RN Review Neurology
153
RN Review_ Neurology Anila Simon PhD-c, RN, CVRN, CMSRN AppleRN Classes
Transcript of RN Review Neurology

RN Review_ Neurology
Anila Simon PhD-c, RN, CVRN, CMSRN AppleRN Classes



CNS• Brain and Spinal cord• Brain - Normal contents are 80% brain tissue, 10%
blood, 10% CSF• Covered and protected by three layers of tissue called
meninges. Dura mater, Arachnoid mater, and Pia mater.– The dura mater is a strong, thick membrane that closely
lines the inside of the skull– The arachnoid mater is a thin, web-like membrane that
covers the entire brain.• The arachnoid is made of elastic tissue.• The space between the dura and arachnoid membranes is called
the subdural space.– The pia mater hugs the surface of the brain and has many
blood vessels that reach deep into the brain.• The space between the arachnoid and pia is called the
subarachnoid space. It is here where the cerebrospinal fluidbathes and cushions the brain.
• Brain and Spinal cord• Brain - Normal contents are 80% brain tissue, 10%
blood, 10% CSF• Covered and protected by three layers of tissue called
meninges. Dura mater, Arachnoid mater, and Pia mater.– The dura mater is a strong, thick membrane that closely
lines the inside of the skull– The arachnoid mater is a thin, web-like membrane that
covers the entire brain.• The arachnoid is made of elastic tissue.• The space between the dura and arachnoid membranes is called
the subdural space.– The pia mater hugs the surface of the brain and has many
blood vessels that reach deep into the brain.• The space between the arachnoid and pia is called the
subarachnoid space. It is here where the cerebrospinal fluidbathes and cushions the brain.
• Brain and Spinal cord• Brain - Normal contents are 80% brain tissue, 10%
blood, 10% CSF• Covered and protected by three layers of tissue called
meninges. Dura mater, Arachnoid mater, and Pia mater.– The dura mater is a strong, thick membrane that closely
lines the inside of the skull– The arachnoid mater is a thin, web-like membrane that
covers the entire brain.• The arachnoid is made of elastic tissue.• The space between the dura and arachnoid membranes is called
the subdural space.– The pia mater hugs the surface of the brain and has many
blood vessels that reach deep into the brain.• The space between the arachnoid and pia is called the
subarachnoid space. It is here where the cerebrospinal fluidbathes and cushions the brain.
• Brain and Spinal cord• Brain - Normal contents are 80% brain tissue, 10%
blood, 10% CSF• Covered and protected by three layers of tissue called
meninges. Dura mater, Arachnoid mater, and Pia mater.– The dura mater is a strong, thick membrane that closely
lines the inside of the skull– The arachnoid mater is a thin, web-like membrane that
covers the entire brain.• The arachnoid is made of elastic tissue.• The space between the dura and arachnoid membranes is called
the subdural space.– The pia mater hugs the surface of the brain and has many
blood vessels that reach deep into the brain.• The space between the arachnoid and pia is called the
subarachnoid space. It is here where the cerebrospinal fluidbathes and cushions the brain.


• Cerebral circulation• Receives 15% to 20% of cardiac output (750 ml per
min)• Carotid arteries (anterior circulation)• Vertebral arteries (posterior circulation)• Cerebral veins empty into venous sinuses- jugular
veins• The sole source of cellular energy for the brain is
glucose. Again, because the brain is unable tostore glucose, it requires a constant supply.
• Brain metabolism• Cerebral glucose < 70 mg/dL = confusion• Cerebral glucose < 20 mg/dL = damage
• Cerebral circulation• Receives 15% to 20% of cardiac output (750 ml per
min)• Carotid arteries (anterior circulation)• Vertebral arteries (posterior circulation)• Cerebral veins empty into venous sinuses- jugular
veins• The sole source of cellular energy for the brain is
glucose. Again, because the brain is unable tostore glucose, it requires a constant supply.
• Brain metabolism• Cerebral glucose < 70 mg/dL = confusion• Cerebral glucose < 20 mg/dL = damage
• Cerebral circulation• Receives 15% to 20% of cardiac output (750 ml per
min)• Carotid arteries (anterior circulation)• Vertebral arteries (posterior circulation)• Cerebral veins empty into venous sinuses- jugular
veins• The sole source of cellular energy for the brain is
glucose. Again, because the brain is unable tostore glucose, it requires a constant supply.
• Brain metabolism• Cerebral glucose < 70 mg/dL = confusion• Cerebral glucose < 20 mg/dL = damage
• Cerebral circulation• Receives 15% to 20% of cardiac output (750 ml per
min)• Carotid arteries (anterior circulation)• Vertebral arteries (posterior circulation)• Cerebral veins empty into venous sinuses- jugular
veins• The sole source of cellular energy for the brain is
glucose. Again, because the brain is unable tostore glucose, it requires a constant supply.
• Brain metabolism• Cerebral glucose < 70 mg/dL = confusion• Cerebral glucose < 20 mg/dL = damage

Blood Brain Barrier• Prevent potentially harmful chemicals entering brain,
while regulating transport of essential molecules.• Metabolic wastes like urea, creatinine, toxins and most
drugs cannot pass BBB• Helps to maintain a stable environment at brain• Barrier is permeable to water, oxygen, CO2, glucose and
lipid soluble compounds.• Vitamins, minerals, glucose can pass. Antidepressants,
anti-anxiety medications, alcohol and cocaine mightalso pass.
• Infection, radiation, hypertension, trauma can alter BBB
• Prevent potentially harmful chemicals entering brain,while regulating transport of essential molecules.
• Metabolic wastes like urea, creatinine, toxins and mostdrugs cannot pass BBB
• Helps to maintain a stable environment at brain• Barrier is permeable to water, oxygen, CO2, glucose and
lipid soluble compounds.• Vitamins, minerals, glucose can pass. Antidepressants,
anti-anxiety medications, alcohol and cocaine mightalso pass.
• Infection, radiation, hypertension, trauma can alter BBB
• Prevent potentially harmful chemicals entering brain,while regulating transport of essential molecules.
• Metabolic wastes like urea, creatinine, toxins and mostdrugs cannot pass BBB
• Helps to maintain a stable environment at brain• Barrier is permeable to water, oxygen, CO2, glucose and
lipid soluble compounds.• Vitamins, minerals, glucose can pass. Antidepressants,
anti-anxiety medications, alcohol and cocaine mightalso pass.
• Infection, radiation, hypertension, trauma can alter BBB
• Prevent potentially harmful chemicals entering brain,while regulating transport of essential molecules.
• Metabolic wastes like urea, creatinine, toxins and mostdrugs cannot pass BBB
• Helps to maintain a stable environment at brain• Barrier is permeable to water, oxygen, CO2, glucose and
lipid soluble compounds.• Vitamins, minerals, glucose can pass. Antidepressants,
anti-anxiety medications, alcohol and cocaine mightalso pass.
• Infection, radiation, hypertension, trauma can alter BBB

Neurological Assessment– Risk factors– Cranial nerves– Level of alertness– Level of consciousness– Vital signs, respirations– Temperature– Pupils– Motor function– Posturing– Reflexes– Sensory function– Glasgow Coma Scale
Neurological Assessment– Risk factors– Cranial nerves– Level of alertness– Level of consciousness– Vital signs, respirations– Temperature– Pupils– Motor function– Posturing– Reflexes– Sensory function– Glasgow Coma Scale
Neurological Assessment– Risk factors– Cranial nerves– Level of alertness– Level of consciousness– Vital signs, respirations– Temperature– Pupils– Motor function– Posturing– Reflexes– Sensory function– Glasgow Coma Scale
Neurological Assessment– Risk factors– Cranial nerves– Level of alertness– Level of consciousness– Vital signs, respirations– Temperature– Pupils– Motor function– Posturing– Reflexes– Sensory function– Glasgow Coma Scale




DTR - A) Biceps, B) Brachioradial, C) Triceps, D) Patellar, E)Achilles, F) Evaluation of ankle clonus


Meningitis• Infectious process of CNS caused by bacteria and viruses;• May be acquired as primary disease or as result of
complications of neurosurgery, trauma, infection of sinuses orears, systemic infections, Viral illnesses such as the mumps,measles, herpes
• Vaccine• Haemophilus influenzae type b (Hib) vaccine – Infants• Pneumococcal polysaccharide vaccine (PPSV) – Vaccinate
adults who are immunocompromised, have a chronicdisease, smokers, live in long-term care facility. Give onedose to adults older than 65 years of age who have notpreviously been vaccinated nor have history of disease.
• Meningococcal vaccine – For adolescents living in aresidential setting in college, military persons againstNeisseria meningitidis
• There is no vaccine against viral meningitis.
Meningitis• Infectious process of CNS caused by bacteria and viruses;• May be acquired as primary disease or as result of
complications of neurosurgery, trauma, infection of sinuses orears, systemic infections, Viral illnesses such as the mumps,measles, herpes
• Vaccine• Haemophilus influenzae type b (Hib) vaccine – Infants• Pneumococcal polysaccharide vaccine (PPSV) – Vaccinate
adults who are immunocompromised, have a chronicdisease, smokers, live in long-term care facility. Give onedose to adults older than 65 years of age who have notpreviously been vaccinated nor have history of disease.
• Meningococcal vaccine – For adolescents living in aresidential setting in college, military persons againstNeisseria meningitidis
• There is no vaccine against viral meningitis.
Meningitis• Infectious process of CNS caused by bacteria and viruses;• May be acquired as primary disease or as result of
complications of neurosurgery, trauma, infection of sinuses orears, systemic infections, Viral illnesses such as the mumps,measles, herpes
• Vaccine• Haemophilus influenzae type b (Hib) vaccine – Infants• Pneumococcal polysaccharide vaccine (PPSV) – Vaccinate
adults who are immunocompromised, have a chronicdisease, smokers, live in long-term care facility. Give onedose to adults older than 65 years of age who have notpreviously been vaccinated nor have history of disease.
• Meningococcal vaccine – For adolescents living in aresidential setting in college, military persons againstNeisseria meningitidis
• There is no vaccine against viral meningitis.
Meningitis• Infectious process of CNS caused by bacteria and viruses;• May be acquired as primary disease or as result of
complications of neurosurgery, trauma, infection of sinuses orears, systemic infections, Viral illnesses such as the mumps,measles, herpes
• Vaccine• Haemophilus influenzae type b (Hib) vaccine – Infants• Pneumococcal polysaccharide vaccine (PPSV) – Vaccinate
adults who are immunocompromised, have a chronicdisease, smokers, live in long-term care facility. Give onedose to adults older than 65 years of age who have notpreviously been vaccinated nor have history of disease.
• Meningococcal vaccine – For adolescents living in aresidential setting in college, military persons againstNeisseria meningitidis
• There is no vaccine against viral meningitis.

Diagnostic Procedures
• Cerebrospinal fluid (CSF) analysis– Most definitive diagnostic procedure.– Appearance of CSF – cloudy (bacterial) or clear
(viral)– Elevated WBC– Elevated protein– Decreased glucose (bacterial)– Elevated CSF pressure
• Cerebrospinal fluid (CSF) analysis– Most definitive diagnostic procedure.– Appearance of CSF – cloudy (bacterial) or clear
(viral)– Elevated WBC– Elevated protein– Decreased glucose (bacterial)– Elevated CSF pressure
• Cerebrospinal fluid (CSF) analysis– Most definitive diagnostic procedure.– Appearance of CSF – cloudy (bacterial) or clear
(viral)– Elevated WBC– Elevated protein– Decreased glucose (bacterial)– Elevated CSF pressure
• Cerebrospinal fluid (CSF) analysis– Most definitive diagnostic procedure.– Appearance of CSF – cloudy (bacterial) or clear
(viral)– Elevated WBC– Elevated protein– Decreased glucose (bacterial)– Elevated CSF pressure


The rash doesn’t fade when you apply pressure to the skin.The rash doesn’t fade when you apply pressure to the skin.


• Infants/toddler additional signs : - Poor feeding; high-pitchedcry; bulging anterior fontanel, sunsetting eyes
• opisthotonus posture (Hyperextended neck and head –relieve some discomfort from meningeal irritation)
Hyperactive deep tendon reflexes, Tachycardia can also bepresent

Nursing Care• Isolate the client as soon as meningitis is
suspected– Droplet isolation for bacterial meningitis
• for first 24 hrs of antibiotics and when oral and nasalsecretions are no longer infectious.
– Standard precautions are implemented for all clientswho have meningitis.
• Report meningococcal infections to the publichealth department.
• Decrease environmental stimuli.• Implement fever-reduction measures, such as a
cooling blanket, if necessary
• Isolate the client as soon as meningitis issuspected– Droplet isolation for bacterial meningitis
• for first 24 hrs of antibiotics and when oral and nasalsecretions are no longer infectious.
– Standard precautions are implemented for all clientswho have meningitis.
• Report meningococcal infections to the publichealth department.
• Decrease environmental stimuli.• Implement fever-reduction measures, such as a
cooling blanket, if necessary
• Isolate the client as soon as meningitis issuspected– Droplet isolation for bacterial meningitis
• for first 24 hrs of antibiotics and when oral and nasalsecretions are no longer infectious.
– Standard precautions are implemented for all clientswho have meningitis.
• Report meningococcal infections to the publichealth department.
• Decrease environmental stimuli.• Implement fever-reduction measures, such as a
cooling blanket, if necessary
• Isolate the client as soon as meningitis issuspected– Droplet isolation for bacterial meningitis
• for first 24 hrs of antibiotics and when oral and nasalsecretions are no longer infectious.
– Standard precautions are implemented for all clientswho have meningitis.
• Report meningococcal infections to the publichealth department.
• Decrease environmental stimuli.• Implement fever-reduction measures, such as a
cooling blanket, if necessary

Nursing care (contd)• Provide a quiet environment.• Minimize exposure to bright light (natural and electric).• Maintain bed rest with the head of the bed elevated to 30°.• Monitor the client for increased intracranial pressure (ICP).
– Tell the client to avoid coughing and sneezing, which increaseICP.
• Maintain client safety, such as seizure precautions.• Replace fluid and electrolytes as indicated by laboratory
values.• Older adult clients are at an increased risk for secondary
complications, such as pneumonia.• Prophylactic antibiotics given to individuals in close contact
with the client.
• Provide a quiet environment.• Minimize exposure to bright light (natural and electric).• Maintain bed rest with the head of the bed elevated to 30°.• Monitor the client for increased intracranial pressure (ICP).
– Tell the client to avoid coughing and sneezing, which increaseICP.
• Maintain client safety, such as seizure precautions.• Replace fluid and electrolytes as indicated by laboratory
values.• Older adult clients are at an increased risk for secondary
complications, such as pneumonia.• Prophylactic antibiotics given to individuals in close contact
with the client.
• Provide a quiet environment.• Minimize exposure to bright light (natural and electric).• Maintain bed rest with the head of the bed elevated to 30°.• Monitor the client for increased intracranial pressure (ICP).
– Tell the client to avoid coughing and sneezing, which increaseICP.
• Maintain client safety, such as seizure precautions.• Replace fluid and electrolytes as indicated by laboratory
values.• Older adult clients are at an increased risk for secondary
complications, such as pneumonia.• Prophylactic antibiotics given to individuals in close contact
with the client.
• Provide a quiet environment.• Minimize exposure to bright light (natural and electric).• Maintain bed rest with the head of the bed elevated to 30°.• Monitor the client for increased intracranial pressure (ICP).
– Tell the client to avoid coughing and sneezing, which increaseICP.
• Maintain client safety, such as seizure precautions.• Replace fluid and electrolytes as indicated by laboratory
values.• Older adult clients are at an increased risk for secondary
complications, such as pneumonia.• Prophylactic antibiotics given to individuals in close contact
with the client.

Complications• Increased ICP (possibly to the point of brain herniation)
– Meningitis can cause ICP to increase.– Nursing Actions
• Monitor for signs of increasing ICP (LOC changes, pupillarychanges, impaired extraocular movements).
• Provide interventions to reduce ICP (positioning and avoidance ofcoughing and straining).
• Mannitol can be administered via IV.
• Septic emboli (leading to disseminated intravascularcoagulation or cardiovascular accident)– Septic emboli can form during meningitis and travel to
other parts of the body, particularly the handsand feet.
• Increased ICP (possibly to the point of brain herniation)– Meningitis can cause ICP to increase.– Nursing Actions
• Monitor for signs of increasing ICP (LOC changes, pupillarychanges, impaired extraocular movements).
• Provide interventions to reduce ICP (positioning and avoidance ofcoughing and straining).
• Mannitol can be administered via IV.
• Septic emboli (leading to disseminated intravascularcoagulation or cardiovascular accident)– Septic emboli can form during meningitis and travel to
other parts of the body, particularly the handsand feet.
• Increased ICP (possibly to the point of brain herniation)– Meningitis can cause ICP to increase.– Nursing Actions
• Monitor for signs of increasing ICP (LOC changes, pupillarychanges, impaired extraocular movements).
• Provide interventions to reduce ICP (positioning and avoidance ofcoughing and straining).
• Mannitol can be administered via IV.
• Septic emboli (leading to disseminated intravascularcoagulation or cardiovascular accident)– Septic emboli can form during meningitis and travel to
other parts of the body, particularly the handsand feet.
• Increased ICP (possibly to the point of brain herniation)– Meningitis can cause ICP to increase.– Nursing Actions
• Monitor for signs of increasing ICP (LOC changes, pupillarychanges, impaired extraocular movements).
• Provide interventions to reduce ICP (positioning and avoidance ofcoughing and straining).
• Mannitol can be administered via IV.
• Septic emboli (leading to disseminated intravascularcoagulation or cardiovascular accident)– Septic emboli can form during meningitis and travel to
other parts of the body, particularly the handsand feet.

Complications of Meningitis
• Syndrome of inappropriate antidiuretic hormone(SIADH)– SIADH can be a complication of meningitis by
abnormal stimulation to the hypothalamic area of thebrain, causing excess secretion of antidiuretichormone (vasopressin).
• Nursing Actions– Monitor for signs and symptoms (dilute blood,
concentrated urine).– Provide interventions, such as the administration of
demeclocycline (Declomycin) and restriction of fluid.
• Syndrome of inappropriate antidiuretic hormone(SIADH)– SIADH can be a complication of meningitis by
abnormal stimulation to the hypothalamic area of thebrain, causing excess secretion of antidiuretichormone (vasopressin).
• Nursing Actions– Monitor for signs and symptoms (dilute blood,
concentrated urine).– Provide interventions, such as the administration of
demeclocycline (Declomycin) and restriction of fluid.
• Syndrome of inappropriate antidiuretic hormone(SIADH)– SIADH can be a complication of meningitis by
abnormal stimulation to the hypothalamic area of thebrain, causing excess secretion of antidiuretichormone (vasopressin).
• Nursing Actions– Monitor for signs and symptoms (dilute blood,
concentrated urine).– Provide interventions, such as the administration of
demeclocycline (Declomycin) and restriction of fluid.
• Syndrome of inappropriate antidiuretic hormone(SIADH)– SIADH can be a complication of meningitis by
abnormal stimulation to the hypothalamic area of thebrain, causing excess secretion of antidiuretichormone (vasopressin).
• Nursing Actions– Monitor for signs and symptoms (dilute blood,
concentrated urine).– Provide interventions, such as the administration of
demeclocycline (Declomycin) and restriction of fluid.

• 1. A nurse is assessing a client who reports severeheadache and a stiff neck. The nurse’sassessment reveals positive Kernig’s andBrudzinski’s signs. Which of the following actionsshould the nurse perform first?
• A. Administer antibiotics• B. Implement droplet isolation precautions• C. Initiate IV access• D. Decrease bright lights
• 1. A nurse is assessing a client who reports severeheadache and a stiff neck. The nurse’sassessment reveals positive Kernig’s andBrudzinski’s signs. Which of the following actionsshould the nurse perform first?
• A. Administer antibiotics• B. Implement droplet isolation precautions• C. Initiate IV access• D. Decrease bright lights

• A. Incorrect: The nurse should administer antibiotics asearly as possible to stop the micro-organisms frommultiplying, but this is not the priority action.
• B. Correct: When using the urgent vs. non urgent approachto care, the nurse determines the priority action is to placethe client in droplet precaution isolation when meningitis issuspected to prevent spread of the disease to others.
• C. Incorrect: The nurse should initiate IV access as early aspossible to allow IV medication and fluid administration,but this is not the priority action.
• D. Incorrect: The nurse should decrease bright lightsbecause of the client’s sensitivity to light, but this is not thepriority action.
• A. Incorrect: The nurse should administer antibiotics asearly as possible to stop the micro-organisms frommultiplying, but this is not the priority action.
• B. Correct: When using the urgent vs. non urgent approachto care, the nurse determines the priority action is to placethe client in droplet precaution isolation when meningitis issuspected to prevent spread of the disease to others.
• C. Incorrect: The nurse should initiate IV access as early aspossible to allow IV medication and fluid administration,but this is not the priority action.
• D. Incorrect: The nurse should decrease bright lightsbecause of the client’s sensitivity to light, but this is not thepriority action.

• 2. A nurse is assessing for the presence ofBrudzinski’s sign in a client who has suspectedmeningitis. Which of the following areappropriate actions by the nurse whenperforming this technique? (Select all that apply.)
• A. Place client in supine position.• B. Flex client’s hip and knee.• C. Place hands behind the client’s neck.• D. Bend client’s head toward chest.• E. Straighten the client’s flexed leg at the knee.
• 2. A nurse is assessing for the presence ofBrudzinski’s sign in a client who has suspectedmeningitis. Which of the following areappropriate actions by the nurse whenperforming this technique? (Select all that apply.)
• A. Place client in supine position.• B. Flex client’s hip and knee.• C. Place hands behind the client’s neck.• D. Bend client’s head toward chest.• E. Straighten the client’s flexed leg at the knee.

• A. Correct: The nurse should place the client in supineposition when assessing for Brudzinski’s sign.
• B. Incorrect: The nurse should flex the client’s hip and kneewhen assessing for Kernig’s sign but not Brudzinski’s sign.
• C. Correct: The nurse should place her hands behind theclient’s neck when assessing for Brudzinski’s sign, in orderto flex the client’s neck.
• D. Correct: The nurse should bend the client’s head towardthe chest when assessing for Brudzinski’s sign; it is apositive if the client reports pain.
• E. Incorrect: The nurse should straighten the client’s flexedleg at the knee when assessing for Kernig’s sign but notBrudzinski’s sign.
• A. Correct: The nurse should place the client in supineposition when assessing for Brudzinski’s sign.
• B. Incorrect: The nurse should flex the client’s hip and kneewhen assessing for Kernig’s sign but not Brudzinski’s sign.
• C. Correct: The nurse should place her hands behind theclient’s neck when assessing for Brudzinski’s sign, in orderto flex the client’s neck.
• D. Correct: The nurse should bend the client’s head towardthe chest when assessing for Brudzinski’s sign; it is apositive if the client reports pain.
• E. Incorrect: The nurse should straighten the client’s flexedleg at the knee when assessing for Kernig’s sign but notBrudzinski’s sign.

• A nurse is reviewing the health record of astudent newly admitted to a university and livingin a dormitory. The health record indicates thestudent requires follow-up immunizations. Whichof the following organisms should the nurse planto vaccinate the student against?
• A. Streptococcus pneumoniae• B. Neisseria meningitidis• C. Bartonella henselae• D. Rickettsia rickettsii
• A nurse is reviewing the health record of astudent newly admitted to a university and livingin a dormitory. The health record indicates thestudent requires follow-up immunizations. Whichof the following organisms should the nurse planto vaccinate the student against?
• A. Streptococcus pneumoniae• B. Neisseria meningitidis• C. Bartonella henselae• D. Rickettsia rickettsii

• B. Correct: The nurse should plan toadminister a vaccine against Neisseriameningitidis because it is recommended thatcollege students living in close proximity beimmunized to against meningitis.
• B. Correct: The nurse should plan toadminister a vaccine against Neisseriameningitidis because it is recommended thatcollege students living in close proximity beimmunized to against meningitis.

• A nurse is planning care for a client who hasbacterial meningitis. Which of the followingactions should the nurse include in the plan ofcare? (Select all that apply.)
• A. Monitor for bradycardia.• B. Provide an emesis basin at the bedside.• C. Administer antipyretic medication as
prescribed.• D. Perform a skin assessment.• E. Keep the head of the bed flat.
• A nurse is planning care for a client who hasbacterial meningitis. Which of the followingactions should the nurse include in the plan ofcare? (Select all that apply.)
• A. Monitor for bradycardia.• B. Provide an emesis basin at the bedside.• C. Administer antipyretic medication as
prescribed.• D. Perform a skin assessment.• E. Keep the head of the bed flat.

• A. Incorrect: The nurse should plan to monitor fortachycardia when a client has meningitis.
• B. Correct: The nurse should provide an emesis basin at thebedside because the client who has meningitis may havenausea and vomiting.
• C. Correct: The nurse should plan to administer antipyreticmedication for fever to a client who has meningitis.
• D. Correct: The nurse should perform a skin assessment todetermine whether the client has a red macular rashassociated with meningococcal meningitis.
• E. Incorrect: The nurse should elevate the head of theclient’s bed 30° to promote venous drainage from the headand prevent increased intracranial pressure (ICP).
• A. Incorrect: The nurse should plan to monitor fortachycardia when a client has meningitis.
• B. Correct: The nurse should provide an emesis basin at thebedside because the client who has meningitis may havenausea and vomiting.
• C. Correct: The nurse should plan to administer antipyreticmedication for fever to a client who has meningitis.
• D. Correct: The nurse should perform a skin assessment todetermine whether the client has a red macular rashassociated with meningococcal meningitis.
• E. Incorrect: The nurse should elevate the head of theclient’s bed 30° to promote venous drainage from the headand prevent increased intracranial pressure (ICP).

Increased Intracranial Pressure (ICP)• Rise in pressure in cranial vault caused by trauma,
hemorrhage, tumors, edema, or inflammation.• ICP Normal level is upto 15 mm Hg (5-15)• ICP may be increased by
– Hypercarbia, which leads to cerebral vasodilation andedema
– Endotracheal or oral tracheal suctioning– Coughing– Blowing the nose forcefully– Extreme neck or hip flexion/extension– Maintaining the head of the bed at an angle less than 30°– Increasing intra-abdominal pressure (restrictive clothing,
Valsalva maneuver).
• Rise in pressure in cranial vault caused by trauma,hemorrhage, tumors, edema, or inflammation.
• ICP Normal level is upto 15 mm Hg (5-15)• ICP may be increased by
– Hypercarbia, which leads to cerebral vasodilation andedema
– Endotracheal or oral tracheal suctioning– Coughing– Blowing the nose forcefully– Extreme neck or hip flexion/extension– Maintaining the head of the bed at an angle less than 30°– Increasing intra-abdominal pressure (restrictive clothing,
Valsalva maneuver).
• Rise in pressure in cranial vault caused by trauma,hemorrhage, tumors, edema, or inflammation.
• ICP Normal level is upto 15 mm Hg (5-15)• ICP may be increased by
– Hypercarbia, which leads to cerebral vasodilation andedema
– Endotracheal or oral tracheal suctioning– Coughing– Blowing the nose forcefully– Extreme neck or hip flexion/extension– Maintaining the head of the bed at an angle less than 30°– Increasing intra-abdominal pressure (restrictive clothing,
Valsalva maneuver).
• Rise in pressure in cranial vault caused by trauma,hemorrhage, tumors, edema, or inflammation.
• ICP Normal level is upto 15 mm Hg (5-15)• ICP may be increased by
– Hypercarbia, which leads to cerebral vasodilation andedema
– Endotracheal or oral tracheal suctioning– Coughing– Blowing the nose forcefully– Extreme neck or hip flexion/extension– Maintaining the head of the bed at an angle less than 30°– Increasing intra-abdominal pressure (restrictive clothing,
Valsalva maneuver).

Increased Intracranial Pressure (ICP)
• Early signs include restlessness and change in level ofconsciousness
• Late signs include increasing systolic blood pressure withwidened pulse pressure, slowed heart rate, irregularrespirations (cushing’s triad)
• A change in body temperature may also occur becauseincreased ICP affects the hypothalamus.
• Cheyne-Stokes respirations• Occular signs• Assess neurological status Q 1 to 2 hrs• Assess bowel (constipation) and bladder (distention) to
avoid valsalva maneuver
• Early signs include restlessness and change in level ofconsciousness
• Late signs include increasing systolic blood pressure withwidened pulse pressure, slowed heart rate, irregularrespirations (cushing’s triad)
• A change in body temperature may also occur becauseincreased ICP affects the hypothalamus.
• Cheyne-Stokes respirations• Occular signs• Assess neurological status Q 1 to 2 hrs• Assess bowel (constipation) and bladder (distention) to
avoid valsalva maneuver
• Early signs include restlessness and change in level ofconsciousness
• Late signs include increasing systolic blood pressure withwidened pulse pressure, slowed heart rate, irregularrespirations (cushing’s triad)
• A change in body temperature may also occur becauseincreased ICP affects the hypothalamus.
• Cheyne-Stokes respirations• Occular signs• Assess neurological status Q 1 to 2 hrs• Assess bowel (constipation) and bladder (distention) to
avoid valsalva maneuver
• Early signs include restlessness and change in level ofconsciousness
• Late signs include increasing systolic blood pressure withwidened pulse pressure, slowed heart rate, irregularrespirations (cushing’s triad)
• A change in body temperature may also occur becauseincreased ICP affects the hypothalamus.
• Cheyne-Stokes respirations• Occular signs• Assess neurological status Q 1 to 2 hrs• Assess bowel (constipation) and bladder (distention) to
avoid valsalva maneuver

Ocular Signs• Compression of cranial nerve (CN) III, the oculomotor
nerve, results in– Dilation of the pupil on the same side (ipsilateral) as the mass/
lesion– Sluggish or no response to light– Inability to move the eye upward– Ptosis of the eyelid.
• These signs can be the result of a shifting of the brain fromthe midline, compressing the trunk of CN III and paralyzingthe muscles controlling pupillary size and shape.
• A fixed, unilateral, dilated pupil is considered a neurologicemergency that indicates herniation of the brain.
• Other cranial nerves may also be affected leading toblurred vision, diplopia, and changes in extraocular eyemovements.
• Compression of cranial nerve (CN) III, the oculomotornerve, results in– Dilation of the pupil on the same side (ipsilateral) as the mass/
lesion– Sluggish or no response to light– Inability to move the eye upward– Ptosis of the eyelid.
• These signs can be the result of a shifting of the brain fromthe midline, compressing the trunk of CN III and paralyzingthe muscles controlling pupillary size and shape.
• A fixed, unilateral, dilated pupil is considered a neurologicemergency that indicates herniation of the brain.
• Other cranial nerves may also be affected leading toblurred vision, diplopia, and changes in extraocular eyemovements.
• Compression of cranial nerve (CN) III, the oculomotornerve, results in– Dilation of the pupil on the same side (ipsilateral) as the mass/
lesion– Sluggish or no response to light– Inability to move the eye upward– Ptosis of the eyelid.
• These signs can be the result of a shifting of the brain fromthe midline, compressing the trunk of CN III and paralyzingthe muscles controlling pupillary size and shape.
• A fixed, unilateral, dilated pupil is considered a neurologicemergency that indicates herniation of the brain.
• Other cranial nerves may also be affected leading toblurred vision, diplopia, and changes in extraocular eyemovements.
• Compression of cranial nerve (CN) III, the oculomotornerve, results in– Dilation of the pupil on the same side (ipsilateral) as the mass/
lesion– Sluggish or no response to light– Inability to move the eye upward– Ptosis of the eyelid.
• These signs can be the result of a shifting of the brain fromthe midline, compressing the trunk of CN III and paralyzingthe muscles controlling pupillary size and shape.
• A fixed, unilateral, dilated pupil is considered a neurologicemergency that indicates herniation of the brain.
• Other cranial nerves may also be affected leading toblurred vision, diplopia, and changes in extraocular eyemovements.



ICP - Intervention• Elevate head at least 30° to reduce ICP and to promote venous
drainage.• Avoid extreme flexion, extension, or rotation of the head, and
maintain the body in a midline neutral position.• Maintain a patent airway. Provide mechanical ventilation as
indicated.• Hyperventilate clients on mechanical ventilation to keep the PaCO2
between 35 to 38 mm Hg. This reduces cerebral blood flow.• Administer oxygen as indicated to maintain an oxygen saturation
level of greater than 92%.• Maintain cervical spine stability until cleared by an x-ray.• Provide a calm, restful environment (limit visitors, minimize noise).• Plan activities to avoid stress- not too long• Monitor fluid and electrolyte values• Maintain safety and seizure precautions
• Elevate head at least 30° to reduce ICP and to promote venousdrainage.
• Avoid extreme flexion, extension, or rotation of the head, andmaintain the body in a midline neutral position.
• Maintain a patent airway. Provide mechanical ventilation asindicated.
• Hyperventilate clients on mechanical ventilation to keep the PaCO2between 35 to 38 mm Hg. This reduces cerebral blood flow.
• Administer oxygen as indicated to maintain an oxygen saturationlevel of greater than 92%.
• Maintain cervical spine stability until cleared by an x-ray.• Provide a calm, restful environment (limit visitors, minimize noise).• Plan activities to avoid stress- not too long• Monitor fluid and electrolyte values• Maintain safety and seizure precautions
• Elevate head at least 30° to reduce ICP and to promote venousdrainage.
• Avoid extreme flexion, extension, or rotation of the head, andmaintain the body in a midline neutral position.
• Maintain a patent airway. Provide mechanical ventilation asindicated.
• Hyperventilate clients on mechanical ventilation to keep the PaCO2between 35 to 38 mm Hg. This reduces cerebral blood flow.
• Administer oxygen as indicated to maintain an oxygen saturationlevel of greater than 92%.
• Maintain cervical spine stability until cleared by an x-ray.• Provide a calm, restful environment (limit visitors, minimize noise).• Plan activities to avoid stress- not too long• Monitor fluid and electrolyte values• Maintain safety and seizure precautions
• Elevate head at least 30° to reduce ICP and to promote venousdrainage.
• Avoid extreme flexion, extension, or rotation of the head, andmaintain the body in a midline neutral position.
• Maintain a patent airway. Provide mechanical ventilation asindicated.
• Hyperventilate clients on mechanical ventilation to keep the PaCO2between 35 to 38 mm Hg. This reduces cerebral blood flow.
• Administer oxygen as indicated to maintain an oxygen saturationlevel of greater than 92%.
• Maintain cervical spine stability until cleared by an x-ray.• Provide a calm, restful environment (limit visitors, minimize noise).• Plan activities to avoid stress- not too long• Monitor fluid and electrolyte values• Maintain safety and seizure precautions

Meds• Diuretics (manitol and lasix)
– Draw water from edematous tissues into vascularsystem.
– Might also disturb glucose and electrolyte levels– Patient need strict I/O (insert foley)
• Corticosteroids :- Reduce inflammation• Teaching
– Avoid coughing , blowing nose, straining, pushingagainst bed/side rails
– Maintain neutral head and neck alignment– Family to maintain quiet environment
• Diuretics (manitol and lasix)– Draw water from edematous tissues into vascular
system.– Might also disturb glucose and electrolyte levels– Patient need strict I/O (insert foley)
• Corticosteroids :- Reduce inflammation• Teaching
– Avoid coughing , blowing nose, straining, pushingagainst bed/side rails
– Maintain neutral head and neck alignment– Family to maintain quiet environment
• Diuretics (manitol and lasix)– Draw water from edematous tissues into vascular
system.– Might also disturb glucose and electrolyte levels– Patient need strict I/O (insert foley)
• Corticosteroids :- Reduce inflammation• Teaching
– Avoid coughing , blowing nose, straining, pushingagainst bed/side rails
– Maintain neutral head and neck alignment– Family to maintain quiet environment
• Diuretics (manitol and lasix)– Draw water from edematous tissues into vascular
system.– Might also disturb glucose and electrolyte levels– Patient need strict I/O (insert foley)
• Corticosteroids :- Reduce inflammation• Teaching
– Avoid coughing , blowing nose, straining, pushingagainst bed/side rails
– Maintain neutral head and neck alignment– Family to maintain quiet environment
The Unconscious Client• State of depressed cerebral functioning with unresponsiveness to
sensory and motor function– Assessment
• Unarousable• Unresponsiveness to sensory and motor stimuli• GCS scale• Diagnostis- CT and MRI (hgs? Tumor? Edema?)
• EEG – (? Seizure)• Cerebral angiography (?circulation, aneurysm)• LP (CSF – infection)• Blood work, ABG
– Interventions• Maintain a patent airway and monitor airway status• Clear secretions, assess breath sounds)• Provide total care to client – side lying position, HOB elevated• Protect the client from injury (aspiration)
The Unconscious Client• State of depressed cerebral functioning with unresponsiveness to
sensory and motor function– Assessment
• Unarousable• Unresponsiveness to sensory and motor stimuli• GCS scale• Diagnostis- CT and MRI (hgs? Tumor? Edema?)
• EEG – (? Seizure)• Cerebral angiography (?circulation, aneurysm)• LP (CSF – infection)• Blood work, ABG
– Interventions• Maintain a patent airway and monitor airway status• Clear secretions, assess breath sounds)• Provide total care to client – side lying position, HOB elevated• Protect the client from injury (aspiration)
The Unconscious Client• State of depressed cerebral functioning with unresponsiveness to
sensory and motor function– Assessment
• Unarousable• Unresponsiveness to sensory and motor stimuli• GCS scale• Diagnostis- CT and MRI (hgs? Tumor? Edema?)
• EEG – (? Seizure)• Cerebral angiography (?circulation, aneurysm)• LP (CSF – infection)• Blood work, ABG
– Interventions• Maintain a patent airway and monitor airway status• Clear secretions, assess breath sounds)• Provide total care to client – side lying position, HOB elevated• Protect the client from injury (aspiration)
The Unconscious Client• State of depressed cerebral functioning with unresponsiveness to
sensory and motor function– Assessment
• Unarousable• Unresponsiveness to sensory and motor stimuli• GCS scale• Diagnostis- CT and MRI (hgs? Tumor? Edema?)
• EEG – (? Seizure)• Cerebral angiography (?circulation, aneurysm)• LP (CSF – infection)• Blood work, ABG
– Interventions• Maintain a patent airway and monitor airway status• Clear secretions, assess breath sounds)• Provide total care to client – side lying position, HOB elevated• Protect the client from injury (aspiration)

Hyperthermia– Description
• A temperature greater than 105 F, which increasescerebral metabolism and risk for hypoxia
– Assessment• A temperature greater than 105 F
– Interventions• Maintain a patent airway• Initiate seizure precautions• Inducement of normothermia with fluids, cool baths, or
hypothermia blanket
Hyperthermia– Description
• A temperature greater than 105 F, which increasescerebral metabolism and risk for hypoxia
– Assessment• A temperature greater than 105 F
– Interventions• Maintain a patent airway• Initiate seizure precautions• Inducement of normothermia with fluids, cool baths, or
hypothermia blanket
Hyperthermia– Description
• A temperature greater than 105 F, which increasescerebral metabolism and risk for hypoxia
– Assessment• A temperature greater than 105 F
– Interventions• Maintain a patent airway• Initiate seizure precautions• Inducement of normothermia with fluids, cool baths, or
hypothermia blanket
Hyperthermia– Description
• A temperature greater than 105 F, which increasescerebral metabolism and risk for hypoxia
– Assessment• A temperature greater than 105 F
– Interventions• Maintain a patent airway• Initiate seizure precautions• Inducement of normothermia with fluids, cool baths, or
hypothermia blanket

Head Injury• Types
– 1. open/ penetrating trauma (skull integrity compromised)– 2. closed/ blunt trauma (skull integrity maintained)
• Fractures– Linear – most common – possible hematoma but dura intact.
• Minimal risk– Comminuted and Depressed – overlying skin and dura can
be damaged.• High risk for brain damage and infection• Need surgery within 24 hrs
– Basilar – involve base of skull – CSF leakage - preventmeningitis
• Types– 1. open/ penetrating trauma (skull integrity compromised)– 2. closed/ blunt trauma (skull integrity maintained)
• Fractures– Linear – most common – possible hematoma but dura intact.
• Minimal risk– Comminuted and Depressed – overlying skin and dura can
be damaged.• High risk for brain damage and infection• Need surgery within 24 hrs
– Basilar – involve base of skull – CSF leakage - preventmeningitis
• Types– 1. open/ penetrating trauma (skull integrity compromised)– 2. closed/ blunt trauma (skull integrity maintained)
• Fractures– Linear – most common – possible hematoma but dura intact.
• Minimal risk– Comminuted and Depressed – overlying skin and dura can
be damaged.• High risk for brain damage and infection• Need surgery within 24 hrs
– Basilar – involve base of skull – CSF leakage - preventmeningitis
• Types– 1. open/ penetrating trauma (skull integrity compromised)– 2. closed/ blunt trauma (skull integrity maintained)
• Fractures– Linear – most common – possible hematoma but dura intact.
• Minimal risk– Comminuted and Depressed – overlying skin and dura can
be damaged.• High risk for brain damage and infection• Need surgery within 24 hrs
– Basilar – involve base of skull – CSF leakage - preventmeningitis

• Basilar Skull Fracture Signs– Battle’s Sign : Ecchymosis over mastoid process– Hemotympanum – Blood visible behind tympanic
membrane– Raccoon eyes – Bilateral peri orbital echymosis– Rhinorrhea – CSF leakage through nose– Otorrhea - CSF leakage through ear
• CSF – test reveal glucose. Mucus – no glucose• Halo sign• 1 hr “golden window” for treatment of head
injuries- emergency treatment provided duringthis time frame decreases the morbidity andmortality
• Basilar Skull Fracture Signs– Battle’s Sign : Ecchymosis over mastoid process– Hemotympanum – Blood visible behind tympanic
membrane– Raccoon eyes – Bilateral peri orbital echymosis– Rhinorrhea – CSF leakage through nose– Otorrhea - CSF leakage through ear
• CSF – test reveal glucose. Mucus – no glucose• Halo sign• 1 hr “golden window” for treatment of head
injuries- emergency treatment provided duringthis time frame decreases the morbidity andmortality
• Basilar Skull Fracture Signs– Battle’s Sign : Ecchymosis over mastoid process– Hemotympanum – Blood visible behind tympanic
membrane– Raccoon eyes – Bilateral peri orbital echymosis– Rhinorrhea – CSF leakage through nose– Otorrhea - CSF leakage through ear
• CSF – test reveal glucose. Mucus – no glucose• Halo sign• 1 hr “golden window” for treatment of head
injuries- emergency treatment provided duringthis time frame decreases the morbidity andmortality
• Basilar Skull Fracture Signs– Battle’s Sign : Ecchymosis over mastoid process– Hemotympanum – Blood visible behind tympanic
membrane– Raccoon eyes – Bilateral peri orbital echymosis– Rhinorrhea – CSF leakage through nose– Otorrhea - CSF leakage through ear
• CSF – test reveal glucose. Mucus – no glucose• Halo sign• 1 hr “golden window” for treatment of head
injuries- emergency treatment provided duringthis time frame decreases the morbidity andmortality


• Head injuries may be associated with hemorrhage– Epidural Hematoma: Between dura and skull
• Usually from a tear in meningeal artery• Rapid deterioration in neurological status
– Subdural Hematoma• Usually involve veins (might involve small arteries)
– Intra cerebral• Bleeding into brain tissue• Most common – frontal or temporal lobes
• Monitor for severe headache, rapid decline in level ofconsciousness, worsening neurological function and herniation,and changes in ICP.
• Surgery needed to remove subdural & epidural hematoma.• Intracranial hemorrhage is treated with osmotic diuretics.
• Head injuries may be associated with hemorrhage– Epidural Hematoma: Between dura and skull
• Usually from a tear in meningeal artery• Rapid deterioration in neurological status
– Subdural Hematoma• Usually involve veins (might involve small arteries)
– Intra cerebral• Bleeding into brain tissue• Most common – frontal or temporal lobes
• Monitor for severe headache, rapid decline in level ofconsciousness, worsening neurological function and herniation,and changes in ICP.
• Surgery needed to remove subdural & epidural hematoma.• Intracranial hemorrhage is treated with osmotic diuretics.
• Head injuries may be associated with hemorrhage– Epidural Hematoma: Between dura and skull
• Usually from a tear in meningeal artery• Rapid deterioration in neurological status
– Subdural Hematoma• Usually involve veins (might involve small arteries)
– Intra cerebral• Bleeding into brain tissue• Most common – frontal or temporal lobes
• Monitor for severe headache, rapid decline in level ofconsciousness, worsening neurological function and herniation,and changes in ICP.
• Surgery needed to remove subdural & epidural hematoma.• Intracranial hemorrhage is treated with osmotic diuretics.
• Head injuries may be associated with hemorrhage– Epidural Hematoma: Between dura and skull
• Usually from a tear in meningeal artery• Rapid deterioration in neurological status
– Subdural Hematoma• Usually involve veins (might involve small arteries)
– Intra cerebral• Bleeding into brain tissue• Most common – frontal or temporal lobes
• Monitor for severe headache, rapid decline in level ofconsciousness, worsening neurological function and herniation,and changes in ICP.
• Surgery needed to remove subdural & epidural hematoma.• Intracranial hemorrhage is treated with osmotic diuretics.
Nursing Care• Assess/monitor the client at regularly scheduled
intervals:– Respiratory status – the priority assessment– Brain function begins to diminish after 3 min of oxygen
deprivation.– Changes in level of consciousness, using the GCS.– Cranial nerve function (eye blink response, gag reflex,
tongue and shoulder movement), Pupillary changes(PERRLA)
– Findings of infection (nuchal rigidity occurs withmeningitis)
– Bilateral sensory and motor responses– Intracranial pressure (ICP)
• Assess/monitor the client at regularly scheduledintervals:– Respiratory status – the priority assessment– Brain function begins to diminish after 3 min of oxygen
deprivation.– Changes in level of consciousness, using the GCS.– Cranial nerve function (eye blink response, gag reflex,
tongue and shoulder movement), Pupillary changes(PERRLA)
– Findings of infection (nuchal rigidity occurs withmeningitis)
– Bilateral sensory and motor responses– Intracranial pressure (ICP)
• Assess/monitor the client at regularly scheduledintervals:– Respiratory status – the priority assessment– Brain function begins to diminish after 3 min of oxygen
deprivation.– Changes in level of consciousness, using the GCS.– Cranial nerve function (eye blink response, gag reflex,
tongue and shoulder movement), Pupillary changes(PERRLA)
– Findings of infection (nuchal rigidity occurs withmeningitis)
– Bilateral sensory and motor responses– Intracranial pressure (ICP)
• Assess/monitor the client at regularly scheduledintervals:– Respiratory status – the priority assessment– Brain function begins to diminish after 3 min of oxygen
deprivation.– Changes in level of consciousness, using the GCS.– Cranial nerve function (eye blink response, gag reflex,
tongue and shoulder movement), Pupillary changes(PERRLA)
– Findings of infection (nuchal rigidity occurs withmeningitis)
– Bilateral sensory and motor responses– Intracranial pressure (ICP)

Craniotomy
• A craniotomy is the removal of nonviable braintissue that allows for expansion and/or removalof epidural or subdural hematomas.
• It involves drilling a burr hole or creating a boneflap to permit access to the affected area.
• This is a life-saving procedure, and is associatedwith many potential complications, such as:– Severe neurological impairment, infection, persistent
seizures, neurological deficiencies, and/or death.
• A craniotomy is the removal of nonviable braintissue that allows for expansion and/or removalof epidural or subdural hematomas.
• It involves drilling a burr hole or creating a boneflap to permit access to the affected area.
• This is a life-saving procedure, and is associatedwith many potential complications, such as:– Severe neurological impairment, infection, persistent
seizures, neurological deficiencies, and/or death.
• A craniotomy is the removal of nonviable braintissue that allows for expansion and/or removalof epidural or subdural hematomas.
• It involves drilling a burr hole or creating a boneflap to permit access to the affected area.
• This is a life-saving procedure, and is associatedwith many potential complications, such as:– Severe neurological impairment, infection, persistent
seizures, neurological deficiencies, and/or death.
• A craniotomy is the removal of nonviable braintissue that allows for expansion and/or removalof epidural or subdural hematomas.
• It involves drilling a burr hole or creating a boneflap to permit access to the affected area.
• This is a life-saving procedure, and is associatedwith many potential complications, such as:– Severe neurological impairment, infection, persistent
seizures, neurological deficiencies, and/or death.

Craniotomy
• Nursing Actions– Postoperative treatment will depend upon the neurological
status of the client after surgery.– For supratentorial surgery, maintain HOB at least 30° with
body positioning to prevent increased ICP.– For infratentorial craniotomy, keep client flat and on either
side for 24 to 48 hr to prevent pressure on neck incision site.– Hyperventilate the mechanically ventilated client for 24 to 48
hr as prescribed to maintain PaCO2 around 35 mm Hg.– Monitor wound dressing and mark drainage every 1 to 2 hr.– Monitor and maintain wound drain, documenting output
every 8 hr.
• Nursing Actions– Postoperative treatment will depend upon the neurological
status of the client after surgery.– For supratentorial surgery, maintain HOB at least 30° with
body positioning to prevent increased ICP.– For infratentorial craniotomy, keep client flat and on either
side for 24 to 48 hr to prevent pressure on neck incision site.– Hyperventilate the mechanically ventilated client for 24 to 48
hr as prescribed to maintain PaCO2 around 35 mm Hg.– Monitor wound dressing and mark drainage every 1 to 2 hr.– Monitor and maintain wound drain, documenting output
every 8 hr.
• Nursing Actions– Postoperative treatment will depend upon the neurological
status of the client after surgery.– For supratentorial surgery, maintain HOB at least 30° with
body positioning to prevent increased ICP.– For infratentorial craniotomy, keep client flat and on either
side for 24 to 48 hr to prevent pressure on neck incision site.– Hyperventilate the mechanically ventilated client for 24 to 48
hr as prescribed to maintain PaCO2 around 35 mm Hg.– Monitor wound dressing and mark drainage every 1 to 2 hr.– Monitor and maintain wound drain, documenting output
every 8 hr.
• Nursing Actions– Postoperative treatment will depend upon the neurological
status of the client after surgery.– For supratentorial surgery, maintain HOB at least 30° with
body positioning to prevent increased ICP.– For infratentorial craniotomy, keep client flat and on either
side for 24 to 48 hr to prevent pressure on neck incision site.– Hyperventilate the mechanically ventilated client for 24 to 48
hr as prescribed to maintain PaCO2 around 35 mm Hg.– Monitor wound dressing and mark drainage every 1 to 2 hr.– Monitor and maintain wound drain, documenting output
every 8 hr.


• 1. A nurse is caring for a client who was recentlyadmitted to the emergency department followinga head-on motor vehicle crash. The client isunresponsive, has spontaneous respirations of22/min, and a laceration on his forehead that isbleeding. Which of the following is the prioritynursing action at this time?
• A. Keep neck stabilized.• B. Insert nasogastric tube.• C. Monitor pulse and blood pressure frequently.• D. Establish IV access and start fluid replacement.
• 1. A nurse is caring for a client who was recentlyadmitted to the emergency department followinga head-on motor vehicle crash. The client isunresponsive, has spontaneous respirations of22/min, and a laceration on his forehead that isbleeding. Which of the following is the prioritynursing action at this time?
• A. Keep neck stabilized.• B. Insert nasogastric tube.• C. Monitor pulse and blood pressure frequently.• D. Establish IV access and start fluid replacement.

• A. CORRECT: The greatest risk to the client ispermanent damage to the spinal cord if a cervicalinjury does exist. The priority nursingintervention is to keep the neck immobile untildamage to the cervical spine can be ruled out.
• B. INCORRECT: Insertion of a nasogastric tube isnot the priority nursing action at this time.
• C. INCORRECT: Frequent monitoring of pulse andblood pressure is important but not the prioritynursing action at this time.
• D. INCORRECT: Establishing IV access for fluidreplacement is important but not the prioritynursing action at this time.
• A. CORRECT: The greatest risk to the client ispermanent damage to the spinal cord if a cervicalinjury does exist. The priority nursingintervention is to keep the neck immobile untildamage to the cervical spine can be ruled out.
• B. INCORRECT: Insertion of a nasogastric tube isnot the priority nursing action at this time.
• C. INCORRECT: Frequent monitoring of pulse andblood pressure is important but not the prioritynursing action at this time.
• D. INCORRECT: Establishing IV access for fluidreplacement is important but not the prioritynursing action at this time.

• A nurse is caring for a client who has increasedICP and a new prescription for mannitol(Osmitrol). For which of the following adverseeffects should the nurse monitor?
• A. Hyperglycemia• B. Hyponatremia• C. Hypervolemia• D. Oliguria
• A nurse is caring for a client who has increasedICP and a new prescription for mannitol(Osmitrol). For which of the following adverseeffects should the nurse monitor?
• A. Hyperglycemia• B. Hyponatremia• C. Hypervolemia• D. Oliguria

• A. INCORRECT: Hyperglycemia is not an adverseeffect of mannitol.
• B. CORRECT: Mannitol is a powerful osmoticdiuretic, and adverse effects include electrolyteimbalances such as hyponatremia.
• C. INCORRECT: Hypovolemia (not hyper) is anadverse effect of mannitol, an osmotic diuretic,and should be monitored.
• D. INCORRECT: Polyuria (not oliguria) is anadverse of mannitol, an osmotic diuretic, andshould be monitored
• A. INCORRECT: Hyperglycemia is not an adverseeffect of mannitol.
• B. CORRECT: Mannitol is a powerful osmoticdiuretic, and adverse effects include electrolyteimbalances such as hyponatremia.
• C. INCORRECT: Hypovolemia (not hyper) is anadverse effect of mannitol, an osmotic diuretic,and should be monitored.
• D. INCORRECT: Polyuria (not oliguria) is anadverse of mannitol, an osmotic diuretic, andshould be monitored
Seizures• Abnormal, sudden, excessive discharge of electrical
activity within the brain.• Risk Factors
– Genetic predisposition – Absence seizures are more commonin children and tend to occur in families.
– Acute febrile state – particularly among infants and childrenyounger than the age of 2 years
– Head trauma – May be early or late onset (up to 9 months)and incidence is increased when the head trauma includes askull fracture.
– Cerebral edema – especially when it occurs acutely andseizure activity tends to disappear when the edema issuccessfully treated
– Abrupt cessation of antiepileptic drugs (AEDs) – as a reboundactivity
• Abnormal, sudden, excessive discharge of electricalactivity within the brain.
• Risk Factors– Genetic predisposition – Absence seizures are more common
in children and tend to occur in families.– Acute febrile state – particularly among infants and children
younger than the age of 2 years– Head trauma – May be early or late onset (up to 9 months)
and incidence is increased when the head trauma includes askull fracture.
– Cerebral edema – especially when it occurs acutely andseizure activity tends to disappear when the edema issuccessfully treated
– Abrupt cessation of antiepileptic drugs (AEDs) – as a reboundactivity
• Abnormal, sudden, excessive discharge of electricalactivity within the brain.
• Risk Factors– Genetic predisposition – Absence seizures are more common
in children and tend to occur in families.– Acute febrile state – particularly among infants and children
younger than the age of 2 years– Head trauma – May be early or late onset (up to 9 months)
and incidence is increased when the head trauma includes askull fracture.
– Cerebral edema – especially when it occurs acutely andseizure activity tends to disappear when the edema issuccessfully treated
– Abrupt cessation of antiepileptic drugs (AEDs) – as a reboundactivity
• Abnormal, sudden, excessive discharge of electricalactivity within the brain.
• Risk Factors– Genetic predisposition – Absence seizures are more common
in children and tend to occur in families.– Acute febrile state – particularly among infants and children
younger than the age of 2 years– Head trauma – May be early or late onset (up to 9 months)
and incidence is increased when the head trauma includes askull fracture.
– Cerebral edema – especially when it occurs acutely andseizure activity tends to disappear when the edema issuccessfully treated
– Abrupt cessation of antiepileptic drugs (AEDs) – as a reboundactivity

Seizures
• Infection – if intracranial, a result of increased intracranialpressure; if systemic, a result of the persistent febrile state
• Metabolic disorder, Fluid and electrolyte imbalance – a result ofinsufficient or excessive chemicals within the brain (hypoglycemiaor hypo natremia)
• Exposure to toxins –pesticides, carbon monoxide, lead poisoning• Brain tumor – if benign, seizures caused by the increased bulk
associated with the tumor; if malignant, associated with theability of the brain tissue to function
• Hypoxia – results in a decreased oxygen level of the brain.• Acute drug and alcohol withdrawal – dehydration that
accompanies withdrawal, creating a toxic level of the drug in thebody
• Infection – if intracranial, a result of increased intracranialpressure; if systemic, a result of the persistent febrile state
• Metabolic disorder, Fluid and electrolyte imbalance – a result ofinsufficient or excessive chemicals within the brain (hypoglycemiaor hypo natremia)
• Exposure to toxins –pesticides, carbon monoxide, lead poisoning• Brain tumor – if benign, seizures caused by the increased bulk
associated with the tumor; if malignant, associated with theability of the brain tissue to function
• Hypoxia – results in a decreased oxygen level of the brain.• Acute drug and alcohol withdrawal – dehydration that
accompanies withdrawal, creating a toxic level of the drug in thebody
• Infection – if intracranial, a result of increased intracranialpressure; if systemic, a result of the persistent febrile state
• Metabolic disorder, Fluid and electrolyte imbalance – a result ofinsufficient or excessive chemicals within the brain (hypoglycemiaor hypo natremia)
• Exposure to toxins –pesticides, carbon monoxide, lead poisoning• Brain tumor – if benign, seizures caused by the increased bulk
associated with the tumor; if malignant, associated with theability of the brain tissue to function
• Hypoxia – results in a decreased oxygen level of the brain.• Acute drug and alcohol withdrawal – dehydration that
accompanies withdrawal, creating a toxic level of the drug in thebody
• Infection – if intracranial, a result of increased intracranialpressure; if systemic, a result of the persistent febrile state
• Metabolic disorder, Fluid and electrolyte imbalance – a result ofinsufficient or excessive chemicals within the brain (hypoglycemiaor hypo natremia)
• Exposure to toxins –pesticides, carbon monoxide, lead poisoning• Brain tumor – if benign, seizures caused by the increased bulk
associated with the tumor; if malignant, associated with theability of the brain tissue to function
• Hypoxia – results in a decreased oxygen level of the brain.• Acute drug and alcohol withdrawal – dehydration that
accompanies withdrawal, creating a toxic level of the drug in thebody

Generalized seizure• A generalized seizure is also called a tonic-clonic seizure (grand mal
seizure).• It may begin with an aura (alteration in vision, smell, hearing, or
emotional feeling).• A generalized seizure begins for only a few seconds with a tonic
episode (stiffening of muscles) and loss of consciousness.• A 1- to 2-min clonic episode (rhythmic jerking of the extremities)
follows the tonic episode.• Breathing may stop during the tonic phase and become irregular
during the clonic phase.• Cyanosis can accompany breathing irregularities.• Biting of the cheek or tongue can occur during clonic phase.• Incontinence can also accompany a seizure.• During the postictal phase, a period of confusion and sleepiness
follows the seizure.
• A generalized seizure is also called a tonic-clonic seizure (grand malseizure).
• It may begin with an aura (alteration in vision, smell, hearing, oremotional feeling).
• A generalized seizure begins for only a few seconds with a tonicepisode (stiffening of muscles) and loss of consciousness.
• A 1- to 2-min clonic episode (rhythmic jerking of the extremities)follows the tonic episode.
• Breathing may stop during the tonic phase and become irregularduring the clonic phase.
• Cyanosis can accompany breathing irregularities.• Biting of the cheek or tongue can occur during clonic phase.• Incontinence can also accompany a seizure.• During the postictal phase, a period of confusion and sleepiness
follows the seizure.
• A generalized seizure is also called a tonic-clonic seizure (grand malseizure).
• It may begin with an aura (alteration in vision, smell, hearing, oremotional feeling).
• A generalized seizure begins for only a few seconds with a tonicepisode (stiffening of muscles) and loss of consciousness.
• A 1- to 2-min clonic episode (rhythmic jerking of the extremities)follows the tonic episode.
• Breathing may stop during the tonic phase and become irregularduring the clonic phase.
• Cyanosis can accompany breathing irregularities.• Biting of the cheek or tongue can occur during clonic phase.• Incontinence can also accompany a seizure.• During the postictal phase, a period of confusion and sleepiness
follows the seizure.
• A generalized seizure is also called a tonic-clonic seizure (grand malseizure).
• It may begin with an aura (alteration in vision, smell, hearing, oremotional feeling).
• A generalized seizure begins for only a few seconds with a tonicepisode (stiffening of muscles) and loss of consciousness.
• A 1- to 2-min clonic episode (rhythmic jerking of the extremities)follows the tonic episode.
• Breathing may stop during the tonic phase and become irregularduring the clonic phase.
• Cyanosis can accompany breathing irregularities.• Biting of the cheek or tongue can occur during clonic phase.• Incontinence can also accompany a seizure.• During the postictal phase, a period of confusion and sleepiness
follows the seizure.

Generalized seizureTonic seizure Clonic seizure Absence seizure Myoclonic seizure
During a seizure,only the tonic phaseis experienced.
Only the clonicphase is experienced
include unconscious,involuntary behaviorassociated with eyefluttering, smackingof the lips, andpicking at clothescalled automatisms.
consist of briefjerking or stiffeningof the extremities,which may besymmetrical orasymmetrical.
include unconscious,involuntary behaviorassociated with eyefluttering, smackingof the lips, andpicking at clothescalled automatisms.
The seizure usuallylasts 30 seconds toseveral minutes.
The seizure lastsseveral minutes
The seizure consistsof a loss ofconsciousnesslasting a fewseconds.
It lasts for seconds.
A loss ofconsciousnessoccurs.
During this type ofseizure, the musclescontract and relax.
It is associated withblank staring.Common in chidren
Partial or focal/local seizure• Complex partial seizure
– Complex partial seizures have associated automatisms(behaviors that the client is unaware of, such as lipsmacking or picking at clothes).
– The seizure can cause a loss of consciousness for severalminutes.
– Amnesia may occur immediately prior to and after theseizure.
• Simple partial seizures– Consciousness is maintained throughout simple partial
seizures.– Seizure activity may consist of unusual sensations, a sense
of deja vu, autonomic abnormalities, such as changes inheart rate and abnormal flushing, unilateral abnormalextremity movements, pain or offensive smell.
• Complex partial seizure– Complex partial seizures have associated automatisms
(behaviors that the client is unaware of, such as lipsmacking or picking at clothes).
– The seizure can cause a loss of consciousness for severalminutes.
– Amnesia may occur immediately prior to and after theseizure.
• Simple partial seizures– Consciousness is maintained throughout simple partial
seizures.– Seizure activity may consist of unusual sensations, a sense
of deja vu, autonomic abnormalities, such as changes inheart rate and abnormal flushing, unilateral abnormalextremity movements, pain or offensive smell.
• Complex partial seizure– Complex partial seizures have associated automatisms
(behaviors that the client is unaware of, such as lipsmacking or picking at clothes).
– The seizure can cause a loss of consciousness for severalminutes.
– Amnesia may occur immediately prior to and after theseizure.
• Simple partial seizures– Consciousness is maintained throughout simple partial
seizures.– Seizure activity may consist of unusual sensations, a sense
of deja vu, autonomic abnormalities, such as changes inheart rate and abnormal flushing, unilateral abnormalextremity movements, pain or offensive smell.
• Complex partial seizure– Complex partial seizures have associated automatisms
(behaviors that the client is unaware of, such as lipsmacking or picking at clothes).
– The seizure can cause a loss of consciousness for severalminutes.
– Amnesia may occur immediately prior to and after theseizure.
• Simple partial seizures– Consciousness is maintained throughout simple partial
seizures.– Seizure activity may consist of unusual sensations, a sense
of deja vu, autonomic abnormalities, such as changes inheart rate and abnormal flushing, unilateral abnormalextremity movements, pain or offensive smell.

Nursing Care• During a seizure:
– Protect the client’s privacy and the client frominjury (move furniture away, hold head in lap if onthe floor).
– Position client to provide a patent airway.– Be prepared to suction oral secretions.– Turn the client to the side to decrease the risk of
aspiration.– Loosen restrictive clothing.
• During a seizure:– Protect the client’s privacy and the client from
injury (move furniture away, hold head in lap if onthe floor).
– Position client to provide a patent airway.– Be prepared to suction oral secretions.– Turn the client to the side to decrease the risk of
aspiration.– Loosen restrictive clothing.
• During a seizure:– Protect the client’s privacy and the client from
injury (move furniture away, hold head in lap if onthe floor).
– Position client to provide a patent airway.– Be prepared to suction oral secretions.– Turn the client to the side to decrease the risk of
aspiration.– Loosen restrictive clothing.
• During a seizure:– Protect the client’s privacy and the client from
injury (move furniture away, hold head in lap if onthe floor).
– Position client to provide a patent airway.– Be prepared to suction oral secretions.– Turn the client to the side to decrease the risk of
aspiration.– Loosen restrictive clothing.

Nursing Care• During a seizure:
– Do not attempt to restrain the client.– Do not attempt to open jaw or insert airway
during seizure activity (may damage teeth, lips,and tongue). Do not use padded tongue blades.
– Document onset and duration of seizure andclient findings/observations prior to, during, andfollowing the seizure (level of consciousness,apnea, cyanosis, motor activity, incontinence).
• During a seizure:– Do not attempt to restrain the client.– Do not attempt to open jaw or insert airway
during seizure activity (may damage teeth, lips,and tongue). Do not use padded tongue blades.
– Document onset and duration of seizure andclient findings/observations prior to, during, andfollowing the seizure (level of consciousness,apnea, cyanosis, motor activity, incontinence).
• During a seizure:– Do not attempt to restrain the client.– Do not attempt to open jaw or insert airway
during seizure activity (may damage teeth, lips,and tongue). Do not use padded tongue blades.
– Document onset and duration of seizure andclient findings/observations prior to, during, andfollowing the seizure (level of consciousness,apnea, cyanosis, motor activity, incontinence).
• During a seizure:– Do not attempt to restrain the client.– Do not attempt to open jaw or insert airway
during seizure activity (may damage teeth, lips,and tongue). Do not use padded tongue blades.
– Document onset and duration of seizure andclient findings/observations prior to, during, andfollowing the seizure (level of consciousness,apnea, cyanosis, motor activity, incontinence).
Nursing Care• Post seizure:
– The postictal phase of the seizure episode.– Maintain the client in a side-lying position to
prevent aspiration and to facilitate drainage of oralsecretions.
– Check vital signs.– Assess for injuries.– Perform neurological checks.– Allow the client to rest if necessary.
• Post seizure:– The postictal phase of the seizure episode.– Maintain the client in a side-lying position to
prevent aspiration and to facilitate drainage of oralsecretions.
– Check vital signs.– Assess for injuries.– Perform neurological checks.– Allow the client to rest if necessary.
• Post seizure:– The postictal phase of the seizure episode.– Maintain the client in a side-lying position to
prevent aspiration and to facilitate drainage of oralsecretions.
– Check vital signs.– Assess for injuries.– Perform neurological checks.– Allow the client to rest if necessary.
• Post seizure:– The postictal phase of the seizure episode.– Maintain the client in a side-lying position to
prevent aspiration and to facilitate drainage of oralsecretions.
– Check vital signs.– Assess for injuries.– Perform neurological checks.– Allow the client to rest if necessary.

Nursing Care• Post seizure:
– Reorient and calm the client (may be agitated orconfused).
– Institute seizure precautions including placing thebed in the lowest position and padding the siderails to prevent future injury.
– Determine if client experienced an aura, which canpossibly indicate the origin of seizure in the brain.
– Try to determine possible trigger (fatigue).
• Post seizure:– Reorient and calm the client (may be agitated or
confused).– Institute seizure precautions including placing the
bed in the lowest position and padding the siderails to prevent future injury.
– Determine if client experienced an aura, which canpossibly indicate the origin of seizure in the brain.
– Try to determine possible trigger (fatigue).
• Post seizure:– Reorient and calm the client (may be agitated or
confused).– Institute seizure precautions including placing the
bed in the lowest position and padding the siderails to prevent future injury.
– Determine if client experienced an aura, which canpossibly indicate the origin of seizure in the brain.
– Try to determine possible trigger (fatigue).
• Post seizure:– Reorient and calm the client (may be agitated or
confused).– Institute seizure precautions including placing the
bed in the lowest position and padding the siderails to prevent future injury.
– Determine if client experienced an aura, which canpossibly indicate the origin of seizure in the brain.
– Try to determine possible trigger (fatigue).

Status Epilepticus• Prolonged seizure activity occurring over a 30-min time
frame.• Complications due to decreased oxygen levels, inability
of the brain to return to normal functioning, andcontinued assault on neuronal tissue.
• The usual causes are withdrawal from drugs or alcohol,sudden withdrawal from antiepileptic medication, headinjury, cerebral edema, infection, and fever.
• Nursing Actions– Maintain an airway, provide oxygen, establish IV access,
perform ECG monitoring, and monitor pulse oximetry andABG results.
– Give medications.
• Prolonged seizure activity occurring over a 30-min timeframe.
• Complications due to decreased oxygen levels, inabilityof the brain to return to normal functioning, andcontinued assault on neuronal tissue.
• The usual causes are withdrawal from drugs or alcohol,sudden withdrawal from antiepileptic medication, headinjury, cerebral edema, infection, and fever.
• Nursing Actions– Maintain an airway, provide oxygen, establish IV access,
perform ECG monitoring, and monitor pulse oximetry andABG results.
– Give medications.
• Prolonged seizure activity occurring over a 30-min timeframe.
• Complications due to decreased oxygen levels, inabilityof the brain to return to normal functioning, andcontinued assault on neuronal tissue.
• The usual causes are withdrawal from drugs or alcohol,sudden withdrawal from antiepileptic medication, headinjury, cerebral edema, infection, and fever.
• Nursing Actions– Maintain an airway, provide oxygen, establish IV access,
perform ECG monitoring, and monitor pulse oximetry andABG results.
– Give medications.
• Prolonged seizure activity occurring over a 30-min timeframe.
• Complications due to decreased oxygen levels, inabilityof the brain to return to normal functioning, andcontinued assault on neuronal tissue.
• The usual causes are withdrawal from drugs or alcohol,sudden withdrawal from antiepileptic medication, headinjury, cerebral edema, infection, and fever.
• Nursing Actions– Maintain an airway, provide oxygen, establish IV access,
perform ECG monitoring, and monitor pulse oximetry andABG results.
– Give medications.

• 1. A nurse is assessing a client who has a seizuredisorder. The client reports he thinks he is about tohave a seizure. Which of the following actions shouldthe nurse implement? (Select all that apply.)
• A. Provide privacy.• B. Ease the client to the floor if standing.• C. Move furniture away from the client.• D. Loosen the client’s clothing.• E. Protect the client’s head with padding.• F. Restrain the client.
• 1. A nurse is assessing a client who has a seizuredisorder. The client reports he thinks he is about tohave a seizure. Which of the following actions shouldthe nurse implement? (Select all that apply.)
• A. Provide privacy.• B. Ease the client to the floor if standing.• C. Move furniture away from the client.• D. Loosen the client’s clothing.• E. Protect the client’s head with padding.• F. Restrain the client.

• A. Correct: The nurse should implement privacy tominimize the client’s embarrassment.
• B. Correct: The nurse should ease the client to the floor toprevent falling.
• C. Correct: The nurse should move the furniture away fromthe client to prevent injury.
• D. Correct: The nurse should loosen the client’s clothing tominimize restriction of movement.
• E. Correct: The nurse should protect the client’s head frominjury by placing the client’s head in her lap or using apillow or blanket under the head during a seizure.
• F. Incorrect: The nurse should not restrain the client, whichmay cause an injury or moreseizure activity.
• A. Correct: The nurse should implement privacy tominimize the client’s embarrassment.
• B. Correct: The nurse should ease the client to the floor toprevent falling.
• C. Correct: The nurse should move the furniture away fromthe client to prevent injury.
• D. Correct: The nurse should loosen the client’s clothing tominimize restriction of movement.
• E. Correct: The nurse should protect the client’s head frominjury by placing the client’s head in her lap or using apillow or blanket under the head during a seizure.
• F. Incorrect: The nurse should not restrain the client, whichmay cause an injury or moreseizure activity.
• A nurse is caring for a client who justexperienced a generalized seizure. Which ofthe following actions should the nurseperform first?
• A. Keep the client in a side-lying position.• B. Monitor the client’s vital signs.• C. Reorient the client to the environment.• D. Check the client for injuries.
• A nurse is caring for a client who justexperienced a generalized seizure. Which ofthe following actions should the nurseperform first?
• A. Keep the client in a side-lying position.• B. Monitor the client’s vital signs.• C. Reorient the client to the environment.• D. Check the client for injuries.

• A. Correct: The greatest risk to the client is aspirationduring the postictal phase. Therefore, the priorityintervention is to keep the client in a side-lying position sosecretions can drain from the mouth.
• B. Incorrect: Monitoring vital signs to determine thestability of the client is important, but it is not the prioritynursing action.
• C. Incorrect: Reorienting the client to the environmentbecause the client may feel confused after a seizure isimportant, but it is not the priority nursing action.
• D. Incorrect: Checking the client for injuries that may ofoccurred from involuntary movement during the seizure isimportant, but it is not the priority nursing action.
• A. Correct: The greatest risk to the client is aspirationduring the postictal phase. Therefore, the priorityintervention is to keep the client in a side-lying position sosecretions can drain from the mouth.
• B. Incorrect: Monitoring vital signs to determine thestability of the client is important, but it is not the prioritynursing action.
• C. Incorrect: Reorienting the client to the environmentbecause the client may feel confused after a seizure isimportant, but it is not the priority nursing action.
• D. Incorrect: Checking the client for injuries that may ofoccurred from involuntary movement during the seizure isimportant, but it is not the priority nursing action.

Cerebral Aneurysm– Description
• Dilation of walls of weakened cerebral artery– Assessment
• Headache• Visual changes• Hemiparesis
– Interventions• Maintain a patent airway• Initiate seizure precautions• Prepare for surgery if indicated• Rupture of a cerebral aneurysm usually results in
increased intracranial pressure (ICP). The first sign ofpressure in the brain is a change in the level ofconsciousness.
Cerebral Aneurysm– Description
• Dilation of walls of weakened cerebral artery– Assessment
• Headache• Visual changes• Hemiparesis
– Interventions• Maintain a patent airway• Initiate seizure precautions• Prepare for surgery if indicated• Rupture of a cerebral aneurysm usually results in
increased intracranial pressure (ICP). The first sign ofpressure in the brain is a change in the level ofconsciousness.
Cerebral Aneurysm– Description
• Dilation of walls of weakened cerebral artery– Assessment
• Headache• Visual changes• Hemiparesis
– Interventions• Maintain a patent airway• Initiate seizure precautions• Prepare for surgery if indicated• Rupture of a cerebral aneurysm usually results in
increased intracranial pressure (ICP). The first sign ofpressure in the brain is a change in the level ofconsciousness.
Cerebral Aneurysm– Description
• Dilation of walls of weakened cerebral artery– Assessment
• Headache• Visual changes• Hemiparesis
– Interventions• Maintain a patent airway• Initiate seizure precautions• Prepare for surgery if indicated• Rupture of a cerebral aneurysm usually results in
increased intracranial pressure (ICP). The first sign ofpressure in the brain is a change in the level ofconsciousness.


Stroke (Brain Attack)– Description
• Sudden, focal neurological deficit– Risk factors : Cerebral aneurysm, AV , DM, HTN,
Obesity, Atherosclerosis, Hyperlipidemia,Hypercoagulability, Atrial fibrillation, Use of oralcontraceptives, Smoking, Cocaine use
– Assessment• Depends on area of brain affected• Airway patency is priority
Stroke (Brain Attack)– Description
• Sudden, focal neurological deficit– Risk factors : Cerebral aneurysm, AV , DM, HTN,
Obesity, Atherosclerosis, Hyperlipidemia,Hypercoagulability, Atrial fibrillation, Use of oralcontraceptives, Smoking, Cocaine use
– Assessment• Depends on area of brain affected• Airway patency is priority
Stroke (Brain Attack)– Description
• Sudden, focal neurological deficit– Risk factors : Cerebral aneurysm, AV , DM, HTN,
Obesity, Atherosclerosis, Hyperlipidemia,Hypercoagulability, Atrial fibrillation, Use of oralcontraceptives, Smoking, Cocaine use
– Assessment• Depends on area of brain affected• Airway patency is priority
Stroke (Brain Attack)– Description
• Sudden, focal neurological deficit– Risk factors : Cerebral aneurysm, AV , DM, HTN,
Obesity, Atherosclerosis, Hyperlipidemia,Hypercoagulability, Atrial fibrillation, Use of oralcontraceptives, Smoking, Cocaine use
– Assessment• Depends on area of brain affected• Airway patency is priority


Thrombotic -Ischemic Embolic - Ischemic Hemorrhagic
Blood clot Emboli bleeding
Most common, atheroticplaque
Thrombolytic enzyme (rtpa) ishelpful
Poor prognosis
HTN, DM Rheumatic heart disease(younger),
Atherosclerosis (older)
Occur secondary to aruptured artery or
aneurysm, HTN
TIA common Warning signs are lesscommon
Sudden onset of symptoms
Symptoms over severalhours to days
Sudden, rapid occurrence ofsevere clinical manifestations.(neurologic deficits or a lossof consciousness instantly
occur)
Fifty percent of the deathsoccur within the first 48
hours.

Left Sided Stroke• The left cerebral hemisphere is responsible for language,
mathematics skills, and analytic thinking.• Symptoms consistent with a left-hemispheric stroke include
the following:– Expressive and receptive aphasia (inability to speak and understand
language respectively)– Agnosia (unable to recognize familiar objects)– Alexia (reading difficulty)– Agraphia (writing difficulty)– Right extremity hemiplegia (paralysis) or hemiparesis (weakness)– Slow, cautious behavior– Depression, anger, and quick to become frustrated– Visual changes, such as hemianopsia (loss of visual field in one or
both eyes)
• The left cerebral hemisphere is responsible for language,mathematics skills, and analytic thinking.
• Symptoms consistent with a left-hemispheric stroke includethe following:– Expressive and receptive aphasia (inability to speak and understand
language respectively)– Agnosia (unable to recognize familiar objects)– Alexia (reading difficulty)– Agraphia (writing difficulty)– Right extremity hemiplegia (paralysis) or hemiparesis (weakness)– Slow, cautious behavior– Depression, anger, and quick to become frustrated– Visual changes, such as hemianopsia (loss of visual field in one or
both eyes)
• The left cerebral hemisphere is responsible for language,mathematics skills, and analytic thinking.
• Symptoms consistent with a left-hemispheric stroke includethe following:– Expressive and receptive aphasia (inability to speak and understand
language respectively)– Agnosia (unable to recognize familiar objects)– Alexia (reading difficulty)– Agraphia (writing difficulty)– Right extremity hemiplegia (paralysis) or hemiparesis (weakness)– Slow, cautious behavior– Depression, anger, and quick to become frustrated– Visual changes, such as hemianopsia (loss of visual field in one or
both eyes)
• The left cerebral hemisphere is responsible for language,mathematics skills, and analytic thinking.
• Symptoms consistent with a left-hemispheric stroke includethe following:– Expressive and receptive aphasia (inability to speak and understand
language respectively)– Agnosia (unable to recognize familiar objects)– Alexia (reading difficulty)– Agraphia (writing difficulty)– Right extremity hemiplegia (paralysis) or hemiparesis (weakness)– Slow, cautious behavior– Depression, anger, and quick to become frustrated– Visual changes, such as hemianopsia (loss of visual field in one or
both eyes)

• Aphasia:- Occur when stroke damages dominant hemisphereof the brain and affects language.– Receptive : Patient unable to understand language in its written
or spoken form.– Expressive : loss of the ability to produce language.– Global : difficulty with both speaking and understanding speech
– Dysphasia refers to impaired ability to communicate.– Non fluent - Minimal speech activity with slow speech– Fluent -Speech is present but contains little meaningful
communication– Many patients experience dysarthria.
– Disturbance in the muscular control of speech– Pronunciation– Articulation– Phonation
• Aphasia:- Occur when stroke damages dominant hemisphereof the brain and affects language.– Receptive : Patient unable to understand language in its written
or spoken form.– Expressive : loss of the ability to produce language.– Global : difficulty with both speaking and understanding speech
– Dysphasia refers to impaired ability to communicate.– Non fluent - Minimal speech activity with slow speech– Fluent -Speech is present but contains little meaningful
communication– Many patients experience dysarthria.
– Disturbance in the muscular control of speech– Pronunciation– Articulation– Phonation
• Aphasia:- Occur when stroke damages dominant hemisphereof the brain and affects language.– Receptive : Patient unable to understand language in its written
or spoken form.– Expressive : loss of the ability to produce language.– Global : difficulty with both speaking and understanding speech
– Dysphasia refers to impaired ability to communicate.– Non fluent - Minimal speech activity with slow speech– Fluent -Speech is present but contains little meaningful
communication– Many patients experience dysarthria.
– Disturbance in the muscular control of speech– Pronunciation– Articulation– Phonation
• Aphasia:- Occur when stroke damages dominant hemisphereof the brain and affects language.– Receptive : Patient unable to understand language in its written
or spoken form.– Expressive : loss of the ability to produce language.– Global : difficulty with both speaking and understanding speech
– Dysphasia refers to impaired ability to communicate.– Non fluent - Minimal speech activity with slow speech– Fluent -Speech is present but contains little meaningful
communication– Many patients experience dysarthria.
– Disturbance in the muscular control of speech– Pronunciation– Articulation– Phonation


Right Sided Stroke• The right cerebral hemisphere is responsible for
visual and spatial awareness and proprioception.– Altered perception of deficits (overestimation of
abilities)– One-sided neglect syndrome (ignore left side of the
body – cannot see, feel, or move affected side, soclient unaware of its existence). Can occur with left-hemispheric strokes, but is more common with right-hemispheric strokes.
– Loss of depth perception– Poor impulse control and judgment– Left hemiplegia or hemiparesis– Visual changes, such as hemianopsia
• The right cerebral hemisphere is responsible forvisual and spatial awareness and proprioception.– Altered perception of deficits (overestimation of
abilities)– One-sided neglect syndrome (ignore left side of the
body – cannot see, feel, or move affected side, soclient unaware of its existence). Can occur with left-hemispheric strokes, but is more common with right-hemispheric strokes.
– Loss of depth perception– Poor impulse control and judgment– Left hemiplegia or hemiparesis– Visual changes, such as hemianopsia
• The right cerebral hemisphere is responsible forvisual and spatial awareness and proprioception.– Altered perception of deficits (overestimation of
abilities)– One-sided neglect syndrome (ignore left side of the
body – cannot see, feel, or move affected side, soclient unaware of its existence). Can occur with left-hemispheric strokes, but is more common with right-hemispheric strokes.
– Loss of depth perception– Poor impulse control and judgment– Left hemiplegia or hemiparesis– Visual changes, such as hemianopsia
• The right cerebral hemisphere is responsible forvisual and spatial awareness and proprioception.– Altered perception of deficits (overestimation of
abilities)– One-sided neglect syndrome (ignore left side of the
body – cannot see, feel, or move affected side, soclient unaware of its existence). Can occur with left-hemispheric strokes, but is more common with right-hemispheric strokes.
– Loss of depth perception– Poor impulse control and judgment– Left hemiplegia or hemiparesis– Visual changes, such as hemianopsia

Nursing Care• Monitor the client’s vital signs every l to 2 hr.• Notify the provider immediately if the client’s blood
pressure exceeds a systolic greater than 180 mm Hg ora diastolic greater than 110 mm Hg. This can indicatethe client is experiencing an ischemic stroke.
• Monitor the client’s temperature. A fever can cause anincrease in intracranial pressure.
• Provide oxygen therapy to maintain the client’s oxygensaturation level greater than 92%, or if the client’s levelof consciousness is decreased.
• Place the client on a cardiac monitor to detectarrhythmias.
• Monitor the client’s vital signs every l to 2 hr.• Notify the provider immediately if the client’s blood
pressure exceeds a systolic greater than 180 mm Hg ora diastolic greater than 110 mm Hg. This can indicatethe client is experiencing an ischemic stroke.
• Monitor the client’s temperature. A fever can cause anincrease in intracranial pressure.
• Provide oxygen therapy to maintain the client’s oxygensaturation level greater than 92%, or if the client’s levelof consciousness is decreased.
• Place the client on a cardiac monitor to detectarrhythmias.
• Monitor the client’s vital signs every l to 2 hr.• Notify the provider immediately if the client’s blood
pressure exceeds a systolic greater than 180 mm Hg ora diastolic greater than 110 mm Hg. This can indicatethe client is experiencing an ischemic stroke.
• Monitor the client’s temperature. A fever can cause anincrease in intracranial pressure.
• Provide oxygen therapy to maintain the client’s oxygensaturation level greater than 92%, or if the client’s levelof consciousness is decreased.
• Place the client on a cardiac monitor to detectarrhythmias.
• Monitor the client’s vital signs every l to 2 hr.• Notify the provider immediately if the client’s blood
pressure exceeds a systolic greater than 180 mm Hg ora diastolic greater than 110 mm Hg. This can indicatethe client is experiencing an ischemic stroke.
• Monitor the client’s temperature. A fever can cause anincrease in intracranial pressure.
• Provide oxygen therapy to maintain the client’s oxygensaturation level greater than 92%, or if the client’s levelof consciousness is decreased.
• Place the client on a cardiac monitor to detectarrhythmias.

Nursing Care• Conduct a cardiac assessment, and auscultate the
client’s apical heart rate to detect murmurs orirregularity.
• Monitor for changes in the client’s level ofconsciousness (increased ICP sign).
• Monitor vital signs, electrocardiogram.• Elevate the client’s head of the bed approximately 30°
to reduce ICP and to promote venous drainage.• Avoid extreme flexion or extension of the neck, and
maintain the client’s head in the midline neutralposition.
• Institute seizure precautions.• Assist with the client’s communication skills if his
speech is impaired.
• Conduct a cardiac assessment, and auscultate theclient’s apical heart rate to detect murmurs orirregularity.
• Monitor for changes in the client’s level ofconsciousness (increased ICP sign).
• Monitor vital signs, electrocardiogram.• Elevate the client’s head of the bed approximately 30°
to reduce ICP and to promote venous drainage.• Avoid extreme flexion or extension of the neck, and
maintain the client’s head in the midline neutralposition.
• Institute seizure precautions.• Assist with the client’s communication skills if his
speech is impaired.
• Conduct a cardiac assessment, and auscultate theclient’s apical heart rate to detect murmurs orirregularity.
• Monitor for changes in the client’s level ofconsciousness (increased ICP sign).
• Monitor vital signs, electrocardiogram.• Elevate the client’s head of the bed approximately 30°
to reduce ICP and to promote venous drainage.• Avoid extreme flexion or extension of the neck, and
maintain the client’s head in the midline neutralposition.
• Institute seizure precautions.• Assist with the client’s communication skills if his
speech is impaired.
• Conduct a cardiac assessment, and auscultate theclient’s apical heart rate to detect murmurs orirregularity.
• Monitor for changes in the client’s level ofconsciousness (increased ICP sign).
• Monitor vital signs, electrocardiogram.• Elevate the client’s head of the bed approximately 30°
to reduce ICP and to promote venous drainage.• Avoid extreme flexion or extension of the neck, and
maintain the client’s head in the midline neutralposition.
• Institute seizure precautions.• Assist with the client’s communication skills if his
speech is impaired.

Nursing Care• Assist with safe feeding.
– Assess swallowing and gag reflexes before feeding.– Speech therapy may request a swallowing study that can
involve swallowing a barium substrate and radiography ofthe peristaltic activity of the esophagus.
– If a swallowing deficit is identified, the client’s liquids mayneed to be thickened with a commercial thickener to avoidaspiration.
– Have the client eat in an upright position and swallow withthe head and neck flexed slightly forward.
– Place food in the back of the mouth on the unaffectedside.
– Have suction on standby.– Maintain a distraction-free environment during meals.
• Assist with safe feeding.– Assess swallowing and gag reflexes before feeding.– Speech therapy may request a swallowing study that can
involve swallowing a barium substrate and radiography ofthe peristaltic activity of the esophagus.
– If a swallowing deficit is identified, the client’s liquids mayneed to be thickened with a commercial thickener to avoidaspiration.
– Have the client eat in an upright position and swallow withthe head and neck flexed slightly forward.
– Place food in the back of the mouth on the unaffectedside.
– Have suction on standby.– Maintain a distraction-free environment during meals.
• Assist with safe feeding.– Assess swallowing and gag reflexes before feeding.– Speech therapy may request a swallowing study that can
involve swallowing a barium substrate and radiography ofthe peristaltic activity of the esophagus.
– If a swallowing deficit is identified, the client’s liquids mayneed to be thickened with a commercial thickener to avoidaspiration.
– Have the client eat in an upright position and swallow withthe head and neck flexed slightly forward.
– Place food in the back of the mouth on the unaffectedside.
– Have suction on standby.– Maintain a distraction-free environment during meals.
• Assist with safe feeding.– Assess swallowing and gag reflexes before feeding.– Speech therapy may request a swallowing study that can
involve swallowing a barium substrate and radiography ofthe peristaltic activity of the esophagus.
– If a swallowing deficit is identified, the client’s liquids mayneed to be thickened with a commercial thickener to avoidaspiration.
– Have the client eat in an upright position and swallow withthe head and neck flexed slightly forward.
– Place food in the back of the mouth on the unaffectedside.
– Have suction on standby.– Maintain a distraction-free environment during meals.

Nursing Care• Prevent complications of immobility.
– Encourage passive ROM every 2 hr to the affectedextremities and active ROM every 2 hr to theunaffected extremities
– SCD, TED hose, PT– Elevate the affected extremities to promote venous
return and reduce swelling.• Maintain skin integrity.
– Reposition the client frequently and use padding.– Monitor bony prominences, paying particular
attention to the affected extremities.– Care of unilateral neglect.
• Prevent complications of immobility.– Encourage passive ROM every 2 hr to the affected
extremities and active ROM every 2 hr to theunaffected extremities
– SCD, TED hose, PT– Elevate the affected extremities to promote venous
return and reduce swelling.• Maintain skin integrity.
– Reposition the client frequently and use padding.– Monitor bony prominences, paying particular
attention to the affected extremities.– Care of unilateral neglect.
• Prevent complications of immobility.– Encourage passive ROM every 2 hr to the affected
extremities and active ROM every 2 hr to theunaffected extremities
– SCD, TED hose, PT– Elevate the affected extremities to promote venous
return and reduce swelling.• Maintain skin integrity.
– Reposition the client frequently and use padding.– Monitor bony prominences, paying particular
attention to the affected extremities.– Care of unilateral neglect.
• Prevent complications of immobility.– Encourage passive ROM every 2 hr to the affected
extremities and active ROM every 2 hr to theunaffected extremities
– SCD, TED hose, PT– Elevate the affected extremities to promote venous
return and reduce swelling.• Maintain skin integrity.
– Reposition the client frequently and use padding.– Monitor bony prominences, paying particular
attention to the affected extremities.– Care of unilateral neglect.

Unilateral neglect• Unilateral neglect is the loss of awareness of the side
affected by the stroke. The client cannot see, feel, or movethe affected side of his body; therefore, he forgets that itexists.– Observe the client’s affected extremities for injury (bruises and
abrasions of the affected hand and arm, hyperflexion of the footfrom it falling off of the wheelchair during transport).
– Apply an arm sling if the client is unable to remember to care forthe affected extremity.
– Ensure the foot rest is on the wheelchair and an ankle brace ison the affected foot.
– Instruct the client to dress the affected side first.– Teach the client how to care for the affected side.– Use the unaffected hand to pull the affected extremity to
midline and out of danger from the wheel of the wheelchair orfrom hitting or smashing it against a doorway.
– Teach the client to look over the affected side periodically.
• Unilateral neglect is the loss of awareness of the sideaffected by the stroke. The client cannot see, feel, or movethe affected side of his body; therefore, he forgets that itexists.– Observe the client’s affected extremities for injury (bruises and
abrasions of the affected hand and arm, hyperflexion of the footfrom it falling off of the wheelchair during transport).
– Apply an arm sling if the client is unable to remember to care forthe affected extremity.
– Ensure the foot rest is on the wheelchair and an ankle brace ison the affected foot.
– Instruct the client to dress the affected side first.– Teach the client how to care for the affected side.– Use the unaffected hand to pull the affected extremity to
midline and out of danger from the wheel of the wheelchair orfrom hitting or smashing it against a doorway.
– Teach the client to look over the affected side periodically.
• Unilateral neglect is the loss of awareness of the sideaffected by the stroke. The client cannot see, feel, or movethe affected side of his body; therefore, he forgets that itexists.– Observe the client’s affected extremities for injury (bruises and
abrasions of the affected hand and arm, hyperflexion of the footfrom it falling off of the wheelchair during transport).
– Apply an arm sling if the client is unable to remember to care forthe affected extremity.
– Ensure the foot rest is on the wheelchair and an ankle brace ison the affected foot.
– Instruct the client to dress the affected side first.– Teach the client how to care for the affected side.– Use the unaffected hand to pull the affected extremity to
midline and out of danger from the wheel of the wheelchair orfrom hitting or smashing it against a doorway.
– Teach the client to look over the affected side periodically.
• Unilateral neglect is the loss of awareness of the sideaffected by the stroke. The client cannot see, feel, or movethe affected side of his body; therefore, he forgets that itexists.– Observe the client’s affected extremities for injury (bruises and
abrasions of the affected hand and arm, hyperflexion of the footfrom it falling off of the wheelchair during transport).
– Apply an arm sling if the client is unable to remember to care forthe affected extremity.
– Ensure the foot rest is on the wheelchair and an ankle brace ison the affected foot.
– Instruct the client to dress the affected side first.– Teach the client how to care for the affected side.– Use the unaffected hand to pull the affected extremity to
midline and out of danger from the wheel of the wheelchair orfrom hitting or smashing it against a doorway.
– Teach the client to look over the affected side periodically.

Nursing Care• Maintain a safe environment to reduce the risk of falls.
– Assistive devices should be used during transfers, such astransfer belts and sliding boards.
– Impaired balance : Leaning towards affected side whilesitting – provide support.
– Shoulder subluxation - painful dislocation of the shoulderfrom its socket due to weight of unused arm. Use arm slingor pillows.
• Client with homonomous hemianopsia (loss of thesame visual field in both eyes)– instruct to use a scanning technique (turning head from
the direction of the unaffected side to the affected side)when eating and ambulating.
• Provide assistance with ADLs as needed.
• Maintain a safe environment to reduce the risk of falls.– Assistive devices should be used during transfers, such as
transfer belts and sliding boards.– Impaired balance : Leaning towards affected side while
sitting – provide support.– Shoulder subluxation - painful dislocation of the shoulder
from its socket due to weight of unused arm. Use arm slingor pillows.
• Client with homonomous hemianopsia (loss of thesame visual field in both eyes)– instruct to use a scanning technique (turning head from
the direction of the unaffected side to the affected side)when eating and ambulating.
• Provide assistance with ADLs as needed.
• Maintain a safe environment to reduce the risk of falls.– Assistive devices should be used during transfers, such as
transfer belts and sliding boards.– Impaired balance : Leaning towards affected side while
sitting – provide support.– Shoulder subluxation - painful dislocation of the shoulder
from its socket due to weight of unused arm. Use arm slingor pillows.
• Client with homonomous hemianopsia (loss of thesame visual field in both eyes)– instruct to use a scanning technique (turning head from
the direction of the unaffected side to the affected side)when eating and ambulating.
• Provide assistance with ADLs as needed.
• Maintain a safe environment to reduce the risk of falls.– Assistive devices should be used during transfers, such as
transfer belts and sliding boards.– Impaired balance : Leaning towards affected side while
sitting – provide support.– Shoulder subluxation - painful dislocation of the shoulder
from its socket due to weight of unused arm. Use arm slingor pillows.
• Client with homonomous hemianopsia (loss of thesame visual field in both eyes)– instruct to use a scanning technique (turning head from
the direction of the unaffected side to the affected side)when eating and ambulating.
• Provide assistance with ADLs as needed.

Medications• Anticoagulants (heparin sodium, enoxaparin [Lovenox], warfarin
[Coumadin])– Use of anticoagulants is controversial and not recommended due to
the high risk of intracerebral bleeding.• Antiplatelets (aspirin)
– Low-dose aspirin is given within 24 to 48 hr following a stroke toprevent further clot formation.
– Other antiplatelets, such as clopidogrel (Plavix), are notrecommended.
• Thrombolytic medications reteplase recombinant (rtPA [Retavase])– Give within 4.5 hours of the initial symptoms.
• Antiepileptic medications (phenytoin [Dilantin], gabapentin[Neurontin])– These medications are not commonly given following a stroke unless
the client develops seizures.– Gabapentin can be given for paresthetic pain in an affected extremity.
• Anticoagulants (heparin sodium, enoxaparin [Lovenox], warfarin[Coumadin])– Use of anticoagulants is controversial and not recommended due to
the high risk of intracerebral bleeding.• Antiplatelets (aspirin)
– Low-dose aspirin is given within 24 to 48 hr following a stroke toprevent further clot formation.
– Other antiplatelets, such as clopidogrel (Plavix), are notrecommended.
• Thrombolytic medications reteplase recombinant (rtPA [Retavase])– Give within 4.5 hours of the initial symptoms.
• Antiepileptic medications (phenytoin [Dilantin], gabapentin[Neurontin])– These medications are not commonly given following a stroke unless
the client develops seizures.– Gabapentin can be given for paresthetic pain in an affected extremity.
• Anticoagulants (heparin sodium, enoxaparin [Lovenox], warfarin[Coumadin])– Use of anticoagulants is controversial and not recommended due to
the high risk of intracerebral bleeding.• Antiplatelets (aspirin)
– Low-dose aspirin is given within 24 to 48 hr following a stroke toprevent further clot formation.
– Other antiplatelets, such as clopidogrel (Plavix), are notrecommended.
• Thrombolytic medications reteplase recombinant (rtPA [Retavase])– Give within 4.5 hours of the initial symptoms.
• Antiepileptic medications (phenytoin [Dilantin], gabapentin[Neurontin])– These medications are not commonly given following a stroke unless
the client develops seizures.– Gabapentin can be given for paresthetic pain in an affected extremity.
• Anticoagulants (heparin sodium, enoxaparin [Lovenox], warfarin[Coumadin])– Use of anticoagulants is controversial and not recommended due to
the high risk of intracerebral bleeding.• Antiplatelets (aspirin)
– Low-dose aspirin is given within 24 to 48 hr following a stroke toprevent further clot formation.
– Other antiplatelets, such as clopidogrel (Plavix), are notrecommended.
• Thrombolytic medications reteplase recombinant (rtPA [Retavase])– Give within 4.5 hours of the initial symptoms.
• Antiepileptic medications (phenytoin [Dilantin], gabapentin[Neurontin])– These medications are not commonly given following a stroke unless
the client develops seizures.– Gabapentin can be given for paresthetic pain in an affected extremity.

• A nurse is caring for a client who has experienceda right-hemispheric stroke. Which of thefollowing are expected findings? (Select all thatapply.)
• A. Impulse control difficulty• B. Left hemiplegia• C. Loss of depth perception• D. Aphasia• E. Lack of awareness
• A nurse is caring for a client who has experienceda right-hemispheric stroke. Which of thefollowing are expected findings? (Select all thatapply.)
• A. Impulse control difficulty• B. Left hemiplegia• C. Loss of depth perception• D. Aphasia• E. Lack of awareness

• A. Correct: A client who has experienced a right-hemispheric stroke will exhibit impulse control difficulty,such as the urgency to use the restroom.
• B. Correct: A client who has experienced a right-hemispheric stroke will exhibit left-sided hemiplegia.
• C. Correct: A client who has experienced a right-hemispheric stroke will experience a loss in depthperception.
• D. Incorrect: A client who has experienced a left-hemispheric stroke will experience aphasia.
• E. Correct: A client who has experienced a right-hemispheric stroke will demonstrate a lack of awareness ofsurroundings.
• A. Correct: A client who has experienced a right-hemispheric stroke will exhibit impulse control difficulty,such as the urgency to use the restroom.
• B. Correct: A client who has experienced a right-hemispheric stroke will exhibit left-sided hemiplegia.
• C. Correct: A client who has experienced a right-hemispheric stroke will experience a loss in depthperception.
• D. Incorrect: A client who has experienced a left-hemispheric stroke will experience aphasia.
• E. Correct: A client who has experienced a right-hemispheric stroke will demonstrate a lack of awareness ofsurroundings.

• A nurse is caring for a client who has lefthomonymous hemianopsia. Which of thefollowing is an appropriate nursing intervention?
• A. Teach the client to scan to the right to seeobjects on the right side of her body.
• B. Place the client’s bedside table on the rightside of the bed.
• C. Orient the client to the food on her plate usingthe clock method.
• D. Place the client’s wheelchair on her left side.
• A nurse is caring for a client who has lefthomonymous hemianopsia. Which of thefollowing is an appropriate nursing intervention?
• A. Teach the client to scan to the right to seeobjects on the right side of her body.
• B. Place the client’s bedside table on the rightside of the bed.
• C. Orient the client to the food on her plate usingthe clock method.
• D. Place the client’s wheelchair on her left side.

• A. INCORRECT: A client who has left homonymoushemianopsia has lost the left visual field of both eyes.Scanning to the right will decrease the client’s field ofvision.
• B. CORRECT: The client is unable to visualize to the leftmidline of her body. Placing the client’s bedside table onthe right side of her bed will permit visualization of itemson the table.
• C. INCORRECT: Using the clock method of food placementwill be ineffective because only half of the plate can beseen.
• D. INCORRECT: The client’s wheelchair should be placed tothe client’s right or unaffected side.
• A. INCORRECT: A client who has left homonymoushemianopsia has lost the left visual field of both eyes.Scanning to the right will decrease the client’s field ofvision.
• B. CORRECT: The client is unable to visualize to the leftmidline of her body. Placing the client’s bedside table onthe right side of her bed will permit visualization of itemson the table.
• C. INCORRECT: Using the clock method of food placementwill be ineffective because only half of the plate can beseen.
• D. INCORRECT: The client’s wheelchair should be placed tothe client’s right or unaffected side.

Multiple Sclerosis
• Neurological disease resulting in impaired andworsening function of voluntary muscles.
• MS affect nerve cells in the brain and spinal cord.• It is an autoimmune disorder characterized by
development of plaque in the white matter of thecentral nervous system (CNS).
• This plaque damages the myelin sheath andinterferes with impulse transmission between theCNS and the body.
• Relapses and remission occur many times. Finallyleading to quadriplegia.
• Neurological disease resulting in impaired andworsening function of voluntary muscles.
• MS affect nerve cells in the brain and spinal cord.• It is an autoimmune disorder characterized by
development of plaque in the white matter of thecentral nervous system (CNS).
• This plaque damages the myelin sheath andinterferes with impulse transmission between theCNS and the body.
• Relapses and remission occur many times. Finallyleading to quadriplegia.
• Neurological disease resulting in impaired andworsening function of voluntary muscles.
• MS affect nerve cells in the brain and spinal cord.• It is an autoimmune disorder characterized by
development of plaque in the white matter of thecentral nervous system (CNS).
• This plaque damages the myelin sheath andinterferes with impulse transmission between theCNS and the body.
• Relapses and remission occur many times. Finallyleading to quadriplegia.
• Neurological disease resulting in impaired andworsening function of voluntary muscles.
• MS affect nerve cells in the brain and spinal cord.• It is an autoimmune disorder characterized by
development of plaque in the white matter of thecentral nervous system (CNS).
• This plaque damages the myelin sheath andinterferes with impulse transmission between theCNS and the body.
• Relapses and remission occur many times. Finallyleading to quadriplegia.

MS Triggers• Viruses and infectious• Living in a cold climate• Physical injury• Emotional stress• Pregnancy• Fatigue• Overexertion• Temperature extremes• Hot shower/bath
• Viruses and infectious• Living in a cold climate• Physical injury• Emotional stress• Pregnancy• Fatigue• Overexertion• Temperature extremes• Hot shower/bath
• Viruses and infectious• Living in a cold climate• Physical injury• Emotional stress• Pregnancy• Fatigue• Overexertion• Temperature extremes• Hot shower/bath
• Viruses and infectious• Living in a cold climate• Physical injury• Emotional stress• Pregnancy• Fatigue• Overexertion• Temperature extremes• Hot shower/bath

Signs of MS• Fatigue – especially of the lower extremities• Pain or paresthesia , Spasticity (rigid muscle)• Visual changes , diplopia, nystagmus• Uhthoff’s sign (temporary worsening of vision &
neurological functions)• Dysphagia, Dysarthria (slurred and nasal speech)• Bowel, bladder and sexual dysfunction• Cognitive changes (memory loss, impaired
judgment)
• Fatigue – especially of the lower extremities• Pain or paresthesia , Spasticity (rigid muscle)• Visual changes , diplopia, nystagmus• Uhthoff’s sign (temporary worsening of vision &
neurological functions)• Dysphagia, Dysarthria (slurred and nasal speech)• Bowel, bladder and sexual dysfunction• Cognitive changes (memory loss, impaired
judgment)
• Fatigue – especially of the lower extremities• Pain or paresthesia , Spasticity (rigid muscle)• Visual changes , diplopia, nystagmus• Uhthoff’s sign (temporary worsening of vision &
neurological functions)• Dysphagia, Dysarthria (slurred and nasal speech)• Bowel, bladder and sexual dysfunction• Cognitive changes (memory loss, impaired
judgment)
• Fatigue – especially of the lower extremities• Pain or paresthesia , Spasticity (rigid muscle)• Visual changes , diplopia, nystagmus• Uhthoff’s sign (temporary worsening of vision &
neurological functions)• Dysphagia, Dysarthria (slurred and nasal speech)• Bowel, bladder and sexual dysfunction• Cognitive changes (memory loss, impaired
judgment)

Meds
• Azathioprine (Imuran) and cyclosporine(Sandimmune)– Immunosuppressive agents are used to reduce
the frequency of relapses.– Monitor for long-term effects.– Be alert for manifestations of infection.– Assess for hypertension.– Assess for kidney dysfunction.
• Azathioprine (Imuran) and cyclosporine(Sandimmune)– Immunosuppressive agents are used to reduce
the frequency of relapses.– Monitor for long-term effects.– Be alert for manifestations of infection.– Assess for hypertension.– Assess for kidney dysfunction.
• Azathioprine (Imuran) and cyclosporine(Sandimmune)– Immunosuppressive agents are used to reduce
the frequency of relapses.– Monitor for long-term effects.– Be alert for manifestations of infection.– Assess for hypertension.– Assess for kidney dysfunction.
• Azathioprine (Imuran) and cyclosporine(Sandimmune)– Immunosuppressive agents are used to reduce
the frequency of relapses.– Monitor for long-term effects.– Be alert for manifestations of infection.– Assess for hypertension.– Assess for kidney dysfunction.

Meds• Prednisone
– To reduce inflammation in acute exacerbations.– Monitor for increased risk of infection,
hypervolemia, hypernatremia, hypokalemia,hyperglycemia
– Taper dose.• Antispasmodics are used to treat muscle
spasticity• Intrathecal baclofen (a CNS depressant used as a skeletal
muscle relaxant) can be used for severe cases of MS . Avoidstopping baclofen abruptly
• Prednisone– To reduce inflammation in acute exacerbations.– Monitor for increased risk of infection,
hypervolemia, hypernatremia, hypokalemia,hyperglycemia
– Taper dose.• Antispasmodics are used to treat muscle
spasticity• Intrathecal baclofen (a CNS depressant used as a skeletal
muscle relaxant) can be used for severe cases of MS . Avoidstopping baclofen abruptly
• Prednisone– To reduce inflammation in acute exacerbations.– Monitor for increased risk of infection,
hypervolemia, hypernatremia, hypokalemia,hyperglycemia
– Taper dose.• Antispasmodics are used to treat muscle
spasticity• Intrathecal baclofen (a CNS depressant used as a skeletal
muscle relaxant) can be used for severe cases of MS . Avoidstopping baclofen abruptly
• Prednisone– To reduce inflammation in acute exacerbations.– Monitor for increased risk of infection,
hypervolemia, hypernatremia, hypokalemia,hyperglycemia
– Taper dose.• Antispasmodics are used to treat muscle
spasticity• Intrathecal baclofen (a CNS depressant used as a skeletal
muscle relaxant) can be used for severe cases of MS . Avoidstopping baclofen abruptly

Nursing care• Assessment (refer to signs)• Avoid triggers• Apply alternating eye patches to treat diplopia
(double vision). Teach scanning techniques.• Fluids-to prevent urinary tract infection.• Bladder and Bowel training (might need
catheterzation)• Promote energy conservation by grouping cares
and planning rest periods.• Safety precautions
• Assessment (refer to signs)• Avoid triggers• Apply alternating eye patches to treat diplopia
(double vision). Teach scanning techniques.• Fluids-to prevent urinary tract infection.• Bladder and Bowel training (might need
catheterzation)• Promote energy conservation by grouping cares
and planning rest periods.• Safety precautions
• Assessment (refer to signs)• Avoid triggers• Apply alternating eye patches to treat diplopia
(double vision). Teach scanning techniques.• Fluids-to prevent urinary tract infection.• Bladder and Bowel training (might need
catheterzation)• Promote energy conservation by grouping cares
and planning rest periods.• Safety precautions
• Assessment (refer to signs)• Avoid triggers• Apply alternating eye patches to treat diplopia
(double vision). Teach scanning techniques.• Fluids-to prevent urinary tract infection.• Bladder and Bowel training (might need
catheterzation)• Promote energy conservation by grouping cares
and planning rest periods.• Safety precautions

Myasthenia gravis (MG)• It is a progressive autoimmune disease that produces
severe muscular weakness.• It is characterized by periods of exacerbation and
remission.• Muscle weakness improves with rest and worsens with
increased activity.• It is caused by antibodies that interfere with the
transmission of acetylcholine at the neuromuscularjunction.– Therapeutic procedure: Plasmapheresis removes
circulating antibodies from the plasma. This is usually doneseveral times over a period of days and may continue on aregular basis for some clients.
• It is a progressive autoimmune disease that producessevere muscular weakness.
• It is characterized by periods of exacerbation andremission.
• Muscle weakness improves with rest and worsens withincreased activity.
• It is caused by antibodies that interfere with thetransmission of acetylcholine at the neuromuscularjunction.– Therapeutic procedure: Plasmapheresis removes
circulating antibodies from the plasma. This is usually doneseveral times over a period of days and may continue on aregular basis for some clients.
• It is a progressive autoimmune disease that producessevere muscular weakness.
• It is characterized by periods of exacerbation andremission.
• Muscle weakness improves with rest and worsens withincreased activity.
• It is caused by antibodies that interfere with thetransmission of acetylcholine at the neuromuscularjunction.– Therapeutic procedure: Plasmapheresis removes
circulating antibodies from the plasma. This is usually doneseveral times over a period of days and may continue on aregular basis for some clients.
• It is a progressive autoimmune disease that producessevere muscular weakness.
• It is characterized by periods of exacerbation andremission.
• Muscle weakness improves with rest and worsens withincreased activity.
• It is caused by antibodies that interfere with thetransmission of acetylcholine at the neuromuscularjunction.– Therapeutic procedure: Plasmapheresis removes
circulating antibodies from the plasma. This is usually doneseveral times over a period of days and may continue on aregular basis for some clients.

• Factors that trigger exacerbations– Infection– Stress, emotional upset, and fatigue– Pregnancy– Increases in body temperature (fever, sunbathing, hot
tubs).• Diagnostic Procedures : Tensilon testing
– Baseline assessment of the cranial muscle strength isdone.
– Edrophonium (Tensilon) is administered.– Medication inhibits the breakdown of acetylcholine,
making it available for use at the neuromuscular junction.– A positive test results in marked improvement in muscle
strength that lasts approximately 5 min.– Have atropine available, which is the antidote for
edrophonium (bradycardia, sweating, and abdominalcramps, V fib)
• Factors that trigger exacerbations– Infection– Stress, emotional upset, and fatigue– Pregnancy– Increases in body temperature (fever, sunbathing, hot
tubs).• Diagnostic Procedures : Tensilon testing
– Baseline assessment of the cranial muscle strength isdone.
– Edrophonium (Tensilon) is administered.– Medication inhibits the breakdown of acetylcholine,
making it available for use at the neuromuscular junction.– A positive test results in marked improvement in muscle
strength that lasts approximately 5 min.– Have atropine available, which is the antidote for
edrophonium (bradycardia, sweating, and abdominalcramps, V fib)
• Factors that trigger exacerbations– Infection– Stress, emotional upset, and fatigue– Pregnancy– Increases in body temperature (fever, sunbathing, hot
tubs).• Diagnostic Procedures : Tensilon testing
– Baseline assessment of the cranial muscle strength isdone.
– Edrophonium (Tensilon) is administered.– Medication inhibits the breakdown of acetylcholine,
making it available for use at the neuromuscular junction.– A positive test results in marked improvement in muscle
strength that lasts approximately 5 min.– Have atropine available, which is the antidote for
edrophonium (bradycardia, sweating, and abdominalcramps, V fib)
• Factors that trigger exacerbations– Infection– Stress, emotional upset, and fatigue– Pregnancy– Increases in body temperature (fever, sunbathing, hot
tubs).• Diagnostic Procedures : Tensilon testing
– Baseline assessment of the cranial muscle strength isdone.
– Edrophonium (Tensilon) is administered.– Medication inhibits the breakdown of acetylcholine,
making it available for use at the neuromuscular junction.– A positive test results in marked improvement in muscle
strength that lasts approximately 5 min.– Have atropine available, which is the antidote for
edrophonium (bradycardia, sweating, and abdominalcramps, V fib)

• Subjective Data– Progressive muscle weakness– Diplopia– Difficulty chewing and swallowing– Respiratory dysfunction– Bowel and bladder dysfunction– Poor posture– Fatigue after exertion
• Assessment– Impaired respiratory status (difficulty managing secretions,
decreased respiratory effort.– Decreased swallowing ability.– Decreased muscle strength, especially of the face, eyes,
and proximal portion of major muscle groups.– Incontinence– Drooping eyelids – unilateral or bilateral
• Subjective Data– Progressive muscle weakness– Diplopia– Difficulty chewing and swallowing– Respiratory dysfunction– Bowel and bladder dysfunction– Poor posture– Fatigue after exertion
• Assessment– Impaired respiratory status (difficulty managing secretions,
decreased respiratory effort.– Decreased swallowing ability.– Decreased muscle strength, especially of the face, eyes,
and proximal portion of major muscle groups.– Incontinence– Drooping eyelids – unilateral or bilateral
• Subjective Data– Progressive muscle weakness– Diplopia– Difficulty chewing and swallowing– Respiratory dysfunction– Bowel and bladder dysfunction– Poor posture– Fatigue after exertion
• Assessment– Impaired respiratory status (difficulty managing secretions,
decreased respiratory effort.– Decreased swallowing ability.– Decreased muscle strength, especially of the face, eyes,
and proximal portion of major muscle groups.– Incontinence– Drooping eyelids – unilateral or bilateral
• Subjective Data– Progressive muscle weakness– Diplopia– Difficulty chewing and swallowing– Respiratory dysfunction– Bowel and bladder dysfunction– Poor posture– Fatigue after exertion
• Assessment– Impaired respiratory status (difficulty managing secretions,
decreased respiratory effort.– Decreased swallowing ability.– Decreased muscle strength, especially of the face, eyes,
and proximal portion of major muscle groups.– Incontinence– Drooping eyelids – unilateral or bilateral

Nursing Care• Assess and intervene as needed to maintain a patent
airway (muscle weakness of diaphragm, respiratory, andintercostal muscles).
• Use energy conservation measures. Allow for periods ofrest.
• Assess swallowing to prevent aspiration.– oxygen, endotracheal intubation, suctioning equipment, and a
bag valve mask available at the client’s bedside.– Provide small, frequent, high-calorie meals and schedule at
times when medication is peaking.– Have the client sit upright when eating, and use thickener in
liquids as necessary.• Apply a lubricating eye drop during the day and ointment at
night if the client is unable to completely close his eyes.– The client may also need to patch or tape his eyes shut at night
to prevent damage to the cornea.
• Assess and intervene as needed to maintain a patentairway (muscle weakness of diaphragm, respiratory, andintercostal muscles).
• Use energy conservation measures. Allow for periods ofrest.
• Assess swallowing to prevent aspiration.– oxygen, endotracheal intubation, suctioning equipment, and a
bag valve mask available at the client’s bedside.– Provide small, frequent, high-calorie meals and schedule at
times when medication is peaking.– Have the client sit upright when eating, and use thickener in
liquids as necessary.• Apply a lubricating eye drop during the day and ointment at
night if the client is unable to completely close his eyes.– The client may also need to patch or tape his eyes shut at night
to prevent damage to the cornea.
• Assess and intervene as needed to maintain a patentairway (muscle weakness of diaphragm, respiratory, andintercostal muscles).
• Use energy conservation measures. Allow for periods ofrest.
• Assess swallowing to prevent aspiration.– oxygen, endotracheal intubation, suctioning equipment, and a
bag valve mask available at the client’s bedside.– Provide small, frequent, high-calorie meals and schedule at
times when medication is peaking.– Have the client sit upright when eating, and use thickener in
liquids as necessary.• Apply a lubricating eye drop during the day and ointment at
night if the client is unable to completely close his eyes.– The client may also need to patch or tape his eyes shut at night
to prevent damage to the cornea.
• Assess and intervene as needed to maintain a patentairway (muscle weakness of diaphragm, respiratory, andintercostal muscles).
• Use energy conservation measures. Allow for periods ofrest.
• Assess swallowing to prevent aspiration.– oxygen, endotracheal intubation, suctioning equipment, and a
bag valve mask available at the client’s bedside.– Provide small, frequent, high-calorie meals and schedule at
times when medication is peaking.– Have the client sit upright when eating, and use thickener in
liquids as necessary.• Apply a lubricating eye drop during the day and ointment at
night if the client is unable to completely close his eyes.– The client may also need to patch or tape his eyes shut at night
to prevent damage to the cornea.

Nursing Care• Patient to wear a medical id band• Medications : Anticholinesterase agents are the first
line in therapy.– Ensure that the medication is given at the specified time,
usually four times a day.– If periods of weakness are observed, discuss change in
administration times with the provider.– Use cautiously in clients who have a history of asthma or
cardiac dysrhythmias.• Client Education
– Take with food to address gastrointestinal side effects.– Eat within 45 min of taking the medication to strengthen
chewing and reduce the risk for aspiration.– Stress the importance of maintaining therapeutic levels
and taking the medication at the same time each day.
• Patient to wear a medical id band• Medications : Anticholinesterase agents are the first
line in therapy.– Ensure that the medication is given at the specified time,
usually four times a day.– If periods of weakness are observed, discuss change in
administration times with the provider.– Use cautiously in clients who have a history of asthma or
cardiac dysrhythmias.• Client Education
– Take with food to address gastrointestinal side effects.– Eat within 45 min of taking the medication to strengthen
chewing and reduce the risk for aspiration.– Stress the importance of maintaining therapeutic levels
and taking the medication at the same time each day.
• Patient to wear a medical id band• Medications : Anticholinesterase agents are the first
line in therapy.– Ensure that the medication is given at the specified time,
usually four times a day.– If periods of weakness are observed, discuss change in
administration times with the provider.– Use cautiously in clients who have a history of asthma or
cardiac dysrhythmias.• Client Education
– Take with food to address gastrointestinal side effects.– Eat within 45 min of taking the medication to strengthen
chewing and reduce the risk for aspiration.– Stress the importance of maintaining therapeutic levels
and taking the medication at the same time each day.
• Patient to wear a medical id band• Medications : Anticholinesterase agents are the first
line in therapy.– Ensure that the medication is given at the specified time,
usually four times a day.– If periods of weakness are observed, discuss change in
administration times with the provider.– Use cautiously in clients who have a history of asthma or
cardiac dysrhythmias.• Client Education
– Take with food to address gastrointestinal side effects.– Eat within 45 min of taking the medication to strengthen
chewing and reduce the risk for aspiration.– Stress the importance of maintaining therapeutic levels
and taking the medication at the same time each day.

Medications
• Pyridostigmine (Mestinon) and neostigmine(Prostigmin)– Used to increase muscle strength in the
symptomatic treatment of MG. It inhibits thebreakdown of acetylcholine and prolongs itseffects.
• Nursing Considerations– Assess the client for a history of seizures.– Use cautiously in clients who have a history of
asthma and cardiovascular disease.
• Pyridostigmine (Mestinon) and neostigmine(Prostigmin)– Used to increase muscle strength in the
symptomatic treatment of MG. It inhibits thebreakdown of acetylcholine and prolongs itseffects.
• Nursing Considerations– Assess the client for a history of seizures.– Use cautiously in clients who have a history of
asthma and cardiovascular disease.
• Pyridostigmine (Mestinon) and neostigmine(Prostigmin)– Used to increase muscle strength in the
symptomatic treatment of MG. It inhibits thebreakdown of acetylcholine and prolongs itseffects.
• Nursing Considerations– Assess the client for a history of seizures.– Use cautiously in clients who have a history of
asthma and cardiovascular disease.
• Pyridostigmine (Mestinon) and neostigmine(Prostigmin)– Used to increase muscle strength in the
symptomatic treatment of MG. It inhibits thebreakdown of acetylcholine and prolongs itseffects.
• Nursing Considerations– Assess the client for a history of seizures.– Use cautiously in clients who have a history of
asthma and cardiovascular disease.

Complications• Myasthenic crisis occurs when the client is
experiencing a stressor that causes anexacerbation of MG (infection, under medication)
• Cholinergic crisis occurs when the client has takentoo much cholinesterase inhibitor (overmedication)
• The manifestations of both can be very similar(muscle weakness, respiratory failure).
• An edrophonium test may be performed todetermine the crisis– Worsening of the symptoms after the test dose of
medication is administered indicates a cholinergiccrisis.
• Myasthenic crisis occurs when the client isexperiencing a stressor that causes anexacerbation of MG (infection, under medication)
• Cholinergic crisis occurs when the client has takentoo much cholinesterase inhibitor (overmedication)
• The manifestations of both can be very similar(muscle weakness, respiratory failure).
• An edrophonium test may be performed todetermine the crisis– Worsening of the symptoms after the test dose of
medication is administered indicates a cholinergiccrisis.
• Myasthenic crisis occurs when the client isexperiencing a stressor that causes anexacerbation of MG (infection, under medication)
• Cholinergic crisis occurs when the client has takentoo much cholinesterase inhibitor (overmedication)
• The manifestations of both can be very similar(muscle weakness, respiratory failure).
• An edrophonium test may be performed todetermine the crisis– Worsening of the symptoms after the test dose of
medication is administered indicates a cholinergiccrisis.
• Myasthenic crisis occurs when the client isexperiencing a stressor that causes anexacerbation of MG (infection, under medication)
• Cholinergic crisis occurs when the client has takentoo much cholinesterase inhibitor (overmedication)
• The manifestations of both can be very similar(muscle weakness, respiratory failure).
• An edrophonium test may be performed todetermine the crisis– Worsening of the symptoms after the test dose of
medication is administered indicates a cholinergiccrisis.

Myasthenic crisis
• Myasthenic crisis Clinical manifestations:• increased diaphoresis, bowel and bladder
incontinence, absent cough and swallowreflex, sudden marked rise in blood pressurebecause of hypoxia, increased heart rate,severe respiratory distress and cyanosis,increased secretions, increased lacrimation,restlessness, and dysarthria.
• Myasthenic crisis Clinical manifestations:• increased diaphoresis, bowel and bladder
incontinence, absent cough and swallowreflex, sudden marked rise in blood pressurebecause of hypoxia, increased heart rate,severe respiratory distress and cyanosis,increased secretions, increased lacrimation,restlessness, and dysarthria.

Parkinson’s disease (PD)
• It is a progressively debilitating disease thatgrossly affects motor function.
• It is characterized by four primary symptoms:tremor, muscle rigidity, bradykinesia (slowmovement), and postural instability.
• These symptoms occur due to overstimulationof the basal ganglia by acetylcholine (anddepletion of dopamine)
• It is a progressively debilitating disease thatgrossly affects motor function.
• It is characterized by four primary symptoms:tremor, muscle rigidity, bradykinesia (slowmovement), and postural instability.
• These symptoms occur due to overstimulationof the basal ganglia by acetylcholine (anddepletion of dopamine)
• It is a progressively debilitating disease thatgrossly affects motor function.
• It is characterized by four primary symptoms:tremor, muscle rigidity, bradykinesia (slowmovement), and postural instability.
• These symptoms occur due to overstimulationof the basal ganglia by acetylcholine (anddepletion of dopamine)
• It is a progressively debilitating disease thatgrossly affects motor function.
• It is characterized by four primary symptoms:tremor, muscle rigidity, bradykinesia (slowmovement), and postural instability.
• These symptoms occur due to overstimulationof the basal ganglia by acetylcholine (anddepletion of dopamine)

Nursing Care• Monitor swallowing and maintain adequate nutrition.• Maintain client mobility for as long as possible.• Monitor client’s mental and cognitive status
– Observe for signs of depression and dementia.– Provide a safe environment (no throw rugs, encourage the
use of an electric razor).• Promote client communication
– Teach the client facial muscle strengthening exercises.– Encourage the client to speak slowly and to pause
frequently.– Use alternate forms of communication as appropriate.– Refer client to a speech-language pathologist
• Monitor swallowing and maintain adequate nutrition.• Maintain client mobility for as long as possible.• Monitor client’s mental and cognitive status
– Observe for signs of depression and dementia.– Provide a safe environment (no throw rugs, encourage the
use of an electric razor).• Promote client communication
– Teach the client facial muscle strengthening exercises.– Encourage the client to speak slowly and to pause
frequently.– Use alternate forms of communication as appropriate.– Refer client to a speech-language pathologist
• Monitor swallowing and maintain adequate nutrition.• Maintain client mobility for as long as possible.• Monitor client’s mental and cognitive status
– Observe for signs of depression and dementia.– Provide a safe environment (no throw rugs, encourage the
use of an electric razor).• Promote client communication
– Teach the client facial muscle strengthening exercises.– Encourage the client to speak slowly and to pause
frequently.– Use alternate forms of communication as appropriate.– Refer client to a speech-language pathologist
• Monitor swallowing and maintain adequate nutrition.• Maintain client mobility for as long as possible.• Monitor client’s mental and cognitive status
– Observe for signs of depression and dementia.– Provide a safe environment (no throw rugs, encourage the
use of an electric razor).• Promote client communication
– Teach the client facial muscle strengthening exercises.– Encourage the client to speak slowly and to pause
frequently.– Use alternate forms of communication as appropriate.– Refer client to a speech-language pathologist


Medication• May take several weeks of use before
improvement of symptoms is seen.• maintenance of therapeutic level• levodopa (Dopar):
– converted to dopamine in the brain.– may be combined with carbidopa (Sinemet) to
decrease peripheral metabolism of levodopa• Anticholinergics : help control tremors and
rigidity– Monitor for anticholinergic effects (dry mouth,
constipation, urinary retention, acute confusion).
• May take several weeks of use beforeimprovement of symptoms is seen.
• maintenance of therapeutic level• levodopa (Dopar):
– converted to dopamine in the brain.– may be combined with carbidopa (Sinemet) to
decrease peripheral metabolism of levodopa• Anticholinergics : help control tremors and
rigidity– Monitor for anticholinergic effects (dry mouth,
constipation, urinary retention, acute confusion).
• May take several weeks of use beforeimprovement of symptoms is seen.
• maintenance of therapeutic level• levodopa (Dopar):
– converted to dopamine in the brain.– may be combined with carbidopa (Sinemet) to
decrease peripheral metabolism of levodopa• Anticholinergics : help control tremors and
rigidity– Monitor for anticholinergic effects (dry mouth,
constipation, urinary retention, acute confusion).
• May take several weeks of use beforeimprovement of symptoms is seen.
• maintenance of therapeutic level• levodopa (Dopar):
– converted to dopamine in the brain.– may be combined with carbidopa (Sinemet) to
decrease peripheral metabolism of levodopa• Anticholinergics : help control tremors and
rigidity– Monitor for anticholinergic effects (dry mouth,
constipation, urinary retention, acute confusion).
Alzheimer’s disease
• Nonreversible type of dementia• Characterized by memory loss, problems with
judgment, and changes in personality leadingto severe physical decline
• Meds- Aricept – Prevent breakdown of Achresult in increased nerve impulses at thenerve sites.– Antipsychotics, anxiolytics, antidepresents– Ginkgo biloba – herbal- memory improvement
• Nonreversible type of dementia• Characterized by memory loss, problems with
judgment, and changes in personality leadingto severe physical decline
• Meds- Aricept – Prevent breakdown of Achresult in increased nerve impulses at thenerve sites.– Antipsychotics, anxiolytics, antidepresents– Ginkgo biloba – herbal- memory improvement
• Nonreversible type of dementia• Characterized by memory loss, problems with
judgment, and changes in personality leadingto severe physical decline
• Meds- Aricept – Prevent breakdown of Achresult in increased nerve impulses at thenerve sites.– Antipsychotics, anxiolytics, antidepresents– Ginkgo biloba – herbal- memory improvement
• Nonreversible type of dementia• Characterized by memory loss, problems with
judgment, and changes in personality leadingto severe physical decline
• Meds- Aricept – Prevent breakdown of Achresult in increased nerve impulses at thenerve sites.– Antipsychotics, anxiolytics, antidepresents– Ginkgo biloba – herbal- memory improvement

Home Safety• Remove scatter rugs, lock cleaning supplies• Install door locks and place alarms on doors.• Keeping a lock on the water heater and thermostat• Provide good lighting, especially on stairs.• Place mattress on the floor.• Install handrails on stairs, mark step edges with colored
tape.• Remove clutter and clearing hallways for walking.• Secure electrical cords to baseboards.• Install handrails in the bathroom, at bedside, and in the
tub; placing a shower chair in the tub.• Having the client wear a medical identification bracelet• Monitoring for improvement in memory and the client’s
quality of life.
• Remove scatter rugs, lock cleaning supplies• Install door locks and place alarms on doors.• Keeping a lock on the water heater and thermostat• Provide good lighting, especially on stairs.• Place mattress on the floor.• Install handrails on stairs, mark step edges with colored
tape.• Remove clutter and clearing hallways for walking.• Secure electrical cords to baseboards.• Install handrails in the bathroom, at bedside, and in the
tub; placing a shower chair in the tub.• Having the client wear a medical identification bracelet• Monitoring for improvement in memory and the client’s
quality of life.
• Remove scatter rugs, lock cleaning supplies• Install door locks and place alarms on doors.• Keeping a lock on the water heater and thermostat• Provide good lighting, especially on stairs.• Place mattress on the floor.• Install handrails on stairs, mark step edges with colored
tape.• Remove clutter and clearing hallways for walking.• Secure electrical cords to baseboards.• Install handrails in the bathroom, at bedside, and in the
tub; placing a shower chair in the tub.• Having the client wear a medical identification bracelet• Monitoring for improvement in memory and the client’s
quality of life.
• Remove scatter rugs, lock cleaning supplies• Install door locks and place alarms on doors.• Keeping a lock on the water heater and thermostat• Provide good lighting, especially on stairs.• Place mattress on the floor.• Install handrails on stairs, mark step edges with colored
tape.• Remove clutter and clearing hallways for walking.• Secure electrical cords to baseboards.• Install handrails in the bathroom, at bedside, and in the
tub; placing a shower chair in the tub.• Having the client wear a medical identification bracelet• Monitoring for improvement in memory and the client’s
quality of life.

Trigeminal Neuralgia– Description
• Sensory disorder of trigeminal cranial nerve– Assessment
• Severe pain on lips, gums, nose, or acrosscheeks
– Interventions• Avoiding hot or cold fluids or foods• Chew food on unaffected side• Administer medications as prescribed• Prepare for surgical intervention if prescribed
Trigeminal Neuralgia– Description
• Sensory disorder of trigeminal cranial nerve– Assessment
• Severe pain on lips, gums, nose, or acrosscheeks
– Interventions• Avoiding hot or cold fluids or foods• Chew food on unaffected side• Administer medications as prescribed• Prepare for surgical intervention if prescribed

Trigeminal Neuralgia

Bell’s Palsy (Facial Paralysis)– Description
• Lower motor lesion of facial nerve that resultsin paralysis on one side of face
– Assessment• Unilateral facial paralysis• Inability to raise eyebrows, frown, smile, close
eyelids, or puff out cheeks– Interventions
• Protect eye from dryness• Prevent client injury• Supportive care
Bell’s Palsy (Facial Paralysis)– Description
• Lower motor lesion of facial nerve that resultsin paralysis on one side of face
– Assessment• Unilateral facial paralysis• Inability to raise eyebrows, frown, smile, close
eyelids, or puff out cheeks– Interventions
• Protect eye from dryness• Prevent client injury• Supportive care
Bell’s Palsy (Facial Paralysis)– Description
• Lower motor lesion of facial nerve that resultsin paralysis on one side of face
– Assessment• Unilateral facial paralysis• Inability to raise eyebrows, frown, smile, close
eyelids, or puff out cheeks– Interventions
• Protect eye from dryness• Prevent client injury• Supportive care
Bell’s Palsy (Facial Paralysis)– Description
• Lower motor lesion of facial nerve that resultsin paralysis on one side of face
– Assessment• Unilateral facial paralysis• Inability to raise eyebrows, frown, smile, close
eyelids, or puff out cheeks– Interventions
• Protect eye from dryness• Prevent client injury• Supportive care

Bell’s Palsy

Guillain-Barré Syndrome– Description
• Acute, infectious neuronitis of cranial and peripheralnerves
– Assessment• Motor weakness and flaccid paralysis , that starts from
lower extremities• Gradual progressive weakness of upper extremities,
facial muscles, and possible progression to respiratoryfailure
• “Ground to brain”– Interventions
• Prepare to initiate respiratory support• Provide supportive care
Guillain-Barré Syndrome– Description
• Acute, infectious neuronitis of cranial and peripheralnerves
– Assessment• Motor weakness and flaccid paralysis , that starts from
lower extremities• Gradual progressive weakness of upper extremities,
facial muscles, and possible progression to respiratoryfailure
• “Ground to brain”– Interventions
• Prepare to initiate respiratory support• Provide supportive care
Guillain-Barré Syndrome– Description
• Acute, infectious neuronitis of cranial and peripheralnerves
– Assessment• Motor weakness and flaccid paralysis , that starts from
lower extremities• Gradual progressive weakness of upper extremities,
facial muscles, and possible progression to respiratoryfailure
• “Ground to brain”– Interventions
• Prepare to initiate respiratory support• Provide supportive care
Guillain-Barré Syndrome– Description
• Acute, infectious neuronitis of cranial and peripheralnerves
– Assessment• Motor weakness and flaccid paralysis , that starts from
lower extremities• Gradual progressive weakness of upper extremities,
facial muscles, and possible progression to respiratoryfailure
• “Ground to brain”– Interventions
• Prepare to initiate respiratory support• Provide supportive care

Amyotrophic Lateral Sclerosis (LouGehrig’s disease)
• ALS is a disease of the upper and lower motor neurons thatresults in deterioration and death of the motor neurons.
• This results in progressive paralysis and muscle wasting thateventually causes respiratory paralysis and death
• ALS does not involve sensory alterations or cognitive changes.– Assessment
– Fatigue, Twitching and cramping of muscles– Objective Data
– Muscle weakness – usually begins in one part of thebody
– Muscle atrophy– Dysphagia, Dysarthria– Hyperreflexia of deep tendon reflexes
Amyotrophic Lateral Sclerosis (LouGehrig’s disease)
• ALS is a disease of the upper and lower motor neurons thatresults in deterioration and death of the motor neurons.
• This results in progressive paralysis and muscle wasting thateventually causes respiratory paralysis and death
• ALS does not involve sensory alterations or cognitive changes.– Assessment
– Fatigue, Twitching and cramping of muscles– Objective Data
– Muscle weakness – usually begins in one part of thebody
– Muscle atrophy– Dysphagia, Dysarthria– Hyperreflexia of deep tendon reflexes
Amyotrophic Lateral Sclerosis (LouGehrig’s disease)
• ALS is a disease of the upper and lower motor neurons thatresults in deterioration and death of the motor neurons.
• This results in progressive paralysis and muscle wasting thateventually causes respiratory paralysis and death
• ALS does not involve sensory alterations or cognitive changes.– Assessment
– Fatigue, Twitching and cramping of muscles– Objective Data
– Muscle weakness – usually begins in one part of thebody
– Muscle atrophy– Dysphagia, Dysarthria– Hyperreflexia of deep tendon reflexes
Amyotrophic Lateral Sclerosis (LouGehrig’s disease)
• ALS is a disease of the upper and lower motor neurons thatresults in deterioration and death of the motor neurons.
• This results in progressive paralysis and muscle wasting thateventually causes respiratory paralysis and death
• ALS does not involve sensory alterations or cognitive changes.– Assessment
– Fatigue, Twitching and cramping of muscles– Objective Data
– Muscle weakness – usually begins in one part of thebody
– Muscle atrophy– Dysphagia, Dysarthria– Hyperreflexia of deep tendon reflexes


Interventions ALS• Care is directed toward treatment of symptoms.• Maintain a patent airway, and suction and/or intubate
as needed.• Monitor ABGs, and administer oxygen• Keep the head of the bed at 45°; turn, cough, and deep
breathe every 2 hr; and conduct incentivespirometry/chest physiotherapy.
• Assess swallow reflex and ensure safety with oralintake. Thicken fluids as needed.
• Meet nutritional needs for calories, fiber, and fluids.When no longer able to swallow, provide enteralnutrition as prescribed.
• Facilitate effective communication.• Use energy conservation measures.
• Care is directed toward treatment of symptoms.• Maintain a patent airway, and suction and/or intubate
as needed.• Monitor ABGs, and administer oxygen• Keep the head of the bed at 45°; turn, cough, and deep
breathe every 2 hr; and conduct incentivespirometry/chest physiotherapy.
• Assess swallow reflex and ensure safety with oralintake. Thicken fluids as needed.
• Meet nutritional needs for calories, fiber, and fluids.When no longer able to swallow, provide enteralnutrition as prescribed.
• Facilitate effective communication.• Use energy conservation measures.
• Care is directed toward treatment of symptoms.• Maintain a patent airway, and suction and/or intubate
as needed.• Monitor ABGs, and administer oxygen• Keep the head of the bed at 45°; turn, cough, and deep
breathe every 2 hr; and conduct incentivespirometry/chest physiotherapy.
• Assess swallow reflex and ensure safety with oralintake. Thicken fluids as needed.
• Meet nutritional needs for calories, fiber, and fluids.When no longer able to swallow, provide enteralnutrition as prescribed.
• Facilitate effective communication.• Use energy conservation measures.
• Care is directed toward treatment of symptoms.• Maintain a patent airway, and suction and/or intubate
as needed.• Monitor ABGs, and administer oxygen• Keep the head of the bed at 45°; turn, cough, and deep
breathe every 2 hr; and conduct incentivespirometry/chest physiotherapy.
• Assess swallow reflex and ensure safety with oralintake. Thicken fluids as needed.
• Meet nutritional needs for calories, fiber, and fluids.When no longer able to swallow, provide enteralnutrition as prescribed.
• Facilitate effective communication.• Use energy conservation measures.

Encephalitis– Description
• Inflammation of brain parenchyma and often meninges– Transmission
• Most often by the bite of infected mosquito or tick– Assessment
• Changes in level of consciousness• Motor dysfunction• Focal neurological deficits
– Interventions• Supportive care• Rehabilitation
Encephalitis– Description
• Inflammation of brain parenchyma and often meninges– Transmission
• Most often by the bite of infected mosquito or tick– Assessment
• Changes in level of consciousness• Motor dysfunction• Focal neurological deficits
– Interventions• Supportive care• Rehabilitation
Encephalitis– Description
• Inflammation of brain parenchyma and often meninges– Transmission
• Most often by the bite of infected mosquito or tick– Assessment
• Changes in level of consciousness• Motor dysfunction• Focal neurological deficits
– Interventions• Supportive care• Rehabilitation
Encephalitis– Description
• Inflammation of brain parenchyma and often meninges– Transmission
• Most often by the bite of infected mosquito or tick– Assessment
• Changes in level of consciousness• Motor dysfunction• Focal neurological deficits
– Interventions• Supportive care• Rehabilitation

West Nile Virus– Description
• Affects the central nervous system and causesneurological damage
– Assessment• Flu-like symptoms that progress to neurological deficits
– Interventions• Supportive care
– Prevention• Use of insect repellent• Wear long sleeves and pants and light-colored clothing
when outdoors• Eliminate mosquito breeding sites from environment
West Nile Virus– Description
• Affects the central nervous system and causesneurological damage
– Assessment• Flu-like symptoms that progress to neurological deficits
– Interventions• Supportive care
– Prevention• Use of insect repellent• Wear long sleeves and pants and light-colored clothing
when outdoors• Eliminate mosquito breeding sites from environment
West Nile Virus– Description
• Affects the central nervous system and causesneurological damage
– Assessment• Flu-like symptoms that progress to neurological deficits
– Interventions• Supportive care
– Prevention• Use of insect repellent• Wear long sleeves and pants and light-colored clothing
when outdoors• Eliminate mosquito breeding sites from environment
West Nile Virus– Description
• Affects the central nervous system and causesneurological damage
– Assessment• Flu-like symptoms that progress to neurological deficits
– Interventions• Supportive care
– Prevention• Use of insect repellent• Wear long sleeves and pants and light-colored clothing
when outdoors• Eliminate mosquito breeding sites from environment

Spinal cord injuries
• Spinal cord injuries (SCIs) involve the loss ofmotor function, sensory function, reflexes, andcontrol of elimination.
• Injuries in the cervical region result inquadriplegia – paralysis/paresis of all fourextremities and trunk.
• Injuries below T1 result in paraplegia –paralysis/paresis of the lower extremities.
• The level of cord involved dictates theconsequences of spinal cord injury
• Spinal cord injuries (SCIs) involve the loss ofmotor function, sensory function, reflexes, andcontrol of elimination.
• Injuries in the cervical region result inquadriplegia – paralysis/paresis of all fourextremities and trunk.
• Injuries below T1 result in paraplegia –paralysis/paresis of the lower extremities.
• The level of cord involved dictates theconsequences of spinal cord injury
• Spinal cord injuries (SCIs) involve the loss ofmotor function, sensory function, reflexes, andcontrol of elimination.
• Injuries in the cervical region result inquadriplegia – paralysis/paresis of all fourextremities and trunk.
• Injuries below T1 result in paraplegia –paralysis/paresis of the lower extremities.
• The level of cord involved dictates theconsequences of spinal cord injury
• Spinal cord injuries (SCIs) involve the loss ofmotor function, sensory function, reflexes, andcontrol of elimination.
• Injuries in the cervical region result inquadriplegia – paralysis/paresis of all fourextremities and trunk.
• Injuries below T1 result in paraplegia –paralysis/paresis of the lower extremities.
• The level of cord involved dictates theconsequences of spinal cord injury

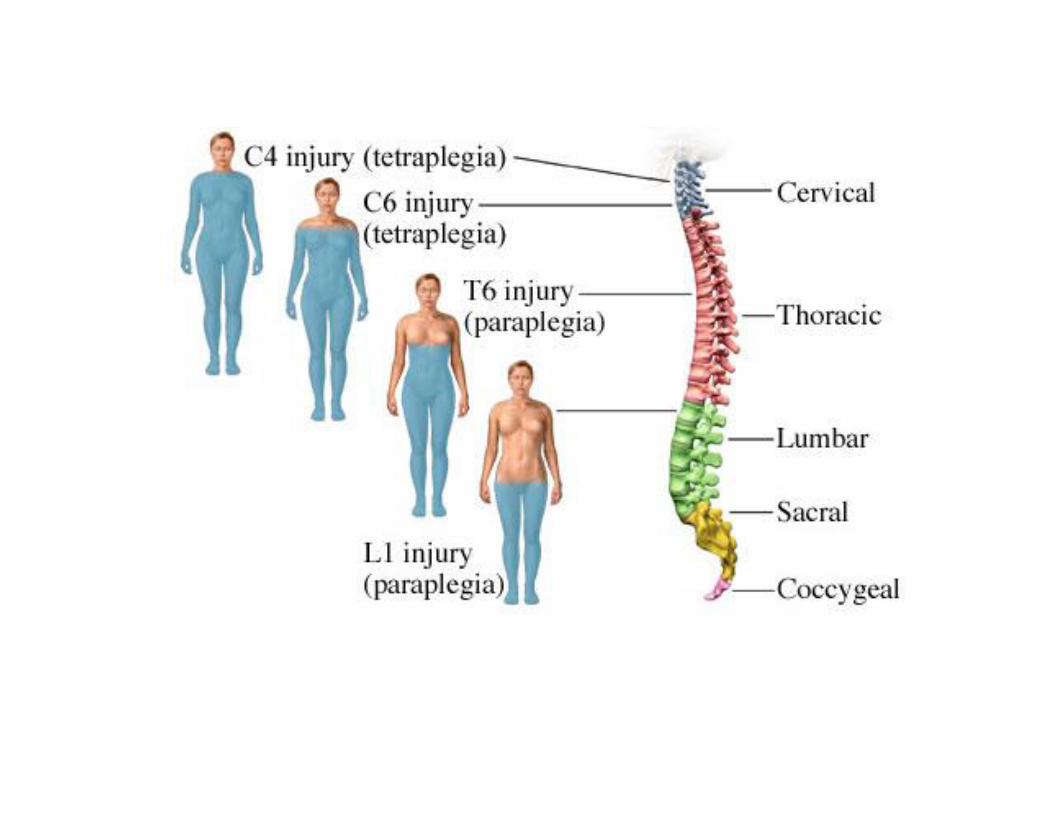

Nursing Care• Respiratory status
– Monitoring the client’s respiratory status is the first priority.– Involuntary respirations can be affected due to a lesion at or
above the phrenic nerve or swelling from a lesionimmediately below C4.
– Lesions in the cervical or upper thoracic area will also impairvoluntary movement of muscles used in respiration(increase in depth or rate).
– Provide the client with oxygen and suction as needed.– Assist with intubation and mechanical ventilation if
necessary.– Assist the client to cough by applying abdominal pressure
when attempting to cough.– Teach client about use of incentive spirometer, and
encourage client to perform coughing and deep breathingregularly.
• Respiratory status– Monitoring the client’s respiratory status is the first priority.– Involuntary respirations can be affected due to a lesion at or
above the phrenic nerve or swelling from a lesionimmediately below C4.
– Lesions in the cervical or upper thoracic area will also impairvoluntary movement of muscles used in respiration(increase in depth or rate).
– Provide the client with oxygen and suction as needed.– Assist with intubation and mechanical ventilation if
necessary.– Assist the client to cough by applying abdominal pressure
when attempting to cough.– Teach client about use of incentive spirometer, and
encourage client to perform coughing and deep breathingregularly.
• Respiratory status– Monitoring the client’s respiratory status is the first priority.– Involuntary respirations can be affected due to a lesion at or
above the phrenic nerve or swelling from a lesionimmediately below C4.
– Lesions in the cervical or upper thoracic area will also impairvoluntary movement of muscles used in respiration(increase in depth or rate).
– Provide the client with oxygen and suction as needed.– Assist with intubation and mechanical ventilation if
necessary.– Assist the client to cough by applying abdominal pressure
when attempting to cough.– Teach client about use of incentive spirometer, and
encourage client to perform coughing and deep breathingregularly.
• Respiratory status– Monitoring the client’s respiratory status is the first priority.– Involuntary respirations can be affected due to a lesion at or
above the phrenic nerve or swelling from a lesionimmediately below C4.
– Lesions in the cervical or upper thoracic area will also impairvoluntary movement of muscles used in respiration(increase in depth or rate).
– Provide the client with oxygen and suction as needed.– Assist with intubation and mechanical ventilation if
necessary.– Assist the client to cough by applying abdominal pressure
when attempting to cough.– Teach client about use of incentive spirometer, and
encourage client to perform coughing and deep breathingregularly.

• Tissue perfusion– Neurogenic shock occurs after a SCI : Hypotension,
dependent edema, and loss of temperature regulation.– When in an upright position, clients who are in neurogenic
shock will experience postural hypotension. Transferringthe client to a wheelchair should occur in stages.
• Raise the client’s head of the bed and be ready to lower the angleif the client reports dizziness.
• Transfer the client into a reclining wheelchair with the back of thewheelchair reclined.
• Be ready to lock and lean the wheelchair back onto the knee to afully reclined position if the client reports dizziness after thetransfer. Do not attempt to return the client to the bed.
– Monitor the client for signs of thrombophlebitis(anticoagulants)
• Tissue perfusion– Neurogenic shock occurs after a SCI : Hypotension,
dependent edema, and loss of temperature regulation.– When in an upright position, clients who are in neurogenic
shock will experience postural hypotension. Transferringthe client to a wheelchair should occur in stages.
• Raise the client’s head of the bed and be ready to lower the angleif the client reports dizziness.
• Transfer the client into a reclining wheelchair with the back of thewheelchair reclined.
• Be ready to lock and lean the wheelchair back onto the knee to afully reclined position if the client reports dizziness after thetransfer. Do not attempt to return the client to the bed.
– Monitor the client for signs of thrombophlebitis(anticoagulants)
• Tissue perfusion– Neurogenic shock occurs after a SCI : Hypotension,
dependent edema, and loss of temperature regulation.– When in an upright position, clients who are in neurogenic
shock will experience postural hypotension. Transferringthe client to a wheelchair should occur in stages.
• Raise the client’s head of the bed and be ready to lower the angleif the client reports dizziness.
• Transfer the client into a reclining wheelchair with the back of thewheelchair reclined.
• Be ready to lock and lean the wheelchair back onto the knee to afully reclined position if the client reports dizziness after thetransfer. Do not attempt to return the client to the bed.
– Monitor the client for signs of thrombophlebitis(anticoagulants)
• Tissue perfusion– Neurogenic shock occurs after a SCI : Hypotension,
dependent edema, and loss of temperature regulation.– When in an upright position, clients who are in neurogenic
shock will experience postural hypotension. Transferringthe client to a wheelchair should occur in stages.
• Raise the client’s head of the bed and be ready to lower the angleif the client reports dizziness.
• Transfer the client into a reclining wheelchair with the back of thewheelchair reclined.
• Be ready to lock and lean the wheelchair back onto the knee to afully reclined position if the client reports dizziness after thetransfer. Do not attempt to return the client to the bed.
– Monitor the client for signs of thrombophlebitis(anticoagulants)

Nursing care (contd)
• Intake and output – The client may be NPO forseveral days.
• Regulation of fluid balance and nutritionalsupport is necessary.
• Maintain an adequate fluid intake for the client;fluid will aid in preventing urinary calculi andbladder infections, and maintain soft stools.
• Neurological status – After determining thebaseline, monitor for an increasing loss ofneurological function.
• Intake and output – The client may be NPO forseveral days.
• Regulation of fluid balance and nutritionalsupport is necessary.
• Maintain an adequate fluid intake for the client;fluid will aid in preventing urinary calculi andbladder infections, and maintain soft stools.
• Neurological status – After determining thebaseline, monitor for an increasing loss ofneurological function.
• Intake and output – The client may be NPO forseveral days.
• Regulation of fluid balance and nutritionalsupport is necessary.
• Maintain an adequate fluid intake for the client;fluid will aid in preventing urinary calculi andbladder infections, and maintain soft stools.
• Neurological status – After determining thebaseline, monitor for an increasing loss ofneurological function.
• Intake and output – The client may be NPO forseveral days.
• Regulation of fluid balance and nutritionalsupport is necessary.
• Maintain an adequate fluid intake for the client;fluid will aid in preventing urinary calculi andbladder infections, and maintain soft stools.
• Neurological status – After determining thebaseline, monitor for an increasing loss ofneurological function.

• Muscle strength and tone – After determining the baseline,monitor for an increasing loss of muscle strength in the affectedextremities.
• Clients who have upper motor neuron (UMN) injuries (above L1and L2) will convert to a spastic muscle tone after neurogenicshock.
• Paraplegics who have lower motor neuron (LMN) injuries (belowL1 and L2) will convert to a flaccid type of paralysis.
• Clients who have UMN injuries will develop a spastic bladder afterthe neurogenic shock resolves.
• Clients who have LMN injuries will develop a flaccid bladder.• Bladder management options for males and females include
intermittent catheterization and Crede’s method (downwardpressure placed on the bladder to manually express the urine).
• Muscle strength and tone – After determining the baseline,monitor for an increasing loss of muscle strength in the affectedextremities.
• Clients who have upper motor neuron (UMN) injuries (above L1and L2) will convert to a spastic muscle tone after neurogenicshock.
• Paraplegics who have lower motor neuron (LMN) injuries (belowL1 and L2) will convert to a flaccid type of paralysis.
• Clients who have UMN injuries will develop a spastic bladder afterthe neurogenic shock resolves.
• Clients who have LMN injuries will develop a flaccid bladder.• Bladder management options for males and females include
intermittent catheterization and Crede’s method (downwardpressure placed on the bladder to manually express the urine).
• Muscle strength and tone – After determining the baseline,monitor for an increasing loss of muscle strength in the affectedextremities.
• Clients who have upper motor neuron (UMN) injuries (above L1and L2) will convert to a spastic muscle tone after neurogenicshock.
• Paraplegics who have lower motor neuron (LMN) injuries (belowL1 and L2) will convert to a flaccid type of paralysis.
• Clients who have UMN injuries will develop a spastic bladder afterthe neurogenic shock resolves.
• Clients who have LMN injuries will develop a flaccid bladder.• Bladder management options for males and females include
intermittent catheterization and Crede’s method (downwardpressure placed on the bladder to manually express the urine).
• Muscle strength and tone – After determining the baseline,monitor for an increasing loss of muscle strength in the affectedextremities.
• Clients who have upper motor neuron (UMN) injuries (above L1and L2) will convert to a spastic muscle tone after neurogenicshock.
• Paraplegics who have lower motor neuron (LMN) injuries (belowL1 and L2) will convert to a flaccid type of paralysis.
• Clients who have UMN injuries will develop a spastic bladder afterthe neurogenic shock resolves.
• Clients who have LMN injuries will develop a flaccid bladder.• Bladder management options for males and females include
intermittent catheterization and Crede’s method (downwardpressure placed on the bladder to manually express the urine).

• Gastrointestinal function – An ileus can developimmediately after injury. Monitor for bowelsounds.
• Skin Integrity – Changing the client’s positionevery 2 hr is critical (every 1 hr when in awheelchair).
• Encourage active range-of-motion (ROM)exercises when possible and assist with passiveROM if the client lacks all motor function.
• Pressure-relief devices in both the bed and thewheelchair must be consistently used.
• Gastrointestinal function – An ileus can developimmediately after injury. Monitor for bowelsounds.
• Skin Integrity – Changing the client’s positionevery 2 hr is critical (every 1 hr when in awheelchair).
• Encourage active range-of-motion (ROM)exercises when possible and assist with passiveROM if the client lacks all motor function.
• Pressure-relief devices in both the bed and thewheelchair must be consistently used.
• Gastrointestinal function – An ileus can developimmediately after injury. Monitor for bowelsounds.
• Skin Integrity – Changing the client’s positionevery 2 hr is critical (every 1 hr when in awheelchair).
• Encourage active range-of-motion (ROM)exercises when possible and assist with passiveROM if the client lacks all motor function.
• Pressure-relief devices in both the bed and thewheelchair must be consistently used.
• Gastrointestinal function – An ileus can developimmediately after injury. Monitor for bowelsounds.
• Skin Integrity – Changing the client’s positionevery 2 hr is critical (every 1 hr when in awheelchair).
• Encourage active range-of-motion (ROM)exercises when possible and assist with passiveROM if the client lacks all motor function.
• Pressure-relief devices in both the bed and thewheelchair must be consistently used.

Traction• Clients who have cervical fractures may be placed in a
halo fixation device or cervical tongs to providetraction and/or immobilize the spinal column.
• Nursing Actions– Maintain body alignment and ensure cervical tong weights
hang freely.– Monitor skin integrity by providing pin care and assessing
the skin under the halo fixation vest as appropriate.– Do not use the halo device to turn or move a client.
• Client Education– If the client goes home with a halo fixation device on,
provide instruction on pin and vest care.– Teach the client signs of infection and skin breakdown.
• Clients who have cervical fractures may be placed in ahalo fixation device or cervical tongs to providetraction and/or immobilize the spinal column.
• Nursing Actions– Maintain body alignment and ensure cervical tong weights
hang freely.– Monitor skin integrity by providing pin care and assessing
the skin under the halo fixation vest as appropriate.– Do not use the halo device to turn or move a client.
• Client Education– If the client goes home with a halo fixation device on,
provide instruction on pin and vest care.– Teach the client signs of infection and skin breakdown.
• Clients who have cervical fractures may be placed in ahalo fixation device or cervical tongs to providetraction and/or immobilize the spinal column.
• Nursing Actions– Maintain body alignment and ensure cervical tong weights
hang freely.– Monitor skin integrity by providing pin care and assessing
the skin under the halo fixation vest as appropriate.– Do not use the halo device to turn or move a client.
• Client Education– If the client goes home with a halo fixation device on,
provide instruction on pin and vest care.– Teach the client signs of infection and skin breakdown.
• Clients who have cervical fractures may be placed in ahalo fixation device or cervical tongs to providetraction and/or immobilize the spinal column.
• Nursing Actions– Maintain body alignment and ensure cervical tong weights
hang freely.– Monitor skin integrity by providing pin care and assessing
the skin under the halo fixation vest as appropriate.– Do not use the halo device to turn or move a client.
• Client Education– If the client goes home with a halo fixation device on,
provide instruction on pin and vest care.– Teach the client signs of infection and skin breakdown.


Halo Traction• The client with a halo fixation device should be taught
to use of a walker and rubber-soled shoes to preventfalls and injury.
• It is helpful for the client to scan the environmentvisually because the client's peripheral vision isdiminished from keeping the neck in a stationaryposition.
• The client with a halo fixation device should avoidbending at the waist because the halo vest is heavy,and the client's trunk is limited in flexibility.
• The nurse instructs the client and family that the metalframe on the device is never used to move or lift theclient because this will disrupt the attachment to theclient's skull, which is stabilizing the fracture.
• The client with a halo fixation device should be taughtto use of a walker and rubber-soled shoes to preventfalls and injury.
• It is helpful for the client to scan the environmentvisually because the client's peripheral vision isdiminished from keeping the neck in a stationaryposition.
• The client with a halo fixation device should avoidbending at the waist because the halo vest is heavy,and the client's trunk is limited in flexibility.
• The nurse instructs the client and family that the metalframe on the device is never used to move or lift theclient because this will disrupt the attachment to theclient's skull, which is stabilizing the fracture.
• The client with a halo fixation device should be taughtto use of a walker and rubber-soled shoes to preventfalls and injury.
• It is helpful for the client to scan the environmentvisually because the client's peripheral vision isdiminished from keeping the neck in a stationaryposition.
• The client with a halo fixation device should avoidbending at the waist because the halo vest is heavy,and the client's trunk is limited in flexibility.
• The nurse instructs the client and family that the metalframe on the device is never used to move or lift theclient because this will disrupt the attachment to theclient's skull, which is stabilizing the fracture.
• The client with a halo fixation device should be taughtto use of a walker and rubber-soled shoes to preventfalls and injury.
• It is helpful for the client to scan the environmentvisually because the client's peripheral vision isdiminished from keeping the neck in a stationaryposition.
• The client with a halo fixation device should avoidbending at the waist because the halo vest is heavy,and the client's trunk is limited in flexibility.
• The nurse instructs the client and family that the metalframe on the device is never used to move or lift theclient because this will disrupt the attachment to theclient's skull, which is stabilizing the fracture.

ComplicationsOrthostatic hypotension• Occurs when clients change position due to the
interruption in functioning of the automaticnervous system and pooling of blood in lowerextremities when in an upright position.
• Nursing Actions– Change the client’s positioning slowly and place the
client in a wheelchair that reclines.– Use thigh-high elastic hose or elastic wraps to increase
venous return.– Elastic wraps may need to extend all the way up the
client’s legs and include the client’s abdomen.
Orthostatic hypotension• Occurs when clients change position due to the
interruption in functioning of the automaticnervous system and pooling of blood in lowerextremities when in an upright position.
• Nursing Actions– Change the client’s positioning slowly and place the
client in a wheelchair that reclines.– Use thigh-high elastic hose or elastic wraps to increase
venous return.– Elastic wraps may need to extend all the way up the
client’s legs and include the client’s abdomen.
Orthostatic hypotension• Occurs when clients change position due to the
interruption in functioning of the automaticnervous system and pooling of blood in lowerextremities when in an upright position.
• Nursing Actions– Change the client’s positioning slowly and place the
client in a wheelchair that reclines.– Use thigh-high elastic hose or elastic wraps to increase
venous return.– Elastic wraps may need to extend all the way up the
client’s legs and include the client’s abdomen.
Orthostatic hypotension• Occurs when clients change position due to the
interruption in functioning of the automaticnervous system and pooling of blood in lowerextremities when in an upright position.
• Nursing Actions– Change the client’s positioning slowly and place the
client in a wheelchair that reclines.– Use thigh-high elastic hose or elastic wraps to increase
venous return.– Elastic wraps may need to extend all the way up the
client’s legs and include the client’s abdomen.

• Neurogenic shock/spinal shock– Neurogenic shock is a common response of the spinal
cord following an injury.– Areflexia characterizes spinal shock; therefore,
reflexes would provide the best information aboutrecovery.
– Symptoms of bradycardia, hypotension, flaccidparalysis, loss of reflex activity below level of injury,and paralytic ileus accompany neurogenic shock dueto the loss of autonomic function.
• Nursing Actions– Monitor vital signs for hypotension and bradycardia.– Treat symptoms with appropriate medications
(vasopressors or atropine).– Normal saline 0.9% - an isotonic solution
• Neurogenic shock/spinal shock– Neurogenic shock is a common response of the spinal
cord following an injury.– Areflexia characterizes spinal shock; therefore,
reflexes would provide the best information aboutrecovery.
– Symptoms of bradycardia, hypotension, flaccidparalysis, loss of reflex activity below level of injury,and paralytic ileus accompany neurogenic shock dueto the loss of autonomic function.
• Nursing Actions– Monitor vital signs for hypotension and bradycardia.– Treat symptoms with appropriate medications
(vasopressors or atropine).– Normal saline 0.9% - an isotonic solution
• Neurogenic shock/spinal shock– Neurogenic shock is a common response of the spinal
cord following an injury.– Areflexia characterizes spinal shock; therefore,
reflexes would provide the best information aboutrecovery.
– Symptoms of bradycardia, hypotension, flaccidparalysis, loss of reflex activity below level of injury,and paralytic ileus accompany neurogenic shock dueto the loss of autonomic function.
• Nursing Actions– Monitor vital signs for hypotension and bradycardia.– Treat symptoms with appropriate medications
(vasopressors or atropine).– Normal saline 0.9% - an isotonic solution
• Neurogenic shock/spinal shock– Neurogenic shock is a common response of the spinal
cord following an injury.– Areflexia characterizes spinal shock; therefore,
reflexes would provide the best information aboutrecovery.
– Symptoms of bradycardia, hypotension, flaccidparalysis, loss of reflex activity below level of injury,and paralytic ileus accompany neurogenic shock dueto the loss of autonomic function.
• Nursing Actions– Monitor vital signs for hypotension and bradycardia.– Treat symptoms with appropriate medications
(vasopressors or atropine).– Normal saline 0.9% - an isotonic solution

• Autonomic dysreflexia– Occurs secondary to the stimulation of the sympathetic
nervous system and inadequate compensatory responseby the parasympathetic nervous system.
– Clients who have lesions below T6 do not experiencedysreflexia because the parasympathetic nervous systemis able to neutralize the sympathetic response.
– Stimulation of the sympathetic nervous system causesextreme hypertension, sudden severe headache, pallorbelow the level of the spinal cord’s lesion dermatome,blurred vision, diaphoresis, restlessness, nausea, andpiloerection (goose bumps).
– Autonomic dysreflexia is a potentially life-threateningcondition and may be triggered by bladder distention,bowel distention, visceral distention, or stimulation of painreceptors in the skin. A daily bowel program eliminates thistrigger.
• Autonomic dysreflexia– Occurs secondary to the stimulation of the sympathetic
nervous system and inadequate compensatory responseby the parasympathetic nervous system.
– Clients who have lesions below T6 do not experiencedysreflexia because the parasympathetic nervous systemis able to neutralize the sympathetic response.
– Stimulation of the sympathetic nervous system causesextreme hypertension, sudden severe headache, pallorbelow the level of the spinal cord’s lesion dermatome,blurred vision, diaphoresis, restlessness, nausea, andpiloerection (goose bumps).
– Autonomic dysreflexia is a potentially life-threateningcondition and may be triggered by bladder distention,bowel distention, visceral distention, or stimulation of painreceptors in the skin. A daily bowel program eliminates thistrigger.
• Autonomic dysreflexia– Occurs secondary to the stimulation of the sympathetic
nervous system and inadequate compensatory responseby the parasympathetic nervous system.
– Clients who have lesions below T6 do not experiencedysreflexia because the parasympathetic nervous systemis able to neutralize the sympathetic response.
– Stimulation of the sympathetic nervous system causesextreme hypertension, sudden severe headache, pallorbelow the level of the spinal cord’s lesion dermatome,blurred vision, diaphoresis, restlessness, nausea, andpiloerection (goose bumps).
– Autonomic dysreflexia is a potentially life-threateningcondition and may be triggered by bladder distention,bowel distention, visceral distention, or stimulation of painreceptors in the skin. A daily bowel program eliminates thistrigger.
• Autonomic dysreflexia– Occurs secondary to the stimulation of the sympathetic
nervous system and inadequate compensatory responseby the parasympathetic nervous system.
– Clients who have lesions below T6 do not experiencedysreflexia because the parasympathetic nervous systemis able to neutralize the sympathetic response.
– Stimulation of the sympathetic nervous system causesextreme hypertension, sudden severe headache, pallorbelow the level of the spinal cord’s lesion dermatome,blurred vision, diaphoresis, restlessness, nausea, andpiloerection (goose bumps).
– Autonomic dysreflexia is a potentially life-threateningcondition and may be triggered by bladder distention,bowel distention, visceral distention, or stimulation of painreceptors in the skin. A daily bowel program eliminates thistrigger.

PEDIATRIC CONSIDERATIONSNeurology

Hydrocephalus– Description
• Results in head enlargement (prior tofontanels closing), increased ICP
– Types• Communicating: Result of impaired
absorption within subarachnoid space• Noncommunicating: Obstruction of
cerebrospinal fluid (CSF) flow withinventricular system
Hydrocephalus– Description
• Results in head enlargement (prior tofontanels closing), increased ICP
– Types• Communicating: Result of impaired
absorption within subarachnoid space• Noncommunicating: Obstruction of
cerebrospinal fluid (CSF) flow withinventricular system
Hydrocephalus– Description
• Results in head enlargement (prior tofontanels closing), increased ICP
– Types• Communicating: Result of impaired
absorption within subarachnoid space• Noncommunicating: Obstruction of
cerebrospinal fluid (CSF) flow withinventricular system
Hydrocephalus– Description
• Results in head enlargement (prior tofontanels closing), increased ICP
– Types• Communicating: Result of impaired
absorption within subarachnoid space• Noncommunicating: Obstruction of
cerebrospinal fluid (CSF) flow withinventricular system

HydrocephalusAssessment
• Infant: Increased head circumference; wideningsutures; bulging fontanel; dilated scalp veins;frontal bossing; sunsetting eyes
• If the head circumference is greater than orequal to 4 cm larger than the chestcircumference, this can be an indication ofhydrocephalus
• Child: Irritability; lethargy; headache onawakening; nausea and vomiting; ataxia;nystagmus
HydrocephalusAssessment
• Infant: Increased head circumference; wideningsutures; bulging fontanel; dilated scalp veins;frontal bossing; sunsetting eyes
• If the head circumference is greater than orequal to 4 cm larger than the chestcircumference, this can be an indication ofhydrocephalus
• Child: Irritability; lethargy; headache onawakening; nausea and vomiting; ataxia;nystagmus
HydrocephalusAssessment
• Infant: Increased head circumference; wideningsutures; bulging fontanel; dilated scalp veins;frontal bossing; sunsetting eyes
• If the head circumference is greater than orequal to 4 cm larger than the chestcircumference, this can be an indication ofhydrocephalus
• Child: Irritability; lethargy; headache onawakening; nausea and vomiting; ataxia;nystagmus
HydrocephalusAssessment
• Infant: Increased head circumference; wideningsutures; bulging fontanel; dilated scalp veins;frontal bossing; sunsetting eyes
• If the head circumference is greater than orequal to 4 cm larger than the chestcircumference, this can be an indication ofhydrocephalus
• Child: Irritability; lethargy; headache onawakening; nausea and vomiting; ataxia;nystagmus

Hydrocephalus (continued)– Surgical interventions
• Goal of treatment to prevent further CSF accumulation bybypassing blockage, draining fluid from ventricles to locationwhere it may be reabsorbed
– Preoperative interventions• NPO status• Reposition head frequently to prevent pressure sores• Prepare the child and family for surgery
– Postoperative interventions• Position on nonoperative side to prevent pressure on shunt
valve• Keep flat as prescribed• Observe for increased ICP; if present, elevate head of bed 15 to
30 degrees
Hydrocephalus (continued)– Surgical interventions
• Goal of treatment to prevent further CSF accumulation bybypassing blockage, draining fluid from ventricles to locationwhere it may be reabsorbed
– Preoperative interventions• NPO status• Reposition head frequently to prevent pressure sores• Prepare the child and family for surgery
– Postoperative interventions• Position on nonoperative side to prevent pressure on shunt
valve• Keep flat as prescribed• Observe for increased ICP; if present, elevate head of bed 15 to
30 degrees
Hydrocephalus (continued)– Surgical interventions
• Goal of treatment to prevent further CSF accumulation bybypassing blockage, draining fluid from ventricles to locationwhere it may be reabsorbed
– Preoperative interventions• NPO status• Reposition head frequently to prevent pressure sores• Prepare the child and family for surgery
– Postoperative interventions• Position on nonoperative side to prevent pressure on shunt
valve• Keep flat as prescribed• Observe for increased ICP; if present, elevate head of bed 15 to
30 degrees
Hydrocephalus (continued)– Surgical interventions
• Goal of treatment to prevent further CSF accumulation bybypassing blockage, draining fluid from ventricles to locationwhere it may be reabsorbed
– Preoperative interventions• NPO status• Reposition head frequently to prevent pressure sores• Prepare the child and family for surgery
– Postoperative interventions• Position on nonoperative side to prevent pressure on shunt
valve• Keep flat as prescribed• Observe for increased ICP; if present, elevate head of bed 15 to
30 degrees

Spina Bifida– Description
• Central nervous system (CNS) defect occurs as result of neural tubefailure to close during embryonic development
– Types• Spina Bifida Occulta• Spina Bifida Cystica - Meningocele , Myelomeningocele
– Assessment• Depends on spinal cord involvement; visible spinal defect; flaccid
paralysis of legs; altered bladder, bowel function; hip, jointdeformities
– Interventions• Protect sac by covering with sterile, moist, nonadherent dressing as
prescribed; change every 2 to 4 hours as prescribed• Prone position• Aseptic technique
Spina Bifida– Description
• Central nervous system (CNS) defect occurs as result of neural tubefailure to close during embryonic development
– Types• Spina Bifida Occulta• Spina Bifida Cystica - Meningocele , Myelomeningocele
– Assessment• Depends on spinal cord involvement; visible spinal defect; flaccid
paralysis of legs; altered bladder, bowel function; hip, jointdeformities
– Interventions• Protect sac by covering with sterile, moist, nonadherent dressing as
prescribed; change every 2 to 4 hours as prescribed• Prone position• Aseptic technique
Spina Bifida– Description
• Central nervous system (CNS) defect occurs as result of neural tubefailure to close during embryonic development
– Types• Spina Bifida Occulta• Spina Bifida Cystica - Meningocele , Myelomeningocele
– Assessment• Depends on spinal cord involvement; visible spinal defect; flaccid
paralysis of legs; altered bladder, bowel function; hip, jointdeformities
– Interventions• Protect sac by covering with sterile, moist, nonadherent dressing as
prescribed; change every 2 to 4 hours as prescribed• Prone position• Aseptic technique
Spina Bifida– Description
• Central nervous system (CNS) defect occurs as result of neural tubefailure to close during embryonic development
– Types• Spina Bifida Occulta• Spina Bifida Cystica - Meningocele , Myelomeningocele
– Assessment• Depends on spinal cord involvement; visible spinal defect; flaccid
paralysis of legs; altered bladder, bowel function; hip, jointdeformities
– Interventions• Protect sac by covering with sterile, moist, nonadherent dressing as
prescribed; change every 2 to 4 hours as prescribed• Prone position• Aseptic technique



Nursing care (Spina Bifida)
• Protect the membrane with a sterile covering andplastic to prevent drying.
• Observe for leakage of the cerebrospinal fluid.• Handle the newborn gently by positioning him prone
or to the side to prevent trauma.• Prevent infection by keeping the area free from
contamination by urine and feces.• Measure the circumference of the newborn’s head to
identify hydrocephalus.• Assess the newborn for increased intracranial pressure.
• Protect the membrane with a sterile covering andplastic to prevent drying.
• Observe for leakage of the cerebrospinal fluid.• Handle the newborn gently by positioning him prone
or to the side to prevent trauma.• Prevent infection by keeping the area free from
contamination by urine and feces.• Measure the circumference of the newborn’s head to
identify hydrocephalus.• Assess the newborn for increased intracranial pressure.
• Protect the membrane with a sterile covering andplastic to prevent drying.
• Observe for leakage of the cerebrospinal fluid.• Handle the newborn gently by positioning him prone
or to the side to prevent trauma.• Prevent infection by keeping the area free from
contamination by urine and feces.• Measure the circumference of the newborn’s head to
identify hydrocephalus.• Assess the newborn for increased intracranial pressure.
• Protect the membrane with a sterile covering andplastic to prevent drying.
• Observe for leakage of the cerebrospinal fluid.• Handle the newborn gently by positioning him prone
or to the side to prevent trauma.• Prevent infection by keeping the area free from
contamination by urine and feces.• Measure the circumference of the newborn’s head to
identify hydrocephalus.• Assess the newborn for increased intracranial pressure.

Reyes Syndrome– Description
• Acute encephalopathy that follows viral illness; characterized by cerebraledema, fatty changes in liver
• Administration of aspirin not recommended for children with varicella orinfluenza
• Acetaminophen (Tylenol) considered medication of choice for pediatricclients
• Goal of treatment is maintenance of effective cerebral perfusion, control ofincreasing ICP
– Assessment• History of systemic viral illness 4 to 7 days preceding onset of symptoms;
malaise; nausea and vomiting; progressive neurological deterioration– Interventions
• Frequent monitoring of neurological status• Monitor intake and output• Provide rest• Decrease environmental stimuli• Monitor for signs of bleeding, impaired coagulation• Monitor liver function studies
Reyes Syndrome– Description
• Acute encephalopathy that follows viral illness; characterized by cerebraledema, fatty changes in liver
• Administration of aspirin not recommended for children with varicella orinfluenza
• Acetaminophen (Tylenol) considered medication of choice for pediatricclients
• Goal of treatment is maintenance of effective cerebral perfusion, control ofincreasing ICP
– Assessment• History of systemic viral illness 4 to 7 days preceding onset of symptoms;
malaise; nausea and vomiting; progressive neurological deterioration– Interventions
• Frequent monitoring of neurological status• Monitor intake and output• Provide rest• Decrease environmental stimuli• Monitor for signs of bleeding, impaired coagulation• Monitor liver function studies
Reyes Syndrome– Description
• Acute encephalopathy that follows viral illness; characterized by cerebraledema, fatty changes in liver
• Administration of aspirin not recommended for children with varicella orinfluenza
• Acetaminophen (Tylenol) considered medication of choice for pediatricclients
• Goal of treatment is maintenance of effective cerebral perfusion, control ofincreasing ICP
– Assessment• History of systemic viral illness 4 to 7 days preceding onset of symptoms;
malaise; nausea and vomiting; progressive neurological deterioration– Interventions
• Frequent monitoring of neurological status• Monitor intake and output• Provide rest• Decrease environmental stimuli• Monitor for signs of bleeding, impaired coagulation• Monitor liver function studies
Reyes Syndrome– Description
• Acute encephalopathy that follows viral illness; characterized by cerebraledema, fatty changes in liver
• Administration of aspirin not recommended for children with varicella orinfluenza
• Acetaminophen (Tylenol) considered medication of choice for pediatricclients
• Goal of treatment is maintenance of effective cerebral perfusion, control ofincreasing ICP
– Assessment• History of systemic viral illness 4 to 7 days preceding onset of symptoms;
malaise; nausea and vomiting; progressive neurological deterioration– Interventions
• Frequent monitoring of neurological status• Monitor intake and output• Provide rest• Decrease environmental stimuli• Monitor for signs of bleeding, impaired coagulation• Monitor liver function studies

Cerebral Palsy– Description
• Disorder characterized by impaired movement and posture; results fromabnormality in extrapyramidal or pyramidal motor system
– Assessment• Abnormal posturing, such as opisthotonos (exaggerated arching of back)• Stiff and rigid arms and legs• Feeding difficulties• Delayed gross motor activity• Alterations of muscle tone• Persistence of primitive infantile reflexes
– Interventions• Assess developmental level• Encourage early intervention programs• Prepare for use of mobilizing devices• Provide safe environment• Provide safe, developmentally appropriate toys• Position upright after meals• Administer muscle relaxants as prescribed
Cerebral Palsy– Description
• Disorder characterized by impaired movement and posture; results fromabnormality in extrapyramidal or pyramidal motor system
– Assessment• Abnormal posturing, such as opisthotonos (exaggerated arching of back)• Stiff and rigid arms and legs• Feeding difficulties• Delayed gross motor activity• Alterations of muscle tone• Persistence of primitive infantile reflexes
– Interventions• Assess developmental level• Encourage early intervention programs• Prepare for use of mobilizing devices• Provide safe environment• Provide safe, developmentally appropriate toys• Position upright after meals• Administer muscle relaxants as prescribed



• A nurse is caring for a client who has justbeen admitted following surgical evacuationof a subdural hematoma. Which of thefollowing is the priority assessment?
• A. Glasgow Coma Scale• B. Cranial nerve function• C. Oxygen saturation• D. Pupillary response
• A nurse is caring for a client who has justbeen admitted following surgical evacuationof a subdural hematoma. Which of thefollowing is the priority assessment?
• A. Glasgow Coma Scale• B. Cranial nerve function• C. Oxygen saturation• D. Pupillary response

• A. INCORRECT: The Glasgow Coma Scale is importantbut not the priority assessment at this time.
• B. INCORRECT: Assessment of cranial nerve function isimportant but not the priority assessment at this time.
• C. CORRECT: Using the airway, breathing, andcirculation (ABC) priority-setting framework,assessment of oxygen saturation is the priority action.Brain tissue can only survive for 3 min beforepermanent damage occurs.
• D. INCORRECT: Assessment of pupillary response isimportant but not the priority assessment at this time.
• A. INCORRECT: The Glasgow Coma Scale is importantbut not the priority assessment at this time.
• B. INCORRECT: Assessment of cranial nerve function isimportant but not the priority assessment at this time.
• C. CORRECT: Using the airway, breathing, andcirculation (ABC) priority-setting framework,assessment of oxygen saturation is the priority action.Brain tissue can only survive for 3 min beforepermanent damage occurs.
• D. INCORRECT: Assessment of pupillary response isimportant but not the priority assessment at this time.

• A nursing is caring for a client who has a closed-head injury with ICP readings range from 16 to 22mm Hg. Which of the following actions shouldthe nurse take to decrease the potential forraising the client’s ICP? (Select all that apply.)
• A. Suction the endotracheal tube.• B. Hyperventilate the client.• C. Elevate the client’s head on two pillows.• D. Administer a stool softener.• E. Keep the client well hydrated.
• A nursing is caring for a client who has a closed-head injury with ICP readings range from 16 to 22mm Hg. Which of the following actions shouldthe nurse take to decrease the potential forraising the client’s ICP? (Select all that apply.)
• A. Suction the endotracheal tube.• B. Hyperventilate the client.• C. Elevate the client’s head on two pillows.• D. Administer a stool softener.• E. Keep the client well hydrated.

• A. INCORRECT: Suctioning increases ICP and should be doneonly when indicated.
• B. CORRECT: Hyperventilation of the client will preventhypercarbia, which can cause vasodilation with a secondaryincrease in ICP.
• C. INCORRECT: Hyperflexion of the client’s neck with pillowscarries the risk of increasing ICP and should be avoided.
• D. CORRECT: Administration of a stool softener willdecrease the need to bear down (Valsalva maneuver)during bowel movements, which can increase ICP.
• E. INCORRECT: Overhydration carries the risk of increasingICP and should be avoided.
• A. INCORRECT: Suctioning increases ICP and should be doneonly when indicated.
• B. CORRECT: Hyperventilation of the client will preventhypercarbia, which can cause vasodilation with a secondaryincrease in ICP.
• C. INCORRECT: Hyperflexion of the client’s neck with pillowscarries the risk of increasing ICP and should be avoided.
• D. CORRECT: Administration of a stool softener willdecrease the need to bear down (Valsalva maneuver)during bowel movements, which can increase ICP.
• E. INCORRECT: Overhydration carries the risk of increasingICP and should be avoided.

• A nurse in the critical care unit is completing anadmission assessment of a client who has agunshot wound to the head. Which of thefollowing assessment findings are indicative ofincreased ICP? (Select all that apply.)
• A. Headache• B. Dilated pupils• C. Tachycardia• D. Decorticate posturing• E. Hypotension
• A nurse in the critical care unit is completing anadmission assessment of a client who has agunshot wound to the head. Which of thefollowing assessment findings are indicative ofincreased ICP? (Select all that apply.)
• A. Headache• B. Dilated pupils• C. Tachycardia• D. Decorticate posturing• E. Hypotension

• A. CORRECT: Headache is a finding associatedwith increased ICP.
• B. CORRECT: Dilated pupils is a finding associatedwith increased ICP.
• C. INCORRECT: Bradycardia, not tachycardia, is afinding associated with increased ICP.
• D. CORRECT: Decorticate or decerebrateposturing is a finding associated with increasedICP.
• E. INCORRECT: Hypertension, not hypotension, isa finding associated with increased ICP.
• A. CORRECT: Headache is a finding associatedwith increased ICP.
• B. CORRECT: Dilated pupils is a finding associatedwith increased ICP.
• C. INCORRECT: Bradycardia, not tachycardia, is afinding associated with increased ICP.
• D. CORRECT: Decorticate or decerebrateposturing is a finding associated with increasedICP.
• E. INCORRECT: Hypertension, not hypotension, isa finding associated with increased ICP.

• A nurse is planning care for a client who has dysphagiaand has a new dietary prescription. Which of thefollowing should the nurse include in the plan of care?(Select all that apply.)
• A. Have suction equipment available for use.• B. Use thickened liquids.• C. Place food on the client’s unaffected side of her
mouth.• D. Assign an assistive personnel to feed the client
slowly.• E. Teach the client to swallow with her neck flexed.
• A nurse is planning care for a client who has dysphagiaand has a new dietary prescription. Which of thefollowing should the nurse include in the plan of care?(Select all that apply.)
• A. Have suction equipment available for use.• B. Use thickened liquids.• C. Place food on the client’s unaffected side of her
mouth.• D. Assign an assistive personnel to feed the client
slowly.• E. Teach the client to swallow with her neck flexed.

• A. CORRECT: Have suction equipment available for use is correct.Suction equipment should be available in case of choking andaspiration.
• B. CORRECT: The client should be given thickened liquids, which areeasier to swallow.
• C. CORRECT: Placing food on the unaffected side of the client’smouth will allow her to have better control of the food and reducethe risk of aspiration.
• D. INCORRECT: Due to the risk of aspiration, an assistive personnelshould not be assigned to feed the client because the client’sswallowing ability should be assessed, and suctioning may beneeded if choking occurs.
• E. CORRECT: The client should be taught to flex her neck, tuckingthe chin down and under, to close the epiglottis during swallowing.
• A. CORRECT: Have suction equipment available for use is correct.Suction equipment should be available in case of choking andaspiration.
• B. CORRECT: The client should be given thickened liquids, which areeasier to swallow.
• C. CORRECT: Placing food on the unaffected side of the client’smouth will allow her to have better control of the food and reducethe risk of aspiration.
• D. INCORRECT: Due to the risk of aspiration, an assistive personnelshould not be assigned to feed the client because the client’sswallowing ability should be assessed, and suctioning may beneeded if choking occurs.
• E. CORRECT: The client should be taught to flex her neck, tuckingthe chin down and under, to close the epiglottis during swallowing.

• A nurse is assessing a client who hasexperienced a left-hemispheric stroke. Whichof the following is an expected finding?
• A. Impulse control difficulty• B. Poor judgment• C. Inability to recognize familiar objects• D. Loss of depth perception
• A nurse is assessing a client who hasexperienced a left-hemispheric stroke. Whichof the following is an expected finding?
• A. Impulse control difficulty• B. Poor judgment• C. Inability to recognize familiar objects• D. Loss of depth perception

• A. Incorrect: A client who has experienced a right-hemispheric stroke will experience difficulty withimpulse control.
• B. Incorrect: A client who has experienced a right-hemispheric stroke will experience poor judgment.
• C. CORRECT: A client who experienced a left-hemispheric stroke will demonstrate the inability torecognize familiar objects. This is also known asagnosia.
• D. Incorrect: A client who experienced a right-hemispheric stroke will experience a loss of depthperception.
• A. Incorrect: A client who has experienced a right-hemispheric stroke will experience difficulty withimpulse control.
• B. Incorrect: A client who has experienced a right-hemispheric stroke will experience poor judgment.
• C. CORRECT: A client who experienced a left-hemispheric stroke will demonstrate the inability torecognize familiar objects. This is also known asagnosia.
• D. Incorrect: A client who experienced a right-hemispheric stroke will experience a loss of depthperception.