Road to Mental Readiness Metro Fire Chiefs Conference May 2, 2015.
22
Road to Mental Readiness Metro Fire Chiefs Conference May 2, 2015
-
Upload
myrtle-cain -
Category
Documents
-
view
217 -
download
3
Transcript of Road to Mental Readiness Metro Fire Chiefs Conference May 2, 2015.

Road to Mental Readiness
Metro Fire Chiefs Conference May 2, 2015

The Need• 7% of adult Canadians have been diagnosed
with a mental illness• 6% are experiencing symptoms but have not
been diagnosed(Lim, K.L., Jacobs, P., Ohinmaa, A. et al., 2008)
• in any given year, 1 in 5 Canadians experiences a mental health or addiction problem
(Centre for Addiction and Mental Health)
The Need
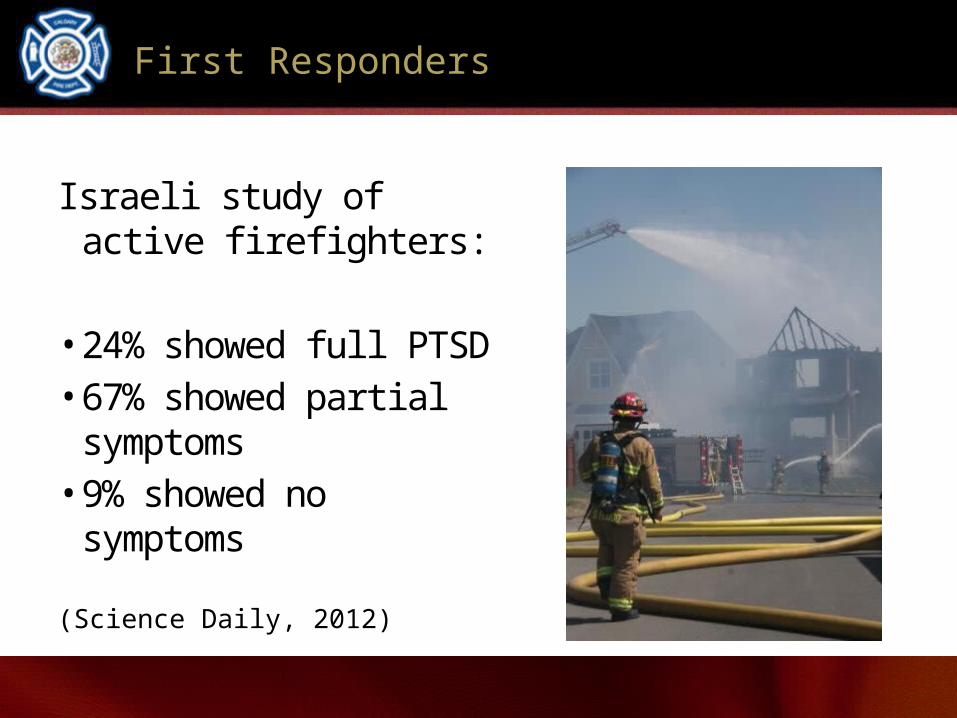
First Responders
Israeli study of active firefighters:
• 24% showed full PTSD• 67% showed partial symptoms• 9% showed no symptoms
(Science Daily, 2012)

First Responders
American Study:Protective services workers exposed to multiple traumatic events are at increased risk of developing new mental disorders, especially in the early stages of their careers.
(Kaufman, Rutkow, Spira & Mojtabi, 2013)

First Responder Suicide
Canada:• April – Dec. 2014 – 27 first responders• Jan. – March 2015 – 6 first responders
(Tema Conter Memorial Trust)
United States:• 2014 – 103 firefighters• Jan. – March 2015 – 23 firefighters
(Firefighter Behavioral Alliance, 2015)
Canadian survey:
• 54% of employees said that disclosing their mental illness to management would jeopardize their chances for promotion
• 26% of employees felt that their supervisor effectively manages mental health issues
(Conference Board of Canada, 2011)
Perceptions of Mental Illness

Ontario survey:
• 39% of workers said that they would not tell their managers if they were experiencing a mental health problem
• 64% of workers would be concerned about how work would be affected if a colleague had a mental illness
(Dewa, 2014)
Perceptions of Mental Illness

Financial Cost
• Estimated cost of lost labour-market participation due to poor mental health in the workplace: $20.7 billion.
(Conference Board of Canada, 2012)
• Mental illness is second-leading cause of short-term disability ($18,000 per leave), double the average cost of all other causes.
(Dewa, Chau & Dermer, 2010)

• annually 3% of workers are on short-term disability related to mental illness
(Dewa, 2014)
• 2020 - expected that mental illness will be the second-leading cause of all disability globally (after heart disease)
(World Health Organization, 2001)
Financial Cost

• Post-incident (Peer Support, CISM)
• Diakonos Workshops for Couples (through Local 255)
• Missing: tool to build resiliency skills across career path
Calgary Fire Department Resources
• Developed by Canadian Forces to increase resiliency and mental health of soldiers
• Adapted by Mental Health Commission of Canada and New Brunswick RCMP for police services
• CFD first to adapt for fire service
Road to Mental Readiness

Objectives - Frontline
• Improve short-term performance and
long-term mental health outcomes
• Reduce stigma and other barriers and encourage early access to help

Objectives - Leadership
• Provide tools/resources to manage and support employees who may be experiencing a mental health problem or illness
• Assist supervisors in maintaining their own mental health and promote positive mental health in their employees
Main Components
• Anti-stigma
• Skills development:• goal setting • mental rehearsal (visualization) • positive self-talk • tactical (diaphragmatic) breathing
• Mental Health Continuum

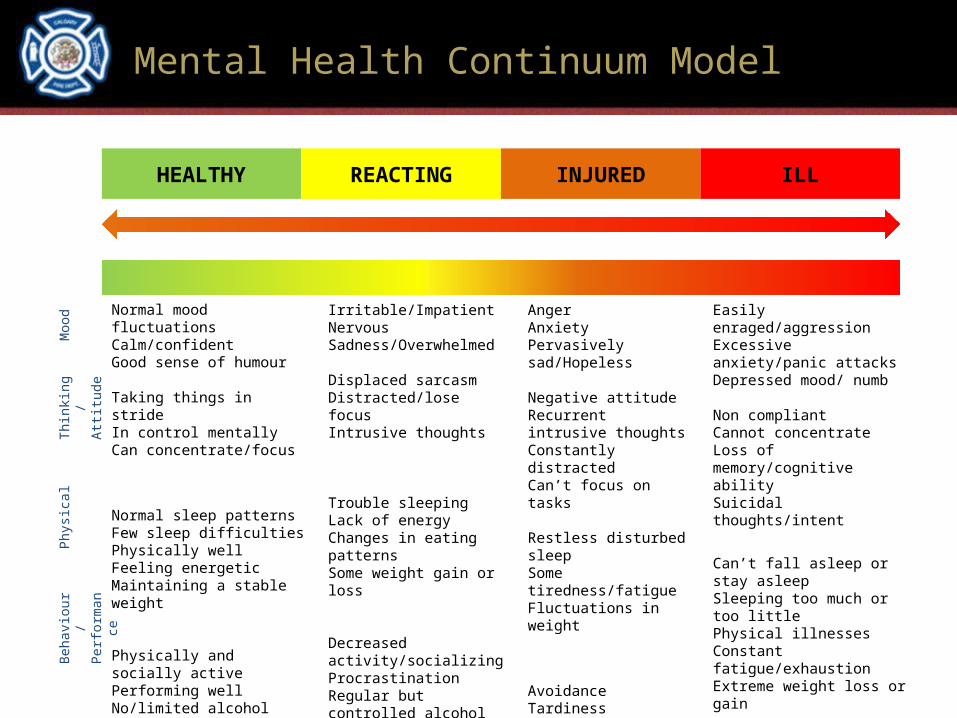
Mental Health Continuum Model
HEALTHY REACTING INJURED ILL
Good Mental healthNormal functioning
Common, self-limiting distress
More severe and persistent functional
impairment
Diagnosable mental illness
Severe and persistent functional
impairment
Adapted from the US Marine Corps.
Mental Health Continuum Model
HEALTHY REACTING INJURED ILL
Normal mood fluctuationsCalm/confidentGood sense of humour
Taking things in strideIn control mentallyCan concentrate/focus
Normal sleep patterns Few sleep difficultiesPhysically wellFeeling energeticMaintaining a stable weight
Physically and socially activePerforming wellNo/limited alcohol use/ gambling
Irritable/ImpatientNervousSadness/Overwhelmed
Displaced sarcasmDistracted/lose focusIntrusive thoughts
Trouble sleepingLack of energyChanges in eating patternsSome weight gain or loss
Decreased activity/socializingProcrastinationRegular but controlled alcohol use/gambling
AngerAnxietyPervasively sad/Hopeless
Negative attitudeRecurrent intrusive thoughtsConstantly distracted Can’t focus on tasks
Restless disturbed sleepSome tiredness/fatigueFluctuations in weight
AvoidanceTardinessDecreased performanceIncreased alcohol use/ gambling – hard to control
Easily enraged/aggressionExcessive anxiety/panic attacksDepressed mood/ numb
Non compliantCannot concentrateLoss of memory/cognitive abilitySuicidal thoughts/intent
Can’t fall asleep or stay asleepSleeping too much or too littlePhysical illnessesConstant fatigue/exhaustionExtreme weight loss or gain
WithdrawalAbsenteeismCan’t perform duties/tasksAlcohol or gambling addictionOther addictions
Moo
dTh
inki
ng/
Attitu
dePh
ysic
alBe
havi
our/
Perf
orm
ance

Delivery Model
• In-class group program
• Wallet cards (Mental Health Continuum)
• Aide Memoire

Three Versions of R2MR
Primary– for everyone - 4 hours
Leadership– supervisors – 8 hours
Train-the-Trainer – 5 days
Evaluation
• Initial evaluation by MHCC using questionnaires (immediate pre- and post-session and 3-month follow-up)
• Long-term tracking using CFD Wellness data

CFD Timeline
2015 Q1/Q2 • adaptation of course materials• engagement of leadership, peer support team• beginning messaging to the floor
2015 Q2• initial testing• training the trainers • continued engagement and communication

CFD Timeline
2015 Q3/4• pilot and evaluation of program• ongoing communication
2016 Q1• additional revisions
2016 Q2• beginning of full roll-out

Questions?