Risk factors in Periodontal Disease
26
Risk Factors Associated with Periodontal Disease Dr. Samjhana Kashaju Joshi
-
Upload
neil-pande -
Category
Health & Medicine
-
view
11.925 -
download
0
description
Risk factors in Periodontal Disease
Transcript of Risk factors in Periodontal Disease

Risk Factors
Associated with
Periodontal Disease
Dr. Samjhana Kashaju Joshi

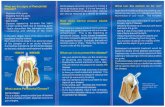
Periodontitis is an inflammatory condition
initiated by microbial plaque
influenced by an array of factors that affect the development and progression of the disease.

The development and course of periodontitis
depends upon
specific inherited, behavioral or environment conditions ---so called risk factors.
Risk factor --- can be modified Risk determinant---cannot be modified

Risk factors
Smoking Diabetes Stress Drugs Systemic disease Nutrition
Risk determinants
•Genetics•Socioeconomic status•Gender

Smoking
Major risk factor
Can be attributed to current or former smoking
Severity is directly related to both –the number of cigarettes smoked per day- the numbers of years a patient has smoked
Clinically---Smokers exhibit reduced gingival bleeding and inflammation---greater levels of periodontal pocketing in anterior maxillary segment
Impairment of local neutrophil function by tobacco smoke and its components
Affect the healing ability

Diabetes
Type 1 diabetes ( IDDM)
Type 2 diabetes ( NIDDM)
Factors contributing are---
The degree of diabetic control The age of onset The duration of the disease

Complex mechanism
a) Dysregulation of polymorph function b) Altered collagen metabolism c) Microvascular damage
“Share similar pathogenic mechanisms with diabetic foot ulcers”
Bi-directional relationship -- Diabetes and Periodontal disease
“Successful treatment and maintenance of periodontal health in diabetic patients should be a major goal, to improve
both the oral and general health of the patient”

Stress
Has impact on the normal functioning of the immune system
--Negative life events --Unemployment --Social strain
Mechanism
Specific periodontal pathogens can utilize stress hormones to stimulate growth and expression of virulence factors
providing another potential mechanism linking stress levels with periodontitis

Drugs
Anticonvulsant– Phenytion Immunosuppressant– Cyclosporin Calcium channel–blocking drugs as Nifedipine, Amlodipine
Induces gingival overgrowth classically begins in the inter-dental papillae

Complex interaction between
the drugs, host fibroblasts and inflammatory cells
resulting in an increased deposition of connective tissue
supporting a hyperproliferative epithelium
Difficulty in plaque control adds oedematous inflammatory
component to the overgrowth

Management should begin by change in medication in consultation with the patient’s physician.
Mechanical cleaning and meticulous plaque control.
Surgical removal of residual redundant tissue may also be required.

Systemic Disease
Tissue destruction associated with periodontitis results from the
host response to bacterial insult.
Bystander Damage---periodontal pathogens and the immune
response
Systemic conditions affect the host defense mechanism
--positive impact on disease progression

Systemic conditions and periodontitis

Nutrition
Potential role of diet and nutrition
Severe Vitamin C deficiency---Scorbutic gingivitis
Ulcerative gingivitis, gingival hemorrhage, rapid periodontal pocket formation, tooth loss
Vitamin- C – an important antioxidant
Role in the inhibition of reactive oxygen species (ROS)
tissue damage in periodontal disease

Genetic Factors
Major role in determining disease severity
Caused by gene polymorphisms, IL-1 acting as a contributory risk factor
IL-1 activates the inflammatory and immune responses to bacterial virulence factors stimulates the release of host proteolytic enzymes and osteoclastic activation --- results in periodontal tissue breakdown

Genetic conditions and periodontal diseases

Socioeconomic status
Complex, multi-faceted parameter
Higher socioeconomic status-
better plaque control and increased dental visits
decreased prevalence of periodontal disease

Gender
Higher in males
Related to poorer plaque control and lower dental attendance rates in males

Tooth-related factors
Increased risk due to an increased risk of plaque retention--- inaccessibility to cleaning.
Occlusal forces—Class II div 2 malocclusions, loss of posterior support.
Affects both the healthy periodontium and the affected teeth with existing periodontal disease.
Removal of --Occlusal interferences in both centric occlusion and lateral excursive movements

Local risk factors for periodontal disease

Microbial factors
Over 500 bacteria have
been identified
Authors categorized
bacterial species into
colour coded groups
based on their
pathogenecity:

Lets take “History” of every patient very carefully keeping all these probable risk factors in our mind!!!
Lets always think of “Risk Assessment”

Complexity 1 BPE Score 1 – 3 in any sextant
Complexity 2 BPE Score of 4 in any sextant Surgery involving the periodontal tissuesComplexity 3 Surgical procedures associated with osseointegrated implants. Surgical procedures involving periodontal tissue augmentation
and/or bone removal (e.g. crown lengthening surgery).
PERIODONTAL TREATMENT ASSESSMENT
Based upon the Basic Periodontal Examination (BPE) Criteria:

BPE score of 4 in any sextant and including one or more of the following:
Patient’s age under 35 years.
Smoking 10+ cigarettes daily.
A concurrent medical factor that is directly affecting the periodontal tissues.
Root morphology that adversely affects prognosis.
Rapid periodontal breakdown >2 mm attachment loss in any one year.

Complexity 1 cases may be treated in general practice,
Complexity 2 cases either referred or treated by the GDP and
Complexity 3 cases mostly referred.