Rex Moulton-Barrett, MD Plastic & Reconstructive Surgery San Leandro Surgery Center
50
Rex Moulton-Barrett, MD Rex Moulton-Barrett, MD Plastic & Reconstructive Surgery Plastic & Reconstructive Surgery San Leandro Surgery Center San Leandro Surgery Center Managing Plastic Surgery Managing Plastic Surgery Patients Patients Part One Part One
description
Managing Plastic Surgery Patients Part One. Rex Moulton-Barrett, MD Plastic & Reconstructive Surgery San Leandro Surgery Center. The 8 Aspects of Plastic Surgery. Congenital: clefts, nevi, vascular tumors - PowerPoint PPT Presentation
Transcript of Rex Moulton-Barrett, MD Plastic & Reconstructive Surgery San Leandro Surgery Center

Rex Moulton-Barrett, MDRex Moulton-Barrett, MDPlastic & Reconstructive SurgeryPlastic & Reconstructive Surgery
San Leandro Surgery CenterSan Leandro Surgery Center
Managing Plastic Surgery PatientsManaging Plastic Surgery Patients Part One Part One

The The 88 Aspects of Plastic Aspects of Plastic SurgerySurgery
• Congenital:Congenital: clefts, nevi, vascular tumors clefts, nevi, vascular tumors
ear reconstruction, hand anomaliesear reconstruction, hand anomalies
• Hand:Hand: nerve compression, tumors/soft tissue, trauma nerve compression, tumors/soft tissue, trauma
• Head and Neck:Head and Neck: resection and reconstructiveresection and reconstructive surgerysurgery
• Skin cancer:Skin cancer: excision and reconstruction excision and reconstruction
• Burn ReconstructionBurn Reconstruction
• General Reconstruction:General Reconstruction: truck, abdomen, lower limb truck, abdomen, lower limb
• Breast:Breast: reduction, reconstruction reduction, reconstruction
• Cosmetic Cosmetic

22 ways to get in trouble in medicine ways to get in trouble in medicine
• DON’T GO WHEN YOU ARE CALLED DON’T GO WHEN YOU ARE CALLED
• DON’T CALL WHEN YOU GET THEREDON’T CALL WHEN YOU GET THERE

Gorney’s RuleGorney’s Rule
• Extent of problem should = the concernExtent of problem should = the concern
• Operate on ‘ Sylvia ’ : Operate on ‘ Sylvia ’ : secure, young, secure, young, listens, verbal,intelligent, attractive listens, verbal,intelligent, attractive
• Don’t operate on ‘Simon’: Don’t operate on ‘Simon’: single, insecure, single, insecure, male, overexpectent, narcissisticmale, overexpectent, narcissistic

Post operative complicationsPost operative complications
• 5.4% complication rate clean surgery cases : 50% preventable5.4% complication rate clean surgery cases : 50% preventable• Blue Cross Aneheim refuses to pay for complications: April 2008Blue Cross Aneheim refuses to pay for complications: April 2008• Specifically: pressure sores, sternal wounds, line/foley sepsisSpecifically: pressure sores, sternal wounds, line/foley sepsis• Record insurance profits 2007: aggressive disclaimer policiesRecord insurance profits 2007: aggressive disclaimer policies• Post op infection most frequent complication: 1/2 mil/yr USAPost op infection most frequent complication: 1/2 mil/yr USA• Average cost per infection is $3,000Average cost per infection is $3,000• Post operative infections associated: 2 x procedure mortalityPost operative infections associated: 2 x procedure mortality

What stops wound healingWhat stops wound healing
• InfectionInfection• Foreign bodyForeign body• Tension/reduced vascularity: Tension/reduced vascularity:
venous,arterial,bothvenous,arterial,both• Inflammation: allergic, autoimmune, mechanical Inflammation: allergic, autoimmune, mechanical • Steroids and cytotoxic agentsSteroids and cytotoxic agents• TumorsTumors• Munchausen’s SyndromeMunchausen’s Syndrome

Controlling Surgical Site Controlling Surgical Site InfectionsInfections
• Saline versus water irrigation similar infections ratesSaline versus water irrigation similar infections rates• Transfusion during cardiac surgery increases rateTransfusion during cardiac surgery increases rate• Supplemental hydration does not change rateSupplemental hydration does not change rate• Hypothermia core temp< 36 C (96.8)Hypothermia core temp< 36 C (96.8)• Prophylactic antibiotics < one hour before incisionProphylactic antibiotics < one hour before incision• One dose IV as good as multiple & less C diff laterOne dose IV as good as multiple & less C diff later• Cardiac patient glucose control < 200 mg/dlCardiac patient glucose control < 200 mg/dl• Best no hair removal < shave < razorBest no hair removal < shave < razor• Maintaining oxygenationMaintaining oxygenation• Maintaining arterial, venous and capillary circulationMaintaining arterial, venous and capillary circulation

Hypothermia and wound Hypothermia and wound infectioninfection• 200 pts undergoing colorectal surgery: hypothermia assoc 200 pts undergoing colorectal surgery: hypothermia assoc
with 19% infection rate, vrs 6% non hypothermia with 19% infection rate, vrs 6% non hypothermia Kurz, et al, 1996: NEJM 334(19):1209-1215Kurz, et al, 1996: NEJM 334(19):1209-1215• Hypothermia leads to vasoconstrictionHypothermia leads to vasoconstriction• Vasoconstriction reduces tissue partial pressure O2Vasoconstriction reduces tissue partial pressure O2• Tissue hypoxygenation = decreased neutrophil Tissue hypoxygenation = decreased neutrophil
phagocytosisphagocytosis• Every drop of 1.5 C assoc. complications cost $ 2,500-Every drop of 1.5 C assoc. complications cost $ 2,500-
7,0007,000• Influenced by warming: preop pt, fluids, bed, irrigations, Influenced by warming: preop pt, fluids, bed, irrigations,
room temp, room temp, length of procedure, body surface area length of procedure, body surface area exposedexposed, inhalation gases, inhalation gases

Patterns of blood Patterns of blood supplysupply
• Random Random (2:1 ratio)(2:1 ratio)
• AxialAxial
• Random and AxialRandom and Axial ( rectus: type 3 )( rectus: type 3 )
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Tension / Tension / CompressionCompression
• Venous: decreased cap refill: < 3 secondsVenous: decreased cap refill: < 3 seconds• Arterial: increased cap refill: > 5 secondsArterial: increased cap refill: > 5 seconds or no refill: > 5 secondsor no refill: > 5 seconds• Creep phenomenon: 3 x 1 minute stretches 3 minutes apartCreep phenomenon: 3 x 1 minute stretches 3 minutes apart• Cyanosis: Cyanosis: requires O2 sat of <80% and 2.38 requires O2 sat of <80% and 2.38
g/deoxyhemoglobing/deoxyhemoglobin not present if arterial ischemia/vasoconstriction or not present if arterial ischemia/vasoconstriction or
severe anemia severe anemia
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

DVDVTT
• Pre surgery prophylaxisPre surgery prophylaxis
• Prevalence: Prevalence: 24% after elective 24% after elective surgery!!surgery!!
• Risks factorsRisks factors
• Who should get Lovenox: enoxaparinWho should get Lovenox: enoxaparin
• Clinical signs of DVTClinical signs of DVT
• Clinical Signs of PEClinical Signs of PE

DVT Preventive StockingsDVT Preventive Stockings• Reduce post-MI DVT p<0.003 (Kier,1993:Eur Heart J 14,1365-68.)Reduce post-MI DVT p<0.003 (Kier,1993:Eur Heart J 14,1365-68.)• May be as effective as pneumatic compression or low dose heparinMay be as effective as pneumatic compression or low dose heparin• Standing position ankle vein pressure in 5´7˝ adult is Standing position ankle vein pressure in 5´7˝ adult is 86mmHg86mmHg• 20-30 mmHg if standing ineffective at compressing s/d leg veins20-30 mmHg if standing ineffective at compressing s/d leg veins• 4 classes: 20-30,30-40,40-50 & 50-60 mmHg4 classes: 20-30,30-40,40-50 & 50-60 mmHg• 2 categories: ready made and custom2 categories: ready made and custom• 2 broad types: elastmeric ( day time ), non-elastameric ( straps )2 broad types: elastmeric ( day time ), non-elastameric ( straps )• Compression garments > 22mm Hg can cause thrombosis: kneeCompression garments > 22mm Hg can cause thrombosis: knee• elastomerics: woven:excellent, expensive, strong elastomerics: woven:excellent, expensive, strong
3 knitted: circular, flat (custom), cut & sew(custom) 3 knitted: circular, flat (custom), cut & sew(custom) elasticity from synthetic rubber or latex weaveelasticity from synthetic rubber or latex weave breathability related to thickness and cotton/nylonbreathability related to thickness and cotton/nylon
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

ManufacturersManufacturers• Jobst: 18-25 or 25-35mmHgJobst: 18-25 or 25-35mmHg• Sigvaris: synthetic rubber threads covering nylonSigvaris: synthetic rubber threads covering nylon• JuZo: increase upper stretch for big thighsJuZo: increase upper stretch for big thighs• Medi: spandex thread inlaid into woven rowMedi: spandex thread inlaid into woven row• Camp: double wrapped yarnsCamp: double wrapped yarns• Venosan: nylon, Lycra and cotton graduatedVenosan: nylon, Lycra and cotton graduated• Convalec: inelastic cohesive unnaflexConvalec: inelastic cohesive unnaflex• 3m Health: elastomeric high stretch adhesive 3m Health: elastomeric high stretch adhesive
microfoammicrofoam• TED: most well knownTED: most well known• Ibizi: Segreta ( Lycra )Ibizi: Segreta ( Lycra )
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Venous Thromboembolism Venous Thromboembolism Assessment Risk Score: Assessment Risk Score:
0-1 Low, 2-4 Moderate, 5 or greater high risk0-1 Low, 2-4 Moderate, 5 or greater high risk
• Hip fracture surgery (5)
• Total hip/knee replacement (5)
• >70 yrs (3)• H/o DVT/PE (3)
• Paralysis (3)• abdo/pelvis/leg (2)• # hip/pelvis/leg (2)• 61-70 yrs (2) (2)
(1)•Obesity >20% ideal body
weight•Varicose veins / varicose
swelling•inflammatory bowel disease•Bedrest preop > 48 hrs•Myeloproliferative•Malignancy•< 6 weeks post-partum•Acute ischaemic stroke•41-60 yrs•Major surgery•CHF•Severe respiratory disease •sepsis

Suggested prophylaxis Suggested prophylaxis RegimenRegimen• Low:Low: early ambulation, TED’s, +/- Sequentials, 20 degree knee flexearly ambulation, TED’s, +/- Sequentials, 20 degree knee flex
• Moderate:Moderate: Sequentials +/- TED’s, 20 degree knee flex Sequentials +/- TED’s, 20 degree knee flex Heparin 5,000 SQ q 8-12 hrs orHeparin 5,000 SQ q 8-12 hrs or
Levenox 40mg SQ q 24 hrs orLevenox 40mg SQ q 24 hrs or Lenenox 30 SQ q 12 hrsLenenox 30 SQ q 12 hrs
• Severe:Severe: Sequentials +/- TED’s Sequentials +/- TED’s Heparin 5,000 SQ q 8 hrs orHeparin 5,000 SQ q 8 hrs or
Lovenox 30 mg q 12 hrsLovenox 30 mg q 12 hrs Place temporary Greenfield Filter prior to surgeryPlace temporary Greenfield Filter prior to surgery

Well’s Clinical Dx Scoring Well’s Clinical Dx Scoring CriteriaCriteria• Entire Leg swollen (1)Entire Leg swollen (1)
• 10cm below tibial tuberosity >3cm calf 10cm below tibial tuberosity >3cm calf enlargement (1)enlargement (1)
• Pitting edema (1)Pitting edema (1)
• Collateral engorged non varicose veins (1)Collateral engorged non varicose veins (1)
• Alternative likely diagnosis (-3)Alternative likely diagnosis (-3)
Anand SS, et. al. Does this patient have deep vein thrombosis? JAMA, 1998; 279:2094-1099
If the score > 3: high risk and 85% probability 0: low risk and 5% probability

Clinical Presentation DVTClinical Presentation DVT
• 1/2 million hospitalized DVT/yr US1/2 million hospitalized DVT/yr US• 10% die10% die• Stasis, hypercoagulation, endothelial injuryStasis, hypercoagulation, endothelial injury• Pain then swelling, Howman’s negative 2/3’sPain then swelling, Howman’s negative 2/3’s• Clinical exam 3/4’s negative, some arise proximalClinical exam 3/4’s negative, some arise proximal• Assoc with popliteal valvular insufficiencyAssoc with popliteal valvular insufficiency• 1/3 of calf thrombi will propagate and embolize1/3 of calf thrombi will propagate and embolize• Di-Dimer: fibrin degrad products: only 2% false negDi-Dimer: fibrin degrad products: only 2% false neg• Colorflow Duplex: Colorflow Duplex: falsefalse negativenegative 20%20% below & below & 5%5% above above
kneeknee• Thrombolytic therapy more successful than anticoagulationThrombolytic therapy more successful than anticoagulation

Symptoms of Pulmonary Symptoms of Pulmonary EmbolusEmbolus
• 73% dyspnea73% dyspnea
• 60% pleuritic chest pain60% pleuritic chest pain
• 43% cough associated chest 43% cough associated chest painpain

Clinical Presentation Pulmonary EmbolusClinical Presentation Pulmonary EmbolusWell’s ScoreWell’s Score
• Score of <4: only 8% had PE by D-dimer testingScore of <4: only 8% had PE by D-dimer testing
• MRI 97% sensitive, 95% specificMRI 97% sensitive, 95% specific
• Anticoagulation prevent DVT propagation, reduces PEAnticoagulation prevent DVT propagation, reduces PE
• Hospitalization with unfractionated heparin Hospitalization with unfractionated heparin
• Thrombolytic therapy for massive emboliThrombolytic therapy for massive emboli
Clinical Signs and Symptoms of DVT?Yes +3PE Is #1 Diagnosis, or Equally LikelyYes +3Heart Rate > 100?Yes +1.5Immobilization at least 3 days, or Surgery in the Previous 4 weeksYes +1.5Previous, objectively diagnosed PE or DVT?Yes +1.5Hemoptysis?Yes +1Malignancy w/ Rx within 6 mo, or palliative?Yes
+1
Thromb Haemost. 2000 Mar;83(3):416-20

Fat Embolus: 5-15% Fat Embolus: 5-15% mortalitymortality
• Who is at risk: closed fractures, Who is at risk: closed fractures, tummy tucks, liposuctiontummy tucks, liposuction• <3 days after surgery<3 days after surgery• 25% have petechial rash25% have petechial rash• SOB, tachypnea, hemoptysis, crackles, ARDSSOB, tachypnea, hemoptysis, crackles, ARDS• Non specific w/u: Non specific w/u: fat in blood, snow storm CXR, serum lipase & phospholipase Bfat in blood, snow storm CXR, serum lipase & phospholipase B• Management: if acute, left lat positionManagement: if acute, left lat position
IV ethanol, dextran, steroidsIV ethanol, dextran, steroids New: IV Lipostabil New: IV Lipostabil (3-sn-phosphatidylcholine ethanol 96% (3-sn-phosphatidylcholine ethanol 96%
V/V)V/V) 250mg in 5ml: 40mls slow IV then 250mg in 5ml: 40mls slow IV then 80ml/day divided 20ml QID 80ml/day divided 20ml QID

MRSAMRSA
• 5% of population have MRSA in the nose5% of population have MRSA in the nose• This group accounts for 38% of MRSA This group accounts for 38% of MRSA
infections arising within hospitalinfections arising within hospital• 62% of MRSA infections arise in hospital62% of MRSA infections arise in hospital• ie 62% are true nosocomial in originie 62% are true nosocomial in origin• watch the housekeeping, lab, clerical, watch the housekeeping, lab, clerical,
catering and ancillary staff carefully for catering and ancillary staff carefully for glove changing between rooms / bedsglove changing between rooms / beds

Specific ProceduresSpecific Procedures• Breast ReconstructionBreast Reconstruction• Cleft SurgeryCleft Surgery• Hand surgeryHand surgery• BurnsBurns• Cosmetic: Cosmetic: AbdominoplastyAbdominoplasty FaceliftFacelift Eyelid SurgeryEyelid Surgery
LiposuctionLiposuction Augmentation +/- mastopexyAugmentation +/- mastopexy
Post - bariatric surgeryPost - bariatric surgery

Breast Breast ReconstructionReconstruction
• Reduction of the opposite breast after Reduction of the opposite breast after lumpectomylumpectomy
• Tissue expansion and exchange implantationTissue expansion and exchange implantation• ‘‘Tram’: Transverse rectus abdominus Tram’: Transverse rectus abdominus
myocutaneousmyocutaneous• Double Trams and supercharged TramsDouble Trams and supercharged Trams• Latissimus Dorsi with implantLatissimus Dorsi with implant• Free Flaps: Tram, Perforator Tram, DIEP, IGF Free Flaps: Tram, Perforator Tram, DIEP, IGF • Fat graftingFat grafting


Delayed, Double Pedicle, Supercharged TRAMsDelayed, Double Pedicle, Supercharged TRAMs

Free Flaps: Free Flaps: Rectus, DIEP SIEA, IGAP FlapsRectus, DIEP SIEA, IGAP Flaps

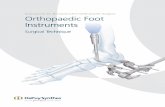
Cleft SurgeryCleft Surgery
• Cleft Lip & Palate > Palate > LipCleft Lip & Palate > Palate > Lip• Pierre Robin syndromePierre Robin syndrome: microgenia and airway : microgenia and airway
obstructionobstruction• Craniofacial Synostoses: Craniofacial Synostoses: Apert’s:Apert’s: hydrocephalus and airway obstruction hydrocephalus and airway obstructionVelocardiofacialVelocardiofacial: palate, cardiac and ectopic : palate, cardiac and ectopic
carotidscarotidsSticklersSticklers: palate and retinal detachments: palate and retinal detachmentsKlippel-FeilKlippel-Feil: palate and C 1-2 subluxation: palate and C 1-2 subluxationCrouzon’sCrouzon’s: 80% optic nerve compression: 80% optic nerve compression

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Pierre Robin
Apert’s
Crouzon’s
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Klippel Feil
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this p icture.
Stickler
Velocardiofacial

Cleft Palate & Cleft Palate & Airway ObstructionAirway Obstruction
• Repair separates oropharynx from nasopharynxRepair separates oropharynx from nasopharynx
• Compensatory tongue hypertrophy Compensatory tongue hypertrophy
• Separation can lead to crowding of orophrynxSeparation can lead to crowding of orophrynx
• Microgenia/midfacial retrusion increase crowdingMicrogenia/midfacial retrusion increase crowding
• IV steroids lead to reduced hospitalizationIV steroids lead to reduced hospitalization
• Tongue suture always placed for airway controlTongue suture always placed for airway control

Hand SurgeryHand Surgery
• Allen’s TestAllen’s Test• Cap refillCap refill• ElevationElevation• Surgical positioning:Surgical positioning: ulnar nerve and ulnar nerve and median nerve median nerve
compression,compression, brachial nerve plexopathybrachial nerve plexopathy

Capillary RefillCapillary Refill
• Normal Normal TissueTissue Capillary Refill is 3-5 seconds Capillary Refill is 3-5 seconds
• NailNail Capillary Refill test is < 2 seconds Capillary Refill test is < 2 seconds
• Unreliable in presence of hypothermia and severe Unreliable in presence of hypothermia and severe anemiaanemia
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

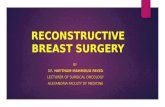
Allen’s TestAllen’s TestDominant Ulnar > Radial Artery 8.1%May be higher in populations with h/o ABG’s
1. Elevate hand 30 seconds2. Make fist elevated3. Apply pressure over Radial and Ulnar Arteries4. Open hand while elevated, it should be blanched5. Release one vessel pressure, should refill in 7 seconds

Median NeuropathyMedian Neuropathy
• Motor: thumb opposition and abductionMotor: thumb opposition and abduction
radial 2 lumbricalsradial 2 lumbricals
• Sensory: radial 3 1/2 fingers Sensory: radial 3 1/2 fingers

• Motor: All intrinsics Motor: All intrinsics exceptexcept thumb thumb opposition & opposition &
abductionabduction
radial 2 lumbricalsradial 2 lumbricals
• Sensory: Ulnar 1 1/2 sensorySensory: Ulnar 1 1/2 sensory
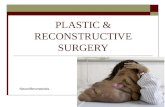
Ulnar NeuropathyUlnar Neuropathy

Brachial PlexopathyBrachial Plexopathy
• poor positioningpoor positioning• downward brachial traction downward brachial traction • shoulder hyperextensionshoulder hyperextension• descent of the thoraxdescent of the thorax• prolonged arm abductionprolonged arm abduction• responds to IV steroidsresponds to IV steroids• true neuropraxia: up to 6 week recoverytrue neuropraxia: up to 6 week recovery
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this p icture.

Cosmetic: Cosmetic: AbdominoplastyAbdominoplasty• Not panniculectomy, umbilicus preservedNot panniculectomy, umbilicus preserved
• Modern technique utilises low incisionModern technique utilises low incision• Corsetting rectus and oblique musclesCorsetting rectus and oblique muscles• Closure in jack- knife sitting positionClosure in jack- knife sitting position• Complications mostly related to tensionComplications mostly related to tension• DVT/PE increased risk if:DVT/PE increased risk if: obese, concomitant hysterectomy, liposuctionobese, concomitant hysterectomy, liposuction• Atelectasis risk when combined breast surgeryAtelectasis risk when combined breast surgery• Commonest cause of SOB: too tight dressingsCommonest cause of SOB: too tight dressings• Muscle relaxants, firm abdominal binders and Muscle relaxants, firm abdominal binders and
jack=knife positioning in a surgical bed reduce jack=knife positioning in a surgical bed reduce painpain

FaceliftFacelift
• 3 component surgery: muscle, fat, skin3 component surgery: muscle, fat, skin• Swelling and bleeding very individualSwelling and bleeding very individual• Skin survives on random pattern blood supply: Skin survives on random pattern blood supply:
tension and smoking can kill (15% smoker tension and smoking can kill (15% smoker slough )slough )
• Unilateral swelling and pain = hematomaUnilateral swelling and pain = hematoma• Bilateral tightness in the neck associated with Bilateral tightness in the neck associated with
platysma corsettingplatysma corsetting• Relative emergency for skin survival and Relative emergency for skin survival and
potential airway compressionpotential airway compression

Eyelid SurgeryEyelid Surgery
• Contents within orbital septum closed spaceContents within orbital septum closed space
• Ophthalmic vein, nerve and artery Ophthalmic vein, nerve and artery contained within the orbital septumcontained within the orbital septum
• Bleeding after surgery is an absolute Bleeding after surgery is an absolute emergency, loss of vision can occur within emergency, loss of vision can occur within 20 minutes ( 1:20,000 )20 minutes ( 1:20,000 )
• Release sutures and or lateral canthotomyRelease sutures and or lateral canthotomy
From Rees, 1996

LiposuctionLiposuction
• Traditional, wet, superwet and Traditional, wet, superwet and tumescenttumescent
• Calculation of Calculation of bloodblood loss loss
• Calculation of fluid resusitationCalculation of fluid resusitation
• Admission to hospital > 6 hours, > 6 Admission to hospital > 6 hours, > 6 litreslitres

Liposuction and fluid Liposuction and fluid rescusitationrescusitation• Traditional 150ml aspirate=drop 1% HctTraditional 150ml aspirate=drop 1% Hct
• ie > 2 L needs transfusionie > 2 L needs transfusion
• IV replacement cc for cc in OR, + cc/cc RRIV replacement cc for cc in OR, + cc/cc RR
• Tumescent: 1 L RL+ 1 cc 1:1,000 epi+ 50cc 1% Tumescent: 1 L RL+ 1 cc 1:1,000 epi+ 50cc 1% lido lido 2 ml in then > 10 minutes 1 cc 2 ml in then > 10 minutes 1 cc asp. out, asp. out,
Up to 6 L no X match requiredUp to 6 L no X match required
can use up to 35mg/kg: lido in fatcan use up to 35mg/kg: lido in fat
replace cc/cc in OR, or lessreplace cc/cc in OR, or less
• Cranberry drainage from the ports for 3 daysCranberry drainage from the ports for 3 days

Breast Augmentation +/- Breast Augmentation +/- MastopexyMastopexy
• Dressings designed to push implants downDressings designed to push implants down
• Commonest cause of SOB: dressings too tightCommonest cause of SOB: dressings too tight
• Implants over the muscle hurt much less Implants over the muscle hurt much less
• Muscle relaxants reduce pain, mostly pectoral painMuscle relaxants reduce pain, mostly pectoral pain
• Unilateral chest pain & no swelling:pneumothorax ?Unilateral chest pain & no swelling:pneumothorax ?
• Unilateral pain and swelling: hematoma ?Unilateral pain and swelling: hematoma ?
• Bilateral pain: tight dressings &/or muscle spasm ?Bilateral pain: tight dressings &/or muscle spasm ?

Post - Bariatic SurgeryPost - Bariatic Surgery
• Risk of bariatric surgery assoc BMIRisk of bariatric surgery assoc BMI• Calculation Calculation BSA=(height cms x weight kg/3600)/2 M2BSA=(height cms x weight kg/3600)/2 M2 BMI=weight kg/M2 heightBMI=weight kg/M2 height
• Procedures after: Procedures after: abdominoplastyabdominoplasty circumferential lipectomycircumferential lipectomy extended thighplastyextended thighplasty brachyplastybrachyplasty mastopexy/augmentationmastopexy/augmentation facelift and eyelid surgeryfacelift and eyelid surgery

Clinical Test case Clinical Test case 11
• 44 yr old Vietnamese male undergoes 44 yr old Vietnamese male undergoes elective cleft palate repair. S/p surgery elective cleft palate repair. S/p surgery he is noted to be cyanotic, O2 sat 85%, he is noted to be cyanotic, O2 sat 85%, inspiratory stridor, intercostal recession, inspiratory stridor, intercostal recession, labored breathing and normal neck and labored breathing and normal neck and oral examoral exam

Clinical Test case 2Clinical Test case 2
• 30 yr old 250 female with h/o bariatric 30 yr old 250 female with h/o bariatric surgery, s/p 150 pound weight loss c/o surgery, s/p 150 pound weight loss c/o SOB, tachycardia 110, 1 day post op. S/p SOB, tachycardia 110, 1 day post op. S/p abdominoplasty, O2 sat 90%, shallow abdominoplasty, O2 sat 90%, shallow breath sounds at bases of lungs, calfs breath sounds at bases of lungs, calfs non tender and feels wellnon tender and feels well

Clinical Test case 3Clinical Test case 3
•74 yr lady 1 day s/p quad blepharoplasty 74 yr lady 1 day s/p quad blepharoplasty c/o left thigh pain 1 day post op and SOB c/o left thigh pain 1 day post op and SOB with mild chest pain on coughing. Her with mild chest pain on coughing. Her HR is 110, O2 sat 88%, decreased BS at HR is 110, O2 sat 88%, decreased BS at left base and some crackles left base of left base and some crackles left base of lunglung

Clinical Test case 4Clinical Test case 4
• 4 hours after heparinization, the patient 4 hours after heparinization, the patient complains of reduced vision in the left complains of reduced vision in the left eye, there is some bulging of the eye eye, there is some bulging of the eye and some early bruising. The pupil is and some early bruising. The pupil is reactive to light and accommodationreactive to light and accommodation

Clinical Test case Clinical Test case 55
• 1 hour after abdominoplasty with liposuction 1 hour after abdominoplasty with liposuction a patient complains of extreme shortness of a patient complains of extreme shortness of breath, right sided chest pain and the urge breath, right sided chest pain and the urge to defecate. The chest exam reveals to defecate. The chest exam reveals crackles and decreased breath sounds at the crackles and decreased breath sounds at the right apex, EKG severe RBBB, blood drawn right apex, EKG severe RBBB, blood drawn for cardiac enzymes normal and serum for cardiac enzymes normal and serum lipase elevated and there are petechiae on lipase elevated and there are petechiae on the anterior chestthe anterior chest

Clinical Test case 6Clinical Test case 6
• 3 hours after abdominoplasty a 66 yr old 3 hours after abdominoplasty a 66 yr old previously hypertensive, post bariatric previously hypertensive, post bariatric patient with a history of severe patient with a history of severe lumbosacral back DJD needs high doses of lumbosacral back DJD needs high doses of PCA meds to control her abdominal PCA meds to control her abdominal dyscomfort. 5 hours after surgery her BP dyscomfort. 5 hours after surgery her BP drops to 70/50 and she becomes drousy drops to 70/50 and she becomes drousy with shallow respirations and pin point with shallow respirations and pin point pupilspupils

Clinical Test 7Clinical Test 7
• A demanding 63 yr old lady undergoes an A demanding 63 yr old lady undergoes an uneventful facelift and 6 hours after uneventful facelift and 6 hours after surgery requests IV MS just 1 hour after surgery requests IV MS just 1 hour after her last pain medication because of her last pain medication because of increased right sided facial pain. Her increased right sided facial pain. Her dressing are intact and there is no sign of dressing are intact and there is no sign of bleeding into her dressings. She says she bleeding into her dressings. She says she feels the right side of her neck is tightfeels the right side of her neck is tight

What’s New In Plastic Surgery ?What’s New In Plastic Surgery ?Rex Moulton-Barrett, MDRex Moulton-Barrett, MD
Plastic & Reconstructive SurgeryPlastic & Reconstructive Surgery
San Leandro Surgery CenterSan Leandro Surgery Center