Rn grand rounds may 2012
34
RN GRAND ROUNDS May 16th, 2012 Thursday, May 17, 12
-
Upload
steven-costalas -
Category
Health & Medicine
-
view
254 -
download
0
description
I do nursing grand rounds for our busy ER. It allows MDs to interface with RNs and discuss though processes, lab testing, studies and how we can all give better care.
Transcript of Rn grand rounds may 2012

RN GRAND ROUNDSMay 16th, 2012
Thursday, May 17, 12

CASE 1
22 yo M , college student
CC: Nausea / Vomiting
PMH: ADHD/ Anxiety
Meds: Adderall
HPI: 3 day hx of N/V, this is his third visit for same
Thursday, May 17, 12

CASE 1- N/V
Vitals: 152/81, P 103, RR 16, T 97.5, Sat 100% RA
Pt seen two other times for same and sent home
IVF, Zofran IV, Compazine PR, CT head neg, K+ was 3.0
Rash on back noted by RN, did not look like Erythema chronicum migrans “bullseye”
Maybe there for several months according to the ID consult
Lyme titer added to labs
Thursday, May 17, 12

WORKUP
Admitted to medicine for workup
CT abdomen was neg
ID consulted for positive Lyme titer ( ELISA)
Western blot added (confirmatory test)
Thursday, May 17, 12

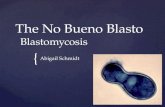
ECM RASH
Note “bullseye pattern” typical for Lyme Disease
Thursday, May 17, 12

LAB TESTS
Laboratory blood tests are helpful if used correctly and performed with validated methods. Laboratory tests are not recommended for patients who do not have symptoms typical of Lyme disease. Just as it is important to correctly diagnose Lyme disease when a patient has it, it is important to avoid misdiagnosis and treatment of Lyme disease when the true cause of the illness is something else.
Source: cdc.gov
Thursday, May 17, 12

LYME TITER
http://www.cdc.gov/lyme/diagnosistreatment/LabTest/TwoStep/
Thursday, May 17, 12

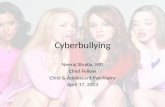
WESTERN BLOT
The confirmatory test for a positive Lyme titer
Many false positives occur with with the Lyme titer
This clarifies equivocal or positive tests
Western Blot sub-fractionates the IgG and IgM
Thursday, May 17, 12

WESTERN BLOT
For Positive Results you must have:
An lgG Western Blot must have five or more of these bands: 18, 21,28, 30, 39, 41,,45, 58, 66 and 93 kDa.
An lgM Western Blot must have two or more these three bands: 23, 39, 41
Source: www.whatislyme.com
Thursday, May 17, 12

OUR PATIENT’S WB
IgG - Negative overallonly 2 bands posProb no chronic infection
IgM- 2 of 3 are positivepresumes acute infection
Thursday, May 17, 12

WB DISCLAIMER
Thursday, May 17, 12

SUMMARY
False positives on the initial Lyme titer and Western blot can occur
Routine testing without actual symptoms causes unnecessary concern, further testing and treatments
Much controversy exists on the actual interpretation of Western blot
Thursday, May 17, 12

WESTERN BLOT
False-positive reactions may occur with patients with other spirochetal diseases (syphilis, yaws, pinta, relapsing fever, or leptospirosis), influenza, autoimmune disorders, multiple sclerosis, or amyotrophic lateral sclerosis.
http://www.mayomedicallaboratories.com/interpretive-guide
Thursday, May 17, 12

CASE 2
22yo F Status post delivery of twins 6 days ago
CC: Headache/ HTN since yesterday
Pain 6/10
PMH: Asthma, Migraine, Pre ecclampsia (RN note)
Arrival 1414hrs, PA time 1448 hrs in FT
BP:144/69 in triage
Thursday, May 17, 12

MD NOTE
2 days of HA
Hx migraines, this was “more severe”
BP running high, repeat in ER at 1651 hrs at 175/99, 1705 hrs Gyn consulted
1739hrs at 189/114
1740 hrs Labetalol 10mg IV
1849hrs Hydralazine ordered IV ? in MD note, not RN
1911 Magnesium IV ordered 4 grams over 15 mins
Thursday, May 17, 12

POST-PARTUM HA/ HTN
Thursday, May 17, 12

HTN IN PREGNANCY
Gestational HTN: found late in pregnancy, no other findings for preeclampsia, “transient” , clears by post partum week 12
Chronic HTN Preceding Pregnancy- ≥140/90, before 20 wks, persists beyond 12 weeks
Chronic HTN with PIH ( preeclamsia or eclampsia) highest risk
Thursday, May 17, 12

PREGNANCY INDUCED HTN
Preeclampsia- mild/ BP ≥ 140/90, > 20 wks gestation, no end organ damage, >300mg protein/ 24hrs.
Severe Preeclampsia- SBP ≥160/110, proteinuria > 5gr/ 24hr, Headache, Epigastric pain, Low PLT, Oligouria < 400mg/ 24hr, Pulmonary edema
Thursday, May 17, 12

PREECLAMPSIA RISK FACTORS
Nulliparity
Previous gestational hypertensive disorders
Diabetes
Malnutrition
Hydatiform mole
Low social status
Chronic Nephritis
Thursday, May 17, 12

PREECLAMPSIA SIGNS & SYMPTOMS
CNS: Headache, visual disturbances, altered mental status, blindness, weakness & malaise
Edema
Epigastric Pain
Dyspnea
Seizures- on top of the criteria for preeclampsia define Eclampsia
Thursday, May 17, 12

MANAGEMENT
Delivery is the only “cure”
HTN management
Hydralazine/ Labetalol IV/ Sodium nitroprusside
IV Magnesium - seizure prevention “eclampsia”
IV Fluids, patients are intravascularly depleted
Thursday, May 17, 12

HELLP SYNDROME
H- Hemolysis
EL- Elevated Liver Enzymes
LP- Low platelets
Occurs in 10-20% of women with Preeclampsia or Ecclampsia
Women usually have HTN/ Preeclampsia before HELLP syndrome is noted.
Thursday, May 17, 12

HELLP SYNDROME
Fatigue
Headache
N/V
Blurry vision
RUQ pain
Fluid retention/ edema
Thursday, May 17, 12

LABS
All women with new onset HTN: CBC, AST/ALT, BMP, Uric acid, LDH, Indirect Bilirubin, PT/PTT
HELLP: check Spot Protein (prot/creat ratio) > 0.3, Proteinuria > 300mg/ 24hr, Uric Acid> 5.6, Creat> 1.2
Also for HELLP: PLT < 100k, Elevated PT/ PTT, Decreased Fibrinogen, Hemolysis markers ( peripheral smear, Indirect Bili > 1.2, LDH>600)
Thursday, May 17, 12

OUR CASE
Pt was seen in triage. BP was144/69, RN noted home BP of 170/110
Pt had Headache, got Reglan (no note of vomiting on chart), had leg edema
Sent to Fast Track
MD involved after PA presentation
Thursday, May 17, 12

PREECLAMPSIA
Lessons learned.......
Thursday, May 17, 12

LACTIC ACIDOSIS
The product of anaerobic metabolism
Number one cause of metabolic acidosis
Causes anion gap
AG= Na⁺ - (Cl⁻ + HCO3⁻)
Bicarb (HCO3⁻) will be low
Lactate above 4meq/L is abnormal
Thursday, May 17, 12

LACTIC ACIDOSIS
Thursday, May 17, 12

METABOLIC ACIDOSIS
MUDPILES Methanol- metabolized to Formic Acid via liver enzymes, cellular hypoxia, blindness
Uremia- increased bicarb wasting leads to acidosis
DKA- ketone formation in the absence of insulin from fatty acid breakdown
Paraldehyde- sedative no longer in use
INH- inhibits lactate dehydrogenase
Lactic Acidosis- type A ( hypoperfusion) and type B ( DM, toxins,
Ethylene glycol- antifreeze degradation produces glycolic acid and oxalate
Salicylates- ie ASA overdose
Thursday, May 17, 12

METABOLIC ACIDOSIS
Anion gap- associated with an unmeasured anion produced or gained
Thursday, May 17, 12

TYPES OF LACTIC ACIDOSIS
Type A: from tissue hypoperfusion/ hypoxia
Type B- Drugs, DM, Liver disease, malignancy, inborn errors of metabolism
Thursday, May 17, 12

LACTIC ACIDOSIS
When to order?
Think of the situation.
Hypoxia- asthma, COPD, CHF
Increased Metabolic Activity- seizure, exercise, shivering ( doesn’t change management)
Sepsis- dead bowel, overwhelming infection, fever
Thursday, May 17, 12

SEPSIS
SIRS definition- Systemic Inflammatory Response Syndrome
Essentially a cytokine storm with abnormal
Thursday, May 17, 12

SEPSIS
SIRS due to an infection is SEPSIS
Non Sepsis Causes- trauma, burns, pancreatitis, ischemia and hemorrhage
Also- anaphylaxis, tamponade, PE, Adrenal insuff., complications of surgery, Overdoses
Complications- organ failure
Thursday, May 17, 12