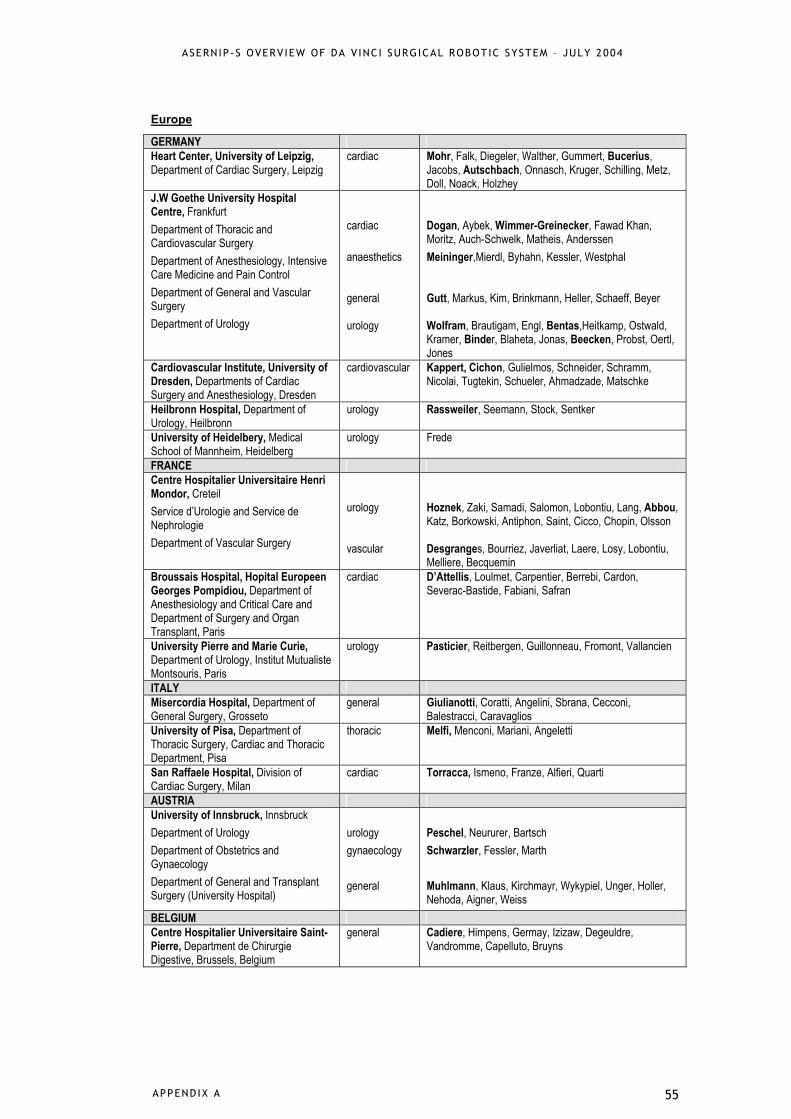
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
APPENDIX A 55
Europe
GERMANY Heart Center, University of Leipzig, Department of Cardiac Surgery, Leipzig
cardiac Mohr, Falk, Diegeler, Walther, Gummert, Bucerius, Jacobs, Autschbach, Onnasch, Kruger, Schilling, Metz, Doll, Noack, Holzhey
J.W Goethe University Hospital Centre, Frankfurt Department of Thoracic and Cardiovascular Surgery Department of Anesthesiology, Intensive Care Medicine and Pain Control Department of General and Vascular Surgery Department of Urology
cardiac anaesthetics general urology
Dogan, Aybek, Wimmer-Greinecker, Fawad Khan, Moritz, Auch-Schwelk, Matheis, Anderssen Meininger,Mierdl, Byhahn, Kessler, Westphal Gutt, Markus, Kim, Brinkmann, Heller, Schaeff, Beyer Wolfram, Brautigam, Engl, Bentas,Heitkamp, Ostwald, Kramer, Binder, Blaheta, Jonas, Beecken, Probst, Oertl, Jones
Cardiovascular Institute, University of Dresden, Departments of Cardiac Surgery and Anesthesiology, Dresden
cardiovascular Kappert, Cichon, Gulielmos, Schneider, Schramm, Nicolai, Tugtekin, Schueler, Ahmadzade, Matschke
Heilbronn Hospital, Department of Urology, Heilbronn
urology Rassweiler, Seemann, Stock, Sentker
University of Heidelbery, Medical School of Mannheim, Heidelberg
urology Frede
FRANCE Centre Hospitalier Universitaire Henri Mondor, Creteil Service d’Urologie and Service de Nephrologie Department of Vascular Surgery
urology vascular
Hoznek, Zaki, Samadi, Salomon, Lobontiu, Lang, Abbou, Katz, Borkowski, Antiphon, Saint, Cicco, Chopin, Olsson Desgranges, Bourriez, Javerliat, Laere, Losy, Lobontiu, Melliere, Becquemin
Broussais Hospital, Hopital Europeen Georges Pompidiou, Department of Anesthesiology and Critical Care and Department of Surgery and Organ Transplant, Paris
cardiac D’Attellis, Loulmet, Carpentier, Berrebi, Cardon, Severac-Bastide, Fabiani, Safran
University Pierre and Marie Curie, Department of Urology, Institut Mutualiste Montsouris, Paris
urology Pasticier, Reitbergen, Guillonneau, Fromont, Vallancien
ITALY Misercordia Hospital, Department of General Surgery, Grosseto
general Giulianotti, Coratti, Angelini, Sbrana, Cecconi, Balestracci, Caravaglios
University of Pisa, Department of Thoracic Surgery, Cardiac and Thoracic Department, Pisa
thoracic Melfi, Menconi, Mariani, Angeletti
San Raffaele Hospital, Division of Cardiac Surgery, Milan
cardiac Torracca, Ismeno, Franze, Alfieri, Quarti
AUSTRIA University of Innsbruck, Innsbruck Department of Urology Department of Obstetrics and Gynaecology Department of General and Transplant Surgery (University Hospital)
urology gynaecology general
Peschel, Neururer, Bartsch Schwarzler, Fessler, Marth Muhlmann, Klaus, Kirchmayr, Wykypiel, Unger, Holler, Nehoda, Aigner, Weiss
BELGIUM Centre Hospitalier Universitaire Saint-Pierre, Department de Chirurgie Digestive, Brussels, Belgium
general Cadiere, Himpens, Germay, Izizaw, Degeuldre, Vandromme, Capelluto, Bruyns
APPENDIX A 56
UNITED KINGDOM Imperial College, Department of Surgical Oncology and Technology, Imperial College School of Science Technology and Medicine, London, UK
urology Munz, Moorthy, Kudchadkar, Hernandez, Martin, Darzi, Rockall
THE NETHERLANDS University Medical Centre Utrecht, Department of Surgery, Utrecht, The Netherlands
general Ruurda, Simmermacher, Rinkes, Broeders, Van Vroonhoven
Rest of world
EGYPT Urology and Nephrology Center, Mansoura, Egypt
urology Shoma, El-Tabey, Shaaban, Abol-Enein, Ghoneim
JAPAN Graduate School of Medical Sciences, Kyushu University, Department of Surgery and Science, Fukuoka, Japan
thoracic Yoshino, Hashizume, Shimada, Tomikawa, Tomiyasu, Suemitsu, Sugimachi
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
APPENDIX B 57
Appendix B – Excluded studies
Aaronson O, Tulipan N, Cywes R, Sundell H, Davis G, Bruner J, Richards W. Robot-assisted endoscopic intrauterine myelomeningocele repair: a feasibility study. Pediatric Neurosurgery 2002; 36(2): 85-89.
Abbou C, Hoznek A, Salomon L, Lobontiu A, Saint F, Cicco A, Antiphon P, Chopin D. Remote laparoscopic radical prostatectomy carried out with a robot. Report of a case. Progres en Urologie 2000; 10(4): 520-523.
Aybek T, Dogan S, Andressen E, Mierdl S, Westphal K, Moritz A, Wimmer-Greinecker G. Robotically enhanced totally endoscopic right internal thoracic coronary artery bypass to the right coronary artery. Heart Surgery Forum 2000; 3(4): 322-324.
Ballantyne G. Robotic surgery, telerobotic surgery, telepresence, and telementoring. Review of early clinical results. Surgical Endoscopy 2002; 16(10): 1389-1402.
Beninca G, Garrone C, Rebecchi F, Giaccone C, Morino M. Robot-assisted laparoscopic surgery. Preliminary results at our Center. Chirurgia Italiana 2003; 55(3): 321-331.
Boehm D, Arnold M, Detter C, Reichenspurner H. Incorporating robotics into an open-heart program. Surgical Clinics of North America 2003; 83(6): 1369-1380.
Binder J, Jones J, Bentas W, Wolfram M, Brautigam R, Probst M, Kramer W, Jonas D. Robotic-assisted laparoscopic procedures in urology. Radical prostatectomy and reconstructive retroperitoneal surgery. Urologe (Ausg.A) 2002; 41(2): 144-149.
Breda G, Nakada S, Rassweiler J. Future developments and perspectives in laparoscopy. European Urology 2001; 40(1): 84-91.
Brunaud L, Bresler L, Ayav A, Tretou S, Cormier L, Klein M, Boissel P. Advantages of using robotic Da Vinci system for unilateral adrenalectomy: early results. Annales de Chirurgie 2003; 128(8): 530-535.
Chitwood W, Nifong L. Minimally invasive videoscopic mitral valve surgery: the current role of surgical robotics. Journal of Cardiac Surgery 2000; 15(1): 61-75.
Chitwood W, Nifong L. Robotic assistance in cardiac surgery. Problems in General Surgery 2001; 18(1): 9-20.
Chitwood W, Nifong L, Chapman W, Felger J, Bailey B, Ballint T, Mendleson K, Kim V, Young J, Albrecht R. Robotic surgical training in an academic institution. Annals of Surgery 2001; 234(4): 475-484.
Cordova D, Ballantyne G. Robotic and telerobotic surgical systems for abdominal surgery. Revista de Gastroenterologia del Peru 2003; 23(1): 58-66.
Cornelius M, Kappert U, Cichon R. The introduction of robots in minimally invasive heart surgery. Kardiotechnik 2000; 9(3): 67-70.

APPENDIX B 58
Cost-Maniere E, Adhami L, Severac-Bastide R, Boissonnat J-D, Carpentier A. Planning and simulation of robotically assisted minimally invasive surgery for coronary bypass grafting. Comptes Rendus Biologies 2002; 325(4): 321-326.
Coste-Maniere E, Adhami L, Mourgues F, Carpentier A. Planning, simulation, and augmented reality for robotic cardiac procedures: The STARS system of the ChIR team. Seminars in Thoracic & Cardiovascular Surgery 2003; 15(2): 141-156.
Dakin G, Gagner M. Comparison of laparoscopic skills performance between standard instruments and two surgical robotic systems. Surgical Endoscopy 2003; 17(4): 574-579.
Diodato M, Damiano R. Robotic cardiac surgery: overview. Surgical Clinics of North America 2003; 83(6): 1351-1367.
Drasin T, Gracia C, Atkinson J. Pediatric Applications of Robotic Surgery. Pediatric Endosurgery & Innovative Techniques 2003; 7(4): 377-384.
Esumi G, Tomikawa M, Hashizume M, Konishi K, Shimada M, Sugimachi K. Current status and future of surgical robotic systems. Fukuoka Igaku Zasshi - Fukuoka Acta Medica 2001; 92(9): 315-318.
Falcone T, Goldberg J. Robotics in gynaecology. Surgical Clinics of North America 2003; 83(6): 1483-1489.
Furukawa T, Wakabayashi G, Ozawa S, Watanabe M, Ohgami M, Kitagawa Y, Ishii S, Arisawa Y, Ohmori T, Nohga K, Kitajima M. Surgery using master-slave manipulators and telementoring. Nippon Geka Gakkai Zasshi.Journal of Japan Surgical Society 2000; 101(3): 293-298.
Gotoh S. Endoscopes with latest technology and concept. Minimally Invasive Therapy & Allied Technologies: Mitat 2003; 12(5): 222-226.
Gould J, Melvin W. Telerobotic foregut and esophageal surgery. Surgical Clinics of North America 2003; 83(6): 1421-1427.
Hanisch E, Markus B, Gutt C, Schmandra T, Encke A. Robot-assisted laparoscopic cholecystectomy and fundoplication--initial experiences with the Da Vinci system. Chirurgia 2001; 72(3): 286-288.
Hashizume M, Shimada M, Yoshino I, Kitamura K, Tomikawa M, Akahoshi T, Konishi K, Yamaguchi S. Departmental review of surgical cases in the last 17 years: Da Vinci system. Fukuoka Igaku Zasshi - Fukuoka Acta Medica 2002; 93(Suppl 3): 47-48.
Hashizume M, Sugimachi K. Robot-assisted gastric surgery. Surgical Clinics of North America 2003; 83(6): 1429-1444.
Haus B, Kambham N, Le D, Moll F, Gourin C, Terris D. Surgical robotic applications in otolaryngology. Laryngoscope 2003; 113(7): 1139-1144.
Heller K, Beyer P, Schaeff B, Gutt C. Laparoscopic cholecystectomy with the telerobotic system Da Vinci in children. Zentralblatt fur Kinderchirurgie 2002; 11(3): 148-151.
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
APPENDIX B 59
Hubens G, Coveliers H, Balliu L, Ruppert M, Vaneerdeweg W. A performance study comparing manual and robotically assisted laparoscopic surgery using the da Vinci system. Surgical Endoscopy 2003a; 17(10): 1595-1599.
Hubens G, Ruppert M, Balliu L, Hoeckx L, Ysebaert D, Vaneerdeweg W. The robot in the operating room: (R)evolution in minimal invasive surgery. Tijdschrift voor Geneeskunde 2003b; 59(11): 705-713.
Hubert J, Feuillu B, Mangin P, Artis M, Villemot JP. Robot-assisted (Da Vinci) laparoscopic uretero-pelvic junction repair. Results of experimental surgery in a series of 14 pigs. Progres en Urologie 2002; 12(4): 592-596.
Hubert J, Feuillu B, Mangin P, Lobontiu A, Artis M, Villemot P. Laparoscopic computer-assisted pyeloplasty: the results of experimental surgery in pigs. BJU International 2003; 92(4): 437-440.
Jacob B, Gagner M. Robotics and general surgery. Surgical Clinics of North America 2003; 83(6): 1405-1419.
Jacobs S, Falk V. Pearls and pitfalls: lessons learned in endoscopic robotic surgery- the da Vinci experience. Heart Surgery Forum 2001; 4(4): 307-310.
Jacobs S, Holzhey D, Kiaii BB, Onnasch JF, Walther T, Mohr FW, Falk V. Limitations for manual and telemanipulator-assisted motion tracking--implications for endoscopic beating-heart surgery. Annals of Thoracic Surgery 2003; 76(6): 2029-2035.
Jacobsen G, Berger R, Horgan S. The role of robotic surgery in morbid obesity. Journal of Laparoendoscopic & Advanced Surgical Techniques - Part A 2003; 13(4): 279-283.
Kleine P, Gronefeld G, Dogan S, Hohnloser S, Moritz A, Wimmer-Greinecker G. Robotically enhanced placement of left ventricular epicardial electrodes during implantation of a biventricular implantable cardioverter defibrillator system. Pacing & Clinical Electrophysiology 2002; 25(6): 989-991.
Kypson A, Nifong L, Chitwood W. Robotic mitral valve surgery. Seminars in Thoracic & Cardiovascular Surgery 2003; 15(2): 121-129.
Malhotra S, Le D, Thelitz S, Hanley F, Kirk R, Suleman S, Mohan R. Robotic-assisted endoscopic thoracic aortic anastomosis in juvenile lambs. Heart Surgery Forum 2003; 6(1): 38-42.
Michler R. Nanotechnology: Potential applications in cardiothoracic surgery. Biomedical Microdevices 2001; 3(2): 119-124.
Moran ME. Robotic Surgery: Urologic Implications. Journal of Endourology 2003; 17(9): 695-708.
Nathoo N, Pesek T, Barnett G. Robotics and neurosurgery. Surgical Clinics of North America 2003; 83(6): 1339-1350.
Olsen L, Deding D, Yeung C, Jorgensen T. Computer assisted laparoscopic pneumovesical ureter reimplantation a.m. Cohen: initial experience in a pig model. APMIS.Supplementum 2003; 109: 23-25.
Onnasch J-F, Schneider F, Falk V, Mierzwa M, Bucerius J, Mohr F. Five years of less invasive mitral valve surgery: From experimental to routine approach. Heart Surgery Forum 2002; 5(2): 132-135.

APPENDIX B 60
Ozawa S, Furukawa T, Wakabayashi G, Kitajima M. Recent advances in robotic surgery. Biotherapy 2001; 15(4): 433-438.
Panait L, Doarn C, Merrell R. Applications of robotics in surgery. Chirurgia (Bucuresti) 2002; 97(6): 549-555.
Rassweiler J, Binder J, Frede T. Robotic and telesurgery: will they change our future? Current Opinion in Urology 2001; 11(3): 309-320.
Rassweiler J, Frede T. Robotics, telesurgery and telementoring--their position in modern urological laparoscopy. Archivos Espanoles de Urologia 2002; 55(6): 610-628.
Reade C, Bower C, Maziarz D, Conquest A, Sun Y, Nifong L, Chitwood W. Sutureless robot-assisted mitral valve repair: An animal model. Heart Surgery Forum 2003a; 6(4): 254-257.
Reade C, Kumar A, Chapman W. Robotic adrenalectomy and splenectomy. Problems in General Surgery 2003b; 20(2): 57-64.
Rockall T, Darzi A. Robot-assisted laparoscopic colorectal surgery. Surgical Clinics of North America 2003; 83(6): 1463-1468.
Ruurda J, Visser P, Broeders I. Analysis of procedure time in robot-assisted surgery: comparative study in laparoscopic cholecystectomy. Computer Aided Surgery 2003; 8(1): 24-29.
Satava R. Robotic surgery: from past to future - a personal journey. Surgical Clinics of North America 2003; 83(6): 1491-1500.
Schluender S, Conrad J, Divino C, Gurland B. Robot-assisted laparoscopic repair of ventral hernia with intracorporeal suturing: An experimental study. Surgical Endoscopy 2003; 17(9): 1391-1395.
Shennib H. Tools for precision enhancement in minimally invasive cardiac surgery: three dimensional visualization, computer enhancement and robotics. European Journal of Cardio-Thoracic Surgery 1999; 16(Suppl 2): S93-S96.
Shennib H, Bastawisy A, Mack MJ, Moll FH. Computer-assisted telemanipulation: an enabling technology for endoscopic coronary artery bypass. Annals of Thoracic Surgery 1998; 66(3): 1060-1063.
Shennib H, Bastawisy A, McLoughlin J, Moll F. Robotic computer-assisted telemanipulation enhances coronary artery bypass. Journal of Thoracic & Cardiovascular Surgery 1999; 117(2): 310-313.
Shimada M and Sugimachi K. Future aspect of robotic surgery. Fukuoka Igaku Zasshi - Fukuoka Acta Medica 2002; 93(4): 57-63.
Stein H, Ikeda M, Jacobs S, Lilagan P, Walther C, Rastan A, Mohr FW, Falk V. Telemanipulatory application of a magnetic vascular coupler on the beating heart with the da Vinci surgical system. Biomedizinische Technik 2003; 48(9): 230-234.
Stylopoulos N, Rattner D. Robotics and ergonomics. Surgical Clinics of North America 2003; 83(6): 1321-1337.
ASERNIP-S OVERVIEW OF DA V INC I SURGICAL ROBOTIC SYSTEM – JULY 2004
APPENDIX B 61
Sung G, Gill I. Robotic laparoscopic surgery: a comparison of the Da Vinci and Zeus systems. Urology 2001; 58(6): 893-898.
Sung G, Gill I. Robotic renal and adrenal surgery. Surgical Clinics of North America 2003; 83(6): 1469-1482.
Talamini M. Robotic surgery: is it for you? Advances in Surgery 2002; 36: 1-13.
Tang L, D'Ancona G, Bergsland J, Kawaguchi A, Karamanoukian H. Robotically assisted video-enhanced-endoscopic coronary artery bypass graft surgery. Angiology 2001; 52(2): 99-102.
Tewari A, Peabody J, Sarle R, Balakrishnan G, Hemal A, Shrivastava A, Menon M. Technique of da Vinci robot-assisted anatomic radical prostatectomy. Urology 2002; 60(4): 569-572.
Weber P, Merola S, Wasielewski A, Ballantyne G, Delaney C. Telerobotic-assisted laparoscopic right and sigmoid colectomies for benign disease. Diseases of the Colon & Rectum 2002; 45(12): 1689-1696.
Yohannes P, Burjonrappa S. Rapid communication: laparoscopic Anderson-Hynes dismembered pyeloplasty using the da Vinci robot: technical considerations. Journal of Endourology 2003; 17(2): 79-83.

APPENDIX C 62
Appendix C – Typical operating room set-up for urological, cardiac and general surgery

OR Monitor
Anesthesiologist
Patient-Side Cart
EndoWrist ®
Instruments aredesigned withseven degreesof freedom andmimic thedexterity of thehuman handand wrist.
Nurse
Assistant
Surgeon atOperative Console
Surgeon uses open-surgeryhand movements which areprecisely replicated in theoperative field by theEndoWrist ® Instruments.
InSite® Visionprovides true to life3-D images of the
operative field.
Foot pedalsrepositionsan image
Image ProcessingEquipment
da Vinci ® Surgical System in a Urology Procedure Setting

OR Monitor
Anesthesiologist
Patient-Side Cart
EndoWrist ®
Instruments aredesigned with seven degreesof freedom andmimic thedexterity of the human handand wrist.
Nurse
CPB Machine/Perfusionist
Surgeon atOperative Console
Surgeon uses open-surgeryhand movements which areprecisely replicated in theoperative field by the EndoWrist ® Instruments.
Assistant
Foot pedalsrepositionsan image
ImageProcessing Equipment
InSite ® Visionprovides
true to life3-D images of
the operative field.
da Vinci ® Surgical System in a Cardiac Procedure Setting

APPENDIX D 66
Appendix D – Study design and results tables Abbreviations used in tables: ASD atrial septal defect BIMA bilateral internal mammary artery BMI body mass index CABG coronary artery bypass grafting CAD coronary artery disease ICU intensive care unit ITA internal thoracic artery LAD left anterior descending coronary artery LAST left anterior small thoracotomy LIMA left internal mammary artery LVEF left ventricular ejection fraction MIDCABG minimally invasive direct coronary artery bypass grafting MMO ‘micro-mitral’ operation *All values are expressed as mean [SD] unless stated otherwise.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
67 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Menon 2002, FRANCE (Level III-2) March 2001 to August 2001. 60 patients. Follow-up: not stated. Comparison: Robotic: 30 patients underwent robot-assisted anatomic prostatectomy; Control: 30 patients underwent conventional radical retropubic prostatectomy. Selection criteria: Patients who were medically fit to undergo surgery, weighed <250 lb, had a waist size <45 inches and BMI <35. Age: Robotic: 62 years (range 51-71); Control: 64 years (range 59-70).
Operative time: Robotic: 288 mins (range 240-420); Control: 138 mins (range 90-300), p<0.001. Length of stay: Hospital stay: Robotic: 1.5 days (range 0.96-4); Control: 2.3 days (range 2-4). Conversions: 1/30 (3%)
Blood loss: Robotic: 329 mL (range 75-1050); Control: 970 mL (range 400-2200), p<0.001. Transfusions: Robotic: 2/30 (7%) – 6 units; Control: 9/30 (30%) – 27 units, p<0.001. Complications: Robotic Control No. (%) No. (%) Intraoperative bleeding (>1000 mL) 1 (3) 5 (17) Rectal injuries 0 1 (3) Urinary retention 1 (3) 1 (3) Postop ileus 3 (9) 3 (9) Exaggeration of arthritis 1 (3) 0 Wound dehiscence 1 (3) 1 (3) Mortality: Robotic: 0 Control: 0
Features unique to the da Vinci system: - 3D visualisation - the freedom of instrument movement - the intuitiveness of surgical motion These features increase surgical precision and reduce surgeon fatigue. Disadvantages: - lack of tactile sensation - cost

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
68 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Menon 2003, USA (Level IV) 100 patients. Follow-up: not stated. Intervention: Patients underwent radical prostatectomies using the da Vinci surgical system.
Operative time: 165 mins with lymphadenectomy and 135 mins without lymphadenectomy.
Blood loss: 150 mL Complications: they report a mean complication rate of 4% but no details as to what the complications were.
This was an article on the technique with little patient data reported.
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Wolfram 2003, GERMANY (Level IV) May 2000 to May 2003. 81 patients. Follow-up: not stated. Intervention: Patients underwent laparoscopic radical prostatectomy using the telerobotic da Vinci surgical system via the Montsouris technique. Selection criteria: Patients with clinically localised prostate cancer. Median age: 63 years (range 45-75)
Median operative time: 250 mins (range 150-390)
Median blood loss: 300 mL (range 100-1500) Transfusion rate: 10/81 (12%) – 1 to 2 units of blood were transfused.
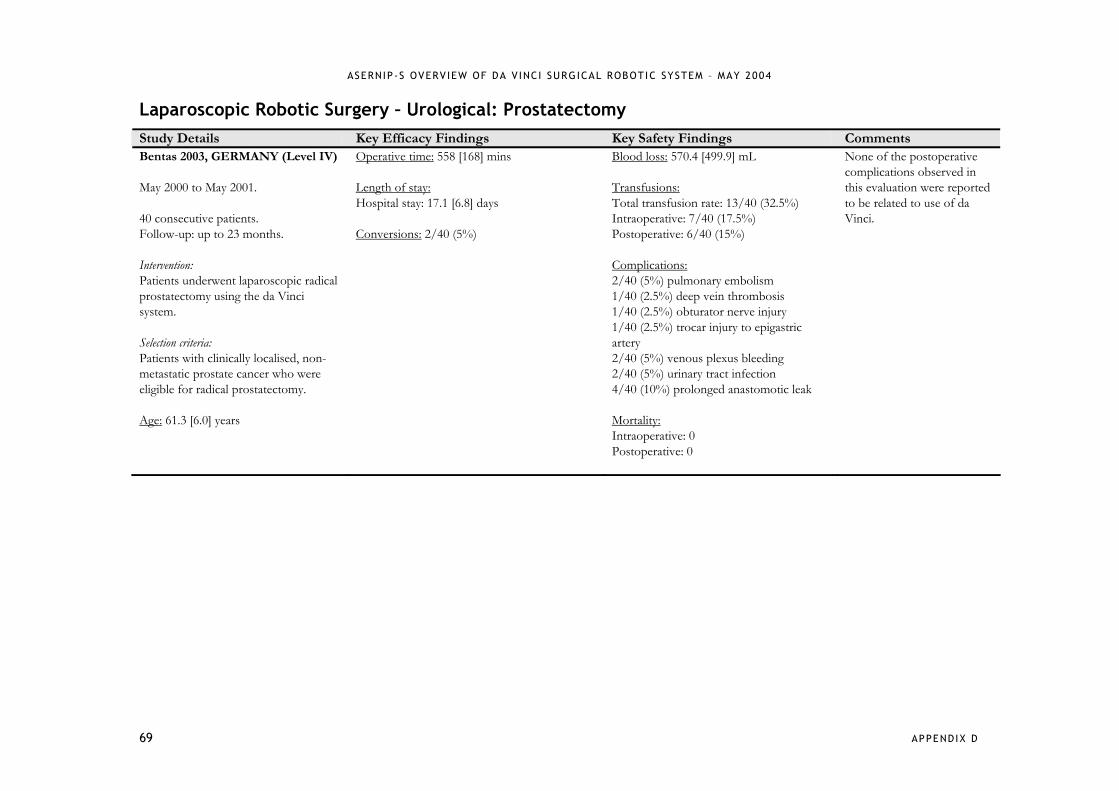
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
69 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Bentas 2003, GERMANY (Level IV) May 2000 to May 2001. 40 consecutive patients. Follow-up: up to 23 months. Intervention: Patients underwent laparoscopic radical prostatectomy using the da Vinci system. Selection criteria: Patients with clinically localised, non-metastatic prostate cancer who were eligible for radical prostatectomy. Age: 61.3 [6.0] years
Operative time: 558 [168] mins Length of stay: Hospital stay: 17.1 [6.8] days Conversions: 2/40 (5%)
Blood loss: 570.4 [499.9] mL Transfusions: Total transfusion rate: 13/40 (32.5%) Intraoperative: 7/40 (17.5%) Postoperative: 6/40 (15%) Complications: 2/40 (5%) pulmonary embolism 1/40 (2.5%) deep vein thrombosis 1/40 (2.5%) obturator nerve injury 1/40 (2.5%) trocar injury to epigastric artery 2/40 (5%) venous plexus bleeding 2/40 (5%) urinary tract infection 4/40 (10%) prolonged anastomotic leak Mortality: Intraoperative: 0 Postoperative: 0
None of the postoperative complications observed in this evaluation were reported to be related to use of da Vinci.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
70 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Ahlering 2003, USA (Level IV) June 2002 to March 2003. 45 patients. Follow-up: the first 9 patients had at least 6 months follow-up; the remaining patients were followed up for 3 months. Intervention: Patients underwent laparoscopic radical prostatectomy using the Vattikuti Institute Prostatectomy technique. Selection criteria: Patients with localised prostate cancer. Age: 61.4 years (range 46-71)
Operative time: Cohort 1 (pts 1-5): 350 mins; Cohort 2 (pts 6-10): 265 mins; Cohort 3 (pts 11-20): 192 mins; Cohort 4 (pts 21-35): 186 mins; Cohort 5 (pts 36-45): 162 mins. Length of stay: Hospital stay: 1.5 days (range 0.75-7.0) Conversions: 0
Blood loss: 134 cc (range 25-350) Transfusions: 0 Complications: 2/45 (4%) urinary extravasation 1/45 (2%) prolonged hospitalisation – leg pain 1/45 (2%) bleeding 1/45 (2%) deep vein thrombosis and anastomotic disruption Bowel injuries: 0

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
71 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Rassweiler 2001, GERMANY (Level IV) 6 patients. Follow-up: 1 month. Intervention: Patients underwent telesurgical laparoscopic radical prostatectomy. Age: 64.2 years (range 57-71)
Operative time: 351.2 mins (range 242-480)
Transfusions: 1/6 (17%) – 2 units Complications: Intraoperative complications: 0 1/6 (17%) 3D vision problems – difficult to adjust to new image 1/6 (17%) difficulty with lack of tactile feedback 1/6 (17%) breakdown of scissors
Another publication by Rassweiler et al. (Eur Urol 2001; 40: 75-83) reports exactly the same data.
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Pasticier 2001, USA (Level IV) September 2000. 5 consecutive patients. Follow-up: 1 month. Intervention: Patients underwent robotically assisted nerve-sparing laparoscopic radical prostatectomy. Selection criteria: Patients with prostate cancer. Age: 58 years
Operative time: 222 mins (range 150-381) Length of stay: Hospital stay: 5.5 days (range 4-7)
Blood loss: 800 cc (range 700-1600) Transfusions: 0 Complications: Postoperative complications: 0
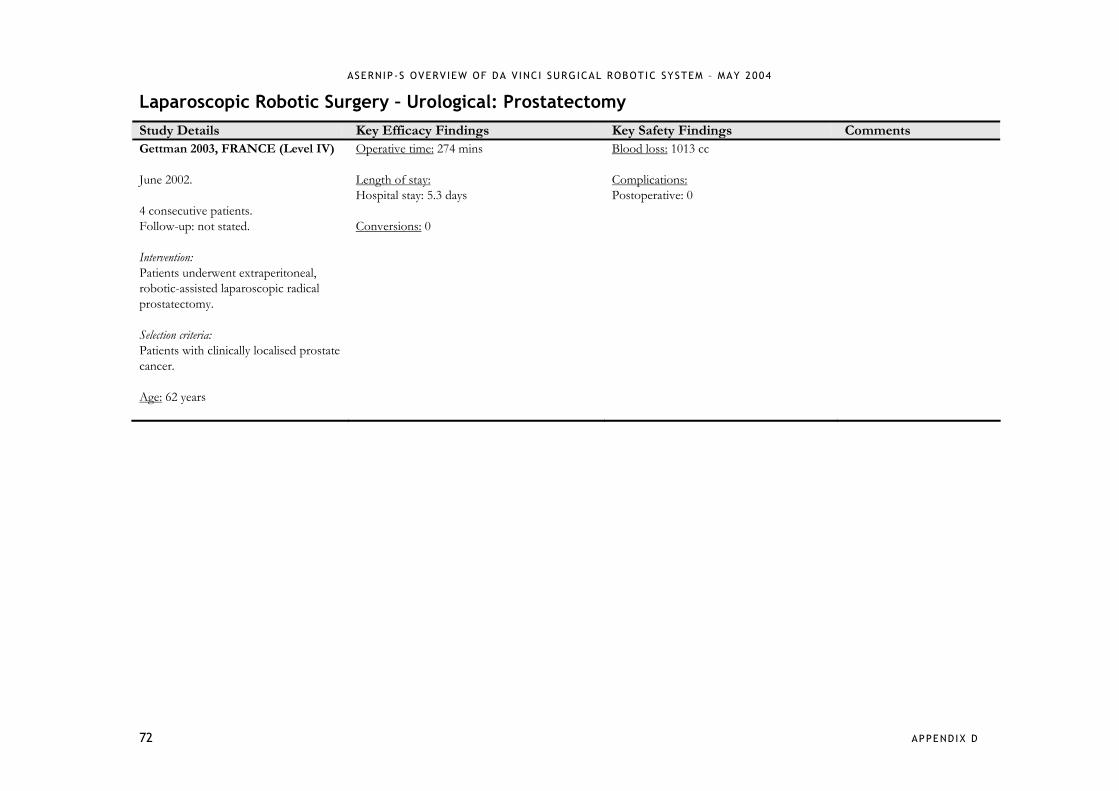
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
72 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Prostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Gettman 2003, FRANCE (Level IV) June 2002. 4 consecutive patients. Follow-up: not stated. Intervention: Patients underwent extraperitoneal, robotic-assisted laparoscopic radical prostatectomy. Selection criteria: Patients with clinically localised prostate cancer. Age: 62 years
Operative time: 274 mins Length of stay: Hospital stay: 5.3 days Conversions: 0
Blood loss: 1013 cc Complications: Postoperative: 0

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
73 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Pyeloplasty Study Details Key Efficacy Findings Key Safety Findings Comments Gettman 2002, AUSTRIA (Level III-3) June 2001 to August 2001 (Robotic); November 1999 to June 2001 (Control). 12 patients. Follow-up: 3 months. Comparison: Robotic/Anderson-Hynes (A-H): 4 patients underwent A-H laparoscopic pyeloplasty (LP) using the da Vinci robotic system; Robotic/Fengerplasty (FP): 2 patients underwent FP LP using the da Vinci robotic system; Control/A-H: 4 patients underwent A-H LP with standard techniques; Control/FP: 2 patients underwent FP LP with standard techniques. Selection criteria: Patients with ureteropelvic junction obstruction (UPJO). Age: mean age of patients in the robotic group and control group were comparable.
Operative time: Robotic/A-H: 140 mins (range 80-215); Robotic/FP: 77.5 mins (range 75-80); Control/A-H: 235 mins (range 210-270); Control/FP: 100 mins (range 80-120). Length of stay: Hospital stay: 4 days for all patients regardless of treatment group. Conversions: 0 Measures of success: objective success rate, based on results of the postoperative radiographic imaging during the third postoperative month, was 100% for all patients in all treatment groups.
Blood loss: <50 mL in all cases. Complications: Postoperative complications: 0 *2/9 (22%) the working mechanism of the robotic forceps broke during suturing *1/9 (11%) reintervention
Occasional collisions were encountered with the working arms of the da Vinci robotic system, but this did not interfere with the successful completion of all robotic procedures.
*Results from another publication by Gettman et al. (Urology 2002; 60: 509-513) as there is a possibility of patient overlap.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
74 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Pyeloplasty Study Details Key Efficacy Findings Key Safety Findings Comments Bentas 2003, GERMANY (Level IV) August 2000 to June 2002. 11 patients. Follow-up: median 21 months. Intervention: Patients underwent pyeloplasty via a laparoscopic transperitoneal approach exclusively with the da Vinci system. Selection criteria: Patients with ureteropelvic junction obstruction (UPJO).
Operative time: 196.8 [75.5] mins Length of stay: Hospital stay: 5.5 [3.5] days Conversions: 0
Blood loss: negligible Complications: Intraoperative complications: 0 1/11 (9%) mild right flank pain Urinary extravasation: 0 Haematomas: 0 Protracted bowel paralysis: 0
The da Vinci surgical system has the potential to enhance operative capability and the ability to restore hand-eye coordination and 3D viewing that are otherwise lost in laparoscopic surgery.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
75 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Cystoprostatectomy Study Details Key Efficacy Findings Key Safety Findings Comments Menon 2003, EGYPT (Level IV) April 2002 to February 2003. 17 patients. Follow-up: not stated. Intervention: Patients underwent nerve-sparing robot-assisted radical cystoprostatectomy using the da Vinci surgical system. Selection criteria: Patients with transitional cell carcinoma of the bladder. Gender (M/F): 14/3
Operative time: 140 mins
Blood loss: <150 mL Complications: 1/17 (6%) incomplete operation – lens malfunction 1/17 (6%) re-exploration 1/17 (6%) port-site haematoma

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
76 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Sacrocolpopexy Study Details Key Efficacy Findings Key Safety Findings Comments DiMarco 2004, USA (Level IV) 5 patients. Follow-up: 4 months. Intervention: Patients underwent robotic sacrocolpopexy. Gender (M/F): 0/5 Median age: 62 years
Operative time: 222 mins (median 210 mins) Length of stay: Hospital stay: 1 night
Complications: 1/5 (20%) persistent vaginal bleeding for 2 days postop Recurrent anterior, posterior or apical prolapse: 0 Robot-related complications: 0
Advantage of using the robot system is that the open transabdominal technique and surgical principles of repair can be mimicked in a non-invasive fashion while avoiding a midline abdominal incision.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
77 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Case Reports Urological Procedure Patients Outcomes
Kaouk 2003 sural nerve grafting after radical prostatectomy
n=3 robotic system used for whole procedure in 1 patient and partially for other 2 patients
nerve sparing procedure for one patient resulted in return to preoperative sexual/erectile function at 1 month postoperatively
2 patients sural nerve grafting did not result in return to normal sexual/erectile function after 1 month (both patients had positive tumour margins after wide resection)
no intra or postoperative complications reported
Abbou 2001 prostatectomy n=1 all steps in bilateral nerve sparing without pelvic lymphadenectomy procedure performed with robotic system
assembly and disassembly of robotic system took 45 of 420 minute operative time
blood loss 300mL
bladder catheter removed POD3
tumour removed successfully with negative margins
Menon 2004 radical cystectomy and urinary diversion with preservation of uterus and vagina
n=3 tumour with clear margin removed in all three cases
success bilateral pelvic lymphadenectomy removed average of 12 lymph nodes (all negative)
mean operative time 160 mins
mean blood loss less than 100mL
Beecken 2003 laparoscopic radical cystectomy and intra-abdominal formation of orthotopic ileal neobladder
n=1 no intraoperative or postoperative complications
patient mobilized POD1
procedure presumed to have curative efficacy as clear tumour margins and no lymph node metastases
5 months postoperative – patient well and tumour free – neobladder functioning well
authors feel that operative time (8.5hours) quite short considering complexity of procedure – attributable to robotic assistance
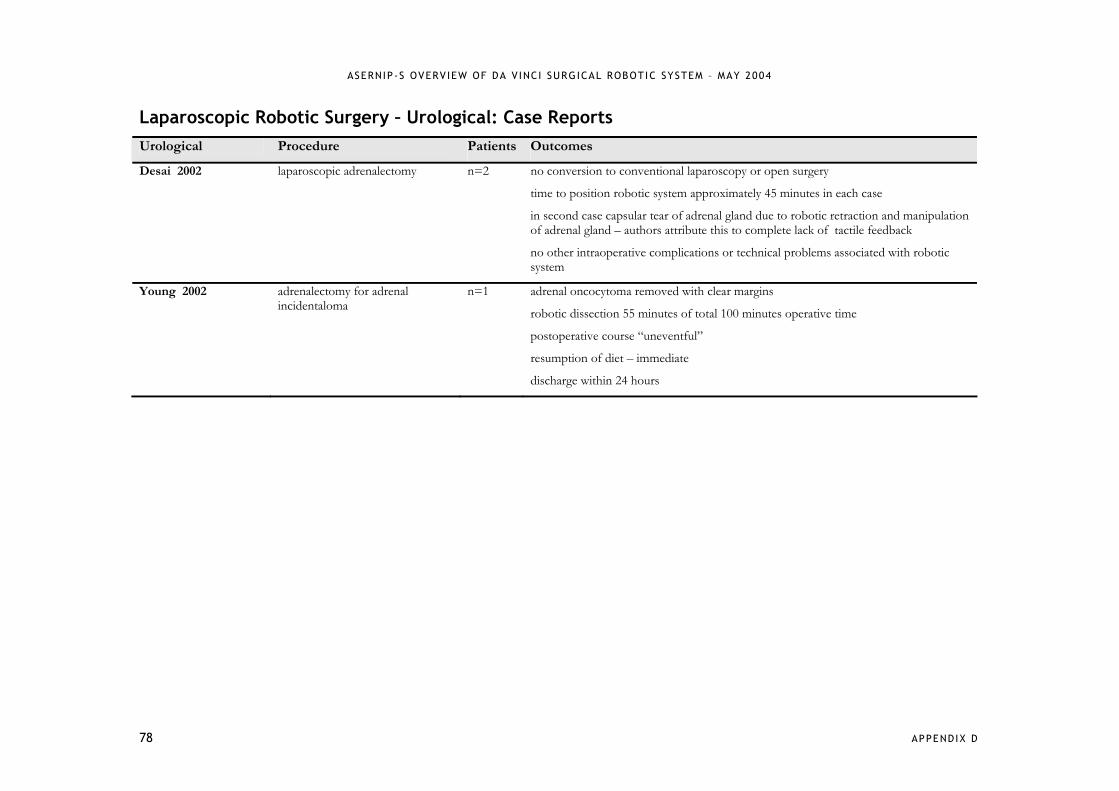
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
78 APPENDIX D
Laparoscopic Robotic Surgery – Urological: Case Reports Urological Procedure Patients Outcomes
Desai 2002 laparoscopic adrenalectomy n=2 no conversion to conventional laparoscopy or open surgery
time to position robotic system approximately 45 minutes in each case
in second case capsular tear of adrenal gland due to robotic retraction and manipulation of adrenal gland – authors attribute this to complete lack of tactile feedback
no other intraoperative complications or technical problems associated with robotic system
Young 2002 adrenalectomy for adrenal incidentaloma
n=1 adrenal oncocytoma removed with clear margins
robotic dissection 55 minutes of total 100 minutes operative time
postoperative course “uneventful”
resumption of diet – immediate
discharge within 24 hours

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
79 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Bucerius 2002, GERMANY (Level III-2) 190 patients. Follow-up: not stated. Comparison: MIDCABG-endo: 24 patients underwent robotic internal thoracic artery (ITA) takedown and MIDCABG via a left minithoracotomy; MIDCABG-conv: 73 patients underwent a conventional MIDCABG with ITA preparation under direct vision; CABG-conv: 93 patients underwent a conventional CABG via a median sternotomy. Selection criteria: Patients requiring coronary artery bypass surgery. Gender (M/F): MIDCABG-endo: 16/8 MIDCABG-conv: 55/18 CABG-conv: 70/23 Age: MIDCABG-endo: 65.3 [6.6] years MIDCABG-conv: 61.6 [9.9] years CABG-conv: 63.9 [9.0] years
Length of stay: Hospital stay: MIDCABG-endo: 8.9 [3.2] days MIDCABG-conv: 15.9 [6.5] days, p<0.05 (vs MIDCABG-endo) CABG-conv: 16.3 [9.0] days, p<0.05 (vs MIDCABG-endo) ICU stay: MIDCABG-endo: 16.3 [7.3] hours MIDCABG-conv: 20.9 [13.1] hours CABG-conv: 29.7 [63.5] hours
Complications: not stated.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
80 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Mohr 2001, GERMANY (Level IV)* By April 2000. 131 patients. Follow-up: up to 6 months. Intervention: 138 patients underwent coronary artery bypass grafting (CABG): Gp 1: In 81 patients, the internal thoracic artery (ITA) was harvested endoscopically with the system. Gp 2: In 15 patients, the anastomosis of the ITA to the left anterior descending coronary artery (LAD) was performed with the system. Gp 3: 27 patients underwent total endoscopic coronary artery bypass (TECAB) on the arrested heart. Gp 4: 8 patients underwent TECAB on the beating heart. Exclusion criteria: Patients with any of the known contraindications for using the Port-Access technique, left ventricular dilatation or diffuse disease of the target vessel. Other contraindications for thoracoscopic ITA takedown were extensive pleural symphysis or intolerance of single lung ventilation because of pulmonary disease. Continued over…
Operative time: Gp 1: 217 [75] mins (total) and 25-40 mins (left internal mammary artery takedown); Gp 2: 16 [11] mins (anastomosis time); Gp 3: 347 [95] mins (total); Gp 4: not stated. Length of stay: Hospital stay: Gp 1: 10.7 [4.2] days; Gp 2: not stated; Gp 3: 9.4 [2.9] days; Gp 4: not stated. ICU stay: Gp 1: 20.1 [11.4] hours; Gp 2: not stated; Gp 3: 15.5 [6.4] hours; Gp 4: not stated. Conversions: Gp 1: 0; Gp 2: 0; Gp 3: 5/27 (18.5%); Gp 4: 6/8 (75%). Measures of success: Gp 1: 79/81 (97.5%) successful endoscopic ITA takedown.
Complications: Gp 1: 2/81 (2.5%) ITA was discarded for occlusion (n=1) and low flow (n=1) 2/81 (2.5%) re-exploration 1/81 (1%) stroke 3/81 (4%) transient atrial fibrillation 1/81 (1%) extensive endarterectomy Gp 2: 1/15 (7%) haemorrhagic stroke Gp 3: 1/27 (4%) re-operation 1/27 (4%) recurrent left lower lobe atelectasis Gp 4: 1/8 (12.5%) graft occlusion 1/8 (12.5%) low-flow graft 1/8 (12.5%) septal branch bleeding 1/8 (12.5%) ventricular fibrillation Mortality: Gp 1: 1/81 (1%) unknown Gp 2: 1/15 (7%) – haemorrhagic stroke Gp 3: 0 Gp 4: 1/8 (12.5%) severe anterior myocardial infarction
The 3 deaths reported were not related to the system.
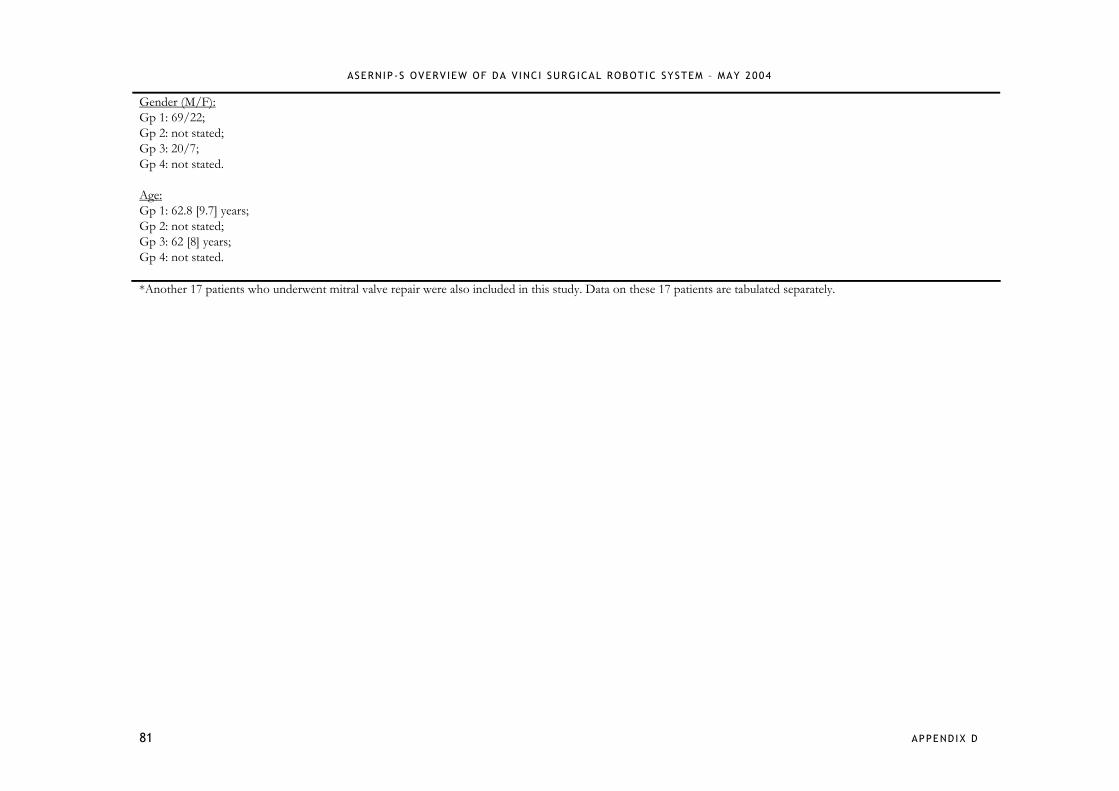
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
81 APPENDIX D
Gender (M/F): Gp 1: 69/22; Gp 2: not stated; Gp 3: 20/7; Gp 4: not stated. Age: Gp 1: 62.8 [9.7] years; Gp 2: not stated; Gp 3: 62 [8] years; Gp 4: not stated. *Another 17 patients who underwent mitral valve repair were also included in this study. Data on these 17 patients are tabulated separately.
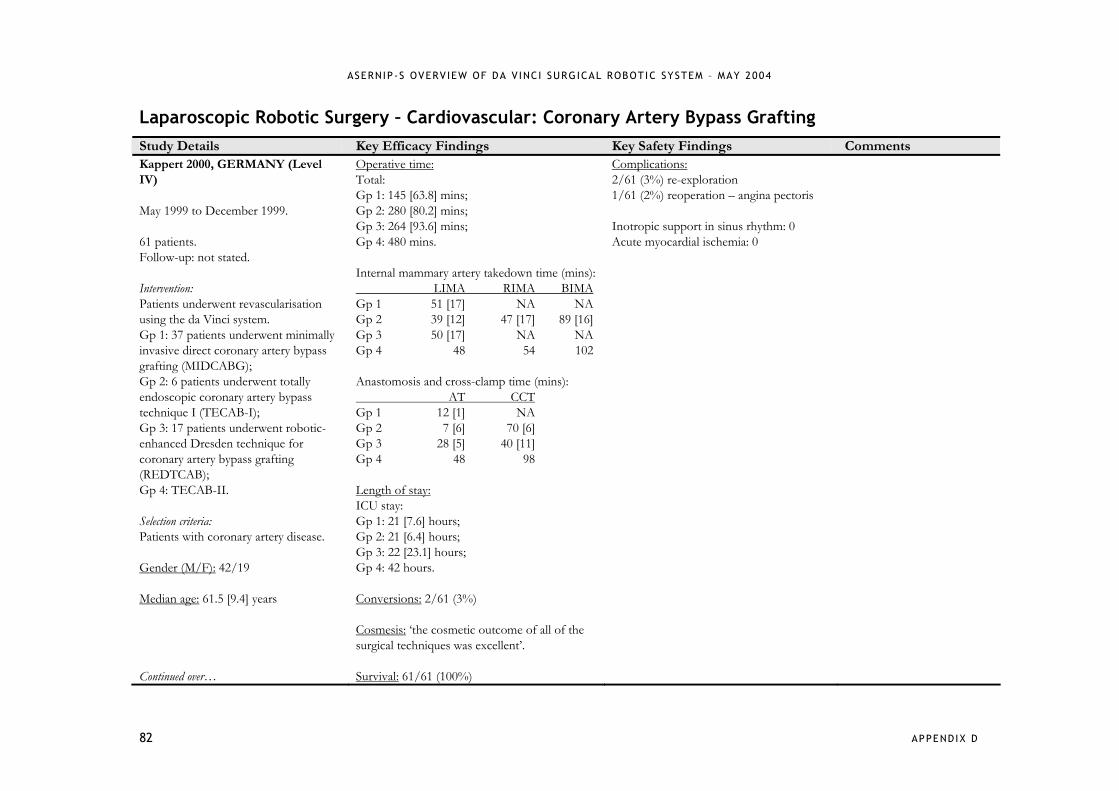
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
82 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Kappert 2000, GERMANY (Level IV) May 1999 to December 1999. 61 patients. Follow-up: not stated. Intervention: Patients underwent revascularisation using the da Vinci system. Gp 1: 37 patients underwent minimally invasive direct coronary artery bypass grafting (MIDCABG); Gp 2: 6 patients underwent totally endoscopic coronary artery bypass technique I (TECAB-I); Gp 3: 17 patients underwent robotic-enhanced Dresden technique for coronary artery bypass grafting (REDTCAB); Gp 4: TECAB-II. Selection criteria: Patients with coronary artery disease. Gender (M/F): 42/19 Median age: 61.5 [9.4] years Continued over…
Operative time: Total: Gp 1: 145 [63.8] mins; Gp 2: 280 [80.2] mins; Gp 3: 264 [93.6] mins; Gp 4: 480 mins. Internal mammary artery takedown time (mins): LIMA RIMA BIMA Gp 1 51 [17] NA NA Gp 2 39 [12] 47 [17] 89 [16] Gp 3 50 [17] NA NA Gp 4 48 54 102 Anastomosis and cross-clamp time (mins): AT CCT Gp 1 12 [1] NA Gp 2 7 [6] 70 [6] Gp 3 28 [5] 40 [11] Gp 4 48 98 Length of stay: ICU stay: Gp 1: 21 [7.6] hours; Gp 2: 21 [6.4] hours; Gp 3: 22 [23.1] hours; Gp 4: 42 hours. Conversions: 2/61 (3%) Cosmesis: ‘the cosmetic outcome of all of the surgical techniques was excellent’. Survival: 61/61 (100%)
Complications: 2/61 (3%) re-exploration 1/61 (2%) reoperation – angina pectoris Inotropic support in sinus rhythm: 0 Acute myocardial ischemia: 0
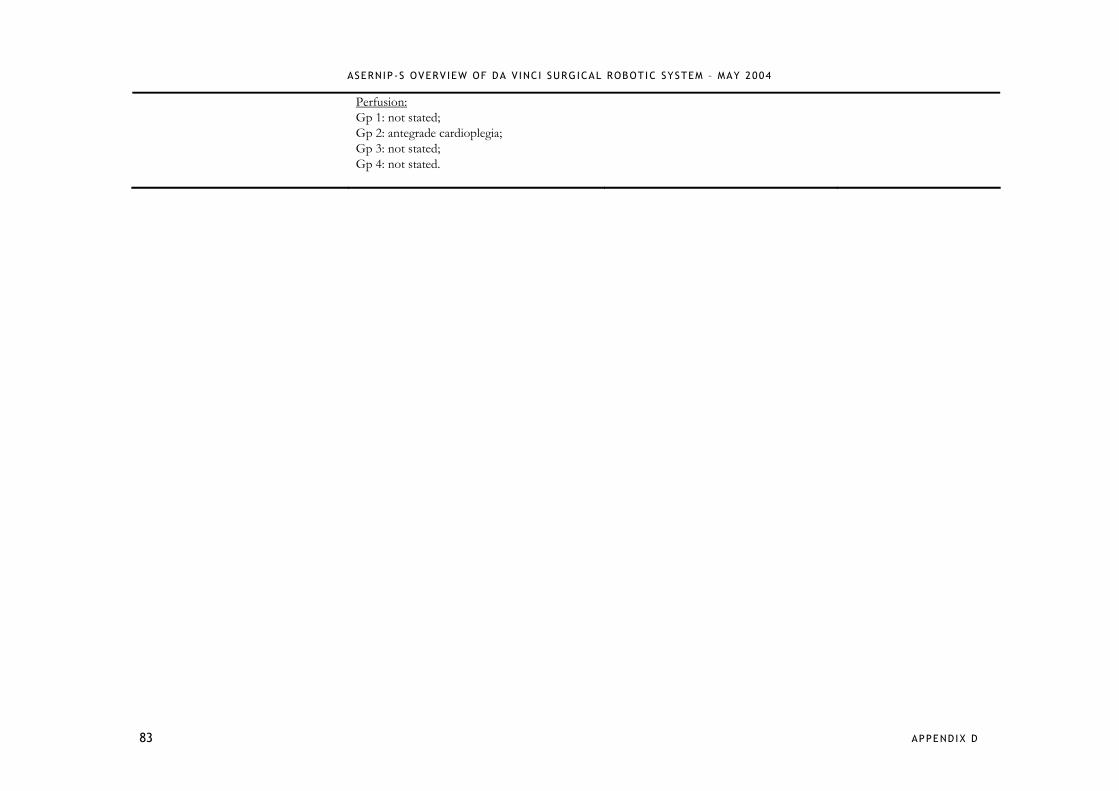
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
83 APPENDIX D
Perfusion: Gp 1: not stated; Gp 2: antegrade cardioplegia; Gp 3: not stated; Gp 4: not stated.
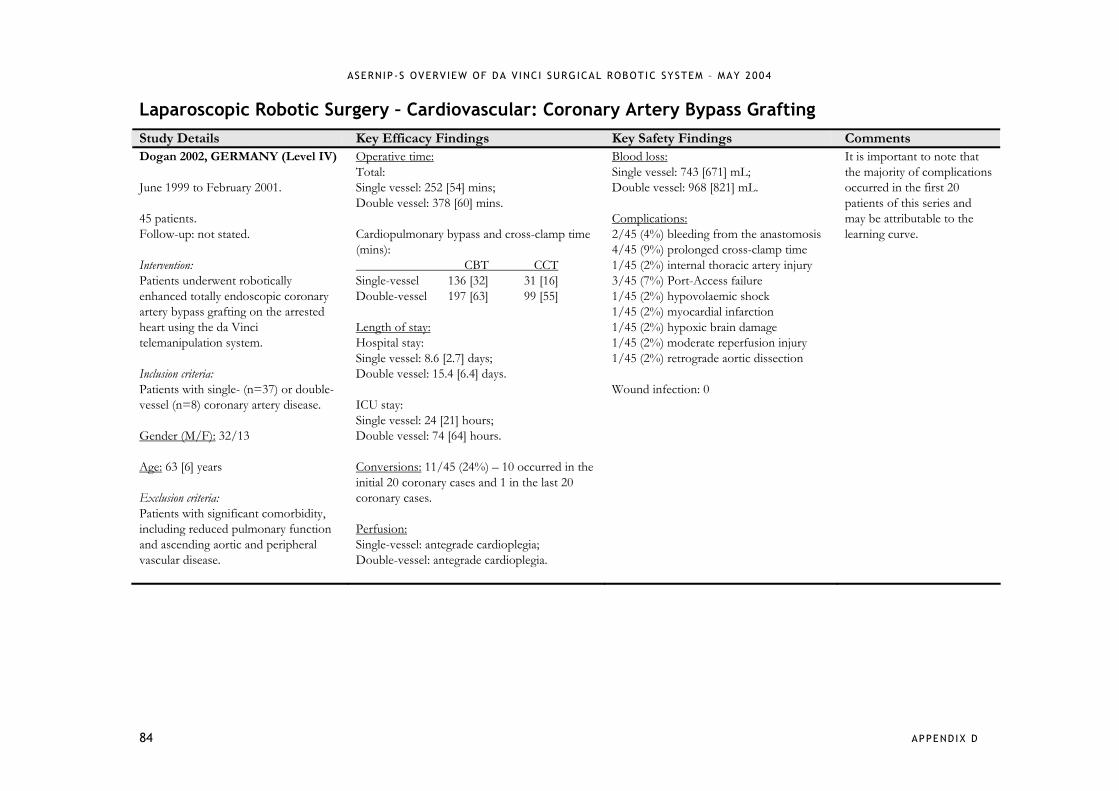
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
84 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Dogan 2002, GERMANY (Level IV) June 1999 to February 2001. 45 patients. Follow-up: not stated. Intervention: Patients underwent robotically enhanced totally endoscopic coronary artery bypass grafting on the arrested heart using the da Vinci telemanipulation system. Inclusion criteria: Patients with single- (n=37) or double-vessel (n=8) coronary artery disease. Gender (M/F): 32/13 Age: 63 [6] years Exclusion criteria: Patients with significant comorbidity, including reduced pulmonary function and ascending aortic and peripheral vascular disease.
Operative time: Total: Single vessel: 252 [54] mins; Double vessel: 378 [60] mins. Cardiopulmonary bypass and cross-clamp time (mins): CBT CCT Single-vessel 136 [32] 31 [16] Double-vessel 197 [63] 99 [55] Length of stay: Hospital stay: Single vessel: 8.6 [2.7] days; Double vessel: 15.4 [6.4] days. ICU stay: Single vessel: 24 [21] hours; Double vessel: 74 [64] hours. Conversions: 11/45 (24%) – 10 occurred in the initial 20 coronary cases and 1 in the last 20 coronary cases. Perfusion: Single-vessel: antegrade cardioplegia; Double-vessel: antegrade cardioplegia.
Blood loss: Single vessel: 743 [671] mL; Double vessel: 968 [821] mL. Complications: 2/45 (4%) bleeding from the anastomosis 4/45 (9%) prolonged cross-clamp time 1/45 (2%) internal thoracic artery injury 3/45 (7%) Port-Access failure 1/45 (2%) hypovolaemic shock 1/45 (2%) myocardial infarction 1/45 (2%) hypoxic brain damage 1/45 (2%) moderate reperfusion injury 1/45 (2%) retrograde aortic dissection Wound infection: 0
It is important to note that the majority of complications occurred in the first 20 patients of this series and may be attributable to the learning curve.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
85 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Kappert 2001, GERMANY (Level IV) May 1999 to January 2001. 37 patients. Follow-up: 12 weeks. Intervention: Patients underwent on-pump (n=8) and off-pump (n=29) totally endoscopic coronary artery bypass grafting (TECAB) surgery using a wrist-enhanced robotic system. Inclusion criteria: Patients with coronary artery disease. Gender (M/F): 32/5 Age: 62 [9] years Exclusion criteria: Patients with decreased LVEF (<40%), decreased lung function (FEV1 < 1.0), obesity (body mass index (BMI) > 35) and intramyocardial LAD course or diffuse coronary artery sclerosis.
Operative time: Total: TECAB on-pump: 280 [80.2] mins; TECAB off-pump: 174 [65.6] mins. Internal mammary artery takedown (mins): LIMA RIMA TECAB on-pump 50 [17] 54 TECAB off-pump 35 [8] 42 [1] Anastomosis and cross-clamp time (mins): AT CCT TECAB on-pump 28 [5] 70 [6] TECAB off-pump 31 [10] NA Length of stay: Hospital stay: 6 [1] days ICU stay: 21 [20] hours Conversions: 1/37 (3%) Survival: 37/37 (100%)
Complications: 3/29 (10%) re-exploration 1/37? (3%) chest pain 1/37 (3%) angina (4 weeks postop) Inotropic support in sinus rhythm: 0 Acute myocardial ischemia: 0
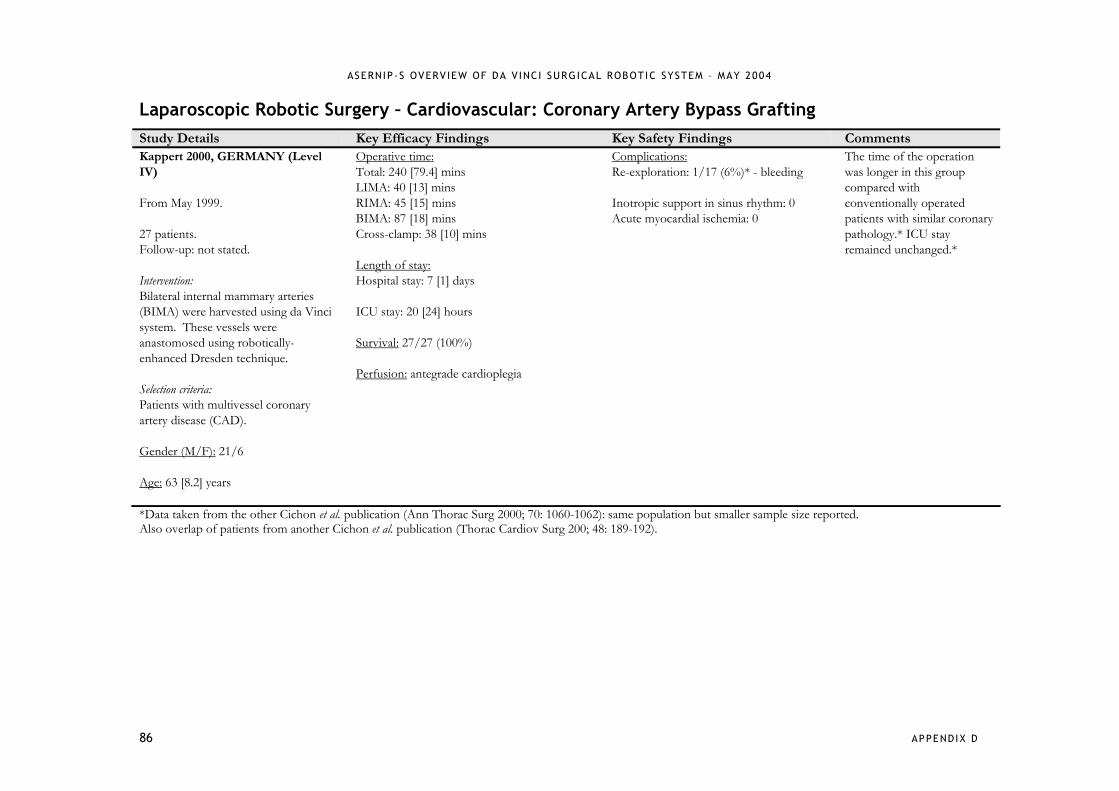
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
86 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Kappert 2000, GERMANY (Level IV) From May 1999. 27 patients. Follow-up: not stated. Intervention: Bilateral internal mammary arteries (BIMA) were harvested using da Vinci system. These vessels were anastomosed using robotically-enhanced Dresden technique. Selection criteria: Patients with multivessel coronary artery disease (CAD). Gender (M/F): 21/6 Age: 63 [8.2] years
Operative time: Total: 240 [79.4] mins LIMA: 40 [13] mins RIMA: 45 [15] mins BIMA: 87 [18] mins Cross-clamp: 38 [10] mins Length of stay: Hospital stay: 7 [1] days ICU stay: 20 [24] hours Survival: 27/27 (100%) Perfusion: antegrade cardioplegia
Complications: Re-exploration: 1/17 (6%)* - bleeding Inotropic support in sinus rhythm: 0 Acute myocardial ischemia: 0
The time of the operation was longer in this group compared with conventionally operated patients with similar coronary pathology.* ICU stay remained unchanged.*
*Data taken from the other Cichon et al. publication (Ann Thorac Surg 2000; 70: 1060-1062): same population but smaller sample size reported. Also overlap of patients from another Cichon et al. publication (Thorac Cardiov Surg 200; 48: 189-192).
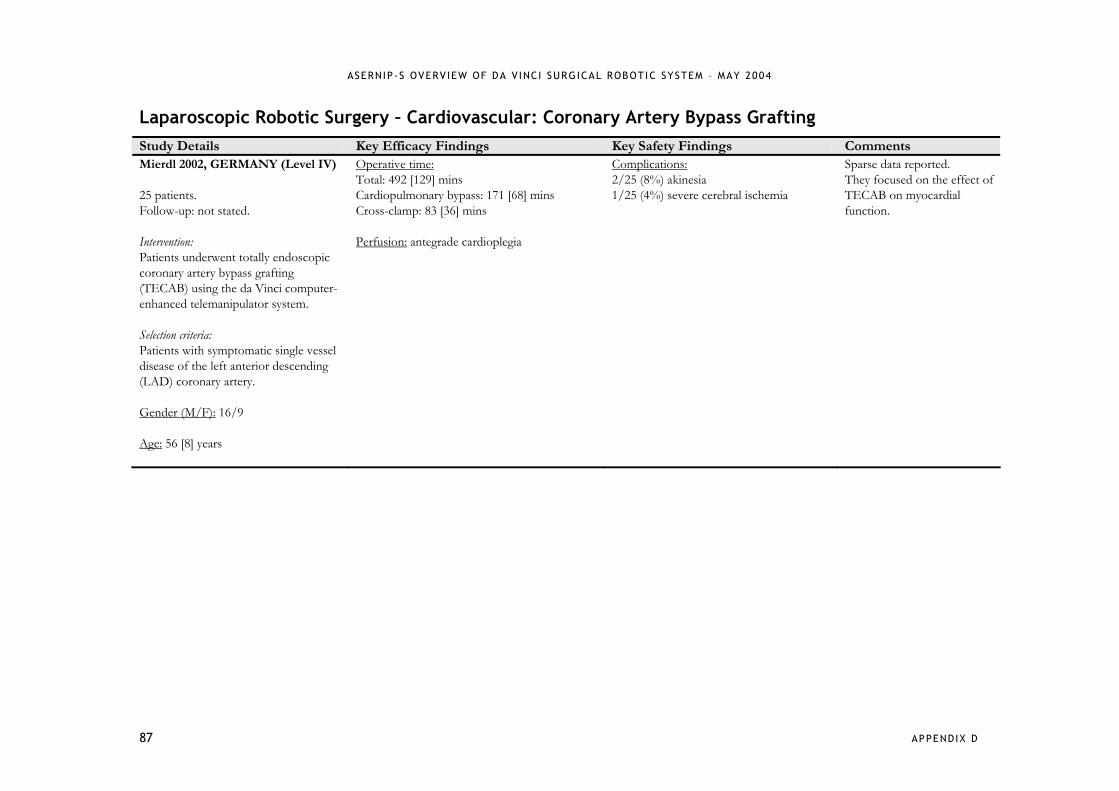
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
87 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Mierdl 2002, GERMANY (Level IV) 25 patients. Follow-up: not stated. Intervention: Patients underwent totally endoscopic coronary artery bypass grafting (TECAB) using the da Vinci computer-enhanced telemanipulator system. Selection criteria: Patients with symptomatic single vessel disease of the left anterior descending (LAD) coronary artery. Gender (M/F): 16/9 Age: 56 [8] years
Operative time: Total: 492 [129] mins Cardiopulmonary bypass: 171 [68] mins Cross-clamp: 83 [36] mins Perfusion: antegrade cardioplegia
Complications: 2/25 (8%) akinesia 1/25 (4%) severe cerebral ischemia
Sparse data reported. They focused on the effect of TECAB on myocardial function.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
88 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments D’Attellis 2002, FRANCE (Level IV) 20 patients. Follow-up: not stated. Intervention: Patients were scheduled for the following procedures: coronary artery bypass graft (CABG) surgery (n=9), mitral valve repair (MVR) (n=5), MVR + atrial septal defect (ASD) repair (n=2), tricuspid valve repair (n=2), ASD + septal aneurysm repair (n=1) and tricuspid valve replacement (n=1). Surgery was done with the aid of the da Vinci surgical robot. Selection criteria: All CABG surgery patients presented with a significant stenosis of the left anterior descending (LAD) coronary artery requiring surgical revascularisation. Gender (M/F): 13/7 Age: 53.5 [5] years
Data reported on 16/20 (80%) patients. The first 4 patients receiving robotic-assisted CABG were reported individually. Operative time: Total cardiopulmonary bypass time: 109 [14] mins Length of stay: Hospital stay: 12 days ICU stay: 47 hours Conversions: 2/16 (12.5%) 2/4 (50%) CABG patients. Perfusion: antegrade cardioplegia
Blood loss: 355 [85] mL during the 1st 24 hours postop Complications: Intraoperative difficulties: 1/16 (6%) video system dysfunction 1/16 (6%) mammary artery bleeding 2/16 (12.5%) tool manipulation 3/16 (19%) patient-robot conflict Postoperative: 2/16 (12.5%) re-exploration 1/16 (6%) mild shoulder pain and paraesthesia 1/16 (6%) groin lymphocele 1/16 (6%) recurrent bacterial endocarditis Mortality: In-hospital mortality: 0 1/16 (6%) 6 months postop – low cardiac output after MVR
The length of anaesthesia and surgery is longer during robotic surgery than with conventional cardiac surgery. It is mostly time-consuming during patient preparation and system (robot) setup. Patient positioning is of fundamental importance in decreasing patient-robot conflict during surgery, defined as a limitation in the free movement of the robot’s telemanipulated arms by interference with the patient’s body.
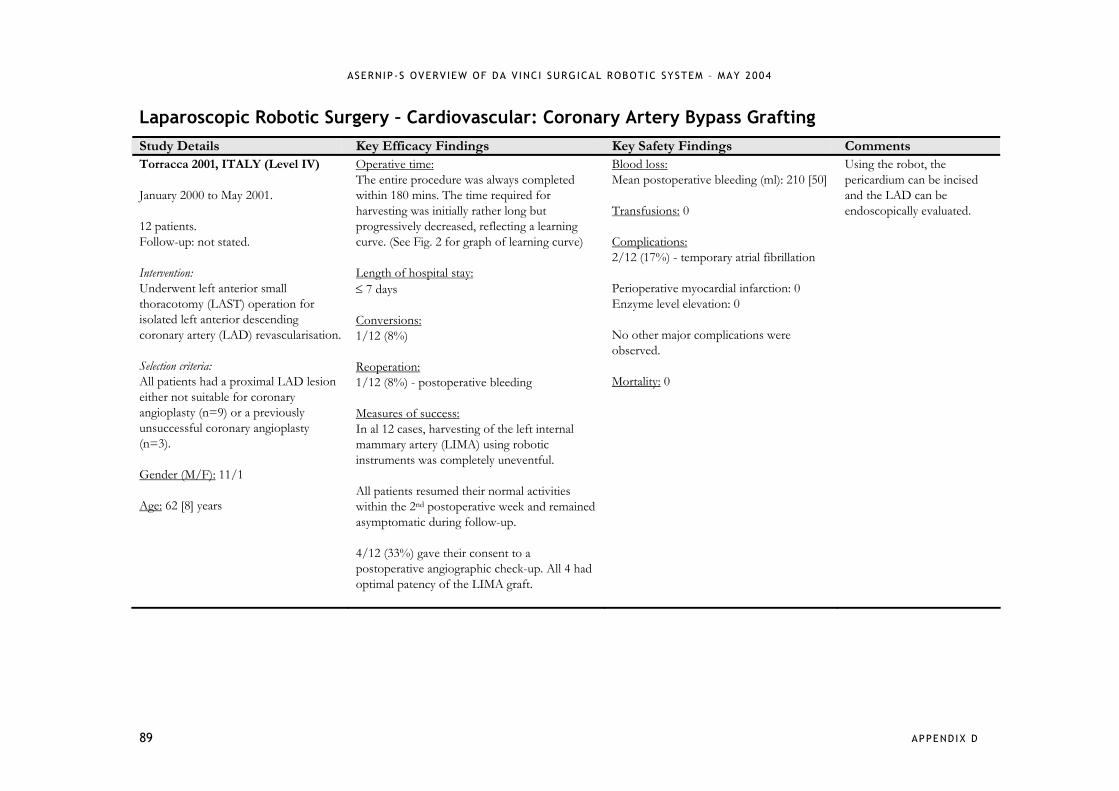
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
89 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Coronary Artery Bypass Grafting Study Details Key Efficacy Findings Key Safety Findings Comments Torracca 2001, ITALY (Level IV) January 2000 to May 2001. 12 patients. Follow-up: not stated. Intervention: Underwent left anterior small thoracotomy (LAST) operation for isolated left anterior descending coronary artery (LAD) revascularisation. Selection criteria: All patients had a proximal LAD lesion either not suitable for coronary angioplasty (n=9) or a previously unsuccessful coronary angioplasty (n=3). Gender (M/F): 11/1 Age: 62 [8] years
Operative time: The entire procedure was always completed within 180 mins. The time required for harvesting was initially rather long but progressively decreased, reflecting a learning curve. (See Fig. 2 for graph of learning curve) Length of hospital stay: ≤ 7 days Conversions: 1/12 (8%) Reoperation: 1/12 (8%) - postoperative bleeding Measures of success: In al 12 cases, harvesting of the left internal mammary artery (LIMA) using robotic instruments was completely uneventful. All patients resumed their normal activities within the 2nd postoperative week and remained asymptomatic during follow-up. 4/12 (33%) gave their consent to a postoperative angiographic check-up. All 4 had optimal patency of the LIMA graft.
Blood loss: Mean postoperative bleeding (ml): 210 [50] Transfusions: 0 Complications: 2/12 (17%) - temporary atrial fibrillation Perioperative myocardial infarction: 0 Enzyme level elevation: 0 No other major complications were observed. Mortality: 0
Using the robot, the pericardium can be incised and the LAD can be endoscopically evaluated.
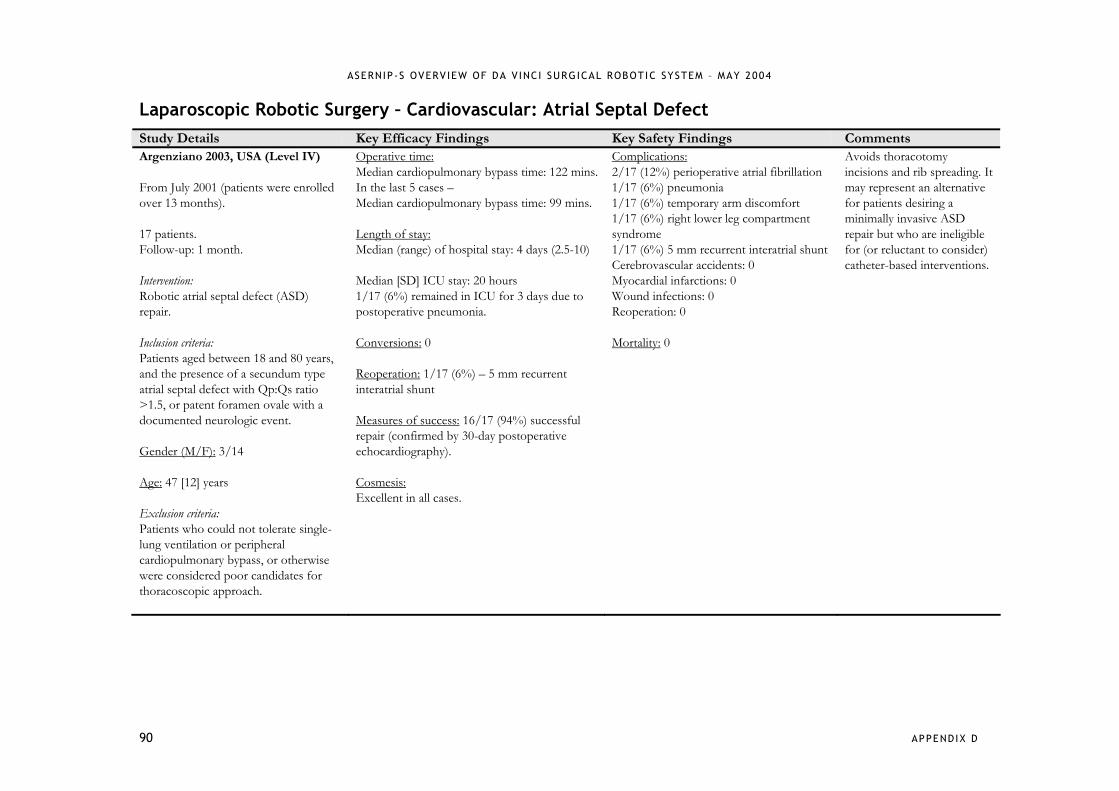
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
90 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Atrial Septal Defect Study Details Key Efficacy Findings Key Safety Findings Comments Argenziano 2003, USA (Level IV) From July 2001 (patients were enrolled over 13 months). 17 patients. Follow-up: 1 month. Intervention: Robotic atrial septal defect (ASD) repair. Inclusion criteria: Patients aged between 18 and 80 years, and the presence of a secundum type atrial septal defect with Qp:Qs ratio >1.5, or patent foramen ovale with a documented neurologic event. Gender (M/F): 3/14 Age: 47 [12] years Exclusion criteria: Patients who could not tolerate single-lung ventilation or peripheral cardiopulmonary bypass, or otherwise were considered poor candidates for thoracoscopic approach.
Operative time: Median cardiopulmonary bypass time: 122 mins. In the last 5 cases – Median cardiopulmonary bypass time: 99 mins. Length of stay: Median (range) of hospital stay: 4 days (2.5-10) Median [SD] ICU stay: 20 hours 1/17 (6%) remained in ICU for 3 days due to postoperative pneumonia. Conversions: 0 Reoperation: 1/17 (6%) – 5 mm recurrent interatrial shunt Measures of success: 16/17 (94%) successful repair (confirmed by 30-day postoperative echocardiography). Cosmesis: Excellent in all cases.
Complications: 2/17 (12%) perioperative atrial fibrillation 1/17 (6%) pneumonia 1/17 (6%) temporary arm discomfort 1/17 (6%) right lower leg compartment syndrome 1/17 (6%) 5 mm recurrent interatrial shunt Cerebrovascular accidents: 0 Myocardial infarctions: 0 Wound infections: 0 Reoperation: 0 Mortality: 0
Avoids thoracotomy incisions and rib spreading. It may represent an alternative for patients desiring a minimally invasive ASD repair but who are ineligible for (or reluctant to consider) catheter-based interventions.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
91 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Atrial Septal Defect Study Details Key Efficacy Findings Key Safety Findings Comments Wimmer-Greinecker 2003, GERMANY (Level IV) From August 1999. 10 consecutive patients. Follow-up: 1 month. Intervention: Totally endoscopic atrial septal repair (TEASR) with the da Vinci surgical system. Selection criteria: All patients had a fossa ovalis type of ASD. Median [SD] age: 45.5 [10.0] years
Operative time: 262 [37] mins Length of stay: Hospital stay: 9.5 [1.9] days ICU stay: 20 [33] hours Conversions: 2/10 (20%) Cosmesis: Excellent
Complications: Perioperative morbidity: 0 Intraoperative complications: 0 Postoperative complications: 0
There are risks with Port-Access technology such as aortic dissections and thromboembolic events.
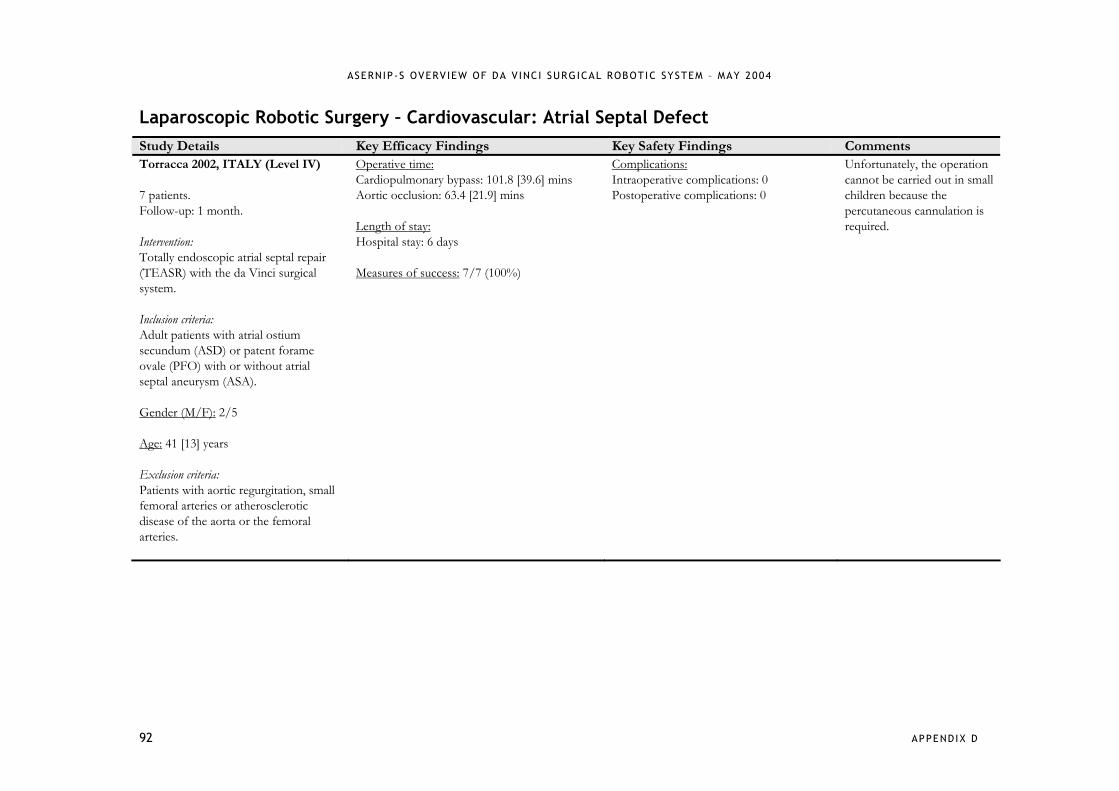
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
92 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Atrial Septal Defect Study Details Key Efficacy Findings Key Safety Findings Comments Torracca 2002, ITALY (Level IV) 7 patients. Follow-up: 1 month. Intervention: Totally endoscopic atrial septal repair (TEASR) with the da Vinci surgical system. Inclusion criteria: Adult patients with atrial ostium secundum (ASD) or patent forame ovale (PFO) with or without atrial septal aneurysm (ASA). Gender (M/F): 2/5 Age: 41 [13] years Exclusion criteria: Patients with aortic regurgitation, small femoral arteries or atherosclerotic disease of the aorta or the femoral arteries.
Operative time: Cardiopulmonary bypass: 101.8 [39.6] mins Aortic occlusion: 63.4 [21.9] mins Length of stay: Hospital stay: 6 days Measures of success: 7/7 (100%)
Complications: Intraoperative complications: 0 Postoperative complications: 0
Unfortunately, the operation cannot be carried out in small children because the percutaneous cannulation is required.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
93 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Mitral Valve Repair Study Details Key Efficacy Findings Key Safety Findings Comments Nifong 2003, USA (Level IV) May 2000 to December 2001. 38 patients. Follow-up: 1 month. Intervention: Mitral valve repairs using the da Vinci surgical system. Gp 1: first 19 patients; Gp 2: last 19 patients. Inclusion criteria: Patients with non-ischemic moderate to severe mitral insufficiency. Age: Gp 1: 55.6 [3.0] years; Gp 2: 60.6 [3.0] years. Exclusion criteria: Patients with renal failure, liver dysfunction, bleeding disorders, pulmonary hypertension (PAS > 60 torr), significant aortic or tricuspid valve disease, coronary artery disease requiring operation, recent myocardial ischemia (< 30 days), severely calcified mitral valve annulus, body mass index (> 35 kg/mtrs2), significant anterior leaflet pathology and those needing valve replacements.
Operative time: Gp 1: 306 [6] mins (5.1 [0.1] hours); Gp 2: 264 [6] mins (4.4 [0.1] hours), p=0.04. Length of stay: Hospital stay: Gp 1: 3.8 [0.3] days; Gp 2: 4.1 [0.4] days, pns. ICU stay: Gp 1: 21.6 [1.8] hours; Gp 2: 23.2 [4.3] hours, pns. Conversions: 0 Reoperation: 1/38 (3%)
Transfusions: Gp 1: 3/19 (16%) – 4.3 units per patient; Gp 2: 3/19 (16%) – 2.7 units per patient. Complications: 1/38 (3%) re-exploration due to bleeding. 1/38 (3%) haemolysis Device-related complications: 0 Mortality: 1/38 (3%) – stroke at 20 days postop. Operative deaths: 0
Comprehensive training should facilitate skill development in this field.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
94 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Mitral Valve Repair Study Details Key Efficacy Findings Key Safety Findings Comments Mohr 2001, GERMANY (Level IV)* July 1997 to April 2000. 17 patients. Follow-up: up to 6 months. Intervention: Mitral valve was repaired using the da Vinci telemanipulation system. Inclusion criteria: Patients with non-ischemic mitral valve insufficiency, a large left atria to allow some work space for the robotic instruments and no substantial concomitant disease requiring additional procedures. Gender (M/F): 7/8* Age: 58 [9] years* Exclusion criteria: Patients with severe involvement in both leaflets, a calcified annulus or concomitant mitral valve disease.
Operative time: 201 [53] mins Length of stay: Hospital stay: 10 [5] days ICU stay: 19 [8] hours Conversions: 0 Measures of success: 14/17 (82%) successful repair
Complications: 1/17 (6%) developed grade 2 mitral insufficiency 2/17 (12%) postoperative confusion 1/17 (6%) re-intubation for respiratory insufficiency 1/17 (6%) persistent pneumothorax 3/17 (18%) minor residual regurgitation Mortality: 0
While robotic videoscopic guidance for a less invasive mitral valve operation has already found widespread application, the use of a telemanipulation system for remote mitral valve repair is still considered experimental surgery.*
*15 patients originally included in Autschbach study (J Card Surg 2000; 15: 82-87).

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
95 APPENDIX D
Laparoscopic Robotic Surgery – Cardiovascular: Case Reports Cardiovascular Procedure Patients Outcomes
Dogan 2001 totally endoscopic sequential arterial coronary artery bypass (“jump graft” technique)
n=2 operative times prolonged compared to normal techniques
moderate reperfusion injury of cannulated right leg in first patient
technique complex and requires close cooperation of surgeon at console, patient site surgeon, anaesthetists, and perfusionist
Dogan 2002 totally endoscopic bilateral internal thoracic artery (ITA) bypass grafting
n=1 patient transferred from ICU on first postoperative day
recovery “uneventful”
POD6 angiogram showed patent ITAs bilaterally
Resley 2003 pericardial patch closure of atrial septal defect
n=1 longer bypass and ischaemic times
condition treated successfully and patient had “normal postoperative course”
Desgranges 2004 aorto-femoral bypass grafting n=5 aortic anastomoses successfully completed in 4/5 patients (3 minilaparotomy, 1 total laparotomy)
no robotic related complications noted
1/5 patients could not perform anastomoses due to external conflict of robot arms – converted to open laparotomy using conventional technique)
authors found that the benefits of the robotic system need to balanced against the problems they encountered with the size of the robotic system, the additional time taken in set-up and the costs associated with the system and its instruments
Killewich 2004 laparoscopic aortic reconstruction for occlusive disease
n=1 procedure successful
return to regular diet – POD2
LOS – 4 days
return to normal activity – 2.5 weeks
operative time considerably longer than for open procedure (8 hours)
no complications reported

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
96 APPENDIX D
Laparoscopic Robotic Surgery – Thoracic: Case Reports Thoracic Procedure Patients Outcomes
Melfi 2002 multiple thoracoscopic procedures - lobectomy (5) - tumour enucleation (3) - excision (3) - bulla stitching for spontaneous pneumothorax (1)
n=12 no technical/operative problems related to robot
operative times considerably longer than for conventional surgery but decreased with experience
no postoperative bleeding
less postoperative analgesia needed than with conventional surgery
Morgan 2003 multiple thoracoscopic procedures - phrenic nerve mobilization and insertion of pacemakers - mediastinal mass resection - lobectomy for lung mass - left ventricular lead placement for biventricular pacing
n=10
Phrenic nerve mobilization (n=6) - phrenic pacemakers successfully implanted in all 6 patients - no intraoperative complications or conversions to open - after mean 8.6 months all patients effective pacing - no device malfunctions or mechanical difficulties Mediastinal mass excisions - mass successfully excised with tumour capsule intact - no conversions to open or postoperative complications Pulmonary lobectomy - no postoperative complications LV lead placement - procedure successful and cardiac resynchronization reestablished
authors comment that robotic assistance allows relatively difficult thoracoscopic surgery to be performed by surgeons with limited thoracoscopic experience
Ashton 2003 totally endoscopic thymectomy for myasthenia gravis
n=1 bilateral approach used to dissect and remove hyperplasic thymus gland (no thymoma)
patient discharged on day 3 without complications
authors believe that robotic approach had limitations compared to other surgical approaches (such as transcervical and unilateral thoracoscopic thymectomy)
significant learning curve

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
97 APPENDIX D
Laparoscopic Robotic Surgery – Thoracic: Case Reports Thoracic Procedure Patients Outcomes
Bacchetta 2003 symptomatic pericardial cyst resection
n=1 cyst identified and removed without damage to phrenic nerve or communication with pericardium
procedure time shorter than for conventional video-assisted surgery
patient recovered within 10 days
at 5 months postoperative no wound complications, shortness of breath, pain
DeRose 2002 mediastinal mass evaluation (for diagnostic purposes and treatment planning)
n=1 robot enabled full 3D visualisation of entire thorax and multiple biopsies
precise electrocautery with the robot allowed for accurate haemostasis
authors report that multiple biopsies across length and depth of tumour aided diagnosis
no complications reported however, authors caution against use of transpleural approach if diagnosis of thymoma possible due to risk of drop metastases and pleural seeding
Yoshino 2002 video-assisted thoracoscopic extirpation of mediastinal mass
n=1 no injury to descending aorta, sympathetic nerve, hemiazygos vein or intercostal vein
well encapsulated bronchogenic cyst completely removed
no wound pain or shortness of breath reported by patient
authors believe that the robotic system allowed them to perform a complete excision more easily and safely than with a conventional thoracoscopic procedure
Yoshino 2001 thoracoscopic thymomectomy n=1 well-capsulated and well-lobulated mediastinal mass successfully removed
postoperative course “uneventful”
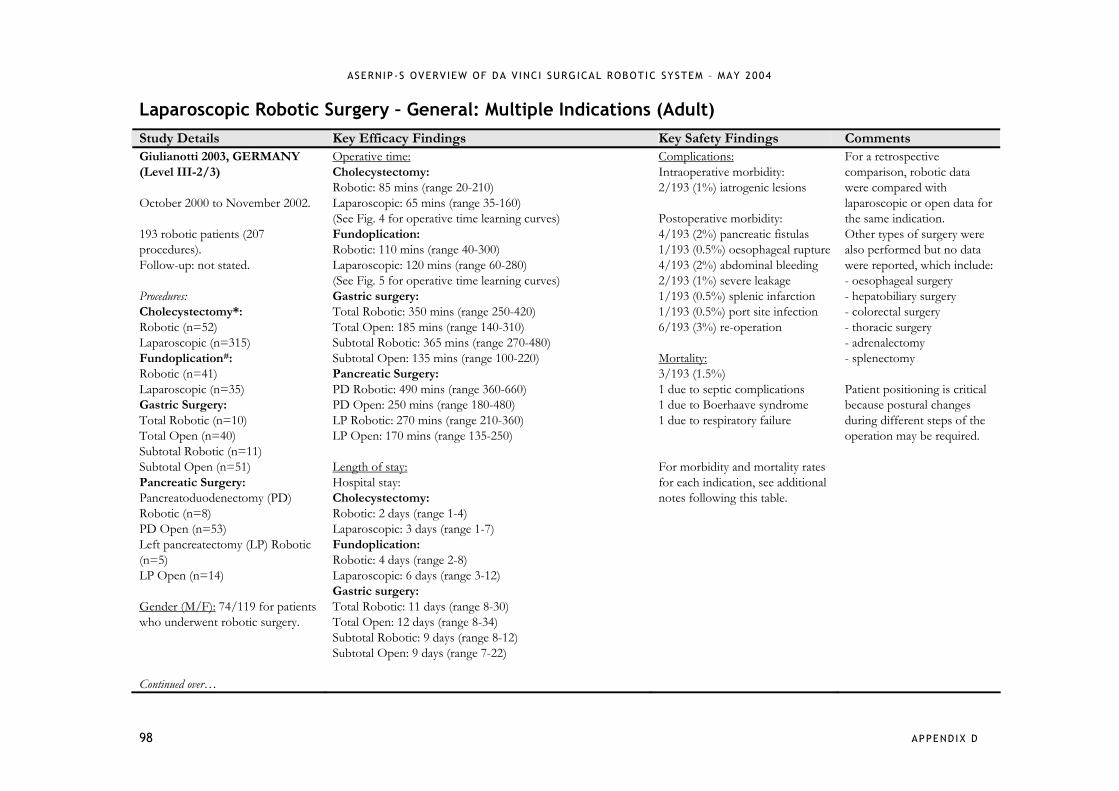
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
98 APPENDIX D
Laparoscopic Robotic Surgery – General: Multiple Indications (Adult) Study Details Key Efficacy Findings Key Safety Findings Comments Giulianotti 2003, GERMANY (Level III-2/3) October 2000 to November 2002. 193 robotic patients (207 procedures). Follow-up: not stated. Procedures: Cholecystectomy*: Robotic (n=52) Laparoscopic (n=315) Fundoplication#: Robotic (n=41) Laparoscopic (n=35) Gastric Surgery: Total Robotic (n=10) Total Open (n=40) Subtotal Robotic (n=11) Subtotal Open (n=51) Pancreatic Surgery: Pancreatoduodenectomy (PD) Robotic (n=8) PD Open (n=53) Left pancreatectomy (LP) Robotic (n=5) LP Open (n=14) Gender (M/F): 74/119 for patients who underwent robotic surgery. Continued over…
Operative time: Cholecystectomy: Robotic: 85 mins (range 20-210) Laparoscopic: 65 mins (range 35-160) (See Fig. 4 for operative time learning curves) Fundoplication: Robotic: 110 mins (range 40-300) Laparoscopic: 120 mins (range 60-280) (See Fig. 5 for operative time learning curves) Gastric surgery: Total Robotic: 350 mins (range 250-420) Total Open: 185 mins (range 140-310) Subtotal Robotic: 365 mins (range 270-480) Subtotal Open: 135 mins (range 100-220) Pancreatic Surgery: PD Robotic: 490 mins (range 360-660) PD Open: 250 mins (range 180-480) LP Robotic: 270 mins (range 210-360) LP Open: 170 mins (range 135-250) Length of stay: Hospital stay: Cholecystectomy: Robotic: 2 days (range 1-4) Laparoscopic: 3 days (range 1-7) Fundoplication: Robotic: 4 days (range 2-8) Laparoscopic: 6 days (range 3-12) Gastric surgery: Total Robotic: 11 days (range 8-30) Total Open: 12 days (range 8-34) Subtotal Robotic: 9 days (range 8-12) Subtotal Open: 9 days (range 7-22)
Complications: Intraoperative morbidity: 2/193 (1%) iatrogenic lesions Postoperative morbidity: 4/193 (2%) pancreatic fistulas 1/193 (0.5%) oesophageal rupture 4/193 (2%) abdominal bleeding 2/193 (1%) severe leakage 1/193 (0.5%) splenic infarction 1/193 (0.5%) port site infection 6/193 (3%) re-operation Mortality: 3/193 (1.5%) 1 due to septic complications 1 due to Boerhaave syndrome 1 due to respiratory failure For morbidity and mortality rates for each indication, see additional notes following this table.
For a retrospective comparison, robotic data were compared with laparoscopic or open data for the same indication. Other types of surgery were also performed but no data were reported, which include: - oesophageal surgery - hepatobiliary surgery - colorectal surgery - thoracic surgery - adrenalectomy - splenectomy Patient positioning is critical because postural changes during different steps of the operation may be required.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
99 APPENDIX D
Age: 55.9 years (range 16-91) for patients who underwent robotic surgery.
Pancreatic surgery: PD Robotic: 20 days (range 14-26) PD Open: 18 days (range 13-34) LP Robotic: 11 days (range 9-21) LP Open: 12 days (range 8-25) Conversions: 4/207 procedures (2.1%) - a cholecystectomy and a splenic aneurysmectomy were converted due to robotic technical problems.
*For cholecystectomy, n=66 – 52 single and 14 associated with another operation. The 52 single were compared with 315 patients who underwent conventional laparoscopic cholecystectomy. #For fundoplication, n=51 – 41 single and 10 associated with cholecystectomy. The 41 single were compared with 35 patients who underwent conventional laparoscopic fundoplication. Reported morbidity rates for each indication: Reported mortality rates for each indication:
Cholecystectomy: Cholecystectomy: Robotic: 1/52 (1.9%) Robotic: 0/52 (0%) Laparoscopic: 7/315 (2.2%) Laparoscopic: 0/315 (0%) Fundoplication: Fundoplication: Robotic: 2/41 (4.8%) Robotic: 0/41 (0%) Laparoscopic: 4/35 (11.4%) Laparoscopic: 0/35 (0%) Gastric Surgery: Gastric Surgery: Total Robotic: 3/10 (30.0%) Total Robotic: 0/10 (0%) Total Open: 5/40 (12.5%) Total Open: 1/40 (2.5%) Subtotal Robotic: 1/11 (9.1%) Subtotal Robotic: 1/11 (9.1%) Subtotal Open: 4/51 (7.8%) Subtotal Open: 0/51 (0%) Pancreatic Surgery: Pancreatic Surgery: PD Robotic: 3/8 (37.5%) PD Robotic: 1/8 (12.5%) PD Open: 17/53 (32.1%) PD Open: 3/53 (5.6%) LP Robotic: 1/5 (20.0%) LP Robotic: 0/5 (0%) LP Open: 4/14 (28.5%) LP Open: 0/14 (0%)

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
100 APPENDIX D
Laparoscopic Robotic Surgery – General: Multiple Indications (Adult) Study Details Key Efficacy Findings Key Safety Findings Comments Talamini 2003, USA (Level IV) June 2000 to June 2001. 211 patients. Follow-up: not stated. Procedures: Antireflux (n=69) Cholecystectomy (n=36) Heller myotomy (n=26) Bowel resection (n=17) Donor nephrectomy (n=15) Internal mammary mobilisation (n=14) Gastric bypass (n=7) Splenectomy (n=7) Adrenalectomy (n=6) Exploratory laparoscopy (n=3) Pyloroplasty (n=4) Gastrojejunostomy (n=2) Distal pancreatectomy (n=1) Duodenal polypectomy (n=1) Esophagectomy (n=1) Gastric mass resection (n=1) Lysis of adhesion (n=1)
Operative time: 188 [83] mins Length of stay: Median hospital stay: 1 day (range 0-37) Conversions: 5/211 (2.4%) – 3 due to technical reasons (too difficult for robotic or laparoscopic approach), 2 due to surgeon’s discomfort with difficult manoeuvres early in the robotic surgery learning curve.
Complications: Technical complications: 8/211 (3.8%) 3/211 (1.4%) system malfunctions 4/211 (1.9%) tip dislodgement 1/211 (0.5%) slipped trocar Medical/surgical complications: 8/211 (3.8%) 3/211 (1.4%) bleeding – 2 gastrointestinal, 1 operative-related 1/211 (0.5%) subcutaneous haematoma 1/211 (0.5%) Clostridium difficile colitis 1/211 (0.5%) atelectasis 1/211 (0.5%) fever Mortality: Intraoperative deaths: 0 Postoperative deaths: 1/211 (0.5%) – issues unrelated to robotic procedure
Authors of this article prefer to use the term ‘computer-enhanced telemanipulator device’ instead of robotic.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
101 APPENDIX D
Laparoscopic Robotic Surgery – General: Multiple Indications (Adult) Study Details Key Efficacy & Safety Findings Cadiere 2001, USA (Level IV) March 1997 to February 2001. 146 patients. Follow-up: not stated. Procedures: Fundoplications (n=39, 36 Nissen and 3 Toupet) Cholecystectomies (n=48) Fallopian tube reanastomoses (n=28) Gastroplasties for obesity (n=10) Intrarectal procedures (n=3) Inguinal hernias (n=3) Hysterectomies (n=2) Cardiac procedures (n=2) Prostatectomies (n=2) Arteriovenous fistulas (n=2) Lumbar sympathectomy (n=1) Appendectomy (n=1) Laryngeal exploration (n=1) Varicocele ligation (n=1) Endometriosis cure (n=1) Neosalpingostomy (n=1) Deferent canal reanastomosis (n=1)
Operating time* Hospital stay* Intervention No. (mins) (days) Complications Fundoplication 39 90 (54-270) 2 (1-4) 1/39 (3%) trocar perforated stomach 1/39 (3%) bleeding Cholecystectomy 48 62 (20-135) 2 (1-15) 1/48 (2%) perioperative bleeding required transfusion (1 unit) Tubal reanastomoses 28 125 (108-244) 1 (1-2) - Gastroplasty 9 60 (55-90) 2 (2-3) - Inguinal hernia 3 60 (50-79) 1 (1) - Intrarectal procedure 3 65 (60-79) 1 (1-2) - Hysterectomy 2 120 3 - Appendectomy 1 40 2 - Laryngoscopy 1 30 1 - Varicocele 1 27 1 - Lumbar sympathectomy 1 40 5 - *Values expressed as median (range). Comments: The articulated tools make the robotic procedure more similar to open surgery and made it easier to dissect the short gastric vessels as the dissecting tools could always come perpendicular to the vessels. A drawback of the robot system is that the 3D optical system is characterised by a narrow field of vision so dissection had to be interrupted to reposition the optics.
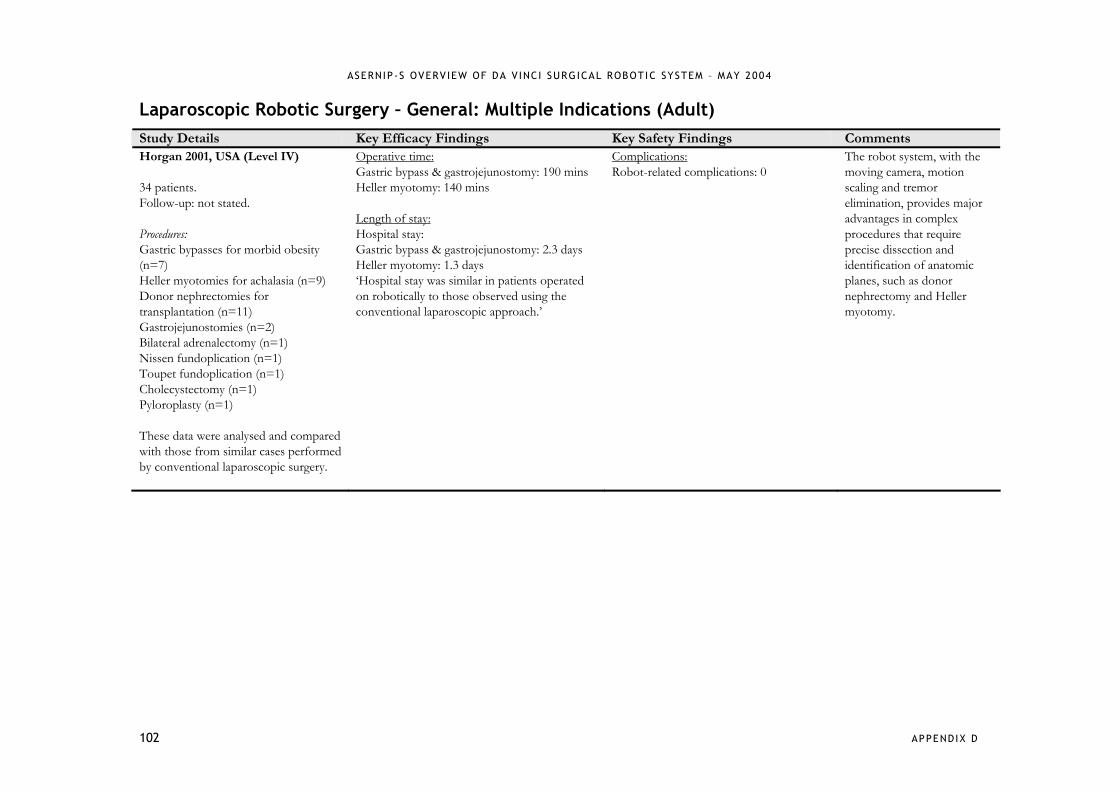
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
102 APPENDIX D
Laparoscopic Robotic Surgery – General: Multiple Indications (Adult) Study Details Key Efficacy Findings Key Safety Findings Comments Horgan 2001, USA (Level IV) 34 patients. Follow-up: not stated. Procedures: Gastric bypasses for morbid obesity (n=7) Heller myotomies for achalasia (n=9) Donor nephrectomies for transplantation (n=11) Gastrojejunostomies (n=2) Bilateral adrenalectomy (n=1) Nissen fundoplication (n=1) Toupet fundoplication (n=1) Cholecystectomy (n=1) Pyloroplasty (n=1) These data were analysed and compared with those from similar cases performed by conventional laparoscopic surgery.
Operative time: Gastric bypass & gastrojejunostomy: 190 mins Heller myotomy: 140 mins Length of stay: Hospital stay: Gastric bypass & gastrojejunostomy: 2.3 days Heller myotomy: 1.3 days ‘Hospital stay was similar in patients operated on robotically to those observed using the conventional laparoscopic approach.’
Complications: Robot-related complications: 0
The robot system, with the moving camera, motion scaling and tremor elimination, provides major advantages in complex procedures that require precise dissection and identification of anatomic planes, such as donor nephrectomy and Heller myotomy.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
103 APPENDIX D
Laparoscopic Robotic Surgery – General: Multiple Indications (Adult) Study Details Key Efficacy Findings Key Safety Findings Comments Hashizume 2002, JAPAN (Level IV) July 2000 to January 2001. 22 patients (23 procedures). Follow-up: not stated. Procedures: Cholecystectomy (n=6) Splenectomy (n=5) Distal gastrectomy (n=2) Herniorrhaphy (n=2) Hiatus hernia repair (n=2) Tumour extraction (n=2) Hemicolectomy (n=1) Ileocecal resection (n=1) Sigmoidectomy (n=1) Thymectomy (n=1) Gender (M/F): 9/13 Age: 60.0 [16.5] years
Operative time: 237.8 [120.3] mins Time of robotic work: 130.0 [102.3] mins Length of stay: Hospital stay: 17.2 [10.2] days
Complications: 2/23 (9%) wire of Endo-wrist forceps broke during surgery 1/23 (4%) electric power went out due to incorrect use of power source for the da Vinci system Major robot-related complications: 0
In the first few cases, all procedures were performed with only the da Vinci system. Thereafter, the da Vinci system was only used partially as one of the endoscopic surgical tools especially in such complicated endoscopic procedures as gastrointestinal tract surgery. It was difficult for the operator to get a good feel of the extent needed to tighten up the ligatures.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
104 APPENDIX D
Laparoscopic Robotic Surgery – General: Cholecystectomy Study Details Key Efficacy Findings Key Safety Findings Comments Hourmont 2003, USA (Level III-2) August 2000 to September 2001. 50 consecutive patients. Follow-up: not stated. Comparison: da Vinci: 25 patients underwent laparoscopic cholecystectomy using the da Vinci system; AESOP: 25 patients underwent laparoscopic cholecystectomy using the AESOP system. Selection criteria: Patients requiring laparoscopic cholecystectomy. Age: da Vinci: 44.6 [16.2] years; AESOP: 48.0 [20.4] years.
Operative time: da Vinci: 152 [22] mins (range 98-228); AESOP: 138 [33] mins (range 88-204), p<0.05. (see Table 5 for learning curve table) Length of stay: Hospital stay: da Vinci: 1.2 [0.6] days (range 1-3); AESOP: 1.6 [1.6] days (range 0-8). Conversions: 0
Blood loss: Average drop in haematocrit: da Vinci: 1.2; AESOP: 1.6. Complications: da Vinci: 2/25 (8%) wound infection at umbilical trocar site AESOP: 1/25 (4%) wound infection at umbilical trocar site 1/25 (4%) re-exploration 1/25 (4%) gallstone pancreatitis Mortality: 0
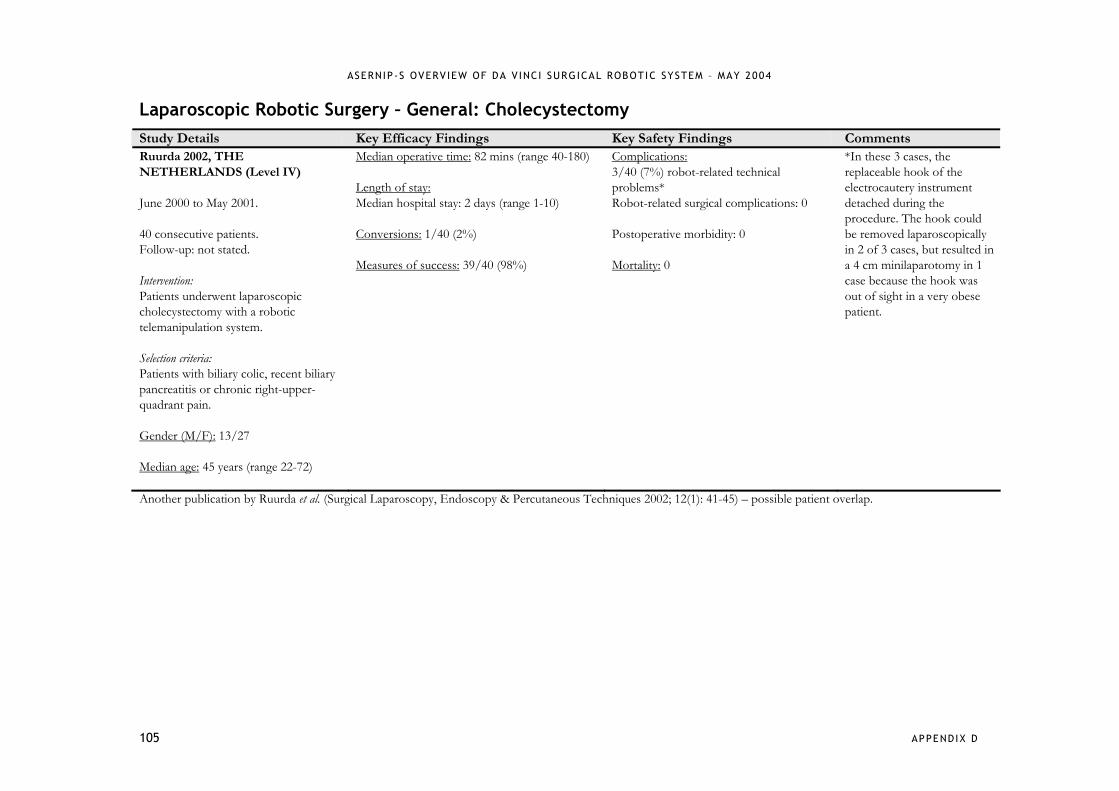
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
105 APPENDIX D
Laparoscopic Robotic Surgery – General: Cholecystectomy Study Details Key Efficacy Findings Key Safety Findings Comments Ruurda 2002, THE NETHERLANDS (Level IV) June 2000 to May 2001. 40 consecutive patients. Follow-up: not stated. Intervention: Patients underwent laparoscopic cholecystectomy with a robotic telemanipulation system. Selection criteria: Patients with biliary colic, recent biliary pancreatitis or chronic right-upper-quadrant pain. Gender (M/F): 13/27 Median age: 45 years (range 22-72)
Median operative time: 82 mins (range 40-180) Length of stay: Median hospital stay: 2 days (range 1-10) Conversions: 1/40 (2%) Measures of success: 39/40 (98%)
Complications: 3/40 (7%) robot-related technical problems* Robot-related surgical complications: 0 Postoperative morbidity: 0 Mortality: 0
*In these 3 cases, the replaceable hook of the electrocautery instrument detached during the procedure. The hook could be removed laparoscopically in 2 of 3 cases, but resulted in a 4 cm minilaparotomy in 1 case because the hook was out of sight in a very obese patient.
Another publication by Ruurda et al. (Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 2002; 12(1): 41-45) – possible patient overlap.
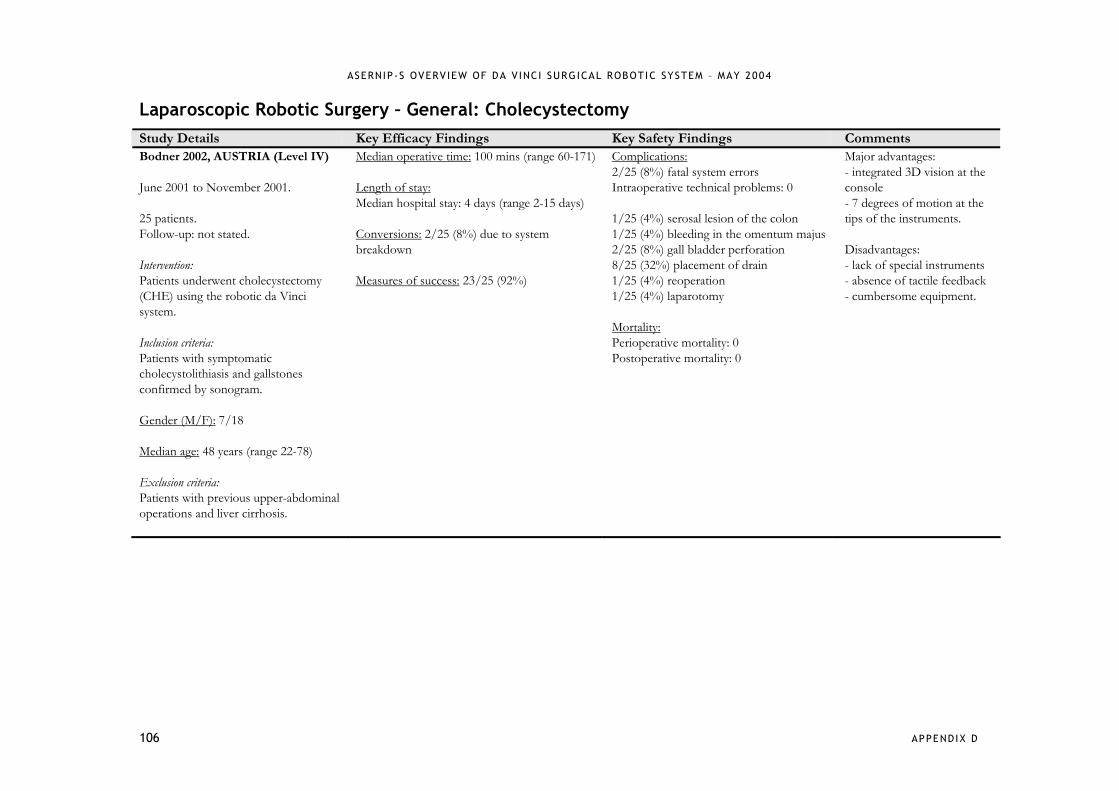
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
106 APPENDIX D
Laparoscopic Robotic Surgery – General: Cholecystectomy Study Details Key Efficacy Findings Key Safety Findings Comments Bodner 2002, AUSTRIA (Level IV) June 2001 to November 2001. 25 patients. Follow-up: not stated. Intervention: Patients underwent cholecystectomy (CHE) using the robotic da Vinci system. Inclusion criteria: Patients with symptomatic cholecystolithiasis and gallstones confirmed by sonogram. Gender (M/F): 7/18 Median age: 48 years (range 22-78) Exclusion criteria: Patients with previous upper-abdominal operations and liver cirrhosis.
Median operative time: 100 mins (range 60-171) Length of stay: Median hospital stay: 4 days (range 2-15 days) Conversions: 2/25 (8%) due to system breakdown Measures of success: 23/25 (92%)
Complications: 2/25 (8%) fatal system errors Intraoperative technical problems: 0 1/25 (4%) serosal lesion of the colon 1/25 (4%) bleeding in the omentum majus 2/25 (8%) gall bladder perforation 8/25 (32%) placement of drain 1/25 (4%) reoperation 1/25 (4%) laparotomy Mortality: Perioperative mortality: 0 Postoperative mortality: 0
Major advantages: - integrated 3D vision at the console - 7 degrees of motion at the tips of the instruments. Disadvantages: - lack of special instruments - absence of tactile feedback - cumbersome equipment.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
107 APPENDIX D
Laparoscopic Robotic Surgery – General: Cholecystectomy Study Details Key Efficacy Findings Key Safety Findings Comments Perez 2003, USA (Level IV) January 2000 to September 2001. 20 patients. Follow-up: not stated. Intervention: Patients underwent telerobotically assisted laparoscopic cholecystectomy (TALC). Selection criteria: Patients with symptomatic cholelithiasis. Gender (M/F): 4/16 Age: 47 [4] years
Operative time: 152 [8] mins Length of stay: Conversions: 0
Complications: Intraoperative complications: 0 Postoperative complications: 0
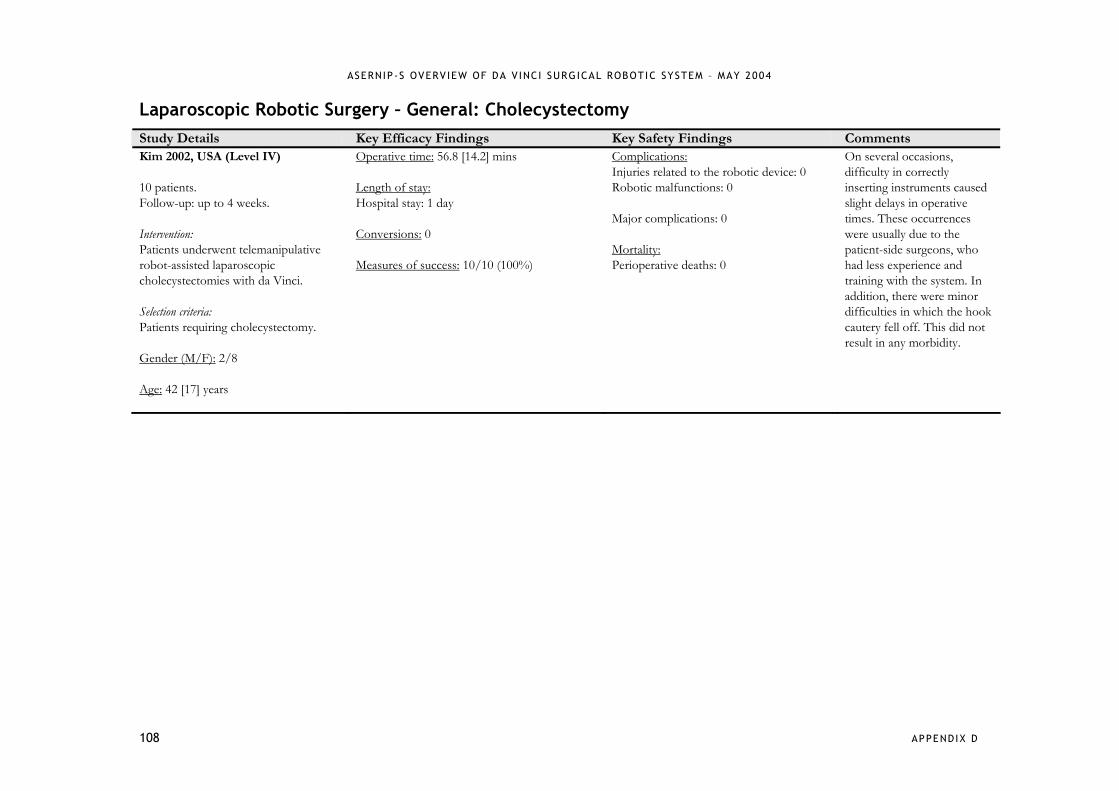
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
108 APPENDIX D
Laparoscopic Robotic Surgery – General: Cholecystectomy Study Details Key Efficacy Findings Key Safety Findings Comments Kim 2002, USA (Level IV) 10 patients. Follow-up: up to 4 weeks. Intervention: Patients underwent telemanipulative robot-assisted laparoscopic cholecystectomies with da Vinci. Selection criteria: Patients requiring cholecystectomy. Gender (M/F): 2/8 Age: 42 [17] years
Operative time: 56.8 [14.2] mins Length of stay: Hospital stay: 1 day Conversions: 0 Measures of success: 10/10 (100%)
Complications: Injuries related to the robotic device: 0 Robotic malfunctions: 0 Major complications: 0 Mortality: Perioperative deaths: 0
On several occasions, difficulty in correctly inserting instruments caused slight delays in operative times. These occurrences were usually due to the patient-side surgeons, who had less experience and training with the system. In addition, there were minor difficulties in which the hook cautery fell off. This did not result in any morbidity.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
109 APPENDIX D
Laparoscopic Robotic Surgery – General: Fundoplication Study Details Key Efficacy Findings Key Safety Findings Comments Melvin 2002, USA (Level III-2) 40 patients. Follow-up: 6.7 months (range 4-10) for robotic group; 11.2 months (range 7-13) for control group. Comparison: Robotic: 20 patients underwent computer enhanced robotic fundoplication; Control: 20 patients underwent standard laparoscopic treatment. Inclusion criteria: Patients referred to a single surgeon’s practice with the diagnosis of gastroesophageal reflux disease (GERD) and selected for surgery. All patients required medical therapy and had symptoms of GERD for at least 6 months. Gender (M/F): Robotic: 13/7; Control: 7/13. Age: Robotic: 42.9 years; Control: 49.6 years. Exclusion criteria: Patients with previous surgery of the gastroesophageal junction, morbid obesity and paroesophageal hernia.
Operative time: Robotic: 140.9 mins (range 88-271); Control: 97.1 mins (range 45-168), p=0.001. Length of stay: Hospital stay: 1-2 days (for both groups).
Complications: Robotic Control No (%) No (%) Endoscopy 3 (15) 2 (10) Dilation 1 (5) 1 (5) Dysphagia 5 (25) 3 (15) Heartburn 4 (20) 3 (15) Regurgitation 4 (20) 0 Bloating 5 (25) 7 (35) Reoperation 1 (5) 0
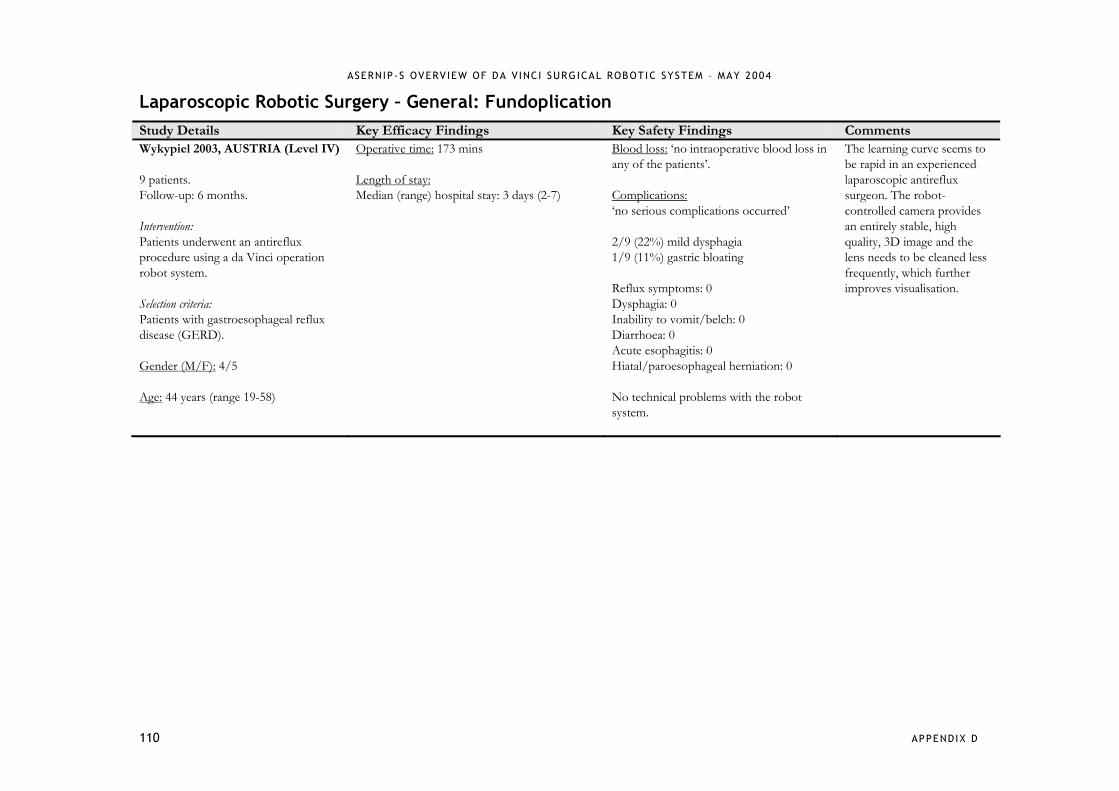
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
110 APPENDIX D
Laparoscopic Robotic Surgery – General: Fundoplication Study Details Key Efficacy Findings Key Safety Findings Comments Wykypiel 2003, AUSTRIA (Level IV) 9 patients. Follow-up: 6 months. Intervention: Patients underwent an antireflux procedure using a da Vinci operation robot system. Selection criteria: Patients with gastroesophageal reflux disease (GERD). Gender (M/F): 4/5 Age: 44 years (range 19-58)
Operative time: 173 mins Length of stay: Median (range) hospital stay: 3 days (2-7)
Blood loss: ‘no intraoperative blood loss in any of the patients’. Complications: ‘no serious complications occurred’ 2/9 (22%) mild dysphagia 1/9 (11%) gastric bloating Reflux symptoms: 0 Dysphagia: 0 Inability to vomit/belch: 0 Diarrhoea: 0 Acute esophagitis: 0 Hiatal/paroesophageal herniation: 0 No technical problems with the robot system.
The learning curve seems to be rapid in an experienced laparoscopic antireflux surgeon. The robot-controlled camera provides an entirely stable, high quality, 3D image and the lens needs to be cleaned less frequently, which further improves visualisation.
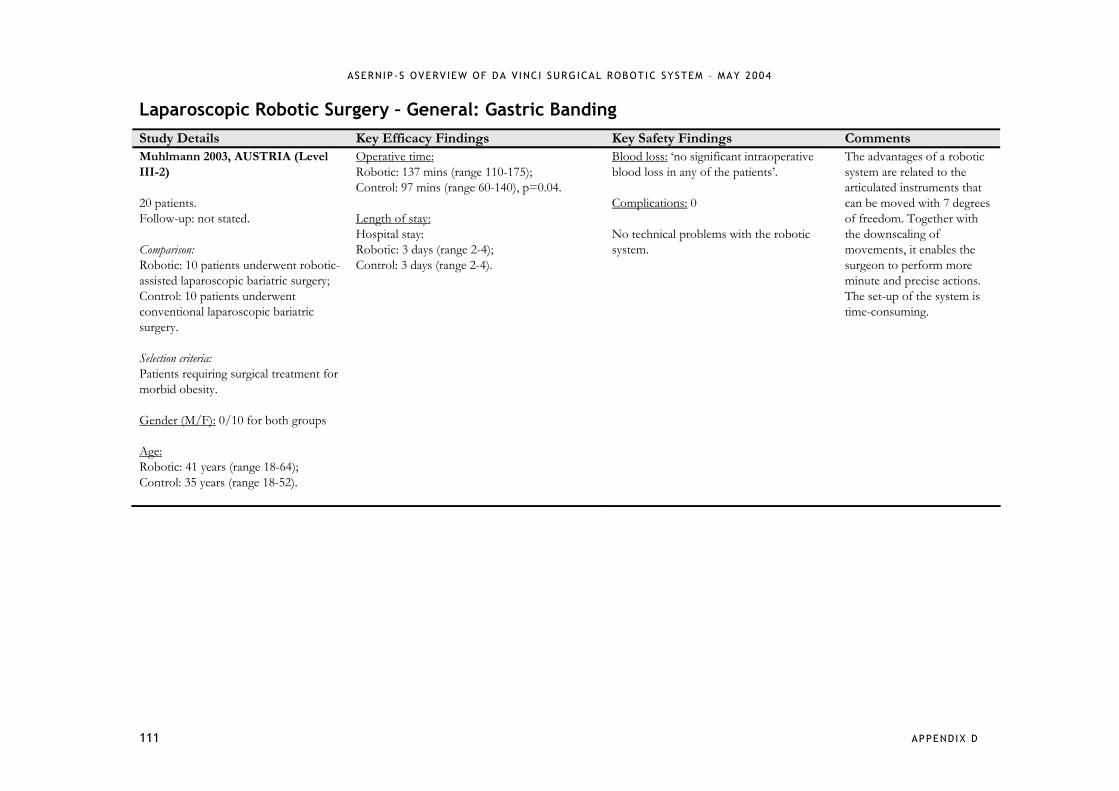
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
111 APPENDIX D
Laparoscopic Robotic Surgery – General: Gastric Banding Study Details Key Efficacy Findings Key Safety Findings Comments Muhlmann 2003, AUSTRIA (Level III-2) 20 patients. Follow-up: not stated. Comparison: Robotic: 10 patients underwent robotic-assisted laparoscopic bariatric surgery; Control: 10 patients underwent conventional laparoscopic bariatric surgery. Selection criteria: Patients requiring surgical treatment for morbid obesity. Gender (M/F): 0/10 for both groups Age: Robotic: 41 years (range 18-64); Control: 35 years (range 18-52).
Operative time: Robotic: 137 mins (range 110-175); Control: 97 mins (range 60-140), p=0.04. Length of stay: Hospital stay: Robotic: 3 days (range 2-4); Control: 3 days (range 2-4).
Blood loss: ‘no significant intraoperative blood loss in any of the patients’. Complications: 0 No technical problems with the robotic system.
The advantages of a robotic system are related to the articulated instruments that can be moved with 7 degrees of freedom. Together with the downscaling of movements, it enables the surgeon to perform more minute and precise actions. The set-up of the system is time-consuming.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
112 APPENDIX D
Laparoscopic Robotic Surgery – General: Laparoscopic Live-Donor Nephrectomy Study Details Key Efficacy Findings Key Safety Findings Comments Horgan 2002, USA (Level III-3) September 2000 to June 2001 for Robotic and 1998 to 2001 for Laparoscopic and Open. 60 patients. Follow-up: not stated. Comparison: Robotic: 12 patients underwent laparoscopic living donor robotic nephrectomy; Laparoscopic: 23 patients underwent standard laparoscopic living donor nephrectomy; Open: 25 patients underwent open nephrectomy. Gender (M/F): Robotic: 7/5; Laparoscopic: 13/10; Open: 16/9. Age: Robotic: 33 years (range 21-55); Laparoscopic: 34 years (range 22-51); Open: 36 years (range 18-55).
Operative time: Robotic: 166 mins Laparoscopic: 110 mins Open: 95 mins (range 70-140) Length of stay: Hospital stay: Robotic: 1.9 days (range 1-5) Laparoscopic: 2.5 days (range 1-5) Open: 5.1 days (range 3-9) Conversions: Robotic: 0 Cosmesis: 12/12 (100%) reported overall satisfaction
Blood loss: Robotic: 68 mL Laparoscopic: <100 mL Open: >100 mL Transfusions: Robotic: 0 Complications: Robotic: 1/12 (8%) superficial wound infection at hand-port site Laparoscopic: 1/23 (4%) wound infection Open: 1/23 (4%) late incisional hernia 3/23 (13%) wound infection Mortality: Robotic: 0 Laparoscopic: 0 Open: 0
Another publication by Horgan et al. (Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 2002; 12(1): 64-70) – possible patient overlap.

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
113 APPENDIX D
Laparoscopic Robotic Surgery – General: Suture Rectopexy Study Details Key Efficacy Findings Key Safety Findings Comments Munz 2004, UK (Level IV) 6 patients. Follow-up: 3 to 6 months. Intervention: Patients underwent robotic-assisted laparoscopic suture rectopexy. Gender (M/F): 1/5 Age: 65 years (range 37-87)
Operative time: 155 mins (range 127-183) Length of stay: Hospital stay: 6 days (range 4-8) Measures of success: 6/6 (100%)
Blood loss: no significant loss Complications: Major complications: 0 1/6 (17%) faecal soiling but improved over preoperative state. Constipation: 0 Mortality: 0
The preprocedural set-up is time consuming and complicated, and is approx. double the set-up time for conventional laparoscopy.
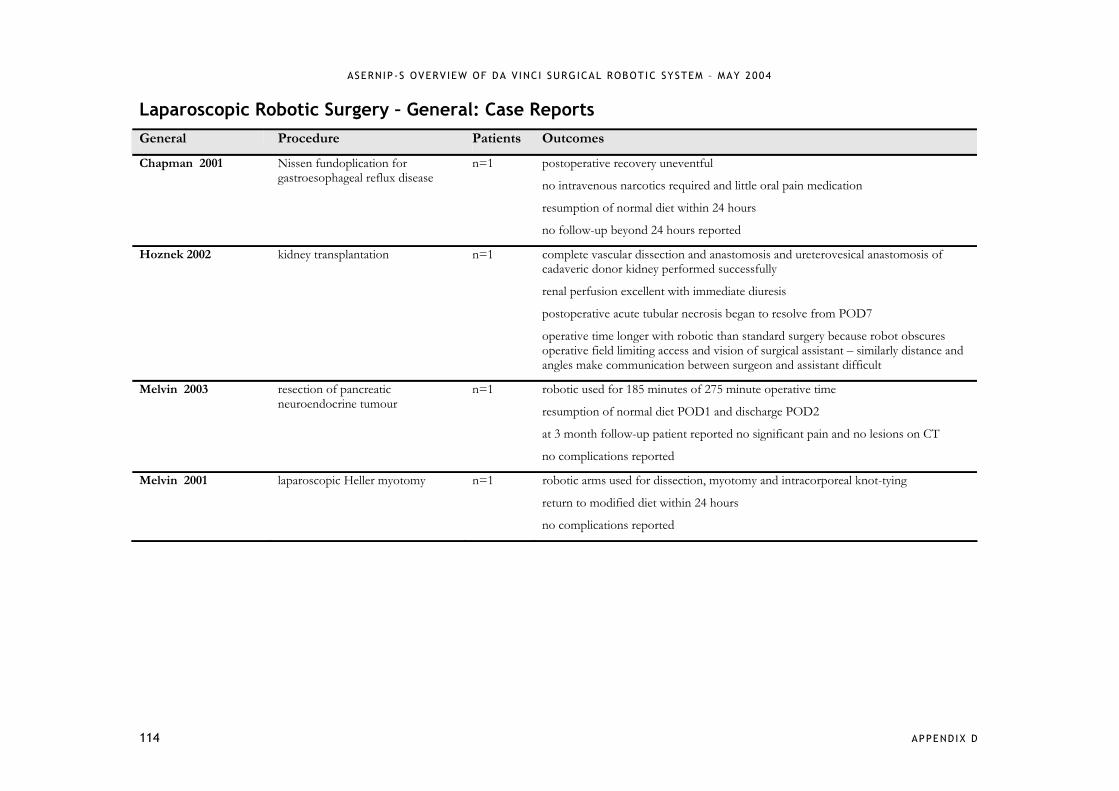
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
114 APPENDIX D
Laparoscopic Robotic Surgery – General: Case Reports General Procedure Patients Outcomes
Chapman 2001 Nissen fundoplication for gastroesophageal reflux disease
n=1 postoperative recovery uneventful
no intravenous narcotics required and little oral pain medication
resumption of normal diet within 24 hours
no follow-up beyond 24 hours reported
Hoznek 2002 kidney transplantation n=1 complete vascular dissection and anastomosis and ureterovesical anastomosis of cadaveric donor kidney performed successfully
renal perfusion excellent with immediate diuresis
postoperative acute tubular necrosis began to resolve from POD7
operative time longer with robotic than standard surgery because robot obscures operative field limiting access and vision of surgical assistant – similarly distance and angles make communication between surgeon and assistant difficult
Melvin 2003 resection of pancreatic neuroendocrine tumour
n=1 robotic used for 185 minutes of 275 minute operative time
resumption of normal diet POD1 and discharge POD2
at 3 month follow-up patient reported no significant pain and no lesions on CT
no complications reported
Melvin 2001 laparoscopic Heller myotomy n=1 robotic arms used for dissection, myotomy and intracorporeal knot-tying
return to modified diet within 24 hours
no complications reported

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
115 APPENDIX D
Laparoscopic Robotic Surgery – Gynaecological: Tubal Reanastomoses Study Details Key Efficacy Findings Key Safety Findings Comments Schwarzler 2002, AUSTRIA (Level IV) August 2001 to December 2001. 5 patients (8 tubes). Follow-up: 1 to 7 months. Intervention: Patients underwent microsurgical reanastomosis of fallopian tubes using robotic technology. Selection criteria: Patients who requested restoration of their fertility after tubal sterilisation. Age: 37 years (range 32-40)
Operative time: 189 [41] mins (anastomosis of both tubes) Length of stay: Hospital stay: 3.5 days Conversions: 0 Measures of success: 5/5 (100%) 3/5 (60%) bilateral anastomoses 2/5 (40%) unilateral anastomoses due to dense intraperitoneal adhesions
Complications: Perioperative complications: 0 Postoperative complications: 0 Robotic device-related complications: 0

ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
116 APPENDIX D
Laparoscopic Robotic Surgery – Paediatric: Multiple Indications Study Details Key Efficacy Findings Key Safety Findings Comments Luebbe 2003, USA (Level IV) July 2002 to April 2003. 20 patients. Follow-up: 1 week to 9 months. Procedures: Nissen fundoplication (n=10) Cholecystectomy (n=3) Splenectomy (n=2) Urachus resection (n=1) Unilateral iliac & retroperitoneal lymphadenectomy (n=1) Incisional biopsy retroperitoneal presacral mass (n=1) Incisional biopsy hepatic mass (n=1) Gortex patch repair of a Morgagni diaphragmatic hernia (n=1) Biopsy of a benign infracarinal mediastinal mass (n=1) Gender (M/F): 11/9 Age: 8.4 years (range 4 months-16 years)
Operative time: 208 mins (range 58-573) Length of stay: Hospital stay: 2.7 days (range 1-16) Conversions: 2/20 (10%) - both splenectomy patients
Blood loss: minimal Complications: Morgagni hernia repair: 1/20 (5%) right-sided pneumothorax Fundoplication: 2/20 (10%) postop dysphagia 1/20 (5%) superficial wound infection Long-term complications: 0 Mortality: 0
System malfunctions that occurred in this series were due to human error, these include: - instrument malfunction due to incorrect insertion - vision system problems due to incorrect calibration - external collisions of the robotic arms due to judgement errors in trocar placement or cart positioning.
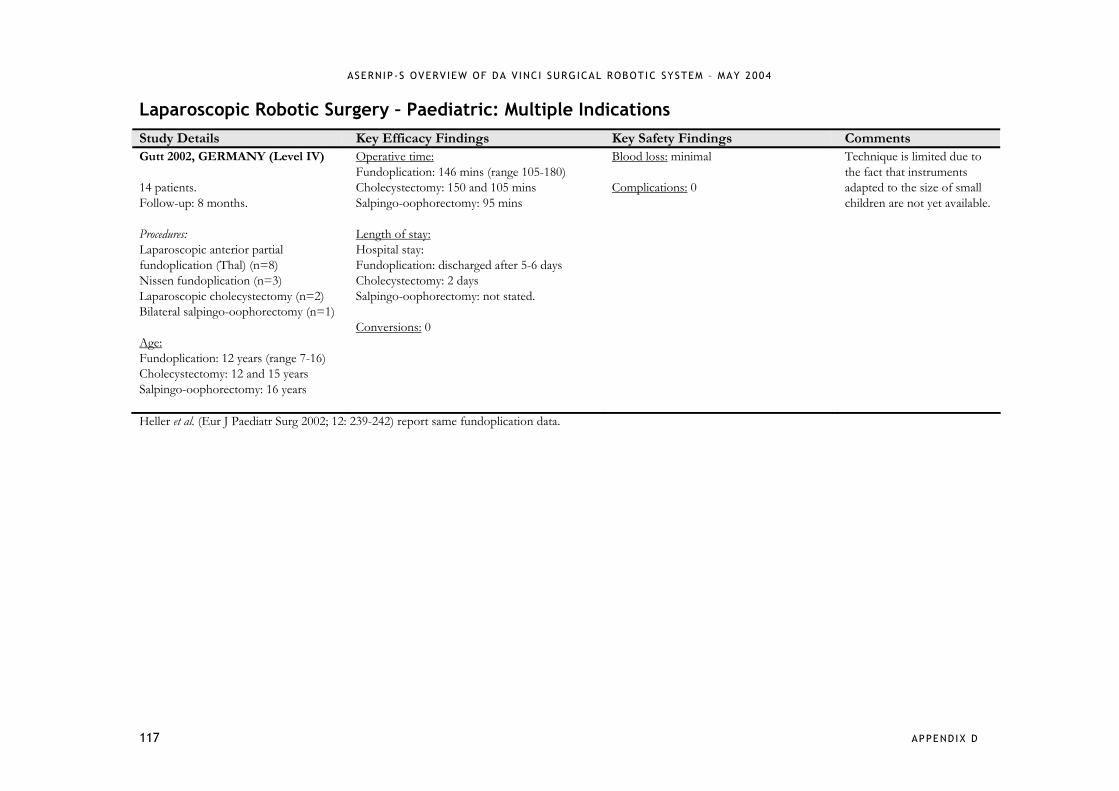
ASERNIP-S OVERV IEW OF DA V INCI SURGICAL ROBOTIC SYSTEM – MAY 2004
117 APPENDIX D
Laparoscopic Robotic Surgery – Paediatric: Multiple Indications Study Details Key Efficacy Findings Key Safety Findings Comments Gutt 2002, GERMANY (Level IV) 14 patients. Follow-up: 8 months. Procedures: Laparoscopic anterior partial fundoplication (Thal) (n=8) Nissen fundoplication (n=3) Laparoscopic cholecystectomy (n=2) Bilateral salpingo-oophorectomy (n=1) Age: Fundoplication: 12 years (range 7-16) Cholecystectomy: 12 and 15 years Salpingo-oophorectomy: 16 years
Operative time: Fundoplication: 146 mins (range 105-180) Cholecystectomy: 150 and 105 mins Salpingo-oophorectomy: 95 mins Length of stay: Hospital stay: Fundoplication: discharged after 5-6 days Cholecystectomy: 2 days Salpingo-oophorectomy: not stated. Conversions: 0
Blood loss: minimal Complications: 0
Technique is limited due to the fact that instruments adapted to the size of small children are not yet available.
Heller et al. (Eur J Paediatr Surg 2002; 12: 239-242) report same fundoplication data.


















