Rhabdomyoma in neonate WJPCHS
4
Case Report Biventricular Repair in a Neonate With Obstructive Inflow Cardiac Rhabdomyoma and Tuberous Sclerosis Hunter W. Hood, MS 1 , Ali Dodge-Khatami, MD, PhD 1 , Aimee S. Parnell, MD 2 , and Jorge D. Salazar, MD 1 Abstract A neonate with prenatally diagnosed large intracardiac rhabdomyomas and suspicion of tuberous sclerosis presented at birth with severe ductal-dependent obstruction at the tricuspid valve and an atrial septal defect (ASD). Biventricular repair at 9 days of life included tumor resection, repair of the posterior leaflet of the tricuspid valve with autologous pericardium, fenestrated ASD clo- sure, and ductus ligation. After an uneventful postoperative recovery, follow-up echocardiography at two months showed excel- lent results with tricuspid valve competency and normal biventricular function. Overall prognosis will probably depend on issues pertaining to tuberous sclerosis. Keywords cardiac tumors, tricuspid valve, neonate Submitted October 3, 2014; Accepted November 3, 2014. Introduction Although primary cardiac tumors are rare in the pediatric pop- ulation, intracardiac rhabdomyomas are most frequently seen in neonates and infants and often associated with tuberous sclerosis. 1-3 Spontaneous regression of intracardiac rhabdo- myomas without medical or surgical intervention is well docu- mented and common. As such, only a minority require surgical intervention, whose indications include medically refractory dysrhythmia, compromised hemodynamic function, and/or hydrops. 4-6 When hemodynamic compromise does occur from systemic or pulmonary inflow and/or outflow obstruction, either single ventricle surgical palliation or biventricular repair may be necessary to allow patient survival. We present the case of a neonate with severe right ventricular (RV) inflow obstruction and ductal-dependent pulmonary blood flow, who underwent successful tumor resection, tri- cuspid valve reconstruction, and biventricular repair. Case Report At 31 weeks of gestation, a prenatal ultrasound identified multiple intracardiac tumors (suspected cardiac rhabdomyo- mas) in a female fetus, including one large right atrial tumor that appeared adherent to the tricuspid valve (Figure 1). Fetal magnetic resonance imaging identified two possible subependymal nodules and four rhabdomyomas, one of 1 Pediatric and Congenital Heart Surgery, Children’s Heart Center, University of Mississippi Medical Center, Jackson, MS, USA 2 Pediatric and Fetal Cardiology, Children’s Heart Center, University of Mississippi Medical Center, Jackson, MS, USA Corresponding Author: Ali Dodge-Khatami, Division of Pediatric and Congenital Heart Surgery, Batson Children’s Hospital, University of Mississippi Medical Center, 2500 North State Street, Room S345, Jackson, MS 39216, USA. Email: [email protected] Figure 1. Prenatal fetal ultrasound at 31 gestational weeks, showing the intracardiac masses and largest tumor attached to the tricuspid valve. RA indicates right atrium; LA, left atrium; Rh, rhabdomyoma. World Journal for Pediatric and Congenital Heart Surgery 2015, Vol. 6(2) 307-310 ª The Author(s) 2014 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/2150135114561689 pch.sagepub.com
-
Upload
ali-dodge-khatami-md-phd -
Category
Documents
-
view
36 -
download
1
Transcript of Rhabdomyoma in neonate WJPCHS

Case Report
Biventricular Repair in a Neonate WithObstructive Inflow Cardiac Rhabdomyomaand Tuberous Sclerosis
Hunter W. Hood, MS1, Ali Dodge-Khatami, MD, PhD1,Aimee S. Parnell, MD2, and Jorge D. Salazar, MD1
AbstractA neonate with prenatally diagnosed large intracardiac rhabdomyomas and suspicion of tuberous sclerosis presented at birth withsevere ductal-dependent obstruction at the tricuspid valve and an atrial septal defect (ASD). Biventricular repair at 9 days of lifeincluded tumor resection, repair of the posterior leaflet of the tricuspid valve with autologous pericardium, fenestrated ASD clo-sure, and ductus ligation. After an uneventful postoperative recovery, follow-up echocardiography at two months showed excel-lent results with tricuspid valve competency and normal biventricular function. Overall prognosis will probably depend on issuespertaining to tuberous sclerosis.
Keywordscardiac tumors, tricuspid valve, neonate
Submitted October 3, 2014; Accepted November 3, 2014.
Introduction
Although primary cardiac tumors are rare in the pediatric pop-
ulation, intracardiac rhabdomyomas are most frequently seen
in neonates and infants and often associated with tuberous
sclerosis.1-3 Spontaneous regression of intracardiac rhabdo-
myomas without medical or surgical intervention is well docu-
mented and common. As such, only a minority require surgical
intervention, whose indications include medically refractory
dysrhythmia, compromised hemodynamic function, and/or
hydrops.4-6 When hemodynamic compromise does occur from
systemic or pulmonary inflow and/or outflow obstruction,
either single ventricle surgical palliation or biventricular
repair may be necessary to allow patient survival. We
present the case of a neonate with severe right ventricular
(RV) inflow obstruction and ductal-dependent pulmonary
blood flow, who underwent successful tumor resection, tri-
cuspid valve reconstruction, and biventricular repair.
Case Report
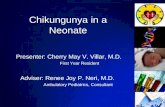
At 31 weeks of gestation, a prenatal ultrasound identified
multiple intracardiac tumors (suspected cardiac rhabdomyo-
mas) in a female fetus, including one large right atrial tumor
that appeared adherent to the tricuspid valve (Figure 1).
Fetal magnetic resonance imaging identified two possible
subependymal nodules and four rhabdomyomas, one of
1 Pediatric and Congenital Heart Surgery, Children’s Heart Center, University
of Mississippi Medical Center, Jackson, MS, USA2 Pediatric and Fetal Cardiology, Children’s Heart Center, University of
Mississippi Medical Center, Jackson, MS, USA
Corresponding Author:
Ali Dodge-Khatami, Division of Pediatric and Congenital Heart Surgery, Batson
Children’s Hospital, University of Mississippi Medical Center, 2500 North State
Street, Room S345, Jackson, MS 39216, USA.
Email: [email protected]
Figure 1. Prenatal fetal ultrasound at 31 gestational weeks, showingthe intracardiac masses and largest tumor attached to the tricuspidvalve. RA indicates right atrium; LA, left atrium; Rh, rhabdomyoma.
World Journal for Pediatric andCongenital Heart Surgery2015, Vol. 6(2) 307-310ª The Author(s) 2014Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/2150135114561689pch.sagepub.com

Abbreviations and Acronyms
ASD atrial septal defectPDA patent ductus arteriosusRV right ventricularTSC tuberous sclerosis complex
which appeared to obstruct the tricuspid valve inflow. Genetic
testing for potential tuberous sclerosis complex (TSC) was rec-
ommended. The patient was born via cesarean section due to
non-reassuring fetal heart tones at 39 weeks of gestation and
monitored in the neonatal intensive care unit. Intravenous pros-
taglandin E1 was administered immediately to maintain ductal
patency. Esmolol therapy was initiated on day 2 of life for
supraventricular dysrhythmia. Postnatal transthoracic echocar-
diography reconfirmed a lobulated mass attached to the poster-
ior leaflet of the tricuspid valve, causing moderate stenosis and
severe regurgitation (Figure 2). Additional tumors were identi-
fied in the left atrium, anterior papillary muscle of the mitral
valve, and left ventricular apex, which were neither obstructive
nor affecting function. Due to the hemodynamic consequences
induced by the right-sided obstructive mass, surgical interven-
tion was indicated, and biventricular repair judged possible.
On day 6 of life, the neonate experienced supraventricular
tachycardia unresponsive to adenosine and 5 J of electrical car-
dioversion, and therapy was converted from esmolol to amio-
darone until the date of operation.
Preoperative transesophageal echocardiography on day 9
of life showed severe RV inflow obstruction, mild tricuspid
valve regurgitation, a stretched foramen ovale with bidirec-
tional atrial shunting, a large patent ductus arteriosus (PDA)
with left-to-right shunting, and mild dilation of both the left
atrium and the left ventricle. Through median sternotomy, a
patch of autologous pericardium was harvested and tanned
for repair of the tricuspid valve. Under aortic and bicaval
cannulation, cardiopulmonary bypass, and moderate
hypothermia, the PDA was ligated. After aortic cross clamp-
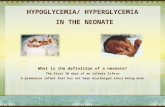
ing, the right atrium was opened and tumor resection
attempted (Figure 3A and B). Surprisingly, the tumor enu-
cleated off the tricuspid valve easily with only minimal
(millimeters) defect creation, and reconstruction of the pos-
terior leaflet of the tricuspid valve was possible with the
patch of tanned pericardium. Intraoperative saline bulb test-
ing of the valve’s competency appeared satisfactory. The
atrial septal defect was partially closed to allow for a
right-to-left pop off. The neonate’s other intracardiac rhab-
domyomas neither was judged to be safely amenable to
resection nor account for any hemodynamically significant
problems and was therefore left in situ for follow-up moni-
toring. The postoperative course was uneventful, with extu-
bation and discharge from the intensive care unit on
postoperative days 2 and 3, respectively. Transthoracic echo-
cardiography prior to hospital discharge on postoperative day
9 documented normal biventricular function, mild tricuspid
regurgitation with no stenosis, a small residual interatrial
Figure 2. Postnatal transthoracic echocardiography on day 1 of life with the rhabdomyoma mass on the tricuspid valve, creating right inflowobstruction with flow acceleration (arrow) and tricuspid valve insufficiency. RA indicates right atrium, LA, left atrium; Rh, rhabdomyoma.
308 World Journal for Pediatric and Congenital Heart Surgery 6(2)

communication with bidirectional shunting, and no pericardial
effusion. Genetic testing after the operation identified a het-
erozygous, nonsense mutation in TSC2, which confirmed
the suspected diagnosis of tuberous sclerosis. The patient’s
neurological status was normal, and electroencephalography
performed for suspected seizure activity was negative. Renal
ultrasound obtained prior to surgery showed bilateral grade 1
hydronephrosis, while ophthalmologic evaluation identified
no evidence of hamartomas. At two-month follow-up, the
echocardiographic findings again confirm a satisfactory valvar
repair with minimal regurgitation and no evidence of stenosis
(Figure 4). The infant is asymptomatic and thriving with only
oral flecainide for sustained atrial tachycardia diagnosed dur-
ing echocardiographic follow-up.
Figure 3. A and B, Intraoperative findings showing the lobulated tumor attached to the tricuspid valve and the surgical situs for sizeperspective.
Figure 4. Postoperative transthoracic echocardiography at two-month follow-up, confirming good coaptation of the tricuspid valve repair,trivial regurgitation (arrow), and normal biventricular function. RA indicates right atrium; LA, left atrium; TR, tricuspid regurgitation.
Hood et al 309

Discussion
Rhabdomyomas are the most common primary tumor in
infancy and are often associated with TSC.1-3 Tuberous sclero-
sis is a multisystem neurocutaneous disorder caused by deleter-
ious mutations in one of the two tumor-suppressor genes, TSC1
and TSC2, encoding for the proteins hamartin and tuberin,
respectively. Abnormal functioning of TSC1 or TSC2 is associ-
ated with development of hamartomas.1 As the clinical manifes-
tations of tuberous sclerosis may not appear until later in
infancy, noninvasive imaging of intracardiac rhabdomyomas
will often serve as the earliest indicator of the disease complex.2
Literature on cardiac tumor resection in neonates is limited,
but ever-improving imaging techniques should allow for earlier
detection and repair.4 Since many rhabdomyomas naturally
regress during childhood, careful consideration must be paid
when contemplating surgery. However, multi-institutional data
analyses have noted the benefit of surgical intervention in
patients with symptomatic intracardiac tumors.5,6 When plan-
ning a potentially complex resection of a tumor creating hemo-
dynamically significant inflow or outflow obstruction, both
biventricular and univentricular repair strategies should be con-
sidered, even in the presence of two functionally adequate ven-
tricles. Biventricular repair seemed suitable in our patient, but a
Starnes RV exclusion procedure was contemplated and kept as a
backup plan in the event the obstructing tumor could not be
safely resected or the tricuspid valve not amenable to repair.7
Although the general prognosis for any patient with tuberous
sclerosis takes into account the risk of lesions in other organs,
our patient’s cardiac outcome is currently favorable, pending
future echocardiograms confirming regression of other, nonob-
structing intracardiac tumors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, author-
ship, and/or publication of this article.
References
1. Kocabas A, Ekici F, Cetin _I_I, et al. Cardiac rhabdomyomas associ-
ated with tuberous sclerosis complex in 11 children: presentation to
outcome. Pediatr Hematol Oncol. 2013;30(2): 71-79.
2. Bader RS, Chitayat D, Kelly E, et al. Fetal rhabdomyoma: prenatal
diagnosis, clinical outcome, and incidence of associated tuberous
sclerosis complex. J Pediatr. 2003;143(5): 620-624.
3. Pucci A, Botta G, Sina N, et al. Life-threatening tumors of the heart
in fetal and postnatal age. J Pediatr. 2013;162(5): 964-969.
4. Padalino MA, Basso C, Milanesi O, et al. Surgically treated pri-
mary cardiac tumors in early infancy and childhood. J Thorac Car-
diovasc Surg. 2005;129(6): 1358-1363.
5. Goldberg SP, Knott-Craig CJ, Boston US, Mari GC, Chin TK.
Surgical management of unusual cardiac tumors in infants and
children. World J Pediatr Congenit Heart Surg. 2010;1(2):
211-216.
6. Bielefeld KJ, Moller JH. Cardiac tumors in infants and children:
study of 120 operated patients. Pediatr Cardiol. 2013;34(1):
125-128.
7. Starnes VA1, Pitlick PT, Bernstein D, Griffin ML, Choy M, Shum-
way NE. Ebstein’s anomaly appearing in the neonate. A new surgi-
cal approach. J Thorac Cardiovasc Surg. 1991;101(6): 1082-1087.
310 World Journal for Pediatric and Congenital Heart Surgery 6(2)