Roadmap to Team Based Care KEY ELEMENTS IN OPERATIONALIZING TEAM BASED CARE IN HEALTH CENTERS...
28
Roadmap to Team Based Care KEY ELEMENTS IN OPERATIONALIZING TEAM BASED CARE IN HEALTH CENTERS OCTOBER 7, 2015 Debra McGrath HIT Director and Suzanne Cohen Director of Member Services
-
Upload
bethanie-washington -
Category
Documents
-
view
214 -
download
1
Transcript of Roadmap to Team Based Care KEY ELEMENTS IN OPERATIONALIZING TEAM BASED CARE IN HEALTH CENTERS...

Roadmap to Team Based Care
KEY ELEMENTS IN OPERATIONALIZING TEAM BASED CARE IN HEALTH CENTERS
OCTOBER 7, 2015 Debra McGrathHIT Director
and
Suzanne CohenDirector of Member Services

Agenda Overview and Background Best Practices for Team-Based Care Obstacles and Solutions First Steps Toward Change

ObjectivesUpon completion of this session, the participants will be able to:
◦ Evaluate the capability of their organization to adopt team based care◦ Identify potential barriers to team based care◦ Articulate different models and key elements of team based care◦ Develop an action plan to implement team based care


Components of a High Performing Medical Practice
Prompt Access to Care Coordination of Care
Patient – Team Partnership Population Management Continuity of Care
Data Driven Improvement Empanelment Team-Based Care
Engaged Leadership/Executive Sponsorship
Adapted from Safety Net Medical Home Initiative, Ed Wagner

State of Primary Care in 2015
Panel Management
Chronic Disease Management
Health Maintenance
Medication Reconciliation
Meaningful Use
PCMH
Patient Education
results follow up
Transitions in Care
patient engagement
insurance Evidence-based practice
Coding/ICD-10
productivity

Guiding Principles of Team Based Care
1. Facilitate all members of the team functioning at the highest level of their capability.
2. Eliminate those things that waste everyone’s time, so that you and the entire team can have more time to do the important things that really determine patient outcomes

Why Team Based Care - Time Significant impact on quality and outcomes Providers need time to
◦ Listen◦ Examine◦ Think◦ Explain◦ Operate◦ Interpret◦ Comfort
Lack of time contributes to job dissatisfaction and burn out

Why Team Based Care - Time Stealers Documenting Care Finding diagnostic study results and reports from specialists Waiting for delays in patient flow Justifying care/medical necessity Authorizations Prescription and referral renewals

How Team Based Care: Core Principles
Provider-MA Dyad Teamlets supported by a broader team Providers as the CEO of the team Risk stratification Care Coordination/Management Empanelment

Provider-MA Dyad is the
Teaming of one provider (or one FTE provider) with a medical assistant Responsible for the care provided to a panel of patients at the point of care as well as follow up care outside the visit including:◦ Following up on lab and diagnostic testing results◦ Following up on consults with referred to providers◦ Medication management◦ Managing health maintenance and health promotion activities◦ Following up with internal referrals to behavioral health, nutrition, social services◦ Co-managing chronic diseases with specialists and other members of the care team

Why are stable MA/provider dyads so important?
The heart of the team Huge gain in efficiency Patients recognize the MA as a stable part of the team MA’s take accountability for “their” patients More familiarity and trust leads to the MA doing more and the providers spending their time doing what only a provider can do.

Ideal Team Model
Shared Support Team(RN, LSW, pharmacist, attorney, health coach, care manager,
panel manager)
Clinician/MA Dyad
Patient Panel
Empowered Front Desk in Expanded Role
Phone Operator or Call Center
Clinician/MA Dyad
Clinician/MA Dyad
Patient Panel Patient Panel
Adapted from Willard, R and Bodenheimer, T. (2012) The Building Blocks of High-Performing Primary Care: Lessons from the Field. Prepared for California Healthcare Foundation
Providers are the CEO of the Team*
Provides clear direction for the team Leads team to proactively solve problems Builds the team Coaches team Manages stakeholder relationships
◦ *Even thought they don’t directly supervise most team members!

Importance of Risk Stratification In most health centers 80% of the care team’s effort is being spent on 20% of the patients
Critical Success Factors◦ Identify the patients requiring intensive care management and coordination◦ Assign these patients to care management/care coordination
Organizations are using the following criteria for risk stratification◦ Polypharmacy◦ 3 or more chronic diseases◦ Poor control of a critical chronic disease such as diabetes or hypertension◦ Chronic no shows or resistance to care or medication adherence◦ Behavioral health diagnoses

Importance of care management Has to be staffed - once you risk stratify, have to have someone to manage the high risk patients
Care transitions Increasingly, there is some reimbursement available for care management◦ New Medicare codes◦ Likelihood of enhanced PMPM in Medicaid
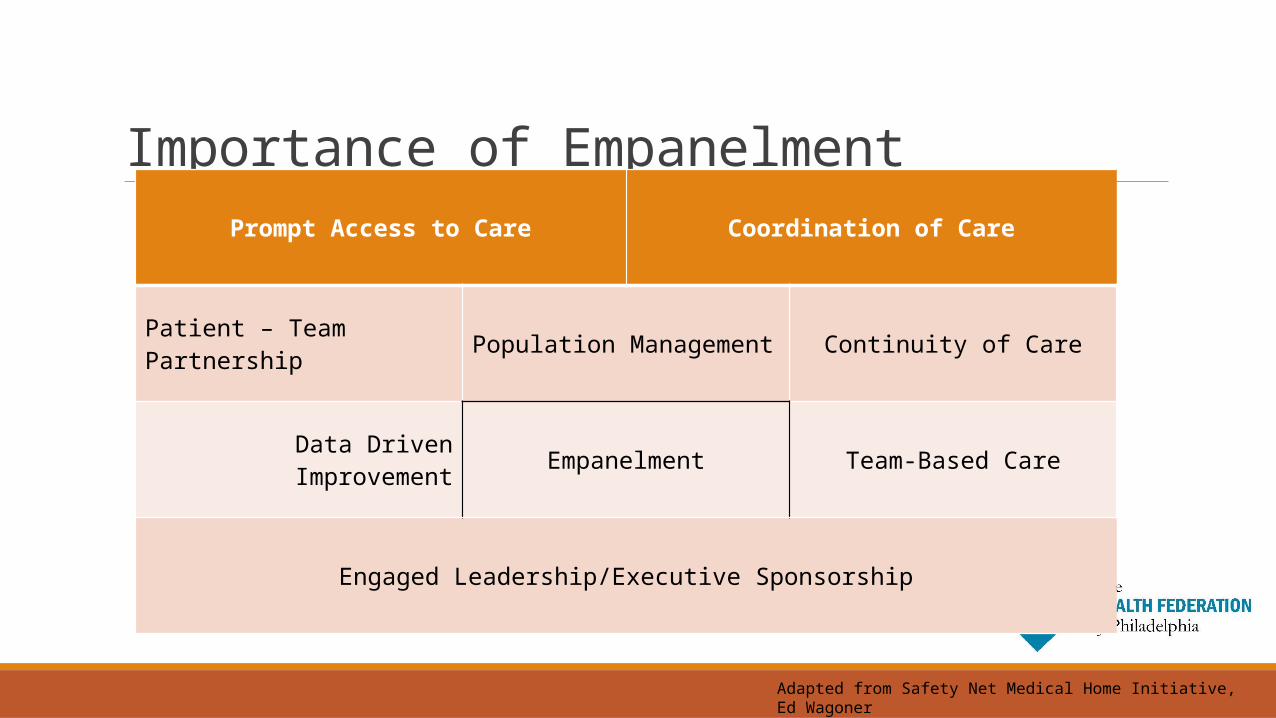
Importance of EmpanelmentPrompt Access to Care Coordination of Care
Patient – Team Partnership Population Management Continuity of Care
Data Driven Improvement Empanelment Team-Based Care
Engaged Leadership/Executive Sponsorship
Adapted from Safety Net Medical Home Initiative, Ed Wagoner

Empanelment Deliberate attempt to identify the group of patients for whom a care team is responsible.
Represents a shift from the care of patients in the context of an encounter to the proactive, planned care of a population of patients
Goes beyond disease-specific interventions to address preventive, chronic and acute patient needs
Allows the practice to manage supply and demand as an information/data driven process

Barriers to Team Based CareNo Time for:
HuddlesTeam Meetings
part – time providers
staff are not capable
Incongruent with Organizational Chart
Providers work 10 hours, MA’s work 8 hours
not enough staff
providers don’t trust staff
Difficult to incorporate Care Managers, Front Desk, BHC’s ….
no funding for care coordinator positions
suzanne cohen
Add - no money for care coordinator positions

Overcoming barriers and getting started
Scheduling ideas Team role analysis tool Cambridge Model Enabling Technology Tools Training Be proactive about new funding/reimbursement possibilities

Scheduling ideas Evaluate provider staffing in terms of FTE Consider assigning 2 or more providers to a team to create one FTE Consider moving to a consistent staffing model where MA’s and providers are working similar hours
Assign responsibilities to teams when providers are not present actively seeing patients
Try to keep providers/MA’s at one location

Getting Started: Team Analysis Tool
Developed by Qualis
Designed to identify which team member is responsible for each role and function and help with staffing ratios
Compare what you’re doing now to where you would like to be – create a roadmap
Team Role Analysis

Cambridge Model Adopted by and designed for safety net providers What is a Team
◦ Session Team◦ Patient’s Planned Care Team◦ Coverage Team◦ Complex Care Team
When/how often should teams meet◦ Daily for a huddle focused on individual patients◦ Weekly, biweekly or monthly focused on the panel and QI measures

Cambridge Model• Track high risk patients• Collaborate with the Planned Care
Team as needed
• Patient's "Go To" Team and each patient is assigned to one.
• Consists of stable Provider-MA dyads, Clerk Assistant, Back-desk
MA, BHC, RN
• Provides a structure to improve access while maintaining
continuity
• Ideally = Planned Care Team• Team of record for the encounter
and participates in the huddle• Communicates with the Planned
Care Team if indicated
Complex Care
Management Team
Planned Care Team
Coverage Team
Session Team

Cambridge ModelSession Team Responsible for the patient’s care on the day of the encounter
Participates in the daily huddle Ideally is the same as the Patient’s Care Team
Patient’s Care Team “Go To” Team Accountable to and for a panel of patients
Regularly evaluated for:◦ Total number of patients in the panel◦ Average number of visits/patient◦ Total number seen >3 times annually◦ Total number of patients with more than
3 chronic illnesses

Cambridge ModelCoverage Team Supports a higher level of access Consists of 2-3 Planned Care Teams
Responsible to communicate among Planned Care Teams
Complex Care Management Team At least one care manager (team leader, ideally an RN), a social worker and/or case manager, community health worker(s), pharmacist, nutrition coach or dietician.
Supports 2 -3 Planned Care Teams Responsible to and for the high risk/high utilizer patients
Collaborates with the Planned Care Teams

Health Information Technology
Optimize HIT to support the team – e.g. enhanced MA intake, care management forms
Consider i2i Tracks or other Population Health Management tools Consider purchasing enabling tools e.g. Phreesia, bi-directional interfaces, bi-directional HIE tools, automated patient contact tools, etc.
Ensure HIT is functioning as well as possible from a performance perspective e.g. hour-glassing, wireless access etc.

Training Evaluate training needs for providers and staff based on their role in the team.
Motivational Interviewing - everyone Clinical Skills Training – MA’s Leadership Training – providers Standardized use of technology tools - everyone