Richard C. Antonelli, MD, MS Medical Director of ... · Richard C. Antonelli, MD, MS Medical...
18
Richard C. Antonelli, MD, MS Medical Director of Integrated Care Boston Children’s Hospital, Harvard Medical School Director, National Center for Care Coordination Technical Assistance November 20, 2015 1
Transcript of Richard C. Antonelli, MD, MS Medical Director of ... · Richard C. Antonelli, MD, MS Medical...
Richard C. Antonelli, MD, MS
Medical Director of Integrated Care
Boston Children’s Hospital, Harvard Medical School
Director, National Center for Care Coordination Technical Assistance
November 20, 2015
1

Take Home Points• Integration is Essential for Success– evidence exists
• Care Coordination is Necessary but not Sufficient to Achieve Integration
• CC is the set of activities which occurs in “the space between”
– Visits, Providers, Hospital stays, Agency contacts
• Only way to succeed is to engage all stakeholders–including patients and families– as participants and partners
• Medical Home is a necessary, but not sufficient, component of high performing system
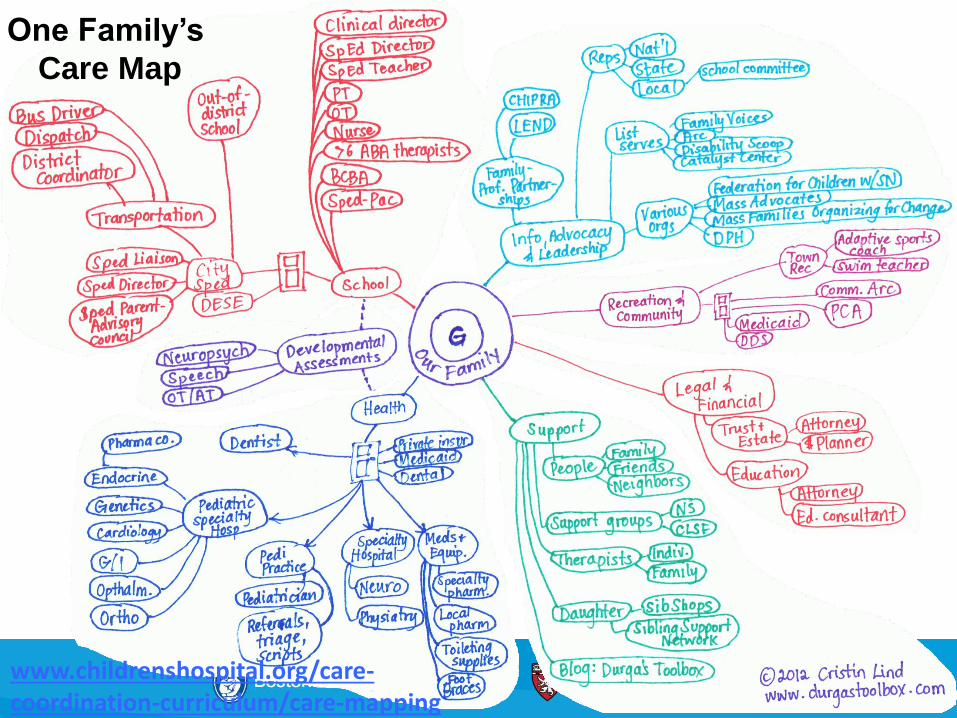
One Family’s
Care Map
www.childrenshospital.org/care-coordination-curriculum/care-mapping

% ofpopulation
0.5%
25%
74.5%
Healthy--Prevention, Surveillance
Chronic
Complex
% ofspend
25%
70%
5%

Healthy--Prevention, Surveillance
Chronic
Complex
Children with complex needs--Neurodevelopmental (Autism, etc.)--Behavioral/Psychiatric--Hematology/ Oncology
• Sickle cell• Hemophilia
--Technology dependent
Children with chronic conditions--Behavioral (ADHD, depression,
anxiety, PTSD) --Asthma-- Obesity--Diabetes

Care Coordination
Integrated Care seamless provision of health care services, from the perspective of the
patient and family, across entire care continuum.
It results from coordinating the efforts of all providers, irrespective of
institutional, departmental, or community-based
organizational boundaries.
Antonelli, Care Integration for Children with Special Health Needs:
Improving Outcomes and Managing Costs.
National Governors Association Center for Best Practices, 2012
Care Coordination is the set of activities in “the space between”-
Visits, Providers, Hospital Stays
Turchi RM, Antonelli RC et al. Patient- and Family-Centered Care Coordination: A Framework for Integrating
Care For Children and Youth Across Multiple Systems. Pediatrics. May 2014.
6

Key Elements Sample Measures
1) Needs assessment, continuing CC engagement
2) Care planning and coordination
3) Facilitating care transitions
4) Connecting with community resources/schools
5) Transitioning to adult care
Use of a structured care coordination needs assessment tool/process
Family engagement in co-creation and implementation of care plan
“Closing the loop”: timely communication after referral visit (to PCP/family/others)
t1Ask family: did you get what you wanted?
Care team members can access, update plan
Measure bundles, adaptations (HEDIS, CTM-P, CAHPS-PCMH/PICS, ABCD)
Link to family partner/family-run org/peersReferral connections madeBi-directional communication of results
Acquisition of self-management skillsID adult providers with capacity, expertise
t2
7

Family
Primary Care
Subspecialty Care
(Ambulatory)
C.B.O./ EI
DPH/Title V
Payer
Family-to-Family
Support
HMVM-CHAT +
Make referral Track referralRegistry entry
Receive reportIncorporate into care
planReview with family
Receive referralEvaluation
Care/Treatment Plan
Track referralsTrack measures
(close the loop outcomes)
Track referralsReport utilization
Quality family and provider experience
Integrated Model: Accountabilities Across All StakeholdersNew Measurement Approaches, Measure Bundles

Overview of measures to track impact of implementing changes
Link measures to Triple Aim outcomes!1.) Improve Patient/Family Experience
administer patient/family experience surveys (eg, PICS)2.) Improve Outcomes– Structural and Process
Tracking Use of CC needs assessments, care plans, care transitions:between providers; to community resources-- Close the loop performanceTrack outcomes using CCMT
3.) Reduce Costs Medical expenses: unnecessary ED utilization; rates of hospitalization and unplanned
readmissions; duplication of testing/resources4.) Triple Aim Plus 1-- Provider Experience matters
USABILITY & FEASIBILITY– Do Not Begin with Pay for Performance!! Provider/care team experienceCCMT or other tracking tooltime and resources it takes to implement, outcomes achieved from provider perspective

Legend
states with entities that are in
early stages of
engagement. Expressed
interest in developing care
coordination workforce
capacity on level of individual
institution and/or state-wide
program.*some sites may have
implemented since our last
communication
states with entities that have
used the Pediatric Care
Coordination Curriculum as a
resource to implement care
coordination workforce
capacity building
+ = states engaged in
statewide implementation,
some partnering with State
Title V programs
Across these states, we are aware of over
20 different institutions using the
Pediatric Care Coordination Curriculum as
a resource
(RI)++
+
+
Updated May 1, 2015
+
+
10

State Area where work is occurring
PediatricCare Coordination Curriculum
CareCoordination Measurement Tool
Alignment withtriple aim(experience, outcomes, cost)
Measures of Care Coordination
MeasuringFamily Experience
Alaska Statewide
California Regional
Hawai’i Regional
Massachusetts Delivery System
Michigan Statewide
Minnesota Statewide
Oregon Delivery System
Pennsylvania Statewide
Rhode Island Statewide
Texas Delivery System
Vermont Statewide
Wisconsin Statewide
Partial Overview of Efforts Across the US

Key RecommendationsAlignment
• Engage families in your planning from the beginning
• Leverage PCMH and specialty practice “certification”
• AMCHP-- Standards for CYSHCN
• Health Home funding (Chapter 2703)
• Meaningful Use
• Integrate with state agency initiatives and grant-funded programs (USMCHB D 70; CMMI, SIM, DSRIP,others)
• ACO Development– generally, bring CYSHCN care into broader model. Child health specific will take special effort
• Engage commercial payers in value-based design
– Employers are also key stakeholders
National Center for Care Coordination Technical Assistance
13
Contact Hannah Rosenberg, Manager, NCCCTA, for more information.
Email: [email protected]
Telephone: 617.919.3627
Mission: to support the promotion, implementation and evaluation
of care coordination activities and measures in child health across
the United States.
The National Center for Care Coordination Technical Assistance is working in partnership with the National Center
for Medical Home Implementation (NCMHI) in the American Academy of Pediatrics. The NCMHI is supported by
the Health Resources and Services Administration (HRSA) of the United States Department of Health and Human
Services (HHS) grant number U43MC09134.



• Care Coordination Measurement Tool: [http://www.childrenshospital.org/care-coordination-curriculum/care-coordination-measurement]
• US MCHB Pediatric Care Coordination
Curriculum [http://www.childrenshospital.org/care-coordination-curriculum]
• Care Map [http://www.childrenshospital.org/care-coordination-curriculum/care-mapping]
• Care Coordination Strengths and Needs
Assessment [http://www.masschildhealthquality.org/work/care-coordination/]
17

• Making Care Coordination a Critical Component of the Pediatric Health System: A Multidisciplinary Framework. Antonelli R, McAllister J, Popp J.. The Commonwealth Fund. May, 2009.
• MA Child Health Quality Coalition Care Coordination Framework. Funded by the Centers for Medicare and Medicaid Services (CMS) through grant funds issued pursuant to CHIPRA section 401(d). Contact: [email protected] www.masschildhealthquality.org/work/care-coordination/
• AAP Policy Statement: Patient- and Family-Centered Care Coordination: A Framework for Integrating Care For Children and Youth Across Multiple Systems. Pediatrics. May 2014.
• AHRQ Care Coordination Atlas (McDonald Nov 2010, June 2014) and companion document Care Coordination Accountability Measures for Primary Care (McDonald Jan 2012).
• Care Coordination Measurement Tool (CCMT). Care Coordination for Children and Youth with Special Health Care Needs: A Descriptive, Multisite Study of Activities, Personnel Costs, and Outcomes. Antonelli RC, Stille CJ, Antonelli DM. Pediatrics 2008; Providing a Medical Home : The Cost of Care Coordination Services in a Community-Based, General Pediatric Practice. Antonelli RC, Antonelli DM. Pediatrics 2004. www.childrenshospital.org/care-coordination-curriculum/care-coordination-measurement
• Care Transition Measure (CTM – Pediatrics). Hospital readmission and parent perceptions of their child’s hospital discharge. Berry, Ziniel, Antonelli, Coleman, et al. Internatl Jnl QHC. Aug 2013; Framework of Pediatric Hospital Discharge. Berry et al. JAMA Pediatrics. Aug 2014.
• Achieving a Shared Plan of Care with Children and Youth with Special Health Care Needs. Jeanne W. McAllister/Lucile Packard Foundation for Children’s Health. May 2014. lpfch-cshcn.org/publications/research-reports/achieving-a-shared-plan-of-care-with-children-and-youth-with-special-health-care-needs/
• Care Coordination Curriculum and Care Mapping Tool User Guides: Antonelli, Browning, Hackett-Hunter, McAllister, Risko; Lind. Boston Children’s Hospital; funded thru Family Voices/MCHB HRSA grant. 2012. www.childrenshospital.org/care-coordination-curriculum
References