Rheumatoid Arthritis(RA)
30
Rheumatoid Arthritis(RA) Dr. Gehan Mohamed
description
Rheumatoid Arthritis(RA). Dr. Gehan Mohamed. Learning objectives:. At the end of this lecture the student should be able to : understand definition,genetic predisposition of RA. Discuss pathophysiology, clinical features of RA. - PowerPoint PPT Presentation
Transcript of Rheumatoid Arthritis(RA)

Rheumatoid Arthritis(RA)
Dr. Gehan Mohamed

Learning objectives: At the end of this lecture the student should be able
to : understand definition,genetic predisposition of RA. Discuss pathophysiology, clinical features of RA. Identify Diagnostic Criteria ,Laboratory Features and
bad prognostic Features of Rheumatoid Arthritis.

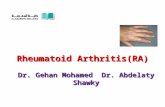
RA Systemic inflammatory autoimmune
disorder Age incidence : 40-70 years of age

Genetics
Patients which have HLA-DRB have Increased risk for : RA development. Increased joint damage Increased joint need for surgery

Pathophysiology

Role of Immunolog in RA Macrophages:
Produce cytokines Cytokines (TNF-α) cause
systemic features Release chemokines recruit
PMNs into synovial fluid/membrane
TNF-α & IL-1: Proliferation of T cells Activation of B cells Initiates proinflammatory/joint-
damaging processes
TH-1 cells: Mediate disease processes Activate B cells
B cells: Release cytokines Plasma cells that produce
Ab
Osteoclasts induce: Bone erosion Juxta-articular & Systemic
osteoporosis

Pathophysiology Swelling of Synovial lining
Angiogenesis
Pannus formation in form of : Synovial thickening/hyperplasia Inflammatory vascularized tissue Generation of Metalloproteinases
Cytokine release Infiltration of leukocytes Change in cell-surface adhesion molecules & cytokines Destruction of bone & cartilage

Sequence of events : Proliferation of synovial membrane
cells with inflammatory cell infiltrate Destruction of joints Disability

Diagnosis:1- clinical criteria2- investigations

1- Diagnostic Criteria Symmetric peripheral polyarthritis Morning Stiffness >1 hour Extraarticular manifestations Rheumatoid nodules

Symmetric Peripheral Polyarthritis 3 or more Joints for >6 weeks Intermittent or Migratory involvement
Small Joints Hands & Feet Peripheral to Proximal
Leads to Deformity & Destruction of Joints Erosion of cartilage and bone

Stiffness Morning or after Prolonged Inactivity Bilateral > 1 hours
Reflects severe joint inflammation Better with movement Pain with pressure to joint Pain with movement of joint Swelling due to hypertrophy of synovium Effusion Hottness Redness

Physical Exam Decreased grip strength Carpal tunnel syndrome(condition
characterized by pain and numbing or tingling sensations in the hand and caused by compression of a nerve in the carpal tunnel at the wrist.
Ulnar deviation Boutonniere/Swan neck deformities Extensor tendon rupture


Extraarticular Involvement Myalgia, fatigue,
low-grade fever, weight loss, depression.
Anemia Rheumatoid nodules Pleuropericarditis Neuropathy
Scleritis Splenomegaly Vasculitis

Rheumatoid Nodules Extensor surfaces
elbows Very Specific Only occur in ~30% Late in Disease

Investigations

Arthrocentesis Confirm diagnoses Differentiate between inflammatory & noninflammatory Labs:
White blood cell count if WBC >2000/µL indicates inflammatory arthritis
Gram stain & Culture
Arthroscopy Evaluate ligamentous & cartilaginous integrity Biopsy Infection: aspirate thick

Rheumatoid arthritis : showing inflammatory cell infiltrate in the synovium

Laboratory Features Rhumatoid Factor
70-80% of pts. - Lab manifestations up to 10 years before clinical - IgM or IgG - If IgM+ve : more severe disease & poorer
outcome. Overlap with Hepatitis C Virus.
Acute Phase reactants ESR, CRP monitoring disease activity

Radiology Evaluate disease activity & joint
damage Bony decalcification

Radiological Studies Plain Films
Bilateral hands & feet
Color Doppler U/S & MRI Early signs of damage i.e. Erosions Bone Edema - even with normal findings on
radiography



DiseaseSeverity

Arthralgias >3 inflamed joints Mild functional limitation Minimally elevated ESR & CRP No erosions/cartilage loss No extraarticular disease
Mild Disease

Moderate Disease 6-20 Inflamed joints Moderate functional limitation Elevated ESR/CRP Radiographic evidence of
inflammation No extraarticular disease

Severe Disease >20 persistently inflamed joints Rapid decline in functional capacity Radiographic evidence of rapid
progession of bony erosions & loss of cartilage
Extraarticular disease

bad prognostic Features RF +ve Early development of multiple inflamed joints
and joint erosions Severe functional limitation Female HLA epitope presence Lower socioeconomic status & Less education Persistent joint inflammation for >12 weeks

Differential diagnosis of arthritis
Seronegative polyarthritis Psoriatic arthritis Osteoarthritis SLE Paraneoplastic syndrome Crystal-induced arthritis
Tophaceous gout Pseudogout