Right Side Up-Falls Prevention Continuum · evaluation and recommendations for patient care....
40
Right Side Up-Falls Prevention Continuum
Transcript of Right Side Up-Falls Prevention Continuum · evaluation and recommendations for patient care....

Right Side Up-Falls
Prevention Continuum
Falls in the Elderly
- Each year 1 in 3 adults age 65 or older falls
- Half of those are repeat fallers
- Lead to significant morbidity and mortality
- Fall related costs for those 65 or older total $19 billion in 2000. Projected to reach $55 billion by 2020
- Fatal fall rates increased 42% between 2000 and 2006
The Scope
1. Falls among older adults: Figures and maps. CDC. [Online] January 19, 2009. [Cited May 14, 2010]. http://www.cdc.gov/ncipc/duip/adultfallsfig-maps.htm.

Falls in the Elderly
A Long-“Standing” Problem
Figure 1. Age adjusted fall injury rates among men and women aged 65 years or older.(1)

Falls in the Elderly
Figure 2. Percent of US population by age divided into five age groups.(1)
An Increasing Problem
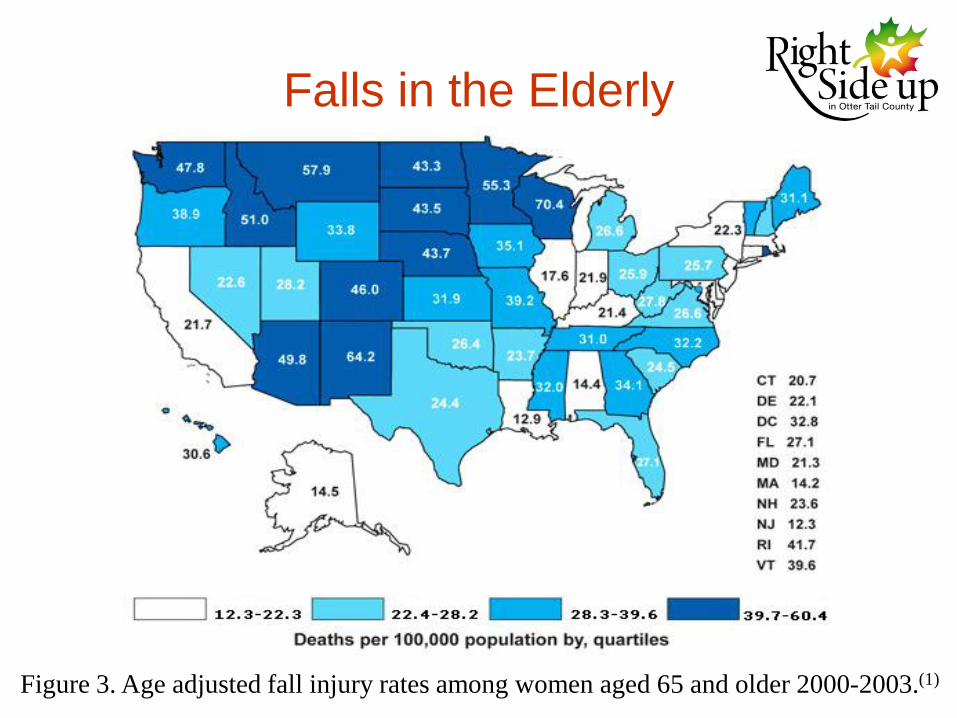
Falls in the Elderly
Figure 3. Age adjusted fall injury rates among women aged 65 and older 2000-2003.(1)

Falls in the Elderly
Figure 4. Age adjusted fall injury rates among men aged 65 years and older 2000-2003.(1)

Falls in the Elderly
Otter Tail County, MN
- 16% female pop. age 70 or older (state
10%)
- 12% male pop. age 70 or older (state 7%)
- Falls the leading cause of injury-related
mortality in those 75 or older
• Project funding from USDA
• Partners:– University of Minnesota Extension Service & Nutrition
Service, Center on Aging & Geriatric Education Center
– Minnesota Department of Health
– Minnesota Board on Aging
– Lake Region Healthcare
– Otter Tail County Public Health
– Central Minnesota Area Health Education Center
– Land of the Dancing Sky Area Agency on Aging.

Goal:
To address the prevention and management
of falls and falls risks in the elderly through
the development of a comprehensive and
coordinated continuum of care.
• Gaps Identified
• Need for instructors for evidence-based programs to reach persons at risk for falls
• Providers assessing risk and making referrals
• Need for communication between provider organizations about persons falls risk when transferred from one setting to another.
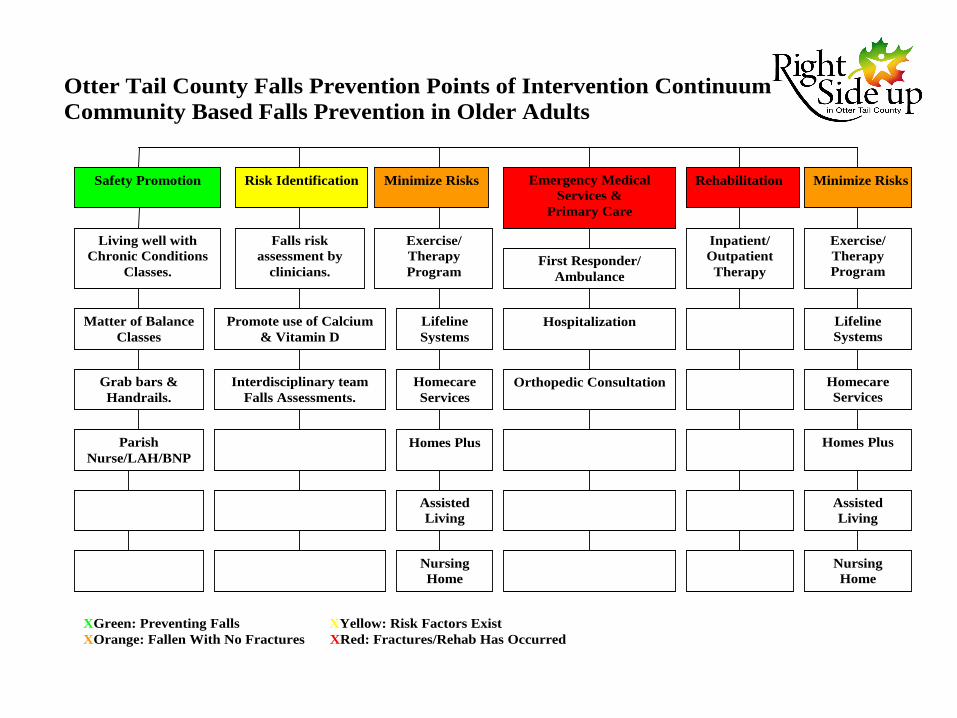
Otter Tail County Falls Prevention Points of Intervention Continuum
Community Based Falls Prevention in Older Adults
Safety Promotion Risk Identification Minimize Risks Emergency Medical
Services &
Primary Care
Rehabilitation Minimize Risks
Living well with
Chronic Conditions
Classes.
Falls risk
assessment by
clinicians.
Exercise/
Therapy
Program First Responder/
Ambulance
Inpatient/
Outpatient
Therapy
Exercise/
Therapy
Program
Matter of Balance
Classes
Promote use of Calcium
& Vitamin D
Lifeline
Systems
Hospitalization Lifeline
Systems
Grab bars &
Handrails.
Interdisciplinary team
Falls Assessments.
Homecare
Services
Orthopedic Consultation Homecare
Services
Parish
Nurse/LAH/BNP
Homes Plus
Homes Plus
Assisted
Living
Assisted
Living
Nursing
Home
Nursing
Home
XGreen: Preventing Falls XYellow: Risk Factors Exist
XOrange: Fallen With No Fractures XRed: Fractures/Rehab Has Occurred

• Safety Promotion
Target Population: Persons living in the community.
Primary Risk Factors: Vision, Environment, Exercise, and Medication Management
Interventions: Educational Classes, Adaptive devices such as grab bars and Handrails or referrals to Parish Nurse or LAH/BNP
• Chronic Disease Management Educational
Programs
• Usually 6 - 8 weeks of classes one time a
week for 2 - 2.5 hours
• Taught by trained peer leaders
• Living Well with Chronic Conditions or
• Matter of Balance or
• Arthritis Exercise Programs
• Inter-Professional Team Falls Assessments
– Public Health/Home Health-home environment
– Medical Students-Medical conditions that can
increase risk of falls
– Pharmacy Students-medication review and
assessment
• Assessment Process•Referrals
– Who can refer?
• Anyone
– Who to refer?
• Individuals with history of falls
• Individuals at risk for falls
– When to refer?
•Home Visit & Reports

Assessment Tool
• Environmental assessment
• Medical history
• Medical systems review
• Mental status
• Physical assessment
– Orthostatic BPs, balance, strength
• Medication Review
Drug-Induced Falls
• Drugs causing orthostasis
• Drugs causing ataxia
• Drug causing lethargy, weakness
• Drugs causing pseudoparkinsonism
Drug-Induced CNS Depression
• Barbiturates
• Sedative/Hypnotics
• Antidepressants
• Antihistamines
• Muscle relaxants
•Narcotic analgesics
•Anxiolytics
•Antipsychotics
•Antihypertensives
•Etc.
Drug-Induced Orthostatic Hypotension
• Antihypertensives (atenolol, metoprolol, CoReg,…)
• Diuretics (HCTZ, furosemide,…)
• Nitrates (NTG, Isosorbide,…)
• Calcium Channel Blockers (Norvasc, Procardia, diltiazem,…)
• ACE Inhibitors (lisinopril,…)
• Antiparkinson (Sinemet, Requip, Parlodel,…)
• Antipsychotics (Risperdal, Seroquel, Zyprexa,…)
• Antidepressants (amitriptyline, imipramine, doxepin,…)
• Alpha Blockers (Minipress, Hytrin, Cardura, Flomax)

Orthostatic Drug
YOUNG PERSON OLD PERSON
Orthostatic Hypotension Orthostatic Hypotension
+
Balance/C.V. Problems
Fall + Osteoporosis
Hip Fracture
Prolonged Healing/Incomplete Healing
Minor Adverse Effect Permanent Disability
(Death)
Case #1
• A.B. is a 56 y.o. female with a complicated medical history including
a long history of chronic pain, for which she was once prescribed
gabapentin. She was taking a large dose of gabapentin (probably
800 mg tid) and during this time she developed a tremor and fell
many times. She ended up in the ED after a fall and the gabapentin
was discontinued. Since that hospitalization (some time in early
2009) she has moved into her current apartment and has not had
any falls.
• Past medical history includes: Spinal Stenosis, Chronic pain,
Fibromyalgia, Type 2 Diabetes, COPD, Chronic bronchitis,
Depression, Dyslipidemia, Possible MS (some confusion about her
diagnosis), Possible PTSD (nurse did not know about this diagnosis)

Case #1
• Medications• Effexor XR 300 mg qd
• Glipizide 5 mg qd
• Glucophage 500 mg bid
• Lantus 20 units qhs
• Novolin R sliding scale
• Spiriva 2 puffs qd
• DuoNeb qid
• Trazodone 100-200 mg qhs
• Amitriptyline 75 mg bid
• Morphine sulfate ER 60 mg q 12 hours
• Diazepam 10 mg bid
• Simvastatin 80 mg qhs
• Zetia 10 mg qd
• Omeprazole 40 mg qd
• Fish oil 1000 mg bid
• Vitamin B Complex bid
• SennaS bid
• Miralax 17gm qd
• Vicodin 5/500 bid prn pain (uses ~2 tabs
daily for breakthrough pain)
• Ibuprofen 800 mg prn pain (for breakthrough
pain, sometimes uses before Vicodin)
• Lasix 20 mg prn qd for swelling (uses 3 or 4
times weekly)
• Propranolol 20 mg 1-2 tabs q 4-6 hours prn
shakes (uses when needs to write)
• Albuterol MDI 2 puffs prn (uses 4-5 x daily)
• Bisacodyl 5 mg 1-2 tabs prn constipation
(uses 2 every 3 days)
• MOM 30 ml prn
• DuoNeb prn
• Refresh eye gtts prn
• Erythromycin eye ung qhs prn

Recommendations• Environmental
– Very little clutter, well maintained
• Level of Care
– Homemaker help with errands
– home health nurse
– consider PT/OT
• Medications
– Pain journal monitoring
– Reassess amitriptyline/Effexor
– Trial decrease diazepam
– Calcium and Vitamin D
• Strength, gait, balance
– Encourage utilization of walker
• Chronic medical problems
– Low back and knee pain
– MS history?
– Improve diabetes control/diabetes educator
Sharing RecommendationsApril 27, 2010
Dear A.B.,
Thank you for visiting with us and participating in the Falls Program. We enjoyed
meeting with you and we appreciate your willingness to help our students learn.
Based on the visit by part of our team on April 7, 2010, our committee has developed
the following recommendations for your consideration:
1. We noticed the following positive things to help decrease your risk of falls during
our assessment. Your apartment was clean and free of clutter. Your bathroom had
grab bars and a seat in the tub.
2. As we discussed during our visit, consider meeting with a Diabetes Educator to
strategize ways to better control your diabetes. We are asking your physician for a
possible referral.
3. We encourage you to use your walker whenever necessary, especially when
leaving the apartment.
4. Meeting with an Occupational or Physical Therapist could be beneficial for you to
reduce your risk of falls. We are asking your physician for a possible referral.
5. As we discussed during our visit, starting a pain journal could be a good way to
understand how effective your pain medications are for you. Consider keeping a
journal that includes a rating of how bad the pain is before you take your medication,
what medication you take, how much medication you take, and a rating of your pain
20-30 minutes after taking your pain medication.
6. The dose of Effexor XR you are on, 300 mg daily, is an effective dose for both
depression and pain management. It works in much the same way as your
amitriptyline and we will have your physician discuss with you if changes are
appropriate or not.
7. Diazepam can cause marked drowsiness and increase your risk of falls. We will
have your physician discuss with you if changes are appropriate or not.
8. Consider the addition of Calcium 600 mg twice daily and Vitamin D 1000 – 2000
IU daily. Calcium and Vitamin D can help strengthen your bones and decrease your
risk of falls.
A letter has been mailed to your doctor with recommendations from the Lake Region
Healthcare Corporation Falls Committee to help prevent future falls. If you have any
questions, please feel free to contact Todd Johnson at 218-736-8157 or Mark Dewey
at 218-736-8057.
Sincerely,
The Falls Committee
Patient: A.B.
D.O.B
Dear Dr.,
One of your patients, A.B., has recently participated in an Interprofessional
Falls Prevention and Education Program. This program combines students
from medicine, pharmacy, nursing, public health and/or physical therapy to
collaboratively assess individuals at risk for falls in an effort to reduce the
incidence of falls. Students then present the patient case to a team of
professionals, the Lake Region Healthcare Corporation Falls Committee, for
evaluation and recommendations for patient care.
Attached is a report of the Falls Committee’s findings from the patient visit,
which occurred at A.B.’s home, along with the corresponding
recommendations from the Falls Committee meeting on April 25, 2010.
Thank you for allowing us to participate in A.B.’s case. If you have any
questions or concerns, please contact Todd Johnson at 218-736-8157.
Sincerely,
Todd Johnson, PharmD
LRHC Falls Committee Chairperson
Case #2
• C.D. is a 87 y.o. female and excellent historian… but
hesitant to report falls. She reports falling 1/16/2010,
4/09, and says fell and “did a number” on her back a
year or so before. Home health nurse reveals patient
experiences “slides” and near falls and patient agrees
these occur more frequently. Patient denies dizziness
and attributes falls to “weakness” and arthritis.
• Past Medical History: Arthritis, HTN, COPD, Restless
Leg Syndrome, Insomnia, Diverticulosis, Urinary
urgency, Hx of hypokalemia?

Case #2
• Medications• Diovan 320mg daily
• Aspirin 81mg daily
• Coumadin as directed… monitored
and adjusted monthly
• Triamterene-HCTZ 37.5/25mg daily
• KlorCon 20mEq ii qam, i qpm
(dissolve in water)
• Trixaicin HP (capsaicin) topical cream
to affected areas nightly
• Silver tonic daily
• Enablex 7.5mg daily (just started, was
on Detrol LA)
• Tylenol 650mg ii bid
• Systane i gtt ou bid
• OTC Vitality Calcium Complete ii qam,
i qam
• OTC B12 1000mcg daily
• OTC Vitamin Replenex for Joints daily
• OTC Vitality MVI w/ Minerals as
directed (1 packet am, 1 packet pm)
• OTC NutraView Vitamins for Eyes
daily
• Carbidopa-Levodopa 25/100mg prn for
RLS... no longer taking
• Clonazepam 1mg prn for RLS
• Fiberwise qhs prn
• Discontinued – Detrol LA 4mg daily,
CranBarrier qhs
Recommendations
• Environmental
– House free of clutter and no notable fall risks
• Level of Care
– Appears appropriate with family and home health assistance
• Medication Recommendations
– Reassess Klonopin, Rule out iron deficiency, trial of Requip or
Mirapex
– Reassess Enablex benefit
• Strength, gait, balance
– Patient gets fatigued/weak easily with no sleep
– Patient states good ambulation with wheeled walker when rested
• Chronic Medical Problems
– Ongoing insomnia and restless legs
Sharing RecommendationsFebruary 23, 2010
Dear C.D.,
Thank you for visiting with us and participating in the Falls Program. We
enjoyed meeting with you and we appreciate your willingness to help our
students learn. Based on the visit by part of our team on February 9, 2010,
our committee has developed the following recommendations for your
consideration:
Restless Leg Syndrome and difficulty sleeping appear to have great impact
on your strength and balance. Please continue to work with your doctor to
improve your ability to sleep. As you were about to begin clonazepam 1mg
as needed for RLS at the time of our visit, please ask yourself these
questions to assess if the medication is safe and effective:
Can I fall asleep when I take the medication?
How long do I sleep when I take the medication?
Do I feel rested the next day or do I feel groggy, tired, or dizzy?
Please inform your doctor if clonazepam is not working well, stops working,
or makes you feel groggy and tired the next day.
You were also starting Enablex 7.5mg daily at the time of our visit. Is this
working for you? Please update your physician if this medication is not
working or if you experience troublesome side effects.
You have made adjustments to your home and lifestyle that benefit your
health and decrease your risk of falls. Continue to enlist the help of your
family and home health agency as needs arise.
A letter has been mailed to your doctor with recommendations from the
Lake Region Healthcare Corporation Falls Committee to help prevent future
falls. If you have any questions, please feel free to contact Eric
Christianson @ 218-736-8199.
Sincerely,
The Falls Committee
Patient: C.D.
DOB:
Dear Dr.,
One of your patients, C.D., has recently participated in an Interprofessional
Falls Prevention and Education Program. This program combines students
from medicine, pharmacy, nursing, public health and/or physical therapy to
collaboratively assess individuals at risk for falls in an effort to reduce the
incidence of falls. Students then present the patient case to a team of
professionals, the Lake Region Healthcare Corporation Falls Committee, for
evaluation and recommendations for patient care.
Attached is a report of the Falls Committee’s findings from the patient visit,
which occurred at C.D.’s home, along with the corresponding
recommendations from the Falls Committee meeting on February 22, 2010.
Thank you for allowing us to participate in JK’s case. If you have any
questions or concerns, please contact Eric Christianson at 218-736-8199.
Sincerely,
Eric Christianson, PharmD
LRHC Falls Committee Member

Physical Therapy Services
• Balance testing
– 8 foot Up & Go
– Romberg
• Outpatient therapy
– Vestibular testing
– Strength testing
– Gait assessment
– Wii

Otter Tail County Falls Prevention Points of Intervention Continuum
Community Based Falls Prevention in Older Adults
Safety Promotion Risk Identification Minimize Risks Emergency Medical
Services &
Primary Care
Rehabilitation Minimize Risks
Living well with
Chronic Conditions
Classes.
Falls risk
assessment by
clinicians.
Exercise/
Therapy
Program First Responder/
Ambulance
Inpatient/
Outpatient
Therapy
Exercise/
Therapy
Program
Matter of Balance
Classes
Promote use of Calcium
& Vitamin D
Lifeline
Systems
Hospitalization Lifeline
Systems
Grab bars &
Handrails.
Interdisciplinary team
Falls Assessments.
Homecare
Services
Orthopedic Consultation Homecare
Services
Parish
Nurse/LAH/BNP
Homes Plus
Homes Plus
Assisted
Living
Assisted
Living
Nursing
Home
Nursing
Home
XGreen: Preventing Falls XYellow: Risk Factors Exist
XOrange: Fallen With No Fractures XRed: Fractures/Rehab Has Occurred
Falls Risk Assessments:
Short-term outcomes
- Telephone Interview
- 16 visits in last 6 months
- Data collected from 11/16 visits
- Data from 7 patients and 6 caregivers
- Average time from visit 3.5 months

Falls Risk Assessments:
Short-term outcomes
Patient Questionnaire
1. Did you find the falls visit helpful?
2. Did you receive our recommendation letter following our visit?
3. Were the suggestions helpful?
If so, what did you find the most helpful (med review, environment analysis, therapy suggestions, ect.)
What wasn’t helpful?
4. Are there things you are doing differently to reduce your risk of falls like exercising or using your walker more?
5. Have you discussed the suggestions with your doctor?
6. Have you had any falls since the visit?
7. Has the number of falls or near falls increased, decreased, or stayed the same since our visit?
8. Do you think this program would be helpful for others you know?
9. Do you have any suggestions to improve the program?
Falls Risk Assessments:
Short-term outcomes
Home Health/Community Services Provider Questionnaire
1. Were you present for the falls visit?2. Did you find the visit helpful?3. On a scale of 1-10, how beneficial was this
program to your patient?4. Has the number of falls or near falls increased,
decreased or stayed the same since our visit?5. Do you think this program would be helpful for
others you know?6. Do you have any suggestions for improvement?

Falls Risk Assessments:
Short-term outcomes
Results:Patient Responses
Follow-up Question Mean (%)
Found the visit to be helpful 100
Doing something differently to reduce falls 78
Recommendations were helpful 100
Discussed suggestions with doctor 57
Have had falls since the visit 17
The program would be helpful for others 86

Falls Risk Assessments:
Short-term outcomes
Results:Caregiver Responses
Follow-up Question Mean %
Present for visit 100
Found the visit helpful 100
Client’s falls have decreased since visit 50
Visit would be helpful for other clients 100
Caregiver rated benefit of visit to patient (1-10): 7

Falls Risk Assessments:
Short-term outcomes
Data Analysis:
Limitations:
- Sample size
- <100% response
- Barriers to implementation of recommendations
- Variable time intervals between visit and
response
Adverse Events:
- 1 pt had fall requiring hospitalization
- 1 pt admitted to NH for other reasons

Falls Risk Assessments:
Short-term outcomes
Implications:
Decrease incidence of falls aging population
• NNT = 2 ?
NNT for other common preventative measures
• NNT= 18…Number of pt >60 with HTN that need to
be treated to prevent one coronary event over 5
years.
• Thrombolytic therapy in acute MI…NNT=33
• Blood pressure control after stroke to prevent over 8
years…NNT=26

Falls Risk Assessments:
Short-term outcomes
Future Strategies:
1.Continue to spread awareness of program
2.Standardize data collection
• Questionnaire at 3 months and 6 months
3.Long-term follow-up
• Outcomes at >12 months
• Does prevention falls= prevention fall related injury?

Questions?