
risk assessment
69
1
-
Upload
dr-vartika-srivastava -
Category
Documents
-
view
82 -
download
0
Transcript of risk assessment
1

Seminar on Risk Assessment
For Periodontal Disease
2
Contents
Introduction
Definitions
Elements for periodontal disease
Risk factors
Clinical risk assessment for periodontal disease.
Current models for periodontal risk assessment
Conclusion
References
3

Introduction
Over the last three decades, our understanding on the pathogenesis
and etiology of periodontal diseases has grown greatly.
Numerous studies have demonstrated that the host plays a major role in
the pathobiology of periodontitis and that risk varies greatly from one
individual to another.
Beck JD. Risk assessment revisited. Community Dent Oral Epidemiol. 1998;26:220–5
Identifying risk factors and indicators, as well as undertaking measures
that can reduce the risk, can help in maintaining oral health and
prevent the onset of any form of periodontal disease
4

Assessing patients risk of developing periodontal disease can have
a significant impact on clinical decision making.
The role of risk factors and risk assessment in the prediction of
clinical periodontal outcomes has been a subject of much
interest.
5
Risk assessment has been defined as the process by which qualitative or
quantitative assessments are made of the likelihood for adverse events
to occur as a result of exposure to specified health hazards or by the
absence of beneficial influences.
According to American Academy Of Periodontology utilizing risk
assessment helps dental professionals predict the potential for
developing periodontal diseases and allows them to focus on early
identification and to provide proactive, targeted treatment for patients
who are at risk for progressive/ aggressive diseases
American Academy of Periodontology statement on risk assessment. Journal of Periodontology 2008; 79: 202.
6

Risk can be identified in terms of
Risk Factors
Risk Indicators
Risk Predictors
Risk determin
ant
7

A risk factor can be defined as any environmental, behavioral, orbiologic factor that, when present, increases the likelihood that anindividual will develop the disease.
.
Risk indicators are probable or putative risk factors that have beenidentified in cross sectional studies but not confirmed throughlongitudinal disease.
Risk predictors / markers are although associated with increased risk fordisease , but do not cause the disease.
The term risk determinant/background characteristic, which issometimes substituted for the term risk factor, should be reserved forthose risk factors that cannot be modified.
Novak K, Novak M. Risk Assessment. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA, editors. Carranza's Clinical Periodontology. 10 ed
8
A risk factor is thought to be a cause for a disease.
It should satisfy two criteria:
(1) it is biologically plausible as a casual agent for disease and
(2) it has been shown to precede the development of disease in
prospective clinical studies.
Risk factors are biologically related to the occurrence of the disease,
but they do not necessarily imply cause and effect.
9

Most accepted risk “elements” for
periodontal disease include
Risk Factors Risk determinants Risk indicators Risk predictors
Tobacco smoking Genetic factors HIV/AIDS Previous history of
periodontal disease
Diabetes Age Osteoporosis Bleeding on probing
Pathogenic bacteria Gender Infrequent dental visits
Microbial tooth deposit Socioeconomic status
Stress
10
TOBACCO SMOKING
Tobacco is well established risk factor for periodontitis .American Academy of Periodontology : position paper : epidemiology of periodontal disease , journal of periodontal 67:935,1996
A wealth of data has established the relationship between the amount
and duration of smoking and the severity of periodontal pathology.
Studies comparing the response to periodontal therapy in smokers,
previous smokers and nonsmokers have shown that smoking has a
negative impact on the response to therapy.
11

According to Bolin et al 1993 periodontitis in smokers respond less to
treatment, former smokers get a slower disease progression.
With increased use of tobacco, patients show higher periodontal
probing depths, increased clinical attachment loss, more alveolar bone
resorption, a higher prevalence of gingival recessions, and a higher risk
for tooth loss
Tonetti MS: Cigarette smoking and periodontal diseases: etiology and management of disease. Ann Periodontol
1998; 3:88.
Both local and systemic mechanisms mediate the negative impact of
tobacco use on oral health.
12
A number of studies indicate that the nicotine found in tobaccoproducts triggers the overproduction of cytokines in the body due tolowered oxygen levels.
Cytokines are signaling chemicals involved in the process ofperiodontal inflammation. When nicotine combines with oral bacteria,such as P. gingivalis, it results in higher levels of cytokines, leading tobreakdown of the supporting tissues of the teeth.
The risk of periodontal disease increases with the number of cigarettessmoked per day.
Johnson GK. Margaret Hill Cigarette smoking and the periodontal patient. J Periodontol. 2004;75:196– 209
13

DIABETES
Diabetes is a clear risk factor for periodontitis.
Epidemiologic data demonstrate that the prevalence and severity of
periodontitis is significantly higher in patients with type I and type II
diabetes than in those without diabetes ,
American Academy of Periodontology: Position paper. Epi- demiology of periodontal diseases. J Periodontol 1996; 67:935-945.
14

Diabetes has been associated with a number of oral complications,
including gingivitis and periodontitis, dental caries, salivary gland
dysfunction and xerostomia, burning mouth syndrome and increased
susceptibility to oral infections.
In these patients, host responses may be impaired, wound healing is
delayed and collagenolytic activity may be enhanced. As a result,
periodontitis may be a particular problem in patients with diabetes,
especially in those with uncontrolled disease.
Vernillo AT. Dental considerations for the treatment of patients with diabetes mellitus. J Am Dent Assoc. 2003;134(supplement I):245–335
15
Diabetes may also contribute to the pathogenesis of periodontitis via
associated vascular compromise, deficits in cell mediated immunity
and the presence of a high glucose content in the blood, which
enhances bacterial growth.
Furthermore, active inflammation characteristics of periodontitis
generates compounds that may increase insulin resistance.
Mealey B. Diabetes and periodontal diseases. J Periodontol. 1999;70:935–49.
Tervonen T, Oliver RC. Long term control of diabetes mellitus and periodontitis. J Clin Periodontol.1993;20:431–5.
16

Pathogenic Bacteria and Tooth
Deposits
It is well documented that accumulation of bacterial plaque at the
gingival margin results in the development of gingivitis and that the
gingivitis can be reversed with the implementation of oral hygiene
measures.
LOE H, Theilade E, Jensen SB: Experimental gingivitis in man. J Periodontol 1965; 36:177-187
Often, patients with severe loss of attachment have minimal levels of
bacterial plaque on the affected teeth, indicating that the quantity of
plaque is not of major importance in the disease process.
17

However, although quantity may not indicate risk, there is evidence that
the composition, or quality, of the complex plaque biofilm is of
importance.
In terms of quality of plaque, three specific bacteria have been
identified as etiologic agents for periodontitis:
I. A. actinomycetemcomitans,
II. P. gingivalis,
III. Bacteroides forsythus.
18

Cross-sectional and longitudinal studies support the delineation of these
three bacteria as risk factors for periodontal disease.
Additional evidence that they are causal agents include:
(1) Their elimination or suppression impacts the success of therapy,
(2) There is a host response to these pathogens,
(3) Virulence factors are associated with these pathogens and
(4) Inoculation of these bacteria into animal models induces periodontal
disease.
Haffajee AD, Socransky SS: Microbial etiological agents of destructive periodontal diseases. Periodontol 2000 1994; 5:78-111.
19

Genetic factors
There is evidence that genetic differences between individuals may
explain why some patients develop periodontal disease and others do
not.
Studies conducted in twins have shown that genetic factors influence
clinical measures of gingivitis, probing pocket depth, attachment loss,
and interproximal bone height.Michalowicz BS, Aeppli DP, Kuba RK, et al: A twin study of genetic variation in proportional radiographic alveolar bone height. J Dent Res 1991;
70:1431-1435
20

The familial aggregation seen in localized and generalized aggressive
periodontitis also is indicative of genetic involvement in these diseases.
A specific interleukin 1 (IL-1) genotype has been associated with severe
chronic periodontitis.
Kornman KS, Crane S, Wang HY, et al: The interleukin-1 genotype as a severity factor in adult periodontal disease. J Clin Periodontol 1997; 24:72-77
Immunologic alterations, such as neutrophil abnormalities, monocytic
hyper responsiveness to lipopolysaccharide stimulation in patients with
localized aggressive periodontitis.
Hart TC, Shapira L, Van Dyke TE: Neutrophil defects as risk factors for periodontal diseases. J Periodontol 1994; 65: 521-529.
21

Research on the Interleukin1 (IL1) polymorphisms has indicated that IL1
genotype positive patients show more advanced periodontitis lesion
that IL1 genotype negative patients of the same age group.
Also there is a trend to higher tooth loss in the IL1 genotype positive
subjects.
In a retrospective analysis of over 300 well maintained periodontal
patients, the IL1 genotype yield higher BOP% during a 1year recall
period than the IL1 genotype negative control patients.Kornman KS, Crane A, Wang HY, Newman MG, Pirk FW, Wilson TG, Jr, et al. The interleukin I genotype as a severity factor in adult periodontal disease.
J Clin Periodontol. 1997;24:72–7.
22

AGE
Both the prevalence and severity of periodontal disease increases with
age .Papapanou PN: Risk assessments in the diagnosis and treatment of periodontal diseases. J Den Edu 1998; 62:822-839
It is possible that degenerative changes related to aging may increase
susceptibility to periodontitis.
However, it also is possible that the attachment loss and bone loss seen
in older individuals is a result of prolonged exposure to other risk factors
over a person's life, creating a cumulative effect over time
23

In a study of people over 70 years old, 86% had at least moderate
periodontitis or a severe form of periodontal disease, and over one
fourth of this 86% had lost their teeth.
The study also showed that the disease accounted for a majority of
tooth extractions in patients older than 35 years of age.Khalaf F, AlShammari , Areej K, AlKhabbaz, Jassem M, AlAnsari, et al. Risk indicators for tooth loss due to periodontal disease. J Periodontol.
2005;76:1910–18
24

GENDER
Gender plays a role in periodontal disease.
United States national surveys conducted since 1960
demonstrate that males have more loss of attachment than
females.U.S. Public Health Service, National Center for Health Statistics: Periodontal Disease in Adults, United States 1960- 1962.
25
In addition, males have poorer oral hygiene than females, as
evidenced by higher levels of plaque and calculus.U.S. Public Health Service, National Institute of Dental Re- search: Oral Health of United States Adults; National Findings
Therefore it appears that gender differences in prevalence and
severity of periodontitis are related to preventive practices rather than
any genetic factor.
26

Socioeconomic Status
Gingivitis and poor oral hygiene can be related to lowersocioeconomic status (SES) .
This can most likely be attributed to decreased dental awareness anddecreased frequency of dental visits when compared with moreeducated individuals of higher SES.
After adjusting for other risk factors such as smoking and poor oralhygiene, lower SES alone does not result in increased risk forperiodontitis.
U.S. Public Health Service, National Center for Health Statistics: Basic Data on Dental Examination Findings of Persons 1-74 years; United States 1971-1974.
27
STRESS
It has been strongly suggested that stress and related body distress are
important risk indicators for periodontal disease.
A recent study shows that people under physical or psychological stress
are prone to elevated biofilm plaque levels and increased gingivitis.
Hildebrand HC, Epstein J, Lorjova H. The influence of psychological stress on periodontal disease. J West Soc Periodontol Periodontal Abstr.
2000;48:69–77.
28

The incidence of necrotizing ulcerative gingivitis increases during
periods of emotional and physiologic stress, suggesting a link between
the two.Shields WD: Acute necrotizing ulcerative gingivitis. A study of some of the contributing factors and their validity in an Army population. J Periodontol
1977; 48:346-349.
Emotional stress may interfere with normal immune function and may
result in increased levels of circulating hormones that can have an
impact on the periodontium.Haffajee AD, Socransky SS: Microbial etiological agents of destructive periodontal diseases. Periodontol 2000 1994; 5:78-111.
Rose RM: Endocrine responses to stressful psychological events. Psychiatr Clin N Am 1980; 3:251-276.
29
Stress diminishes saliva flow and increases dental plaque formation.
Emotional stress modifies the saliva pH and its chemical
composition like the IgA secretion .Reners M, Breex M. Stress and periodontal disease. Int J Dent Hygiene 2007; 5: 199–204.
A series of studies made by Deinzer et al., examine the impact of
academic stress by students at university during their examination
period on periodontal health. Academic stress was shown to be
a risk factor for gingival inflammation with increasing crevicular
interleukin-1b levels and a diminution of the quality of the oral hygiene .
Deinzer R, Ru ttermen S, Mo bes O, Herforth A. Increase in gingi val inflammation under academic stress. J Clin Periodontol 1998; 25:431–433.
30
Human Immunodeficiency
Virus/Acquired Immunodeficiency
Syndrome
It has been hypothesized that the immune dysfunction associated with
human immunodeficiency virus (HIV) infection and acquired
immunodeficiency syndrome (AIDS) increases susceptibility to
periodontal disease.
Early reports on the periodontal status of patients with AIDS or
individuals who are HIV seropositive revealed that these patients often
had severe periodontal destruction characteristic of necrotizing
ulcerative periodontitis.Winkler JR, Herrera C, Westenhouse J, et al: Periodontal dis- ease in HIV-infected and uninfected homosexual and bisex- ual men [letter]. AIDS 1992;
6:1041-1043
31
In a 20-month study of 114 homo- sexual and bisexual men, the relative
risk of longitudinal attachment loss >3 mm was 4.8 when CD4 counts
were less than 400/mm3 and increased to 6.16 when CD4 counts were
less than 200/mm 3, suggesting a correlation between the severity of
periodontal disease and the level of immunosuppression.
Barr C, Lopez MR, Rua-Dobles A: Periodontal changes by HIV serostatus in a cohort of homosexual and bisexual men. J ClinPeriodontol 1992; 19:794-801
32

OSTEOPOROSIS
Osteoporosis has been suggested as another risk factor for periodontitis.
Although studies in animal models indicate that osteoporosis does not
initiate periodontitis, there is evidence that the reduced bone mass
seen in osteoporosis may aggravate periodontal disease progression.
Krook L, Whalen JP, Lesser GV, et al: Experimental studies on osteoporosis. Methods Achiev Exp Pathol 1975; 7:72-108
However, reports in humans are conflicting. In a study of 12 women with
osteoporosis and 14 healthy women, Von Wowern et al reported that
the women with osteoporosis had greater loss of attachment than the
control subjects.
Van Wowern J, Klausen B, Kollerup G: Osteoporosis: a risk factor in periodontal disease. J Periodontol 1994; 65: 134.
33

Infrequent Dental Visits
Identifying failure to visit the dentist on a regular basis as a risk factor for
periodontitis is controversial.
Study demonstrated an increased risk for severe periodontitis in
patients who had not visited the dentist for three or more years,
whereas another demonstrated that there was no more loss of
attachment or bone loss in individuals who did not seek dental care
when compared with those that did over a 6-year period.
Page RC, Beck JD: Risk assessment for periodontal diseases. Int Den J 1997; 47:61-87
34

Previous History of Periodontal Disease
A history of previous periodontal disease is a good clini- cal predictor of
risk for future disease .
Patients with the most severe existing loss of attachment are at the
greatest risk for future loss of attachment.
Conversely, patients currently free of periodontitis have decreased risk
for developing loss of attachment than those who currently have
periodontitis.Page RC, Beck JD: Risk assessment for periodontal diseases. Int Den J 1997; 47:61-87
35
Bleeding on Probing
Bleeding on probing is the best clinical indicator of gingivalinflammation.
Although bleeding on probing alone does not serve as a predictor forloss of attachment, bleeding on probing coupled with increasingpocket depth may serve as an excellent predictor for future loss ofattachment.
Lack of bleeding on probing does appear to serve as an excellentindicator of periodontal health.
Page RC, Beck JD: Risk assessment for periodontal diseases. Int Den J 1997; 47:61-87
36

In assessing the patient's risk for disease progression, BOP percentages
reflect a summary of the patient's ability to perform proper plaque
control, the patient's host response to the bacterial challenge and the
patient's compliance, especially when only few residual pockets remain
after active periodontal therapy.
The percentage of BOP, therefore, is used as the first risk factor in the
functional diagram of risk assessment .
Lang & Tonetti Periodontal Risk Assessment (PRA) for Patients in Supportive Periodontal Therapy (SPT) : Oral Health & Preventive Dentisty 2003, S. 7-16
37

CLINICAL RISK ASSESSMENT
FOR PERIODONTAL
DISEASE
38

Risk assessment in periodontal disease is that the diseases are
multifactorial and assessment should therefore be at multiple levels.
The presence of pathogenic bacteria alone is not sufficient to cause
the disease.
In simple terms, there are four levels to consider:
39
The patient level Perform at initial
examination
The whole mouth level
Perform at initial examination
and post initial therapy
The tooth level Perform post-
initial/definitive therapy and
maintenance
The site level Perform post
definitive therapy and
during maintenance
40

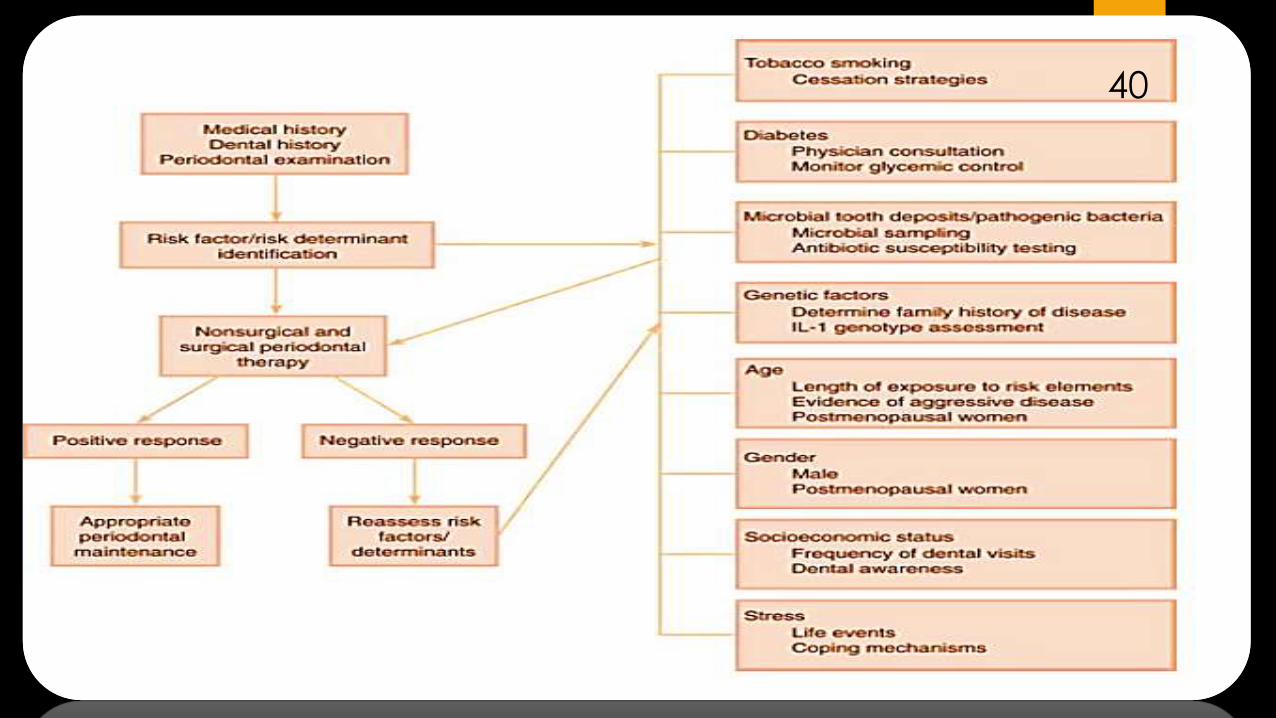
Patient level risk assessment
Patient level risk assessment can be determined at the initial consultation by performing the following :
•Family history for hereditary, inborn or genetic risk factors. Take adetailed history of gum disease or early tooth loss in the family.
•Medical history for systemic diseases, e.g. diabetes mellitus,cardiovascular diseases, osteoporosis
•Present dental history Assess motivation to oral hygiene.
•Social history, which includes smoking current or former smokerHabits like bruxism
41
Patientlevel risk assessment Patientlevel risk assessment can be determined at the initial consultation by performing the following:

Mouth level risk assessment
Mouth level risk assessment would be performed at the initial examination, after a basic periodontal examination, and would include:
• Examination of attachment loss relative to age
• Occlusal examination in static relationship
• Occlusal examination in dynamic relationship
• Examination of levels of oral hygiene
• Examination of levels of plaqueretentive factors
• Presence of removable prosthesis
• Levels of recession
• Gingival inflammation and depth of pockets
42
.

Tooth level risk assessment
Tooth level risk assessment may or may not be carried out at the initial examination.
A detailed periodontal chart and radiographic assessment should be performed. Part of this assessment includes:
• Individual tooth mobility
• Tooth movement or drifting of periodontally compromised teeth
• Residual tooth support (radiographically). The extent of residual radio graphic bone support helps determine long term prognosis.
• Presence, location and extent of furcation lesions
• Individual tooth anatomy Presence of "talon cusps" or bulbous crowns
• Anatomy of tooth embrasures and contact points
• Presence of ledges or deficiencies on restorations
• Individual occlusal contacts Prematurities Soft tissue contours
• Subgingival calculus
43
.

Site level risk assessment
Site level risk assessment would include:
•Bleeding on probing
•Exudation from periodontal pockets
•Local root grooves or root concavities
• Individual probing pocket depth
•Attachment levels
•Other anatomical factors like enamel pearls, root grooves.
44
Current Methods For Periodontal Risk
Assessment :
45

In periodontology, current methods to assess
periodontal risk factors include:
Periodontalrisk calculator(PRC),
Healthinformationsuite (OHIS),the Previserrisk calculatorTM
Thehexagonalrisk diagramforperiodontalriskassessment(PRA),
Theperiodontalriskassessmentmodeldevelopedby Chandra
The simplifiedmethod(UniFe) (Unionof Europeanrailwayindustries) forperiodontalriskassessment.
46
Douglass CW. Risk assessment and management of periodontal disease. J Am Dent Assoc. 2006;137:275–315

The Periodontal Risk Calculator (PRC)
Page et al. developed a computer-based risk assessment tool, the
PRC, for objective, quantitative assessment of risk.
The PRC is a web based tool that can be accessed through a dental
office computer.Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc.
2002;133: 569-576.
47

The calculation of risk using this model is based on
mathematically derived algorithms that assign relative
weights to nine factors including
Patient age,
Smoking history,
Diagnosis of diabetes,
History of periodontal surgery,
Pocket depth
furcation involvements,
Restorations or calculus below the gingival margin
Radiographic bone height and vertical bone
lesions
48

A three point scale is used to document pocket depth and
radiographic bone height.
The PRC assigns the individual a level of risk on a scale from 1 (lowest
risk) to 5 (highest risk).
An algorithm was developed to quantify disease severity from pocket
depth and bone height values.
49
The base risk score is calculated using an algorithm that correlates
disease severity with age
The risk score is increased if there is a positive history of periodontal
surgery and if the patient smokes more than 10 cigarettes per day, or
the patient has diabetes that is poorly controlled.
The existence of furcation involvements, vertical bone lesions or sub-
gingival restorations or calculus increase risk when the risk score is
otherwise less than four.
50

Health information suite (OHIS),
Previser risk calculator TM
The OHIS is an information system that compiles, analyzes and
quantifies clinical information about factors like current oral health
status, interventions needed and treatment outcomes, be they
beneficial or detrimental, that are attributable to treatment and
behavioral decisions.
The OHIS satisfies the need for a quantitative way to assess risk for
periodontitis, as well as providing, for the first time, quantification of
periodontal status and changes in status over time.
Page RC, Martin JA, Loeb CF. The Oral Health Information Suite (OHIS): its use in the management of periodontal disease. J Dent Educ. 2005;69:509–
20
51
The Periodontal Assessment Tool (PAT) is an integral part of the Oral
Health Information Suite (OHIS)TM (PreViser, Inc., Mount Vernon, WA;
www.previser. com) and is considered as a modification of the PRC
method.
Following the input of only twenty-three items taken from a routine
periodontal examination, the system generates linguistic and numeric
periodontal diagnoses and a risk score for future disease, and prepares
a report in two versions; one for the dentist’s clinical documentation
and another for the patient.
52

The hexagonal risk diagram for
Periodontal Risk Assessment (PRA)
Lang and Tonetti described a functional diagram based on six
parameters for use in estimating an individuals’ risk for progression of
periodontitis.Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent. 2003;1:7-16.
The PRA model consists of an assessment of :
53
Percentage of bleeding on probing,
Prevalence of residual
pockets greater
than 4 mm (³ 5 mm),
Loss of teeth from
a total of 28 teeth,
Loss of periodontal support in relation to
the patient's
age,
Systemic and
genetic conditions,
and
Environmental factors,
such as cigarette smoking.

CALCULATING THE PATIENT'S
INDIVIDUAL PERIODONTAL RISK
ASSESSMENT (PRA)
Based on the six parameters
specified above, a multi-
functional diagram is
constructed for the PRA.
In this diagram, the vectors
have been formed on the
basis of the scientific
evidence available.
54

A low PRA patient has all parameters within the low-risk categories or at the most one parameter in the moderate-
risk category
55

A moderate PRA patient has at least two parameters in the moderate category, but at most one parameter in the high-
risk category
56

A high PRA patient has at least two parameters in the high-risk category
57
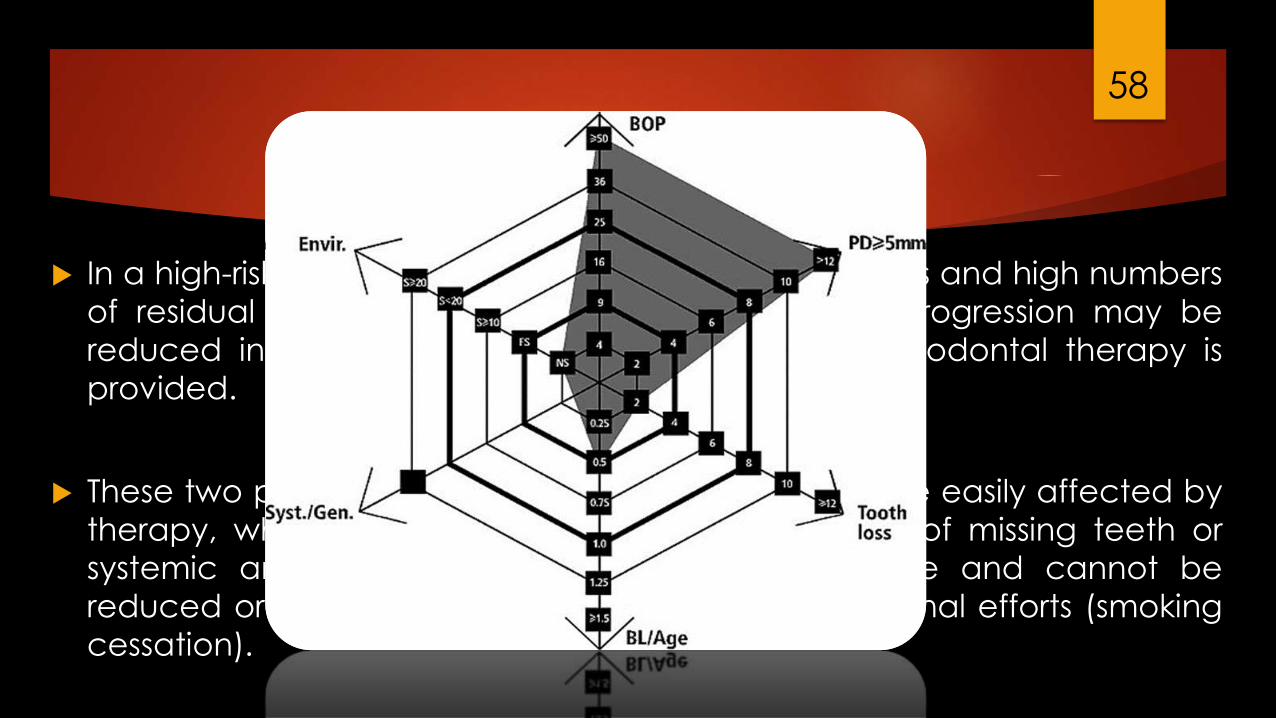
In a high-risk patient who yields high BOP percentages and high numbers
of residual pockets, the patient's risk for disease progression may be
reduced into the moderate category if further periodontal therapy is
provided.
These two parameters (BOP and residual pockets) are easily affected by
therapy, while other parameters, such as numbers of missing teeth or
systemic and genetic factors are either irreversible and cannot be
reduced or may only be affected with great additional efforts (smoking
cessation).
58

The periodontal risk assessment model
developed by Chandra
In 2007, Chandra evaluated a novel periodontal risk assessment model in patients presenting for dental care.
This new model based on the periodontal risk assessment model by Lang and Tonetti where the following parameters are recorded:
Chandra RV. Evaluation of a novel periodontal risk assessment model in patients presenting for dental care. Oral Health Prev Dent. 2007;5:39-48
59
other risk determin
ants.
dental status,
smoking status,
diabetic
attachment
loss/age ratio,
number of teeth
lost,
number of sites
with pocket
depths ≥ 5mm,
percentage of
sites with bleeding
on probing,

It is a continuous multilevel risk
assessment model that
incorporates subjective tooth
and site risk assessments and
generates a functional
diagram, and depending on
the area of the polygon
categorizes the patient into
low-, medium- and high-risk
categories.
60

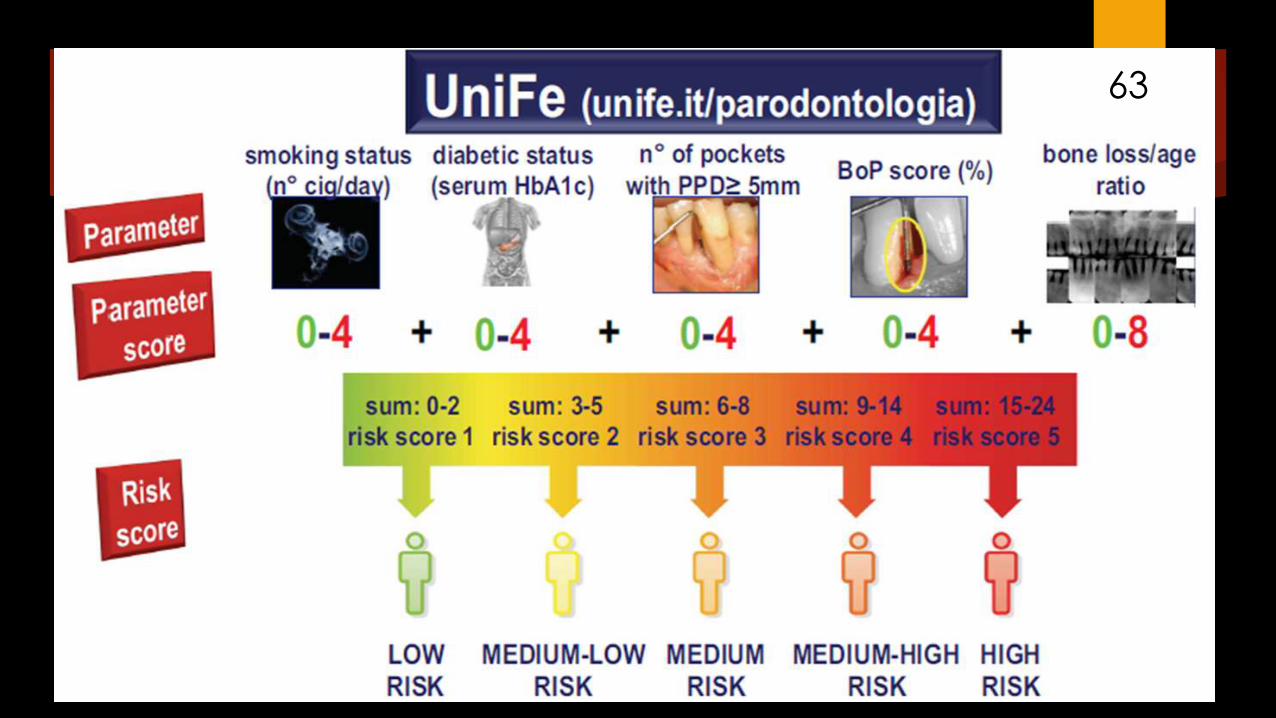
The simplified method(UniFe) for
periodontal risk assessment
In 2009, Trombelli and co-workers proposed a new objective method
(UniFe) (Union of European Railway Industries) in order to simplify the risk
assessment procedures.
Risk assessment according to UniFe method is based on five
parameters, derived from the patient medical history and clinical
recordings.
Trombelli L, Farina R, Ferrari S, Pasetti P, Calura G. Comparison between two methods for periodontal risk assessment. Minerva Stomatol. 2009;58:277-287
61

62
Smoking status,
Diabetic status (both type 1 and
type 2),
Number of sites with probing
depth ≥ 5mm,
Bleeding on probing score,
Bone loss/age records
63
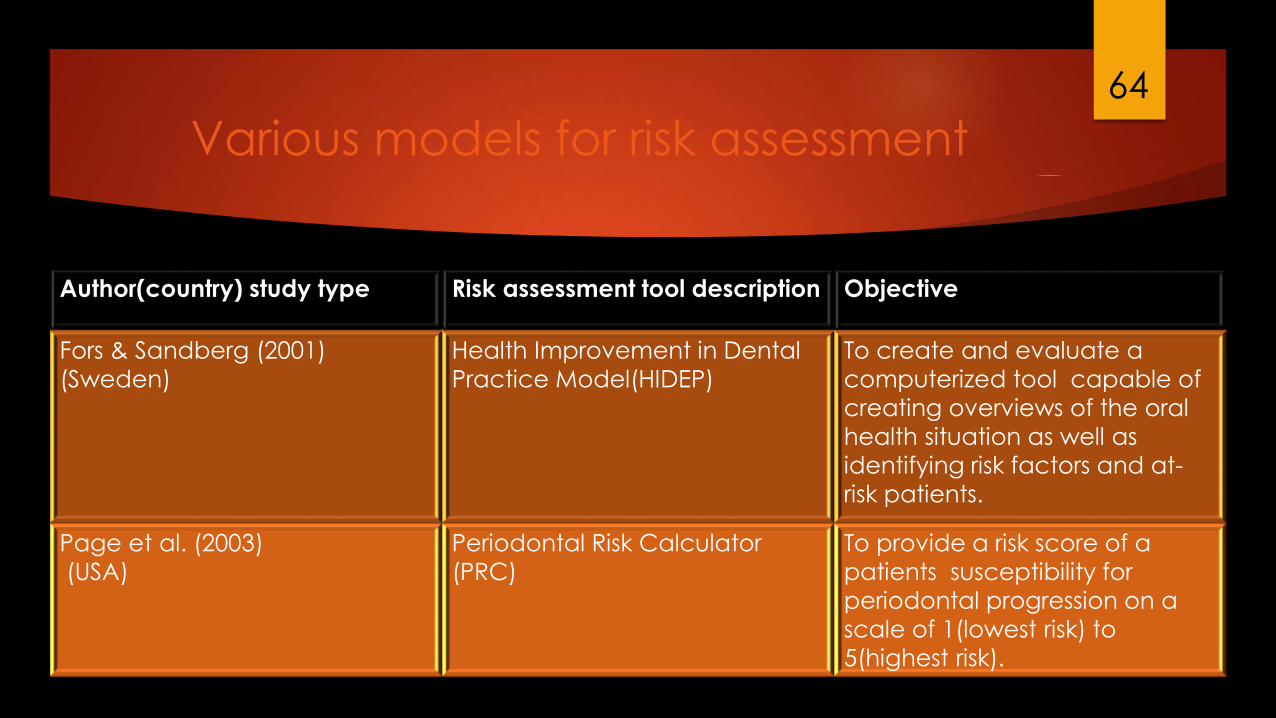
Various models for risk assessment
Author(country) study type Risk assessment tool description Objective
Fors & Sandberg (2001)
(Sweden)
Health Improvement in Dental
Practice Model(HIDEP)
To create and evaluate a
computerized tool capable of
creating overviews of the oral
health situation as well as
identifying risk factors and at-
risk patients.
Page et al. (2003)
(USA)
Periodontal Risk Calculator
(PRC)
To provide a risk score of a
patients susceptibility for
periodontal progression on a
scale of 1(lowest risk) to
5(highest risk).
64
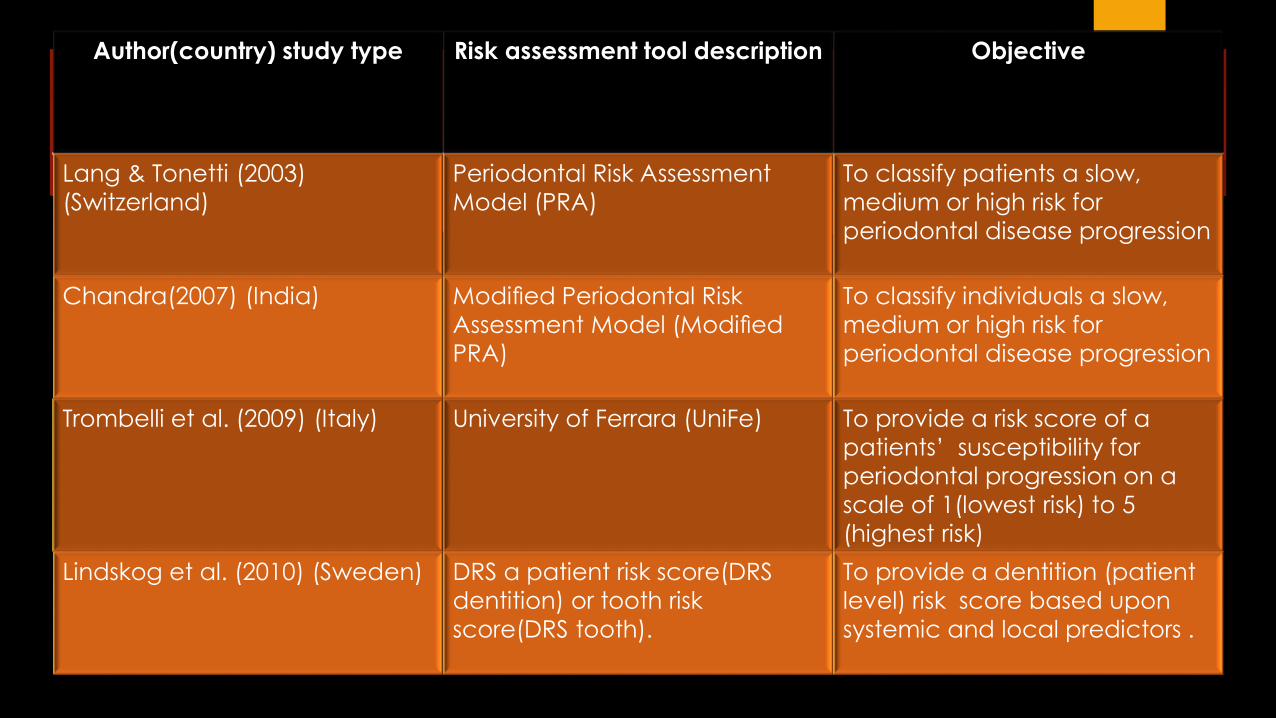
Author(country) study type Risk assessment tool description Objective
Lang & Tonetti (2003)
(Switzerland)
Periodontal Risk Assessment
Model (PRA)
To classify patients a slow,
medium or high risk for
periodontal disease progression
Chandra(2007) (India) Modified Periodontal Risk
Assessment Model (Modified
PRA)
To classify individuals a slow,
medium or high risk for
periodontal disease progression
Trombelli et al. (2009) (Italy) University of Ferrara (UniFe) To provide a risk score of a
patients’ susceptibility for
periodontal progression on a
scale of 1(lowest risk) to 5
(highest risk)
Lindskog et al. (2010) (Sweden) DRS a patient risk score(DRS
dentition) or tooth risk
score(DRS tooth).
To provide a dentition (patient
level) risk score based upon
systemic and local predictors .
65

Author(country) study type Risk assessment tool description Objective
Teich (2013) (USA) Risk Assessment-Based
Individualized Treatment(RABIT)
To classify patients as low,
medium or high risk for
periodontal disease progression
or caries risk with
accompanying
recommendation for
maintenance visit interval
L€uetal.(2013) (China) PRA(as proposed by Lang &
Tonetti 2003):
To classify patients as low,
medium or high risk for
periodontal disease
progression.
Busby et al. (2014) (UK) Oral Health Status(OHS) as part
of Den Plan Excel/ Previsor
Patient Assessment(DEPPA)
To provide patient-level risk
scores for periodontal disease,
caries and oral cancer.
66

Conclusion
Risk assessment is an important part of modern day periodontal practice. It isrecommended that systemic and local risk factors are documented alongside the
diagnosis in patients′ case records.
The practice of risk assessment allows dental care professionals the opportunity toimprove dental and medical outcomes in the general population and in specificpopulation groups by focusing on early identification and prevention of dentaldiseases, especially periodontal disease.
67

References Carranza. Clinical periodontology 9th , 10th and 11th edition
Periodontal risk assessment, diagnosis and treatment planning Periodontology 2000, Vol. 25, 2001, 37–58
Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health PrevDent. 2003;1:7-16
Chandra RV. Evaluation of a novel periodontal risk assessment model in patients presenting for dental care. Oral Health Prev Dent. 2007;5: 39-48
Beck JD. Risk assessment revisited. Community Dent Oral Epidemiol. 1998;26:220–5
American Academy of Periodontology statement on risk assessment. Journal of Periodontology 2008; 79: 202.
Haffajee AD, Socransky SS: Microbial etiological agents of destructive periodontal diseases. Periodontol 2000 1994; 5:78-111.
Elizabeth Koshi, S. Rajesh, Philip Koshi,and P. R. ArunimaRisk assessment for periodontal disease J Indian Soc Periodontol. 2012 JulSep; 16(3): 324–328
Aous Dannan PERIODONTAL RISK ASSESSMENT; ARE WE ON THE RIGHT TRACK? Archives of Oral Sciences & Research 2011;1(3):162-167
Kornman KS, Crane A, Wang HY, Newman MG, Pirk FW, Wilson TG, Jr, et al. The interleukin I genotype as a severity factor in adult periodontal disease. J Clin Periodontol. 1997;24:72–7
Papapanou PN: Risk assessments in the diagnosis and treatment of periodontal diseases. J Den Edu 1998; 62:822-839
Page RC, Beck JD: Risk assessment for periodontal diseases. Int Den J 1997; 47:61-87
68

69


















