Risk Factors for Acute Kidney Injury in Congenital Heart Defects Ronald G. Grifka, MD Chief,...
42
Risk Factors for Acute Kidney Injury in Congenital Heart Defects Ronald G. Grifka, MD Chief, Cardiology Division Helen DeVos Children’s Hospital Professor of Pediatrics MSU College of Human Medicine
-
Upload
corey-cobb -
Category
Documents
-
view
214 -
download
1
Transcript of Risk Factors for Acute Kidney Injury in Congenital Heart Defects Ronald G. Grifka, MD Chief,...

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
Ronald G. Grifka, MDChief, Cardiology Division Helen DeVos Children’s HospitalProfessor of Pediatrics MSU College of Human Medicine

Risk Factors for Acute Kidney Injury in Congenital Heart
DefectsThe Elephant…

Risk Factors for Acute Kidney Injury in Congenital Heart
DefectsThe Elephant…

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Hypertension• FeNa• GFR Calculations• Lupus
What I Will Not Discuss

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Normal cardiac index = 3.5 L/min/m2
• Cardiac index = cardiac output/BSA
• For a newborn: 3.2 kg, 0.22 m2
• Cardiac output = 770 ml/min• If HR = 140/min• Each heart beat = 5.5 ml
• RBF = 20% of the CO- RBF = 1.1 ml/heart beat
Cardiac Hemodynamics

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Low cardiac output state: CI = 2.0 L/min/m2
• For a newborn: 3.2 kg, 0.22 m2
• Cardiac output = 440 ml/min• If HR = 170/min• Each heart beat = 2.6 ml
• RBF = 20% of the CO• RBF = 0.52 ml/heart beat
Cardiac Hemodynamics

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Acute vs. Chronic• New post-op, Myocarditis vs. Dilated CM, DMD, old post-op
• Right ventricle vs. Left ventricle• TOF, Pulm HTN vs. Anomalous left cor art from PA, DCM
• High output vs. Low output• Anemia, Hyperthyroid vs. DCM, Myocarditis
• Congenital vs. Acquired• Mitochondrial disorder, DMD vs. Kawasaki disease, Myocarditis
Types of Heart Failure

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Left to right shunts• VSD, PDA, AV Canal, ASD
• Right to left shunts• TOF, Pulmonary atresia
• Transposition physiology• Obstructive / Regurgitant defects
• AS, PS, CoA, “HLHS”, MS, MR, AI
• Cardiomyopathy• Dilated, Hypertrophic, Restrictive
5 Physiologies of Congenital Heart Defects

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• VSD, AV Canal, PDA, ASD, Ao-PA Window, Truncus arteriosus, Single V without PS
• Results in pulmonary overcirculation• *RARELY causes heart failure (”CHF”), renal
failure• Tx: Diuretics, ACE inhibitor, ± digoxin• *Neonates - Truncus Arteriosus, Premie (PDA)
- Intestinal steal NEC, Renal failure
Physiology #1 Left to Right Shunt

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Tetralogy of Fallot, Pulmonary atresia, Single ventricle with PS
• Does not cause pulmonary overcirculation!• Does not cause heart failure (”CHF”)• Does cause: Cyanosis, Polycythemia, Bleeding • Partial exchange transfusion if Hct > 62-65%
Physiology #2 Right to Left Shunt

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Blue blood to the body, red blood to the lungs• Not compatible with life as we know it!
• Profoundly cyanotic, hypoxic, acidotic, hypotensive• Can cause multi-system organ damage if not
treated immediately• Immediate treatment:
• PDA (PGE1 infusion)• ASD (Balloon atrial septostomy)
Physiology #3 Transposition Physiology

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Aortic stenosis/regurge, Pulmonary stenosis, Coarctation of the aorta, “HLHS”, Mitral stenosis or regurge
• CAN cause heart failure!• CAN cause inadequate perfusion to:
• Coronaries (infarction)• Intestines (NEC)• Kidneys (ARF)
Physiology #4 Obstructive/Regurgitant Defects

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Dilated, Hypertrophic, Restrictive• CAN cause heart failure!
• LHF: Inadequate organ perfusion, Pulm edema, SOB, Activity• RHF: 1° or 2°, Hepato-splenomegally, systemic edema
• DCM: Diuresis, ACE inhibitor, Inotrope, ± Anti-arrhythmic• HCM: NO: diuresis or inotrope (unless end stage)
YES: beta blocker, ± Anti-arrhythmic, AICD
• End stage Tx: LVAD (DCM), Heart transplant
Physiology #5 Cardiomyopathy

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Acute insult
• Chronic insult
• An acute insult to a chronic condition
Cardiac Related Renal Injury
Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
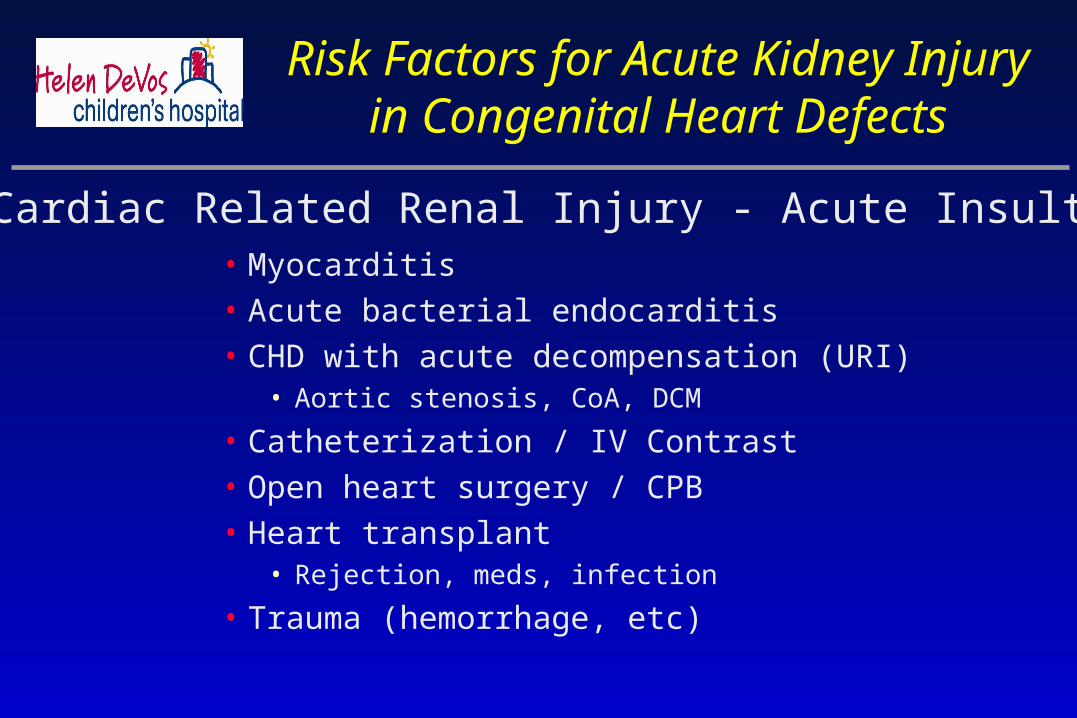
• Myocarditis• Acute bacterial endocarditis• CHD with acute decompensation (URI)
• Aortic stenosis, CoA, DCM
• Catheterization / IV Contrast• Open heart surgery / CPB• Heart transplant
• Rejection, meds, infection
• Trauma (hemorrhage, etc)
Cardiac Related Renal Injury - Acute Insult

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• (Systemic) Ventricular failure• CHD, DCM natural history• Post-op failure• Myocarditis• Transplant: Coronary vasculopathy,
rejection, meds, infection
• Cyanosis• Repetitive embolic events
• Arrhythmia, thrombotic substrate
Cardiac Related Renal Injury - Chronic Insult

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Nephrotoxic antibiotics• Furosemide, mannitol Diuresis, but IVF not replaced• Epi, Norepi, high dose Dopamine Renal vasoconstriction• Anesthetic agents Hypotension• Low cardiac output, low blood pressure• Sepsis• Pre-existing renal disease (cyanosis, Hct, low cardiac output)
• Cardiopulmonary bypass
Peri-Operative Renal Insults

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Allows surgery in a bloodless field• Arrests the heart, decreases MVO2• Perfuses other organs during surgery• Can adjust the blood flow, add medications
Cardiopulmonary Bypass - Positives

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Fragments RBC’s• Activates platelets• Alters clotting factors• Liberates vasoactive compounds• Hypothermic insult (18-25° C)• Metabolic acidosis• Perfuses organs during surgery with
NON-PULSATILE flow• P/O transfusions
Cardiopulmonary Bypass – Negatives

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Phenoxybenzamine pre-op• Increase renal blood flow
• Dopamine, fenoldapam, neseritide
• Intra-op, Post-op diuretics• ± IVF replacement: colloid vs. crystalloid
• Increase BP• But pressors SVR, HR , ? CO
• Peritoneal dialysis
Peri-Operative Treatment

BeBenephnephititTMTM Infusion System Infusion System(FlowMedica, Inc., Fremont, CA)(FlowMedica, Inc., Fremont, CA)
FDA (510K) Cleared January 2004FDA (510K) Cleared January 2004
Intrarenal infusionIntrarenal infusion
-Dopamine, Fenoldopam-Dopamine, Fenoldopam
-Nesiritide (BNP)-Nesiritide (BNP)

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Enlargement of the glomerular capillary tuft• Mesangial hypercellularity• Accumulation of eosinophilic material• Capillary basement membrane thickening• IgM deposits in the mesangium• Fibrin in the glomerular capillary walls• Clinically – GN: hematuria, proteinuria, HTN
Cyanotic Heart Disease

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Kidneys normal to slightly enlarged• Glomerular immune complex deposition
- C3, IgG. Occasionally IgM, IgA
• Treat SBE, renal function improves• Advanced SBE disease
• Microabcesses• Embolization, infarction
• May not recover renal function
Infective Endocarditis

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
• Well described entity in adults• Adults have more pre-existing renal disease, HTN• Rare in children following cardiac cath
• New contrast much safer• IVF from anesthesiologist and catheter flushes• Contrast given over several hour cath procedure
- Up to 12 ml/kg over 7 hr procedure• Much IV fluids, foley
Contrast Induced Nephropathy

The Evolution of Contrast MediaThe Evolution of Contrast Media
R
R
RRR
R
CH3CONH
RRR
II
II
IIII
IIII
II
RR
II
R COO–Na+/Meg+
I
R
COO–Na+/Meg+
I
Ionic monomerDiatrizoateIothalamate
Nonionic monomerIopamidol
IohexolIoversol
Ionic dimerIoxaglate
Nonionic dimerIodixanol(Iotrolan)
ExamplesMolecular Structure Era
1950s
1980s
1980s
1990s
Comment
High Osmolality, 5 – 8 blood
Low Osmolality,2 – 3 blood,
improved hydrophilicity
Low Osmolality,~2 blood
Iso-osmolalityOsmolality = blood

Osmolalities of Contrast MediaOsmolalities of Contrast Media
Iodixanol is a nonionic dimer, formulated with balanced levels of Ca2+ and Na+, that is isosmolar with plasma at all iodine
concentrations
0
500
1000
1500
2000
2500Blo
odIo
dixa
nol
Ioxa
glat
eIo
mep
rol
Iove
rsol
Iopr
omid
eIo
pam
idol
Iope
ntol
Iohe
xol
Iobi
trid
olDia
triz
oate
Osm
ola
lity
(m
Osm
/kg
H
2O)
+
*
* 320 mg I/mL† 350 mg I/mL‡ 370 mg I/mL
* *†† † †
‡ ‡
‡

Contrast enters renal vasculatureEndothelium-independent transient vasodilation (minutes)
Reduced nephron mass vulnerable to injuryAssociated factors: diabetes, poor renal perfusion, others
Sustained intrarenal vasoconstriction (hours)
Ischemic injury and death
Acute Kidney Injury
Prostaglandindysregulation
Decreased Nitric Oxide Synthesis/Release
Prolonged contrast transit time in kidneysIncreased contrast exposure to renal tubular cells
Contrast direct cellular injury and death
Medullary hypoxia
Catalytic iron-driven oxidative Stress, inflammation, other organ injury processes
Adenosine release from macula densa
(tubulo-glomerular feedback)
Endothelinrelease
McCullough PA, JACC 2008

73 y/o with multiple myeloma, Cr 2.3 mg/dl, CrCl=23 ml/min, Cr rise 0.3 mg/dl
Nephrol Dial Transplant (2004) 19: 1654–1655

One-Year Kaplan-Meier Survival Curves Stratified by CrCl Levels after Primary Angioplasty in CADILLAC
Time (days)
Su
rviv
al (%
)
CrCl >60CrCl >60CrCl 50-60CrCl 50-60
CrCl 40-50CrCl 40-50CrCl 30-40CrCl 30-40
CrCl 20-30CrCl 20-30
CrCl <20CrCl <20
PP<.0001 (all groups)<.0001 (all groups)40
50
60
70
80
90
100
0 50 100 150 200 250 300 350 400 450 500
Sadeghi HM et al. Circulation. 2003;108:2769–2775.

*Plans should be made in case AKI occurs and dialysis is required
† Potentially beneficial agents:
N-Acetylcysteine
Ascorbic acid
Aminophylline
Prostaglandin E1
None approved for this indication
AKI=acute kidney injuryCr = creatinineCrCl=creatinine clearance; eGFR=estimated glomerular filtration rate NSAIDs= nonsteroidal anti-inflammatory drug
Calculate eGFR or CrClCalculate eGFR or CrClAssess contrast-induced AKI riskAssess contrast-induced AKI risk
eGFR <30 ml/mineGFR <30 ml/minStart/continue statinStart/continue statin
Discontinue NSAIDs, Discontinue NSAIDs, other nephrotoxic drugs, metforminother nephrotoxic drugs, metformin
eGFR 30-59 mL/mineGFR 30-59 mL/minStart/continue statinStart/continue statin
Discontinue NSAIDs, other nephrotoxic Discontinue NSAIDs, other nephrotoxic drugs, metformindrugs, metformin
eGFR eGFR ≥≥60 ml/min60 ml/minDiscontinue metforminDiscontinue metformin
• Hospital admissionHospital admission
• Other strategies as for Other strategies as for eGFR 30-59 mleGFR 30-59 ml
• Nephrology Nephrology consultation*consultation*
• Consider hemofiltration Consider hemofiltration pre- and post-procedurepre- and post-procedure
• IV isotonic (NaCl/NaHCOIV isotonic (NaCl/NaHCO33))•1.0-1.5 ml/kg/min 3-12 hrs pre and 6-24 post1.0-1.5 ml/kg/min 3-12 hrs pre and 6-24 post
•Ensure urine flow rate > 150 ml/hrEnsure urine flow rate > 150 ml/hr
• Iso-osmolar contrastIso-osmolar contrast•DM, ACS, other added risksDM, ACS, other added risks
• Low osmolar contrastLow osmolar contrast•No other added risksNo other added risks
• Limit contrast volumeLimit contrast volume•< 30 cc diagnostic< 30 cc diagnostic
•<100 cc diagnostic+intervention<100 cc diagnostic+intervention
• Consider adjunctive medicationsConsider adjunctive medications††
•AntioxidantsAntioxidants
•N-acetylcycteine 1200 mg po bid pre- N-acetylcycteine 1200 mg po bid pre- and post-procedureand post-procedure
oror
•Ascorbic acid 3 g po pre- Ascorbic acid 3 g po pre-
2 g po bid post-procedure2 g po bid post-procedure
Good clinical Good clinical practicepractice
Serum Cr before Serum Cr before discharge or 24–72 hrdischarge or 24–72 hr
Expectant CareExpectant Care

IV Hydration and Urine OutputIV Hydration and Urine Output
Stevens MA et al. J Am Coll Cardiol. 1999.
4.5
3.5
2.5
1.5
0.5
-0.5
-1.5
Ch
an
ge in
Cr
from
Baselin
e
(mg
/dL)
0 60 120 180 240 300
Urine Flow Rate (mL/h)
r = -0.36, F = 5.73, r = -0.36, F = 5.73, PP = 0.005 = 0.005Urine Flow Rate (mL/hr), beta = -0.36, t = -3.33, Urine Flow Rate (mL/hr), beta = -0.36, t = -3.33, PP = 0.001 = 0.001
Baseline CrCI (mL/min), beta = 0.10, t = 0.93, Baseline CrCI (mL/min), beta = 0.10, t = 0.93, PP = 0.36 = 0.36
Regression 95% CI

Treitl M, et al, Nephrol Dial Transplant (2008)Treitl M, et al, Nephrol Dial Transplant (2008)

Hemofiltration Hemofiltration works to ensure
– Adequate intravascular volume– Reduce uremic toxins which may worsen AKI– Provides stability to the high risk patient after the procedure reducing the
risks of oliguria, volume overload, and electrolyte imbalance that are associated with short-term mortality.
Double lumen catheter is placed in a jugular or femoral vein for blood withdrawal and reinfusion and connected to an extracorporeal circuit.
6 hours before contrast: Peristaltic pump (e.g. Prisma hemofiltration pump) at 100 mL/min. Isotonic replacement fluid (post-dilution hemofiltration) 1000 mL/h, matched with the rate of ultrafiltrate production so no net fluid loss occurs.
5000 IU heparin bolus before initiation followed by a continuous heparin infusion of 500 to 1000 IU/h through the inflow side of the catheter.
At the time of the cardiac procedure, the hemofiltration treatment should be stopped, the circuit temporarily filled with a saline solution and short-circuited to exclude the patient without interruption of the flow.
Immediately after the cath, hemofiltration should be restarted for 12-18 hours.

AKI (Cr >0.5 mg/dL [> 44.2µmol/L])
Marenzi G et al. Am J Med. 2006 Feb;119(2):155-62.
47
42
3
0
10
20
30
40
50
Control Post-hemofiltration
group
Pre/post-hemofiltration
group
%
P<0.001
NS
Dialysis
9 (30%) 3 (10%) 0 (0%) P=0.002
Death
6 (20%) 3 (10%) 0 (0%) P=0.03

Anatomical Basis: The Coronary SinusAnatomical Basis: The Coronary Sinus
69 y.o. with CRI, SCr. 2.9, CTO, 240cc dye69 y.o. with CRI, SCr. 2.9, CTO, 240cc dye
AIVAIV
CSCS
AIV
AIV
MC
VM
CV
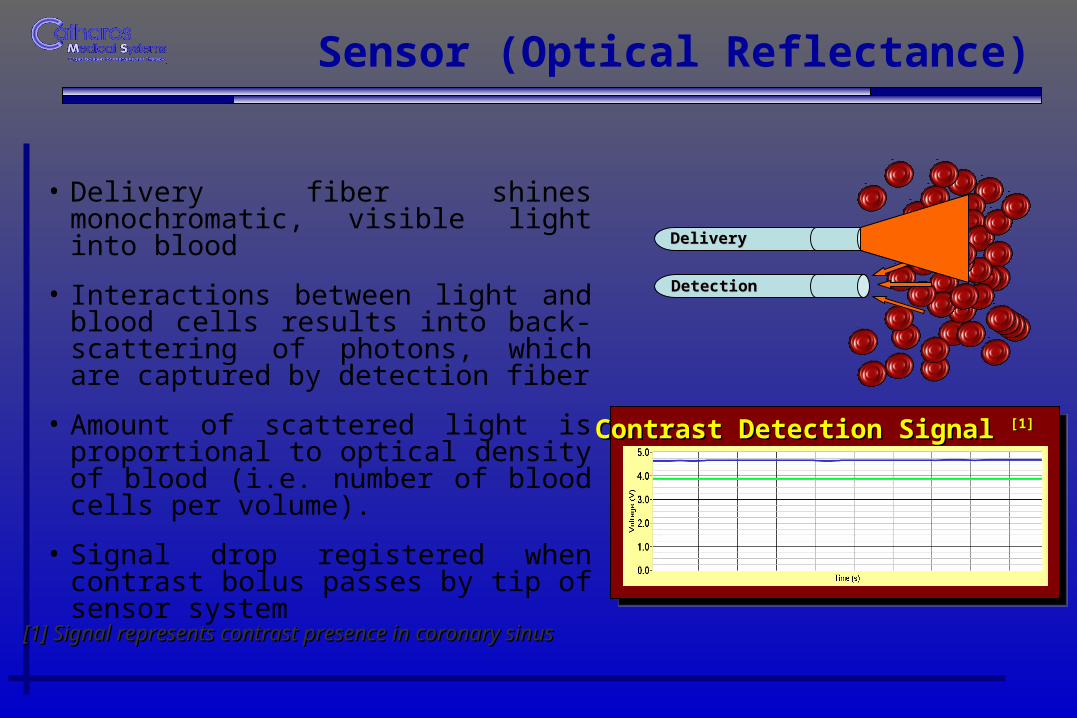
Sensor (Optical Reflectance)
• Delivery fiber shines monochromatic, visible light into blood
• Interactions between light and blood cells results into back-scattering of photons, which are captured by detection fiber
• Amount of scattered light is proportional to optical density of blood (i.e. number of blood cells per volume).
• Signal drop registered when contrast bolus passes by tip of sensor system
DeliveryDelivery
DetectionDetection
[1] Signal represents contrast presence in coronary sinus[1] Signal represents contrast presence in coronary sinus
Contrast Detection Signal Contrast Detection Signal [1][1]

•Successful device deployment in CS
•Arterial injection of contrast
•Appropriate size & seal at CS level
•Contrast recovery: 70%*
Source: CAN-12 CD1_IMG008Source: CAN-12 CD1_IMG008 * Contrast recovery established by UV Spectrometry* Contrast recovery established by UV Spectrometry
In-Vivo Contrast RemovalIn-Vivo Contrast Removal

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
This is not the end.Nor is it the beginning of the end.But perhaps, this is the end of the beginning.

Risk Factors for Acute Kidney Injury in Congenital Heart
DefectsThank you, and looking toward the future in Grand Rapids….

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects

Risk Factors for Acute Kidney Injury in Congenital Heart
Defects
Ronald G. Grifka, MDChief, Cardiology Division Helen DeVos Children’s HospitalProfessor of Pediatrics MSU College of Human Medicine


















