
Robot-Assisted Bladder Diverticulectomy
6
Techniques in Endourology Robot-Assisted Bladder Diverticulectomy Andre Luis de Castro Abreu, MD, Sameer Chopra, MD, Arjuna Dharmaraja, Hooman Djaladat, MD, Manju Aron, MD, Osamu Ukimura, MD, PhD, Mihir M. Desai, MD, Inderbir S. Gill, MD, MCh, and Monish Aron, MD Abstract Purpose: To describe our technique for robot-assisted bladder diverticulectomy (RABD). Patients and Methods: Ten patients underwent RABD using an extra- or transvesical approach. Three (30%) patients underwent concomitant procedures: Robot-assisted radical prostatectomy, robot-assisted simple pros- tatectomy, and transurethral resection of the prostate. Results: All RABDs were performed successfully. Median estimated blood loss, operative time, and diverti- culectomy time were 75 mL, 210 minutes, and 80 minutes, respectively. Median follow-up time was 18 months. Median International Prostate Symptom Score decreased by 57%, P = 0.001. Conclusions: RABD is feasible and safe. It can be performed via a trans- or extravesical approach, as a stand- alone, or concomitant procedure. Introduction T he majority of bladder diverticulae are acquired, occur in male adults, and are associated with bladder outlet obstruction. 1 This is in contrast to Hutch diverticulae that are congenital and occur in the pediatric population. 1,2 An asymptomatic bladder diverticulum does not need treatment. Bladder diverticulectomy (BD) may become necessary, how- ever, in patients who have incomplete emptying, lower urinary tract symptoms refractory to medical treatment, recurrent urinary tract infections, or stone(s) in the diverticulum. In these cases, diverticulectomy in conjunction with the treatment of the patient’s underlying condition provides long-term func- tional and symptomatic improvement. 3 BD has been performed using several approaches, such as open, laparoscopic, or robotic. 4–6 Although robotic surgery has recently gained popularity, limited reports exist with regard to robot-assisted bladder diverticulectomy (RABD) within the literature. 7 We report our surgical technique of extra- and transvesical RABD, and perioperative and short-term outcomes of our initial case series, which to our knowledge is one of the largest series of RABD for acquired bladder diverticulae to date. A supplementary video demonstrating this technique is avail- able at www.liebertpub.com/end Technique Patient evaluation We retrospectively reviewed the data of 10 male patients with acquired bladder diverticulae and refractory lower uri- nary tract symptoms (LUTS) that failed medical intervention and who underwent RABD between August 2011 and May 2013. The main indications for RABD were incomplete emptying, LUTS, and recurrent urinary tract infections. Pa- tients were evaluated using validated questionnaires, urine and blood tests, cystoscopy, imaging studies (ultrasonogra- phy, urethrocystography, and/or CT scan), and urodynamics. Patient preparation With the patient under general anesthesia and in the li- thotomy position, a cystoscopy is performed and a ureteral stent is placed ipsilateral to the diverticulum. A 16F Foley catheter is inserted. Pneumoperitoneum is established, and five ports are placed transperitoneally and positioned similar to the port configuration for robot-assisted radical prosta- tectomy (RARP) (Fig. 1). Extravesical approach The bladder is filled with saline and, under direct visuali- zation (zero-degree lens), the peritoneum over the divertic- ulum is incised (Fig. 2). Using blunt and sharp dissection, the diverticulum is circumferentially dissected to its neck. A cystotomy is made at the diverticulum neck, and the diver- ticulum is excised and placed in an endocatch bag (Endo Catch TM , Covidien, Norwalk, CT). The scope is advanced toward the cystotomy, and the bladder is surveyed to ensure no injuries to the ureteral orifices (UOs). The ureteral catheter is removed, and a watertight running closure of the cystotomy USC Institute of Urology, Center for Advanced Robotic Surgery, Keck School of Medicine, University of Southern California, Los Angeles, California. A video demonstrating this technique is available online at www.ftp.liebertpub.com/end JOURNAL OF ENDOUROLOGY Volume 28, Number 10, October 2014 ª Mary Ann Liebert, Inc. Pp. 1159–1164 DOI: 10.1089/end.2014.0149 1159
Transcript of Robot-Assisted Bladder Diverticulectomy

Techniques in Endourology
Robot-Assisted Bladder Diverticulectomy
Andre Luis de Castro Abreu, MD, Sameer Chopra, MD, Arjuna Dharmaraja,Hooman Djaladat, MD, Manju Aron, MD, Osamu Ukimura, MD, PhD,
Mihir M. Desai, MD, Inderbir S. Gill, MD, MCh, and Monish Aron, MD
Abstract
Purpose: To describe our technique for robot-assisted bladder diverticulectomy (RABD).Patients and Methods: Ten patients underwent RABD using an extra- or transvesical approach. Three (30%)patients underwent concomitant procedures: Robot-assisted radical prostatectomy, robot-assisted simple pros-tatectomy, and transurethral resection of the prostate.Results: All RABDs were performed successfully. Median estimated blood loss, operative time, and diverti-culectomy time were 75 mL, 210 minutes, and 80 minutes, respectively. Median follow-up time was 18 months.Median International Prostate Symptom Score decreased by 57%, P = 0.001.Conclusions: RABD is feasible and safe. It can be performed via a trans- or extravesical approach, as a stand-alone, or concomitant procedure.
Introduction
The majority of bladder diverticulae are acquired,occur in male adults, and are associated with bladder
outlet obstruction.1 This is in contrast to Hutch diverticulaethat are congenital and occur in the pediatric population.1,2 Anasymptomatic bladder diverticulum does not need treatment.Bladder diverticulectomy (BD) may become necessary, how-ever, in patients who have incomplete emptying, lower urinarytract symptoms refractory to medical treatment, recurrenturinary tract infections, or stone(s) in the diverticulum. In thesecases, diverticulectomy in conjunction with the treatment ofthe patient’s underlying condition provides long-term func-tional and symptomatic improvement.3
BD has been performed using several approaches, suchas open, laparoscopic, or robotic.4–6 Although robotic surgeryhas recently gained popularity, limited reports exist with regardto robot-assisted bladder diverticulectomy (RABD) within theliterature.7 We report our surgical technique of extra- andtransvesical RABD, and perioperative and short-term outcomesof our initial case series, which to our knowledge is one of thelargest series of RABD for acquired bladder diverticulae to date.A supplementary video demonstrating this technique is avail-able at www.liebertpub.com/end
Technique
Patient evaluation
We retrospectively reviewed the data of 10 male patientswith acquired bladder diverticulae and refractory lower uri-
nary tract symptoms (LUTS) that failed medical interventionand who underwent RABD between August 2011 and May2013. The main indications for RABD were incompleteemptying, LUTS, and recurrent urinary tract infections. Pa-tients were evaluated using validated questionnaires, urineand blood tests, cystoscopy, imaging studies (ultrasonogra-phy, urethrocystography, and/or CT scan), and urodynamics.
Patient preparation
With the patient under general anesthesia and in the li-thotomy position, a cystoscopy is performed and a ureteralstent is placed ipsilateral to the diverticulum. A 16F Foleycatheter is inserted. Pneumoperitoneum is established, andfive ports are placed transperitoneally and positioned similarto the port configuration for robot-assisted radical prosta-tectomy (RARP) (Fig. 1).
Extravesical approach
The bladder is filled with saline and, under direct visuali-zation (zero-degree lens), the peritoneum over the divertic-ulum is incised (Fig. 2). Using blunt and sharp dissection, thediverticulum is circumferentially dissected to its neck. Acystotomy is made at the diverticulum neck, and the diver-ticulum is excised and placed in an endocatch bag (EndoCatchTM, Covidien, Norwalk, CT). The scope is advancedtoward the cystotomy, and the bladder is surveyed to ensureno injuries to the ureteral orifices (UOs). The ureteral catheteris removed, and a watertight running closure of the cystotomy
USC Institute of Urology, Center for Advanced Robotic Surgery, Keck School of Medicine, University of Southern California, LosAngeles, California.
A video demonstrating this technique is available online at www.ftp.liebertpub.com/end
JOURNAL OF ENDOUROLOGYVolume 28, Number 10, October 2014ª Mary Ann Liebert, Inc.Pp. 1159–1164DOI: 10.1089/end.2014.0149
1159
is performed in two layers. A Jackson-Pratt drain is placed,the ports are removed, and the specimen is retrieved.
Transvesical approach
This is our preferred approach for diverticulae that arelarge or close to the UOs. With the bladder filled with saline, amidline cystotomy is performed. The edges of the cystotomyare retracted laterally using stay sutures (Fig. 3). The UOs areidentified and the neck of the diverticulum is scored. The tipof the Foley catheter is advanced into the diverticulum, theballoon is inflated, and the diverticulum is filled with saline.From outside the bladder, the diverticulum is dissected to itsneck. The bladder mucosa at the diverticulum neck is incised,and the diverticulectomy and bladder closure are performedas described previously.
Concomitant procedure technique
If a concomitant procedure is planned, a sequential ap-proach is used. For simultaneous RARP, the extravesical
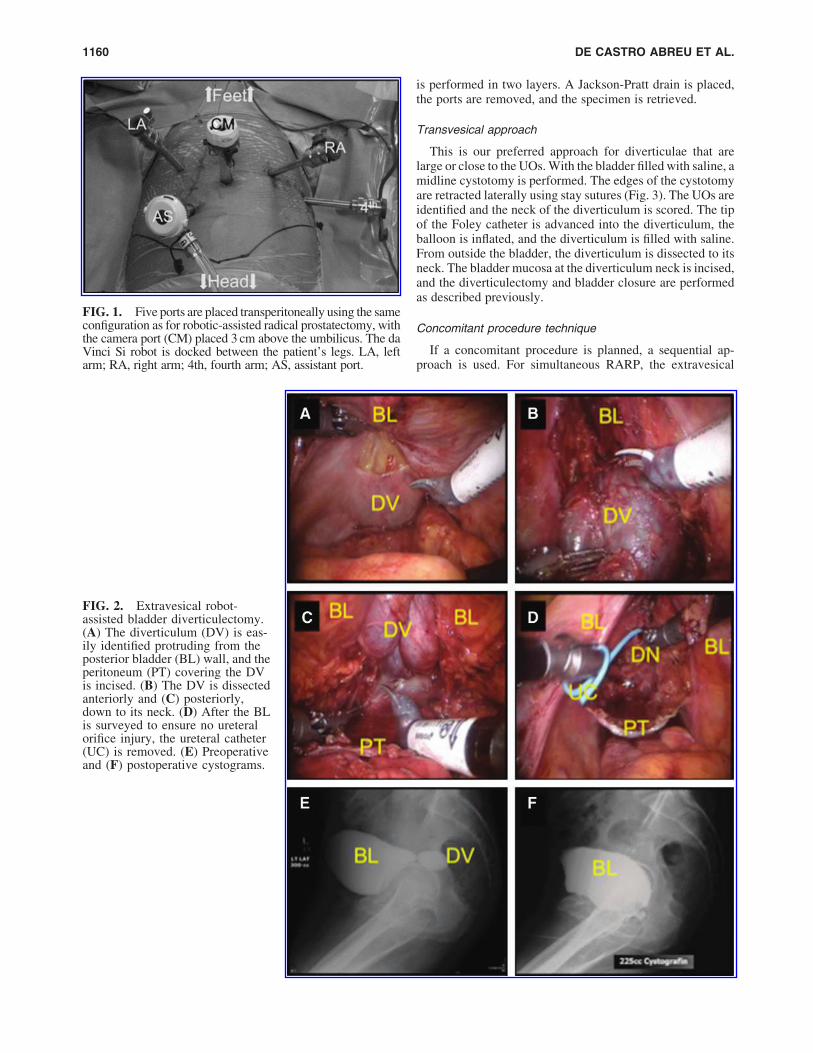
FIG. 2. Extravesical robot-assisted bladder diverticulectomy.(A) The diverticulum (DV) is eas-ily identified protruding from theposterior bladder (BL) wall, and theperitoneum (PT) covering the DVis incised. (B) The DV is dissectedanteriorly and (C) posteriorly,down to its neck. (D) After the BLis surveyed to ensure no ureteralorifice injury, the ureteral catheter(UC) is removed. (E) Preoperativeand (F) postoperative cystograms.
FIG. 1. Five ports are placed transperitoneally using the sameconfiguration as for robotic-assisted radical prostatectomy, withthe camera port (CM) placed 3 cm above the umbilicus. The daVinci Si robot is docked between the patient’s legs. LA, leftarm; RA, right arm; 4th, fourth arm; AS, assistant port.
1160 DE CASTRO ABREU ET AL.

RABD is performed first, followed by RARP. For simulta-neous robot-assisted simple prostatectomy (RASP), a trans-vesical approach is used to perform RABD followed bytransvesical adenomectomy. As such, the bladder is suturedat the end of the RASP. For a concomitant transurethral re-section of the prostate (TURP), the TURP is performed first,followed by RABD.
Postoperative and follow-up
The patient is discharged to home with an indwelling 18FFoley catheter that is removed after cystography on postop-erative day (POD) 7 to 8 (Fig. 4).
Complications were analyzed up to 30 days postopera-tively and were graded according to the Clavien-Dindoclassification. Follow-up included administering validatedquestionnaires to assess symptomatic improvement. The two-tailed Student t test was performed to assess statistical sig-nificance (P < 0.05).
Equipment
� da Vinci Si Robot (Intuitive, Sunnyvale, CA)� 2-0 Vicryl� (Ethicon, Cincinnati, OH) sutures on a CT-
1 needle� 2-0 V-Loc� (Covidien, Norwalk, CT) sutures� PrograspTM Forceps (Intuitive, Sunnyvale, CA)� Hot ShearsTM (Monopolar Curved Scissors) (Intuitive,
Sunnyvale, CA)
Role in Urologic Practice
Results
All procedures were successfully performed robotically.Three (30%) patients underwent a concomitant procedure:RARP, RASP, and TURP. The patient who underwent RABDand concomitant RARP had, on postoperative cystography, asmall leak from the vesicourethral anastomosis but not fromthe cystotomy. In this case, the Foley catheter was left in place
FIG. 3. Transvesical robot-assisted bladder (BL) diverticu-lectomy and concomitant roboticsimple prostatectomy. (A) A verti-cal cystotomy is performed, and theedges are sutured to the abdominalwall using intracorporeal stay su-tures. (B) With the ureteral catheter(UC) already in place, the Foleycatheter (FC) is advanced and in-serted into the diverticulum, andthe diverticulum neck (DN) isscored. (C) The diverticulum mu-cosa is incised, and a diverticu-lectomy is performed. (D) The BLis sutured in two layers using 2-0V-Loc� (Covidien, Norwalk, CT)sutures. (E) Preoperative and (F)postoperative cystograms.AD = adenoma of the prostate.
ROBOT-ASSISTED BLADDER DIVERTICULECTOMY 1161
for 16 days with resolution of the leak. Postoperative com-plications occurred in three (30%) patients, two (20%) ofwhich were low-grade. The patient with a high-grade com-plication underwent RABD and concomitant RASP and pre-sented with small bowel obstruction from intra-abdominaladhesions on POD 30 that necessitated reoperation. On his-tologic evaluation, all diverticulae were found to be benign(Fig. 5). Median (range) follow-up was 18 months (7–27); allpatients were doing well and the median International ProstateSymptom Score (IPSS) improved 57%, P = 0.001 (Table 1).
Discussion
The literature is scarce regarding acquired BD. Approxi-mately 45 cases have been reported to date, of which 30 arefor acquired diverticulae and 15 for congenital diverticulae.2
Open BD has been performed with satisfactory long-termoutcomes.3 More recently, laparoscopic BD has been pro-
posed as an alternative, because of the benefits of minimallyinvasive surgery (MIS).4,5 Porpiglia and associates4,5 re-ported that laparoscopic BD provided decreased blood lossand postoperative analgesic requirement, and shorter hospi-talization compared with open surgery. We report perio-perative outcomes similar to other MIS-BDs reported.2,7
Median estimated blood loss was minimal, median total op-erative time was 210 minutes, and median diverticulectomytime was 80 minutes. Hospital stay and Foley catheter du-ration were as expected, and a high-grade complication oc-curred in one patient with concomitant RASP. On follow-up,median IPSS decreased by 57%.
Altunrende and colleagues8 report a case series of six adultpatients who underwent RABD. We report similar patientindications, perioperative, and postoperative outcomes forRABD. In the present study, we used pre- and postoperativevalidated questionnaires that demonstrated the efficacy of oursurgical treatment.
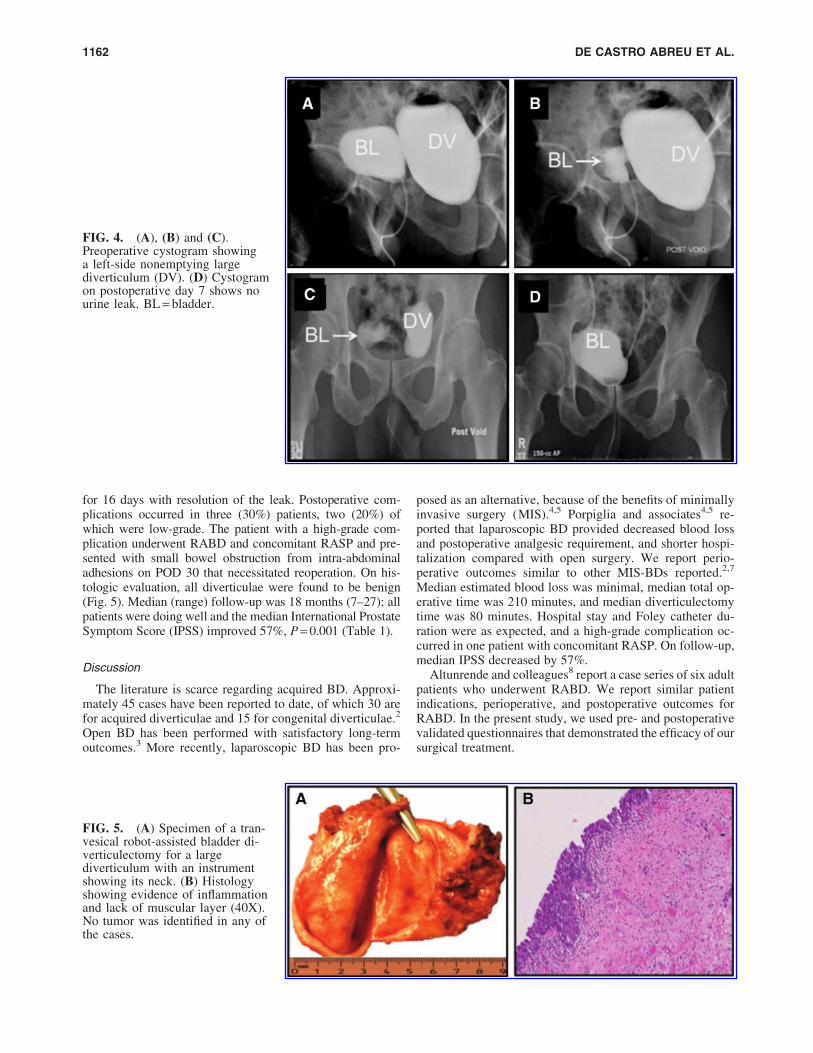
FIG. 4. (A), (B) and (C).Preoperative cystogram showinga left-side nonemptying largediverticulum (DV). (D) Cystogramon postoperative day 7 shows nourine leak. BL = bladder.
FIG. 5. (A) Specimen of a tran-vesical robot-assisted bladder di-verticulectomy for a largediverticulum with an instrumentshowing its neck. (B) Histologyshowing evidence of inflammationand lack of muscular layer (40X).No tumor was identified in any ofthe cases.
1162 DE CASTRO ABREU ET AL.

There are several approaches to perform BD: Extravesical,transvesical, extraperioneal or transperitoneal. While themajority of reported cases use an extravesical approach, weperformed the transvesical approach in 60% of our patients.7
While this choice was based on the surgeon’s discretion, somefactors favored the transvesical approach: Multiple diverticu-lae, large diverticulum close to the UOs, and certain concom-itant procedures (RASP). We performed RABD extravesicallyif the diverticulum was small and in a favorable location.From our experience, either approach is feasible, safe, and mayprovide similar outcomes. We performed RABD transper-itoneally because we are familiar with this approach (similar toRARP), and it provides a larger intra-abdominal workspace,allowing better visualization of the anatomy.
Several maneuvers to identify the UOs and the diverticu-lum are reported.5,8,9 We were able to identify the divertic-ulum protruding from the bladder and directly approached iteither trans- or extravesically. In cases performed transve-sically, the diverticulum was usually large and close to theUO. We advanced the Foley catheter under direct visuali-zation into the diverticulum and filled it to facilitate dis-section. We routinely placed a ureteral catheter beforeRABD if the BD was close to the ureter. The distal part ofthe ipsilateral ureter was first dissected down to the bladderand looped up. These preventive maneuvers do not addsignificant time to the procedure but can decrease chancesof ureteral injury. In our series, we did not experience injuryto the ureter or UOs.
It is important to manage the underlying disease thatcauses the diverticulum.1,3 RABD can be performed as asingle-stage or stepwise procedure (two separate opera-tions).4,5,10 We report a total MIS single-stage approach inthree patients. One patient underwent RABD with concom-itant RARP. Because the diverticulum was located in theposterior midline and close to the dome, we performedRABD before dropping the bladder from the anterior ab-dominal wall for RARP. One patient had a large prostate(80 g) and a large diverticulum (8.3 cm). We performedRABD tranvesically with subsequent transvesical RASP.This patient was reoperated on POD 30 for adhesive smallbowel obstruction. The final patient who underwent a con-comitant procedure had a 69 g prostate gland with four di-verticulae. To avoid tension on the suture line of the bladder,we performed TURP before the RABD.4,5 This patient had noperioperative complications, and no leak was noted onpostoperative cystography.
Conclusion
RABD is feasible and safe. It can be performed trans- orextravesically and as a stand-alone or concomitant procedure.
Disclosure Statement
No competing financial interests exist.
References
1. Gerridzen RG, Futter NG. Ten-year review of vesical di-verticula. Urology 1982;20:33–35.
2. Eyraud R, Laydner H, Autorino R, et al. Robot-assistedlaparoscopic bladder diverticulectomy. Curr Urol Rep2013;14:46–51.
Table 1. Demographics and Perioperative
Outcomes of Robotic Bladder Diverticulectomy
Demographics Median (range) or N (%)
N 10Age (years) 65 (43–73)Sex – Male 10 (100)BMI (kg/m2) 26 (21–32)ASA 2 (2–3)History
Urinary retention 7 (70)UTI 4 (40)Previous TURP 4 (40)Previous RP 1 (10)
No. diverticula per patient 1 (1–4)1/2/4 7 (70)/ 2 (20)/ 1 (10)
Diverticulum size (cm)a 7.2 (4.6–9.8)Diverticulum laterality – Righta 5 (50)Diverticulum locationa
Posterolateral 6 (60)Lateral 3 (30)Posterior 1 (10)
Prostate size (g)b 56 (30–145)Postvoid residuum (mL) 269 (110–815)IPSSc 22 (3–31)Quality of life – IPSSd 4 (2–6)
Perioperative Median (range) or N (%)
Concomitant procedureRARP/RASP/TURP 1 (10)/ 1 (10)/ 1 (10)
Conversion to open 0 (0)Approach
Transvesical 6 (60)Extravesical 4 (40)
Total operative time (min) 210 (80–360)Diverticulectomy time (min) 80 (55–116)Estimated blood loss (mL) 75 (20–150)Intraoperative complication 0 (0)Transfusion 0 (0)Length of stay (days) 2 (1–3)Foley stay (days) 8 (6–16)Urine leake 1 (10)No. complicationf 3 (30)Clavien grade – detail
I 1 (10) – drug-induced rashII 1 (10) – UTIIIIbf 1 (10) – Small bowel
obstructionf
Histology – Benign/cystitis 10 (100)
Follow-up Median (range)
Follow up time (months) 18 (7–27)IPSSc 8 (0–16)Quality of life – IPSSd 2 (0–3)
aData pertaining to the largest diverticulum.bOne patient with previous radical prostatectomy.cDifference between preoperative and postoperative IPSS was
significant, P = 0.001.dDifference between preoperative and postoperative quality of
life was significant, P = 0.002.eConcomitant RARP, the urine leaked from the bladder-urethral
anastomosis.fConcomitant RASP. This patient presented with small bowel
obstruction from adhesions 30 days after the operation.BMI = body mass index; ASA = American Society of Anesthesiol-
ogists; UTI = urinary tract infection; TURP = transurethral resectionof the prostate; RP = radical prostatectomy; IPSS = InternationalProstate Symptom Score; RARP - robot-assisted radical prostatec-tomy; RASP = robot-assisted simple prostatectomy.
ROBOT-ASSISTED BLADDER DIVERTICULECTOMY 1163

3. Fox M, Power RF, Bruce AW. Diverticulum of thebladder—presentation and evaluation of treatment of 115cases. Br J Urol 1962;34:286–298.
4. Porpiglia F, Tarabuzzi R, Cossu M, et al. Is laparoscopicbladder diverticulectomy after transurethral resection of theprostate safe and effective? Comparison with open surgery.J Endourol 2004;18:73–76.
5. Porpiglia F, Tarabuzzi R, Cossu M, et al. Sequentialtransurethral resection of the prostate and laparoscopicbladder diverticulectomy: Comparison with open surgery.Urology 2002;60:1045–1049.
6. Myer EG, Wagner JR. Robotic assisted laparoscopicbladder diverticulectomy. J Urol 2007;178:2406–2410.
7. Moreno Sierra J, Galante-Romo I, Ortiz-Oshiro E,Castillon-Vela IT, Fernandez-Perez C, Silmi-Moyano A.Bladder diverticulum robotic surgery: Systematic review ofcase reports. Urol Int 2010;85:381–385.
8. Altunrende F, Autorino R, Patel NS, et al. Robotic bladderdiverticulectomy: Technique and surgical outcomes. Int JUrol 2011. Epub ahead of print.
9. Thiel DD, Young PR, Wehle MJ, et al. Robotic-assistedbladder diverticulectomy: Tips and tricks. Urology 2011;77:1238–1242.
10. Ploumidis A, Skolarikos A, Sopilidis O, et al. Sequentialrobotic-assisted bladder diverticulectomy and radical
prostatectomy. Technique and review of the literature. Int JSurg Case Rep 2013;4:81–84.
Address correspondence to:Monish Aron, MD
1441 Eastlake Avenue, Ste. 7416Los Angeles, CA 90089
E-mail: [email protected]
Abbreviations UsedBD¼ bladder diverticulectomyCT¼ computed tomography
IPSS¼ International Prostate Symptom ScoreMIS¼minimally invasive surgeryPOD¼ postoperative day
RARP¼ robot-assisted radical prostatectomyRABD¼ robot-assisted bladder diverticulectomyRASP¼ robot-assisted simple prostatectomyTURP¼ transurethral resection of the prostate
UOs¼ ureteral orifices
DOI: 10.1089/end.2014.0483
Editorial Comment for de Castro Abreu et al.
Jay T. Bishoff, MD
In this edition, Luis de Castro Abreu and colleaguespresent a small, retrospective series (N = 10) of robot-assisted
diverticulectomy, which is one of the largest found in the lit-erature. The authors explain two different approaches tothe acquired bladder diverticulum, extravesical and transvesical,with outcomes similar to those in the other reported series. Ifound the report to be interesting and their approaches suffi-ciently explained and demonstrated with the included images.
While the laparoscopic approach remains an excellent ap-proach in treating patients with bladder diverticulum, I havefound the dissection and extensive suturing needed for closureof the large mouth diverticulum and in the transvesical ap-proach to be expeditious with the assistance of robotics. Theirapplication of an expensive reconstructive surgical instrumentfor what is often a true reconstructive case is refreshing.
Placement of a ureteral stent facilitates dissection when thediverticulum is located laterally near the ureter. Occasionallycystoscopy, especially flexible cystoscopy, can help to locatethe diverticulum. The large mouth diverticulum may not beseen easily in the extravesical approach. The tip of the flex-ible scope can be placed in the diverticulum. The combina-
tion of distension of the bladder and illumination of thediverticulum with the flexible scope facilitates localizationand excision. The surgical trick of placing the bladder cath-eter inside of the diverticulum and distending the balloonto fill the diverticular cavity is described in the article andis frequently very helpful, especially in the transvesical ap-proach. Concomitant procedures are often needed in themanagement of bladder diverticulum, and the authors alsooffer helpful advice on the order of other procedures at thesame time as diverticulectomy.
While their follow-up in this series is short, I believe thatthis article offers the minimally invasive surgeon some helpfulideas about how to approach this disease process robotically.
Address correspondence to:Jay T. Bishoff, MD
Intermountain Urological Institute5169 S. Cottonwood Street, Suite 420
Murray, UT 84107
E-mail: [email protected]
Intermountain Urological Institute, Murray, Utah.
1164 DE CASTRO ABREU ET AL.


















