
Right heart test for the right HF patient // Mexico ...
28
©2013 MFMER | 3248567-1 ©2013 MFMER | 3248567-1 Right heart test for the right HF patient // Mexico, October 2016 Hector I. Michelena MD FASE FACC Associate Professor of Medicine
Transcript of Right heart test for the right HF patient // Mexico ...

©2013 MFMER | 3248567-1©2013 MFMER | 3248567-1
Right heart test for the right HF
patient // Mexico, October 2016
Hector I. Michelena MD FASE FACCAssociate Professor of Medicine

©2013 MFMER | 3248567-2
DISCLOSURE
No Relevant Financial Relationship(s)
No Off Label Usage

©2013 MFMER | 3248567-3
Case
• 50 year old white female, dilated CMP
• Hx Mv repair, severe functional MR
• Presented with syncopal event
• Noted to have 3rd Degree Heart Block
• PPM implanted
• Father died at age 59 of “heart disease”
• Needed AICD for VT later

©2013 MFMER | 3248567-4
Case
• Blood work
• Hgb 14.8 WBC 5.7 Plt 190
• NA 142 K 4.2 Cr 1.1
• Physical exam
• Normotensive, Normal Weight
• Paradoxically Split S2, otherwise Nl

©2013 MFMER | 3248567-5
Case

©2013 MFMER | 3248567-6
©2013 MFMER | 3248567-7
Case
A. Coronary artery Disease
B. Cardiac Sarcoid
C. Hypertrophic Cardiomyopathy
D. Dilated Cardiomyopathy

©2013 MFMER | 3248567-8
Case
A. Coronary artery Disease
B. Cardiac Sarcoid (Isolated)
C. Hypertrophic Cardiomyopathy
D. Dilated Cardiomyopathy
Left atrial wall from Mv repair surgery: pathologic confirmation

©2013 MFMER | 3248567-9
Cardiac Sarcoidosis
**
*Extensive Transmural
fibrosis non-coronary distribution
non-necrotizing granulomatous
inflammation, giant multinucleated cells,
and epithelioid hystiocytes

©2013 MFMER | 3248567-10
Sarcoidosis
• Granulomatous inflammatory disease of unknown etiology involving multiple organs (immune system disorder)
• Main manifestations caused by pulmonary involvement
• pulmonary fibrosis
• right-sided heart failure
• pulmonary hypertension

©2013 MFMER | 3248567-11
PulmonaryNodules
SarcoidCXR

©2013 MFMER | 3248567-12
Cardiac SarcoidosisClinical Cardiac Features
• Can affect any portion of the heart
• Can produce a myriad clinical problems that may simulate other more common disorders (palpitations, atypical chest pain, syncope, etc)
• Syncope or sudden death
• Heart Block, VT, VF
• CHF
• Can also be asymptomatic

©2013 MFMER | 3248567-13
Cardiac SarcoidosisEchocardiographic Features
• Early: LV walls may be thick
• Late LV findings:
• Segmental thinning
• Regional wall motion abnormalities
• LV aneurysms
• LV enlargement, reduced function
• Diastolic dysfunction
• Pericardial effusion
• Valvular dysfunction(MR)
• With pulmonary involvement
• RVE, decreased RV function and RVH
©2013 MFMER | 3248567-14
Cardiac SarcoidosisIn Who??
• <55 yo ECG BLOCK
• Known extracardiac sarcoidwith heart symptoms
• <55 yo
• Monomorphic VT
• Dilated CMP
• HCM
• ARVD
©2013 MFMER | 3248567-15
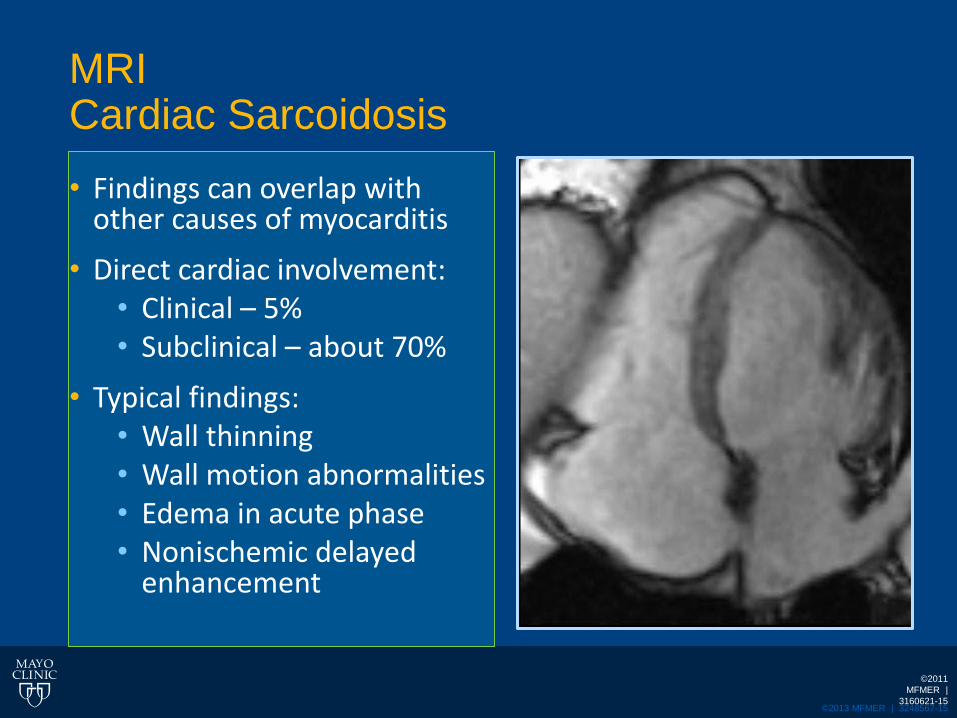
MRICardiac Sarcoidosis
• Findings can overlap with other causes of myocarditis
• Direct cardiac involvement:• Clinical – 5%• Subclinical – about 70%
• Typical findings:• Wall thinning• Wall motion abnormalities• Edema in acute phase• Nonischemic delayed
enhancement
©2011
MFMER |
3160621-15
©2013 MFMER | 3248567-16
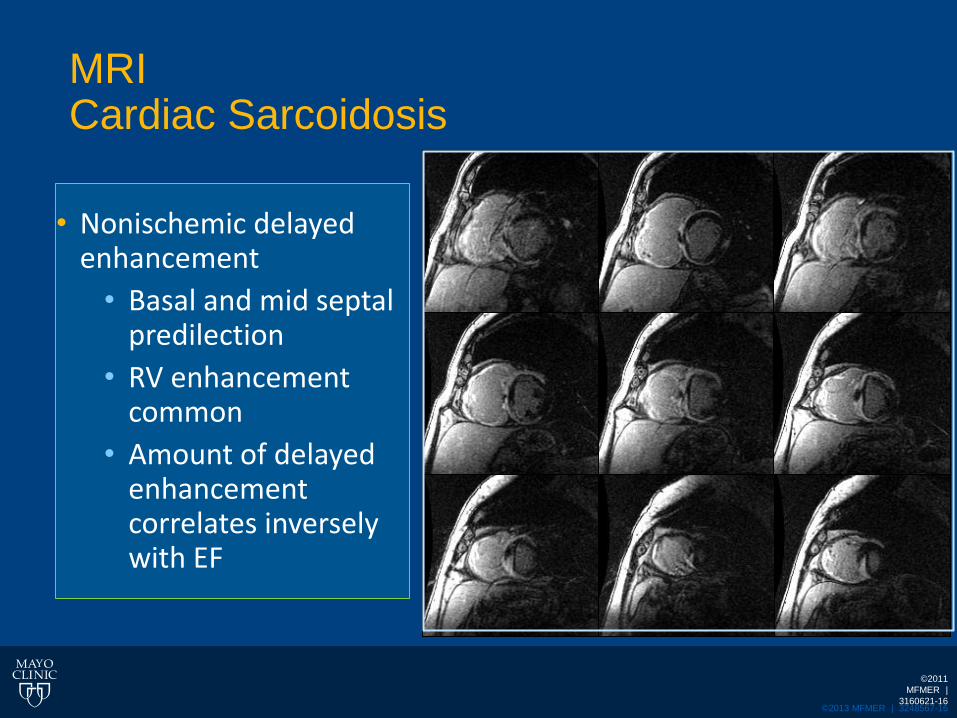
MRICardiac Sarcoidosis
©2011
MFMER |
3160621-16
• Nonischemic delayed enhancement
• Basal and mid septal predilection
• RV enhancement common
• Amount of delayed enhancement correlates inversely with EF
©2013 MFMER | 3248567-17
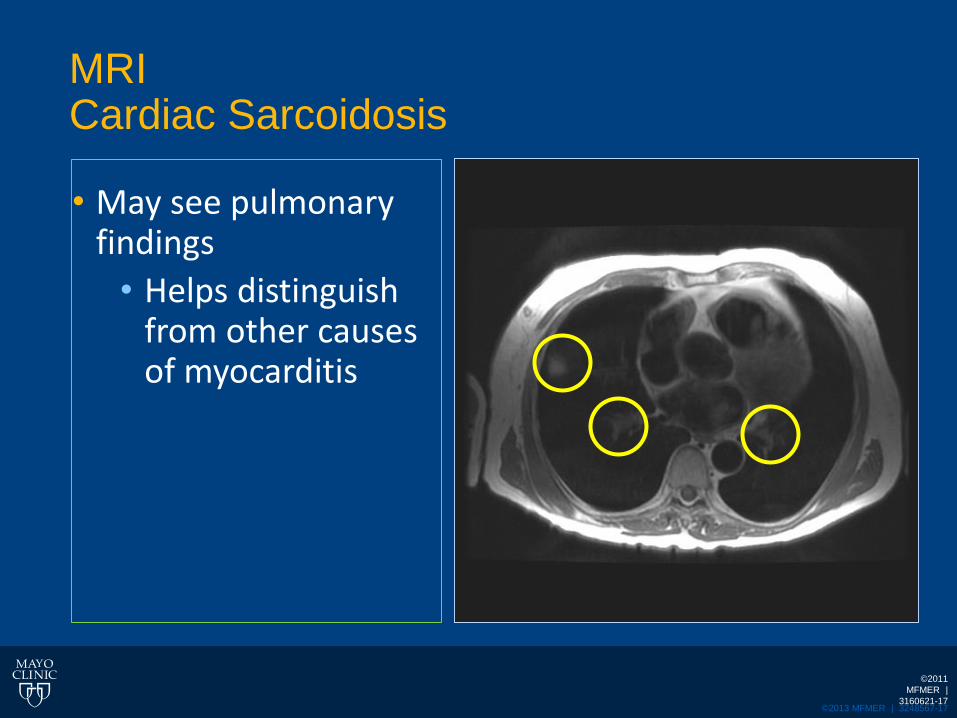
MRICardiac Sarcoidosis
• May see pulmonary findings
• Helps distinguish from other causes of myocarditis
©2011
MFMER |
3160621-17

©2013 MFMER | 3248567-18
Greulich et al: J Am Coll Cardiol Img 6:501, 2013
©2013 MFMER | 3248567-19
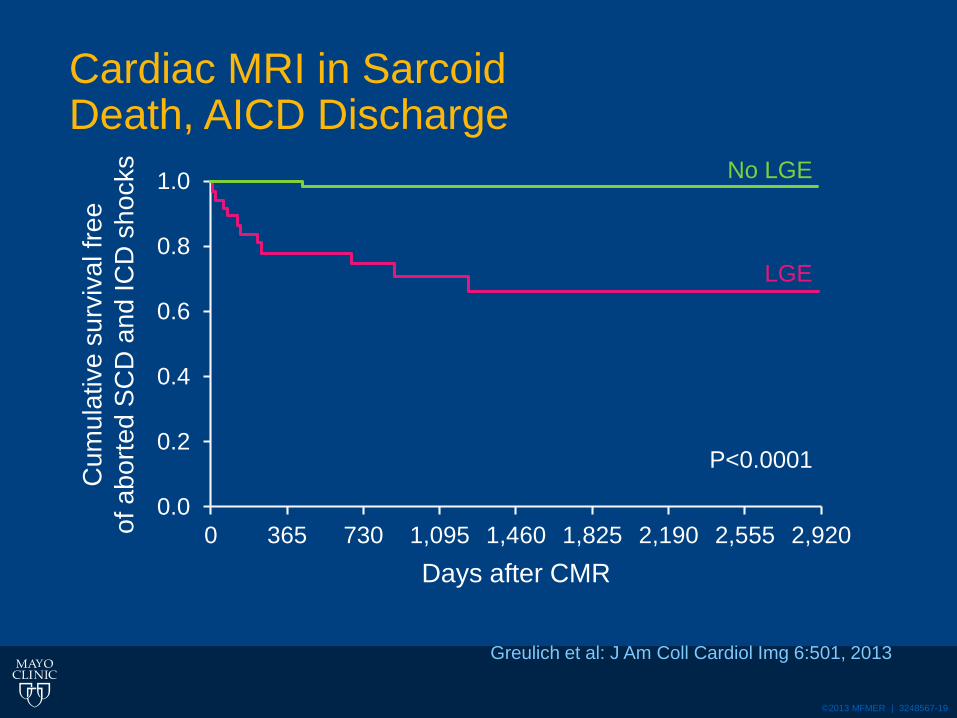
Cardiac MRI in SarcoidDeath, AICD Discharge
0.0
0.2
0.4
0.6
0.8
1.0
0 365 730 1,095 1,460 1,825 2,190 2,555 2,920
Greulich et al: J Am Coll Cardiol Img 6:501, 2013
Days after CMR
Cu
mu
lative
su
rviv
al fr
ee
of a
bo
rte
d S
CD
an
d IC
D s
ho
cks No LGE
LGE
P<0.0001

©2013 MFMER | 3248567-20
Cardiac MRI in SarcoidDeath, AICD Discharge, VT
0.0
0.2
0.4
0.6
0.8
1.0
0 365 730 1,095 1,460 1,825 2,190 2,555 2,920
Greulich et al: J Am Coll Cardiol Img 6:501, 2013
Days after CMR
Cu
mu
lative
su
rviv
al fr
ee
of
ab
ort
ed
IC
D s
ho
cks, V
T a
nd
nsV
T
Patients at risk
No LGE 89 63 44 29 20 15 10 5
LGE 23 20 17 11 5 4 4 2
No LGE
LGE
P<0.0001

©2013 MFMER | 3248567-21
©2013 MFMER | 3248567-22
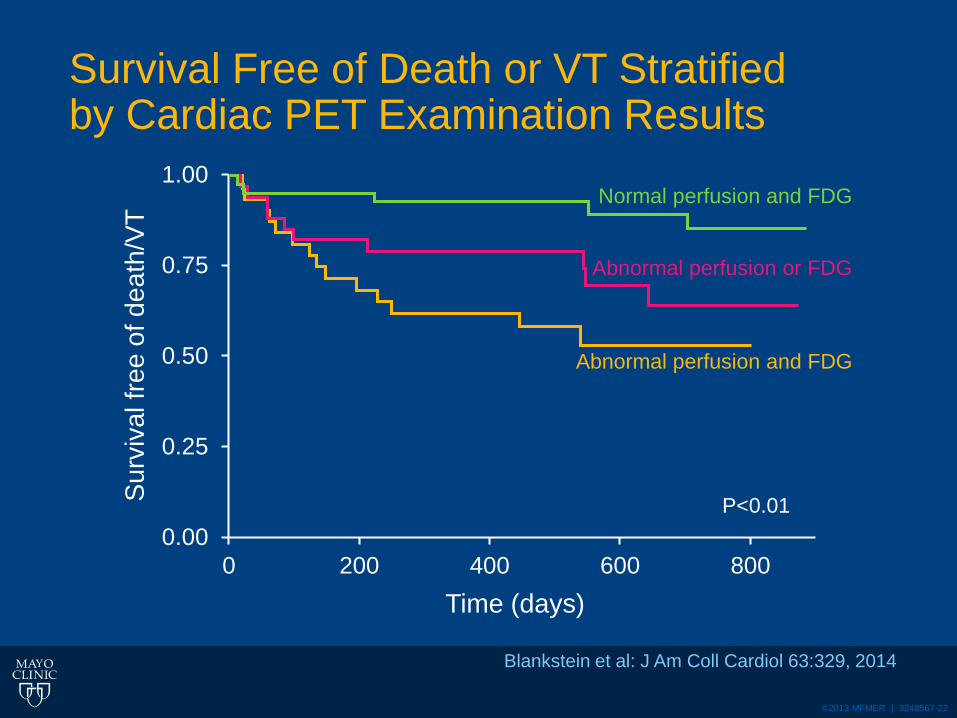
Survival Free of Death or VT Stratifiedby Cardiac PET Examination Results
0.00
0.25
0.50
0.75
1.00
0 200 400 600 800
Blankstein et al: J Am Coll Cardiol 63:329, 2014
Time (days)
Su
rviv
al fr
ee
of d
ea
th/V
T
P<0.01
Normal perfusion and FDG
Abnormal perfusion or FDG
Abnormal perfusion and FDG

©2013 MFMER | 3248567-23
Mantini et al: Clin Cardiol 35, 7, 410, 2012
©2013 MFMER | 3248567-24
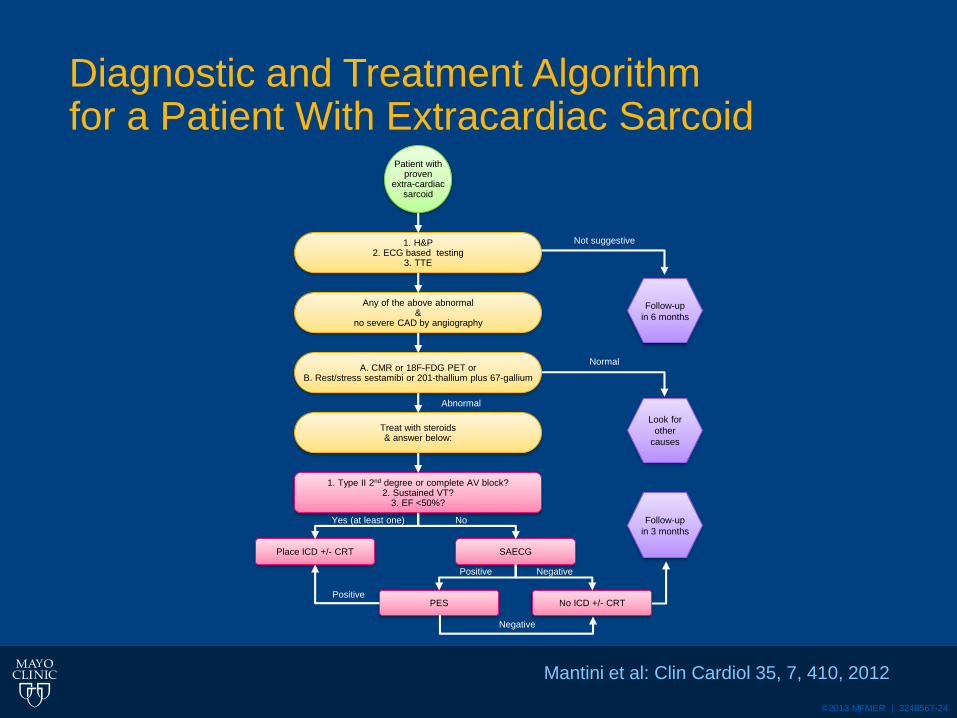
Diagnostic and Treatment Algorithmfor a Patient With Extracardiac Sarcoid
Mantini et al: Clin Cardiol 35, 7, 410, 2012
Patient withproven
extra-cardiacsarcoid
1. H&P2. ECG based testing
3. TTE
Any of the above abnormal&
no severe CAD by angiography
A. CMR or 18F-FDG PET orB. Rest/stress sestamibi or 201-thallium plus 67-gallium
Treat with steroids& answer below:
1. Type II 2nd degree or complete AV block?2. Sustained VT?
3. EF <50%?
Place ICD +/- CRT SAECG
PES No ICD +/- CRT
Follow-up
in 6 months
Look for
other
causes
Follow-up
in 3 months
Not suggestive
Normal
Negative
Positive
Positive Negative
NoYes (at least one)
Abnormal
©2013 MFMER | 3248567-25
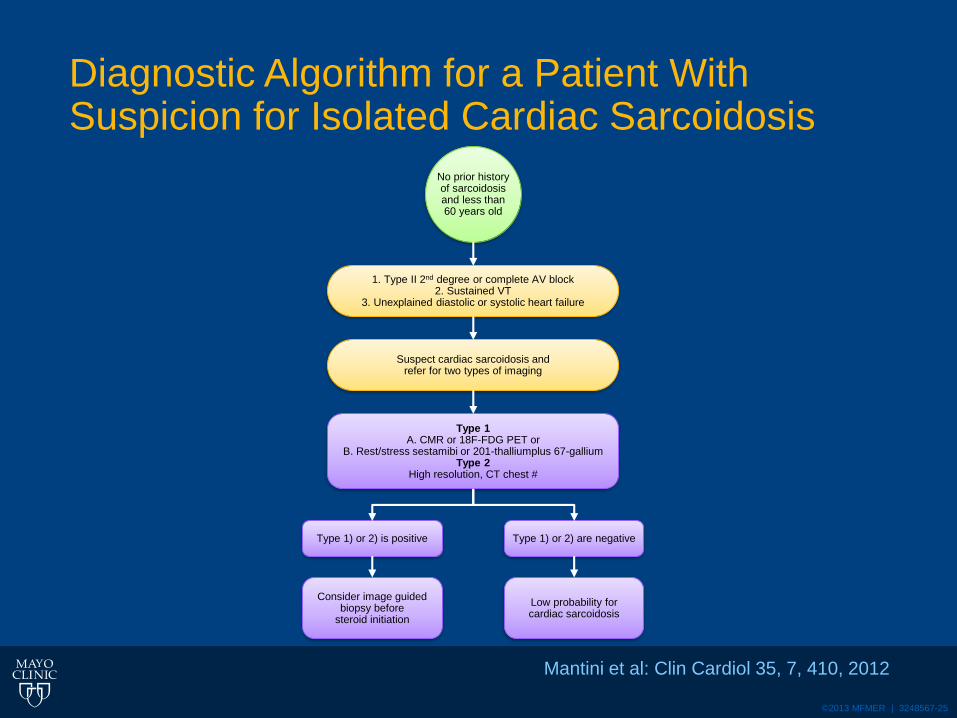
Diagnostic Algorithm for a Patient With Suspicion for Isolated Cardiac Sarcoidosis
Mantini et al: Clin Cardiol 35, 7, 410, 2012
No prior historyof sarcoidosisand less than60 years old
1. Type II 2nd degree or complete AV block2. Sustained VT
3. Unexplained diastolic or systolic heart failure
Suspect cardiac sarcoidosis andrefer for two types of imaging
Type 1A. CMR or 18F-FDG PET or
B. Rest/stress sestamibi or 201-thalliumplus 67-galliumType 2
High resolution, CT chest #
Type 1) or 2) is positive Type 1) or 2) are negative
Consider image guided biopsy before
steroid initiation
Low probability forcardiac sarcoidosis
©2013 MFMER | 3248567-26
Cardiac Sarcoid
• CMR may have a higher specificity for diagnosis of cardiac sarcoid
• PET appears to be more sensitive
• Both PET and CMR appear predictive of outcomes
• Local expertise and patient factors will determine optimal testing
• RV Biopsy is gold standard
• Low sensitivity in 20% range (Patchy distribution)---Guided

©2013 MFMER | 3248567-27
Cardiac SarcoidTreatment
• Steroids remain treatment of choice
• No Randomized Trials
• Steroid therapy
• Appears to decrese mortality (non randomized)
• Appears to maintain LV function if initiated in patients with normal function at time of diagnosis
• LVEF improves in patients with mild to moderate LV dysfunction at time of diagnosis (our case)
• No improvement in LVEF in patients with severe LV dysfunction (<30%) at time of diagnosis

©2013 MFMER | 3248567-28
Questions & Discussion
28


















![[HF] FREEWEIGHT PRODUCTS - HOIST Fitness · [hf] flat bench hf-5163 [hf] 7-position folding f.i.d. bench hf-5167 new! warranty new! warranty [hf] 7-position f.i.d. olympic bench hf-5170](https://static.fdocuments.us/doc/165x107/5b5909d87f8b9ad0048c899a/hf-freeweight-products-hoist-fitness-hf-flat-bench-hf-5163-hf-7-position.jpg)