Riccardo Offredi Thesis - Reduced Version
33
Università degli Studi di Trieste LAUREA SPECIALISTICA IN INGEGNERIA CLINICA MEDICAL EQUIPMENT PREVENTIVE MAINTENANCE: IS A NEW APPROACH POSSIBLE? ~ REDUCED VERSION: INTRODUCTION, CASE STUDY, PROPOSALS & CONCLUSIONS AUTHOR: RICCARDO OFFREDI SUPERVISORS: PROF. ENG. AGOSTINO ACCARDO; PROF. ENG. STEFANO BERGAMASCO. ACADEMIC YEAR: 2009/2010
-
Upload
riccardo-offredi -
Category
Business
-
view
1.434 -
download
2
description
Most interesting chapters of my Thesis about Preventive Maintenance protocols (English version).
Transcript of Riccardo Offredi Thesis - Reduced Version
Università degli Studi di Trieste
LAUREA SPECIALISTICA IN INGEGNERIA CLINICA
MEDICAL EQUIPMENT PREVENTIVE
MAINTENANCE:
IS A NEW APPROACH POSSIBLE?
~
REDUCED VERSION:
INTRODUCTION, CASE STUDY,
PROPOSALS & CONCLUSIONS
AUTHOR: RICCARDO OFFREDI
SUPERVISORS: PROF. ENG. AGOSTINO ACCARDO;
PROF. ENG. STEFANO BERGAMASCO.
ACADEMIC YEAR: 2009/2010
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
2
KEYWORDS
PREVENTIVE MAINTENANCE
PATIENT SAFETY
EVIDENCE-BASED MAINTENANCE
RELIABILITY-CENTERED MAINTENANCE
CHANGE MANAGEMENT
Author: Riccardo Offredi - [email protected]
3
TABLE OF CONTENTS
Table of contents .................................................................................................................................. 3
Introduction .......................................................................................................................................... 4
Chapter 6: Case study: Preventive Maintenance recommendations .................................................... 7
6.1. Introduction ............................................................................................................................... 7
6.2. Anaesthetic machines description ............................................................................................. 7
6.3. Protocol analysis ....................................................................................................................... 8
6.3.1. Equipment “A”: Spanish protocol ...................................................................................... 8
6.3.2. Equipment “A”: French protocol ....................................................................................... 8
6.3.3. Equipment “A”: Considerations ......................................................................................... 9
6.3.4. Workstation “B”: Spanish protocol.................................................................................... 9
6.3.5. Workstation “B”: French protocol ..................................................................................... 9
6.3.6. Workstation “B”: Considerations..................................................................................... 10
6.4. Different protocols .................................................................................................................. 10
6.5. Considerations ......................................................................................................................... 11
6.6. Conclusion and proposals ....................................................................................................... 12
Chapter 7: Proposals .......................................................................................................................... 14
7.1 Introduction .............................................................................................................................. 14
7.2 Operative proposals.................................................................................................................. 14
Preamble..................................................................................................................................... 14
Expedient ................................................................................................................................... 15
Self-criticism .............................................................................................................................. 17
7.3 Systematic proposals ................................................................................................................ 17
7.3.1. Technical Area ................................................................................................................. 17
7.3.2. Legislative Area ............................................................................................................... 19
A. Preventive Maintenance protocols selection ......................................................................... 19
B. Collaborative process for Preventive Maintenance protocols ............................................... 21
C. Maintenance Service Organization ....................................................................................... 25
D. Biomedical Equipment Technician ....................................................................................... 26
Conclusions ........................................................................................................................................ 28
Optimistic Scenario ........................................................................................................................ 28
Realistic Scenario ........................................................................................................................... 30
Final considerations ....................................................................................................................... 31
Future developments ...................................................................................................................... 31
Appendix A – Notified Bodies........................................................................................................... 32
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
4
INTRODUCTION
Considering the current European-wide financial situation, hospitals localized in Member states of
the European Union, and so clinical engineering department, are going to receive less and less
resources (human, technological, and financial) to cope with increasing healthcare request.
Clinical engineer who is responsible for the department, will be asked to contribute to resources
optimization, with the principal target to enhance (or at least maintain) care quality level delivered
to patients.
One of the historical clinical engineer skills is organizing maintenance and its consequent activities.
An Italian law impose on the clinical engineer to follow Preventive Maintenance protocols
recommended by original equipment manufacturers (in the case those protocols exist) which are
broadly characterized by fixed interval intervention.
The resulting activities require a lot of man power and their efficiency is not demonstrated for an
increasing share of medical equipment used in hospitals; in the last 40 years the clinical engineer
community have been watching a double shift: medical equipment moved from machines typified
by mechanical friction that brings wearing (in which fixed intervals of maintenance are
appropriate), to machines characterized by electronic components (in which few parts have to be
replaced), to medical systems and devices that are interconnected among them for diagnosis and
therapy goal (wide use of Information Technology).
The evolution outlined above entails a reduction of usual issues (Preventive Maintenance at fixed
intervals), and first appearance of new issues (relating Information Technology), to which clinical
engineers will have to give a quick answer to reduce patients’ uncomfortableness toward the
minimum level.
In my thesis I am going to consider Preventive Maintenance as “True Preventive Maintenance” that
is restoration or replacement of medical device non-durable parts.
According to Malcolm Ridgway, some devices that appear to be very similar in function and design
have manufacturer-recommended intervals that vary by a factor of two or more. So some
perplexities rose about the fact that those intervals are based on meaningful test data. If so, would
manufacturers share those informations? If there are no test data, nor willingness to share, nor other
rationale is provided, than it is easy to understand the concern about the validity of those
recommended values.
Many clinical engineers are thinking that is given too much emphasis on fixed intervals
maintenance tasks even if those tasks don’t cause, for much medical equipment, an improvement
for reliability and safety.
The goal of my thesis is to understand if it is possible to find and to implement Preventive
Maintenance protocols which are different from OEMs’ Preventive Maintenance protocols to
improve patient quality of care, considering hospital peculiar necessities where medical equipment
is used.
The reasons that pushed me to investigate on that topic can be summarized in the curiosity evoked
by the following questions:
Why Preventive Maintenance is done in a certain way?
What is the benefit coming from a certain maintenance task for healthcare sector?
In the continuation of my thesis I am trying to answer to the following questions:
What are the different maintenance techniques that are alternative to the prevailing ones?
In which condition new techniques find the best application?
What are the involved consequences?
Considering that each healthcare organization has unique features coming from users,
patients, environmental stresses, may a hospital have the necessity for a specific protocol for
the same make-model of medical equipment?
May a clinical engineer (having a deep knowledge of a certain hospital) modify OEMs’
protocols with better results on patient safety?
Author: Riccardo Offredi - [email protected]
5
What kind of information should be based on the adoption of a certain maintenance
strategy?
What is the best source for that information?
What process is necessary to adopt in order to derive from the available information the
choice about the best strategy to implement?
Is it possible to learn from other sectors that are involved in maintenance tasks to improve
patient safety through the application of a certain maintenance strategy that is different from
the prevailing one?
How can a clinical engineer optimize resources, that is where we have to cut resources and
where it is better to invest more resources?
What kind of effort will be asked to clinical engineer due to the increasing use of more and
more electronic and intercommunicating devices?
The instruments used to reach the answers corresponding the questions written above are listed as
follows:
Exchanging e-mails with some clinical engineers that are conducting experiments abroad
Italy (U.S.A and South Australia); those experiments cause the application of maintenance
strategies which are different from OEMs’ maintenance strategies;
Interviews through e-mail made to an expert clinical engineering working for a third party
organization (whose goal is to find new process to improve patient care);
Interviews made to a operant Biomedical Equipment Technician;
Comprehension of clinical engineering conference presentations discussed by innovative
leaders about maintenance strategies;
Study of the process through which is determined Preventive Maintenance protocols in
European / American civil aeronautics;
Analysis of European Law about medical devices and aircraft safety;
Analysis of Italian Laws about medical technology and public contracts for services and
supplies;
Analysis of near event distribution communicated by Public Health Service (UK and
Australia);
Reading a handbook about new approaches to maintenance management (Reliability-
centered Maintenance).
The topic treated by this thesis is particularly up-to-date, because in literature traditional
Preventive Maintenance has been criticized by illustrious members of clinical engineer sector since
2009:
Malcolm Ridgway deals with this topic in “Optimizing Our PM Programs” , Biomedical
Instrumentation & Technology, May/ June 2009; “Reducing Equipment Downtime: A New
Line of Attack”, Journal of clinical engineering, October/December 2009; “Manufacturer-
Recommended PM Intervals: Is It Time for a Change?”, Biomedical Instrumentation &
Technology, November/December 2009;
Binseng Wang deals with this topic in “Evidence-Based Maintenance - Part I: Measuring
Maintenance Effectiveness With Failure Codes”, Journal of clinical engineering,
July/September 2010; “Evidence-based Maintenance – Part II: Comparing maintenance
Strategies Using Failure Codes”, Journal of clinical engineering, October / December 2010.
My thesis is structured in 7 chapters.
In the first one I am highlighting exogenous factors that are affecting the healthcare sector evolution
in Europe and particularly in Italy, considering economics, demography and society. This chapter
makes clear the necessity for optimizing available resources for healthcare sector of every Country
in European Community. In the remaining part of the thesis I am trying to understand how a clinical
engineer can contribute to optimize resources.
In the second chapter I am showing basic definitions such as clinical engineering, clinical engineer,
biomedical equipment technician; I am clarifying the difference between health technology, medical
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
6
device and electromedical equipment; I am describing Health Technology Assessment concept; I
am treating healthcare aspects of Information Technology and its very probable future impact on
organization and task relative to Clinical Engineer Department; I am examining the reliability
notion, the original equipment manufacturer definition, and the concept of Preventive Maintenance.
The third chapter is titled “re-think Preventive Maintenance”: firstly I am examining the legislation
in force in Italy and in Europe, and the rules emanated by the most important hospital accrediting
organization in the world, set outside European Directives; then I am analysing the incentives that
encourage us to think critically the current way of organizing and managing Preventive
Maintenance; lastly I am registering the obstacles that prevent the adoption of different protocols
from the ones indicated by manufacturers.
In the fourth chapter I am describing current and future techniques relating Preventive Maintenance;
I am dealing with Reliability-centered Maintenance, because it is the process that allowed deriving
an evolution compared to traditional maintenance strategies in many industrial sectors, and I am
treating its application in biomedical technology field: Evidence-based Maintenance. At last I am
analysing how experiments conducted by innovative technology managers made concrete the
principals of Reliability-centered Maintenance in healthcare and what are their outcomes.
In the fifth chapter, considering how safety has been growing in civil aviation sector, I am
investigating the process through which Preventive Maintenance protocols are established in that
sector: I discovered that it is based on Reliability-centered Maintenance principles and it is shared
by stakeholders. Then I am analysing automotive sector, realizing that following some principles of
that market, it would be possible to reduce Preventive Maintenance cost for healthcare
organizations, increasing competition among maintenance service provider.
The sixth chapter is made by a case-study: in two different cases, for a specific make-model of
electro-medical equipment, which is sold in two different Countries of European Community, the
same manufacturer recommends different Preventive Maintenance protocols. It is impossible that
both protocols are the best for maximizing patient safety goal and for minimizing resources request
goal. So I am suggesting to uniform Preventive Maintenance protocols at European-level for the
same make-model.
The most original side of my thesis is pinpointed in the seventh chapter, relating to proposals: at the
beginning I am showing a way to get a more appropriate protocol for a specific hospital needing; it
is obtained during a single piece of electromedical equipment negotiation, without modifying any
existing Italian Law and straight spendable by Italian Clinical Engineering Services.
Secondly I am putting forward the adoption of the same failure classification, which happen on
medical device; the adoption is made hopefully by as much as possible healthcare organizations.
Then I am promoting the choice -made by clinical engineers- to select the more opportune
Preventive Maintenance protocols, asking for the modification of Law Decree n. 81 in 2008.
Subsequently I am proposing a process to realize an initial Preventive Maintenance protocols for
medical devices valuable inside European Community, subject to amendment of European
Directive on Medical Device.
Next I am suggesting the certification for medical equipment Preventive Maintenance service
companies working inside the European Community; the certification is subject to the promulgation
of a specific European Directive.
At last I am proposing the constitution of a specific European Directive that imposes a maintenance
licence to the people who wants to do Preventive Maintenance tasks on medical equipment inside
the European Community.
In the present work I am just dealing with the following chapters: introduction, chapter 7
(proposals) and conclusions.

Author: Riccardo Offredi - [email protected]
7
CHAPTER 6: CASE STUDY: PREVENTIVE MAINTENANCE
RECOMMENDATIONS
6.1. INTRODUCTION
In brief I was able to examine two pairs of Preventive Maintenance protocols which concern two
models of the same class of medical device; such class of medical device is used by every advanced
healthcare organization to implement a vital healthcare process, which is anaesthetic therapy.
The first pair of protocols are different between them and they regard the same make-model of
medical device (I will call that model “A” for legal issues) which is currently used in some French
and Spanish hospitals.
The second pair of protocols are different between them and they concern another make-model of
medical device (I will call that model “B”): even that one is marketed and it is working in some
French and Spanish hospitals.
Inside each pair of above-mentioned protocols, it is interesting to investigate differences in
Preventive Maintenance recommendations set by the same manufacturer for the same make-model
of medical device, which is commercialized in two different Countries of the European Union.
6.2. ANAESTHETIC MACHINES DESCRIPTION
Both “A” and “B” are two anaesthetic machine models, coming from the same Manufacturer and so
they belong to the same make, but they have different features: in a nutshell the first model (“A”) is
more essential in its functionality, while the second (“B”) has all the features that someone may
require to an advanced anaesthetic workstation.
Anaesthetic machines may be set up whether as modular systems or as integrated machines.
In the case of modular approach –device “A”-, anaesthetic system platform is constituted by trolley,
with mixers and rotameters, by ventilator, and by monitor for airway pressure, for expired gas
volumes and for inspired oxygen concentration. The benefits coming from modular configuration
include flexibility in choosing during integration or possible system improvement. Among the
drawbacks there are problems coming from interfacing different modules or the presence of
multiple alarms and displays.
The medical device “B” is an integrated anaesthetic workstation in which it is evident the benefit to
have an integrated system of parameters visualization and a system which control alarm priority.
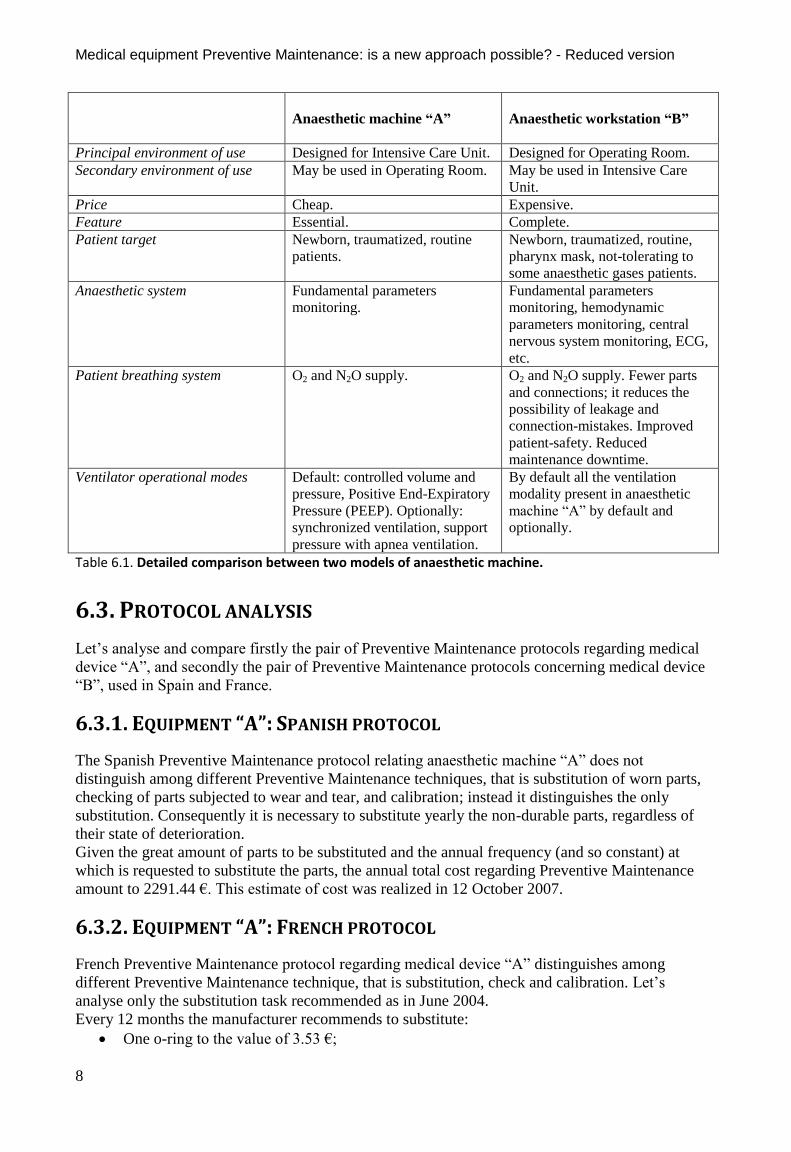
Table 6.1 shows differences between “A” and “B” medical deices in their features, in target patients
and in environment of use.
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
8
Anaesthetic machine “A”
Anaesthetic workstation “B”
Principal environment of use Designed for Intensive Care Unit. Designed for Operating Room.
Secondary environment of use May be used in Operating Room. May be used in Intensive Care
Unit.
Price Cheap. Expensive.
Feature Essential. Complete.
Patient target Newborn, traumatized, routine
patients.
Newborn, traumatized, routine,
pharynx mask, not-tolerating to
some anaesthetic gases patients.
Anaesthetic system Fundamental parameters
monitoring.
Fundamental parameters
monitoring, hemodynamic
parameters monitoring, central
nervous system monitoring, ECG,
etc.
Patient breathing system O2 and N2O supply. O2 and N2O supply. Fewer parts
and connections; it reduces the
possibility of leakage and
connection-mistakes. Improved
patient-safety. Reduced
maintenance downtime.
Ventilator operational modes Default: controlled volume and
pressure, Positive End-Expiratory
Pressure (PEEP). Optionally:
synchronized ventilation, support
pressure with apnea ventilation.
By default all the ventilation
modality present in anaesthetic
machine “A” by default and
optionally.
Table 6.1. Detailed comparison between two models of anaesthetic machine.
6.3. PROTOCOL ANALYSIS
Let’s analyse and compare firstly the pair of Preventive Maintenance protocols regarding medical
device “A”, and secondly the pair of Preventive Maintenance protocols concerning medical device
“B”, used in Spain and France.
6.3.1. EQUIPMENT “A”: SPANISH PROTOCOL
The Spanish Preventive Maintenance protocol relating anaesthetic machine “A” does not
distinguish among different Preventive Maintenance techniques, that is substitution of worn parts,
checking of parts subjected to wear and tear, and calibration; instead it distinguishes the only
substitution. Consequently it is necessary to substitute yearly the non-durable parts, regardless of
their state of deterioration.
Given the great amount of parts to be substituted and the annual frequency (and so constant) at
which is requested to substitute the parts, the annual total cost regarding Preventive Maintenance
amount to 2291.44 €. This estimate of cost was realized in 12 October 2007.
6.3.2. EQUIPMENT “A”: FRENCH PROTOCOL
French Preventive Maintenance protocol regarding medical device “A” distinguishes among
different Preventive Maintenance technique, that is substitution, check and calibration. Let’s
analyse only the substitution task recommended as in June 2004.
Every 12 months the manufacturer recommends to substitute:
One o-ring to the value of 3.53 €;
Author: Riccardo Offredi - [email protected]
9
One oxygen-cell to the value of 229.86 €;
Every 24 months the manufacturer recommends to substitute:
One lead-acid battery, with a voltage of 12 V to the value of 81.55 €;
One flapper-valve to the value of 7.70 €;
One free-will respiration o-ring to the value of 1.00 €;
Every 2 years the total cost of substitution is equal to (3,53 * 2 + 229,86 * 2 + 81,55 +7,70 + 1,00) €
= 557,03 €.
In conclusion the yearly total cost of substitution is equal to 278,52 € (rounded off to the second
decimal point).
6.3.3. EQUIPMENT “A”: CONSIDERATIONS
The parts which have to be substituted and which are present in the Spanish protocol for anaesthetic
machine “A” are all comprised in the French protocol.
Comparing the two protocols regarding anaesthetic machine “A”, the Spanish protocol causes an
expense about 8 times greater than the French analogous protocol, regarding to the only
substitution.
Note that if the checks scheduled in the French protocol for medical device “A” entailed the
necessity to substitute any non-durable parts, yearly cost of substitution would increase compared to
the only substitution expense.
6.3.4. WORKSTATION “B”: SPANISH PROTOCOL
The Spanish Preventive Maintenance protocol relating anaesthetic workstation “B” does not
distinguish among different Preventive Maintenance techniques, that is substitution of worn parts,
checking of parts subjected to wear and tear, and calibration; instead it distinguishes the only
substitution. Every year it is necessary to substitute the parts which are subject to wear. Such parts
comprise all the parts which are present in the French protocol of the same medical device and other
parts which the French protocol does not consider for substituting.
Given the great amount of parts to substitute, and the fixed frequency (annual) at which it is
recommended to substitute the parts, the total cost of Preventive Maintenance amount to 1390.69 €.
This estimate of cost was realized in 12 October 2007.
6.3.5. WORKSTATION “B”: FRENCH PROTOCOL
The French Preventive Maintenance protocol distinguishes among different Preventive
Maintenance technique, that is substitution, check and calibration. Let’s analyse only the
substitution task recommended as in June 2004.
The protocol regarding substitution requires the execution of different tasks depending on
considered range. The intervals are fixed at 12 months, 2 years or 4 years.
Every 12 months it is requested to substitute 4 o-rings any of which was worth 3.53 € depending the
price list. The number of the pieces is compatible with the 4 o-rings scheduled in the Spanish
protocol.
Every 2 years it is requested to substitute:
Everything that is substituted every 12 months;
One flapper-valve (in the Spanish protocol one flapper-valve is requested to be substituted
every 12 months);
One free-will respiration o-ring (in the Spanish protocol one free-will respiration o-ring is
requested to be substituted every 12 months);
Every 4 years it is requested to substitute:
Everything that is substituted every 2 years;
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
10
2 batteries (in the Spanish protocol 2 batteries are required to be substituted every 12
months);
The total cost regarding the part to be substituted every 4 years becomes:
3.53 € / 1 o-ring * 4 o-rings /years * 4 years +
(7.70 € / 1 valve + 1 € / 1 o-ring) * 2 years +
(81.55 € / battery * 2 batteries) = (56.48 * 17.4 + 163.1) €= 236.98 €
That is equal to 59.25 € / year.
6.3.6. WORKSTATION “B”: CONSIDERATIONS
The parts to be substituted, which are present in the Spanish protocol for anaesthetic workstation
“B”, coincide with all the part which are present in the French protocol and with other parts that the
French Protocol does not consider for substitution.
Comparing the two protocols about workstation “B”, the Spanish protocol causes an expense about
23 times greater than the analogous French protocol regarding to the only substitution.
If the scheduled checks in the French protocol for workstation “B” entailed the necessity to
substitute non-durable parts, the value of yearly substitution would increase compared to the
expense relating to the only substitution.
6.4. DIFFERENT PROTOCOLS
In brief in at least one Spanish hospitals is made a sort of “heavy maintenance” where the
maintenance organization requires to substitute many parts at fixed intervals; differently in at least
one French hospital is made a sort of “light maintenance”, where maintenance requirements ask to
clinical engineering service to
Substitute a lower amount of components compared to the Spanish case and
Verify the wearing condition of other non-durable parts and
Calibrate some components.
Note that the manufacturer issues those protocols regardless to local hospital features.
Preventive Maintenance is influenced in each hospital at least by the following local factors:
Environment of use: that is in which department the medical device is used;
Which category of caregiver uses it: physician, nurse;
Which kind of maintenance experience the clinical engineering service has in a specific
hospital: new service where few and neophyte technical staff is working, versus skilled
service where much technical staff is working.
Frequency of use of medical device: it is probable that in an Operating Room, the stress to
which medical equipment is undergone is greater compared to other departments.
In my opinion, such consideration is important because the Preventive Maintenance request made
by a specific medical equipment manufacturer have to be designed for a standard healthcare
organization; so the recommendations should be the result of considerations which are on average
valid for every hospital.
Making the hypothesis that the feature of Spanish and French hospitals are on the average very
similar in the above-mentioned points (as it is reasonable to think), the Preventive Maintenance
protocols for the same make-model of medical device should bring to the same result, that is
identical Preventive Maintenance recommendations for both Countries.
Reasoning for absurd, it would be logic to expect that medical equipment manufacturer
recommends Preventive Maintenance protocols that would schedule the only headings of
substitution of the components which are subject to wear at fixed interval to every hospital of a
certain Country if the large majority of clinical engineering service of the same Country are
showing similar serious technical gap, such as incapacity to verify the wearing condition.
Author: Riccardo Offredi - [email protected]
11
Ability to do maintenance comes from mainly the schooling level in technical field and it is likely
to expect that, where there is a good ability in teaching to physicians, there is at least a basilar
ability in teaching to BMET’s. I think it is reasonable to expect serious gap in teaching maintenance techniques in a Country which is
not evolved with regard to the effectiveness by which healthcare services are supplied.
Using the sentence “effectiveness by which healthcare services are supplied” I mean mainly the capacity
of a government to improve the health of their citizen and it is -according to the World Health
Organization- the only feasible way to compare different healthcare systems belonging to different
Countries.
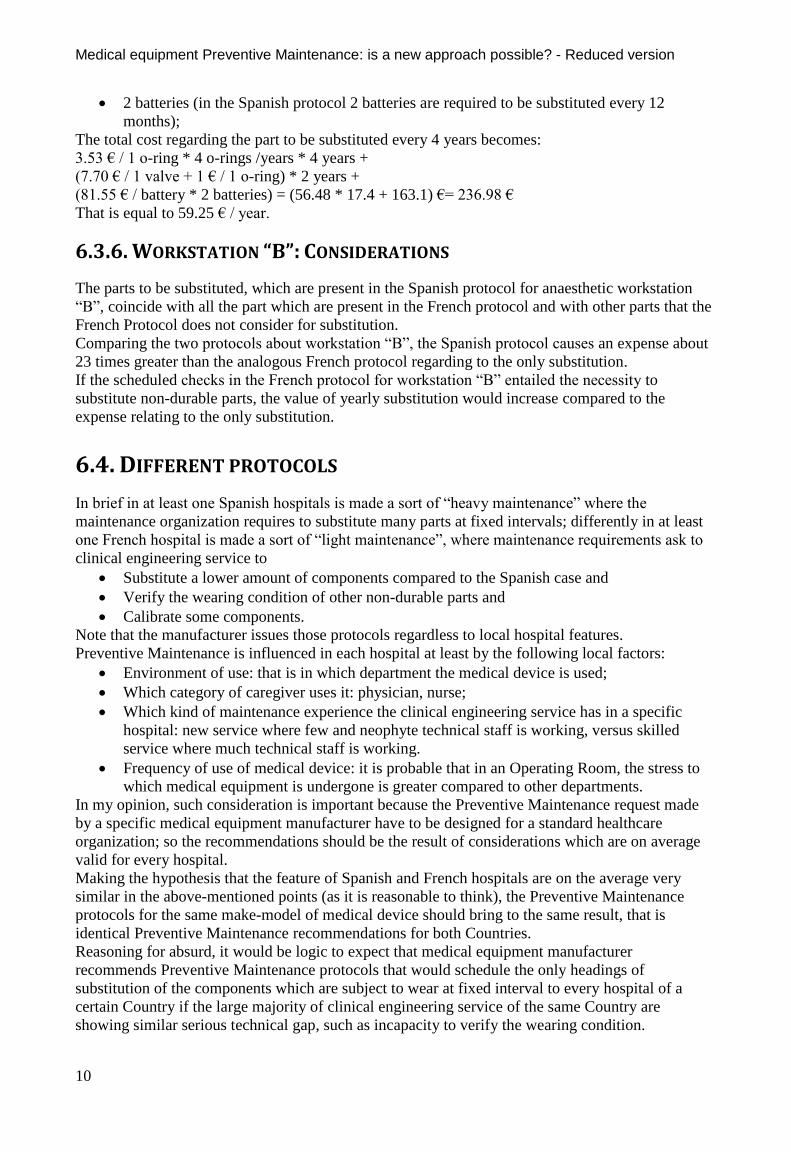
A study made by World Health Organization1 places Spain and France inside the top-ten of the
Healthcare Service with the best effectiveness in the World, as table 6.2 shows.
Table 6.2. Effectiveness ranking of the top-ten Healthcare Service in the World.
By my argument I conclude that there are similar skills in France and in Spain regarding medical
equipment Preventive Maintenance; in my opinion Spanish BMET’s are able to do inspections and
calibration as well as French BMET’s.
Spanish protocols are characterized by low efficiency of Preventive Maintenance because, after an
inspection task, BMET’s could notice that some tasks are useless, because some parts did not reach
their respective “useful life” limit.
That is the reason why I consider spurious from a manufacturer to recommend Preventive
Maintenance protocols which are based on different parameters for the same make-model, that is
fixed interval for Spanish protocol and a combination of fixed interval and metered maintenance for
the French protocol.
The true reason of a fixed interval request could lie in the will to increase the invoice coming from a
low efficiency Preventive Maintenance tasks.
6.5. CONSIDERATIONS
Considering so both French and Spanish protocols, and ignoring which one of the two is the best,
necessarily we could be alternately in one of the two situations examined afterwards. Each instance
causes some anomalies which in brief causes a physical risk for the patient and/or a bad allocation
of economic resources.
Let’s examine the two possible situations:
A) Preventive Maintenance protocol which entails to substitute a few parts (“light
maintenance”, as in the case of above-mentioned French protocol) is the best one, that is it
requires to do all Preventive Maintenance tasks that entail demonstrable benefit to reduce
failure onset. Consequently Preventive Maintenance protocol which schedules the
substitution of many components (“Heavy maintenance”) is characterized by excessive, so it
1 Tandon A., Murray C. JL, Lauer J. A., Evans D. B., “Measuring overall health system performance for 191
countries”, - GPE Discussion Paper Series: No. 30 - EIP/GPE/EQC - World Health Organization. Disponibile on-line
www.who.int/healthinfo/paper30.pdf
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
12
entails an inefficient Preventive Maintenance (in the sense that it requires to do tasks which
don’t entail any demonstrable benefit) and even very expensive for the healthcare
organization that is forced for (supposed) safety-related reasons to follow the
recommendations issued by manufacturer. Such a practice entails de facto to subtract some
resources which could have been invested in more added-value activities for patient. After,
we should not undervalue the possibility that “Service-induced Failure” (cf. 3.3.6) could
occur which increases the failure probability of medical device to the detriment of patient
safety.
B) Preventive Maintenance protocol that entails to substitute many components (“heavy
maintenance”, as in the case of Spanish protocols) is the best one, that is it requires to
follow all the Preventive Maintenance tasks which entail demonstrable benefits to reduce the
failure onset. Consequently Preventive Maintenance protocol that schedules to substitute
few parts (“light maintenance”) is characterized by insufficient maintenance
recommendations, so it involves the execution of an incomplete set of Preventive
Maintenance tasks, in the sense that some tasks which would reduce the probability of a
failure are not performed. Such a failure could happen during the patient treatment2. Given
that we are talking about anaesthetic machine, so it is possible that adverse event happen
during the surgical intervention. This situation is absolutely not acceptable for patient safety.
Table 6.3. shows how French and Spanish protocols cannot be contemporaneously the best for
patient-safety and Preventive Maintenance efficiency.
Instance A Instance B
France Best Not best
Spain Not best Best
Table 6.3: French and Spanish protocols cannot be contemporaneously the best.
6.6. CONCLUSION AND PROPOSALS
As summarized in table 6.3. and thinking logically, I can draw the following conclusions:
French and Spanish protocols related to the same make-model of medical device are never
contemporaneously the best;
Within a European-wide vision, none of the condition present in the examined protocols is:
o Tolerable for patient-safety;
o Reasonable, considering the approach to maintenance.
The solution in view of the described situation, in my opinion, is just one and more distinctly: every
medical equipment manufacturer which operates in European Community market, should issue
Preventive Maintenance protocols which are the exact copy for the same model of medical device,
before that the same piece of medical device is put into commerce.
Such Preventive Maintenance protocol should be just the “initial” one and after it should be subject
to improving modifications. In fact with passing of time, a particular medical device would be used
by healthcare professionals, allowing to BMET’s and clinical engineers to gather specific
knowledge about Preventive Maintenance: some parts are subject to a certain degree of wear, other
parts are subject to a different degree of wear and so they have different expected useful life span.
This specific knowledge would allow clinical engineers to modify Preventive Maintenance
protocols; such modifications would make maintenance contemporaneously safer for the patient and
more efficient for resources allocation.
2 The probability of such failure on the patient depends on the share of time in which the machine is working on the
patient compared to the range in which the machine is switched on.

Author: Riccardo Offredi - [email protected]
13
In order to know how it is possible to implement a couple of conditions by which any medical
equipment manufacturer writes a initial reasonably safe and efficient Preventive Maintenance
protocol for any piece of medical equipment, I refer you the next chapter (cf. 7.2 and 7.3.2.).
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
14
CHAPTER 7: PROPOSALS
7.1 INTRODUCTION
A doubtless original feature inside my thesis lies in the elaboration of different proposals that are
helpful for clinical engineering field.
Particularly it is possible to subdivide my suggestions contained after in two sections:
The first one encompasses pragmatic ideas, which are immediately spendable by clinical
engineering services operating today in Italy to improve Preventive Maintenance protocols
used by healthcare organizations (cf. 7.2. “Operative Proposals”);
The second one is more subject to external and systemic conditions, and so the ideas lying
there could be implemented only in favourable circumstances. However their application
would cause structural and lasting improvements in the quality of Preventive Maintenance
supply (cf. 7.3 “System Proposal”).
As we will see, operative and systematic proposal are interrelated.
7.2 OPERATIVE PROPOSALS
There are many operative proposals, but these are all based on the sole following idea: a certain
clinical engineering service is able to obtain, by negotiation, a specific Preventive Maintenance
protocol for a specific make-model of piece of medical equipment that is going to be used in its own
healthcare organization; such protocol fits better than the previous one to the necessities expressed
by the same organization.
PREAMBLE
Not each and every piece of medical equipment put on the European (and Italian) market is
furnished with the relating initial Preventive Maintenance protocol. This fact derives directly by the
application of European Directive on Medical Devices 93/42 and following.
“Where appropriate, the instructions for use must contain the following particulars: […]
d) all the information needed to verify whether the device is properly installed and can operate
correctly and safely, plus details of the nature and frequency of the maintenance and calibration
needed to ensure that the devices operate properly and safely at all times;”
The lack of a initial Preventive Maintenance protocol causes some problems to clinical engineering
services that must strive to understand what is the best protocol: in Italy the Decree-law called
“Testo unico in materia di salute e sicurezza nei luoghi di lavoro” (D. Lgs. 81/2008 and following)
indicates to seek among best practice techniques or coming from fine procedure codes.
In the case the medical equipment manufacturer communicates Preventive Maintenance protocol,
we still don’t know if that is the same for all healthcare organizations spread throughout a certain
Country.
The case study presented in the sixth chapter highlights that a specific manufacturer communicated
two different protocols for the same make-model of medical device to two different healthcare
organizations located in different Countries of the European Community: for this reason wondering
if the practice to supply different Preventive Maintenance protocols may be implemented even
inside the same Country, could appear legitimate.
Let’s consider the hypothesis that the practice described above is conducted inside the Italian
territory: this preamble is necessary to maintain valid both European Directive on Medical Device
and Italian Decree-law “D. Lgs. /2008 - Testo unico in materia di salute e sicurezza nei luoghi di
Author: Riccardo Offredi - [email protected]
15
lavoro”. In compliance with the latter law the healthcare organizations are imposed to use
manufacturer Preventive Maintenance protocol, if it exists.
In my opinion this Decree-law constitutes an important constrain for medical device maintenance
managers, because it cancels the possibility to adapt the protocol to peculiar necessities of
healthcare organization in which medical equipment is used.
For a specific make-model of piece of medical equipment which contains non-durable parts,
different external conditions exist, typical of a specific healthcare organization, that influence the
best maintenance protocol; the conditions are the following:
Intensity of use;
Exposure to different environmental stresses like:
o Electricity supply out-of-service;
o Medical gas supply out-of-specification;
o Environmental temperature out-of-specification;
o Contaminant fluid (for example rainwater or trickling drink);
o Electromagnetic interference;
Users:
o Training;
o Experience;
Patients:
o Demography;
o Epidemiology.
A clinical engineer who have experience and who have been working since many years in the same
healthcare organization should deeply know the influence of the elements described above, each
one of them affects on Preventive Maintenance requirements of single piece of medical equipment.
Consequently qualified clinical engineers could know suboptimal Preventive Maintenance protocol
for a specific make-model of a piece of medical equipment in his/her own hospital whether in the
case that model is working, or in the case in which a certain technology – that meets similar
requirement compared to the previous one - has been already programmed for being acquired by the
healthcare organization.
EXPEDIENT
The core of the operative proposal: during the negotiation done to acquire a piece of medical
equipment, and if needed the relating Preventive Maintenance service, the expert clinical engineer
bargains Preventive Maintenance protocol features with medical device manufacturer/distributor.
It is necessary to make a distinction between public healthcare company and private healthcare
company.
A) In the case a clinical engineer deals with acquisition for a private healthcare organization, he
has the opportunity to call any manufacturer/distributor company, to fix an appointment
with a technician of the same company and to know if the company would be willing to
communicate/modify Preventive Maintenance protocol to fit with clinical engineer
necessities; in short private company can free itself form the competitive tender rules.
B) In the case a clinical engineer deals with acquisition for a public healthcare organization,
that professional would be a civil servant, and so that person should not favour in any way
any competitor during the tender. The request for Preventive Maintenance protocol
modification would be done during the negotiation for the medical device acquisition: the
negotiation is ruled by “D. Lgs. 163 del 2006”, known as “il Codice dei contratti pubblici
relativi a lavori, servizi e forniture” in force in Italy. For this reason the request for
collaboration for building the maintenance protocol must fit in one of the mechanism
expressed by “D. Lgs. 163 del 2006”: the request for a maintenance protocol must never
favour any competitor company compared to any other company. The contracting
companies (healthcare organizations) can award a public contract through procedures called
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
16
“procedura aperta”, “procedura ristretta”, “procedura negoziata” or “dialogo competitivo”.
The contracting companies use preferably “procedura ristretta” when the awarding criterion
is that of the more economically profitable offer. The “procedure ristrette” are procedures in
which any economic operator may ask to be involved in, and in which only economic
operator that have been invited by contracting companies may make an offer in the way
expressed by “Codice degli appalti”. I am trying to describe how my operative proposal
may fit into the public contract negotiation for the acquisition of a medical technology: how
must the current procedure be modified into the bureaucracy of “procedura ristretta” to
realize my operative proposal?
I am describing the “procedura ristretta” that has a request for collaboration among
producer/distributor technicians and healthcare organization technicians, in order to find an initial
Preventive Maintenance protocol of a specific piece of medical equipment.
The necessities for public body during the acquisition process are the following:
To verify the market condition in order to pick the more economically profitable one;
To negotiate with many economic operators;
To make sure each competitor has the same opportunities;
The “appalti pubblici” are onerous contracts, stipulated in writing between a contracting company
and one or more economic operator, that deal with work-execution, products supply, and service
giving.
The civil servant, as the clinical engineer who is responsible for conducting competitive tenders,
must demonstrate a posteriori that:
Acted in the authorization limits;
Was impartial.
In order to achieve this aim, the civil servant must stringently follow “D. Lgs. 163 del 2006, Codice
unico degli Appalti”. The “D. Lgs 163 del 2006” considers the award of the competition called
“ristretta”: in that procedure the minimum requisitions are communicated to the economical
operators to participate to the contest in the notice. The companies that think to have the minimum
requisitions send a request for participating to public administration. The awarding organization
verifies which are the companies that satisfy the Law. The awarding company sends an invitation
letter to all deserving companies: in this document any hospital must specify which are the
preferential requisitions, among which I am proposing the collaboration in order to find a
Preventive Maintenance protocol.
The competitor companies that received the “lettera invito” can send their offer. Any offer that gets
to the hospital should be structured in three envelopes: one which keeps various documentation; one
which contains what the company is offering; and one which embodies the economical offer
subscribed by competitor company holder. Inside the envelope which contains what the company is
offering should be the “technical project”, that is a standard description of some elements in a
certain order so that it is possible to compare the offers among them. In the case of a technical
project for a service (such that of supplying Preventive Maintenance tasks) the suggested elements
to insert are the following:
The structure and organization of the service, the base and the representatives;
The number and the qualification of staff that will be available for the service referred above
with details relating to professional profile of everyone and details relating the integration in
organization with reference to tasks assigned to everyone;
The list of analysis and measurement instruments that will be used during the intervention
and of medical device and classes of materials;
If-needed technical-operative ways through which to collaborate to establish initial
Preventive Maintenance protocols and the staff qualification that will be made available for
contribution;
Informative flow which guarantees successful outcome and quality of tasks both for
preventive and corrective maintenance, and for management, and for modification/extension
of the system and to guarantee continuous improvement;

Author: Riccardo Offredi - [email protected]
17
Management modalities of different sort of failure and of repair service as a general rule;
If-needed procedures that will be imposed to if-needed subcontractors;
After receiving all the offers, those are valued by the professional staff in charge of management of
contract depending on a certain criterion, in order to award.
Such criterion should include a bonus for all those competitors that formulate the willingness to
collaborate in realizing Preventive Maintenance protocols. In fact the following high-quality
protocol trades-off a reasonably high level of patient safety, coming from a high level of reliability
of the machine, and a low maintenance tasks cost.
This union represent a quality factor for the machine. So such element should be rewarded -in a
different way depending on algorithm used- in the method which enables to find the more
economical profitable offer in a competitive tender. After the awarding, the contracting agreement
is stipulated.
Let’s consider the case in which the hospital chooses a manufacturer in order to get the piece of
medical equipment and concerning Preventive Maintenance task; the manufacturer communicated
its agreement in the collaboration: in that case in the specification will be present the detailed
description of the agreement of the collaboration.
In brief, Preventive Maintenance tasks are negotiated with manufacturer/distributor of the piece of
medical equipment. Next Preventive Maintenance team assess if it is better 6 months fixed interval
technique, 12 months fixed interval technique, if it is more clever do metered maintenance, or
predictive maintenance, or else the team could decide not to do any kind of Preventive Maintenance
(run-to-failure) on medical device that have no non-durable parts.
SELF-CRITICISM
At the end of the description of proposed expedients used to establish Preventive Maintenance
protocols more suitable for the healthcare organization, I think it is worth to make a self-criticism.
Only clinical engineering services operating in a hospital which are experienced (people that were
employed long time ago) would be able:
1) To communicate the features of the hospital that influence preventive protocol;
2) To understand if the proposal about Preventive Maintenance of the winner competitor were
right;
3) If-needed to thwart effectively excessive requests of fixed interval Preventive Maintenance
tasks.
Consequently not much expert clinical engineering services could hardly negotiate efficiently
Preventive Maintenance initial protocol. To find a systematic and definitive solution to this
problem, where the solution is not depending on the skills of a single clinical engineering service, I
invite you to read paragraph 7.3.2.
7.3 SYSTEMATIC PROPOSALS
The applicability of “systematic proposals” is conditioned to decisions accepted by different
legislative bodies.
In order to explain, I decided to subdivide this section in two portions, in which the first one is
about technical area (cf. 7.3.1.), while the second one has a legislative core (cf. 7.3.2).
7.3.1. TECHNICAL AREA
In the technical area I am dealing with a proposal that consists in the adoption of the same
classification of failures that happen on medical devices for as many hospitals as possible.
Historically and presently Italy lacks a defined codification for causes of medical equipment failure
which is shared among different hospitals that use different clinical engineering services.
Examples of cause coding have been presented by B. Wang and M. Ridgway.
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
18
A classification of failure cause could be implemented in Italy and shared among many hospitals,
but just for those healthcare organizations which are using the same independent service
organization (ISO) that requires to its technicians to distinguish and to record the cause according to
the same codification.
In all those situations the common element is given by the fact that a company which sells
maintenance services decided in a strategic, autonomous and voluntary way to classify the
happening failures; the necessary condition is that the ISO has a computerized maintenance
management system (CMMS). In the case of ARAMARK Healthcare® the unique CMMS allowed
to B. Wang to do “lateral comparison”, that is to compare failure data from healthcare organizations
that used different maintenance techniques.
So in Italy, in general terms, it is impossible to collect data coming from different hospitals in just
one database. So we cannot analyse failure data and make comparison on different elements among
hospitals.
My proposal is the following: as many Italian healthcare organizations as possible adopt the same
failure code classification, and make their biomedical equipment technicians record failure data in a
standard way on a database.
That discrimination would go down to a make-model level, or alternately, to a certain type of
medical equipment class using CIVAB class of technology3.
In order to get that result, it is necessary the intervention of a Law enacted by Health Department or
by any Italian region, considering the power those bodies exercise on healthcare organizations:
anyway it is necessary the intervention of a regulatory body.
The consequence of the application of this law would consist in obtaining shortly a large database
about recorded failures on medical equipment; in addition the hospitals would get reciprocal
benefits sharing that volume of informations.
It would become possible for just one centralized entity to analyse data. That analysis would allow :
A. For each healthcare organization to know the distribution of the frequency of any failure
cause for each model/class.
B. To make comparisons among different hospitals, with regard to differences between failure
pattern for model/class.
The knowledge coming from point A could allow to every healthcare organization to understand
where should be more appropriate to invest resources in health, choosing in macro-areas like user
training, communication, Preventive Maintenance, advice on purchasing, etc.
M. Ridgway suggested the necessity to pay attention on better user training and purchasing better
designed equipment, instead of useless Preventive Maintenance in his PowerPoint presentation
“Effective maintenance strategies: Identifying the best practices for your facility” (AAMI 2010
Conference, Tampa, June 2010).
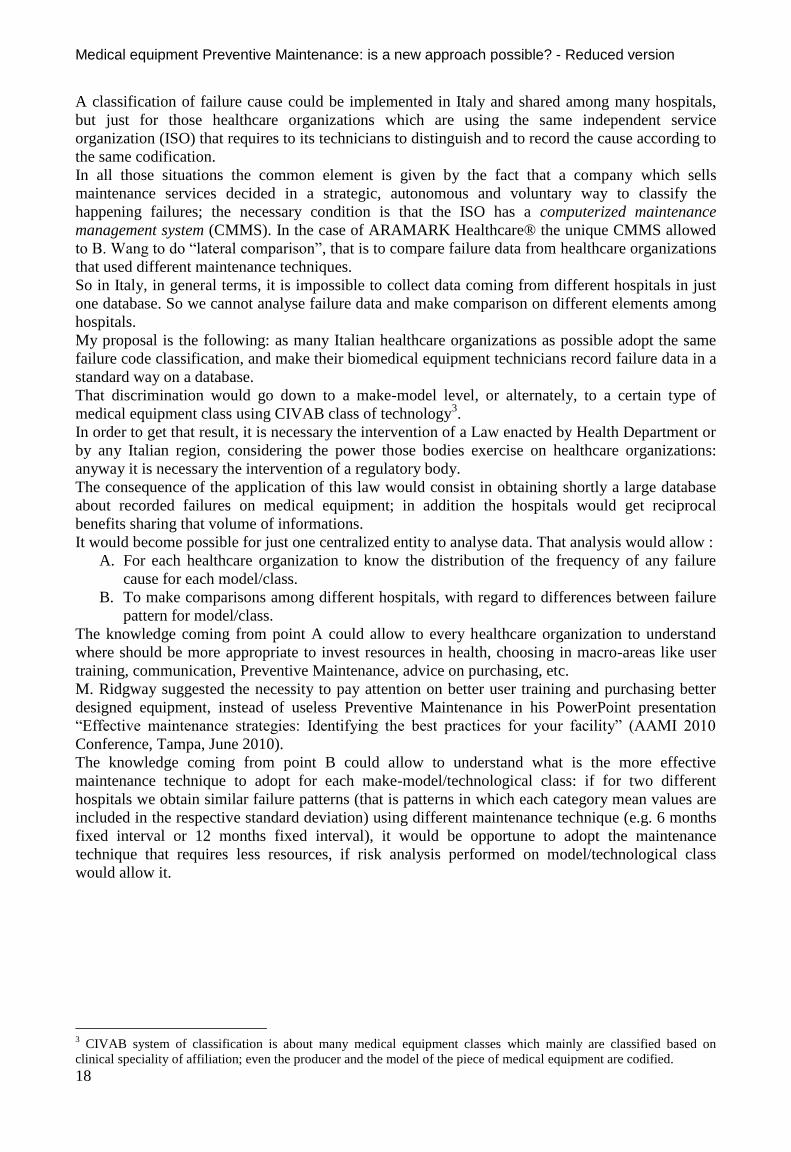
The knowledge coming from point B could allow to understand what is the more effective
maintenance technique to adopt for each make-model/technological class: if for two different
hospitals we obtain similar failure patterns (that is patterns in which each category mean values are
included in the respective standard deviation) using different maintenance technique (e.g. 6 months
fixed interval or 12 months fixed interval), it would be opportune to adopt the maintenance
technique that requires less resources, if risk analysis performed on model/technological class
would allow it.
3 CIVAB system of classification is about many medical equipment classes which mainly are classified based on
clinical speciality of affiliation; even the producer and the model of the piece of medical equipment are codified.
Author: Riccardo Offredi - [email protected]
19
Figure 7.1: Annual failure probability distribution for pulse oximeters in 3 groups of hospitals. Gained from Wang B., Fedele J., Pridgen R, et al., “Evidence-Based Maintenance - Part II: Comparing Maintenance Strategies Using Failure Codes”, Journal of clinical engineering, October/December2010; p. 228.
Figure 7.1 is about experiment detailed in paper titled “Evidence-Based Maintenance - Part II:
Comparing Maintenance Strategies Using Failure Codes”, Journal of clinical engineering,
October/December 2010 by Bang W., Fedele J., Pridgen R, et al. Data were collected by 6 hospitals
subdivided into 3 groups: one group were made of a single hospital and adopted statistical
sampling, a second group with 3 hospitals adopted 12 months fixed intervals Preventive
Maintenance; a third group with 2 hospitals that adopted run-to-failure technique.
Within each failure class, the height of each bar that derives form the second and third group is the
mean of the failure probabilities obtained by hospital within the corresponding group, whereas the
error bars represent ±1 standard deviation. The adoption of the best technique (i.e. the most
economic technique considering a certain failure pattern for each piece of medical equipment
model, pattern that is reasonably safe for patient) would allow saving of resources. The economized
resources would be invested in macro-areas coming from the knowledge of point A.
7.3.2. LEGISLATIVE AREA
I called this side “legislative area” because the most part of the efforts to implement structural
reforms must be accomplished by European and Italian Public Bodies.
In this section I am going to deal with the following themes:
A. Chance for clinical engineer to establish more appropriate Preventive Maintenance protocols
in Italian healthcare organizations;
B. Collaborative process to realize an initial Preventive Maintenance protocol that is effective
within European Community;
C. Preventive Maintenance service organization certification within European Community;
D. Maintenance task licence for biomedical equipment technicians within European
Community.
A. PREVENTIVE MAINTENANCE PROTOCOLS SELECTION
In this section I am proposing more freedom of choice and contextually a greater responsibility
assumption for clinical engineer during the selection and the implementation of medical equipment
maintenance protocols under his/her administration.
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
20
In the previous proposal I described the importance of collecting failure data to allow a maintenance
strategy change: this is absolutely useless if a Law forbids the clinical engineer’s choice about the
protocol to use, which is considered the most appropriate.
The Decree-law called “D. Lgs. N. 81 del 2008” (“Testo unico in materia di salute e sicurezza nei
luoghi di lavoro”) imposes de facto to clinical engineers to adopt, whenever it is possible, the only
protocol that was recommended by the manufacturer.
Nevertheless manufacturer recommended protocol may not be efficient for a set of reasons listed in
3.3.4. and 3.3.6.
Thinking valid the considerations that I produced in the previous chapters, it becomes obvious that
resources used in useless Preventive Maintenance entail a bad allocation of resources at disposal of
clinical engineering department. Resources are de facto stolen from other activities that have a
greater added value for patient care quality.
At the present time many clinical engineers are showing their willingness to have more decisional
capacity, i.e. they think that they should be allowed to decide if Preventive Maintenance task is
necessary, and if so, what is the frequency and what kind of tasks they must do (consider American
Society for Healthcare Engineering4 and Stiefel
5).
In B. Wang opinion it is necessary to call into question Preventive Maintenance strategy that has
been adopted, in the case new evidences collected on failure data indicate that opportunity.
The Decree-law called “Testo unico in materia di salute e sicurezza nei luoghi di lavoro” is
presently in force in Italy: consequently my proposal about giving the possibility to choose
Preventive Maintenance protocols requests to modify such Decree-law in article n. 71 paragraph n.
8. Particularly I am proposing to place at the same level of validity the manufacturer
recommendations and another protocol that has been obtained by clinical engineer (as medical
equipment manager): such protocol derives from reliable scientific considerations based on real
failure data coming from the same medical equipment managed by the clinical engineer.
In my opinion the consequences of this amendment are the following:
a) A new clinical engineering service would limit itself in following manufacturer
recommendation;
b) An expert clinical engineering service, basing on data collected from its own equipment,
could elaborate Preventive Maintenance protocols and verify any consequent change in
failure pattern.
Personally I am against the fact that any novice clinical engineering service modifies their protocols
without scientific evidence basis.
The implementation of the “technical proposal” (cf. 7.3.1.) could allow obtaining a homogeneous
classification of the failures that happen on medical equipment in Italian healthcare organizations.
Such information could allow comparing different failure patterns for specific make-models/
CIVAB technology classes.
The skilled clinical engineer will be able to compare failure patterns coming from the
implementation of different techniques with techniques that the same manager have already
implemented to modify possibly his/her own protocols.
Implementing a Preventive Maintenance technique that is cheaper and reasonably safe for the
patients, could allow optimizing resources at clinical engineering department disposal.
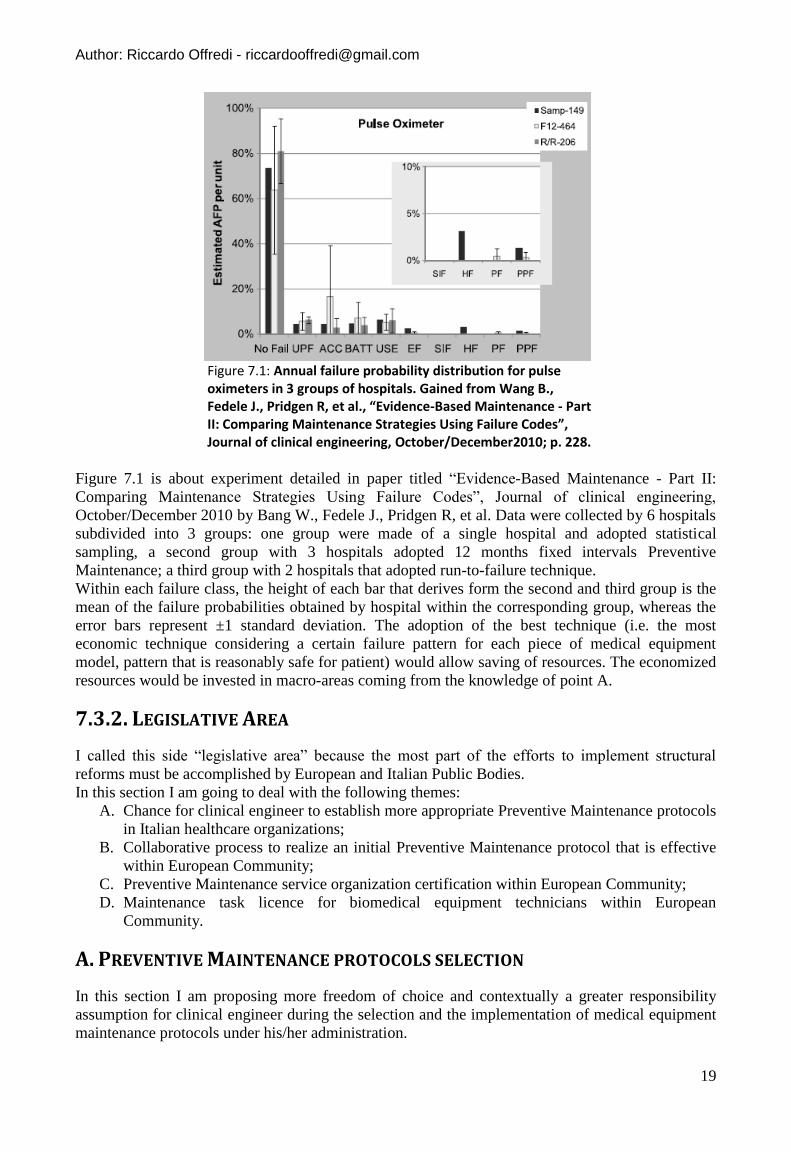
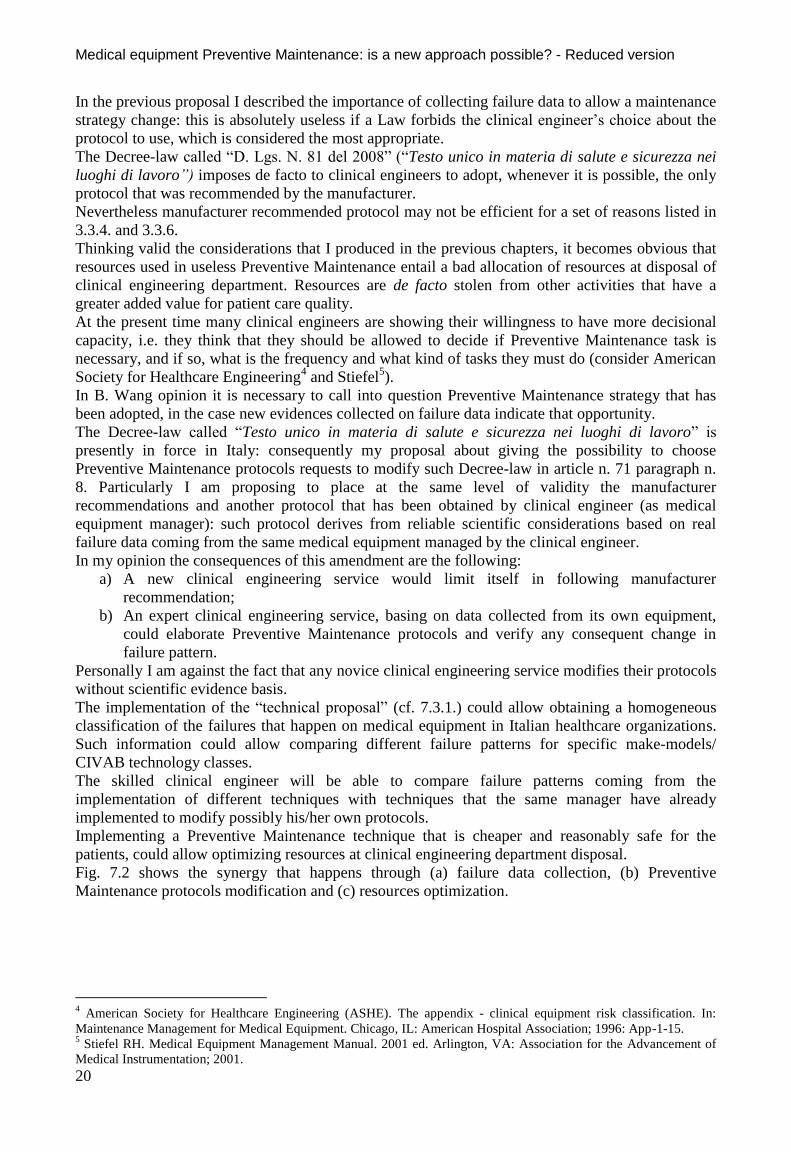
Fig. 7.2 shows the synergy that happens through (a) failure data collection, (b) Preventive
Maintenance protocols modification and (c) resources optimization.
4 American Society for Healthcare Engineering (ASHE). The appendix - clinical equipment risk classification. In:
Maintenance Management for Medical Equipment. Chicago, IL: American Hospital Association; 1996: App-1-15. 5 Stiefel RH. Medical Equipment Management Manual. 2001 ed. Arlington, VA: Association for the Advancement of
Medical Instrumentation; 2001.
Author: Riccardo Offredi - [email protected]
21
Figure 7.2: Synergic action of my proposals
B. COLLABORATIVE PROCESS FOR PREVENTIVE MAINTENANCE PROTOCOLS
In this section I am proposing to build an original process to realize an initial Preventive
Maintenance protocol for medical device that would be valid within the European Community, after
the amendment of European Directive on Medical Device in force.
Current Scenario
European Directive on Medical Device (n. 93/42 and following amendments) in force does not deal
with electromedical equipment management after that medical equipment is acquired by the
healthcare organization, but it deals with necessary conditions so that medical device may be put
onto the market. (cf. 3.2.2.).
Nevertheless in order to keep high the reliability level of a medical device, and so to guarantee high
patient safety level, it is necessary to carry out an appropriate Preventive Maintenance. It follows
the necessity for the hospitals to know -at least for the more dangerous devices for patient safety-
the relative Preventive Maintenance protocols when medical devices are put onto the market.
So I am proposing that European Parliament assess the possibility to introduce an amendment to
European Directive on Medical Device, in a way that every manufacturer -that want to put onto the
market dangerous medical devices- must issue a certified Preventive Maintenance protocol.
In my opinion two important gaps exist in current reality:
1) Manufacturer is not constrained to issue any Preventive Maintenance protocol. In annex I
(“essential requirements”) of European Directive 93/42 (and following amendments), in
“requirements regarding design and construction”, paragraph 13.6 it is written that:
“Where appropriate, the instructions for use must contain the following particulars: details
of the nature and frequency of the maintenance and calibration needed to ensure that the
devices operate properly and safely at all times;”
2) The process through which the manufacturer establish Preventive Maintenance protocol of a
medical device in unknown. So the protocol may not be the consequence of logical
consideration nor based on real evidences. This argument was suggested by M. Ridgway in
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
22
“Manufacturer-Recommended PM Intervals: Is It Time for a Change?”, Biomedical
Instrumentation & Technology, November/December 2009; pp. 498-500. In addition the
manufacturer has not any economical benefit in sharing data and information about technical
features and intrinsic reliability of the components.
So if a Preventive Maintenance protocol is not issued by the manufacturer when the medical device
is put onto the market, probably it will never be communicated by the same manufacturer.
Proposal
So my proposal is twofold: from one side I ask an amendment to impose the existence of a
Preventive Maintenance protocol for every dangerous medical device, and on the other side any
protocol must be certified through a process that involves an independent body compared to
manufacturer interests.
In this case the independent body is the Notified Body that any manufacturer chooses in order to get
the “Declaration of Conformity” of medical devices.
The Preventive Maintenance protocol would have the following features:
It would have been established through the collaboration between manufacturer and Notified
Body (chosen by manufacturer);
Through a defined process;
Valid anywhere in European Community;
Established before that any medical device is put onto the market;
Only for medical devices that are more dangerous (classes IIa, IIb and III).
Notified Body is characterized even today by a set of features that in my opinion make it
appropriate for being involved in the proposed process.
I am listing a set of features originated from annex XI of European Directive on Medical Devices
that specifies the essential criteria for designating Notified Bodies:
The Notified Body, its director and the assessment and verification staff shall not be the
designer, manufacturer, supplier, installer or user of the devices which they inspect, nor the
authorized representative of any of these persons. They may not be directly involved in the
design, construction, marketing or maintenance of the devices, nor represent the parties
engaged in these activities. This in no way precludes the possibility of exchanges of
technical information between the manufacturer and the body.
The Notified Body and its staff must carry out the assessment and verification operations
with the highest degree of professional integrity and the requisite competence in the field of
medical devices and must be free from all pressures and inducements, particularly financial,
which might influence their judgment or the results of the inspection, especially from
persons or groups of persons with an interest in the results of the verifications.
The Notified Body must have:
- sound vocational training covering all the assessment and verification operations for
which the body has been designated,
- satisfactory knowledge of the rules on the inspections which they carry out and
adequate experience of such inspections,
- the ability required to draw up the certificates, records and reports to demonstrate
that the inspections have been carried out.
The impartiality of the Notified Body must be guaranteed. Their remuneration must not
depend on the number of inspections carried out, nor on the results of the inspections.
The staff of the notified body are bound to observe professional secrecy with regard to all
information gained in the course of their duties (except vis-à-vis the competent
administrative authorities of the State in which their activities are carried out) pursuant to
this Directive or any provision of national law putting it into effect.
In brief, the staff is qualified, the Notified Body is free from conflict of interests with any
manufacturer.

Author: Riccardo Offredi - [email protected]
23
Notified Bodies is reliable in order to guarantee the safety deriving from medical device because:
Notified Bodies are designated by Competent Authority in member States;
In order to be designated, the Notified Bodies must meet strict criteria contained in
Directives and Regulation of European Union;
Notified Bodies have the safety as a founding value.
Consequently I am proposing that Notified Body chosen by the manufacturer, beyond carrying out
tasks requested currently by European Directive on Medical Device, would deal with manufacturer
Preventive Maintenance protocol certification.
I am outlining in figure 7.3 the collaborative process in order to obtain the Preventive Maintenance
protocol.
Figure 7.3: Process flowchart in order to obtain Preventive Maintenance protocol.
In my opinion, the manufacturer should define the rationale through which each non-durable part
contained in the medical device should be substituted/restored (fixed intervals, metered
maintenance, predictive maintenance, other) to the chosen Notified Body; such rationale should
derive from technical analysis or testing on non-durable parts.
Implementing my proposal to obtain Preventive Maintenance protocol certified by a Notified Body
would become a necessary condition in order to put any dangerous medical device into the
European market.
I am explaining briefly the reasons for which, in my opinion, it is so important to know a Preventive
Maintenance protocol associated to any quite dangerous medical device.
The lack of a Preventive Maintenance protocol causes problem to clinical engineering service that
must do its best to understand what may be the most appropriate protocol: in Italy, the Decree-law
called “Testo Unico in Materia di Salute e Sicurezza nei luoghi di lavoro” (D. Lgs. 81/2008)
recommends to seek among good techniques rules, or in absence of the latter, that may be deduced
from best practice codes. Probably the alternative consequences may be the following:
If the technology is quite simple, clinical engineering service will elaborate a protocol
without having data coming from the device and so that protocol could be approximate;
If the technology is complex, clinical engineering service may turn to the manufacturer that
may impose high price.
Let’s consider the proposal that is about involving Notified Bodies for establishing a shared
Preventive Maintenance protocol: in my opinion the proposal is feasible because, even if the
quantity of the brand-new class IIa, IIb, and III medical device models put onto the market is high,
even the number of Notified Bodies is considerable. In particular in November 2010 the total of
Notified Bodies6 approved under the European Directive on Medical Device is 73.
Consequences of hoped proposal
The application of the two described above proposals would cause to obtain the following benefits:
At least one Preventive Maintenance protocol exists for each dangerous class (IIa / IIb / III)
of medical devices;
6 Notified Bodies list is present in appendix A.
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
24
Protocol validation made by an independent body, whose mission is safety;
Probably the effectiveness of the protocol is improved: particularly Preventive Maintenance
tasks considered useless by the Notified Body are reduced/deleted; such tasks could have
increased the possibility of service-induced failure or simply could have reduced the
possibility to supply health care services, because of downtime;
Probably “infant mortality” event of non-durable part would reduce (cf. 3.3.6.):
consequently medium reliability levels should increase for each medical device;
Expected patient safety improvement;
Expected reduction of Preventive Maintenance management cost in hospital: the healthcare
organization, if it has got the technical skills within, is able to accomplish Preventive
Maintenance task autonomously, following the protocol recommendation (that would be
known) and save. I remind that, for the same financing received by the hospital, the money
saved in medical device management could be invested in other activities, that have a
greater added value for patient healthcare quality.
Reduction of clinical engineering service manager responsibility, because the manager
should not risk any more through the adoption of an approximate protocol, that could be
dangerous for patients or, in the opposite case, expensive.
Appreciation in brand value of manufacturer: considering the globalization in existence, the
manufacturer that put its products onto European market would be well-known all over the
world for its care for patient-safety, demonstrated by the effort for establishing a Preventive
Maintenance protocol, that is offshoot of a collaborative process.
I must point out that there could be negative consequences for the manufacturer, that is the
reduction of the profit coming from:
Raising of safety cost deriving from the process of protocol determination;
If the fixed interval technique is maintained, probable reduction of the frequency of
intervention, and so reduction of total number of technicians’ task;
Possible introduction of maintenance techniques that are different compared to the interval
fixed one (metered maintenance, run-to-failure, predictive maintenance);
Considering that currently the manufacturer can resort to an auto-certification in order to put its not
very dangerous medical devices (that is class I) onto the market, my proposal in accordance is not
applicable to the same medical devices.
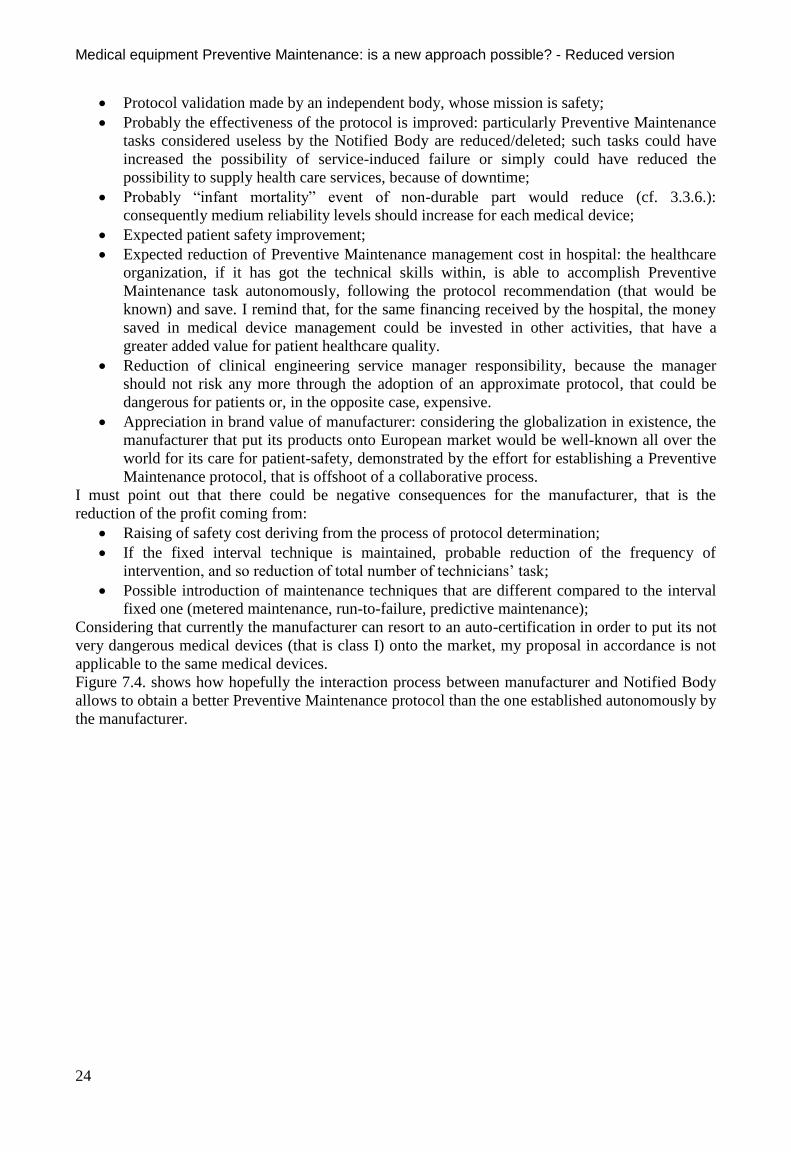
Figure 7.4. shows how hopefully the interaction process between manufacturer and Notified Body
allows to obtain a better Preventive Maintenance protocol than the one established autonomously by
the manufacturer.
Author: Riccardo Offredi - [email protected]
25
Figure 7.4: Interaction between manufacturer and Notified Body allows to obtain a Preventive Maintenance protocol that is shared and probably better than the one established autonomously by the manufacturer.
Considering still valid at the same time both the proposal A (“Preventive Maintenance protocols
selection”) in which I describe the chance for clinical engineers to establish which Preventive
Maintenance protocol to use, and the proposal B, in which I describe the possibility to establish
Preventive Maintenance protocols offshoot of a collaborative process between manufacturer and
Notified Body, I hope that clinical engineering service initially adopts the manufacturer protocol
and only in a second step the clinical engineering service modifies such protocol, in order to apply a
technique judged more in compliance with the necessities of the hospital in which the medical
device is working.
C. MAINTENANCE SERVICE ORGANIZATION
The companies that deal with Preventive Maintenance tasks and their staff which is authorized to
that job are fundamental in healthcare sector to hold a high level of reliability of medical equipment
and so they help to maintain high level of safety.
Nevertheless it does not exist any prescription -which demand specific quality standards- in the
healthcare sector valid for all the independent companies that sell Preventive Maintenance service.
Considering the Commission Regulation (EC) No 2042/2003 of 20 November 2003 (cf. 5.2.5.), I
am suggesting that European Commission imposes to any company that sells Preventive
Maintenance service for medical technology, to satisfy the following requirements:
The maintenance service company must supply a handbook that contains a declaration
signed by the responsible manager, in which it is declared that the company is going to
accomplish all the necessary tasks.
The maintenance service company must designate a responsible manager invested with the
authority that needs to make sure that all the maintenance tasks requested by medical device
manager could be financed and performed according to prescribed standards.
All the employees in the company that are dealing with maintenance tasks must demonstrate
to have skills, background, or experience in medical device maintenance sector.
The maintenance service company must have the necessary equipment and tools in order to
accomplish maintenance tasks established.
The maintenance service company must hold maintenance data and use them in the
execution of its assignments, comprising preventive and corrective maintenance;
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
26
Each maintenance service company will have be subject to a complete audit at least once in
24 months;
The competent authority must record all non-conformities, the corrective interventions to
compensate, and the recommendations.
Implementing this law in European Community, a higher general degree of quality would be
guaranteed in medical equipment maintenance service organizations. That consequence would
cause a higher level of medical device reliability and so a probable improvement in patient & staff
safety (cf. figure 7.5.).
Figure 7.5: Consequences coming from the modification of European directive on reliability of medical device.
D. BIOMEDICAL EQUIPMENT TECHNICIAN
Considering the Commission Regulation (EC) No 2042/2003 of 20 November 2003 (cf. 5.2.5.), I
am suggesting that European Commission would bind the technicians who desire to perform any
kind of maintenance task on a medical device to obtain the following requirements.
People must be more that 18 years old in order to make a request of licence of maintenance.
They who require a medical equipment maintenance licence have to demonstrate through
examination to have an appropriate level of knowledge of pertinent modules of subjects.
In addiction they have to possess certain requirements of matured experiences.
According to the kind of licence that the technician possesses (for example specialized in
bioimaging medical equipment), this person will be allowed to accomplish specific maintenance
tasks and to release specific certification to readmit in service the piece of equipment, following up
an appropriate maintenance task.
The practice of certification privileges is subordinated to some conditions, among the following
ones:
Six month experience in maintenance sector, matured in the last two previous years,
according to privileges granted by maintenance licence;
Ability to read, write and to communicate at a comprehensible level in a language in which
the documentation is drawn up.
Achieving a medical equipment maintenance licence would supply to the hospital managers a more
homogeneous and standardized way to select the professionals that are working in the healthcare
organization, compared to current practice in which the hospital managers require technician’s
curriculum vitae and on this basis the manager valuates the professionalism of the same technician.
Author: Riccardo Offredi - [email protected]
27
Figure 7.6: Biomedical Equipment Technician’s certified professionalism.
Figure 7.6 outlines how through the constitution of European Community Law, it would be possible
to impose to technicians, who want to deal with Preventive Maintenance, the achievement of a
maintenance licence: the Law described above would allow to healthcare organization managers to
lay up for technicians with certified skills.
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
28
CONCLUSIONS
The initial goal of my thesis was to understand if it is possible to find and to implement Preventive
Maintenance protocols which are different from OEMs’ Preventive Maintenance protocols to
improve patient quality of care, considering hospital peculiar necessities where medical equipment
is used.
Through the evidence collection and my thinking, I noticed that the current maintenance strategies
recommended by medical equipment manufacturers written on paper very probably are not feasible
by any Italian hospital with a degree of completion equal to 100% for all the pieces of equipment:
the principal reason lies in the scarcity of resources at disposal of clinical engineer department.
The Italian Law imposes to use manufacturers’ protocols (if they have been communicated) which
often schedule fixed interval technique. Currently Preventive Maintenance techniques that are more
appropriate to the necessities exist, but those techniques cannot be implemented because technology
managers are not allowed to select arbitrarily Preventive Maintenance protocol considered more
appropriate for any piece of equipment.
If we do not want to see the concrete, even when it is evident, we are not doing our best for overall
patient safety: in a situation of shortage of resources, rough choices would be made on how to
invest the same resources, that is probably it would be done Preventive Maintenance tasks on a
certain number of medical device operating in quite critical areas, which are operating room,
intensive-care unit and emergency department, excluding other medical equipment, which is
important for patient safety, working in other departments.
Consequently it would be appropriate to focus on prevention of the failures that cause the greater
damage on patient (or on hospital mission) and that happen with a greater frequency: in brief a risk
analysis should be done on medical equipment which is operating in each hospital. Such risk
analysis would prefigure the necessity to exclude a set of medical equipment from Preventive
Maintenance task.
Considering that overall manufacturers’ recommendations are not feasible contextually, it would be
opportune to revise accordingly the “rules of the game”, that is to modify the Decree-law “D. Lgs.
81 / 2008” in order to allow the responsible choice of more appropriate maintenance technique
made by clinical engineering service managers: we could take example from state of the art
accrediting organization (for example “The Joint Commission”).
Waiting for those amendments to come, I proposed an expedient to obtain Preventive Maintenance
protocols quite appropriate for necessities of the Italian public hospital companies (that can be
extended to Italian private hospital companies): in the negotiation of contracting agreement it is
inserted a bonus coming from the will of collaboration between manufacturer and hospital; the
collaboration is apt to determine the Preventive Maintenance protocol to apply on the piece of
medical equipment which is negotiated.
How can a clinical engineer, as a technology manager, improve the patient healthcare quality,
considering all the activities that this person presides?
To answer to this question, let’s examine two differing scenarios according to available resources.
OPTIMISTIC SCENARIO
In the first scenario, the least probable one, I am supposing that the healthcare sector funding in a
certain Country of the European Union, is going to increase proportionally to the evolution of the
growing requirements of healthcare sector.
In my opinion, in such a case the perspective to improve patient healthcare quality would be
feasible. Such goal, from the technology manager point of view, consists mainly in the best
allocation of available resources.
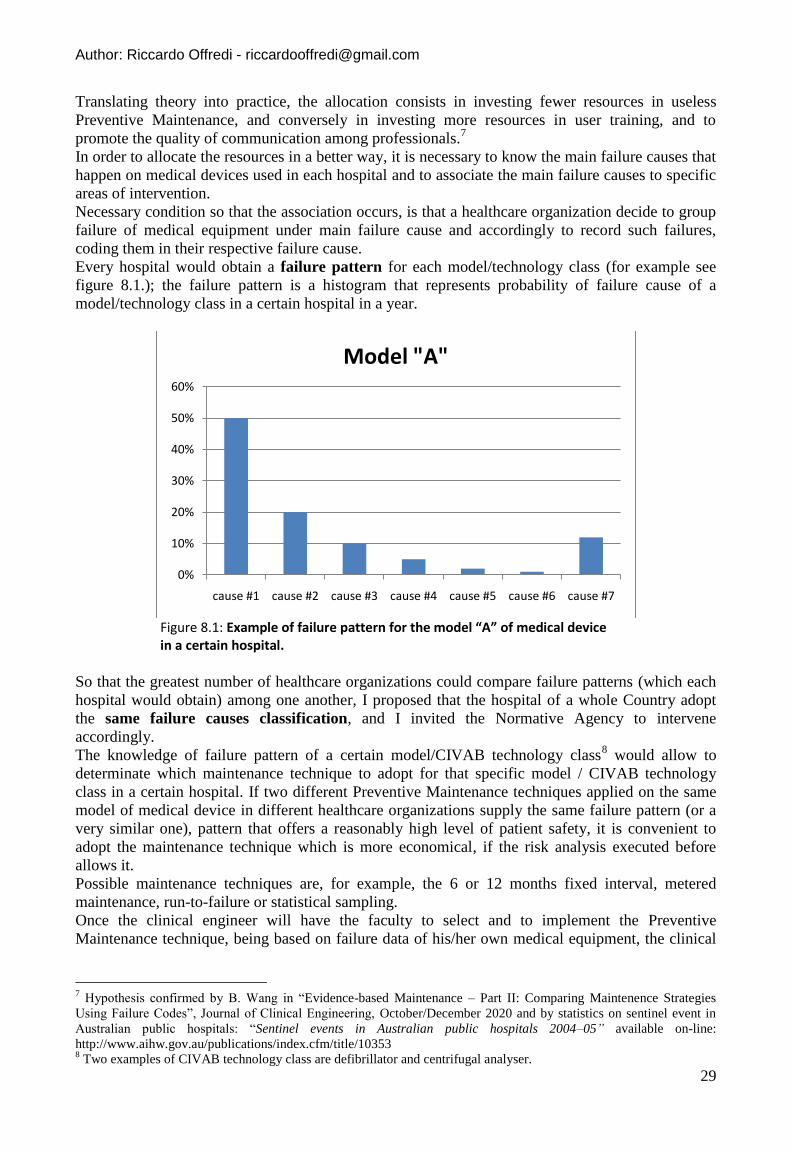
Author: Riccardo Offredi - [email protected]
29
Translating theory into practice, the allocation consists in investing fewer resources in useless
Preventive Maintenance, and conversely in investing more resources in user training, and to
promote the quality of communication among professionals.7
In order to allocate the resources in a better way, it is necessary to know the main failure causes that
happen on medical devices used in each hospital and to associate the main failure causes to specific
areas of intervention.
Necessary condition so that the association occurs, is that a healthcare organization decide to group
failure of medical equipment under main failure cause and accordingly to record such failures,
coding them in their respective failure cause.
Every hospital would obtain a failure pattern for each model/technology class (for example see
figure 8.1.); the failure pattern is a histogram that represents probability of failure cause of a
model/technology class in a certain hospital in a year.
Figure 8.1: Example of failure pattern for the model “A” of medical device in a certain hospital.
So that the greatest number of healthcare organizations could compare failure patterns (which each
hospital would obtain) among one another, I proposed that the hospital of a whole Country adopt
the same failure causes classification, and I invited the Normative Agency to intervene
accordingly.
The knowledge of failure pattern of a certain model/CIVAB technology class8 would allow to
determinate which maintenance technique to adopt for that specific model / CIVAB technology
class in a certain hospital. If two different Preventive Maintenance techniques applied on the same
model of medical device in different healthcare organizations supply the same failure pattern (or a
very similar one), pattern that offers a reasonably high level of patient safety, it is convenient to
adopt the maintenance technique which is more economical, if the risk analysis executed before
allows it.
Possible maintenance techniques are, for example, the 6 or 12 months fixed interval, metered
maintenance, run-to-failure or statistical sampling.
Once the clinical engineer will have the faculty to select and to implement the Preventive
Maintenance technique, being based on failure data of his/her own medical equipment, the clinical
7 Hypothesis confirmed by B. Wang in “Evidence-based Maintenance – Part II: Comparing Maintenence Strategies
Using Failure Codes”, Journal of Clinical Engineering, October/December 2020 and by statistics on sentinel event in
Australian public hospitals: “Sentinel events in Australian public hospitals 2004–05” available on-line:
http://www.aihw.gov.au/publications/index.cfm/title/10353 8 Two examples of CIVAB technology class are defibrillator and centrifugal analyser.
0%
10%
20%
30%
40%
50%
60%
cause #1 cause #2 cause #3 cause #4 cause #5 cause #6 cause #7
Model "A"

Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
30
engineer will improve the effectiveness of his/her job, reducing costs and maintaining unaltered the
reliability levels of the responsibly selected portion of medical equipment.
The knowledge of the most important failure cause is useful for different equipment classes. Let’s
consider the department “A”, in which a significant portion of medical equipment is subjected to
failures relating to “user related” reason: it is probable that in such department the users’ care for
the medical equipment is poor, maybe due to new workers. In such a case, the area in which to
invest more resources would be staff training. The knowledge of failure pattern and failure causes
contributes to improve patient healthcare quality (see figure 8.2.).
Figure 8.2: Proposal to improve patient healthcare quality.
REALISTIC SCENARIO
In the most probable scenario technology manager’s goal is to maintain unaltered the high level of
patient healthcare quality and to cope with a growth in financing that is less than proportional to the
increasing necessities of Healthcare sector of Member Countries in the European Union: de facto
the technology manager is going to support a reduction in available resources.
It results that clinical engineering department must optimize the resources, and, differently from the
previous case, it is not posed the problem that is about where to invest the resources obtained from
the optimization.
The main proposed way to get this result is that of the selection of the best technique to adopt,
basing on the comparison of failure patterns of each model/CIVAB technology class, if risk analysis
allows it.
Author: Riccardo Offredi - [email protected]
31
FINAL CONSIDERATIONS
Both scenarios converge on the necessity to code the failures that happen on technology manager’s
medical equipment in respective failure cause, within a homogeneous classification that is shared
among healthcare organizations.
The more healthcare organization will share the same classification, the more quickly it will be
possible to benchmark different Preventive Maintenance techniques.
It will be possible to classify at a more general level (CIVAB technology classes) or more specific
level (make-model of medical equipment): in the former case the timetable would be quite short in
order to obtain a great amount of data and to make comparisons among different techniques; in the
latter case the classification would give orienting results with a higher degree of confidence in terms
of which technique to adopt.
The collection of data coming from technology manager’s medical equipment influences
maintenance techniques that will be adopted on the same set of medical devices, following a critical
reconsideration of methods and results: consequently the organization of Preventive Maintenance
models itself on the necessities of a single hospital. In brief this process is the teaching of Evidence-
based Maintenance which is Reliability-centered Maintenance applied in the healthcare sector.
Remembering this thesis title, changing the approach to Preventive Maintenance is not just possible,
but even hoped. Through risk analysis and the knowledge of failure pattern, it is possible to deduce
what is the best maintenance technique to apply to each model/technological class. Such technique
entails the adoption of a certain maintenance protocol –and so even Preventive Maintenance
protocol- for each model of medical equipment.
The Preventive Maintenance protocol recommended by manufacturer could differ from the one
resulting from the process described above, because the former aims at minimizing the number of
failures on a specific piece of medical equipment, while the latter has the goal to improve overall
patient healthcare quality.
FUTURE DEVELOPMENTS
Considering that medical equipment manufacturers tendentially don’t disclose the rationale by
which the manufacturers establish Preventive Maintenance protocols, and that such behaviour could
be less and less tolerable by the buyers (i.e. healthcare organizations), I am proposing the
development of a Preventive Maintenance protocol to be defined through rational criteria and goals
in cooperation with a healthcare organization.
The manufacturer would obtain the following advantages:
The producer could benefits from the hospital collaboration to receive a feedback about the
protocol quality and to improve medical device user interface;
The manufacturer could show the image of open-mindedness and listening to the customer.
The healthcare organizations would obtain the benefit of enjoying in usufruct a piece of medical
equipment not-so-expensive in terms of invested resources in Preventive Maintenance and
contemporaneously more reliable in order to improve patient safety.
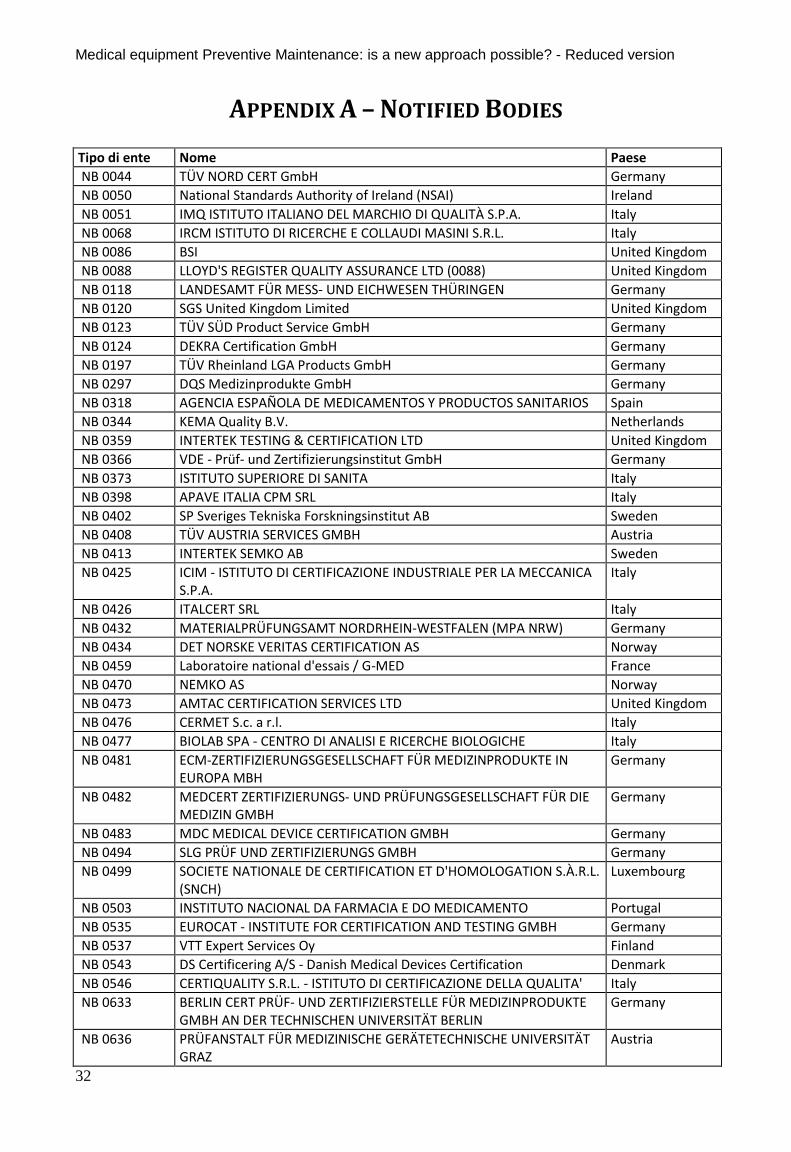
Medical equipment Preventive Maintenance: is a new approach possible? - Reduced version
32
APPENDIX A – NOTIFIED BODIES
Tipo di ente Nome Paese NB 0044 TÜV NORD CERT GmbH Germany NB 0050 National Standards Authority of Ireland (NSAI) Ireland NB 0051 IMQ ISTITUTO ITALIANO DEL MARCHIO DI QUALITÀ S.P.A. Italy NB 0068 IRCM ISTITUTO DI RICERCHE E COLLAUDI MASINI S.R.L. Italy NB 0086 BSI United Kingdom NB 0088 LLOYD'S REGISTER QUALITY ASSURANCE LTD (0088) United Kingdom NB 0118 LANDESAMT FÜR MESS- UND EICHWESEN THÜRINGEN Germany NB 0120 SGS United Kingdom Limited United Kingdom NB 0123 TÜV SÜD Product Service GmbH Germany NB 0124 DEKRA Certification GmbH Germany NB 0197 TÜV Rheinland LGA Products GmbH Germany NB 0297 DQS Medizinprodukte GmbH Germany NB 0318 AGENCIA ESPAÑOLA DE MEDICAMENTOS Y PRODUCTOS SANITARIOS Spain NB 0344 KEMA Quality B.V. Netherlands NB 0359 INTERTEK TESTING & CERTIFICATION LTD United Kingdom NB 0366 VDE - Prüf- und Zertifizierungsinstitut GmbH Germany NB 0373 ISTITUTO SUPERIORE DI SANITA Italy NB 0398 APAVE ITALIA CPM SRL Italy NB 0402 SP Sveriges Tekniska Forskningsinstitut AB Sweden NB 0408 TÜV AUSTRIA SERVICES GMBH Austria NB 0413 INTERTEK SEMKO AB Sweden NB 0425 ICIM - ISTITUTO DI CERTIFICAZIONE INDUSTRIALE PER LA MECCANICA
S.P.A. Italy
NB 0426 ITALCERT SRL Italy NB 0432 MATERIALPRÜFUNGSAMT NORDRHEIN-WESTFALEN (MPA NRW) Germany NB 0434 DET NORSKE VERITAS CERTIFICATION AS Norway NB 0459 Laboratoire national d'essais / G-MED France NB 0470 NEMKO AS Norway NB 0473 AMTAC CERTIFICATION SERVICES LTD United Kingdom NB 0476 CERMET S.c. a r.l. Italy NB 0477 BIOLAB SPA - CENTRO DI ANALISI E RICERCHE BIOLOGICHE Italy NB 0481 ECM-ZERTIFIZIERUNGSGESELLSCHAFT FÜR MEDIZINPRODUKTE IN
EUROPA MBH Germany
NB 0482 MEDCERT ZERTIFIZIERUNGS- UND PRÜFUNGSGESELLSCHAFT FÜR DIE MEDIZIN GMBH
Germany
NB 0483 MDC MEDICAL DEVICE CERTIFICATION GMBH Germany NB 0494 SLG PRÜF UND ZERTIFIZIERUNGS GMBH Germany NB 0499 SOCIETE NATIONALE DE CERTIFICATION ET D'HOMOLOGATION S.À.R.L.
(SNCH) Luxembourg
NB 0503 INSTITUTO NACIONAL DA FARMACIA E DO MEDICAMENTO Portugal NB 0535 EUROCAT - INSTITUTE FOR CERTIFICATION AND TESTING GMBH Germany NB 0537 VTT Expert Services Oy Finland NB 0543 DS Certificering A/S - Danish Medical Devices Certification Denmark NB 0546 CERTIQUALITY S.R.L. - ISTITUTO DI CERTIFICAZIONE DELLA QUALITA' Italy NB 0633 BERLIN CERT PRÜF- UND ZERTIFIZIERSTELLE FÜR MEDIZINPRODUKTE
GMBH AN DER TECHNISCHEN UNIVERSITÄT BERLIN Germany
NB 0636 PRÜFANSTALT FÜR MEDIZINISCHE GERÄTETECHNISCHE UNIVERSITÄT GRAZ
Austria
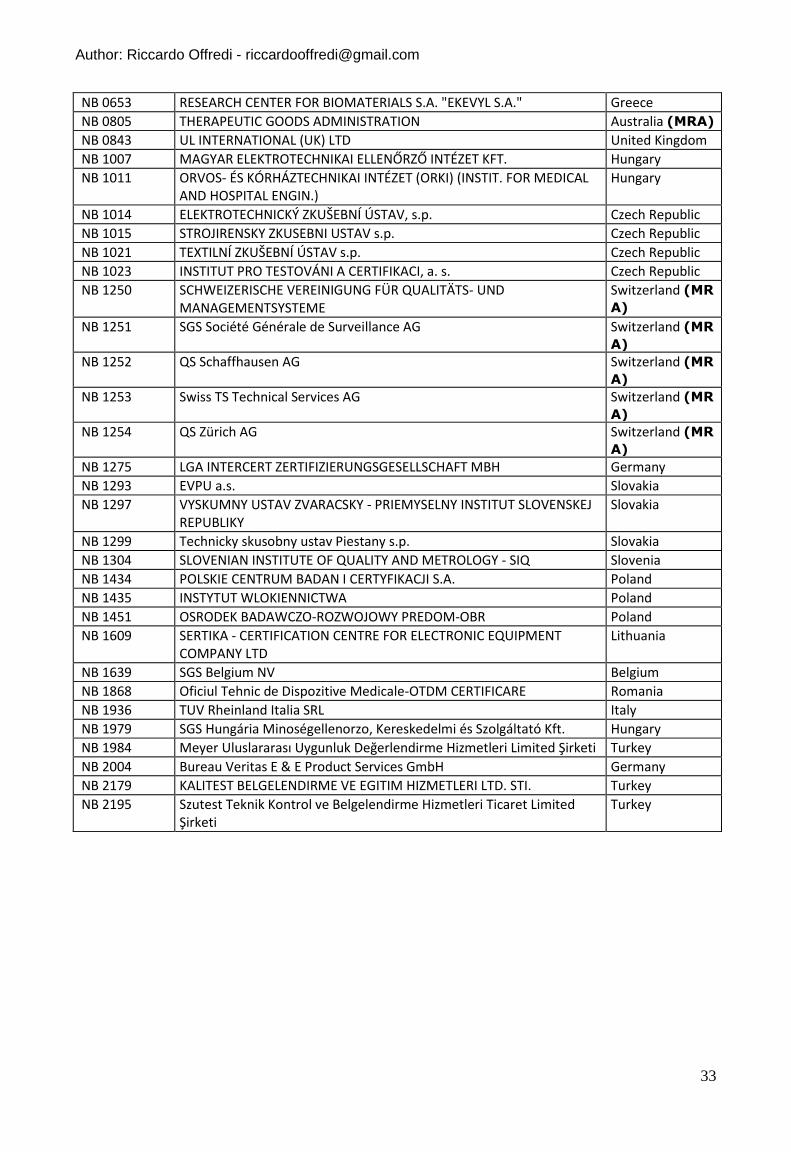
Author: Riccardo Offredi - [email protected]
33
NB 0653 RESEARCH CENTER FOR BIOMATERIALS S.A. "EKEVYL S.A." Greece NB 0805 THERAPEUTIC GOODS ADMINISTRATION Australia (MRA)
NB 0843 UL INTERNATIONAL (UK) LTD United Kingdom NB 1007 MAGYAR ELEKTROTECHNIKAI ELLENŐRZŐ INTÉZET KFT. Hungary NB 1011 ORVOS- ÉS KÓRHÁZTECHNIKAI INTÉZET (ORKI) (INSTIT. FOR MEDICAL
AND HOSPITAL ENGIN.) Hungary
NB 1014 ELEKTROTECHNICKÝ ZKUŠEBNÍ ÚSTAV, s.p. Czech Republic NB 1015 STROJIRENSKY ZKUSEBNI USTAV s.p. Czech Republic NB 1021 TEXTILNÍ ZKUŠEBNÍ ÚSTAV s.p. Czech Republic NB 1023 INSTITUT PRO TESTOVÁNI A CERTIFIKACI, a. s. Czech Republic NB 1250 SCHWEIZERISCHE VEREINIGUNG FÜR QUALITÄTS- UND
MANAGEMENTSYSTEME Switzerland (MR
A)
NB 1251 SGS Société Générale de Surveillance AG Switzerland (MR
A)
NB 1252 QS Schaffhausen AG Switzerland (MR
A)
NB 1253 Swiss TS Technical Services AG Switzerland (MR
A)
NB 1254 QS Zürich AG Switzerland (MR
A)
NB 1275 LGA INTERCERT ZERTIFIZIERUNGSGESELLSCHAFT MBH Germany NB 1293 EVPU a.s. Slovakia NB 1297 VYSKUMNY USTAV ZVARACSKY - PRIEMYSELNY INSTITUT SLOVENSKEJ
REPUBLIKY Slovakia
NB 1299 Technicky skusobny ustav Piestany s.p. Slovakia NB 1304 SLOVENIAN INSTITUTE OF QUALITY AND METROLOGY - SIQ Slovenia NB 1434 POLSKIE CENTRUM BADAN I CERTYFIKACJI S.A. Poland NB 1435 INSTYTUT WLOKIENNICTWA Poland NB 1451 OSRODEK BADAWCZO-ROZWOJOWY PREDOM-OBR Poland NB 1609 SERTIKA - CERTIFICATION CENTRE FOR ELECTRONIC EQUIPMENT
COMPANY LTD Lithuania
NB 1639 SGS Belgium NV Belgium NB 1868 Oficiul Tehnic de Dispozitive Medicale-OTDM CERTIFICARE Romania NB 1936 TUV Rheinland Italia SRL Italy NB 1979 SGS Hungária Minoségellenorzo, Kereskedelmi és Szolgáltató Kft. Hungary NB 1984 Meyer Uluslararası Uygunluk Değerlendirme Hizmetleri Limited Şirketi Turkey NB 2004 Bureau Veritas E & E Product Services GmbH Germany NB 2179 KALITEST BELGELENDIRME VE EGITIM HIZMETLERI LTD. STI. Turkey NB 2195 Szutest Teknik Kontrol ve Belgelendirme Hizmetleri Ticaret Limited
Şirketi Turkey