Rhabdomyosarcoma of the Buttock Producing Hypoglycemia
9
Rhabdomyosarcoma of the Buttock Producing Hypoglycemia ANAXAGORAS N. PAPAIOANNOU,** M.D., CHARLES J. MCPEAK, M.D. From the Department of Surgery of Memorial Sloan-Kettering Cancer Center, New York TwO EXTRAPANCREATIC neoplasms pro- ducing hypoglycemia were first reported in 19302,18 and several others before 1955.5 12, 29, 34, 50, 57, 64, 65 Since then, this syndrome has been recognized and reported with considerable frequency. Nevertheless, de- spite intensive study in this area in the last few years, the exact mechanism of hypo- glycemia associated with these tumors still remains unclear and the etiology of the syndrome intriguing. Curiously, only two reports on this subject have appeared in the American surgical literature. This study was undertaken with the fol- lowing objectives: 1) to present one such case which is interesting because of its his- tologic appearance as rhabdomyosarcoma and its anatomic origin in the buttock, a combination never to our knowledge previ- ously reported; 2) to review the status of present knowledge concerning this interest- ing disorder; and 3) to discuss the basic aspects of study and management of these cases. Case Report A 24-year-old white woman was admitted to Memorial Hospital on February 18, 1963. Her his- tory began with pain in her left buttock in April, 1962. In July, 1962 this painful area was surgically explored at another institution and a "lipoma" overlying the gluteal fascia was found and excised. The pain apparently subsided for a while only to reappear along with gradual swelling of the but- tock in October, 1962. Three months later a new exploration of the painful and now bulging area revealed a diffusely infiltrating tumor which was considered unresectable and the patient was re- ferred to Memorial Hospital. About five days before admission to Memorial Hospital her mental status began to change and she was becoming alternatingly drowsy and de- lirious with visual hallucinations. Her state of con- sciousness gradually decreased until she became deeply and constantly confused. On admission she was comatose, had a huge tumor and draining sinuses in the left buttock, and was in the sixth month of her fourth pregnancy with a live fetus. Although most of her neurologic findings could be explained on the basis of toxic encephalopathy, there was also evidence of a left cerebral focus. Because of pyogenic focus in the buttock, the possibility of brain abscess was also considered. Emergency laboratory tests on admis- sion revealed: blood sugar 50 mg. %o; blood urea nitrogen (BUN) 33.2 mg. %; and normal electro- lytes. The blood sugar was subsequently reported as low as 28 mg. %. Lumbar puncture (LP) revealed slightly xan- thochromic fluid with normal pressure and cell count, proteins 20 mg. %, chlorides 114 mEq./L., and glucose 46 mg. %. (The LP was performed while hypertonic dextrose was being infused.) The slight xanthochromia was subsequently at- tributed to jaundice that became clinically mani- fest a few days later. With the working diagnosis of hypoglycemia- producing tumor and in view of her poor overall status, treatment was initiated with small doses of radiation therapy (RT) to the tumor. Elaborate measures were undertaken to limit scattered radia- tion to the fetus insofar as possible. The estimated dose to the fetus was less than 3%o of the tumor dose. After the second treatment (250 r in air, 158 r tumor dose) a live baby girl was spontane- ously delivered. The premature baby gasped a few times but died despite resuscitative efforts. The night of delivery, deep coma and hypo- tension developed and did not respond to ad- ministration of blood, but were partially corrected with 50%'o dextrose in water intravenously. The day following delivery, the patient's overall status began to improve. RT was liberally administered and the tumor responded satisfactorily to 2,325 r 553 * Submitted for publication April 25, 1964. ** Present address: Department of Surgery, Bronx Municipal Hospital Center, 1N48 Jacob, Bronx, N. Y.
Transcript of Rhabdomyosarcoma of the Buttock Producing Hypoglycemia

Rhabdomyosarcoma of the Buttock Producing Hypoglycemia
ANAXAGORAS N. PAPAIOANNOU,** M.D., CHARLES J. MCPEAK, M.D.
From the Department of Surgery of Memorial Sloan-Kettering Cancer Center,New York
TwO EXTRAPANCREATIC neoplasms pro-ducing hypoglycemia were first reported in19302,18 and several others before 1955.5 12,29, 34, 50, 57, 64, 65 Since then, this syndromehas been recognized and reported withconsiderable frequency. Nevertheless, de-spite intensive study in this area in the lastfew years, the exact mechanism of hypo-glycemia associated with these tumors stillremains unclear and the etiology of thesyndrome intriguing. Curiously, only tworeports on this subject have appeared inthe American surgical literature.
This study was undertaken with the fol-lowing objectives: 1) to present one suchcase which is interesting because of its his-tologic appearance as rhabdomyosarcomaand its anatomic origin in the buttock, acombination never to our knowledge previ-ously reported; 2) to review the status ofpresent knowledge concerning this interest-ing disorder; and 3) to discuss the basicaspects of study and management of thesecases.
Case Report
A 24-year-old white woman was admitted toMemorial Hospital on February 18, 1963. Her his-tory began with pain in her left buttock in April,1962. In July, 1962 this painful area was surgicallyexplored at another institution and a "lipoma"overlying the gluteal fascia was found and excised.The pain apparently subsided for a while only toreappear along with gradual swelling of the but-tock in October, 1962. Three months later a newexploration of the painful and now bulging arearevealed a diffusely infiltrating tumor which was
considered unresectable and the patient was re-ferred to Memorial Hospital.
About five days before admission to MemorialHospital her mental status began to change andshe was becoming alternatingly drowsy and de-lirious with visual hallucinations. Her state of con-sciousness gradually decreased until she becamedeeply and constantly confused.
On admission she was comatose, had a hugetumor and draining sinuses in the left buttock, andwas in the sixth month of her fourth pregnancywith a live fetus. Although most of her neurologicfindings could be explained on the basis of toxicencephalopathy, there was also evidence of a leftcerebral focus. Because of pyogenic focus in thebuttock, the possibility of brain abscess was alsoconsidered. Emergency laboratory tests on admis-sion revealed: blood sugar 50 mg. %o; blood ureanitrogen (BUN) 33.2 mg. %; and normal electro-lytes. The blood sugar was subsequently reportedas low as 28 mg. %.
Lumbar puncture (LP) revealed slightly xan-thochromic fluid with normal pressure and cellcount, proteins 20 mg. %, chlorides 114 mEq./L.,and glucose 46 mg. %. (The LP was performedwhile hypertonic dextrose was being infused.)The slight xanthochromia was subsequently at-tributed to jaundice that became clinically mani-fest a few days later.
With the working diagnosis of hypoglycemia-producing tumor and in view of her poor overallstatus, treatment was initiated with small dosesof radiation therapy (RT) to the tumor. Elaboratemeasures were undertaken to limit scattered radia-tion to the fetus insofar as possible. The estimateddose to the fetus was less than 3%o of the tumordose. After the second treatment (250 r in air,158 r tumor dose) a live baby girl was spontane-ously delivered. The premature baby gasped a fewtimes but died despite resuscitative efforts.
The night of delivery, deep coma and hypo-tension developed and did not respond to ad-ministration of blood, but were partially correctedwith 50%'o dextrose in water intravenously. Theday following delivery, the patient's overall statusbegan to improve. RT was liberally administeredand the tumor responded satisfactorily to 2,325 r
553
* Submitted for publication April 25, 1964.** Present address: Department of Surgery,
Bronx Municipal Hospital Center, 1N48 Jacob,Bronx, N. Y.

PAPAIOANNOU AND MC PEAK Annals of SurgeryApril 1965
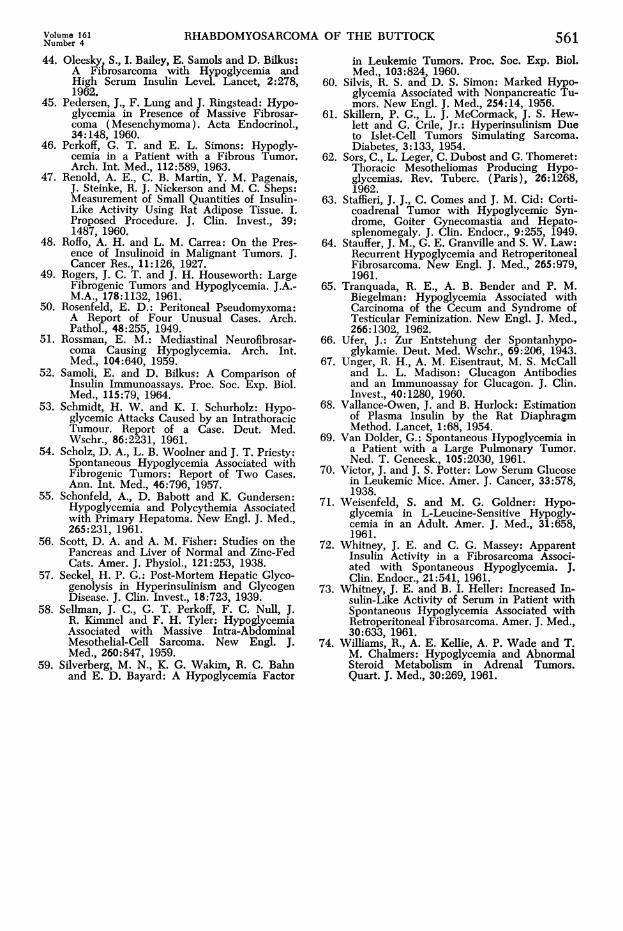
FIG. 1. High power photomicro-graph of the tumor from resectedspecimen. Faint cytoplasmic striationsare present in few cells at the rightupper corner (Arrows).
in air (1,545 tumor dose) over an 8-day period.As the tumor was undergoing necrosis and shrink-age, the demands of intravenous hypertonic dex-trose decreased and the state of consciousness was
gradually restored to normal.For the management of hypoglycemia, in ad-
dition to the intravenous hypertonic dextrose,glucagon was used but discontinued because ofallergic skin reaction. Corticosteroids were alsoadministered, but it was felt that the major benefithad been derived from radiation therapy.
Three days after delivery, she was taking sixfeedings of high carbohydrate diet, and she main-tained a fasting blood sugar of 74-103 mg. %
without intravenous dextrose. Jaundice also de-veloped with peak total bilirubin value of 6.62mg. %, (direct 2.58 mg. %S) on the day of de-livery, but this abated in 4 days (total bilirubin1.03 mg. %,).
Azotemia, present since admission, reached itspeak the day following delivery with BUN of 75mg.%, but came down to 23.2 mg. %o 7 dayslater. During the period of azotemia, serum calciumwas 10.2 mg. %o and phosphorus 8.6%. Thesetests were not repeated.
On March 8, 1963 left hemipelvectomy was
performed including subtotal vaginectomy and ex-
cision of the entire left buttock. The procedure was
attended by considerable bleeding attributed to therecent pregnancy, the vascularity of the tumor andthe preoperative radiation therapy.
Toward the end of the resection, hypotensiondeveloped leading to cardiac standstill. Resuscita-tion initially achieved by closed cardiac massagewas later continued by open massage. The patientremained in extremely poor condition, unrespon-
sive, with dilated pupils, unable to maintain spon-
taneou5 breathing without the use of the respirator.
Bleeding tendency, associated with increased fi-brinolytic activity, responded somewhat to theintravenous administration of epsilon amino caproicacid. The patient died 2 hours after the completionof the operation.
At autopsy, the tumor was found to be a fullymalignant rhabdomyosarcoma (Fig. 1) growing inmicroscopic sheets along the sacrum and beyondthe midline. Of interest were the extensive meta-static calcifications of the alveolar septi of thelungs, and metastatic nephrocalcinosis. The para-
thyroid glands could not be identified. The pan-creas showed slight interstitial pancreatitis, but noevidence of tumor on multiple sections. The brainwas not examined. Gomori's 24 hematoxylin-phlox-ine stain for beta-cell cytoplasmic granules doneon sections of the tumor were negative. Tumorassays * showed: 1) Insulin immunoassay (Ber-son-Yallow9 = 141 U/Gm. of wet weight (notelevated); 2) Insulin-like activity (Vallence-Owen) 68 = 2.5 U/Gm. of tumor (not elevated);3) Glucagon (Unger-Eisentraut) 67 = 11 mg./Gm.of wet weight (slightly elevated, but not sig-nificant).
Autopsy of the baby revealed a premature(2,220 Gm.) but normally developed baby girl.Gross and microscopic examination of all endocrineorgans revealed no abnormalities. There was bi-lateral intraventricular cerebral hemorrhage.
DiscussionLowbeer 36 in 1961 collected 48 cases of
these tumors, 23 of which were of epithelial
* We are indebted to Dr. R. H. Unger of theVeteran's Administration Hospital in Dallas, Texasfor performing the tumor assays.
554

RHABDOMYOSARCOMA OF THE BUTTOCK 555TABLE 1. Extrapancreatic ncoplas;ns associated szwitIi hypoglycemia and other endocrine distnrbanccs
Age Histologic Associated enidocrineSenior Autlhor Sex Site of Tumor Diagnosis disturbances Results
Lawrence34 24 Adrenal Adrenal carcinoma Amenorrhea, breast, atrophy, Died 2 years after ex-
Broster:2
Staffieri63
Makotta38
Makotta38
Howard30
Meyer-Hofmann45
Willianms79
Adrenal carcinoma
Sarcomatous, dys-embryoplasia
Fibrosarcoma
Fibroma
Hemangiopericytoma
Seminoma or dys-germinoma
Adrenocortical carci-noma
estrogen deficiency
Menses never appeared. Hir-sutism, deep voice for 18 mo.
Goiter, gynecomastia
ploration
Died 4 years after oper-ation
No available followup
Goiter, alpha islet cell hyper- Died in hypoglycemicplasia coma
Goiter, hypertrophy of adeno- Died in hypoglycemiahypophysis and adrenal cortex coma
Hirsutism, decreased urinary 4 recurrences and even-gonadotropins and ketoste- tual death with he-oids, increased estrogens patic metastases 10
Goiter, acromegaly, focal in-crease of eosinophilic pitu-itary cells, widening of zonafesciculata of adrenal cortex,lobular breast proliferation
Increased 17-ketosteroids and1 7-hydroxysteroids, perinu-clear hyalinization of basophiland increased activity of acido-philic pituitary cells. Hypo-gonadism
years after initial oper-ation
Died in hypoglycemiccoma
Died in hypoglycemiccoma
Adenocarcinoma ofthe cecum
Testicular feminization, low Died in hypoglycemicurinary steroids, Leydig cell comaadenoma
Case reported herein 24 ButtockF
Rhabdomyosarcoma Pregnancy, metastatic nephro-calcinosis, pulmonary alveolarcalcification, hyperphosphate-mia
Died 2 hours after oper-
ation from uncon-
trolled hemorrhage.
and 25 of mesodermal origin. To our knowl-edge, 35 ** have been reported in additionto those collected by Lowbeer, thus bring-ing the total up to 83. There was no sex
preponderance. The ages of the patientsranged from 141/2 to 82 years and the pre-senting symptoms were usually mental dys-function ranging from mild personalitychanges and amnesia to frank irrationalityand coma. Many of these patients wereinitially considered psychotic and somewere admitted for psychiatric care.The majority of tumors were of meso-
dermal origin, a smaller group ectodermal
0* 8, 10, 11, 16, 19, 21-23, 25, 27, 28, 32, 33,
35, 37, 40, 43-36, 49, 51, 53, 55, 62, 63, 65, 66,
69, 72-74.
and a few 25,65 endodermal. The most com-
mon histologic structure described was
fibrosarcoma, although a variety of othertypes such as hepatoma, mesothelioma, lipo-sarcoma, neurofibroma, spindle cell sar-
coma, hemangiopericytoma, adrenal car-
cinoma, pseudomyxoma peritonei, adeno-carcinoma, and leiomyosarcoma were alsofound. The most common location was theretroperitoneal space, followed by the tho-racic cavity. One case originated from thececum,65 two others 25 from the stomach,one from the urinary bladder37 and ours
from the left buttock.The degree of malignancy varied widely
and seemed to be related to that charac-
teristic of the histologic pattern present in
Volume 161Number 4
F
14 AdrenalF
25 RetroperM
62 MediastiF pleura
55 MediastiF pleura
1 7 RetropeF
ritoneum
inal
inal
ritoneum
36 OvaryF
48 AdrenalM
Tranquada65 65 PelvisF

556 PAPAIOANNOU AND MC PEAK
each case. The gravity of coexisting hypo-glycemia was associated with size but boreno relationship to aggressiveness of thetumor, although in a few instances boutsof hypoglycemia were lethal. Ten patientsshowed evidence of another associated en-docrine problem (Table 1). It is of interestthat four had had colloid goiter and thatin three, histologic evidence of anteriorpituitary dysfunction was present. In manycase reports, however, usually no postmor-tem findings were described and in some,it was not clear whether or not the pituitarywas examined.Although no definite association between
hypoglycemia and other endocrine disturb-ances can be deduced from available evi-dence, the incidence (10:84) is sufficientlygreat to warrant continued interest andmore thorough study of cases in the future,with special attention to the pituitary.The large size of these tumors was always
the single outstanding feature common inall cases. Also the glucose tolerance test incases studied was invariably abnormal, bothbefore and after operation. Before opera-tion there was early flattening of the curve,indicating rapid peripheral utilization ofglucose; after operation, if the tumor wassuccessfully removed, there developed adiabetic type of curve f', 11 72 which gradu-ally returned to normal, usually after 10days, indicating restitution of depressedislet cell function. A similar phenomenonis known to occur after removal of func-tioning islet cell adenomas.'7 It is interest-ing that of the 83 cases reported, onlythree 18, 47 appeared in the American sur-gical literature in 1930 and none since.Mechanism of Associated Hypoglyce-
mia. Although most of the theories ad-vanced to explain the mechanism of hypo-glycemia are postulates not necessarilybased on sound cause and effect relation-ship or objective supportive evidence, abrief historical account of each will begiven in the chronologic order in whichthe theories appear in the literature.
Annals of SurgeryApril 1965
1) Interference with the cerebral circula-tion (1930).'18
2) Mechanical action of the tumor on thesplenchic nerve and ganglia (1939 ) .57
3) Glucose hunger (1943 ) .294) Adrenocortical insufficiency (1949).645) Origin from ectopic islet cell tissue
(1954).616) Pressure on autonomic neuroreceptors
of the liver (1956) .67) Secretion of insulinase inhibitor
(1957). 54
8) Production of insulin-like substance(1958 ).69) Inhibition of hepatic insulinase; tumor
production of material stimulating insulinsecretion by the pancreas (1959 ) .58
10) Dissociation of the normally protein-bound insulin by the tumor (1963).1
Theories 1, 2, 4 and 6 obviously cannotbe considered as unifying theories and willnot be discussed further. In Theories 7 and9, intact or increased inlet-cell activity isimplied. Although this is theorectically pos-sible, it is unlikely in view of the fact thatthe previously mentioned transient post-operative diabetic-type curve on the glucosetolerance test indicates pancreatic hypo-function during the presence and followingremoval of the offending tumor.
In Theory 5, Skillern, reporting twocases, suggested that these may actually beislet-cell tumors originating from ectopicpancreatic tissue, histologically simulatingspindle cell sarcoma, but retaining theability to secrete insulin. Sections of oneof their specimens stained by Gomori'shematoxylin-phloxin technic showed an oc-casional round cell containing blue cyto-plasmic granules, thus indicating similaritywith beta islet cells. However, functioningislet-cell tumors arising from ectopic pan-creatic tissue were found in only six pa-tients by Barbosa and his colleagues 7 intheir extensive review of the literature, andin all six the tumors were small and locatedin the upper abdomen. In any event, thesignificance of Gomori stain has been ques-

RHABDOMYOSARCOMA OF THE BUTTOCK
tioned," since mast cells in such tumorscan also take up the stain.One case of functioning islet-cell car-
cinoma metastasizing as spindle cell tumorsubsequently reported by Karsh 32 lent in-direct support to Skillern's hypothesis. InKarsh's case, however, the metastatic cells,although morphologically different, retainedthe distinct staining characteristics of betacells; in many subsequently reported cases
the pancreas was carefully sectioned, andon no occasion was islet-cell tumor un-
covered.Theory 10 is based on the recent evi-
dence that in the fasting state, insulin cir-culates in a complex form combined withprotein, the binding process being catalyzedmost likely in the liver.8 The insulin com-
plex is subsequently dissociated by fibro-areolar tissue and other dissociating fac-tors,4 and the "free" insulin then exerts itsmetabolic effects. It is postulated that fibro-sarcomas may act as "dissociating factors"much as does fibro-areolar tissue to whichthey are closely allied. Here again, it is im-plied that the pancreas is primarily respon-sible for the production of insulin itself,and this is not consistent with the view thatthe pancreas actually hypofunctions bothduring and for a short time after removalof these tumors.The overwhelming majority of evidence
favors the glucose utilization by the tumor(Theory 3) and the tumor production ofinsulin-like substance (Theory 8).The glycolytic activity and lactic acid
production of tumors has been known sincethe work of Cori in 1925.14 Experimentally,severe hypoglycemia has been produced byinjecting extract of spindle cell sarcoma ofwhite rats in rabbits 48; it has also been ob-served in strain C58 mice with lymphaticleukemia 70 and in AKR mice inoculatedwith leukemic tumor BW5147.59
Active glucose uptake was demonstratedin a human fibrosarcoma by incubatingfresh tumor slices in buffered glucose solu-tion,46 and insulin-like activity was shown
to exist in tumor extracts that stimulatedglucose uptake by the rat epididymal fatpad,78 the rat diaphgram,41 .46 or both.65
Insulin-like activity in vitro was alsodemonstrated by the ability of tumor toform glycogen from C14-labeled glucose,an action which is considered to be a more
specific activity of insulin." This activitywas largely negated by specific anti-beefinsulin antibody of the guinea pig and byN-ethylimaleimide, a sulfhiydryl inhibitor."1Similar sulfhydryl-containing proteins were
also found in abundance in another fibro-sarcoma recently reported.35Whereas no insulin activity has ever been
demonstrated in tissue extracts by immuno-assay there has been, to our knowledge, a
single reported case of fibrosarcoma withincreased plasma insulin activity44 meas-
ured by this technic. In this same case,
hypoglycemia could also be induced by ad-ministration of leucine, and following re-
duction of the tumor size by radiotherapy,serum insulin level fell to normal. This isthe only case in which hypoglycemia, ifnot produced by insulin itself, must havebeen due to material indistinguishable fromit, at least immunologically.
Available evidence therefore seems to in-dicate that both glucose utilization and pro-
duction of insulin-like material by the tu-mor are the most likely mechanisms ofhypoglycemia associated with these tumors.As pointed out by Perkoff and Simons,"these two mechanisms are not mutually ex-
clusive and may coexist in one patient.Diagnosis. The single most important
factor for the establishment of diagnosis isawareness of the existence of this syndrome.Once symptoms of hypoglycemia have
developed, the determination of low bloodsugar and the subsequent alleviation ofsymptoms by oral or intravenous adminis-tration of glucose will establish the diag-nosis of hypoglycemia. Differential diag-nosis should then be made between func-tional and organic hypoglycemia.
Distinction between functional hypogly-
Volume 161Number 4 557
PAPAIOANNOU AND MIC PEAK
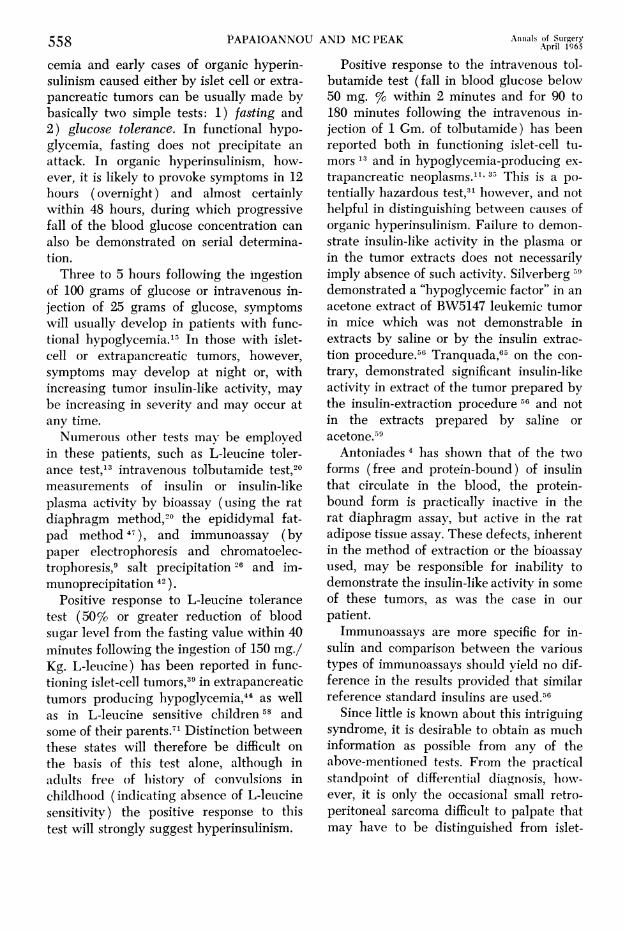
cemia and early cases of organic hyperin-sulinism caused either by islet cell or extra-pancreatic tumors can be usually made bybasically two simple tests: 1) fasting and2) glucose tolerance. In functional hypo-
glycemia, fasting does not precipitate an
attack. In organic hyperinsulinism, how-ever, it is likely to provoke symptoms in 12hours (overnight) and almost certainlywithin 48 hours, during which progressivefall of the blood glucose concentration can
also be demonstrated on serial determina-tion.Three to 5 hours following the ingestion
of 100 grams of glucose or intravenous in-jection of 25 grams of glucose, symptomswill usually develop in patients with func-tional hypoglycemia.1 In those with islet-cell or extrapancreatic tumors, however,symptoms may develop at night or, withincreasing tumor insulin-like activity, may
be increasing in severity and may occur atany time.Numerous other tests may be employed
in these patients, such as L-leucine toler-ance test,13 intravenous tolbutamide test,20measurements of insulin or insulin-likeplasma activity by bioassay (using the ratdiaphragm method,'° the epididymal fat-pad method 47 ), and immunoassay (bypaper electrophoresis and chromatoelec-trophoresis,9 salt precipitation 26 and im-munoprecipitation 42 ).
Positive response to L-leucine tolerancetest (50% or greater reduction of bloodsugar level from the fasting value within 40minutes following the ingestion of 150 mg./Kg. L-leucine) has been reported in func-tioning islet-cell tuLmors,39 in extrapancreatictumors producing hypoglycemia,44 as wellas in L-leucine sensitive children 58 andsome of their parents.71 Distinction betweenthese states will therefore be difficult on
the basis of this test alone, although inadults free of hiistory of convulsions inchildhood (indicating absence of L-leucinesensitivity) the positive response to thistest will strongly suggest hyperinsulinism.
Positive response to the intravenous tol-butamide test (fall in blood glucose belov50 mg. % within 2 minutes and for 90 to180 minutes following the intravenous in-jection of 1 Gm. of tolbutamide) has beenreported both in functioning islet-cell tu-mors 13and in hypoglycemia-producing ex-
trapancreatic neoplasms.""35 This is a po-
tentially hazardous test," however, and nothelpful in distinguishing between causes oforganic hyperinsulinism. Failure to demon-strate insulin-like activity in the plasma or
in the tumor extracts does not necessarilyimply absence of such activity. Silverberg5ldemonstrated a "hypoglycemic factor" in an
acetone extract of BW5147 leukemic tumorin mice which was not demonstrable inextracts by saline or by the insulin extrac-tion procedure.56 Tranquada,6' on the con-
trary, demonstrated significant insulin-likeactivity in extract of the tumor prepared bythe insulin-extraction procedure 56 and notin the extracts prepared by saline or
acetone.'9Antoniades 4 has shown that of the two
forms (free and protein-bound) of insulinthat circulate in the blood, the protein-bound form is practically inactive in therat diaphragm assay, but active in the ratadipose tissue assay. These defects, inherentin the method of extraction or the bioassayused, may be responsible for inability todemonstrate the insulin-like activity in someof these tumors, as was the case in our
patient.Immunoassays are more specific for in-
sulin and comparison between the varioustypes of immunoassays should yield no dif-ference in the results provided that similarreference standard insulins are used.56
Since little is known about this intriguingsyndrome, it is desirable to obtain as much
information as possible from any of theabove-mentioned tests. From the practicalstandpoint of differential diagnosis, howv-ever, it is only the occasional small retro-peritoneal sarcoma difficult to palpate thatmay have to be distinguished from islet-
558 Anniials of SurgeryApril 1965

Volume 161 RHABDOMYOSARCOMA OF THE BUTTOCK 559Number 4
cell tumor. In this instance, determinationof plasma insulin activity by immunoassay,if positive, will suggest islet-cell tumor,since up to the present there has been onlyone case of fibrosarcoma that has yieldedhigh levels of plasma insulin by thismethod.44Methods of Treatment. Surgical removal
of the tumor is presently the treatment ofchoice. Even if complete extirpation is notpossible, removal of as much of the tumoras possible is advisable as a highly gratify-ing palliative treatment.Most low-grade fibrosarcomas are insensi-
tive to radiation. Occasionally, however,radiation therapy may be quite helpful asin our case and otbers.44Sudden neurologic and other symptoms
of hypoglycemia should be treated promptlyby intravenous hypertonic dextrose, 1 mg.of epinephrine subcutaneously, or 5 mg. ofglucagon subcutaneously or intravenously.Large doses of corticosteroids may also behelpful.
Subsequent treatment can be adjusted tothe patient's mental status. If hypoglycemiaand coma are prolonged, restitution ofmental function with intravenous dextrosemay be slow and occasionally incomplete,but the deficiencies are not necessarilypermanent.Hypoglycemic bouts can be prevented by
frequent meals of high carbohydrate con-tent as well as glucagon and corticosteroids.Human growth hormone recently has beentried with fair results in one case.37
It must be emphasized that treatment ofhypoglycemia is also needed during opera-tion, especially if the procedure is time-consuming and thereby combining bothprolonged fasting and manipulation of thetumor which might result in elaboration ofhypoglycemic factor in greater quantitiesinto the circulation.Hyperglycemia usually seen following
the removal of these tumors, owing to thetemporary suppression of islet-cell function,
is usually mild and does not require treat-ment.
SummaryA 24-year-old pregnant woman with pro-
found hypoglycemia due to a bulky rhabdo-myosarcoma of the buttock was initiallytreated by irradiation with shrinkage of thetumor and amelioration of hypoglycemicsymptoms. Extended hemipelvectomy wassubsequently performed and the patientdied shortly after operation from uncon-trolled hemorrhage.
Including the case discussed herein, 84cases of extrapancreatic neoplasms produc-ing hypoglycemia have been reported inthe world literature since 1930. These tu-mors originated from all three blastodermnsusually presented in the peritoneal or tho-racic cavities, but also in the gastro-in-testinal tract and buttock, and manifesteda wide spectrum of histologic types andmalignant potential.The most likely mechanism of hypo-
glycemia appears to be production of aninsulin-like substance and increased utiliza-tion of glucose by the tumor. The basicmethods of diagnosis and treatment em-ployed are outlined.
AcknowledgmentWe are indebted to Dr. Alvin Freiman and Mr.
Milton Zitzowitz for advice in the preparation ofthe manuscript.
References1. Amzomin, G. D.: Suggested Mechanism of Ex-
trapancreatic Neoplasm and Hypoglycemia.New Engl. J. Med., 268:682, 1963.
2. Anderson, H. B.: A Tumor of the AdrenalGland with Fatal Hypoglycemia. Amer. J.Med. Sci., 180:71, 1930.
3. Antoniades, H. N., J. A. Bougas and H. M.Pyle: Studies of the State of Insulin inBlood: Examination of Splenic, Portal andPeripheral Blood Serum of Diabetic andNon-diabetic Subiects for "Free" Insulinand Insulin Complexes. New Engl. J. Med.,267:218, 1962.
4. Antoniades, H. N., P. M. Beigelman, R. B.Tranquada and K. Gundersen: Studies onthe State of Insulin in Blood "Free" Insulinand Insulin Complexes in Human Sera andTheir in vitro Biological Properties. Endo-frinnlAru 6Q946 1Q1.
PAPAIOANNOU AND MC PEAK Annals of Surgery560 April 1965
5. Arkles, H. A.: Coincidence of Rhabdomyo-sarcoma of the Diaphragm, Idiopathic Hypo-glycemia and Retroperitoneal Sarcoma. Med.Bull. Vet. Admin., 19:225, 1942.
6. August, J. T. and H. H. Hiatt: Severe Hypo-glycemia Secondary to Nonpancreatic Fibro-sarcoma with Insulin Activity. New Engl. J.Med., 258:17, 1958.
7. Barbosa, J. J., M. B. Dockerty and J. M.Waugh: Pancreatic Heterotopia. Surg. Gynec.& Obstet., 82:527, 1946.
8. Barjon, P. and R. Labange: Mesenchymal Tu-mors Producing Hypoglycemia. Presse Med.,69:2635, 1961.
9. Berson, S. A. and R. S. Yalow: Immunoassayof Plasma Insulin, in Ciba Foundation Col-loquia on Endocrinology, Vol. 14, Immuno-assay of Hormones, 1962. p. 182.
10. Bonsvaros, G. A.: Hypoglycemia in MetastaticFibrosarcoma of Liver. Brit. Med. J., 1:836,1960.
11. Boskell, B. R., J. J. Kirschenfeld and P. S.Soteres: Extrapancreatic Insulin-SecretingTumor. New Engl. J. Med., 270:338, 1964.
12. Broster, L. R. and J. Patterson: An UnusualCase of Adrenal Carcinoma with a Note onApplication of New Colour Test. Brit. Med.J., 1:781, 1948.
13. Cochrane, W. A.: Idiopathic Infantile Hypo-glycemia and Leucine Sensitivity. Metab-olism, 2:386, 1960.
14. Cori, C. F. and G. T. Cori: CarbohydrateMetabolism of Tumors. I. Free Sugar, LacticAcid and Glycogen Content of MalignantTumors. J. Biol. Chem., 64:11, 1925.
15. Conn, J. W. and H. S. Seltzer: SpontaneousHypoglycemia. Amer. J. Med., 12:460, 1957.
16. DeCoster, A., M. Payfa, R. Bellens, V. Conardand P. A. Bastenic: Intrathoracic Tumors andHypoglycemia. J. Franc. Med. Chir. Thor.,16:191, 1962.
17. DePeyster, F. A. and R. K. Gilchrist: SurgicalAspects of Spontaneous Hypoglycemia Dueto Occult Insulinoma. Arch. Surg., 67:330,1953.
18. Dodge, K. W.: Fibrosarcoma of Mediastinum.Ann. Surg., 92:955, 1930.
19. Duncan, G. G. and G. L. Schless: MassiveRetroperitoneal Fibrosarcoma, SpontaneousHypoglycemia and Generalized Splanch-nomegaly. Metabolism, 10:200, 1961.
20. Fajans, S. S. and J. W. Conn: IntravenousTolbutamide Test as Adjunct in Diagnosis ofFunctioning Islet Cell Adenomas. J. Lab.Clin. Med., 54:811, 1959.
21. Fikenscher, T. F. and P. S. Blons: Hypogly-cemia and Fibrosarcoma. Net. T. Geneesk.,107:1076, 1963.
22. Froesch, E. R., H. Burg, W. Ziegler, P. Ballyand A. Labhart: Pathogenesis of Tumor-In-duced Hypoglycemia without Hyperinsulin-ism. Schweiz. Med. Wschr., 93:1250, 1963.
23. Garfield, C. R., H. V. Belcher and J. S.Shuttleworth: Fibrous Mesothelioma withHypoglycemia Psychosis and Coma. J.A.M.A.,181:380, 1962.
24. Gomori, G. L.: Observations with DifferentialStains of Human Islets of Langerhouns.Amer. J. Pathol., 20:665, 1950.
25. Gonzalez, F. M., L. G. Gold and B. Schnider:Gastrointestinal Carcinoma and Concomitant
Hypoglycemia. Ann. Int. Med., 58:149,1963.
26. Grodsky, G. H. and P. H. Forsham: Compara-tive Binding of Beef and Human Insulin toInsulin Antibodies in Man and Guinea Pigs.J. Clin. Invest., 40:799, 1961.
27. Hayes, D. M., C. L. Spurr, J. H. Felts andE. C. Miller: Von Recklinghausen's Dis-ease with Massive Intra-Abdominal Tumorand Spontaneous Hypoglycemia: MetabolicStudies Before and After Perfusion of Ab-dominal Cavity with Nitrogen Mustard. Me-tabolism, 10:183, 1961.
28. Heiskala, H., and M. Gylling: Sarcoma andHypoglycemia. Duodecim, 79:543, 1963.
29. Hines, R. E.: Hypoglycemia Apparently Dueto Retroperitoneal Sarcoma. Med. Bull. Vet.Admin., 20:102, 1943.
30. Howard, J. W. and P. L. Davis: Retroperi-toneal Hemangiopericytoma Associated withHypoglycemia and Masculinization. Dela-ware Med. J., 31:29, 1959.
31. Johnston, R., F. C. Goetz and B. Zimmermann:Insulin-Secreting Tumors of the Pancreas:Report of a Case with an Untoward Responseto Tolbutamide and with a Study of thePossible Mechanism of Postoperative Hyper-glycemia. New Engl. J. Med., 263:1345,1960.
32. Karsch, R. S., H. Freedman and H. T. Blumen-thal: Functional Islet Cell Carcinoma Metas-tasizing as Spindle Cell Tumor. Amer. J.Med., 30:619, 1961.
33. Kujjer, P. J.: A Tumor of the Lung with Dis-turbances in the Sugar Metabolism. Arch.Chir. Neerl., 13:81,1961.
34. Lawrence, C. H.: Adrenal Cortical Tumor.Ann. Int. Med., 11:938, 1937.
35. Leger, L., C. Sors, C. Dubosi, M. Magdelaine,J. Lejeune, E. Roseau and G. Lemaigre:Hypoglycemies des Tumeurs Mesenchyma-tenses Extrapancreatigues. Presse Med., 71:219, 1963.
36. Lowbeer, L.: Hypoglycemia Producing Extra-pancreatic Neoplasma. Amer. J. Clin. Pathol.,35:233, 1961.
37. Mahon, W. A., M. L. Mitchell, J. Steinke andM. S. Raben: Effect of Human Growth Hor-mone on Hypoglycemia States. New Engl. J.Med., 267:1179, 1962.
38. Makkota, S.: Spontaneous HypoglycemiaCaused by Large Mesenchymatous Tumorsof the Lung. Zdrav. Vestn., 27:326, 1958.
39. Marrack, D., V. Marks and F. C. Rose: ALeucine-Sensitive Insulin Secreting Tumor.Lancet, 2:1329, 1960.
40. Meyer-Hofmann, G., H. Schwartzkopf and H.Hartmann: Spontaneous Hypoglycemia withExtrapancreatic Tumors. Deutsch. Med.,Wschr., 85:2106, 2109, 1960.
41. Miller, D. R., R. E. Bollinger, D. Janigan J.R. Crockett and S. R. Friesen: HypoglycemiaDue to Nonpancreatic Mesodermal Tumors:Report of Two Cases. Ann. Surg., 150:684,1959.
42. Morgan, C. R. and A. Lazarow: Immunoassayof Insulin: Two Antibody Systems. Diabetes,12:115, 1963.
43. Oda, M., H. Oka, Y. Fujita, T. Kaneto and T.Takenchi: Spontaneous Hypoglycemia withPrimary Hepatoma. Acta. Haemat. Jap., 4:33, 1962.
Volume 161 RHABDOMYOSARCOMA OF THE BUTTOCK 561Number 4
44. Oleesky, S., I. Bailey, E. Samols and D. Bilkus:A Fibrosarcoma with Hypoglycemia andHigh Serum Insulin Level. Lancet, 2:278,1962.
45. Pedersen, J., F. Lung and J. Ringstead: Hypo-glycemia in Presence of Massive Fibrosar-coma (Mesenchymoma). Acta Endocrinol.,34:148, 1960.
46. Perkoff, G. T. and E. L. Simons: Hypogly-cemia in a Patient with a Fibrous Tumor.Arch. Int. Med., 112:589, 1963.
47. Renold, A. E., C. B. Martin, Y. M. Pagenais,J. Steinke, R. J. Nickerson and M. C. Sheps:Measurement of Small Quantities of Insulin-Like Activity Using Rat Adipose Tissue. I.Proposed Procedure. J. Clin. Invest., 39:1487, 1960.
48. Roffo., A. H. and L. M. Carrea: On the Pres-ence of Insulinoid in Malignant Tumors. J.Cancer Res., 11:126, 1927.
49. Rogers, J. C. T. and J. H. Houseworth: LargeFibrogenic Tumors and Hypoglycemia. J.A.-M.A., 178:1132, 1961.
50. Rosenfeld, E. D.: Peritoneal Pseudomyxoma:A Report of Four Unusual Cases. Arch.Pathol., 48:255, 1949.
51. Rossman, E. M.: Mediastinal Neurofibrosar-coma Causing Hypoglycemia. Arch. Int.Med., 104:640, 1959.
52. Samoli, E. and D. Bilkus: A Comparison ofInsulin Immunoassays. Proc. Soc. Exp. Biol.Med., 115:79, 1964.
53. Schmidt, H. W. and K. I. Schurholz: Hypo-glycemic Attacks Caused by an IntrathoracicTumour. Report of a Case. Deut. Med.Wschr., 86:2231, 1961.
54. Scholz, D. A., L. B. Woolner and J. T. Priesty:Spontaneous Hypoglycemia Associated withFibrogenic Tumors: Report of Two Cases.Ann. Int. Med., 46:796, 1957.
55. Schonfeld, A., D. Babott and K. Gundersen:Hypoglycemia and Polycythemia Associatedwith Primary Hepatoma. New Engl. J. Med.,265:231, 1961.
56. Scott, D. A. and A. M. Fisher: Studies on thePancreas and Liver of Normal and Zinc-FedCats. Amer. J. Physiol., 121:253, 1938.
57. Seckel, H. P. G.: Post-Mortem Hepatic Glyco-genolysis in Hyperinsulinism and GlycogenDisease. J. Clin. Invest., 18:723, 1939.
58. Sellman, J. C., G. T. Perkoff, F. C. Null, J.R. Kimmel and F. H. Tyler: HypoglycemiaAssociated with Massive Intra-AbdominalMesothelial-Cell Sarcoma. New Engl. J.Med., 260:847, 1959.
59. Silverberg, M. N., K. G. Wakim, R. C. Bahnand E. D. Bayard: A Hypoglycemia Factor
in Leukemic Tumors. Proc. Soc. Exp. Biol.Med., 103:824, 1960.
60. Silvis, R. S. and D. S. Simon: Marked Hypo-glycemia Associated with Nonpancreatic tu-mors. New Engl. J. Med., 254:14, 1956.
61. Skillern, P. G., L. J. McCormack, J. S. Hew-lett and G. Crile, Jr.: Hyperinsulinism Dueto Islet-Cell Tumors Simulating Sarcoma.Diabetes, 3:133, 1954.
62. Sors, C., L. Leger, C. Dubost and G. Thomeret:Thoracic Mesotheliomas Producing Hypo-glycemias. Rev. Tuberc. (Paris), 26:1268,1962.
63. Staffieri, J. J., C. Comes and J. M. Cid: Corti-coadrenal Tumor with Hypoglycemic Syn-drome, Goiter Gynecomastia and Hepato-splenomegaly. J. Clin. Endocr., 9:255, 1949.
64. Stauffer, J. M., G. E. Granville and S. W. Law:Recurrent Hypoglycemia and RetroperitonealFibrosarcoma. New Engl. J. Med., 265:979,1961.
65. Tranquada, R. E., A. B. Bender and P. M.Biegelman: Hypoglycemia Associated withCarcinoma of the Cecum and Syndrome ofTesticular Feminization. New Engl. J. Med.,266:1302, 1962.
66. Ufer, J.: Zur Entstehung der Spontanhypo-glykamie. Deut. Med. Wschr., 69:206, 1943.
67. Unger, R. H., A. M. Eisentraut, M. S. McCalland L. L. Madison: Glucagon Antibodiesand an Immunoassay for Glucagon. J. Clin.Invest., 40:1280, 1960.
68. Vallance-Owen, J. and B. Hurlock: Estimationof Plasma Insulin by the Rat DiaphragmMethod. Lancet, 1:68, 1954.
69. Van Dolder, G.: Spontaneous Hypoglycemia ina Patient with a Large Pulmonary Tumor.Ned. T. Geneesk., 105:2030, 1961.
70. Victor, J. and J. S. Potter: Low Serum Glucosein Leukemic Mice. Amer. J. Cancer, 33:578,1938.
71. Weisenfeld, S. and M. G. Goldner: Hypo-glycemia in L-Leucine-Sensitive Hypogly-cemia in an Adult. Amer. J. Med., 31:658,1961.
72. Whitney, J. E. and C. G. Massey: ApparentInsulin Activity in a Fibrosarcoma Associ-ated with Spontaneous Hypoglycemia. J.Clin. Endocr., 21:541, 1961.
73. Whitney, J. E. and B. I. Heller: Increased In-sulin-Like Activity of Serum in Patient withSpontaneous Hypoglycemia Associated withRetroperitoneal Fibrosarcoma. Amer. J. Med.,30:633, 1961.
74. Williams, R., A. E. Kellie, A. P. Wade and T.M. Chalmers: Hypoglycemia and AbnormalSteroid Metabolism in Adrenal Tumors.Quart. J. Med., 30:269, 1961.