Rheumatology, Orthopaedics and Trauma...Musculoskeletal Physiological Phenomena– Handbooks. 3....
13
Transcript of Rheumatology, Orthopaedics and Trauma...Musculoskeletal Physiological Phenomena– Handbooks. 3....



Rheumatology, Orthopaedics and Trauma at a Glance


Rheumatology, Orthopaedics and Trauma at a GlanceCatherine SwalesMRCP, PhDClinical Lecturer in RheumatologyNuffi eld Orthopaedic CentreOxford
Christopher BulstrodeMCh, FRCS(Orth)Emeritus Professor in Trauma and OrthopaedicsUniversity of OxfordOxford
Second edition
A John Wiley & Sons, Ltd., Publication

This edition fi rst published 2012 © 2012 by John Wiley & Sons, Ltd
Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s global Scientifi c, Technical and Medical business with Blackwell Publishing.
Registered offi ce: John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial offi ces: 9600 Garsington Road, Oxford, OX4 2DQ, UK The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK 111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offi ces, for customer services and for information about how to apply for permission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell.
The right of the author to be identifi ed as the author of this work has been asserted in accordance with the UK Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that the publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional should be sought.
First edition published 2007
Second edition published 2012
Library of Congress Cataloging-in-Publication Data
Swales, Catherine. Rheumatology, orthopaedics, and trauma at a glance / Catherine Swales, Christopher Bulstrode. – 2nd ed. p. ; cm. – (At a glance) Rev. ed. of: The musculoskeletal system at a glance / Christopher Bulstrode, Catherine Swales. 2007. Includes bibliographical references and index. ISBN-13: 978-0-470-65470-5 (pbk. : alk. paper) ISBN-10: 0-470-65470-8 (pbk. : alk. paper) 1. Musculoskeletal system. I. Bulstrode, C. J. K. (Christopher J. K.) II. Bulstrode, C. J. K. (Christopher J. K.). Musculoskeletal system at a glance. III. Title. IV. Series: At a glance series (Oxford, England) [DNLM: 1. Musculoskeletal Diseases–Handbooks. 2. Musculoskeletal Physiological Phenomena–Handbooks. 3. Musculoskeletal System–injuries–Handbooks. 4. Orthopedics–methods–Handbooks. 5. Rheumatic Diseases–Handbooks. WE 39] QP301.B8956 2012 616.7–dc23 2011015187
A catalogue record for this book is available from the British Library.
1 2012

Contents 5
Preface 6Guide to anatomical terminology 7
Section 1 Introduction1 Musculoskeletal structure and function 82 Calcium homeostasis and bone metabolism 103 History and examination – an overview 124 Imaging 14
Section 2 The arm5 Anatomy of the arm 166 History and examination of the arm 197 Problems presenting in the arm 228 Upper arm trauma 249 Lower arm trauma 26
Section 3 The spine 10 Anatomy of the spine 2811 History and examination of the spine 3012 Problems presenting in the spine 3213 Trauma of the spine 34
Section 4 The leg14 Anatomy of the leg 3615 History and examination of the leg 3816 Problems presenting in the hip 4017 Joint replacement 4218 Problems presenting in the lower leg 4419 Upper leg trauma 4620 Lower leg trauma 48
Section 5 Rheumatology21 Rheumatological history and examination 5022 Pathogenesis of rheumatoid arthritis 5223 Rheumatoid arthritis 54
Contents
24 Systemic lupus erythematosus 5725 Ankylosing spondylitis 6026 The spondyloarthropathies 6227 Acute joint disease 6428 Infection and malignancy 6629 Fibromyalgia 6830 Osteoporosis 7031 Disorders of bone metabolism 7232 Vasculitis 1: Giant cell arteritis 7433 Vasculitis 2: Medium and small vessel vasculitis 7634 Scleroderma 7835 Infl ammatory muscle diseases 8036 The medical management of infl ammatory disease 8237 Rehabilitation 84
Section 6 Orthopaedics38 Orthopaedics in children 8639 Sports medicine 8840 Neurological disorders and orthotics 9041 Orthopaedics in the elderly 92
Section 7 Trauma42 Initial management of the polytraumatised patient 9443 Wound management 9644 Plastic surgery 9745 Burns 9846 Peripheral and spinal nerve injuries 10047 Head injuries 10248 Fractures and dislocations 10449 Compartment syndrome 106
Self-assessment case studies: questions 108Self-assessment case studies: answers 110
Index 113

6 Preface
Preface
This is the second edition of a book specially designed for clinical students who are doing their rheumatology, orthopaedics and trauma attachments. It is one of a very successful ‘ At a Glance ’ series which gives you, the student, the minimum information you need to pass your exams. It is short and very visual, so it should work well as a fast revision text too. It is based on the 8 week course taught at the Oxford Medical School by the two authors.
However, it should also be very useful for GP trainees who have such a huge range of subjects to cover, and so need essential informa-tion on each subject in a quick and easily digestible form.
Each chapter is one page of diagrams combined with one page of text. We have tried to cover the basic science (including anatomy and physiology) right through to practical procedures such as how to examine a joint in a systematic way which will warm the heart of an examiner.
The three subjects rheumatology, orthopaedics and trauma comple-ment each other really well. If you are still a little shy with patients
and want to build up your competence and confi dence, then the rheu-matology ward is for you. The patients are delightful, the diseases a cornucopia of fascinating physical signs, the staff are true problem solvers and the treatments are at the cutting edge of modern science, and they work! Orthopaedics is very logical and has big simple opera-tions which transform a patient ’ s quality of life. If you need an adrena-line burst, then the trauma room is for you. There, life - saving decisions have to be taken quickly and boldly. No place for the faint - hearted! This book gives you all you need to know to step boldly into any of these three worlds.
A short section at the end provides you with some clinical cases to test your teeth on. These are the sort of questions that you will face at fi nals.
Our thanks must go to Jane Fallows and Roger Hulley for illustra-tions which throw life and clarity onto the concepts we so clumsily describe in the text, and to Elizabeth Bishop and Laura Murphy for steering the project through in a relaxed but timely way. Enjoy!

Guide to anatomical terminology 7
Guide to anatomical terminology
Some anatomical terminology
Coronalplane
Foot extended(dorsiflexed)
Foot flexed(plantar flexed)
Sagittalplanes
Medianplane
Leg mediallyrotated
Leglaterallyrotated
Medialside
Lateralside
Fingersadducted
Varus
Valgus
Forearmsupinated
Elbowextended
Armadducted
Arm abducted andlaterally rotated
Elbow flexed
Forearmpronated
Proximal
Distal
Supinate
Pronate
Fore foot InvertHind foot
Evert
Fingersabducted

Rheumatology, Orthopaedics and Trauma at a Glance, Second Edition. Catherine Swales, Christopher Bulstrode. © 2012 John Wiley & Sons, Ltd.
8 Published 2012 by John Wiley & Sons, Ltd.
Musculoskeletal s tructure and f unction
1
Cl–H+MMP
Sealingzone
Bone
Resorptive lacunae within ruffled zone
z disc m line
Sarcomere–contractile unit
A bandActin myofilaments
z disc
Low pH/proteolytic enzymes
Bone resorption by osteoclasts
ATPHCO3
–
Cl–ADP + Pi Trabecular/spongy bone
Structure of bone unit
Motor unit Muscle unit
Osteoclast
Structure of long bone
Cortical bone
Trabeculae of bone surroundingmarrow
Collection ofHaversian (osteon) units
Motorneuron
Muscle fibrecontainingmyofibril
Myosin myofilamentscontaining globular heads
Synapses
Haversiancanal – bloodvessels
Canaliculi – route throughmatrix
Lamellaeof matrix
Articular cartilage
Lacunae containingosteocytes
Epiphyseal lineSpongy bone
Medullarycavity
Metaphysis
Metaphysis
Diaphysis
Epiphysis
Epiphysis

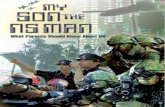
Musculoskeletal structure and function Introduction 9
The locomotor system is composed of bone, cartilage, muscle, tendons and ligaments.
Bone Bone is essentially a mineralised connective tissue. It is comprised of two subtypes: 1 Woven bone is formed when bone is laid down rapidly, as in the developing foetus, healing fractures or bone - forming tumours. 2 Lamellar bone is laid down slowly. It is structurally strong and forms the adult skeleton. It is arranged in two forms:
• Cortical or compact bone comprises 80% of the skeleton, accounting for most of the shafts of long bones. It is formed by Haversian systems: rings of collagen and matrix containing central blood vessels and lining cells called osteocytes. • Trabecular or medullary bone is found in contact with bone marrow cells between the cortices, at the end of long bones and in vertebral bodies. In trabecular bone the collagen and matrix run as sheets (lamellae) parallel to the bone surface.
The three main cell types in bone are: 1 Osteoblasts ( ‘ builders ’ ) are responsible for bone formation by forming organised lamellae of mineralised matrix and collagen. Osteoblasts lie in sheets on the surface of bone trabeculae and their activity is closely coupled to osteoclasts. 2 Osteoclasts ( ‘ cutters ’ ) resorb bone. These giant multinucleated cells migrate across bone, settle on an area to be resorbed and the plasma membrane adjacent to the bone surface becomes a ‘ ruffl ed border ’ . Secretion of proteolytic enzymes (e.g. matrix metalloprotei-nases, MMP) and hydrochloric acid onto the bone surface remove mineral and matrix simultaneously. 3 Osteocytes are mature, relatively inactive osteoblasts that lie in lacunae within bone. Osteoblasts and osteoclasts are coupled into bone remodelling units that keep adult bone mass relatively constant.
See Chapter 31 ‘ Disorders of Bone Metabolism ’ for more details of osteoclast/osteoblast cell biology.
Bone is covered in a vascular membrane (the periosteum) which is a major source of blood supply to the bone (the other supply is derived from perforating vessels which then run up in the medulla). The peri-osteum is helpful when reducing fractures, as it is often partly intact and can be used to guide the broken frgments together. The periosteum is also important in fracture healing, supplying cells which ‘ organise the haematoma ’ around the fracture site (see below).
The protein matrix of bone consists largely of type I collagen. Osteoblasts lay down triple helices of type I collagen into organised lamellae containing unmineralised matrix (osteoid). The tensile strength of bone is increased by covalent bonds between collagen sheets; rigidity is conferred by mineralisation of bone matrix, with deposition of hydroxyapatite crystals between the lamellae.
Bone remodelling occurs throughout life to repair damaged bone. Alternating cycles of recruitment, differentiation and activation of osteoclasts and osteoblasts maintain the structural integrity of bone throughout life; with advancing age however, bone loss exceeds for-mation. Vigorous bone remodelling follows fracture in 5 stages: 1 – Clot or haematoma formation from bleeding vessels within bone. 2 – Organisation and recruitment of new populations of osteoblasts. 3 – Callus formation from new osteoid and woven bone formation. 4 – Modelling by osteoblasts/clasts transforms woven to lamellar bone. 5 – Remodelling strengthens bone in direction of maximal stress.
Movement stimulates this process, so rigid fi xing of fractures with plates prevents callus formation, and healing occurs more slowly on the background of standard bone remodelling. Bone is unique in its ability to heal without scar formation.
Bone increasese its circumference by the generation of new bone immediately under the periosteum, but length increases at epiphyseal growth plates. These are cartilage plates with their own blood supply which lie between the epiphysis (end of the bone) and the metaphysis , the part of the bone which connects with the diaphysis (shaft of the bone). These epiphyseal plates are weaker than the surrounding bone and therefore fractures in growing skeletons tend to occur at this site. If the fracture affects the blood supply or the anatomy of the growth plate then development may be affected.
Cartilage Cartilage is composed of chondrocytes and chondroblasts , which create a matrix of type II collagen , and proteoglycans to bind water. Adult cartilage consists of four layers – the superfi cial, middle, deep and calcifi ed zones, which differ in pattern of collagen fi bre deposi-tion, and water and cell content. Articular (hyaline) cartilage is an avascular and aneural shock absorber. It covers articular surfaces and allows friction - free movement of joints. Fibrocartilage forms the menisci and intervertebral discs.
Cartilage is lost either through mechanical degeneration at points of load - bearing (in osteoarthritis) or through resorption in an infl amed joint (in rheumatoid arthritis) or both. As cartilage contains no blood vessels, it heals slowly if damaged.
Muscle Muscle is formed by fi bres that differ according to their twitch rate and fatiguability. • Type 1 muscle fi bres are slow twitch (red) fi bres that are highly resistant to fatigue. They have abundant mitochondria and are designed to maintain sustained contractions such as needed in posture control. • Type 2 muscle fi bres are fast twitch (white) fi bres and are designed to produce greater force and rapidity of contraction but fatigue rapidly.
Fibres of similar types group together with a lower motor neuron to form a motor unit . Muscle fi bres contain myofi brils formed by the contractile myofi laments actin and myosin . The myosin - binding sites on actin are covered by tropomyosin and troponin. However, when an action potential reaches a motor unit, stimulation causes calcium release into the surrounding cytoplasm (sarcoplasm). The calcium binds with troponin sites on tropomyosin, revealing the active binding sites and disinhibiting actin fi laments. These cross - link with the globu-lar heads on myosin, causing shortening of the motor unit. The muscle relaxes once calcium levels fall and the cross - links are broken.
Tendons and l igaments Both of these specialised connective tissues are composed of type I collagen. Tendons attach muscle to bone, while ligaments connect bones to one another, supplying support to a joint.
Nerves Nerves are arranged in a segmental fashion, one pair at each level. The sensory nerves enter dorsally, supplying sensory information from a stereotyped strip of skin (dermatome). The motor root exits ventrally; a myotome is the motor equivalent of a dermatome i.e. the muscles served by a single nerve root.
Knowledge of the nerve roots is very useful in determining the site and level of injury in the nervous system.

Calcium h omeostasis and b one m etabolism 2
The b asics The skeleton is more than a structural framework. During constant cycles of bone formation and resorption, it plays a vital role in calcium homeostasis. Calcium is the most abundant mineral in the body and 99% of it is contained in bone. Half of plasma calcium is bound to albumin and is therefore inactive. Calcium results must be adjusted to account for albumin levels by adding or subtracting 0.02 mmol/l for each g/l by which the albumin is below or above 40 g/l, respectively.
Calcium homeostasis and bone metabolism are principally gov-erned by vitamin D and parathyroid hormone . Bone metabolism is
also modulated by calcitonin, glucocorticoids, sex hormones, growth hormone and thyroxine. See Chapter 31 ‘ Disorders of bone metabo-lism ’ for a description of osteomalacia, rickets and Paget ’ s disease; also see Chapter 30 ‘ Osteoporosis ’ .
Vitamin D This fat - soluble vitamin is found in the diet and its precursors are also generated in the skin in response to sunlight. Following renal and hepatic hydroxylation, the active component 1,25 - dihydroxy - D 3 is released. Its actions are:
Ca PO4
Cholecalciferol D3
Diet UV light on skin
Increases renalhydroxylation of
vitamin Dprecursors
Suppressesrelease
QT interval
25(OH)D3
Liver
Kidney24, 25(OH)2D3(inactive)
Depression, thirst,abdominal pain, nausea,constipation, renal stones
'Bones, stones, groans and moans'
Malignancy
1°/3° hyper PTHSarcoidosis
Rehydration, bisphosphonates, frusemide
Myeloma
Bony deposits
PTHrP
Depression, paraesthesia
Facial twitching when facial nervetapped – Chvostek's sign
Flexion wrist and fingers withocclusion of brachial artery – Trousseau's sign
1, 25(OH)2D3(active)
Hypercalcaemia Hypocalcaemia
Ca PO4
Parathyroidhormone
Vitamin D
Renal Ca absorption PO4 excretion
Bone resorption
QT interval
Gut Ca absorption
Bone resorption
Gut Ca absorption
Causes
Treatment
Hypo PTHPseudohypo PTHChronic renal failurePancreatitis
Ca supplementation
Causes
Treatment
Rheumatology, Orthopaedics and Trauma at a Glance, Second Edition. Catherine Swales, Christopher Bulstrode. © 2012 John Wiley & Sons, Ltd.
10 Published 2012 by John Wiley & Sons, Ltd.

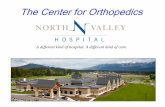
Calcium homeostasis and bone metabolism Introduction 11
• Gut: increases calcium absorption from the small bowel. • Bone: increases mineralisation and resorption.
Parathyroid h ormone Parathyroid hormone (PTH) is released in response to low plasma calcium levels. Its overall function is to increase plasma calcium and decrease plasma phosphate levels via actions on the gut, bone and renal tract: • Gut: increases intestinal absorption of calcium. • Bone: increases osteoclastic resorption of bone. • Renal: increases calcium reabsorption and phosphate excretion; increases renal hydroxylation of vitamin D precursors. Vitamin D and PTH levels are interlinked: PTH responds to low levels of vitamin D by increasing renal hydroxylation of vitamin D precur-sors into the active form; high levels of vitamin D feedback to inhibit PTH release.
Disorders of c alcium h omeostasis Hypercalcaemia Elevated calcium levels can cause abdominal pain, nausea, constipa-tion, polyuria, depression and renal stones. They shorten the Q - T interval. The most common cause is malignancy (myeloma, bony metastases, PTH - related protein release from some tumours) or primary hyperparathyroidism. Treatment is with rehydration and frusemide or bisphosphonates.
Hypocalcaemia The main symptoms of hypocalcaemia are depression and paraesthe-sia. Obstruction of the brachial artery causes carpopedal spasm (Trousseau ’ s sign) and tapping the facial nerve causes the facial muscles to twitch (Chvostek ’ s sign). The Q - T interval is prolonged. Causes include (pseudo)hypoparathyroidism, chronic renal failure or pancreatitis. Treatment is with calcium supplementation and reversal of the underlying cause.
Hyperparathyroidism Primary h yperparathyroidism Inappropriate production of PTH in the presence of a raised calcium level. Most commonly due to a single adenoma but carcinoma and
hyperplasia may also be responsible. It causes the symptoms of hyper-calcaemia as discussed above and biochemical testing reveals a raised calcium, unsuppressed PTH (i.e. normal or high plasma level), reduced phosphate and elevated alkaline phosphatase. There may be radiologi-cal evidence of bone resorption (brown tumours, pepper - pot skull). Treatment is surgical.
Secondary h yperparathyroidism Appropriate production of PTH in the presence of a low calcium level. The most likely cause is chronic renal failure.
Tertiary h yperparathyroidism Inappropriate and autonomous production of PTH following pro-longed secondary hyperparathyroidism. Calcium is elevated, and treat-ment is as for primary disease.
Hypoparathyroidism Primary h ypoparathyroidism Reduced PTH secretion due to autoimmune destruction of the parathy-roid glands or their surgical removal. It causes symptoms of hypocal-caemia. Calcium is reduced, phosphate elevated and alkaline phosphatase normal. Treatment is with alfacalcidol.
Pseudohypoparathyroidism Similar symptoms and treatment to primary condition, but aetiology is due to end - organ resistance to PTH, so hormone levels may rise. Additional features include a round face and short metacarpals/tarsals.
Pseudopseudohypoparathyroidism Phenotypic appearance of pseudohypoparathyroidism but normal endocrine and biochemical features.